Embed Size (px)
Citation preview

Chapter 6. Results
A total of 1233 recruitment letters were mailed, and 529 persons were identified as
being eligible to participate. Of these, 348 (65.8%) completed the study (Table 6-1).
The significantly higher response from Bungendore participants is possibly explained
by the concern shared by Bungendore participants about water quality issues. Prior to
this study commencing, the Yarrowlumla Shire Council had undertaken discussions
with the local residents about the possibility of chlorinating the Bungendore water
supply.
Table 6-1. Study response rate
Unexposed Exposed
Bungendore (%) Canberra (%) Adelaide (%) Total (%)
Letters sent 412 403 418 1233
No. eligible 203 (100) 174 (100) 152 (100) 529 (100)
No. completed 147 (72.4) 110 (63.2) 91 (59.9) 348 (65.8)
χ2 = 7.38 (unexposed vs exposed); df = 1; p = 0.007
Of the 348 participants who took part in the study, 228 (65.5%) had slides scored for
micronuclei. Slides from the remaining 120 participants were found to be unsuitable for
scoring because of insufficient cells, or due to debris and bacteria covering cells
preventing a clear image of cells and micronuclei. To determine if the two groups
differed significantly, a comparison of characteristics of those participants whose slides
were scorable with those that were not scorable, was made.
82

6.1 Comparison of characteristics of participant with scorable slides
and non-scorable slides.
The comparison was made to determine whether there were differences in age
distribution, proportion of smokers, and level of education between the two groups.
6.1.1 Age distribution
Age of participants was normally distributed, and ranged from 30 – 65 years. The two
groups did not differ significantly in age distribution (Table 6-2).
Table 6-2. Mean age of participants, by slide scorability
Slides scorable n mean Std deviation
Yes 119 45.43 9.15
No 227 47.02 8.40
Total 346* 46.47 8.91
* Note: Age was missing in two records.
t = -1.58, df = 344, p = 0.12
6.1.2 Smoking
The percentage of smokers in the two groups did not differ significantly with 22.4% of
those with scorable slides, and 23.8% of those whose slides were not suitable for
scoring, being smokers (Table 6-3).
83

Table 6-3. Smoking status of participants, by slide scorability
Slides scorable Smoking (%) Non smoking (%) Total (%)
Yes 26 (22.4) 90 (77.6) 116 (100)
No 54 (23.8) 173 (76.2) 227 (100)
Total 80 (23.3) 263 (76.7) 343* (100)
*Smoking status was missing in 5 records
χ2 = 0.08; df = 1; p = 0.78
6.1.3 Education
Participants were asked to provide information on the total number of years of primary
and secondary school attended; whether they completed further education; and if so,
what was the highest level of education attained. These were optional questions. A
total of 335 participants responded to the question on the number of years of primary
and secondary schooling, with the number of years ranging from 2 – 18. The two
groups with and without scorable slides did not differ significantly with the average
number of years spent in school being 10.97 (n = 217) and 10.94 (n = 118) respectively
(t = -0.1332, df = 333, p = 0.89). Table 6-4 shows that similar proportions completed
secondary school.
The proportions of participants with further qualifications (post-secondary schooling)
were similar for both groups with 71.1% (n = 81) of those without scorable slides, and
72.7% (n = 152) of those with scorable slides completed further training or education (p
= 0.7, χ2 = 0.1029). The two groups had similar distributions in the highest level of
post-secondary school education attained as shown in table 6-5. Thirty-six percent of
84

participants with scorable slides, and 33.4% of those whose slides were not scorable,
had a bachelors degree or higher.
Table 6-4. Proportion of participants completing high school, by slide scorability
Slide scorable
No (%) Yes (%) Total (%)
No of years of schooling
< 10 years 18 (15.3) 43 (19.8) 61 (18.2)
10 – 11 years 47 (39.8) 83 (38.2) 130 (38.8)
12 – 13 years 52 (44.1) 83 (38.2) 135 (40.3)
> 13 years 1 (0.8) 8 (3.7) 9 (2.7)
Total 118 (100) 217 (100) 335 (100)
χ2 = 3.8583; df = 3; p=0.28
Table 6-5. Highest level of post-secondary school education, by slide scorability
Slide scorable Highest education level (post-secondary) No (%) Yes (%)
Total (%)
Vocational certificate
Trades certificate
Associate diploma
Full diploma
Bachelors’ degree
Graduate diploma
Masters degree or higher
Total
7 (8.6)
36 (44.4)
9 (11.1)
2 (2.5)
16 (19.8)
3 (3.7)
8 (9.9)
81 (100)
20 (13.2)
56 (36.8)
12 (7.9)
10 (6.6)
33 (21.7)
14 (9.2)
7 (4.6)
152 (100)
27 (11.6
92 (39.5)
21 (9.0)
12 (5.2)
49 (21.0)
17 (7.3)
15 (6.4)
233 (100)
χ2 = 8.6161, df = 6, p = 0.196
85

These results clearly indicate that the two groups did not differ significantly in age,
smoking status, or education level. A further comparison of available dose and fluid
intake showed that participants with and without scorable slides did not differ
significantly (table 6-6).
Table 6-6. Available dose and fluid intake, by slide scorability
Slide scorable No Yes p
Median (range)* median (range)* (ranksum) AVAILABLE DOSE (in µg/l)
Canberra (n = 25) (n = 85)
Chloroform 52 (36.5 to 68.75) 58.75 (36.5 to 68.75) 0.2 Bromodichloromethane 1.5 (0.75 to 3) 1.5 (0.75 to 3) 0.9 Dibromochloromethane 0 (0 detected) 0 (0 detected) - Bromoform 0 (0 detected) 0 (0 detected) - Total THM 53.5 (37.75 to 71.75) 59.5 (37.75 to 71.75) 0.1 AOX 230 (140 to 265) 210 (140 to 265) 0.8
Adelaide (n = 33) (n=58)
Chloroform 26 (23.2 to 29.75) 26 (23.2 to 29.75) 0.8 Bromodichloromethane 44.2 (20.25 to 51) 44.2 (20.25 to 51) 0.7 Dibromochloromethane 52.4 (21.5 to 60.75) 52.4 (21.5 to 60.75) 0.7 Bromoform 13.2 (6 to 16.5) 13.5 (6 to 16.5) 0.7 Total THM 137.5 (74 to 157.25) 137.5 (74 to 157.25) 0.7 AOX 340 (220 to 425) 340 (220.79 to 425) 0.5
FLUI D INTAKE REPORTED IN DIARY (in ml/day)
(n = 96) (n = 185)
Tap water 350 (0 to 5,150) 280 (0 to 3,050) 0.69 Hot water 925 (0 to 4,400) 965 (0 to 3,840) 0.98 Alcohol 360 (0 to 2,900) 340 (0 to 3,400) 0.08
FLUI D INTAKE REPORTED IN QUESTIONNAIRE (in ml/day)
n = 96 n = 185
Tap water 130 (0 to 3,800) 130 (0 to 4,400) 0.67 Hot water 1,000 (0 to 3,900) 1,200 (0 to 3,300) 0.48 Alcohol 240 (0 to 2,800) 200 (0 to 3,300) 0.58 * Similar ranges for available dose for both groups not unexpected because THM concentration
obtained at local sampling point was used as the available dose for all participants within that sampling zone (section 5.4.1, pages 54 - 55)
86
A comparison was then made of characteristics of study participants whose slides were
scorable, by place of residence.
6.2 Characteristics of participants with micronuclei score, by
exposure status
The term ‘participants’ from here on refers to those whose slides were found to be
scorable, and therefore have a micronuclei result. A total of 228 participants had
micronuclei results, and were therefore included in the analysis.
6.2.1 Age distribution
The age distribution ranged from 31 to 65 years. The mean age for Bungendore and
Canberra participants was 46 years, and Adelaide was 51 years (Figure 6-1). Adelaide
participants were significantly older with analysis of variance for the three groups
resulting in F = 9.52, df = 226, and p = 0.0001. Age has been adjusted for in the risk
assessment analysis.
6.2.2 Smoking
Bungendore had a higher proportion of smokers compared to Canberra and Adelaide
(Table 6-7 and Table 6-8). Smoking has also been adjusted for in the analysis.
87

Figure 6-1. Age (in quartiles) of participants by region of residence
Age
in y
ears
30
35
40
45
50
55
60
65
Bungendore (n=85) Canberra (n=85) Adelaide (n=58)
Table 6-7. Proportion of smokers by region of residence
Smoker (%) Non smoker (%) Total (%)
Bungendore 27 (32) 58 (68) 85 (100)
Canberra 13 (15) 72 (85) 85 (100)
Adelaide 13 (22) 45 (78) 58 (100)
Total 53 (23) 175 (77) 228 (100)
χ2 = 6.4921, df = 2, p = 0.04
88
Table 6-8. Proportion of smokers by exposure status
Smokers (%) Non smokers (%) Total (%)
Unexposed (Bungendore) 27 (32) 58 (68) 85 (100)
Exposed 26 (18) 117 (82) 143 (100) (Canberra +Adelaide)
Total 53 (23) 175 (77) 228 (100)
χ2 = 5.5126, df = 1, p = 0.02
6.2.3 Education
The mean number of years of primary and secondary schooling for Bungendore,
Canberra, and Adelaide were 10.5 (± 1.69) years, 11.5 (± 1.73) years, and 11.0 (±1.95)
years respectively. The median schooling years were 11, 12 and 11 years respectively.
The number of years of completed primary and secondary schooling differed
significantly for the three groups, with p = 0.007 (Anova of log transformed number of
school years. n = 217).
Table 6-9 clearly shows that a significantly higher proportion of Canberra participants
(59.5%) have completed 12 or more years of schooling compared to participants from
Bungendore (31.8%) and Adelaide (34.5%).
89
Four participants (two each from Canberra and Adelaide) had given the number of years
of schooling as 15 and above. These were verified on the questionnaires. All four of
them had further education with one each from the following categories; vocational
certificate (15 years), full diploma (18 years), bachelors degree (18 years), and masters
or higher (15 years). It is possible that they have included the number of post-school
training with the number of schooling years. These four participants were removed and
the groups compared by Anova of log transformed number of school years. The
difference was still significant with a p value of 0.01.
Table 6-9. Proportion of participants completing high school, by region of
residence
Slide scorable
Bungendore (%) Canberra (%) Adelaide (%) Total (%)
No of years of schooling
< 10 years 23 (27.1) 11 (14.9) 9 (15.5) 43 (19.8)
10 – 11 years 35 (41.2) 19 (25.7) 29 (50.0) 83 (38.2)
12 – 13 years 26 (30.6) 40 (54.1) 17 (29.3) 83 (38.2)
> 13 years 1 (1.2) 4 (5.4) 3 (5.2) 8 (3.7)
Total 85 (100) 74 (100) 58 (100) 217 (100)
χ2 = 18.7912; df = 6; p=0.005
The proportion of participants with and without further education (beyond secondary
school) did not differ did not differ significantly amongst the three groups, with 71% of
Bungendore, 70% of Canberra, 79% of Adelaide participants having post-secondary
school education (p value = 0.05). The highest level of post-secondary school
qualifications obtained is presented in Table 6-10. A relatively high proportion of
Canberra participants had a bachelor’s degree or higher qualification. The percentage
of participants with post-graduate qualifications was 27.1% for Bungendore, 53% for
Canberra, and 27.3% for Adelaide. A comparison of the unexposed group
(Bungendore) with those exposed (Canberra and Adelaide) revealed that the two groups
were not significantly different (χ2 = 3.79; df = 1; p = 0.05).
90

Table 6-10. Highest level of completed post-secondary school education obtained
by study participants, by region of residence
Highest education level
(post-secondary) Bungendore (%) Canberra (%) Adelaide (%) Total (%)
Vocational certificate 10 (16.9) 4 (8.2) 6 (13.6) 20 (13.2)
Trades certificate 25 (42.4) 13 (26.5) 18 (40.9) 56 (36.8)
Associate diploma 7 (11.9) 3 (6.1) 2 (4.6) 12 (7.9)
Full diploma 1 (1.7) 3 (6.1) 6 (13.6) 10 (6.6)
Bachelors’ degree 10 (16.9) 13 (26.5) 10 (22.7) 33 (21.7)
Graduate diploma 5 (8.5) 8 (16.3) 1 (2.3) 14 (9.2)
Masters degree or higher 1 (1.7) 5 (10.2) 1 (2.3) 7 (4.6)
Total 59 (100) 49 (100) 44 (100) 152 (100)
6.2.4 Beverage consumption
Patterns of beverage consumption were also compared among the three study groups.
Table 6-11 below presents the number, and proportions from each study community,
reporting consumption of the various beverages. The table shows that Adelaide
residents consumed less tap water at both the work place and at home. Bungendore and
Adelaide residents consumed more bottled water compared to Canberra residents.
Bungendore and Canberra residents consumed more alcohol than did Adelaide
residents. Adelaide water, although meeting both WHO and Australian Drinking water
guidelines, is of lower aesthetic quality compared to either Canberra or Bungendore. It
is therefore not surprising that Adelaide residents consume more bottled water.
91

Table 6-11. Fluid consumption by study participants during two-week study
period, by region of residence
Number (%) reporting intake
Bungendore n = 85
Canberra n = 85
Adelaide n = 58
χ2 (df) p value
Tap water*
Work water**
Bottled water
Coffee
Hot beverages
(incl. Coffee)
Alcohol
61 (72)
32 (38)
18 (21)
78 (92)
82 (96)
75 (88)
71 (84)
32 (38)
13 (15)
73 (86)
83 (98)
76 (89)
34 (59)
10 (17)
19 (33)
49 (84)
55 (95)
44 (76)
10.9 (2)
8.21 (2)
6.19 (2)
2.12 (2)
5.92 (2)
0.004
0.02
0.046
0.35
1.00***
0.05
*Tap water = tap water from the community water supply at place of residence
**Work water = water from the community water supply at work place
***Fisher’s exact test for combined Canberra / Adelaide (exposed) vs Bungendore (unexposed)
6.3 Exposure levels
Exposure levels for the three regions have been presented as available dose
(concentration of THM and absorbable organic halogen (AOX) in reticulated water),
intake dose (adjusted for individual variation in exposure), and internal dose (THM
concentrations in urine). In the following box plots created in STATA version 6, the
dots outside the box plot are outliers, defined by STATA program to be readings > 1.5
times the inter quartile range.
92

6.3.1 Available dose (concentration in reticulated water)
The unchlorinated Bungendore water contained no detectable levels of THMs. In
Canberra and Adelaide, total THM in reticulated water ranged from 37.75 – 157.25 µg/l
(mean = 88.20, std deviation = 39.73, median = 64.25). The distributions differed
significantly in the two regions (figure 6-2) with Adelaide having significantly higher
levels compared with Canberra (Mann-Whitney test: Canberra vs Adelaide: z = -10.145,
p <0.0001).
Figure 6-2. Distribution of available dose of total THM, by region of residence
Tota
l TH
M c
once
ntra
tion
in m
icro
gram
s/lit
re
0
40
80
120
160
Bungendore (n=85) Canberra (n=85)Adelaide (n=58)
The four THM compounds, when examined separately, showed that chloroform (the
principle chlorinated compound) occurred predominantly in Canberra water, while
bromoform and the mixed haloforms were found in Adelaide water (Figure 6-3 and 6-
4). The relatively higher proportion of brominated compounds in reticulated water in
Adelaide (as seen in figure 6-4) was also shown by Simpson et al in a comparison of
drinking water of Adelaide and Newcastle in NSW. The predominance of brominated
THMs in Adelaide has been attributed to the higher salinity, and occurrence of natural
93

bromide ion which reacts with the relatively higher concentration of naturally occurring
organic matter [6].
To compare the relative proportions of THM compounds in Canberra and Adelaide
reticulated water, the mean total THM concentration has been proportionately
represented in figure 6-4 such that the area of the chart represents the magnitude of
(mean) total THM in the water. The square root of the mean THM concentration was
obtained, and the graphs proportioned accordingly. Bungendore has not been included
in the comparison, as THMs were not detected in Bungendore water.
94

Figure 6-3. Distribution of available dose of THMs, by compound and region of
residence
Chloroform p value Mann Whitney test) itr
e 80
ram
s/ l
<0.0001 mic
rC
once
ntra
tion
inog
0
20
40
60
Bungendore (n= 85) Canberra (n = 85) Adelaide (n = 58)
Bromodichloromethane
0.0001
ogra 60
atio
n i
40
Con
cent
rn
mic
rm
s/ li
tre
0
20
80
Bungendore (n=85) Canberra (n=85) Adelaide (n=58)
Dibromochloromethane
ms/
litr
<0.0001
mic
rC
once
ntra
tion
inog
rae
0
20
40
60
80
Bungendore (n=85) Canberra (n=85) Adelaide (n=58)
Bromoform
0.0001
ogra
m
once
ntr
20
Cat
ion
in m
icr
s/ li
tre
0
40
60
80
Bungendore (n=85) Canberra (n=85) Adelaide (n=58)
95

Figure 6-4. Proportionate representation of mean total THM concentrations in Canberra and Adelaide reticulated water (Available dose)
Canberra – Mean total THM = 57.74
Canberra
Dibromochloro-methane 37.9%
Bromoform 9.8%
Adelaide – Mean total THM = 133.09
Bromodichloro-methane 2.2%
µg/l
Chloroform 97.8%
Bromodichloro-methane 32.4%
Chloroform 19.8%
µg/l
96

AOX levels in Canberra ranged from 140 – 265 µg/l, with mean and standard deviations
being 219.29 µg/l and 33.78 µg / l respectively (n=85). In Adelaide, AOX
concentrations ranged from 220 – 425 µg/l with mean and standard deviations of 327.33
µg/l and 59.18 µg/l respectively (n=58). These concentrations differed significantly
with t = -13.8558; p<0.0001. Bungendore was not included in the comparison as no
AOX was detected in Bungendore water. AOX distributions have been graphically
represented in Figure 6-5.
Figure 6-5. Mean AOX concentration in quartiles for reticulated water, by region
of residence
00
100
200
300
400
500
Bungendore (n=85) Canberra (n=85) Adelaide (n=58)
Con
cent
ratio
n in
µg/
litre
6.3.2 Intake dose (available dose adjusted for individual beverage consumption)
The following section describes intake dose for study participants, as estimated by fluid
intake diary records and by a retrospective questionnaire. All intake dose distributions
showed extreme negative skewness. Intake dose of total THM from the fluid intake
diary was nil for all Bungendore participants (since the water contained no DBPs) while
the estimates for Canberra and Adelaide ranged from 2.9 to 469.5 µg/kg -day (mean =
97

139.9 µg/kg - day, std deviation = 95.6 µg/kg-day, and median = 117.6 µg/kg-day). The
estimate using retrospective questionnaire ranged from 0 to 409.4 µg/kg-day, (mean =
35.4 µg/kg-day, std deviation = 82.8 µg/kg-day, and median = 20.0 µg/kg-day). Figure
6-6 presents the distributions in quartiles for the three study communities. The Mann
Whitney test comparing Canberra and Adelaide showed that the distributions of the
individual THM compounds differed significantly between the two communities (by
both estimates), with all p values being <0.0001. Adelaide water contained a
significantly higher proportion of brominated compounds. This is due to the trace
amounts of bromide ions in Adelaide raw water supply and preferential formation of the
bromide by-products. Intake dose of total THMs, when estimated by fluid intake diary
records, differed significantly between the two groups, with Adelaide having
significantly higher levels (p = 0.03). The estimate by of total THM intake by
retrospective questionnaire however, did not differ significantly (p=0.2).
Chapter seven provides a comparison of fluid intake estimates made by fluid intake
diary and questionnaire. Although the two estimates did not differ greatly, wherever
intake dose was used in a regression analysis (chapter eight), the analysis was
undertaken using both estimates of intake dose (i.e. by fluid intake diary and
questionnaire).
98

Figure 6-6. Distributions of intake dose of THM as estimated by fluid intake diary
and retrospective questionnaire, for the three study communities
Fluid intake diary Retrospective questionnaire
Chloroform
0B ) C
Bromodichloromethane
50
100
150
200
250
300
350
ungendore (n=85 anberra (n=85) Adelaide (n=58)0
50
100
150
200
250
300
350
400
Bungendore (n=85) Canberra (n=85) Adelaide (n=58)
Inta
ke d
ose
in m
icro
gram
s/kg
-day
0
50
100
150
Bungendore (n=85) Canberra (n=85) Adelaide (n=58)
Inta
ke d
ose
in m
icro
gram
s/kg
-day
0
50
100
150
Bungendore (n=85) Canberra (n=85) Adelaide (n=58)
Con
cent
ratio
nin
mic
rogr
ams/
liter
Inta
ke d
ose
in m
icro
gram
s/kg
-day
Inta
ke d
ose
in m
icro
gram
s/kg
-day
Cont’d
99

Figure 6-6. Cont’d. Distributions of intake dose of THM as estimated by fluid
intake diary and retrospective questionnaire, for the three study communities
Dibromochloromethane
100100
Inta
ke d
ose
in m
icro
gram
s/kg
-day
Bromoform
Total THM
0
25
50
Bungendore (n=85) Canberra (n=85) Adelaide (n=58)0
25
50
Bungendore (n=85) Canberra (n=85) Adelaide (n=58)
0
100
200
300
400
500
Bungendore (n=85) Canberra (n=85) Adelaide (n=58)0
100
200
300
400
500
Bungendore (n=85) Canberra (n=85) Adelaide (n=58)
Inta
ke d
ose
in m
icro
gram
s/kg
-day
Inta
ke d
ose
in m
icro
gram
s/kg
-day
0
50
150
200
Bungendore (n=85) Canberra (n=85) Adelaide (n=58) 0
50
150
200
Bungendore (n=85) Canberra (n=85) Adelaide (n=58)
Inta
ke d
ose
in m
icro
gram
s/kg
-day
Inta
ke d
ose
in m
icro
gram
s/kg
-day
Inta
ke d
ose
in m
icro
gram
s/kg
-day
100

6.3.1 Internal dose (concentrations in urine)
Internal dose for Canberra and Adelaide were also distributed with negative skewness.
Total THM concentrations in Canberra ranged from 0 to 6.82 µg/l (mean = 0.67 µg/l,
std deviation = 1.17 µg/l, median = 0.33 µg/l), while Adelaide had levels ranging from
0.1 to 3.14 µg/l (mean = 0.60 µg/l, std deviation = 0.51 µg/l, median = 0.48 µg/l). As
expected, no THMs were detected in urine of Bungendore participants. This
demonstrated that the Bungendore participants (i.e. the unexposed group) were not
exposed to THMs from other sources. The distributions of internal dose are compared in
Figure 6-7 and show numerous outliers defined by Stata to be readings > 1.5 times the
inter quartile range.
The Mann Whitney test was employed to effect a meaningful comparison of exposure
of Canberra and Adelaide trial participants (figure 6-7). Overall exposure to THMs was
highest in Adelaide. Adelaide has highly modified local water supply catchments and
also relies on Murray River water pumped from Mannum. Natural organic matter levels
are relatively high and, while strenuous efforts have been made to avoid DBP formation
in recent years, THM levels are still relatively high by international standards. Since
Adelaide water is slightly brackish and contains small amounts of bromide ion, the
proportion of brominated DBPs and THMs is higher in Adelaide than in Canberra
water.
Overall, however, the amounts of bromoform are similar in both Adelaide and Canberra
water. The amount of chloroform in Canberra water is actually higher than for
Adelaide, but when the mixed bromochloro-THMs are taken into account, the total
exposure of Adelaide participants to THMs (and to AOX) is actually much higher.
101

Figure 6-7. Distribution of internal dose of THM concentrations (in quartiles), by
compound and region of residence
Chloroform Mann Whitney test
p = 0.0001
og
ram
sco
ncen
tratio
n in
mic
r/li
tre
0
.5
1
1.5
2
Bungendore (n=85) Canberra (n=85) Adelaide (n=56)
Bromodichloromethane
p <0.0001
ogra
ms
e
2
conc
entra
tion
in m
icr
/litr
0
1
Bungendore (n=85) Canberra (n=85) Adelaide (n=56)
Dibromochloromethane
p <0.0001
gra 4
conc
entra
tion
in m
icro
ms/
litre
0
2
6
Bungendore (n=85) Canberra (n=85) Adelaide (n=56)
Bromoform 6
p = 0.08 tre
rogr
a 4
conc
entra
tion
in m
icm
s/li
0
2
Bungendore (n=85) Canberra (n=85) Adelaide (n=56)
102

Figure 6-7 cont’d. Distribution of internal dose of THM concentration (in
quartiles), by region of residence
Mann Whitney test t p = 0.01 8
conc
entra
tion
in m
icro
gram
s/lit
re
0
2
4
6
otal THM
Bungendore (n=85) Canberra (n=85) Adelaide (n=56)
Internal dose for total THM has been proportioned graphically in figure 6-8. It depicts
the abundance of the individual compounds. In comparison to available dose of total
THM shown in figure 6-4 where only chloroform and bromodichloromethane were
detected in Canberra water, in urine, bromine compounds accounted for over 70% of the
total THM components. There are several possible reasons for this difference in THM
components in water and urine. A likely explanation is that the assay used for THMs in
urine had a lower detection level (of 0.01 µg/l) compared to the assay used for water
(0.1 µg/l). It is therefore possible that the bromine compounds may have been present
in low concentrations in the water, but not at levels sufficient to be detected with the 0.1
µg/l threshold level. This does not however explain the difference in the proportions of
the various compounds in water and urine and is therefore an unlikely proposition.
Bromoform is used in food processing, and is a potential – if not a highly probable -
source of exposure to this compound. Chloroform, which is highly volatile can be
easily lost by evaporation, or by being metabolised.
103

In the presence of bromine, even at vanishingly low concentrations, brominated DBPs
are formed in water from organic matter - in the presence of hypochlorous acid - in
preference to chlorinated byproducts. To explain the higher proportion of bromine
compounds in urine, it is necessary to assume that either the more volatile fractions
(mainly chloroform) are selectively removed and expired or that selective
biodegradation of chloroform and C-Cl bonds of mixed trihalomethanes occurs in vivo.
A much less likely proposition is that carbon-chlorine bonds are replaced by bromine in
vivo and that the water source makes a critical contribution to body bromide levels.
What is also clear from comparing available and internal doses of total THM is that,
with available dose, Adelaide had a higher mean total THM level compared to
Canberra, whereas with internal dose, mean total THM was higher in Canberra. This is
possibly explained by the differences in true exposure between the two communities.
Even though the reticulated water in Adelaide had higher concentrations of THMs, tap
water intake in Adelaide was shown to be lower in Adelaide when compared with
Canberra (table 6-10). It was noted from interviews (although this information was not
formally collected) that many Adelaide residents used rainwater tanks for domestic use
including showering. Exposure is also determined by dermal and inhalation exposure.
Combining the lower tap water intake and possible use of other sources of water for
domestic use, it is highly likely that Adelaide participants are exposed to less THMs
than the Canberra participants are. This would result in lower concentrations of THMs
in the body, resulting in lower internal dose. This further highlights the importance of
individual exposure assessment and the benefits if using a biological marker rather than
estimating exposure from interview data.
104

Figure 6.8. Proportionate representation of mean total THM concentrations in urine of Canberra and Adelaide participants (internal dose)
Chloroform 13.8%
Bromoform 61.3%
Canberra – Mean total THM = 0.80 µg/l
Bromodichloromethane13.8%
Dibromochloromethane 11.3%
Dibromochloro-methane 7.7%
Bromodichloro-methane 32.3%
Bromoform 41.5%
Chloroform 18.5%
Adelaide – Mean total THM = 0.64 µg/l
105

6.4 Outcome – Micronuclei frequency
The prevalence of micronuclei in bladder epithelial cells has been summarised by
region, in table 6-12. The total number of cells scored for Bungendore, Canberra and
Adelaide were 127 431, 74 585, and 52 781 respectively. The average numbers of cells
scored per participant for the three regions were 929, 496, and 430 respectively.
Although it was intended to score a minimum of 1000 cells per participant, the density
of cells on slides did now enable as large numbers as that to be scored per participant.
Table 6-12. Unadjusted prevalence of micronuclei in bladder epithelial cells, by
region
Cells % abnormal micronuclei per 1000 Counted* cells normal cells
range mean median
Bungendore (n=85) 127,431 34.0 0 to 22.7 1.7 0.9
Canberra (n=85) 74,585 32.9 0 to 11.4 1.0 0.4
Adelaide (n=58) 52,781 37.1 0 to 20.4 1.7 0.1
* Cells counted = normal and degenerated / abnormal cells
The proportion of abnormal cells did not differ significantly between the three regions,
with 32.9 to 37.1% of cells being abnormal. A chi-square test was performed to
compare the expected proportions: this resulted in p=0.78 (χ2 = 0.50; df=2).
Flow cytometry data have been described in chapter nine.
106

6.5 Association between exposure and outcome
Scatter plots examining associations between the exposure indices and prevalence of
micronuclei did not show an obvious linear or non-linear association (appendices 1 to
3a). Detailed assessment of the association using regression models, is presented in
chapters 8 and 9.
6.6 Association of potentially confounding variables with exposure
and outcome
The potentially confounding variables were examined for associations with the exposure
indices (appendices 4 to 7). The variables were not correlated with the highest
correlation coefficient being 0.40 between available dose of chloroform and serum
folate levels (appendix 4).
Potentially confounding variables were also examined for associations with the
frequency of micronuclei (appendix 8). Lifetime history of working with paint, and
lifetime history of working with leather as part of a hobby were the only two variables
that were significantly associated with the outcome measure. Of these, the former
association was protective (rr=0.61, 95% CI 0.41 to 0.92). This is likely to be a chance
occurrence more than a true estimate of effect.
The variables considered as potential confounders in this study are factors that are
known to be risk factors for bladder cancer and / or known to effect cell integrity. The
confounding role of these variables has been assessed further in chapter eight by
examining the effect of introducing these variables in to the regression analysis.
107

6.7 Bladder cancer incidence in the three study communities
Prior to examining the association between exposure to THM and frequency of
micronuclei at an individual level for study participants, the rates for bladder cancer (for
which micronuclei is being used as an early pre-clinical marker) for the three study
communities was examined. Bungendore is situated within the Local Government Area
(LGA) of Yarrowlumla. This LGA mainly consist of rural villages where community
water supplies are not chlorinated.
Table 6-13. Bladder cancer incidence rates for the study communities
Males Females n ASR1 ASR2 n ASR1 ASR2 (Australia 1991) (World) (Australia 1991) (World)
Yarrowlumla NSW 1991-953 2 - 10.9 0 - 0 ACT 1985-894 11 - 11.6 4 - 2.9 ACT 1991-955 12 15.6 4 - 4.3 ACT 1992-966 15 17.6 - 4 3.7 - ACT 1993-977 15 17.2 - 5 4.1 - SA 1985-894 119 - 12.5 41 - 3.2 SA 1991 –955 122 17.0 41 - 4.2 SA 1992-966 124 17.0 - 40 4.0 - SA 1993-977 125 16.7 - 43 4.2 - Australia 85-894 1609 - 15.2 563 - 4.3 Australia 91-955 1976 23.7 15.9 646 6.1 4.2
Australia 93-977 1986 22.6 15.1 695 6.2 4.2 1 Age standardised incidence rates using Australian Population Standard, per 100,000 population 2 Age standardised incidence rates using World Population Standard, per 100,000 population 3 Source: [91] 4 Source: [92] 5 Source: [93] 6 Source: [94] 7 Source: [46] 108

Comparable incidence rates were available for the years 1991 to 1995, although
incidence rates adjusted for World Standards were not available for ACT and SA. By
examining available information, it may appear that the ASR (adjusted for World
Standards) show a trend with increasing rates going from Yarrowlumla LGA, to ACT,
and SA. This may very well suggest a correlation between chlorination and bladder
cancer incidence rates. This picture is however not so clear when examining subsequent
incidence rates for 1991-95, 1992-96 and 1993-97, which have been adjusted for the
Australian Standard 1991. Here, ACT and SA have similar incidence rates, which are
lower than the overall Australian rates. The higher Australian rate is due to the high
incidence rates in VIC, QLD and TAS, where incidence rates are in the high 20’s [93],
[94], [46]. Without knowing the chlorination and DBP levels in these States, it is not
possible to know whether this information supports the association between chlorination
and bladder cancer.
An ecological comparison such as this does not take into account other factors that may
be contributing to the observation of bladder cancer incidence rates. The prevalence of
other risk factors to bladder cancer (such as cigarette smoking, use of pesticides or
chemicals) may differ between these communities and may be contributing to the
observed differences in bladder cancer incidence.
Such an ecological comparison can however suggest an association between the two
factors (chlorination level and bladder cancer), and would justify further investigation of
this association.
109

Chapter 7. Estimation of fluid intake by diary records
and by retrospective questionnaire
The study presented in this dissertation builds on previous studies by assessing exposure
at an individual level. In order to estimate individual exposure to disinfection by-
products (DBP) from drinking chlorinated water, participants were asked to report fluid
intake over a two-week study period. This was achieved using two methods, a fluid
intake diary and a retrospective interviewer administered questionnaire.
7.1 Aim
The aim of this component of the study was to assess the level of agreement between
two methods for estimating fluid intake, using fluid intake diary records and using a
retrospective interviewer administered questionnaire. Comparisons were made for tap
water, water based hot beverages (coffee and tea), and for alcohol intake.
7.2 Methods
The study period was of two-week duration. During which time, participants were
asked to keep a record of all beverages consumed. A fluid intake diary was provided
for this purpose. At the end of the two-week period, a questionnaire was administered
by telephone to recall fluid intake for the duration of the study period.
110

7.2.1 The diary
The diary was based on a format presented by Armstrong et al, and modified to suit the
purpose of this study [95, page 210]. A member of the research team met with the
participants individually and explained the procedure. Participants were instructed to
record fluid intake at least on a daily basis. Information to be recorded on the page per
day diary included date, time, type of drink, amount (using a code), number of serves,
and place (Appendix 26). Time was included to aid participants to recall fluid intake
over the day, especially if they were recording on a daily basis instead of on an ongoing
basis. For the ‘amount’ pre-coded categories were provided. e.g. cup, mug, small glass,
medium glass etc. Space was allocated to place where beverage consumed. This
information was to determine the chlorination status of the water consumed.
Intake volume for the two weeks was computed by converting the amount or portion
size in to milliliters (ml) and summing intake by beverage type. This was then
converted to average daily intake.
7.2.2 The questionnaire
At the end of the two-week period, a member of the research team telephoned the
participant and administered a questionnaire to independently determine fluid intake
over the study period, without referring to the diary. The participants were asked to
recall what he or she had to drink over the preceding two weeks, without reference to
diary records. The questions were worded as follows:
Have you drunk tap water in the last two-weeks?
If No, the interviewer would go on to the next beverage. If Yes:
Was it every day, every week, or less often?
111

If the participant had responded every day, he was asked:
On average, how many drinks would you have had a day?
Or if every week:
On average, how many drinks would you have had per week?
Or if less often:
How many drinks in total would you have had in the last two weeks?
This was followed up by:
What size portion did you usually have? Was it a cup, mug, small, medium, or
large glass, half bottle, small or large bottle?
Intake volume over the two-weeks was calculated for each beverage using the following
formula:
{(portions per day x portion size in ml) x 14} + {(portions per week x portion
size in ml) x 2} + one-off intake in ml
Average daily intake was computed from this information.
With both methods, conversion of amount or portion size to volume consumed was
done using the following conversion rates.
Cup = 250 ml Half bottle/stubbie/normal can = 375 ml
Mug = 300 ml Standard bottle = 750 ml
Small glass/pony = 100 ml Half nip = 15 ml
Medium glass/middy = 284 ml Nip = 30 ml
Large glass/schooner = 425 ml Double nip = 60 ml
Small bottle/can = 285 ml Other = as specified
Beverages were grouped in to broad categories. The main groups of interest were tap
water, water based hot beverages (coffee and tea), and alcohol. With each beverage, if
no intake were reported, it was assumed that there was no intake of that beverage during
the study period, and therefore entered in the database as zero intake.
112

7.2.3 Comparison of fluid intake estimates
Diaries and questionnaires that had been incompletely filled were not used for the
comparison. Statistical comparison of the two methods was undertaken using two
techniques. The first technique utilised a method recommended by Bland and Altman
for method comparison studies [96], [97, chapter14.2]. The two variables were plotted
against each other, followed by plotting the average readings against the difference at an
individual level. This provides a graphical estimate of the differences.
The second technique for comparing fluid intake estimates made by the two methods
was the kappa test. Water intake was categorised in quintiles, and the level of
agreement between categories was examined by weighted kappa test. When dividing in
to quintiles, if zero intake was the 20th centile, zero was categorised as the first category,
and the rest were equally divided in to four groups. Kappa was used because it is a
quantitative method of assessing level of consistency between two methods used on the
same subject, whether it be by two observers, on two occasions, or using two
procedures. Kappa is the usual test to assess agreement in dietary records. Weighted
kappa is used here giving different weights to the magnitude of difference. For
example, in using weighted kappa, a difference of one category is considered to be less
of a discrepancy than a difference of two or three categories.
7.2.4 Test-retest reliability of questionnaire
The ability for an instrument to reproduce results when used at a different time (i.e.
reliability of questionnaire) was tested for in Bungendore only for logistic reasons.
113

Administering the questionnaire a fortnight after administering the initial retrospective
questionnaire tested repeatability. The period of recall was the preceding two-weeks,
i.e. the two weeks since administering the last questionnaire. Due to the demand on
respondent time, repeatability of fluid intake diary was not conducted.
7.3 Results
A total of 281 participants had complete records for diary and questionnaire. These
records were used in the comparison presented here. All participants were males due to
a selection criterion set for the main study, and they were aged between 30 and 65 years
(section 5.3).
7.3.1 Fluid intake
According to the fluid intake diary, 81.9% of participants drank tap water, 97.5% drank
hot beverages, and 92.5% drank alcohol during the study period. The retrospective
questionnaire identified a lower intake of tap water (70%) and alcohol (83.3%) intake in
terms of both proportion consuming and amount consumed (Table 7-1). Hot beverage
consumption did not differ greatly except for a small increase in the amount estimated
by questionnaire.
7.3.2 Bland and Altman Method
Plotting of fluid intake by diary records versus questionnaire (figure 7-1) indicate that
there is a linear relationship between the two variables. As with most of such data, there
is clustering of points at the base making it difficult to assess the differences.
114

Table 7-1. Beverage consumption pattern during the study period, as estimated by diary records and by questionnaire
Daily Intake in ml (rounded to the nearest 100 ml)
Diary (n=281) Questionnaire (n=281)
Beverage type
Number reporting beverage
consumption (%)
Range Median Number reportingbeverage
consumption (%)
Range Median
Tap water 230 (81.9) 100 – 5200 300 191 (70.0) 100 - 4400 100
Hot beverages 274 (97.5) 100 – 3400 1000 272 (96.8) 100 - 3900 1100
Alcohol 260 (92.5) 100 – 4400 400 234 (83.3) 100 - 3300 200
115

Figure 7-1. Scatter plots of diary versus questionnaire intake estimates
Spearman rank correlation
Tap water r = 0.74 5.
Dia
ry e
stim
ate
in
l/day
questionnaire estimate - in l/day0 2.2 4.4
0
2.6
2
Hot beverages r = 0.84 2.
Dia
ry e
stim
ate
- in
l/day
questionnaire estimate - in l/day0 1.25 2.5
0
1.05
1
Alcohol r= 0.76 2.
Dia
ry e
stim
ate
- in
l/day
questionnaire estimate - in l/day1.0
0 2.00
6
1.3
116

Plotting of differences between the two variables (diary – questionnaire) showed the
scatter of difference increasing as the average of the two measures increase, i.e. the
difference is proportional to the mean (figure 7-2). The recommendation for this
situation by Bland and Altman is to plot log transformed data. However, the authors
also mention that due to the complexity of interpreting back transformed data, only log
transformation is recommended for this technique. The fluid intake data contains many
zeros, and log transformation requires further manipulation. The back transformation
results in negative numbers, which as indicated by Bland and Altman, are difficult to
interpret. Therefore, in spite of large standard deviations obtained, raw data are used to
examine any difference.
Figure 7-2 also includes the 95% confidence intervals demonstrating the limits of
agreement. With tap water, the mean difference (diary – questionnaire) was 13.6
ml/day. Based on these data, questionnaire intake of tap water could under estimate or
exceed diary intake by about 1200 ml/day. Similarly, the mean difference in hot
beverage intake was not big at 169 ml/day, but the difference could be anything from
about -1000 to 700 millilitres. A similar difference was observed with alcohol intake.
These differences are not huge, but the impact would depend on the purpose of the
comparison.
117
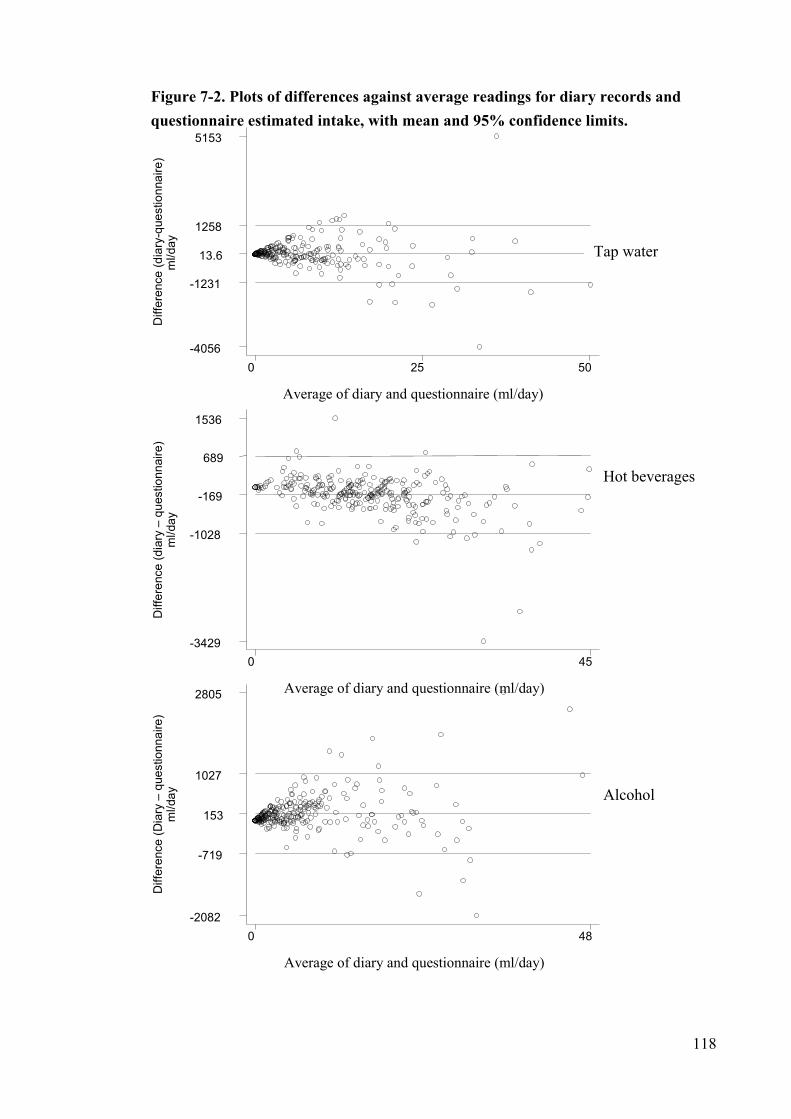
Figure 7-2. Plots of differences against average readings for diary records and questionnaire estimated intake, with mean and 95% confidence limits.
1258
s
Diff
eren
ce (d
iary
-que
stio
nnai
re)
ml/d
ay
Average of diary and questionnaire (ml/day)
0 25 50-4056
-1231
13.6
5153D
iffer
ence
(dia
ry –
que
stio
nnai
re)
ml/d
ay
Average of diary and questionnaire (ml/day)
0 45-3429
-1028
-169
689
1536
Diff
eren
ce (D
iary
– q
uest
ionn
aire
)m
l/day
Average of diary and questionnaire (ml/day)
0 48-2082
-719
153
1027
2805
Hot beverage
AlcoholTap water
118
7.3.3 Kappa test
Test for level of agreement using quintiles of intake revealed good to very good
agreement (table 7-3). Interpretation of kappa values is based on guidelines provided by
Altman.
Value of κ Strength of agreement <0.20 Poor
0.21 – 0.40 Fair
0.41- 0.60 Moderate
0.61 – 0.80 Good
0.81 – 1.00 Very good
(Source: [97, page 404])
119

Table 7-2. Level of agreement between fluid intake diary and questionnaire
Quintiles
1 2 3 4 5 Total Weighted
Kappa (95% CI)
Tap water
1 53 1 0 1 0 55
2 18 22 13 3 1 57
3 9 15 18 11 4 57 0.68
4 6 4 10 23 13 56 (0.57 to 0.80)
5 4 6 5 12 29 56
Total 90* 48 46 50 47 281
Hot beverage
1 42 11 1 0 1 55
2 13 28 14 1 0 56
3 0 14 28 12 4 58 0.84
4 0 3 13 27 13 56 (0.72 to 0.96)
5 1 0 1 16 38 56
Total 56 56 57 56 56 281
Alcohol
1 34 16 4 1 0 55
2 13 24 17 3 0 57
3 5 12 19 19 2 57 0.78
4 1 4 13 27 11 56 (0.66 to 0.90)
5 1 2 3 7 43 56
Total 54 58 56 57 56 281
*All zero intake
120

7.3.4 Test-rest reliability
Of the original 147 participants from Bungendore, 139 completed the retrospective fluid
intake questionnaire two-weeks after completing the initial questionnaire. Short-term
repeatability of the retrospective questionnaire (after two-weeks) was found to be
moderate with Spearman’s correlation coefficients and kappa values for the three
beverage groups ranging from 0.51 to 0.56 (Table 7-3).
Table 7-3. Repeatability of the retrospective fluid intake questionnaire
Beverage
Spearman’s correlation
coefficient
Kappa value (95% CI)
Tap water Hot beverages Alcohol
0.55
0.51
0.56
0.55 (.039 to 0.72)
0.51 (0.35 to 0.67)
0.56 (0.40 to 0.72)
7.4 Discussion
Data from this study show that for the study population, the two methods had good
levels of agreement when estimating fluid intake over the two-week study period. This
finding is in keeping with Shimokura et al’s comparison of water intake by
questionnaire and a three day water diary, where Spearman’s correlation coefficient was
reported to be 0.75 [98]. Kappa values were not reported in this study. A similar study
conducted by the Cooperative Research Centre for Water Quality and Treatment also
found moderate to good level of agreement between a questionnaire and three-day water
intake diary, with weighted kappa for three age groups ranging from 0.57 to 0.74
(Personal communication from paper in preparation - [99]).
121

A comparison of alcohol intake estimates by quantitative food frequency questionnaire
and food diary reported Pearson’s correlation coefficients varying from 0.68 to 0.79 for
all respondents [100]. Un-weighted kappa statistics reported for the same study were
fair to moderate. It is possible that had weighted kappa statistics been estimated, the
level of agreement may have been higher. In general, use of food frequency
questionnaires to estimate alcohol intake has been found to compare well with other
methods, particularly weighed food records (WFR), as summarised by Smith et al
[101]. The authors summarise several studies with Pearson’s correlation coefficient for
alcohol ranging from 0.74 to 0.90. Their study reported energy adjusted Spearman’s
correlation coefficient of 0.66 for alcohol (comparing self-administered food frequency
questionnaire and WFR). Findings from the study presented here are consistent with
these previous reports.
The general picture obtained from this study shows that with tap water and alcohol, the
retrospective questionnaire estimates were higher than the diary estimates, whereas with
hot beverages, the diary estimate marginally exceeded the retrospective questionnaire
estimate. It is not possible to know for certain the reason for this pattern. If we assume
that the diary provides a more accurate estimate of intake, we could speculate that
intake of beverages such as water and alcohol that are likely to be influenced by
weather, social gatherings, and physical activity, can be overestimated by questionnaires
because of generalising behaviour. In contrast, hot beverage intake maybe more
routine, therefore its intake could be more accurately estimated by even generalising
behaviour.
122

Browsing of diaries and questionnaires obtained in this study revealed that discrepancy
appeared to be more of a problem when a particular beverage was not a regular intake,
although there was the occasional participant who had recorded regular intake in one
method but not in the other. Another common finding was that there was a general
tendency for one method to underestimate or overestimate intake compared to the other
method. That is, there was no haphazard variation in estimating fluid intake for a
particular beverage type.
The inconsistencies in obtaining information using the two methods may have
contributed towards the differences in fluid intake estimates observed. When the
retrospective questionnaire was administered by an interviewer, beverage types were
specified (e.g. tap water from community, tap water from work place, bottled water,
tank water, tea, brewed coffee, instant coffee, decaffeinated coffee, beer, wine, fortified
wine, and spirits). In the fluid intake diary, beverage type was left open, which may
have resulted in certain omissions. This is likely to have contributed to some of the
discrepancy in the estimates obtained from the two methods.
There are advantages and disadvantages associated with the use of diaries and
retrospective questionnaires in quantifying food or fluid intake. The main advantage of
using diaries is not requiring participants to summarise patterns of behaviour, whereas
questionnaires ask for usual behaviour. This is important for estimating intake of
beverages that may differ from day to day depending on person’s activities, weather etc.
Summarising may result in loss of information. For this reason, diaries are assumed to
have a high level of accuracy, especially in measuring current behaviour, because they
do not rely on memory.
123

However, they are associated with a large respondent burden, which may have been
responsible for only 81.4% (n=281) of the total 345 participants completing the diary
without leaving any pages blank. A review of response rates of studies using diaries
found the response rate to be generally between 50 – 96%. This is quite a wide range.
Feedback received in general from this study indicates that time was the main hindrance
to maintaining the diary.
Participation rates in studies utilising diaries have been found to be lower for those with
less than high school education, lower socio-economic class, elderly, and those who
have recently experienced stressful life events [95, page 213]. Diaries are also
associated with sources of error unless they are carefully prepared and participants
provided with proper instructions. They may require certain skills from participants.
Training of participants in recording and measuring is time consuming both to the
participant and research team. As a result, recruiting a representative sample may be
difficult. In the study presented here, each participant was visited individually and the
study procedure (including completing diary) was explained. These visits varied in
duration lasting from 15 minutes to up to an hour in a few cases. Instructions on
completing the diary took up a large proportion of this time. In addition, a toll-free
telephone number was provided for participants to call if they required assistance in
filling up the diary. The major proportion of calls received on this number were
clarification inquiries, and not technical details on filling in the diary.
Another matter requiring consideration related to the use of diaries to estimate intake is
the fact that the act of recording in a diary may influence the person’s behaviour. In this
study, this was not an issue because the outcome was a marker of acute exposure
124

relating to the two-week study period. Therefore, a change in behaviour from the norm
would not have a great impact on the findings.
Questionnaires are also associated with advantages and disadvantages. On the positive
side, questionnaires have less respondent burden, they provide an estimate of past and
usual behaviour, and are less costly to the research team. However, they depend on
memory, and require subjects to summarise behaviour.
The repeatability measure of the questionnaire was found to be moderate. It is expected
that with measures such as fluid intake, estimates of repeatability would be lower
compared with reliability. Fluid intake is influenced by weather conditions, social, and
work behaviour, and is therefore likely to vary from fortnight to fortnight. A finding of
poor repeatability would however suggest that the questionnaire was not accurate in
quantifying intake. With moderate repeatability, it is reasonable for the questionnaire to
be compared against another method.
The decision to use a retrospective questionnaire or diary to estimate fluid intake has to
be made by balancing the pros and cons of the two methods, keeping in mind the
objective of the exercise. In the present study, the purpose was to quantify fluid intake
in order to create individual exposure profiles of intake dose for the various DBPs in
chlorinated drinking water. It was reassuring to obtain good levels of correlation and
agreement between the two methods. Also, the levels of agreement detected by the
kappa test indicate that the misclassification between the two methods is not a
significant issue. The findings support existing literature that a daily diary and
retrospective questionnaire differs somewhat, although not to a large extent, in
125

estimating fluid intake. In the present study, both measures have been used to estimate
exposure to the study factor.
Caution must be exercised when generalising the findings from this study to the general
population because the study population was all male. It has been shown with the
Dietary and Nutritional Survey of British Adults that reporting of diet (energy) intake
may be different in the two sexes [102].
126

Chapter 8. Risk assessment analysis
Many of the smaller water utilities monitor total THM without breakdown by the
individual THM compounds (i.e. total THM is used as a surrogate indicator of the
health risk). In order to assess the appropriateness of monitoring total THM (without
breakdown by compound), the association between total THM and bladder cell DNA
damage has been studied separate to the association between the four THM compounds
and bladder cell damage. Risk assessments have been undertaken separately for the
three exposure indices (available dose, intake dose, and internal dose).
Analysis undertaken has been described in detail in the methods chapter (5) of this
thesis. Results in this chapter are presented in two parts; the first part identifies the
variables for inclusion in the final regression model for each exposure index, and the
second part presents the findings from the final regression models for the various
exposure indices.
Since appendices 1 to 3a do not show an obvious relationship between exposure and
outcome, the Poisson regression model assumes a linear relationship. Relative risks
presented are for increase in DNA damage to bladder cells per one-microgram per litre
increase in exposure.
127

8.1 Results part I: Identifying variables to be included in the final
models for assessing relationships between exposure to THM and
micronuclei frequency
The various components presented below identify the variables to be included in the
final models. Relative risks adjusting for the identified variables are summarised in the
next section (8.2).
8.1.1 Individual THM compounds
The following section identifies the interaction terms and potential confounders that are
to be adjusted for in the models assessing risk when exposure is examined in terms of
THM compounds.
8.1.1.1 Available dose
Concentrations of the four THM compounds chloroform (CHCl3),
bromodichloromethane (CHBrCl2), dibromochloromethane (CHBr2Cl), and bromoform
(CHBr3), and of absorbable organic halogen (AOX) were measured in reticulated water.
These concentrations formed the available dose concentrations.
The mixed compounds (bromodichloromethane and dibromochloromethane) were
highly correlated with bromoform with correlation coefficients of greater than 0.9
(Table 8-1). Therefore, the two mixed compounds were excluded, and the baseline
model for available dose individual THM compounds included chloroform, bromoform,
and AOX concentration in reticulated water as the exposure variables.
128

Examining chloroform, bromoform, and AOX univariately or separately in a multiple
regression resulted in relative risks varying from 0.996 to 1.014 with confidence
intervals including one, indicating that there was no significant difference in the
unadjusted risk of DNA damage, when exposure was measured at level of available
dose (Table 8-2).
Table 8-1. Correlations between available dose for THM compounds
n=228 CHCl3 CHBrCl2 CHBr2Cl CHBr3 AOX
CHCl3 1.0000
CHBrCl 0.0001 1.0000 2
ChBr2Cl -0.0320 0.9992 1.0000
CHBr3 -0.0306 0.9950 0.9960 1.0000
AOX 0.6426 0.7239 0.7020 0.7014 1.0000
Table 8-2. Unadjusted relative risks for the association between available dose of THMs (exposure) and frequency of micronuclei in bladder epithelial cells
Crude (unadjusted) Exposure variable(s)
(n=226) Relative risk 95% CI
*Chloroform
* Bromoform
* AOX
** Chloroform, and
Bromoform
** Chloroform,
Bromoform, and
AOX
0.996
1.014
1.00001
0.996
1.02
0.985
0.968
1.003
0.990 to 1.002
0.988 to 1.040
0.999 to 1.001
0.990 to 1.003
0.98 to 1.04
0.968 to 1.003
0.896 to 1.048
0.998 to 1.007 * Univariate analysis with individual compounds ** multiple regression model with two or more compounds
129

Available dose interaction terms were found to be highly correlated with each other
with correlation coefficients of >0.98 (table 8-3). Interaction term three (table 5-1) was
chosen to assess the effect of interaction, as it included the two baseline variables in the
model (chloroform and bromoform).
Table 8-3. Correlations between interaction terms of available dose for THM compounds
n=226 Term 1 Term 2 Term 3 Term 4 Term 5 Term 6
Term 1 1.0000
Term 2 1.0000 1.0000
Term 3 0.9934 0.9934 1.0000
Term 4 0.9874 0.9874 0.9809 1.0000
Term 5 0.9900 0.9900 0.9901 0.9971 1.0000
Term 6 0.9883 0.9883 0.9890 0.9966 0.9999 1.0000
Interaction term three did not demonstrate a significant effect by the likelihood-ratio test
(p=0.35), and was therefore not retained for the final model of available dose THM
compounds.
The potentially confounding variables also did not make a significant contribution to the
model, and were therefore not retained for the final model (appendix 9). It is likely that
exposure to the potential confounders was not sufficient to demonstrate the confounding
effect. Larger numbers would be required to demonstrate such relatively small
confounding effects. Because of the strong evidence from the literature for a
130

confounding role, age and smoking were included as potential confounders in the final
model (section 5-11).
8.1.1.2 Intake dose as estimated by fluid intake diary
As with available dose, the computed intake dose for the four THM compounds (using
information from fluid intake diaries) also showed high correlation (>0.99) between the
mixed compounds (table 8-4). Because of the high correlation of the mixed compounds
with bromoform, the mixed compounds were dropped, and bromoform and chloroform
formed the baseline model.
Table 8-4. Correlation between intake dose for the THM compounds
n=226 CHCl3 CHBrCl2 CHBr2Cl CHBr3
CHCl3 1.000
CHBrCl2 0.0888 1.0000
CHBr2Cl 0.0473 0.9988 1.0000
CHBr3 0.0514 0.9941 0.9957 1.0000
Intake dose of chloroform and bromoform were examined univariately against the
frequency of micronuclei, prior to undertaking the multiple regression analysis. As
shown in table 8-5, the relative risks for chloroform and bromoform, whether assessed
univariately or as a multiple regression, were around one, with the 95% confidence
intervals all including one. This indicates that there is no significant increase in risk of
DNA damage to bladder cells when exposure is examined at intake dose level.
131

Table 8-5. Crude and adjusted relative risks for the association between intake dose of THMs (exposure) as estimated by fluid intake diary, and frequency of micronuclei in bladder epithelial cells
Crude (unadjusted) Exposure variable(s)
(n=226) Relative risk 95% CI
*Chloroform
*Bromoform
**Chloroform, and
Bromoform
1.000
1.004
1.000
1.004
0.997 to 1.002
0.987 to 1.021
0.997 to 1.002
0.987 to 1.021 * Univariate analysis with the individual compounds * multiple regression model
The interaction terms for intake dose as estimated by fluid intake diary were found to be
highly correlated with each other with correlation coefficients of > 0.90 (table 8-6).
Interaction term three was chosen to represent the terms for reasons given in section
5.11. This term was retained for the final model based on a likelihood ratio test p-value
of 0.06. No potential confounders to the association were identified as shown in
appendix ten.
Table 8-6. Correlation between interaction terms of intake dose as estimated by fluid intake diary
n=226 Term 1 Term 2 Term 3 Term 4 Term 5 Term 6
Term 1 1.0000
Term 2 1.0000 1.0000
Term 3 0.9898 0.9898 1.0000
Term 4 0.9898 0.9898 0.9883 1.0000
Term 5 0.9910 0.9910 0.9957 0.9971 1.0000
Term 6 0.9903 0.9903 0.9954 0.9967 0.9999 1.0000
132

8.1.1.3 Intake dose as estimated by questionnaire
Once again, the two mixed compounds were highly correlated with each other and with
bromoform, with correlation coefficients of greater than 0.99 (table 8-7). As a result,
intake dose of chloroform and bromoform were used as the baseline model.
Table 8-7. Correlations between available dose for THM compounds
n=226 CHCl3 CHBrCl2 CHBr2Cl CHBr3
CHCl3 1.0000
CHBrCl2 0.2022 1.0000
CHBr2Cl 0.1609 0.9986 1.0000
CHBr3 0.1629 0.9972 0.9984 1.0000
Assessment of unadjusted relative risks for DNA damage showed that there was no
significant increase in risk with exposure to THM compounds when exposure was
measured as intake dose as estimated by questionnaire (table 8-8).
Table 8-8. Unadjusted relative risk for the association between intake dose of THMs (exposure) as estimated by questionnaire, and frequency of micronuclei in bladder epithelial cells
Crude (unadjusted) Exposure variable(s)
(n=226) Relative risk 95% CI
*Chloroform
*Bromoform
**Chloroform, and
Bromoform
1.0001
1.009
1.000
1.009
0.997 to 1.003
0.986 to 1.032
0.996 to 1.003
0.986 to 1.033
* Univariate analysis with individual compounds
** multiple regression model with two compounds
133

Correlation between interaction terms for intake dose as estimated by questionnaire was
assessed. All interaction terms were highly correlated with each other with correlation
coefficients of greater than 0.95 (table 8-9). Term three was chosen to assess the effect
of interaction. The interaction term was retained for the final model based on the
likelihood-ratio test (p=0.7). The potential confounders did not alter the association by
more than one percent (appendix 11). None of the variables were retained for the final
model.
Table 8-9. Correlations between interaction terms for intake dose of THM compounds, as estimated by questionnaire
n=226 Term 1 Term 2 Term 3 Term 4 Term 5 Term 6
Term 1 1.0000
Term 2 1.0000 1.0000
Term 3 0.9829 0.9829 1.0000
Term 4 0.9619 0.9619 0.9791 1.0000
Term 5 0.9636 0.9636 0.9824 0.9991 1.0000
Term 6 0.9599 0.9599 0.9792 0.9988 0.9998 1.0000
8.1.1.4 Internal dose
With internal dose, dibromochloromethane was not included in the analysis because of
the large proportion (79%) of zero values in the variable. Concentrations of the
remaining three THM compounds chloroform, bromodichloromethane, and bromoform
in urine (i.e. internal doses) were not highly correlated with each other, with the highest
level of correlation being 0.25 (table 8-10). All three compounds composed the
baseline model for testing this association. Analysis was undertaken including and
excluding outliers of internal dose measures. Outliers were identified for this purpose
by examining the distribution and excluding values that were extremely large compared
134

to the rest of the distribution. For chloroform, bromodichloromethane and bromoform,
values exceeding 0.9 µg/l, 0.7 µg/l, and 4.0 µg/l respectively, were considered to be
outliers.
Table 8-10. Correlations between internal dose for THM compounds
n=219 CHCl3 CHBrCl2 CHBr3
CHCl3 1.0000
CHBrCl2 0.2025 1.0000
CHBr3 0.2481 0.1830 1.0000
The unadjusted relative risk for univariate and multiple regression analysis examining
the internal dose measures of the three individual THM compounds against micronuclei
frequency is shown in table 8-11. Although the relative risk for chloroform in the
univariate or multiple regression analysis appears to be protective, the 95% confidence
intervals include one, and are very wide. Therefore, little importance should be attached
to the estimate.
135

Table 8-11. Unadjusted relative risk for the association between internal dose of THMs (exposure), and frequency of micronuclei in bladder epithelial cells
All data Excluding outliers Exposure variable(s)
(n=224) Relative risk
95% CI Relative risk
95% CI
611 observations, n=224 608 observations, n=222
*Chloroform
*Bromodichloromethane
*Bromoform
0.54
1.20
1.06
(0.16 to 1.76)
(0.62 to 2.32)
(0.81 to 1.40)
0.91
1.10
1.19
(0.15 to 5.39)
(0.29 to 4.19)
(0.87 to 1.61)
611 observations, n=224 601 observations, n=220
**Chloroform
Bromodichloromethane, and
Bromoform
0.43
1.28
1.12
(0.12 to 1.59)
(0.65 to 2.53)
(0.84 to 1.49)
1.23
1.17
1.17
(0.07 to 22.92)
(0.18 to 7.71)
(0.85 to 1.61)
* Univariate analysis of individual compounds
** multiple regression model with the three compounds
When assessing correlation between interaction terms for internal dose of THM
compounds, because of the high proportion of zero values in dibromochloromethane,
only terms not including this variable were assessed. The three terms correlated highly
with correlation coefficients greater than 0.9 (table 8-12). Interaction term three was
chosen to assess the effect of interaction on the association, and this was found not have
a significant effect (p=0.19). Excluding outliers resulted in p=0.8. The interaction term
was therefore retained for the final (excluding outliers) model.
136

Table 8-12. Correlations between interaction terms of internal dose for THM compounds
n=220 Term 1 Term 3 Term 5
Term 1 1.0000
Term 3 0.9440 1.000
Term 5 0.9367 0.9802 1.000
Several confounders were identified for inclusion in the internal dose model (appendix
12). These include lifetime history of working with chemicals or paint, ever working
with leather in non-work related activities, working with paint in non-work related
activities in the preceding year or fortnight, other hobbies, particularly gardening or
recreational farming, and exposure to passive smoking at home or workplace. Smoking
during study period and age were also included in the final model. The adjusted RR is
given in table 8-14.
When outliers were excluded, several more potential confounders were found to change
the association by five percent or more (appendix 12a), and were included in the final
regression model.
8.1.2 Total THM
Table 8-13 presents the relative risk estimates for the associations between the various
indices of total THM, and DNA damage to bladder cells. When available dose of total
THM was taken as the exposure variable, AOX concentrations in reticulated water was
not included because of the high colinearity with total THM (correlation coefficient =
0.93). None of the interaction terms or potential confounders were identified to have
significant effects, or to make a large enough contribution to the associations
137

(appendices 13 – 16). However, when outliers were excluded from the internal dose
measure, lifetime history of working with leather, and other hobbies, changed the
baseline relative risk by more than five percent. These variables were therefore retained
for the final model (appendix 16a). Relative risks for all indices were adjusted for
smoking during study period, and age. These estimates are presented in table 8-14.
Table 8-13. Unadjusted relative risks for DNA damage to bladder cells with exposure to total THM in community water supplies, by exposure indices
Relative risk 95% confidence interval
616 observations / n=226 Total THM
Available dose 1.002 0.998 to 1.003
Intake dose by diary 1.0001 0.9990 to 1.0017
Intake dose by questionnaire 1.0006 0.9990 to 1.0026
Internal dose (611 observations, n=244) 1.05 0.89 to 1.23
Internal dose – excluding outliers 1.18 0.90 to 1.54
(601 observations, n=220)
The risk estimates for DNA damage to bladder cells with exposure measured as total
THM, varied from 1.0001 to 1.18 depending on the exposure index. The estimates for
internal dose were higher than with the other indices. None of the associations were
significant.
8.2 Results part II: Relative risks for the final models
For each of the exposure indices, the variables for inclusion identified above were used
to estimate the adjusted relative risks for DNA damage to bladder cells. Table 8-14
presents the adjusted estimates, by exposure index. The risk estimates for available
138

dose and intake dose were around one, and were slightly higher for internal dose
excluding outliers. None of the associations were significant.
139

Table 8-14. Relative risk estimates for DNA damage to bladder cells with exposure to THMs in community water supplies, by exposure measure, adjusted for interaction and confounding
615 observations, n=225 Relative risk * 95% confidence intervalAvailable dose
Chloroform, 0.985 (0.967 to 1.003) Bromoform 0.970 (0.896 to 1.050)
AOX 1.003 (0.998 to 1.007)
Total THM 1.0002 (0.997 to 1.003) Intake dose by diary
Chloroform and 0.9998** (0.997 to 1.003) Bromoform 1.053** (0.998 to 1.111)
Total THM 1.0001 (0.998 to 1.002)
Intake dose by questionnaire
Chloroform and 0.999** (0.996 to 1.003) Bromoform 0.993** (0.918 to 1.075)
Total THM 1.001 (0.999 to 1.003)
Internal dose (577 observations, n=214)
Chloroform, 0.35 *** (0.09 to 1.34) Bromodichloromethane, and 1.07 *** (0.55 to 2.10)
Bromoform 1.10 *** (0.83 to 1.46) (611 observations, n = 224)
Total THM 1.05 (0.89 to 1.24)
Internal dose excl. outliers (512 observations, n= 190)Chloroform, 2.02 **** ( 0.09 to 48.05)
Bromodichloromethane, and 1.08 **** (0.15 to 7.70) Bromoform 1.43 **** (0.65 to 3.19)
(601 observations, n= 220)
Total THM 1.19 ***** 0.90 to 1.56 * Adjusted for age and smoking during study period. ** Also adjusted for interaction term 3 (table 5-1) *** Also adjusted for lifetime history of working with chemicals or paint, ever working with leather in non-work related activities, working with paint in non-work related activities in the preceding year or fortnight, other hobbies, particularly gardening or recreational farming, and exposure to passive smoking at home or workplace. **** Also adjusted for interaction term 3, history of bladder infection prior to last 12 months, lifetime history of working with chemicals, paint, electrical cables or making rubber, working with dyes and paint in the preceding year, working with paint in the preceding fortnight, lifetime history of using chemicals or leather in non-work related activities, use of paint in non-work related activity in the preceding year, other hobbies, particularly gardening or recreational farming, lifetime history of using hair rinses or smoking, or exposed to passive smoking at workplace, serum folate and vitamin B12 levels, use of paint at work or use of paint in non-work related activity during the two-week study period, other hobbies and smoking during study period. ***** Also adjusted for lifetime history of working with leather in non-work related activity, and other hobbies
140

Chapter 9. Flow cytometry
A random sample of 130 participants was asked to provide a third urine sample for flow
cytometry analysis. Providing this additional sample was not compulsory. A total of
112 participants provided this sample, and had flow cytometry analysis undertaken.
Thirty-two of these were from Bungendore, while Canberra and Adelaide had 58 and 24
participants respectively. Characteristics of participants with flow cytometry were
compared with all participants recruited to the study (table 9-1). Participants in the flow
cytometry analysis did not differ significantly from those in the main study sample, in
age or smoking status. Exposure levels were higher among the flow cytometry group.
Some participants who had a result from flow cytometry did not have a micronuclei
score due to unsuitable slide quality or insufficient cells to score for micronuclei.
Table 9-1. Characteristics of participants with flow cytometry results, compared
with all study participants
All Flow data p value (n=346) (n=112) (flow vs no flow result) Mean age (years) 46 48 0.44 (Anova)
Smoke (%) 80 (22%) 23 (20%) 0.38 (chi sq.)
Available dose total THM 52.6 59.4 0.03 (ranksum) mean level (µg/l) Internal dose total THM 0.33 0.58 0.000 (ranksum) mean level (µg/l)
141
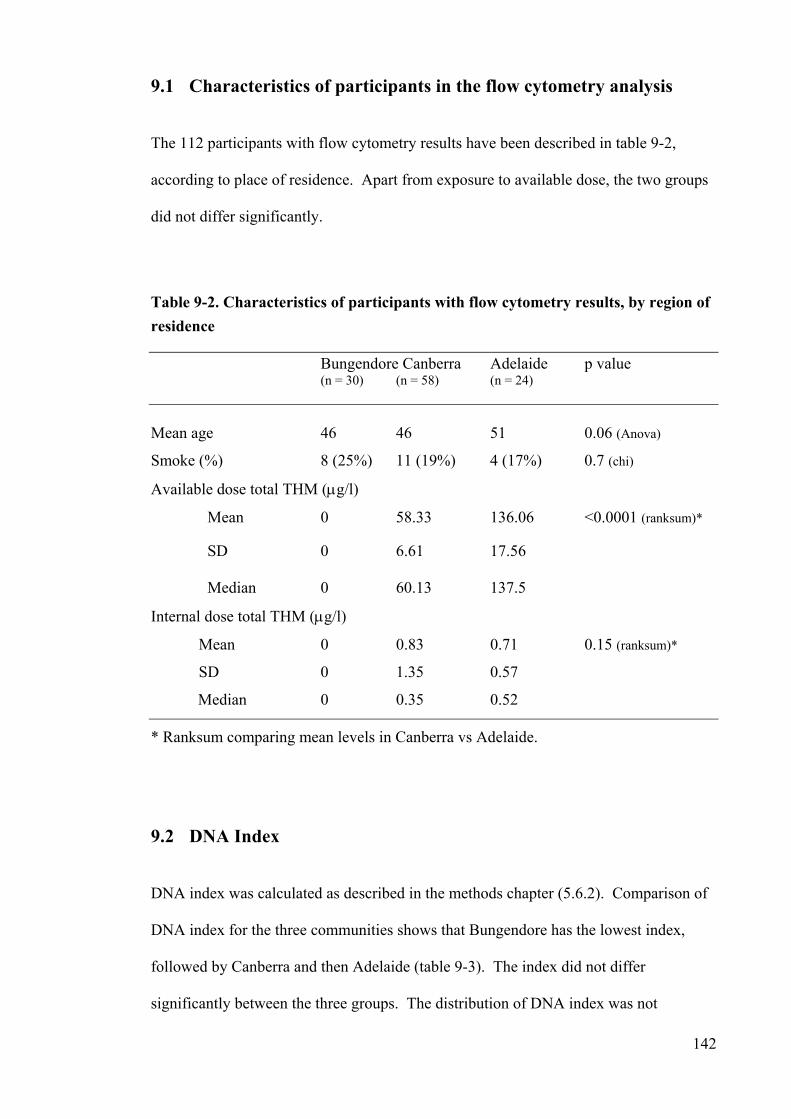
9.1 Characteristics of participants in the flow cytometry analysis
The 112 participants with flow cytometry results have been described in table 9-2,
according to place of residence. Apart from exposure to available dose, the two groups
did not differ significantly.
Table 9-2. Characteristics of participants with flow cytometry results, by region of residence
Bungendore Canberra Adelaide p value (n = 30) (n = 58) (n = 24) Mean age 46 46 51 0.06 (Anova)
Smoke (%) 8 (25%) 11 (19%) 4 (17%) 0.7 (chi)
Available dose total THM (µg/l)
Mean 0 58.33 136.06 <0.0001 (ranksum)*
SD 0 6.61 17.56
Median 0 60.13 137.5
Internal dose total THM (µg/l)
Mean 0 0.83 0.71 0.15 (ranksum)*
SD 0 1.35 0.57
Median 0 0.35 0.52
* Ranksum comparing mean levels in Canberra vs Adelaide.
9.2 DNA Index
DNA index was calculated as described in the methods chapter (5.6.2). Comparison of
DNA index for the three communities shows that Bungendore has the lowest index,
followed by Canberra and then Adelaide (table 9-3). The index did not differ
significantly between the three groups. The distribution of DNA index was not
142

normally distributed, and was transformed to a normal distribution by log
transformation. All analysis undertaken with DNA index utilises log-transformed
values.
Table 9-3. DNA index (untransformed) by region of residence
Mean SD Median Range
Bungendore (n=30) 4.40 3.89 3.70 0.68 to 18.66
Canberra (n=58) 8.61 19.58 3.59 0.50 to 138.6
Adelaide (n=24) 8.81 8.36 5.92 0.92 to 36.78
p = 0.06*/ 0.07**
* anova of log transformed DNA index, comparing the three groups
** ttest comparing Bungendore (unexposed) vs Canberra/Adelaide (exposed)
Examining the relationship between exposure and DNA index from flow cytometry was
undertaken using multiple regression models. The steps in identifying interaction terms
and confounding variables for inclusion in the models were the same as for the Poisson
regression model described in the previous chapter.
9.3 Association between THM and DNA index
Exposure levels in terms of available dose and internal dose were plotted against DNA
index to examine for linear or non-linear patterns of relationship. No obvious
relationship was visible (appendices 1a and 3a).
The association between exposure and outcome was assessed using a multiple
regression model, adjusting for interaction and confounding. Identifying highly
143
correlated THM compounds was done in the previous chapter and has not been repeated
here. Correlating interaction terms with each was also done in the previous chapter and
has not been repeated here. Because of the high level of correlation between terms, for
each of the exposure indices, interaction terms three (chloroform*bromoform) was used
to represent the interaction terms in the various regression models (see section 8.1.1.1).
Confounding was assessed by adding each potentially confounding variable to the
baseline regression model consisting of exposure and outcome. If introducing a
potential confounding variable changed the relative risk by five percent or more, that
variable was considered to be a confounder in the relationship being studied, and was
therefore retained for inclusion in the final model.
9.3.1 THM compounds
Linear regression models were run for each exposure index (with DNA index)
separately. Identification of the variables to be included in the final THM compound
models is presented here, by exposure index. The risk estimates for the final multiple
regression models are given in table 9-9.
9.3.1.1 Available dose
Chloroform and bromoform concentrations in reticulated water formed the base model
for the regression analysis in the association between available dose THM compounds
and DNA index. The mixed compounds were not included because of the high level of
correlation of these compounds with bromoform (table 8-1). Table 9-4 presents the
relative risks for the association of DNA index with chloroform, bromoform and AOX
examined univariately and in a multiple regression analysis. For available dose of
chloroform and bromoform when examined univariately, there was no significant
144

increase in DNA damage, as estimated by DNA index. AOX when examined
univariately indicates a significant association with DNA index, however when included
with chloroform and bromoform in a multiple regression model, this significance is lost.
Table 9-4. Unadjusted relative risks for the association between available dose of
THMs (exposure) and DNA index from flow cytometry
Exposure variable(s) Crude (unadjusted) (n=112) Relative risk 95% confidence interval
* Chloroform 1.003 0.996 to 1.011
* Bromoform 1.031 0.999 to 1.065
* AOX 1.002 1.0002 to 1.007
** Chloroform, 0.9996 0.982 to 1.017
Bromoform, and 1.01 0.94 to 1.09
AOX 1.001 0.997 to 1.006
* Univariate analysis with individual compounds
** multiple regression with three exposure variables
Interaction term three did not demonstrate a significant effect (p=0.57, likelihood-ratio
test), and was therefore not retained for the final model. Introducing the potentially
confounding variables did not alter the relative risk estimates by more than 1% as
shown in appendix 17. Therefore, only age and smoking were included in the multiple
regression models, for reasons explained in section 5.11. Adjusted relative risks are
presented in table 9-9.
145

9.3.1.2 Intake dose estimated by fluid intake diary
When exposure was measured as intake dose (estimated by fluid intake diary), the
relative risk for DNA damage by DNA index was not significant whether examined
univariately or in a multiple regression model (table 9-5). Introducing interaction term
three did not demonstrate a significant effect (p=0.9), and was therefore not retained for
the final model. The potential confounders contributed very little (less than one
percent) towards the association (appendix 18). None of these variables were therefore
retained for the model, and once again, only age and smoking were included in the final
regression model. The adjusted relative risks are presented in table 9-9.
Table 9-5. Unadjusted relative risks for the association between intake dose of
THMs as estimated by fluid intake diary (exposure), and DNA index from flow
cytometry
Exposure variable(s) Crude (unadjusted)
(n=112) Relative risk 95% confidence interval
* Chloroform 1.002 0.999 to 1.005
* Bromoform 1.006 0.832 to 1.031
** Chloroform and 1.002 0.999 to 1.005
Bromoform 1.006 0.998 to 1.030
* Univariate analysis with individual compounds
** Complex mixture model with two or more compounds
9.3.1.3 Intake dose estimated by questionnaire
Table 9-6 below presents relative risk estimates for DNA index examined against
available dose of chloroform and bromoform estimated by questionnaire. As with the
above exposure indices, the relative risk estimates does not support increased DNA
146

damage to bladder cells. The interaction effect did not demonstrate a significant effect
(likelihood-ratio test p=0.4). Introducing the potentially confounding variables made
minimal contribution to the association (appendix 19.).
Table 9-6. Unadjusted relative risks for the association between intake dose of
THMs as estimated by questionnaire (exposure) and DNA index from flow
cytometry
Exposure variable(s) Crude (unadjusted)
(n=112) Relative risk 95% confidence interval
* Chloroform 1.002 0.997 to 1.004
* Bromoform 0.999 0.960 to 1.040
** Chloroform and 1.000 0.997 to 1.004
Bromoform 0.999 0.960 to 1.040
* Univariate analysis with individual compounds
** Complex mixture model with two or more compounds
9.3.1.4 Internal dose
The baseline model for internal dose of THMs included concentrations of chloroform,
bromodichloromethane, and bromoform in urine (see section 8.1.1.4 and table 8-10).
Examining these compounds univariately or as a complex mixture did not support
evidence of increased DNA damage (measured by DNA index) with exposure to THMs
(table 9-7). However, similar to the picture seen when micronuclei frequency was used
as the outcome measure, the confidence intervals were somewhat wider than what was
obtained with other exposure measures.
147

Table 9-7. Unadjusted relative risks for the association between internal dose of
THMs (exposure) and DNA index from flow cytometry
Exposure variable(s) Crude (unadjusted)
(n=112) Relative risk 95% confidence interval
* Chloroform 1.06 0.55 to 2.05
* Bromodichloromethane 1.13 0.50 to 2.55
* Bromoform 1.04 0.81 to 1.34
** Chloroform, 1.04 0.53 to 2.04
bromodichloromethane, and 1.11 0.48 to 2.54
Bromoform 1.04 0.80 to 1.34
* Univariate analysis with individual compounds
** Complex mixture model with two or more compounds
The interaction term did not result in a change to the association of 5% or more, and
was therefore not retained for the final regression model. Several of the potential
confounders however resulted in changing the association by 5% or more (appendix
20). These variables (Family history of bladder cancer, ever worked with dyes,
chemicals, and truck driver, lifetime history of using dyes in hobbies, or using dyes in a
hobby in the last year, ever working with leather as part of a hobby, Using paint in non-
work related activity in the last fortnight, ever smoked tobacco, exposure to passive
smoking in home environment, swimming in chlorinated water during the study period,
and plasma folate level) were retained for inclusion in the multiple regression model.
148

9.3.2 Total THM
The following table summarises the relative risks, unadjusted for interaction terms or
confounders, for the four exposure indices (table 9-8). Although the relative risk for
exposure measured as available dose total THM was small, this association appeared
significant, while none of the other exposure measures showed a significant increase in
DNA damage to bladder cells with exposure to total THM.
Table 9-8. Unadjusted relative risks for the association between total THM and
DNA index from flow cytometry, by exposure index
Exposure measure Crude (unadjusted) (n=112) Relative risk 95% confidence interval
Available dose 1.004 1.0004 to 1.0079 Intake dose by diary 1.001 0.999 to 1.003 Intake dose by questionnaire 1.00007 0.997 to 1.003 Internal dose 1.03 0.86 to 1.22
Introducing potentially confounding variables to the various baseline models did not
result in a change in the association by five percent or more for any of the exposure
indices of total THM, and were therefore not retained for the final regression models
(appendix 21). Having identified the variables for inclusion in the final models, a
multiple regression analysis was undertaken to quantify the association between THMs
and DNA index from flow cytometry. In all models, smoking during study period and
age were included as potential confounders. Table 9-9 below presents the findings from
these analyses.
149

Table 9-9. Relative risk for DNA damage to bladder cells (estimated by DNA
index from flow cytometry), with exposure to THMs in community water supplies,
by exposure index, adjusted for interaction and confounding
n=112 Relative risk* 95% confidence interval
Available dose
Chloroform, 0.999 0.982 to 1.017
Bromoform, and 1.01 0.94 to 1.09
AOX 1.01 0.997 to 1.006
Total THM 1.0042 1.0003 to 1.0081
Intake dose by diary
Chloroform and 1.002 0.999 to 1.005
Bromoform 1.003 0.978 to 1.029
Total THM 1.001 0.999 to 1.003
Intake dose by questionnaire
Chloroform and 1.0005 0.997 to 1.004
Bromoform 0.994 0.953 to 1.037
Total THM 1.00008 0.997 to 1.003
Internal dose (n=107)
Chloroform, 1.38 ** 0.64 to 2.97
Bromodichloromethane, and 1.81 ** 0.71 to 4.65
Bromoform 0.97 ** 0.74 to 1.25
Total THM 1.03 0.87 to 1.23
*Adjusted for age and smoking during the study period ** Also adjusted for family history of bladder cancer, ever worked with dyes, chemicals, ever worked as a truck driver, lifetime history of using dyes in hobbies, ever worked with leather as part of a hobby, worked using paint in non-work related activity in the last fortnight, ever smoked tobacco, exposure to passive smoking in home environment, swimming in chlorinated water during the study period and plasma folate level. 150

Chapter 10. Discussion
The risk of developing cancer with exposure to by-products of chlorination is of
significant public health concern because of the large numbers of people the world over
who use chlorinated water for drinking and domestic purposes. This study examines the
association between exposure to DBPs (indicated by THMs levels), and DNA damage
to bladder cells. It overcomes some of the limitations of the earlier studies by obtaining
individual measures of exposure prospectively. It also overcomes the difficulty of
measuring long-term (chronic) exposure by using a pre-clinical biomarker of
genotoxicity to predict the carcinogenic potential of THMs.
The results from this study do not demonstrate a significant association between
exposure to THMs from community water supplies, and DNA damage to bladder
epithelial cells. Of the twenty regression models undertaken to examine the association
between the various exposure measures and DNA damage (estimated by prevalence of
micronuclei or DNA index from flow cytometry), one model (examining available dose
of total THM with DNA index) revealed a significant risk estimate, while all others
were insignificant. A one in twenty significant finding is likely to be a chance
occurrence, and is unlikely to demonstrate a true association. It must be emphasised
that the null findings in this study are for THM levels that were within the Australian
guideline levels for drinking water. The findings cannot be therefore generalised to
THM levels that exceed guideline levels.
151

10.1 Precision and validity of study
Selection of study groups and sampling are important factors that contribute to precision
of a study. This, being a prospective cohort study, is less subject to sampling errors
commonly associated with case-control studies. However, cohort studies are not free of
random error. This cohort study was composed of three communities, and although the
groups did not differ in many of the attributes examined, there may be differences
between the groups that could distort the association under study. All attempts were
made to identify and adjust for factors (such as relevant medical history, occupational
and recreational exposure to chemicals, dyes etc.) that are known to confound the
association.
One important difference between the communities was the water source. Bungendore
water was from a groundwater source whereas water supplies in Canberra and Adelaide
were derived from surface water. Surface water is more susceptible to contamination by
organic matter or potentially carcinogenic pollutants compared to groundwater, and may
therefore exhibit more mutagenic properties. Such an effect, if present, would have
resulted in a bias away from the null, and is therefore unlikely to have been a significant
source of bias in this study.
152
Sample size is another factor that contributes to precision of a study of this kind. The
sample size for this study was based on prevalence of micronuclei in exfoliated bladder
epithelial cells with exposure to arsenic [103]. The desired sample size was achieved
and we can be confident that there was adequate power to detect an association with the
estimates for available dose (i.e. concentration of THM in reticulated water) and intake
dose (which is derived from available dose). The wide confidence intervals around the
risk estimates for internal dose suggest lack of power. This is possibly due to the much
lower concentrations at which THMs occur in urine compared to water. At such low
concentrations, detecting an effect would require larger numbers. Lack of power for the
internal dose analysis would also explain the widening of confidence intervals when
outliers were excluded from the analysis. Excluding outliers reduced the number of
observations in the multiple regression analysis from 577 (n=214) to 512 (n=190)
observations. The risk estimates for internal dose are less robust.
Sampling within the groups is also a potential source of bias that needs to be considered.
In Bungendore, no sampling was done, and all eligible persons in Bungendore were
asked to participate. In Canberra and Adelaide, areas with higher THMs levels in
reticulated water were identified, and within each area, a strict random sample was
selected. In all three communities, households were identified from telephone
directories. This would lead to exclusion of people at the two extremes of the socio-
economic scale because of the exclusion of those without telephone connections and
those with silent numbers. The selection enables us to broadly generalise about the
issue on which the cohort was chosen – level of exposure to THMs in community water.
Selection bias results from the sample completing the study not being representative of
the population under study. No information is available on persons who were eligible
but not willing to participate, and a comparison of this group with those who
participated cannot be made to determine if the two groups differed.
A strength of this study was the detailed exposure measures obtained at an individual
level. In addition, three indices of exposure were obtained for each participant, and
exposure from ingestion, dermal and inhalation was considered. It is recognised that
dermal and inhalation exposure was computed using estimated shower air concentration
153

(based on experimental models). It is unlikely that a resulting error in the estimated
dermal or inhalation exposure would make a significant difference to the final risk
estimate. This is the first study (to our knowledge) that has even attempted to estimate
dermal and inhalation exposure.
Contributing to the precision of exposure measure were the standards associated with
THM testing. THM assays for this study were carried out by two laboratories that were
accredited by the National Association of Testing Authorities, Australia (NATA), and
are therefore required to comply with national standards.
The study presented here is limited to exploring the suitability of non-invasive exposure
measures (i.e. in water and urine) to assess genotoxicity of chlorine disinfected water
supplies. Blood concentrations of THMs may have provided a more accurate measure
of internal dose, although assay of volatile compounds in blood is also prone to loss of
compounds during collection and analysis. This was not however investigated in this
study. When measuring volatile organic compounds, the loss of compounds through
evaporation must be considered. Due to the semi volatile nature of THMs, it is
recognised that there could be a non-measurable loss of compound on collection and
handling of urine samples, resulting in lower than actual readings. However, urinary
concentration of chloroform has been shown to increase following exposure from
swimming in chlorinated pools, with at least 3-7% of chloroform being secreted via
urine [104].
The failure to adjust the urine THM concentrations in this study for urine volume and
urinary creatinine may have affected the validity of urinary THM concentration as a
measure of internal dose.
154

Non-differential misclassification of outcome also needs to be considered as a possible
explanation for the null findings, as it can produce a bias towards the null. This raises
the matter of validity of the outcome measure, micronuclei.
Micronuclei prevalence has been used successfully to assess genotoxicity of potential
carcinogens such as arsenic, benzene, radiation and smoking [64], [66], [105], [88],
[106], [103], [63], [107], [75]. Micronuclei are a pre-clinical stage in the pathway to
cancer development and it is therefore a biologically plausible outcome measure to
predict carcinogenic potential of a substance.
Preparation of urothelial cells for scoring requires basic laboratory skills with some
specific training. Any effects of the preparation technique for this study would be
randomised across the three study groups as the cells were prepared by the one person,
and is therefore unlikely to result in differential error. Scoring of micronuclei is a
tedious activity and is a subjective process leaving room for error. If specimens from
the various exposure groups are randomly assigned to scorers, or if one scorer does all
the scoring, this error would not contribute to a systematic misclassification. In this
study, there were two scorers, and each scorer kept a record of the position of cells with
micronuclei. An experienced scorer verified a ten percent sample. It is therefore
unlikely that a differential error would result from scoring. Scorers were blind to the
exposure status of participants. Therefore, a diagnostic bias (resulting in differential
misclassification of outcome) was unlikely.
The accuracy of micronuclei assay can be influenced by the number of cells scored,
with random variation having a significant effect if less than 500 cells per participant
155

are scored. Accuracy is said to increase and stabilise when 1500 – 2000 cells per
participant are scored [61]. In this study, the unexposed group had on average 929 cells
per participant, scored. In the two exposed groups, the average number of cells scored
was 463. This is likely to lead to a bias towards the null, and therefore constitutes a
major weakness of this study. However, the fact that flow cytometry analysis, which
is an automated process that was set to pick up 50,000 particles, also revealed similar
results adds confirmatory strength to the null findings of this study.
Flow cytometry technique is less subject to measurement bias compared to the
micronuclei assay. When assessed at an ecological level (comparing results between
study sites), the borderline significantly higher DNA index from flow cytometry among
the exposed group compared to the unexposed group, provides weak evidence that
exposure to chlorinated water may be associated with increased DNA damage to
bladder cells (table 9-3). Given that an association with THM levels was not
demonstrated, it is possible that one of the other potentially carcinogenic substances in
chlorinated water (such as MX Furanone or any of the other DBPs) may be contributing
to this suggestion of increased DNA damage observed by flow cytometry. This
assessment is however subject to the considerable weaknesses of ecological
comparisons.
Flow cytometry was used as an additional outcome measure because it was automated
and fast. There is little or no literature on the use of flow cytometry to quantify DNA
damage in exfoliated epithelial cells, as was used in this study. Exfoliated cells are cells
that have been shed from the epithelium, and are no longer healthy living cells. The fact
that the results obtained were very similar to those obtained with micronuclei possibly
suggests that flow cytometry may prove a suitable option for assessing DNA damage
156

even in exfoliated epithelial cells. A decision on the suitability of the test cannot be
based on a single study, and further investigation of this approach is desirable.
Adding to the strengths of the study was that unlike with animal experimental studies,
participants were exposed to the complex mixture of compounds present in chlorinated
water. Therefore, although the analysis was undertaken in relation to THM levels in the
water, the measured DNA damage to bladder cells was the effect of exposure to the
complex mixture. This effect will be well observed in a follow-up study that was
undertaken in October / November 1999 after chlorination of Bungendore water supply
in May 1999, in which Canberra was the control group. Water samples were obtained
from the reticulation system in Bungendore and Canberra, and participants were asked
to provide urine samples for THM assay and scoring of micronuclei cells. The results
of the follow up study are pending. If this follow-up study demonstrates that the
(unadjusted) prevalence of micronuclei in Bungendore has risen compared to Canberra,
this would indicate that by-products of chlorination have had a genotoxic effect on
bladder cells.
10.2 Implications for the water industry
This study utilised THM concentrations (in water and urine) as the exposure measure.
THMs are routinely monitored DBPs in chlorinated water supplies the world over, and
in the case of smaller water utilities are the only DBP to be monitored. Keeping in mind
the limitations identified, the failure to demonstrate a genotoxic effect on bladder cells
with exposure to THMs, supports recent suggestions that THMs (chloroform in
particular) are not genotoxic, and that the mode of action is cell death from mechanisms
other than DNA damage [4], [108], [48], [109].
157

It is known that THMs are not the most mutagenic compound, and that there are
compounds such as MX Furanone that account for a large proportion of the
mutagenicity of chlorinated water. Given the null findings from this study for an
association between exposure to THMs and genotoxic changes to bladder cells, the next
step in assessing carcinogenicity of DBP in chlorinated waters should be to examine the
relationship between THMs and the more mutagenic compounds. If THM levels
correlate well with the mutagenic compounds in water, THMs may serve as a surrogate
marker for cancer risk from DBP, and the null findings of this study are reassuring for
the water industry. However, no published information was accessible to determine the
correlation. From discussions with experts in the water industry, it appears that water
rich in dissolved organic matter that have been shown to have relatively higher levels of
MX Furanone, tend to have higher levels of THMs. But the correlation between MX
and THM is not established and at this stage, it is not possible to determine the
occurrence of MX based on THM levels alone.
If it is demonstrated that THM levels in treated water do not correlate well with the
more mutagenic compounds, the next step would be to assess the association between
MX Furanone and DNA damage to bladder cells. Although it is recognised that such a
study would be rather costly, it would be of great benefit to the water industry. If an
association is demonstrated between exposure to MX Furanone and genotoxic changes
to bladder cells, this would suggest the need to identify more appropriate predictors of
carcinogenic potential to be monitored in chlorinated water. It is worth noting at this
stage that it was originally intended to measure MX Furanone levels in this study, but
the associated cost made this not feasible.
158

Identifying a suitable indicator for assessing health risks associated with chemicals in
water is important to obtain a balance between microbial and chemical risks. The lack
of consensus on guideline levels or maximum admissible concentrations, compounded
by the fear of cancer with chemical use, has led to much uncertainty, and a trend
towards decreasing chemical standards by regulatory authorities. Alterations in
treatment processes need to be judged carefully to ensure continued microbial safety of
drinking water. The continuing occurrence of water borne disease outbreaks in the
industrial countries as illustrated by a few recent reports, are a constant reminder of the
possible public health consequences of transient water supply contamination [110],
[111], [112], [113], [114]. It is therefore essential that the water treatment process be
carefully monitored, and an appropriate indicator for health risk assessment from
chemical disinfection be identified.
Whatever the final conclusion is in regard to the cancer risk associated with DBP in
chlorinated water, we need to recognise that at the present time, chlorine is the most
cost-effective method of disinfecting large community water supplies. This measure
had an enormous public health impact by reducing water-borne disease transmission.
Alternative disinfection methods have their own problems. Ozone provides no residual
disinfection and generates different by-products (such as aldehydes, glyoxals,
formaldehydes, and brominated compounds) that are also toxic. It is also costly to
implement, and by itself does not provide residual disinfection [5]. Chlorine dioxide is
a powerful disinfectant with no THM formation [115], [116]. It is by itself toxic, and
generates toxic by-products similar to those of ozone. Chloramination is a less powerful
biocide than chlorine, ozone or chlorine dioxide, but it retains activity for longer periods
of time, and therefore ideal for situations where low residual levels are require. Ultra
violet radiation disinfects by disrupting the chemical bonds of many molecules. It has
159

been found to be effective in water treatment, especially when used in conjunction with
activated carbon filtration, but it provides no residual disinfection effect [117].
Therefore, it is important that all effort be put in to maximising the benefits from
chlorination.
10.3 Conclusion
This study has not demonstrated an association between exposure to THMs from
chlorinated water and DNA damage to bladder epithelial cells. While this is reassuring
to the water industry, this study needs to be supplemented by studies correlating THM
levels with the other more mutagenic compounds such as MX Furanone in chlorinated
drinking water. If there is no strong correlation between THMs and these compounds,
studies will then be needed to examine the association between exposure to these
mutagenic compounds and DNA damage to bladder cells. Such information is
important for the development of drinking water guidelines that are currently focused on
THMs.
The possibility of an association between THMs and DNA damage to bladder cells
should be further explored in populations with exposure to higher THM levels.
160





























