Embed Size (px)
Citation preview
Chapter 5Diarrhoea
Case I
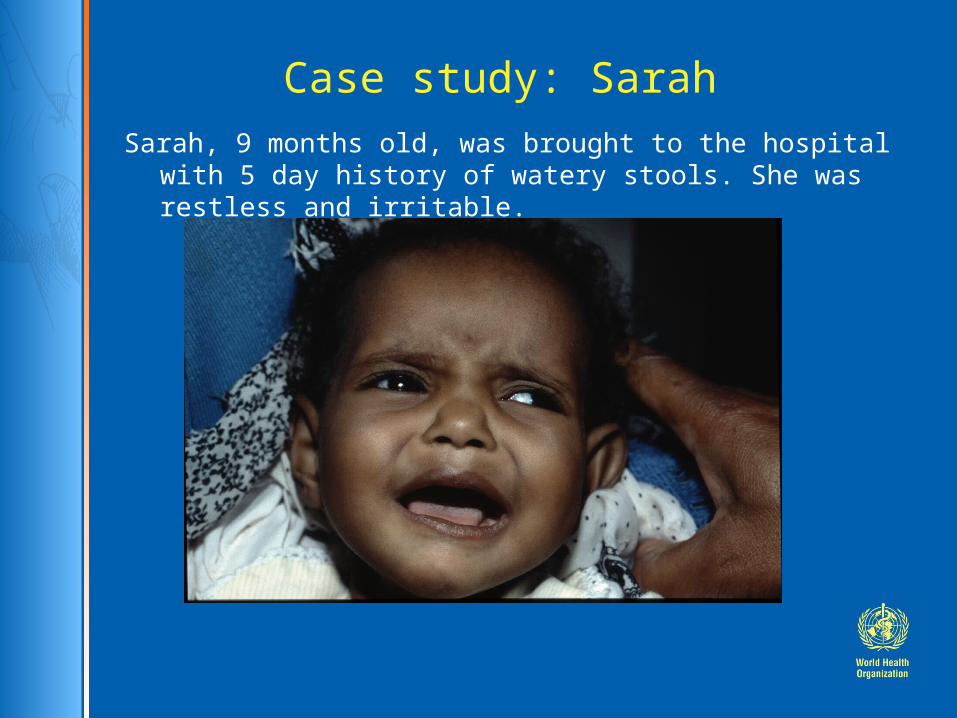
Case study: SarahSarah, 9 months old, was brought to the hospital with 5
day history of watery stools. She was restless and irritable.
What are the stages in the management of Sarah?
Stages in the management of a sick child (Ref. Chart 1, p. xxii)
1. Triage
2. Emergency treatment
3. History and examination
4. Laboratory investigations, if required
5. Main diagnosis and other diagnoses
6. Treatment
7. Supportive care
8. Monitoring
9. Discharge planning
10. Follow-up
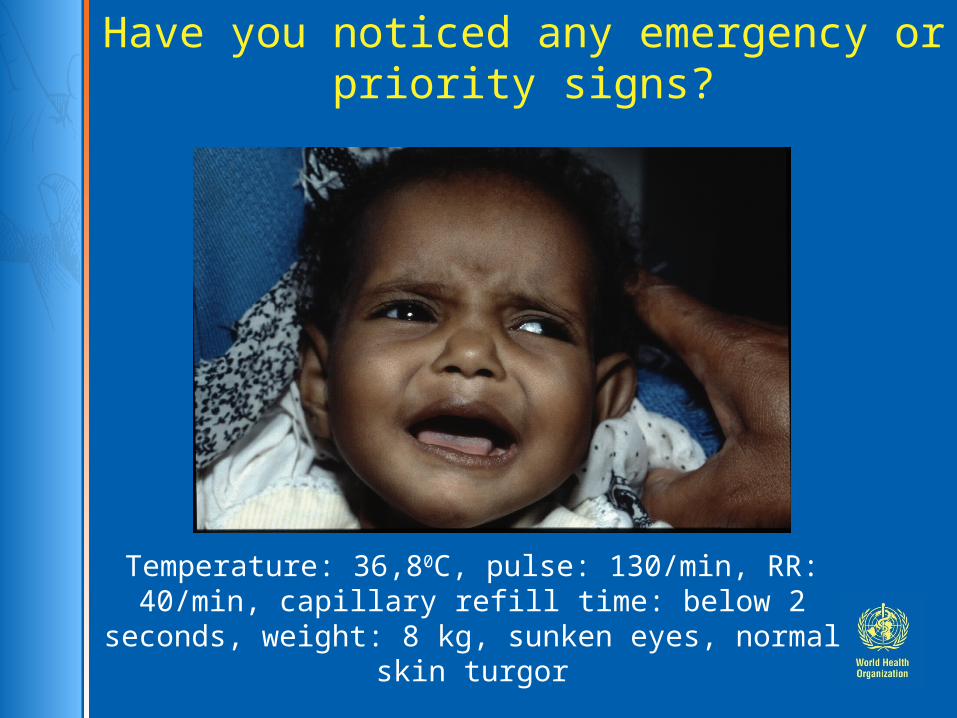
Have you noticed any emergency or priority
signs?
Temperature: 36,80C, pulse: 130/min, RR: 40/min, capillary refill time: below 2 seconds, weight: 8
kg, sunken eyes, normal skin turgor
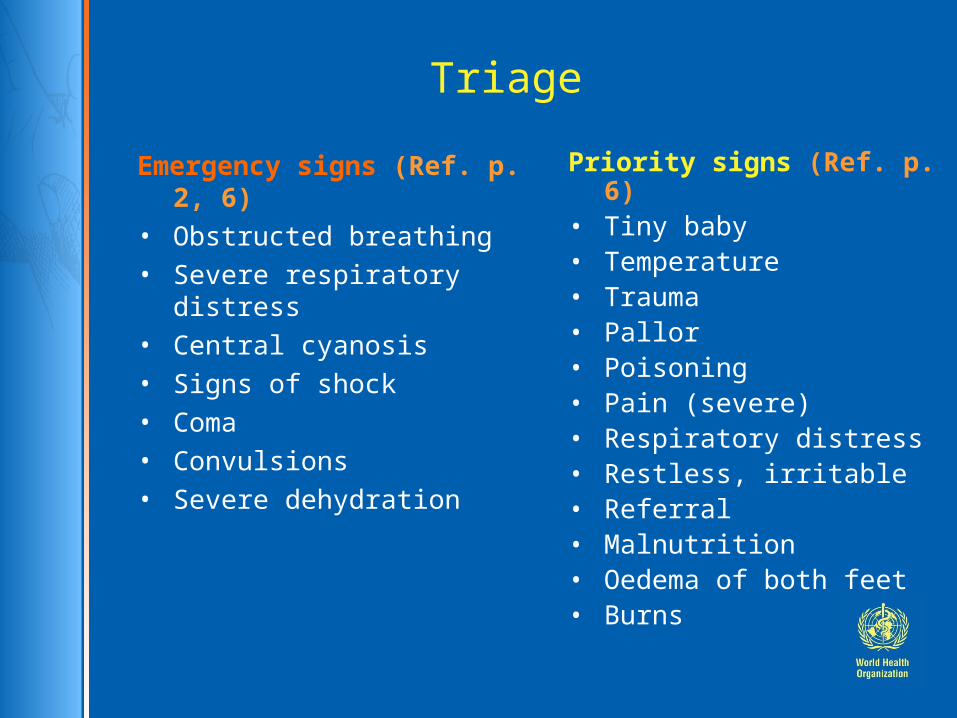
Triage
Emergency signs (Ref. p. 2, 6)
• Obstructed breathing• Severe respiratory distress• Central cyanosis• Signs of shock• Coma• Convulsions• Severe dehydration
Priority signs (Ref. p. 6)• Tiny baby• Temperature• Trauma• Pallor• Poisoning• Pain (severe)• Respiratory distress• Restless, irritable• Referral• Malnutrition• Oedema of both feet• Burns
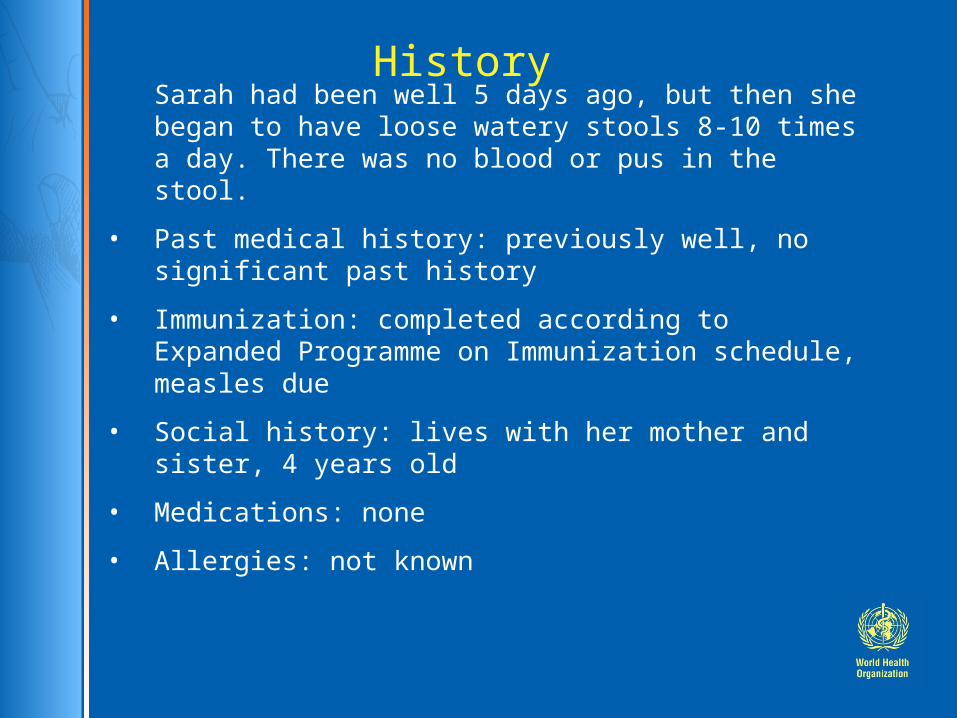
HistorySarah had been well 5 days ago, but then she began to have loose watery stools 8-10 times a day. There was no blood or pus in the stool.
• Past medical history: previously well, no significant past history
• Immunization: completed according to Expanded Programme on Immunization schedule, measles due
• Social history: lives with her mother and sister, 4 years old
• Medications: none
• Allergies: not known
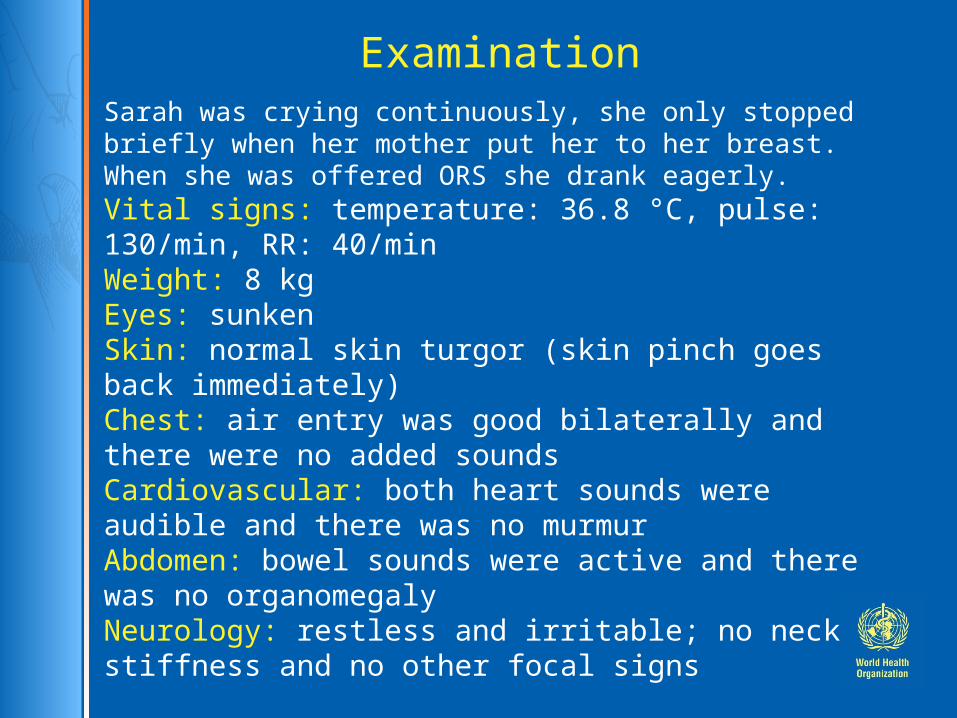
ExaminationSarah was crying continuously, she only stopped briefly when her mother put her to her breast. When she was offered ORS she drank eagerly. Vital signs: temperature: 36.8 °C, pulse: 130/min, RR: 40/minWeight: 8 kgEyes: sunkenSkin: normal skin turgor (skin pinch goes back immediately)Chest: air entry was good bilaterally and there were no added soundsCardiovascular: both heart sounds were audible and there was no murmurAbdomen: bowel sounds were active and there was no organomegaly Neurology: restless and irritable; no neck stiffness and no other focal signs
Differential diagnoses
• List possible causes of the illness • Main diagnosis• Secondary diagnoses • Use references to confirm (Ref. p.
127)
Differential diagnoses (continued)
• Acute (watery) diarrhoea• Cholera• Dysentery• Persistent diarrhoea• Diarrhoea with severe malnutrition• Diarrhoea associated with recent antibiotic
use• Intussusception
Additional questions on history
• Diarrhoea
– frequency of stools
– number of days
– blood in stools
• Local reports of cholera outbreak
• Recent antibiotic or other drug treatment
• Attacks of crying with pallor in an infant
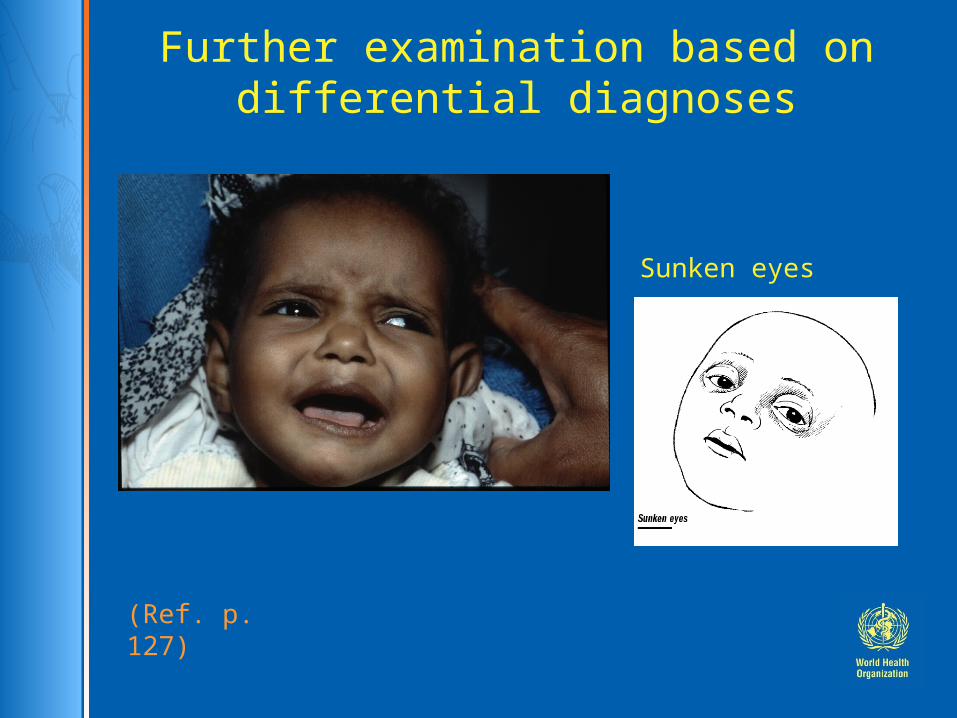
Further examination based on differential diagnoses
Look for:• Signs of dehydration such as: restlessness, irritability, lethargy, sunken eyes, skin pinch returns slowly• Blood in stool• Severe malnutrition• Abdominal mass• Abdominal distension
Further examination based on differential diagnoses
Sunken eyes
(Ref. p. 127)
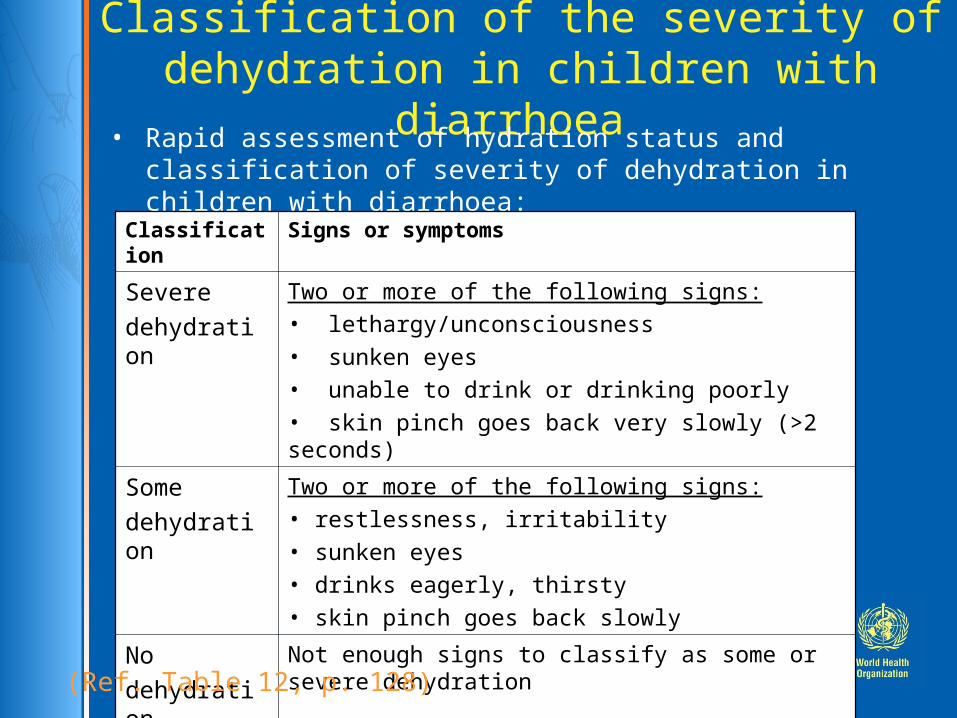
Classification of the severity of dehydration in children with diarrhoea • Rapid assessment of hydration status and classification of
severity of dehydration in children with diarrhoea:
Classification Signs or symptoms
Severe
dehydration
Two or more of the following signs:
• lethargy/unconsciousness
• sunken eyes
• unable to drink or drinking poorly
• skin pinch goes back very slowly (>2 seconds)
Some
dehydration
Two or more of the following signs:
• restlessness, irritability
• sunken eyes
• drinks eagerly, thirsty
• skin pinch goes back slowly
No
dehydration
Not enough signs to classify as some or severe dehydration
(Ref. Table 12, p. 128)
Please summarize the signs of
dehydration you noticed in Sarah
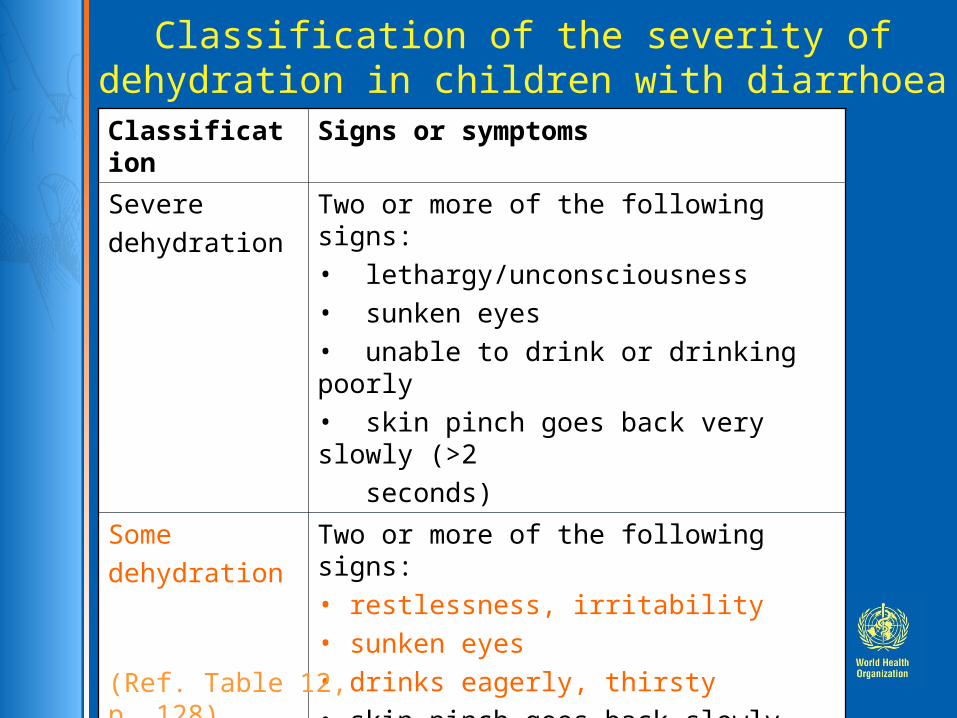
Classification of the severity of dehydration in children with diarrhoea
Classification Signs or symptoms
Severe
dehydration
Two or more of the following signs:• lethargy/unconsciousness • sunken eyes• unable to drink or drinking poorly• skin pinch goes back very slowly (>2
seconds)
Some
dehydration
Two or more of the following signs: • restlessness, irritability• sunken eyes• drinks eagerly, thirsty• skin pinch goes back slowly
No
dehydration
Not enough signs to classify as some or severe dehydration
(Ref. Table 12, p. 128)
What investigations would you
like to do to make your diagnosis ?
At this stage no additional
investigations are necessary
Summary of findings:
Examination: restlessness, irritability, sunken eyes, drinks eagerly, thirsty
Acute diarrhoea with some dehydration
Diagnosis

How would you treat Sarah?
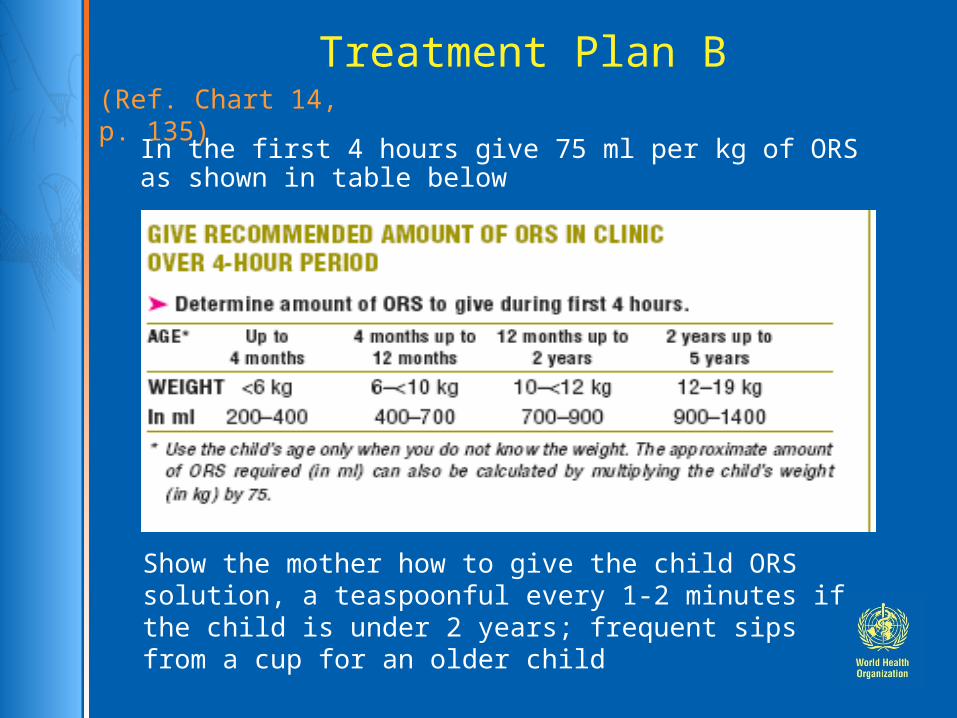
Treatment Plan B
In the first 4 hours give 75 ml per kg of ORS as shown in table below
Show the mother how to give the child ORS solution, a teaspoonful every 1-2 minutes if the child is under 2 years; frequent sips from a cup for an older child
(Ref. Chart 14, p. 135)
Treatment (continued)• After 4 hours:
- Reassess the child and check the signs of dehydration
- Select the appropriate plan to continue (discharge if necessary to Treatment Plan A or C)
- Begin feeding the child in clinic
• If the mother must leave before completing treatment:
- Show her how to prepare ORS at home- Give her enough ORS packets to complete
rehydration- Explain the 4 Rules of Home Treatment:
1.Give extra fluid2.Give zinc supplements3.Continue feeding 4.When to return
Treatment (drugs)
• Antibiotic treatment is rarely necessary (Ref. p. 126)Only for:
Dysentery (mostly Shigella) Cholera Neonates with diarrhoea and fever
• Anti-diarrhoeal agents Never necessary and often harmful!
What supportive care and monitoring are required?
Supportive Care
•Check regularly to see if there are problems (Ref. p. 132-136 )
–If the child vomits, wait 10 minutes, then, resume giving ORS solution more slowly–If the child's eyelids become puff, stop ORS solution and give plain water or breast milk
•Advise breastfeeding mothers to continue to breastfeed whenever the child wants
•Infection control: hand washing in clinic and hospital
Monitoring
• The child should be checked by nurses frequently
• Use a Monitoring chart (Ref. p. 320, 413) • Pay special attention to signs of dehydration such as:
lethargy/unconsciousness sunken eyes unable to drink or drinking poorly skin pinch goes back slowly or very slowly (>2 seconds) restlessness, irritability drinks eagerly, thirsty
Summary• Sarah was rehydrated with oral rehydration solution.
• She was discharged on the same day when she was alert, able to drink and eat.
• Before discharge home Sarah was given zinc supplements.
• At the time of discharge her mother was given advice on how to give extra fluid, to continue feeding and when to return.
• She was also given a Mother’s card containing this information and two packets of oral rehydration solution.