Embed Size (px)
Citation preview

Special Populations & SituationsK9 CareChapter
International Trauma Life Support Military, 3rd Edition 0
20

K9 CareBradley S Butler, MD, FACEP
CDR MC (FMF), USNEmergency Medicine Specialty Leader- Navy ReserveMedical Director- Arizona Chapter ITLSAssociate Professor- University of Arizona College of Medicine PhoenixAssociate Professor- Creighton University School of MedicineClinical Faculty- Maricopa Medical Center Emergency Medicine Residency

Conflict of Interest Disclosure
I have no conflict of interest with this presentation.

K9 Care

Objectives• Understand the importance of basic knowledge in care of the traumatically injured Military Working Dog (WMD).
• Understand the role of the dog handler in care of WMD’s.• Understand the importance and techniques of healthcare provider (HCP) safety when dealing with WMD’s.
• Describe the differences between WMD’s and human patients in the trauma setting.
• Describe initial assessment and management of WMD’s.• Describe other injuries/illnesses/situations in WMD’s. • Describe the medications and dosages for MWD’s

Pre Test QuestionWhich of the following is NOT TRUE regarding the difference between the care of canines and humans in the trauma setting?1) Normal temperature is higher for canines (102.5F)2) For canine needle decompression both sides are needled.3) Surgical airway for a canine is a tracheostomy, not a
cricothyroidotomy.4) Only IV’s can be used in canines, not I/O’s.5) Initial fluid bolus is higher in canines than humans
(90cc/kg in canines vs 20cc/kg in humans)

Introduction• Over 2,300 military working dogs (MWD’s) deployed worldwide.
• These dogs provide many capabilities to our military.• Ideally, the medical care of MWD’s will be provided by veterinarians and animal care technicians.
• Medical personnel may have to provide initial trauma care to MWD’s due to the lack of veterinarians in some of the more austere environments.
• Expectation that MWD’s will receive the highest level of resuscitative care as far forward as possible.

K9 Roles

K9 Roles

K9 Roles• PEDD‐ Patrol Explosive Detector Dog• PNDD‐ Patrol Narcotic Detector Dog• SSD‐ Specialized Search Dog• MDD‐Mine Detector Dog• IDD‐ IED Detector Dog• TEDD‐ Tactical Explosive Detector Dog• CTD‐ Combat Tracker Dog• AAA/AAT‐ Animal Assisted Therapy Dog• CWD‐ Contract Working Dog• MPC‐Multi Purpose Canine• HRD‐ Human Remains Detector

HCP Safety & Dog Handler Role• Only perform the evaluation and management of MWD’s beyond the capabilities of the dog handler when no trained veterinarian is available.
• Limited to emergency care required to evaluated/manage problems that immediately threaten life, limb or sight and to prepare the MWD for evacuation to definitive veterinary care.
• Safety of the HCP is paramount.• MWD’s are often unpredictable and potentially dangerous to those around them.
10

HCP Safety & Dog Handler Role• Ideally, the dog handler should be with the animal at all times and take the lead with MWD.
• If unavailable, the animal should be muzzled unless for emergency airway management.
• Standard muzzles.• Improvised muzzles using gauze.• Keep away from muzzle of MWD.• Use kennel for transport.
11

Anatomy & Physiology• Basic anatomy and physiology is similar• Normal size 25‐40kg (estimate 30kg)• Taking care of MWD is similar to taking care of pregnant patient– Two patients
• WMD• Dog Handler
– VS are similar except temperature• Normal temperature in WMD higher (up to 102.5 F)
– Blood pressure, heart rate, respirations similar

Airway• Evaluate like human
– Abnormal sounds: gurgling or stridor – Pawing at the muzzle.
• Jaw more mobile– Easier to intubate (prone, pull tongue forward, large tube (9‐11ETT)
– Tracheostomy (3rd/4th or 4th/5th) not cricothyroidotomy• 7‐11 cuffed ETT• 14 g angiocath for temporary

Breathing/Chest Trauma• Chest trauma common• Anatomy/Pathophysiology similar to humans• Look, listen, feel• Simple PTX, tension PTX, massive hemothorax, open PTX, rib FX, flail, pulmonary contusion.
• Treatment same as humans– Chest seal– Needle decompression with 14 g 6‐8th IC space
• Difference is both sides must be decompressed

Circulation• Anatomy/Pathophysiology similar to humans• Chest trauma common• Palpate femoral pulse
• Shock– Signs: Tachycardia, tachypnea, hypotension, AMS– Treatment
• Pressure dressings or elastic/rubber TQ• Higher volume of IVF (90cc/kg over 1 hr) NS or LR

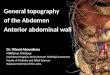
Circulation- IV AccessCephalic vein‐ foreleg Saphenous vein‐ hindleg

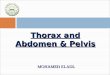
Circulation- IO Access

Circulation- IO AccessProximal/lateral humerus Proximal/medial tibia

Assessment & Management• The basic approach to MWD’s follows the same structure as in ITLS.
• Remember physiologic and anatomic similarities as well as differences when evaluating WMD’s.
• HCP safety is paramount. • Life threatening injuries in WMD’s need to be evaluated, treated, and prioritized as if they were a human patient.

Scene Size Up• The Scene Size‐up includes standard precautions, hazards, number of patients, need for additional help or equipment, and mechanism of injury
• Additional considerations– Unique situation in which you treat two patients at once. In addition, the potential second patient (the dog handler) must be involved in the evaluation and treatment of the MWD if at all possible.
– Safety of HCP’s is paramount, and the dog should be muzzled at all times if possible when it is not being directly controlled by the handler.

Initial Assessment• The initial assessment of the MWD should follow the same steps as when caring for a human– General Impression– LOC– Major bleeding– Airway– Breathing– Circulation

Rapid Trauma Survey• Head and Neck‐ can be difficult with MWD’s, due to high likelihood of airway involvement.
• Chest‐ evaluated and treated much like that in a human patient.
• Abdomen/Pelvis‐ occult bleeding common. Difficult to identify in the MWD due to the difficulty in safely examining this area and the inability for the MWD to communicate.
• Lower Extremities• Back

Interventions/Transport• Similar to human patients• REMEMBER:
– May have normal vital signs and still be critically injured. – Transport: essential to get them to definitive veterinary care as soon as possible.
– Oxygen administration, 100% by non‐rebreather or advanced airway, if required, should be rapid.
– Prompt venous access and administration of IV fluid should occur when indicated, but do not delay transport.
– Assessment of pupils and GCS are not indicated in the MWD as treatment by non‐veterinary HCP’s is not possible for significant head injuries evaluated by these exams.

Secondary Survey/Ongoing Exam• ITLS secondary Survey is not as vital in WMD’s as in human patients as only life/limb/sight threats are going to be dealt with by the non‐veterinarian HCP.
• Ongoing Exams during transport should proceed as normal ITLS, with the following special considerations. – Frequent assessment and reassessment for signs of shock and respiratory distress should take place.
– If possible, additional monitoring should include continuous pulse oximetry (on the tongue or ear).

Other Injuries/Illnesses• Musculoskeletal injuries are common in MWD’s.
– Life threatening injuries should be identified and managed first! – Manage suspected fractures using splints as in humans.– Treat open fractures as in humans, including irrigating wounds, wound dressings, and initiating antibiotic treatment.
– Suspected pelvic fractures treated by minimizing movements.
• Heat illness is common in the MWD.– Treated in a similar manner in MWD’s‐ cooling and IV hydration. – Rectal temperatures should be monitored– Aggressive cooling should be stopped when the temperature reaches 103 F (normal temperature for a MWD is up to 102.5 F)

Other Injuries/Illnesses• Burns in MWD’s are not as common as in humans, due to their fur and lack of clothing to burn the skin. – Treated the same as humans. – As in humans, pay close attention to airway involvement and intubate early if airway is involved.
• Eye injuries– Treated in a similar fashion to that in humans. – Penetrating eye injuries should have any impaled object stabilized.
– Fox shields should be utilized to patch MWD’s eyes. – Topical/oral antibiotics should be utilized, as indicated.

Other Injuries/Illnesses• Gastric Dilatation Volvulus (GDV)
– Most common in large breeds.– Occurs after recent feedings. – Presentation
• Abdominal distension• Unproductive retching
– Emergency treatment is decompression with a needle in the right or left flank, 2 fingers posterior to last rib, using a 14‐18g catheter, a 3‐way stopcock, and a 60cc syringe.
– Uncommon in MWD due to prophylactic gastropexy performed prior to deployment.

Other Injuries/Illnesses• CPR in MWD.
– In general it is not recommended. If the tactical situation and resources permit, it can be CONSIDERED in cardiopulmonary arrest due to blast injury, blunt trauma, or penetrating trauma.
– Survival rate is <<< 5%.• Euthanasia in WMD’s can be CONSIDERED by non‐veterinarian HCP’s
in the case of catastrophic injuries with poor prognosis for recovery in order to relieve the WMD of undue suffering.– 60mg/kg of pentobarbital can be used as a single agent Or– Appropriate anesthesia (such as ketamine) followed by 2 mEq/kg of KCl (potassium chloride).

Medications for MWD’s• Medications for MWD’s are similar to medications in human trauma.
• The doses are also similar. • Transfusions are not utilized. • TXA
– TXA and similar medications (epsilon aminocaproic acid) are commonly used in veterinary surgery to decrease blood loss and are proven to be safe.
– TXA be CONSIDERED in the setting of massive traumatic hemorrhage in MWD’s when able to give 1gm IV/IO in the first 3 hours.

Medications for MWD’s• Cefazolin 20‐30mg/kg IV/IO Q8hr• Ceftriaxone 25mg/kg IV/IO Q12hr• Diazepam 15‐20mg IV/IO/IM/IN/PR x 1 dose for seizures• Fentanyl 2‐10mcg/kg/hr IV/IO• Ketamine 2mg/kg IV/IO or 5mg/kg IM Q15‐60 min• Midazolam 0.3mg/kg IV/IO/IM (consider for sedation or in conjunction with ketamine)
• Morphine 0.2‐0.5mg/kg IV/IO/IM Q4hr• Ondansetron 0.1‐1mg/kg IV/IO• Propofol 1‐6mg/kg IV/IO

Summary• Increasing likelihood of being called upon to deal with an increasing number of MWD’s.
• HCP safety paramount‐ utilization of the WMD’s handler as much as possible during their care.
• Evaluate and treat only life/limb/sight threatening injuries
• ITLS evaluation and treatment is similar to humans• Transport safely and as soon as possible to definitive veterinary care.

Post Test QuestionWhich of the following is NOT TRUE regarding the difference between the care of canines and humans in the trauma setting?1) Normal temperature is higher for canines (102.5F)2) For canine needle decompression both sides are needled.3) Surgical airway for a canine is a tracheostomy, not a
cricothyroidotomy.4) Only IV’s can be used in canines, not I/O’s.5) Initial fluid bolus is higher in canines than humans
(90cc/kg in canines vs 20cc/kg in humans)

Post Test QuestionWhich of the following is NOT TRUE regarding the difference between the care of canines and humans in the trauma setting?1) Normal temperature is higher for canines (102.5F)2) For canine needle decompression both sides are needled.3) Surgical airway for a canine is a tracheostomy, not a
cricothyroidotomy.4) Only IV’s can be used in canines, not I/O’s.5) Initial fluid bolus is higher in canines than humans
(90cc/kg in canines vs 20cc/kg in humans)

SummaryFIVE KEY POINTS TO REMEMBER1) HCP Safety paramount‐muzzle MWD2) Normal temp higher in MWD (102.5 F)3) For chest injuries, NEEDLE BOTH SIDES4) Tracheostomy not cricothyroidotomy5) Fluid bolus higher‐ 90cc/kg (3 liters)