Embed Size (px)
Citation preview
CHAPTER III
METHODOLOGY
3.1 PROBLEM:
“To identify the Emotional Intelligence, Stress, Coping Styles of
Nursing Staff in Corporate Hospitals”.
3.2 OBJECTIVES:
The objectives of the current study are:
1. To assess the Occupational stress of Nurses working in different
corporate hospitals.
2. To examine the relationship between Emotional Intelligence and
Stress.
3. To identify the efficiency of Coping Styles.
4. To study the effectiveness of intervention on Stress and Emotional
Intelligence in Nurses.
3.3 HYPOTHESIS:
1. Stress levels will be higher in Nursing Staff working in Intensive
Critical Wards as compared to the Cubical General Ward.
2. The Emotional Intelligence will be higher in Nurses working in Critical
Care as compared to other wards.
3. The higher the Emotional Intelligence the lower will be the Stress level.
4. Nurses with cognitive focused coping styles will have lower levels of
stress.
5. Nurses with cognitive focused coping styles will have higher level of
Emotional Intelligence.
6. Intervention will lower the stress level of nurses.
7. Intervention will increase the Emotional Intelligence in Nurses.
3.4 SUB-HYPOTHESIS:
a. The higher the experience of Nurses in working area the lower
will be the Stress than compared to those who are less
experienced.
b. Nurses with higher age will have high Stress as compared to
lower age.
c. Nurses with more number of work experiences have higher
Emotional Intelligence.
d. Nurses of General Nursing Midwife will have higher Emotional
Intelligence than ANMC / B.Sc.
e. Emotional Intelligence is lower in low age group Nurses.
f. Nurses working in intensive and critical area have higher
Emotional Intelligence.
g. Nurses with higher working experience will have good coping
styles.
h. Nurses with higher education will have higher Coping Styles
compared to those of other Nurses
i. Higher Coping Styles will be adopted by GNM Nurses than those
compared to ANM ONES.
j. Nurses of age 30 – 50 years have higher Coping Styles.
3.5 SAMPLE:
In this research, Working Nurses of Corporate Hospitals were
selected for the study. Target sample was 250 (Two hundred and Fifty)
working nurses in three different Corporate Hospitals were selected for the
present study. All the three hospitals are corporate hospitals with 150-350
bedded hospitals.
The various courses completed by Nurses are GNM, ANM,
B.Sc.(Nursing).
ANM – Auxiliary Nursing & Midwife course which is of 18 months
duration and those who have completed 10th Class are eligible
for this course.
GNM – General Nursing & Midwife course which is of 3 ½ Years
duration and those who have completed Intermediate are
eligible for this course.
B.Sc.(N) – Bachelor of Science (Nursing) is a 4 years degree course and
those who have completed Intermediate with Science group are
eligible for this course.
The academic qualifications of the nurses help us to understand the
maturity of the mind of nurses.
The working areas of nurses :
IP – In Patient Wards
OPD – Out Patient Ward
OT - Operation Theatre
CT - Cardiac Intensive
Post OT – Post Operated Patient Ward
INCU – Neuro Intensive Unit
LTC – Liver Transplant Unit
S.I.C. - Surgery Unit
General Ward – Two types - Male & Female Units
Cubical – Common Ward
Dialysis – Place of dialysis
Cath Lab – Unit related to Cardiac analysis
Casualty – Emergency Ward
Though male nursing staff are also working, but for the current study
data is collected from female nursing staff those who completed their
professional Diploma, Degree courses such as ANM, GNM and
B.Sc.(Nursing).
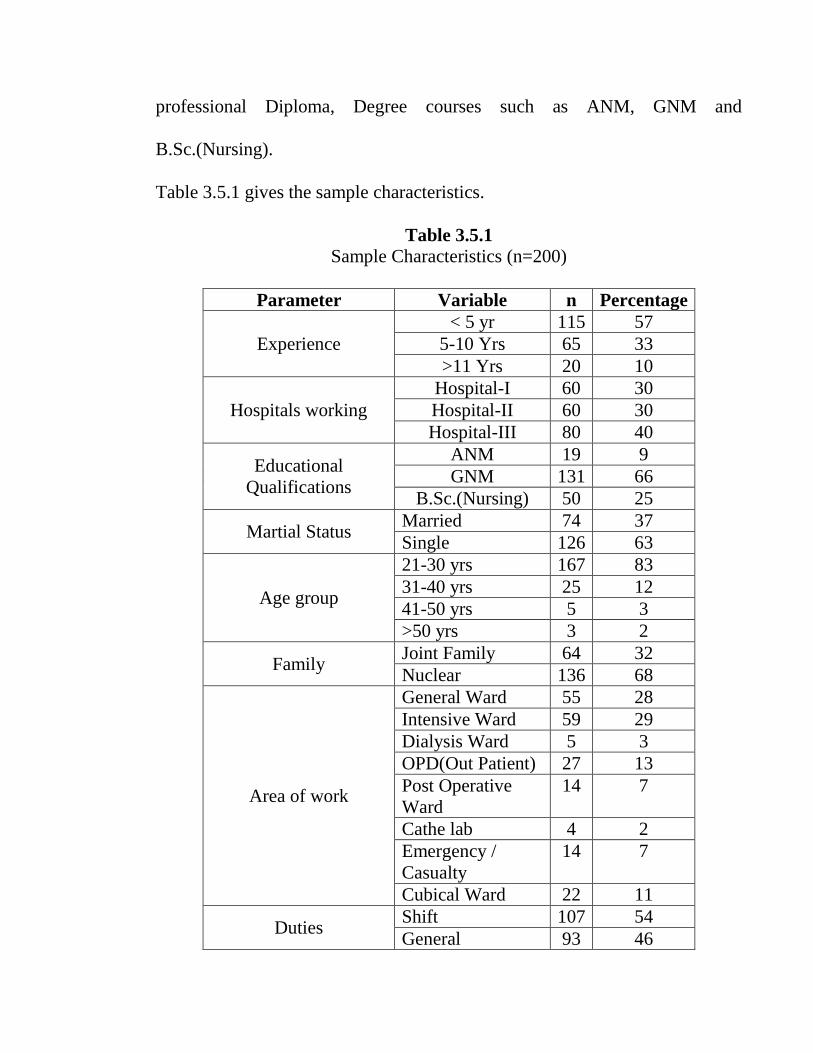
Table 3.5.1 gives the sample characteristics.
Table 3.5.1
Sample Characteristics (n=200)
Parameter Variable n Percentage
Experience
< 5 yr 115 57
5-10 Yrs 65 33
>11 Yrs 20 10
Hospitals working
Hospital-I 60 30
Hospital-II 60 30
Hospital-III 80 40
Educational
Qualifications
ANM 19 9
GNM 131 66
B.Sc.(Nursing) 50 25
Martial Status Married 74 37
Single 126 63
Age group
21-30 yrs 167 83
31-40 yrs 25 12
41-50 yrs 5 3
>50 yrs 3 2
Family Joint Family 64 32
Nuclear 136 68
Area of work
General Ward 55 28
Intensive Ward 59 29
Dialysis Ward 5 3
OPD(Out Patient) 27 13
Post Operative
Ward
14 7
Cathe lab 4 2
Emergency /
Casualty
14 7
Cubical Ward 22 11
Duties Shift 107 54
General 93 46
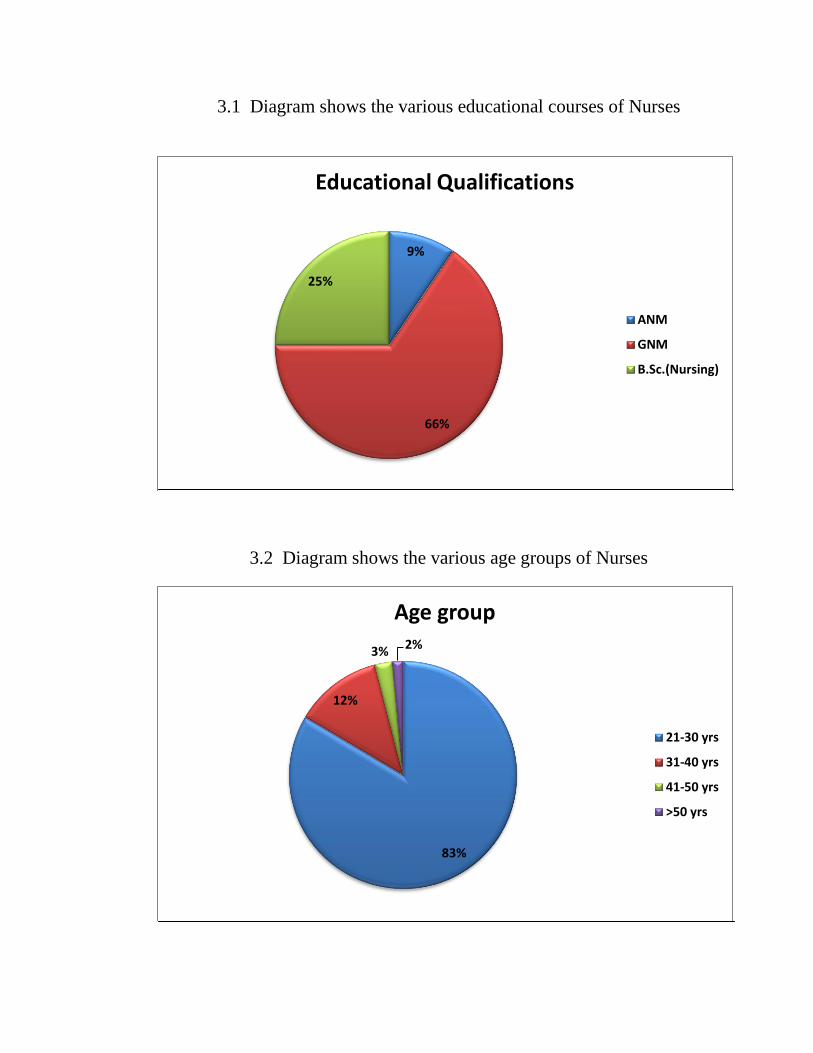
3.1 Diagram shows the various educational courses of Nurses
3.2 Diagram shows the various age groups of Nurses
9%
66%
25%
Educational Qualifications
ANM
GNM
B.Sc.(Nursing)
83%
12%
3% 2%
Age group
21-30 yrs
31-40 yrs
41-50 yrs
>50 yrs
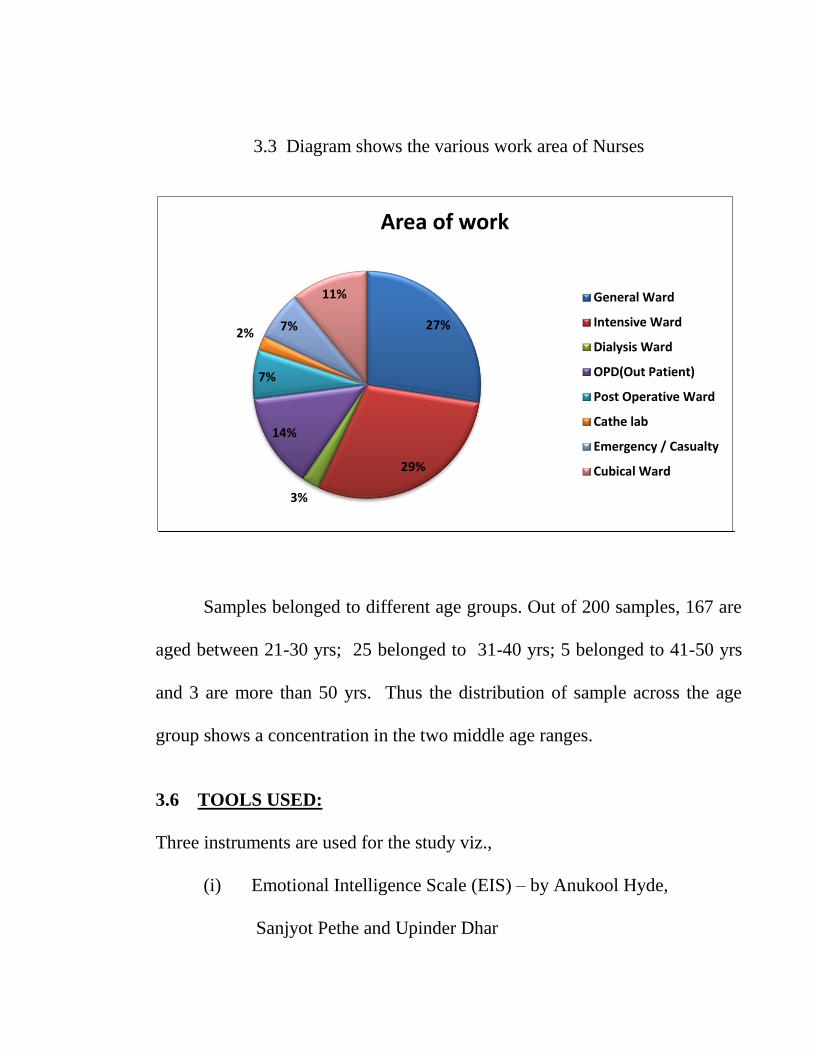
3.3 Diagram shows the various work area of Nurses
Samples belonged to different age groups. Out of 200 samples, 167 are
aged between 21-30 yrs; 25 belonged to 31-40 yrs; 5 belonged to 41-50 yrs
and 3 are more than 50 yrs. Thus the distribution of sample across the age
group shows a concentration in the two middle age ranges.
3.6 TOOLS USED:
Three instruments are used for the study viz.,
(i) Emotional Intelligence Scale (EIS) – by Anukool Hyde,
Sanjyot Pethe and Upinder Dhar
27%
29%
3%
14%
7%
2% 7%
11%
Area of work
General Ward
Intensive Ward
Dialysis Ward
OPD(Out Patient)
Post Operative Ward
Cathe lab
Emergency / Casualty
Cubical Ward
(ii) Occupational Stress Index Scale (OSIS) – by A.K.Srivastava and
A.P.Singh; and
(iii) Coping Strategies Scale (CSS) – by A.K.Srivastava.
Each of these instruments is described in detail in the following paragraphs.
(1) Emotional Intelligence Scale (E I S) :
This instrument is developed by Anukool Hyde, Sanjyot Pethe and
Upinder Dhar for suitable self-report measure for Indian milieu. The scale
purports to measure learned optimism of which the subject has some
awareness. It should not be used as a tool for individual diagnosis unless
supported by other evidences. Therefore, observation of other self-related
perceptions is also required. The scale contains 34 items (Appendix I),
measuring 10 different dimensions that are directly related to the concept of
Emotional intelligence of an individual. Each of these items were rated on a
five point scale varying from “Strongly Agree” to “Strongly Disagree” on the
degree of agreement with the statement. The subject’s emotional intelligence
is measured based on the responses of agreement with the statement. The
following table 3.5.1 gives five dimensions and the appropriate items under
each dimension.
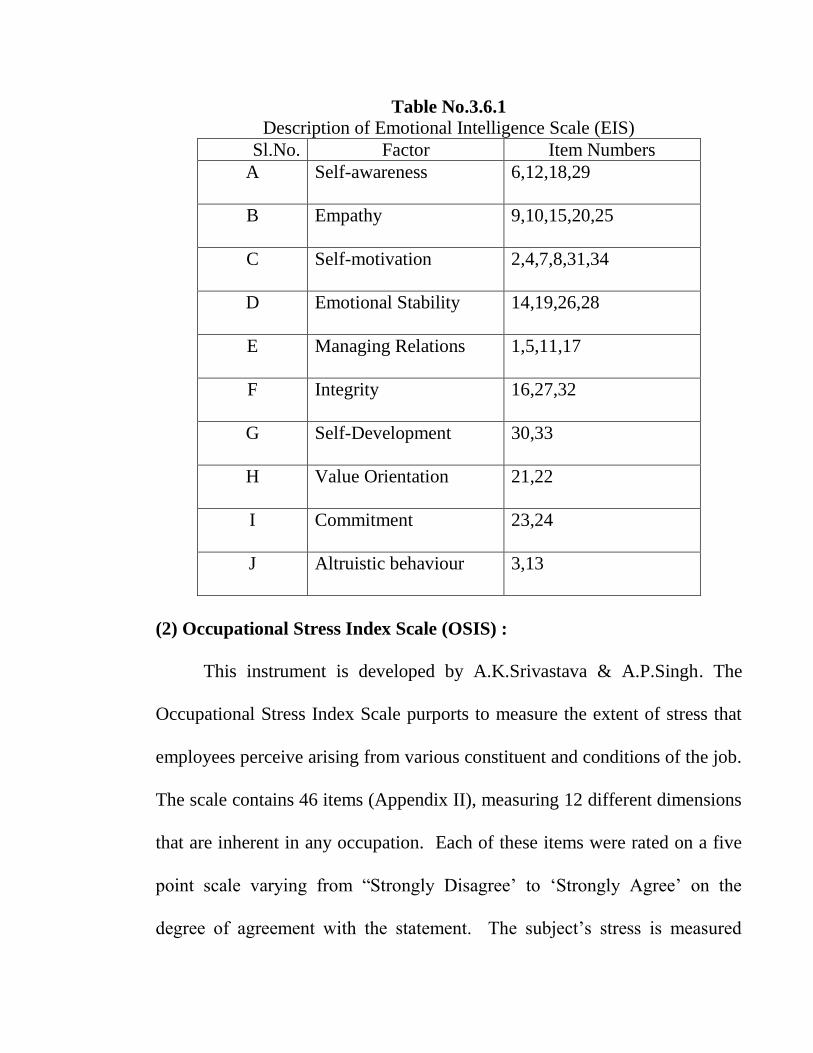
Table No.3.6.1
Description of Emotional Intelligence Scale (EIS)
Sl.No. Factor Item Numbers
A Self-awareness 6,12,18,29
B Empathy 9,10,15,20,25
C Self-motivation 2,4,7,8,31,34
D Emotional Stability 14,19,26,28
E Managing Relations 1,5,11,17
F Integrity 16,27,32
G Self-Development 30,33
H Value Orientation 21,22
I Commitment 23,24
J Altruistic behaviour 3,13
(2) Occupational Stress Index Scale (OSIS) :
This instrument is developed by A.K.Srivastava & A.P.Singh. The
Occupational Stress Index Scale purports to measure the extent of stress that
employees perceive arising from various constituent and conditions of the job.
The scale contains 46 items (Appendix II), measuring 12 different dimensions
that are inherent in any occupation. Each of these items were rated on a five
point scale varying from “Strongly Disagree’ to ‘Strongly Agree’ on the
degree of agreement with the statement. The subject’s stress is measured
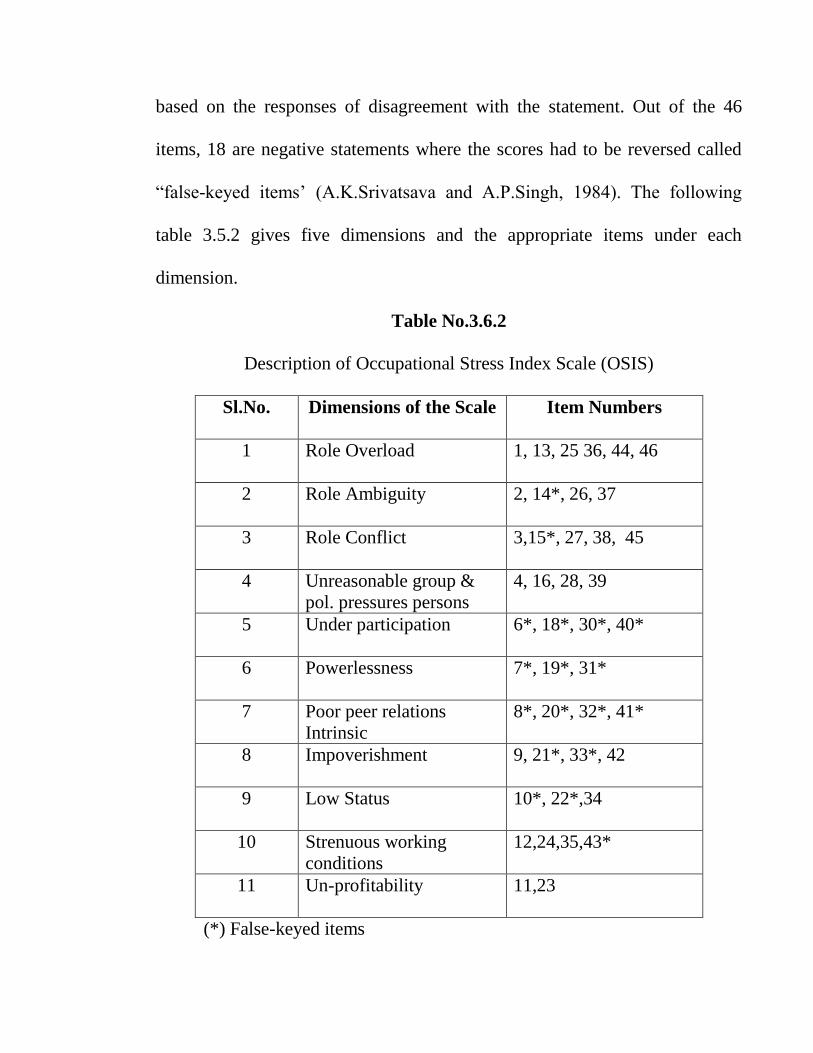
based on the responses of disagreement with the statement. Out of the 46
items, 18 are negative statements where the scores had to be reversed called
“false-keyed items’ (A.K.Srivatsava and A.P.Singh, 1984). The following
table 3.5.2 gives five dimensions and the appropriate items under each
dimension.
Table No.3.6.2
Description of Occupational Stress Index Scale (OSIS)
Sl.No. Dimensions of the Scale Item Numbers
1 Role Overload 1, 13, 25 36, 44, 46
2 Role Ambiguity 2, 14*, 26, 37
3 Role Conflict 3,15*, 27, 38, 45
4 Unreasonable group &
pol. pressures persons
4, 16, 28, 39
5 Under participation 6*, 18*, 30*, 40*
6 Powerlessness 7*, 19*, 31*
7 Poor peer relations
Intrinsic
8*, 20*, 32*, 41*
8 Impoverishment 9, 21*, 33*, 42
9 Low Status 10*, 22*,34
10 Strenuous working
conditions
12,24,35,43*
11 Un-profitability 11,23
(*) False-keyed items
(3) Coping Strategies Scale (C S S) :
This instrument is developed by A.K.Srivastava. The Coping Strategies
Scale purports to measure the extent of Coping Strategies that employees
perceive arising from various constituent and conditions of the job. The scale
contains 50 items (Appendix III), to be rated on five point scale, describing
values of coping behaviour underlying following five major categories of
Coping Strategies based on the combinations of ‘operation’ and ‘orientation’
of the coping behaviour :
1. ACTIVE / APPROCH COPING (Problem- Focused Coping)
a. Behavioural Approach Coping Strategies
b. Cognitive Approach Coping Strategies
c. Cognitive Behavioural Approach Coping Strategies
2. AVOIDANCE COPING (Emotion – Focused Coping)
a. Behavioural Avoidance Coping Strategies
b. Cognitive Avoidance Coping Strategies
Each of these items was rated on a five point scale varying from
“Never’ to ‘Almost Always’ on the degree of agreement with the statement.
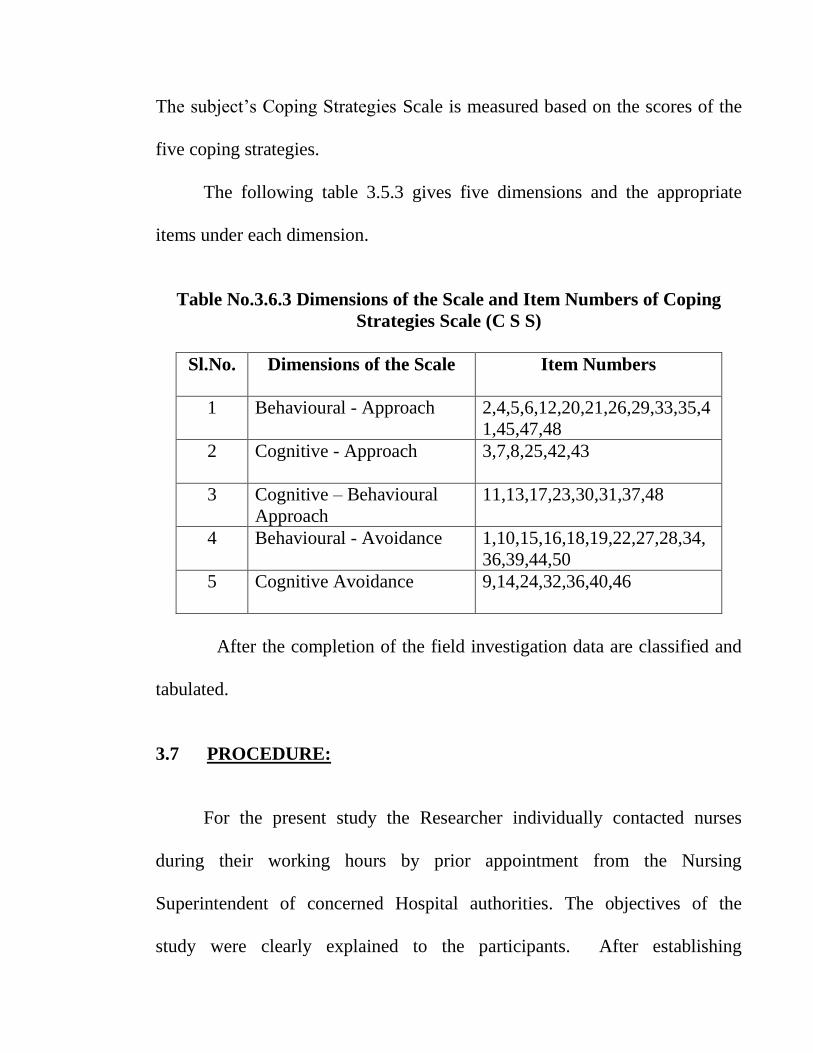
The subject’s Coping Strategies Scale is measured based on the scores of the
five coping strategies.
The following table 3.5.3 gives five dimensions and the appropriate
items under each dimension.
Table No.3.6.3 Dimensions of the Scale and Item Numbers of Coping
Strategies Scale (C S S)
Sl.No. Dimensions of the Scale Item Numbers
1 Behavioural - Approach 2,4,5,6,12,20,21,26,29,33,35,4
1,45,47,48
2 Cognitive - Approach 3,7,8,25,42,43
3 Cognitive – Behavioural
Approach
11,13,17,23,30,31,37,48
4 Behavioural - Avoidance 1,10,15,16,18,19,22,27,28,34,
36,39,44,50
5 Cognitive Avoidance 9,14,24,32,36,40,46
After the completion of the field investigation data are classified and
tabulated.
3.7 PROCEDURE:
For the present study the Researcher individually contacted nurses
during their working hours by prior appointment from the Nursing
Superintendent of concerned Hospital authorities. The objectives of the
study were clearly explained to the participants. After establishing
sufficient rapport with them, the tools for study were administered.
After making clear about the study they filled the bio-data sheet. The
nurses were requested to read the structured instructions carefully provided for
answering each scale before giving their response. They were assured that the
response would be kept confidential and used for study for Research purpose
only. They were given the Emotional Intelligence Scale and Occupational
Stress Index Scales first. On submission of these two, they were given the
Coping Strategies Scale questionnaire.
The researcher administrated the questionnaire to 250 nurses but among
250 some were incomplete while other lacked information on demographic
variables, hence they had to be discarded. Finally only 200 completed
questionnaires of nurses were available which has constituted the sample for
the present study. After obtaining the response of the subjects, scoring was
done accordingly to the guidelines specified in the test manuals.
3.8 INTERVENTION:
Intervention is a methodology in which the Nurses with stress are given
education and self management skills about the problem, counseled about
coping strategies. A person gradually learns to cope with difficult situations
on stimuli often through controlled exposure to them. The goal is to modify
and gain control over unwelcome fear, anxieties and behaviours. The study
introduces interventions which form the core of comprehensive care in the
field of nursing care.
After identifying the specific area to be focused for intervention, the
therapeutic progrommes are :
1. Counseling on psycho socio factors and other concerned stress
2. Relaxation Techniques - (Jackson) Progressive Muscle Relaxation
Technique to help Nurses develop more control over somatic symptoms
of anxiety - Brief relaxation technique like rapid relaxation (20-30
seconds)
Therapeutic progrommes are described in detail in the following
paragraphs.
Relaxation therapy:
Jacobson’s Technique - Progressive relaxation (15-20 mts) :
Relaxation Technique can help individual develop the ability not only
to manage the stresses that increase their anxiety, but also to control some of
the physical symptoms. This treatment includes breathing re-training and
exercises.
P Muscle R.Jacobson 1938, Wolpe 1958, 1969, 1973) developed by
American physician Edmund Jackson in the early 1920s PMR (PMR) is a
popular relaxation training technique for anxiety stress that works on several
basic principles. Anxiety is often associated by muscle tension so by reducing
muscle tension, anxiety reduces.
It involves that the relaxation training technique for stress requires sleep
concentration in a relaxed setting. Mentally focus on distinct muscles, muscle
groups or body parts and systematically attempt to relax each one by one. The
process is often called body scanning. Body scanning is a great way to relax
muscles prior to or after physically working out as well. Time commitment it
requires 15-20 minutes. It is alone once a day at first, than as required daily
verbal instructions can be taped to help you proceed. The first stage of
relaxation training involves the progressive relaxation technique in which the
body is divided up into a series of large muscle groups and each group is
tensed and then relaxed by attaining tension and relaxation are taught to
discriminate between these two states and to become more relaxed of the parts
of the body in which they are particularly tense. In order to facilitate tension
to natural situation, Nurses do not lie on a couch during Progressive
Relaxation Technique. Instead they are asked to sit in a comfortable chair.
First the therapist models how the different groups of muscles should be
tensed and relaxed. Later the Nurses does the various tension relax exercises
at the same time, with the therapist checking that these are done correctly.
Then the Nurse closes his / her eyes and the therapist takes his / her through
tensing and releasing the different muscle groups in the right order and at the
right tempo. Tension is normally maintained for about 5 seconds with the
subsequent relaxation of a muscle group lasting 10 – 15 seconds. Normally
each muscle group is tensed and relaxed only once. Therapist should check
whether Nurses are experiencing any problems in relaxing particular muscle
groups and help to deal with them. For the purpose of Progressive Relaxation
the body is divided into two parts. In the first session, relaxation of the hands,
arm, face, neck and shoulders is practiced. In the second session, the rest of
the body is also included. The main muscle group involved in each session
and instructions for tensing them as follows:
Session 1 – Clinch the right first, feeling tension in the forearm clinch
the left first, feeling the tension in the fist and forearm bend the elbow of tense
the biceps, keeping the hands relaxed, straighten the arm and tense the biceps
leisure the lower tri cups leaving the lower arm supported by the chair with
the hands relaxed. Winkle the forehead by raising the eyebrow bring the
eyebrows close together (as in a frown) – screw up the muscles around the
eyes tense the jaw by biting the tech together. Press the tongue hard and fist
against the root of the mouth and lips closed, notice tension in the throat. Press
the lips tightly together, push the head back as far as it will go (against a
chair) press the chin down on to the chest – hunch the shoulders up towards
the ears bend the shoulders towards the ears and circle the shoulders.
Session – 2 : First go through the exercises learnt in session 1. This
should take about 10 minutes. After completing the last shoulder exercise, go
straight into the following set of exercises breath calmly and regularly with
the stomach take a deep breath, completely fitting the lungs, hold the breath
for a few seconds then positively exhale tense the stomach muscles pull in the
stomach and the lower back away from the chair. Tense the buttocks and hip
muscles by pressing the hands to the floor keeping the legs straight. Tense the
calves by pressing the feet and toes downward tense the shrine by binding the
feet and toe upwards – continue breathing calmly and regularly with the
stomach.
Following each session the home work assignment is to practice
progressive relaxation procedure of practice on every day basis. Nurses should
choose a place and time when they will be comfortable and unlikely to be
interpreted. They should also keep a record of the time taken to relax and the
amount of relaxation achieved during each practice.
Rapid Relaxation Technique : 20-30 seconds -- 15-20 times per day
Rapid relaxation is the next phase after teaching progressive muscle
relaxation technique in applied relaxation which has two purpose (1) teaching
nurses to relax in natural in stressful situations (2) further reduce the time and
time takes to get relaxed. The goal being 20 – 30 seconds. in order to active
these goals, the person should relax 10 – 20 times a day in natural situations.
In Rapid Relaxation Technique the aim is to further reduce the time it take to
relax and give persons extensive practice in relaxing in natural, non stressful
situation. Therapist and nurses identify a series of cues which can be used to
remind the person to relax in the natural environment.
Steps:
1. Take 2-3 deep breath, slowly exhaling after each breath
2. Think relax before each exhaling
3. Scan the body for tension, and try to relax as much as possible
in the situation
Counselling: (A psycho education programme for Nurses relating to
Occupational Stress, Coping Styles and Emotional Intelligence
in work place.)
This programme of counseling help nurses to have possible change in
their areas. It is done in specific area viz., initial phase, middle phase and
termination.
After the psychological assessment of Nurses related to high stress they
were given required therapy in duration of 2 – 3 weeks and after ten week of
intervention on psychological tests the Nurses were measured in the areas of
Emotional Intelligence, Stress and Coping Styles.
Intervention was given in duration of 2-3 weeks. A gap of 2 weeks was
given depending on the grade of stress in Nurses so that intervention helped
them to activate stress levels, gain more confidence and support on coping
factors.
The whole intervention took place in duration of one month and the
plan was to assess immediate effects of the interventions. Hence after the
intervention, Emotional Intelligence, Stress and Coping Styles were assessed
to understand the effect of intervention on these functions.
Inclusion criteria:
Only female nurses
Profession – Nursing completed
Age group between 18 – 55 years
Corporate Hospitals
Working in various wards such as critical to general wards.
3.9 DATA COLLECTION:
The raw scores are collected from the response sheets of nurses. The
scoring is done as directed in the manual. Three scores viz., coping strategies,
stress and emotional intelligence of each sample are obtained. The trait
coping strategies have been scored separately with all subsets. Occupational
stress factor is also scored separately with all sub areas.
3.10 DATA ANALYSIS:
The raw scores are converted into Statistical Analysis using the
following methods:
a) Measures of Central Tendency
b) Measures of Variability
c) ‘t’ ratio to find the difference among the Group
d) Multivariate Analysis to see the trends and factors relating to
Stress.
------













![List of GNM Colleges[1]](https://img.pdfslide.us/doc/110x75/55cf987c550346d03397edec/list-of-gnm-colleges1.jpg)














