Embed Size (px)
Citation preview
Chapter 56
Management of Patients With Dermatologic Problems
Primary Skin Lesions Macule, Patch: Flat, nonpalpable skin color change
(color may be brown, white, tan, purple, red) Macule: <1 cm, circumscribed border Patch: >1 cm, may have irregular border
Papule, Plaque: Elevated, palpable, solid massCircumscribed border Papule: <0.5 cm Plaque: >0.5 cm
Nodule, Tumor: Elevated, palpable, solid mass. Extends deeper into the dermis than a papule Nodule: 0.5–2 cm; circumscribed Tumor: >1–2 cm; tumors do not always have
sharp borders Vesicle, Bulla: Circumscribed, elevated,
palpable mass containing serous fluid Vesicle: <0.5 cm Bulla: >0.5 cm
Pustule: Pus-filled vesicle or bulla
Bacterial Skin Infections/Impetigo caused by staphylococci, streptococci, or
multiple bacteria. face, hands, neck, and extremities are most
frequently involved It is contagious and may spread to other parts
of the patient's skin or to other members of the family who touch the patient or use towels or combs that are soiled with the exudate of the lesions.

Starts as red macules, changed to thin-walled vesicles that rupture and become covered with a loosely adherent honey-yellow crust
Management: Antibiotics Complications: Acute glomerulonephritis Nsg: good hygiene to prevent spread of
infection to others.
Cellulitis Deep infection of the skin and subcutaneous tissue
caused by Group A Strep or S Aureus Bacteria enters through a break in the skin, then
Inflammation spreads horizontally Warm, red, swollen and painful Fever, malaise, chills, leukocytosis, elevated
Sedimintation Rate Bed rest, elevation of affect part, antibiotics Resolves in 2 weeks with TX
Folliculitis & furuncle
Folliculitis is an infection of bacterial or fungal origin that arises within the hair follicles.
A furuncle (boil) is an acute inflammation arising deep in one or more hair follicles and spreading into the surrounding dermis. It is a deep form of folliculitis.

Carbuncle An abscess of the skin and subcutaneous tissue that
represents an extension of a furuncle that has invaded several follicles and is large and deep-seated.
Caused by a staphylococcal infection. Appear in areas where the skin is thick and inelastic;
the back of the neck and the buttocks are common sites.
Purulent secretions, high fever, pain, leukocytosis, and even extension of the infection to the bloodstream.

Herpes Zoster Caused by the varicella-zoster virus Usually, patients have a history of
chickenpox. The virus becomes dormant and lies inside nerve cells near the brain and spinal cord
The viruses become latent, until immunity decrease, then it will become active. They travel by way of the peripheral nerves to the skin.
Herpes Zoster
S & S: painful vesicular eruption (usually on face, neck & thorax). Vesicles contain serum, then become purulent.
Treatment: Antiviral agents such as acyclovir (Zovirax) Pain is controlled with analgesics ? Corticosteroids
Herpes Simplex
Orolabial Herpes (fever blisters or cold sores) clusters of grouped vesicles on the lips. The onset is often accompanied by high fever,
regional lymphadenopathy, and generalized malaise.
Genital Herpes Minor infections may produce no symptoms Severe infections can cause systemic flulike
illness. Lesions appear as grouped vesicles on the vagina, rectum, or penis.
Fungal (Mycotic) Infections Tinea Capitis Person to person transmission Commonly known as ringworm Affect the Scalp Scaling area with broken hair shafts, plaques, pustules Possible permanent hair loss Treatment Oral Griseofulvin Selenium Sulfide shampoos Topical antifungal agents
Tinea Corporis (Body)
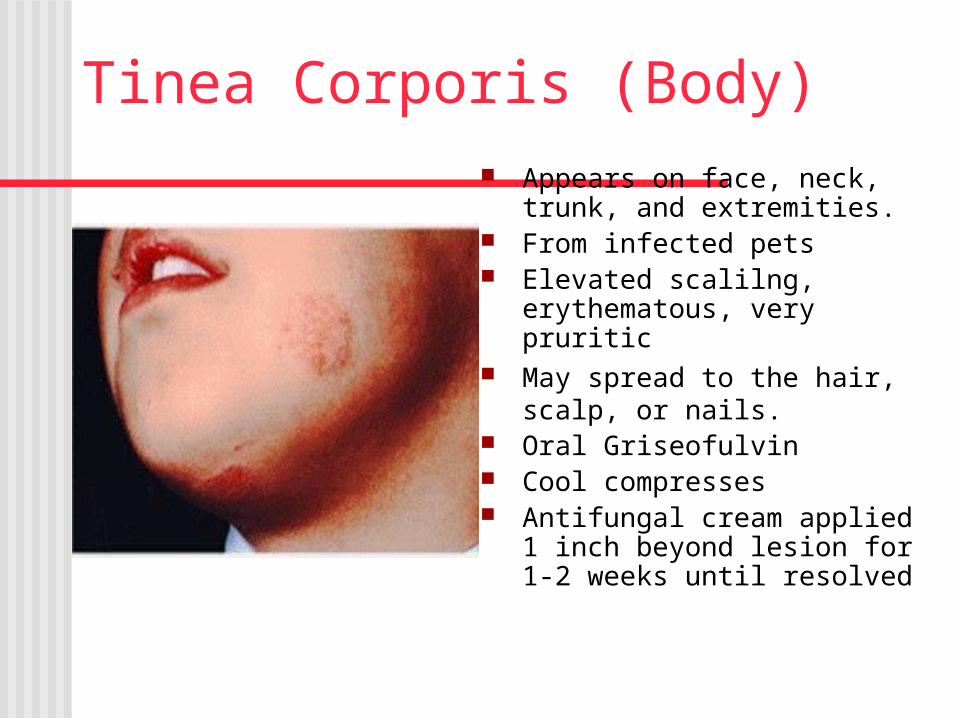
Appears on face, neck, trunk, and extremities.
From infected pets Elevated scalilng,
erythematous, very pruritic May spread to the hair,
scalp, or nails. Oral Griseofulvin Cool compresses Antifungal cream applied 1
inch beyond lesion for 1-2 weeks until resolved
Tenia Cruris (Groin) Begins with small, red scaling patches, which
spread to form circular elevated plaques, very pruritic
Clusters of pustules may be seen around borders.
Local application of Tolnaftate liquid Wet compresses or sitz baths may be soothing
Tenia Pedis (athlete's foot) Between toes and soles of the feet Maceration and fissuring between toes May have pinhead vesicles Oral Griseofulvin Antifungal powder Eliminate heat and perspiration by clean light socks,
well ventilated shoes, avoidance of occlusive shoes Soak feet in vinegar and water solution.
Nondermatophyte InfectionsCandidiasis Yeast fungal infection Glistening, fiery red or moist pink, beefy red with
satellite pustules, severe itching/burning Sites: skin folds/groin area, oral-thrush, diaper rash Teach prevention and management
Disposable diapers or cloth diapers without rubber pants, Change as soon as soiled
Exposure to open air, apply ointments (zinc oxide), avoid over washing, caution with perfumed soaps

Psoriasis Chronic hereditary
disorder Light-skinned race Environmental factors
that trigger Skin injury Infections Hormone changes Stress Drugs Alcohol Smoking obesity
Psoriasis Con’t.
Erythematous plaque with sharp well defined borders and silvery white scales.
Elbows, knees, scalp, lumbosacral skin, can occur anywhere
Management Topical treatment Photo-therapy Teach reducing
pruritus• Avoid scratching• Room humidifier• Warm not hot
bathing• Avoid strong soaps• Lubricate skin• antihistamines
Neoplasms: Malignant
Skin cancer is one of the most common malignant neoplasms in the United States and one of the most preventable.
Three most common types are: Basal Cell Carcinoma. Squamous Cell Carcinoma. Malignant Melanoma.
Risk factors Fair-skinned, fair-haired, blue-eyed people. People who sustain sunburn Chronic sun exposure (i.e. farmers) Exposure to chemical pollutants Sun-damaged skin (elderly people) History of x-ray therapy Scars from severe burns Chronic skin irritations Immunosuppression Genetic factors

Basal Cell Carcinoma
Most frequent type of skin cancer, arises from epidermis.
Prolonged sun exposure, poor tanning ability, and previous therapy with x-rays for facial acne are associated
with it.
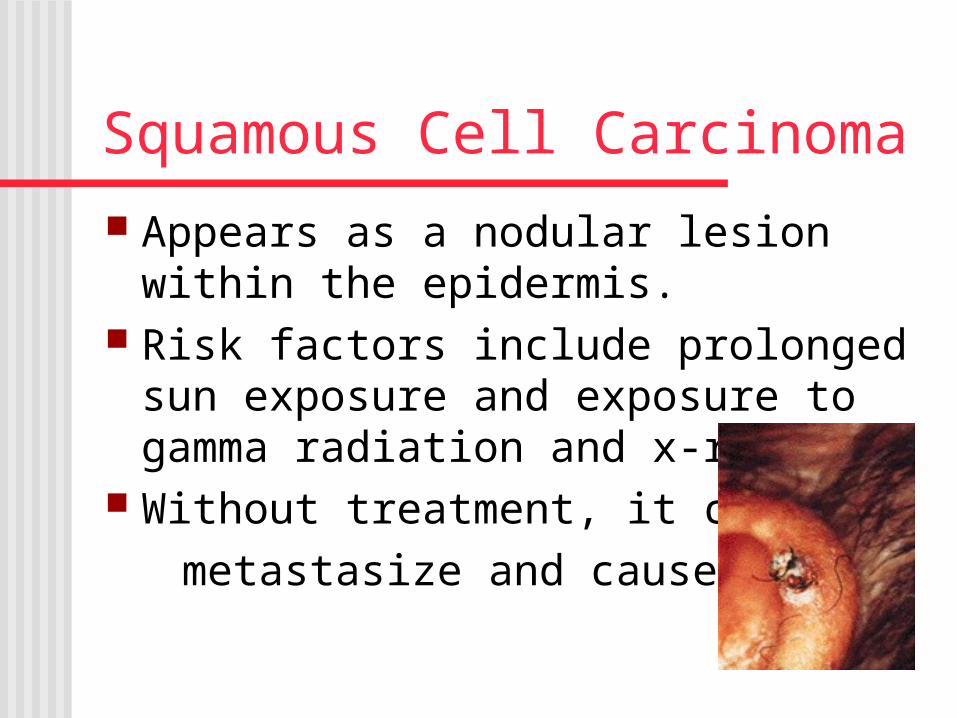
Squamous Cell Carcinoma
Appears as a nodular lesion within the epidermis.
Risk factors include prolonged sun exposure and exposure to gamma radiation and x-rays.
Without treatment, it can
metastasize and cause death.
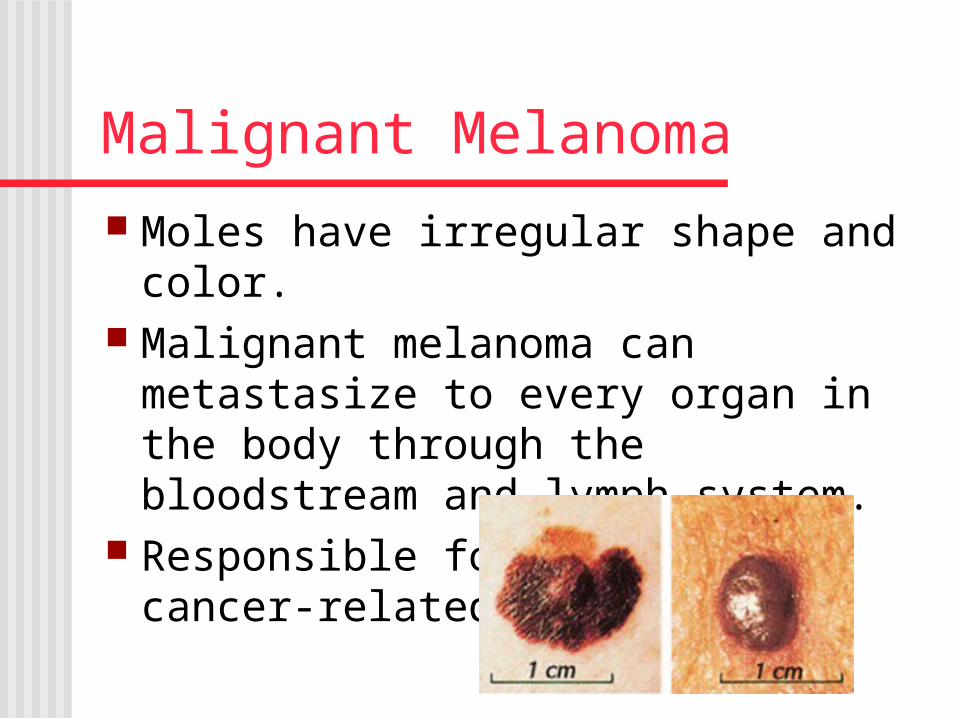
Malignant Melanoma
Moles have irregular shape and color. Malignant melanoma can metastasize to
every organ in the body through the bloodstream and lymph system.
Responsible for 3% of all cancer-related deaths.
Preventing Skin Cancer Avoid sun between 10
AM and 3 PM Sunscreen cream Reapply after
swimming, strenuous exercises, or prolonged sun bathing
Lip balm Protective clothing Inspect skin
regularly
Nonmalignant
Benign tumor of the skin include: Warts Lipomas (benign fatty tumors). Keloids (abnormal growth of scar
tissue). Sebaceous cysts. Nevi (moles). Angiomas (birthmarks).
Inflammatory Disorders of the Skin:
Dermatitis/Eczema In current usage, eczema has almost
become synonymous with dermatitis, although eczema tends to be used most often to refer to chronic forms of dermatitis.
Eczema is an atopic dermatitis often associated with rhinitis and asthma. It is a chronic superficial inflammation that evolves into pruritic, red, weeping, crusted lesions.

Contact Dermatitis Skin reacts to external irritants like:
allergens (e.g. poison ivy or cosmetics). harsh chemical substances (detergents,
insecticides). metals such as nickel. mechanical irritations from wool or
glass fibers. body substances like urine or feces.
Strategies for Avoiding Contact Dermatitis
Avoid contact with causative materials. Avoid heat, soap, and rubbing. Choose bath soaps, detergents, and
cosmetics that do not contain fragrance. Avoid topical medications, lotions, or
ointments, except those specifically prescribed for your condition.
Wash your skin thoroughly immediately after exposure to possible irritants.