Embed Size (px)
Citation preview

163
Chapter 4
Efficacy of screening
The core concept of screening is thatdetection of early disease offers theopportunity to change its prognosis.Earlier diagnosis may improve prospectsfor survival because early interventionpermits treatment at a more tractablestage (Morrison, 1992). However, asexperience with screening has accumu-lated and understanding of cancer biologyhas evolved, it has become apparentthat there is much heterogeneity amongcancers at particular sites, and that thisheterogeneity can influence the impactof screening. Models of screeningshould take account of this heterogeneity.
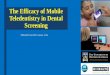
General definitionsA simplified model of screening is pre-sented in Figure 47. Several definitionsare needed to understand this model.First, the model assumes that there isa period in which there is no detectabledisease, but early malignant changesmay have taken place and a clone ofcells is dividing and de-differentiatinguntil it attains a size that can bedetected by screening. The point atwhich a lesion can be found by screen-ing is the beginning of the sojourn time(Zelen & Feinleib, 1969) or ‘detectablepreclinical phase’ (DPCP) (Cole &Morrison, 1980). For cervical cancerscreening, lesions during the DPCPare mainly preinvasive, but also include
some early invasive and microinvasivelesions. ‘Lead time’ refers to the periodbetween the moment a lesion is foundby screening and the time of diagnosisof the invasive cancer that would havedeveloped (Morrison, 1992). Sojourntime is a combined function of thelesions and of the screening test. Leadtime will in addition usually be affectedby the frequency of screening, depend-ing on the distribution of the sojourntime. Both sojourn time and lead timewill vary widely in a population. Neitheris directly observable for an individual,unless a screening test is repeated atfrequent intervals, the results of a posi-tive screening test are ignored and thewoman is observed until she becomessymptomatic. Such a situation is clearlynot tenable. However, in a populationthat has undergone screening, the dis-
tribution of lead time and sojourn timecan be estimated (Walter & Day, 1983).
Sensitivity of the screening testfor early detection of invasivelesionsIn addition to sojourn time and leadtime, two parameters traditionally ofimportance in screening are sensitivityand specificity. For a condition whicheither exists or does not, such as Tay–Sachs disease, these two parametersare defined in terms of a 2 x 2 table:
Methodology and analytical issues inassessment of efficacy
Figure 47 Scheme of progression of a chronic disease, with the interventionof an early-detection screening test
No detectable disease Sojourn time
Asymptomatic detectable disease
Symptomatic invasive disease
Time
Lead time
Screening testdetects
preclinical disease
Delay time
T0 T1T2
Result of ‘True’ disease statescreening test Positive Negative
Positive a bNegative c d
Sensitivity = a/(a + c), specificity = d/(b + d)
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 163

164
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
The situation is more complex forscreening for cervical cancer, becauseit is a progressive condition. At the timeat which screening is performed, thereis no ‘gold standard’ diagnostic test forthe disease: the condition beingscreened for is a future invasive dis-ease. The ‘true’ disease state beingsought at the time of screening is alesion that will progress into an inva-sive cancer. This state can be deter-mined for an individual only by follow-ing her forward in time. Since, however,a positive result at screening shouldlead to an intervention to prevent thedevelopment of a clinical cancer, muchof the information required for directestimation of sensitivity and specificitywill be missing, so that there is nodirect measure of the quantity a in thetable. If one follows forward in time agroup of individuals who showed nolesion on the screening test, some willdevelop invasive disease. There is atradition to estimate the unknownquantity c by follow-up after screening:the women who develop invasive dis-ease after a negative screening resultthus constitute the cell entry c in thetable above.
The length of time after screeningthat is used to define this group of‘screen-negative’ and ‘disease-positive’individuals is variable, and is a some-what arbitrary interval. The intervalbetween screening rounds is a naturalchoice if an organized rescreening pro-gramme is being evaluated.
In actual screening programmes, avariety of screening intervals are usedand a relatively long interval may beused to define sensitivity. This has theadvantage that it is less subject to sta-tistical variation due to small numbersand less dependent on the exact dateof diagnosis, although more affectedby bias due to new cancers. Clearly,the longer the interval used to definesensitivity, the lower will be the result-ing estimate (as follows from the dis-cussions below and Figure 48).
To estimate sensitivity, one mustthen identify the individuals, or indi-rectly estimate their number, who con-stitute the cell entry a. The ‘true’ dis-ease state is agreed to be invasivecancer appearing after a positivescreening episode. Thus one needs toestimate the number of lesions,detected at screening and treated,which in the absence of screeningwould have progressed to an invasivecancer. This group forms the screen-positive, disease-positive group. Thequantity a + c is the number of cancersthat would have presented as franklyinvasive cases in the screened group ifno screening had taken place. If onehas a directly comparable unscreenedpopulation, as in a randomized trial,the quantity a + c is observable. In theabsence of a comparison group strictlydefined by randomization, otherapproaches are needed, but for anygeneral population sample, estimatesbased on age-adjusted cancer inci-dence data from a comparable popula-tion or a time when screening was notpractised should provide a goodapproximation, if used judiciously. Thequantity a is then obtained by subtrac-tion, and the episode sensitivity esti-mate is given as before (Day, 1985):
a/(a + c).This approach to the estimation of
sensitivity, called the ‘incidence method’,
can be expressed graphically as inFigure 48 and can be used to estimatesensitivity by means of the proportion-ate incidence of interval cancers (seebelow).
Since screening for cervical canceris aimed at detection of preclinicallesions, most of which are preinvasive,the estimate of a/(a + c) (for invasivedisease) is to be interpreted as the pro-portion of screen-detected preinvasivelesions that would have progressed toinvasion among all lesions in theDPCP that would have progressed toinvasion.This is equal to one minus theproportion of observed invasive cancerpost-screening to the expected inva-sive cancer rate in the absence ofscreening.
An additional issue is the catego-rization of microinvasive (stage IA1)disease. This is almost always screen-detected and can be effectively treatedwith minimal morbidity. While this cate-gory is usually included among theinvasive cancers, for the evaluation ofscreening, it should be considered as asuccess and is best included with thecarcinoma in situ or CIN 3 cases as aless than fully invasive lesion.
It should be realized that diagnosticissues related to disease verification asdiscussed in Chapter 2 are fundamen-tal to this discussion. The frequency ofdisease that is identified in a screening
Figure 48 Sensitivity defined in terms of one-year proportionate incidence:incidence of interval cancers as a proportion of the incidence in a comparableunscreened population
Incidence in a comparableunscreened population
Incidence after screening,among individuals screened
negative
100%
Time since screening (years)
163-200 ( VOIR IMAGES) 24/01/05 14:57 Page 164

programme is also dependent on thediagnostic methods that are used toaugment colposcopy and biopsy (e.g.,LEEP investigation) and on howaggressively one looks for disease.
Positive predictive value andspecificityA similar approach can be taken to thedefinition of specificity and positivepredictive value, as, if one has esti-mates of the values of a and c, and a +b and c + d are known from the resultsof screening, then clearly one has esti-mates of b and d. For positive predic-tive value, for example, it is of specialinterest to estimate the proportion oflesions detected at screening thatwould have progressed to clinical can-cers (i.e., a/(a + b)) before the nextround in a periodic screening pro-gramme. For specificity, or rather itscomplement, one might be interestedin the proportion of individuals whohad a positive screening result amongthose who would not have developed aclinical cancer in the interval betweenscreening tests (i.e., b/(b + d)). Thepositive tests that were confirmed neg-ative should be included for the testspecificity. The test validity indicatorscorrespond to each other like those ofepisode validity. In particular, it is defi-cient to report (only) episode speci-ficity and only test sensitivity.
Attention should also be paid to thedefinition of the screening test.Screening for cervix cancer is essen-tially a multiple-step process, with theinitial screening test leading, if positive,to more detailed investigations, culmi-nating in a biopsy for a definitive diag-nosis. The definitions of sensitivity andspecificity discussed in this sectionrefer to the complete screeningepisode, the final assessment of posi-tivity or negativity being based on theresults of the screening test and all further assessment. It is a commonexperience that women with a positivetest but classified as negative (i.e.,
disease-free) on further assessmentare at higher risk of subsequent dis-ease than the general population. Theimplication is that if only the screeningtest is considered, it will be more sen-sitive than the overall screeningepisode, although of course with lessspecificity. The sensitivity of screeningtests could be estimated in analogousfashion to the sensitivity of the com-plete screening episode, but in practicesuch estimation is rarely attempted.
Relative sensitivity of differentscreening testsThe preceding paragraph consideredsensitivity as the capacity of a screen-ing episode and test to detect futureinvasive disease. This measure mightbe termed absolute sensitivity. Often,however, one requires a more rapidand direct method of comparing thesensitivity of two screening tests, probably based on cross-sectionalrather than follow-up data. In this situa-tion, it is useful to define the relativesensitivity of the two tests in terms of asurrogate measure of future invasivedisease. In the context of cervicalscreening, this surrogate is usuallytaken as histological diagnosis of thescreen-detected lesions.
It should be noted that not alllesions diagnosed histologically asmalignant would have progressed toinvasive cancers. It is known that manypreinvasive lesions, including CIN 3 andcarcinoma in situ, will regress. Further-more, colposcopically directed biopsies
are known to miss significant lesions. Itis therefore clear that relative sensitivityand absolute sensitivity are measuresof different quantities. Relative sensitiv-ity would normally be larger thanabsolute sensitivity, due to overdiagno-sis at histology and the length bias ofcytologically detected lesions. Hence, ifrelative and absolute sensitivities differ,due to inherent bias in the relative sen-sitivity, the absolute sensitivity will givethe more correct estimate.
To determine relative sensitivity, asample of women would undergo bothscreening tests (e.g., split-samplestudies; see Chapter 2). In some stud-ies, all women then undergo col-poscopy as well, and the histologicaldiagnosis is obtained on the entiresample. The results would then besummarized as in the table below.
The sensitivity of test 1 relative tohistology is then w1/(w1 + x1), and oftest 2 is w2/(w2 + x2). The specificity oftest 1 relative to histology is z1/(y1 +z1), and of test 2 is z2/(y2 + z2).
Since the same women undergoboth tests, w1 + x1 = w2 + x2 (the num-ber positive by histology), so the com-parison of the relative sensitivities ofthe two tests is given simply by theratio w1/w2.
Thus to compare the relative sensi-tivities of the two screening tests, it isonly necessary to obtain histologicaldiagnosis on all women positive on atleast one of the two tests.
Many studies of comparative sensi-tivity and specificity in fact only have
165
Efficacy of screening
Histological diagnosisPositive Negative
Screening test 1 Positive w1 y1
Negative x1 z1
Screening test 2 Positive w2 y2
Negative x2 z2
Detection rate of Test 1 is w1/(w1 + x1 + y1 + z1)Test positivity rate of Test 1 is (w1 + y1 )/(w1 + x1 + y1 + z1)
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 165

histological diagnosis available onthose positive on one of the screeningtests to be compared. These studiesgive an unbiased estimate of the ratioof their respective relative sensitivities,provided all those positive on one ofthe two screening tests have a histo-logical diagnosis available. However,they give a biased overestimate of thesensitivity relative to histology, as theyexclude from the denominator womenpositive by histology but negative on thescreening tests under consideration.
Estimates of specificity can also beobtained from such studies, sincethere will be women negative on one ofthe screening tests among the womenwho are positive on at least one of thetests. This estimate will be severelybiased (underestimated), since a majorcomponent of a correct specificity esti-mate will be women negative on bothscreening tests and by histology.
This bias in sensitivity and speci-ficity is known as the verification bias(Franco, 2000, 2003). Some studieshave chosen a sub-sample of womennegative on the screening test toundergo a histological diagnosis, inorder to attempt to correct for verifica-tion bias. This attempt may be more orless successful, depending on the sizeof the sample, the comparability of thecolposcopy and perhaps other factorsin reducing verification bias. An exam-ple of correction for verification bias isgiven in Table 58 (taken from Ratnamet al., 2000). The effects are clearlylarge. [The ratio of the uncorrectedsensitivities differs slightly from theratio of the corrected sensitivities sincenot all women positive on one or bothof the two tests were included in theuncorrected estimates, althoughincluded in the corrected estimates.]
One must also be alert to potentialbias in the interpretation of the net efficacy of screening when two testsare used in series or in parallel in thesame women (Macaskill et al., 2002).A nominal increase in relative sensitivity
always occurs by chance whenever anadjunct test (e.g., HPV DNA testing) isused in parallel with a conventionalone (e.g., cytology), even if the newtest gives totally random results withrespect to the disease being evalu-ated.This increase in sensitivity can bemisleading, even if deemed significantby a statistical test. Combined testingprevents a loss in specificity but mayoffer no real sensitivity gain in certainconditions (Franco & Ferenczy, 1999).An empirically valuable adjunct test,such as the HPV assay, should com-plement cytological testing so that thenet combined sensitivity and specificitywill be truly superior to those of cytol-ogy alone. In practice, we can computethe "expected null values" for sensitiv-ity and specificity using the followingformulae (Franco, 2000):
Sexp = Scyt + P (1 – Scyt)
for the expected null sensitivity, and
Wexp = Wcyt – P (Wcyt)
for the expected null specificity,where S = sensitivity, W = speci-
ficity, Scyt and Wcyt represent, respec-tively, the sensitivity and specificity forthe original cytological test, Sexp andWexp denote the adjusted (for the addition of the new test) sensitivity andspecificity, and P is the expected
positivity rate for HPV testing or anyother test used as an adjunct to cytologyin the same population. These expectedvalues should then be used in a com-parison with the equivalent indices fromthe combined testing approach.
An analogous issue to the latterbias that stems from the application ofadjunctive testing may also appear inrandomized controlled trials as anasymmetry problem. Figure 49 illus-trates this problem using a genericexample with two screening tests, one(test A) that serves as the paradigm(e.g., cytology) and the other (test B)that serves as the adjunctive, experi-mental technology (e.g., HPV DNAtesting), whose benefit is to be evalu-ated. If a trial is designed without long-term follow-up, it will probably misinter-pret the difference between arms indetection rates of preinvasive lesionsas being indicative of the putative effi-cacy attributable to the intervention.One needs to exercise caution andavoid inadvertently claiming that thecombination of cytological and HPVDNA testing in such trials is superiorsimply because it detected moreprevalent (or short-term incident) high-grade lesions than the cytology-onlyarm, as a measure of the greater sen-sitivity of the combined testing approach.The asymmetry bias virtually guaranteesthat this would happen even if the HPVtest performed randomly with respect to
166
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
Screening Definition of Uncorrected Corrected
Sensitivity Specificity Sensitivity Specificity
Cytology LSIL or worse 38.2 80.5 26.8 96.2
HPV Positive 85.3 58.0 68.1 90.6
Combination HPV+ or ≥ LSIL 97.1 51.3 76.3 89.3
From Ratnam et al. (2000)
Table 58. The effect of verification bias on estimate of sensitivity andspecificityNewfoundland Study: screening performance after correction for verification bias(HSIL or worse)
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 166

lesions and cytology. This is becausethere will be more women selected fortriage, which will increase the probabilityof detecting incipient lesions that wouldnever be found were it not for the contri-bution of the adjunctive test, howeverinadequate it may be (Franco, 2004).
A more complex view of cancerThe model shown in Figure 47describes the operational process ofscreening, incorporating no informa-tion on the biology of the carcinogenicprocess. Current knowledge of theneoplastic process allows us to distin-guish a number of steps, which maybegin with mutation at specific geneticloci and other cellular events and con-tinue until cells divide and disseminatethroughout the organism. Cancerdevelopment is a long process, and notall the steps are necessarily irre-versible. In the future, screeningmodalities may be developed to targetthese early molecular changes. In thatcase, more complex models of thescreening process will be required.
If all women do not undergo eachtest, w1 + x1 is no longer equal to w2 + x2
(as in the direct-to-vial studies men-tioned in Chapter 2). While cross-sec-tional analysis mimics the relationshipbetween relative sensitivities, follow-upmay allow estimation of the absolutesensitivities, depending on the validityof controls.
Methods used to evaluate theefficacy of screeningReductions in mortality and/or inci-dence of invasive disease are funda-mental measures of the efficacy ofscreening. A reduction in the incidenceof invasive disease as a consequenceof the treatment of disease precursorsis a predictor of a reduction in mortalityfrom cervical cancer.
Because screening for cervical can-cer results in the detection and treat-ment of precursors, reduction in theincidence of the disease is an appropri-ate outcome measure. Reduction inmortality was used in some early stud-ies to evaluate cervix cancer screening.It is accepted that case survival is notan appropriate outcome, because oflead time, length bias, selection biasand overdiagnosis bias.
Randomized controlled trials arethe most valid method to assessreductions in mortality or incidenceconsequent on screening (Prorok etal., 1984), but until recently have notbeen employed in the evaluation ofscreening for cervical cancer.
Use of observational studies inevaluation of screeningObservational studies can be used toevaluate the efficacy of screening,provided that the programme wasintroduced sufficiently long before thestudy that an effect can be expectedto have occurred. The major bias thatpotentially affects observational stud-ies in the evaluation of screening isselection bias, as the health-consciousmay select themselves for screeningand are likely to have different underly-ing (lower) risks of developing cancerof the cervix from those who refusescreening. Thus any comparison thatessentially compares the incidence ofcancer of the cervix in those whoaccept invitations to attend for screen-ing with those who decline such invita-tions is potentially affected by selectionbias.
In the cohort study design, the inci-dence of cancer of the cervix in anindividually identified and followedscreened group (the cohort) is com-pared with the incidence in a controlpopulation, often derived from the gen-eral population, sometimes using datafrom before screening started, or fromanother study population in whichscreening has not been used. The inci-dence in the controls should beadjusted for the incidence in therefusers (Cuzick et al., 1997) for a validestimate of efficacy. An estimate of efficiency is obtained by comparing theincidence in those offered screening(attenders and refusers) with thatamong controls. A historical comparisoncould be biased if changes in risk fac-tors in the population are affecting theincidence of the disease. If mortality
167
Efficacy of screening
Figure 49 Intervention asymmetry bias in randomized controlled trials of anadjunctive screening test with short-term follow-up
Intervention asymmetry
Cross-sectional detection of lesions with or without follow-up
Greater frequency of patients with lesions in combination armbecause more women are referred to the gold standard test
Randomization
Test A (conventional) Test A + Test B
163-200 ( VOIR IMAGES) 27/01/05 16:09 Page 167

were to be used as the end-point, itmust be recognized that thoserecruited into a screening programmeare initially free of the disease of inter-est, so that it is not appropriate toapply population mortality rates for thedisease to the person-years experienceof the study cohort. Rather, as isrequired in estimating the sample sizerequired for a controlled trial of screen-ing, it is necessary first to determine theexpected incidence of the cases ofinterest, then apply to that expectationthe expected case-fatality rate from thedisease to derive the expectation for thedeaths (Moss et al., 1987). In practice, itis difficult in a cohort study of screeningto adjust for selection, so the resultshave to be interpreted with caution.
A case–control study of screeningis another approach that can be usedto evaluate screening. Case–controlstudies should be designed to mimicrandomized controlled trials as far aspossible, especially in terms of thecases used (ideally, in this instance,cases of invasive cancer of the cervix).They depend on comparing thescreening histories of the cases withthe histories of comparable controlsdrawn from the population from whichthe cases arose. Individuals with early-stage disease if sampled would be eli-gible as a control, providing the date ofdiagnosis was not earlier than that ofthe case, as diagnosis of disease trun-cates the screening history. However, abias would arise if advanced diseasewere compared only with early-stagedisease, as the latter is likely to bescreen-detected, though this is just afunction of the screening process, not itsefficacy (Weiss, 1983). Cases have toreflect the end-points used to evaluate screening, i.e., those that wouldbe expected to be reduced by screening.
Selection bias may be difficult toadjust for in the analysis, though thisshould be attempted if relevant data onrisk factors for the disease (con-founders) are available. Such bias may
not be a problem, however, if it can bedemonstrated that the incidence ofcancer in those who declined the invi-tation to the screening programme issimilar to that expected in anunscreened population. This is onlyseldom true, however (see Chapter 3).
Even if data are available on riskfactors for disease, control for themmay not result in avoiding the effect ofselection bias. Experience in breastcancer screening studies in Swedenand the United Kingdom, wherecase–control studies were performedwithin trials, shows that althoughbreast cancer incidence among thosewho refuse invitations for screening issimilar to that of controls, their breastcancer mortality experience is worsethan that of controls. This means thatthe estimate of the effect of screeningin such case–control studies will begreater than could be expected in thetotal population (Miller et al., 1990).This differential could also arisebecause the case–control analysisdirectly measures the effect in thosescreened.
There are other problems withcase–control studies of screening,notably two relating to the exposuremeasure (Weiss, 1994, 1998). One isthe issue of excluding tests that aredone because the disease is present.These are so-called diagnostic tests,often performed in women with symp-toms, or suspected to be at high risk.The second is that of bias due tocounting only negative tests as expo-sure to screening. This will bias theresult by omitting positive tests,although these are the only tests thatcan possibly influence risk of disease.
Assessing the efficacy of a newscreening testWhen a new screening test becomesavailable as a supplement or even areplacement for a screening test that isknown to be effective in reducing inci-dence of invasive cancer, a compara-
tive assessment can be made in termsof absolute sensitivity. Since absolutesensitivity, as defined earlier, quantifiesthe reduction in the incidence of inva-sive disease following screening, acomparison between two tests of theirabsolute sensitivity should be predic-tive of the comparative efficacy of thetwo tests. Often, however, it will initiallybe easier to compare relative sensitiv-ity, and specificity, in cross-sectionalstudies using histological diagnosis ofpreinvasive lesions as a surrogate.These results need to be interpretedwith caution, since a proportion of suchpreinvasive lesions will have littlepotential to progress to invasion.However, if the new test identifies boththe lesions detected by the existingtest (or the great majority of suchlesions) together with additionallesions, the problem of differentialregression of lesions identified by thenew test is of less concern.Nevertheless, confirmation, preferablyby follow-up studies to establishabsolute sensitivity, would normally berequired before the new test can beconsidered of at least equal efficacy tothe existing test.
The Working Group concluded thatat present no surrogate marker suit-able for evaluating the efficacy of anew screening test for cervical cancerhas been fully established.
Randomized trialsEfficacy of cervical cancer screeningprogrammes using cytological testingwas never tested in a randomized trial.Evidence has therefore been derivedfrom observational studies (cohort andcase–control). Studies relating trendsin cervical cancer incidence or mortal-ity to screening have also providedvery convincing evidence in support ofthe effectiveness of these pro-grammes, as described in Chapter 5.
168
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
Cytological screening
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 168

Cohort studiesIn the evaluation of cervical cancerscreening, the ‘exposure’ has beendefined in cohort studies either by invi-tation to screening or by participationin screening. In efficacy trials (random-ized), there is no bias, but in observa-tional studies several biases must beassumed. In the early studies, therates expected in the absence ofscreening were usually calculated fromthe population rates during the latestperiod before screening was imple-mented or from concurrent rates inareas without a screening programme.More recently, reference rates wereobtained either from those among non-screened or non-participants, or fromthe average rates in the general popu-lation during the screening period. Instudies that followed incidence amongparticipants and compared it with thatamong non-participants, there ispotential for selection of a morehealthy group to participate comparedwith non-participants (see Chapter 3),which would introduce a bias towardsoverestimation of the impact of screen-ing. In studies using the general popu-lation rates as the reference, a largepart of the general population hadbeen screened in the programme.Therefore, only the early studies with anon-targeted population (not intendedto be screened) as controls will in prin-ciple give estimates on efficiency withless bias, i.e., on the effect if screenedalbeit not in ideal but in routine condi-tions. This, however, assumes that therisk in the control population wasadjusted for the risk among non-responders to screening (Cuzick et al.,1997). Such adjustment was done by theWorking Group and is indicated in brack-ets in the following and called an efficacyestimate. Not all cohort studies providedthe necessary information for such a cor-rection, however, and none of the studieswith non-responders as controls or inci-dence in the total population as refer-ence value can yield such an estimate.
Several of the cohort studiesreviewed below, which use invasivecervical cancer as the main outcomeparameter, were included in a reviewby Lynge (2000), upon which thischapter is based.Table 59 summarizesthe characteristics and main findings ofthe cohort studies.
British Columbia, CanadaThe British Columbia cervical cancerscreening project started in 1949. In1959, about 8% of women above theage of 20 years were screened, andabout 44% in 1971. The first cohortstudy was based on the population incidence data and individual screen-ing records from 1958 to 1966. In1965, 13 clinical invasive carcinomaswere detected among the screenedwomen, with 81.2 cases expectedbased on the 1955–57 incidence rates(standardized incidence ratio (SIR) =0.16). Among the unscreened women,the numbers were 67 and 62.1 respec-tively (SIR = 1.08).The effectiveness ofthe programme was estimated for thetotal population at 80 observed versus143.4 expected (SIR = 0.56). [The effi-cacy estimate of the SIR corrected for selective participation (Cuzick et al.,1997) was 0.17.] Pre-clinical invasivecancers were not included among theobserved cases (Fidler et al., 1968). Alater cohort study from the same pro-gramme reported cancer incidencerates after negative tests (vanOortmassen & Habbema, 1986)(included in the IARC study (IARC,1986), see below).
FinlandOne of the first indications of the mag-nitude of the effect of screening for cer-vical cancer in the Nordic countrieswas provided by a cohort study(Hakama & Räsänen-Virtanen, 1976).In Finland, an organized screeningprogramme started in 1963 and itgradually developed to become nation-wide. A cytological test was offered
every fifth year to all women aged30–55 years. Data on 407 000 womenscreened at least once during1963–71 and followed up from theirfirst screening until the end of 1972revealed that the (relative) risks ofinvasive cervical cancer were 0.2 aftera negative test and 1.6 among non-attenders, in terms of the unit risk ofreference from the overall Finnish inci-dence in years preceding the start ofthe programme. There were 1.4 millionwoman-years in the follow-up of inva-sive carcinoma among screenedwomen, and their average follow-uptime was thus 3.5 years. The effect ofthe screening test applied was 80%(100 x (1.0 – 0.2)), without correctionfor the selective attendance. The atten-dance rate was 85%, and the effective-ness of the public health service wasestimated at 60%, indicating the resultof outcome evaluation of the pro-gramme among the whole populationin that early follow-up phase. [The effi-cacy estimate for SIR corrected forselective attendance was 0.22].
A further cohort follow-up study inFinland was based on the follow-up ofa sample of 45 572 women with aPapanicolaou group I test result in themass screening programme during1971–76, when up to the third invita-tional round was in action (Viikki et al.,1999). The follow-up was performedusing the files of the cancer registry upto 1994, and the reference risk wasobtained from expected numbers cal-culated from the general populationrates, including women screened inthe programme. Overall, 48 invasivecancers were observed (SIR = 0.5;95% CI 0.4–0.7). In the five-year fol-low-up since screening, the SIR esti-mates were, respectively, 0.3 and 6.5among those with Papanicolaou groupI or II–V results but no malignancy con-firmed in the screening episode.Follow-up of those with a positive testresult at entry was also reported byViikki et al. (2000). The SIR estimate
169
Efficacy of screening
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 169

170
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
Table 59. Characteristics and main findings from the cohort follow-up studies on screening impact on cervicalcancer
Location(reference)
BritishColumbia,Canada(Fidler etal., 1968)
Finland(Hakama &Räsänen-Virtanen,1976)
Iceland(Johannes-son et al.,1978)
Maribo,Denmark(Berget,1979;Mellem-gaard et al.,1990;Lynge,2000)
Østfjold,Norway(Magnus etal., 1987)
Cervicalcancerend-point
Incidence,clinicalsquamouscarcinoma(invasive)in 1965
Incidence,invasivecarcinomaafter thefirst pro-grammetest
Mortalityfrom cer-vical can-cer
Incidenceof cervicalcancer
Incidenceand mor-tality, inva-sive carci-noma[after invi-tation]
Screeningassessment
Screened previ-ously at leastonce in the pro-gramme
Unscreened inthe programme
Screened atleast once inthe programme
Unscreened inthe programme
Women with aninitial negativescreeningNever-screened,follow-up in1965–69Never-screened,follow-up1970–74
Participated inscreening (afterinvitation)
Not participated(after invitation)
Whole studypopulation
Screened
Unscreened
Observed(expected) rate per 100 000
4.2 (26.2)
28.8(26.6)
7.7 [38.5]
NR
2.6 (NR)
29.5 (NR)
23.5 (NR)
NR
No. ofcases/deathsobserved(expected)
13 (81.2)
67 (62.1)
109 [545]
NR
115 (217)
63 (35.96)
267 (341.5)incidence103 (123.9)mortality178 (286.1)incidence55 (102.6)mortality89 (55.4)incidence48 (21.3)mortality
Rela-tiverisk
0.16
1.08
0.2
1.6
0.53
1.75
0.78
0.83
0.62
0.54
1.61
2.25
Comments
Pre-clinical'occult' invasivecarcinoma notincluded
Average follow-uptime 3.5 yearsamong screenedwomen (1.4 mil-lion person-years).Expectation wasdrawn from timebefore screening.
Comparisongroup was thewhole Danishfemale population
.
Expectation with-out screeningwas calculatedfrom same periodand age groupsamong women in5 neighbouringregions
Cohort description: Numbers ofwomen, screening period, sourceof screening data, follow-up peri-od and source of follow-up dataa ,screening recommendation
310 000 screened and 233 000unscreened women, screening in1958–65, screening laboratorydatabase, incidence follow-up to1965, laboratory database andpathological files in the provinceplus a mortality registry, screeningrecommendation in 20+ years oldwomen once a year
406 358 screened and 35 279unscreened women, screening1963–71, screening registry, inci-dence follow-up in 1963–72, can-cer registry, screening 30–55-yearwomen every 5 years
Not reported [percentage ofwomen in 1974 who had everbeen screened was approx. 89%in women aged 30–54], screening1964–74, screening registry, mor-tality follow-up in 1965–74, cancerand mortality registry, screeningwomen of 25–59 (25–70 from1969) every 2–3 years
16 187 women invited to the firstscreening round, screening1967–70, not described, incidenceand mortality follow-up to the endof 1984, not described, notdescribed
45 960 women without previousinvasive or preinvasive lesions ofthe cervix and invited to screening,screening 1959–77, notdescribed, incidence and mortali-ty follow-up in 1959–82, cancerregistry, screening women of25–59 every 2–4 years
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 170

171
Efficacy of screening
a Vital status or losses from follow-up were not reported.NR, not reportedIf not available in the original publication, confidence intervals were estimated based on an assumption that the observed number ofcases followed a Poisson distribution (indicated in square brackets).
Table 59 (contd)
Location(reference)
Sweden(Sparén,1996)
Finland(Viikki et al.,1999)
Cervicalcancerend-point
Screenedever vsnever
Incidence,invasivecarcinomaafter 1st,2nd or 3rdpro-grammesmear
Screeningassessment
Women withany negativetests in the pro-gramme
Women with 5negative testsin the pro-gramme
Womenreferred togynaecologistwith other diag-nosis thansevere dyspla-sia, ca. in situor invasive car-cinoma
NR
Screened neg-ative
Screened neg-ative, follow-up5 years
Screened posi-tive, follow-up 5years
All attenders,follow-up 5years
Observed(expected) rate per 100 000
NR
NR
No ofcases/deathsobserved(expected)
125 (259.4)incidence
41 (92.6)mortality6 (34.2)incidence
11 (26.6)incidence
5 (10.0)mortality
438 (500among un-screened)
48 (94)
Rela-tiverisk
0.48
0.44
0.18
0.41
0.50
0.55
0.5
0.3
6.5
0.7
Comments
SIR estimate frompopulation ratesduring thescreening period(including thescreened popula-tion).Follow-up ofwomen with posi-tive results report-ed also in Viikki etal. (2000)
Cohort description: Numbers ofwomen, screening period, sourceof screening data, follow-up peri-od and source of follow-up dataa ,screening recommendation
386 990 women, screening andpopulation registries, incidence fol-low-up in 1968–92, cancer registry,any screenings
A sample of 45 572 womenscreened negative, screening in1971–76, screening registry, inci-dence follow-up in 1971–94, can-cer registry, screening 30–55 y oldwomen every 5 y
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 171

for all attenders combined was 0.7.Among non-attenders, the estimatedSIR was 1.6. The approximate relativerisk (RSIR) between attenders andnon-attenders was 0.7/1.6 = 0.44; andbetween test negatives and non-atten-ders 0.3/1.6 = 0.19 (confidence inter-vals not available). The long-term pro-tection provided by screening sched-uled every five years was evaluated.The SIR for invasive cancer remainedless than unity (with a 3% annualincrease) during all the 23-year follow-up. The SIR of preinvasive lesionsexceeded unity at follow-up year 10,i.e., at the second screening round.The results confirmed the appropriate-ness of the five-year screening intervalused in Finland.
IcelandCervical cancer screening started inIceland in 1964 and became nation-wide in 1969. Women aged 25–59were invited every 2–3 years (laterextended to women aged 25–70). In1974, approximately 89% of womenaged 30–54 had had at least one test;the age-group-specific coverage pro-portions varied from 81% to 95%.Among women aged 25–29 and 55–59years, the proportions were lower(47% and 77%). In all Icelandic womenaged 25–59, the mortality from cervicalcancer changed from 20 per 100 000in 1955–59, to 21 in 1960–64, 32 in1965–69 and 15 in 1970–74(Johannesson et al., 1978). The ratesin never-screened women 25–59 yearsold were 30 in 1965–69 and 23 in1970–74. The average mortality rateamong women with an initial negativescreening result was 2.6 per 100 000in ten years of follow-up. The popula-tion mortality rate had decreased in alater study by 60% between 1959–70and 1975–78, and the mortality ratesamong the unscreened populationwere more than ten-fold greater thanamong the screened (Johannesson etal., 1982).
Maribo, DenmarkAn organized screening programmewas started in 1967 in Maribo County,Denmark, among women aged 30–49years. The 16 187 women who wereinvited to the first round in 1967–70were followed up for incidence of cervi-cal cancer to the end of 1984 and theobserved numbers were comparedwith the expected number based onrates for all Danish women. In the 87%of the invited women who participated,115 cervical cancer cases wereobserved compared with 217 expected(SIR 0.53), whereas the numbers were63 and 35.96 (SIR 1.75) among the13% of invited women who did not par-ticipate (Berget, 1979; Mellemgaard etal., 1990; Lynge, 2000). The effective-ness of the programme estimated bythe SIR for the total population was 0.70(178/253). The comparison group wasthe total population of Denmark, wherethere was extensive spontaneousscreening, and some other organizedprogrammes were operating. TheMaribo cohort was later extended toinclude all women screened in the areain 1967–82; the results on the follow-upfor cervical cancer incidence after neg-ative tests were included in the IARCstudy (see below; IARC, 1986). [Theefficacy estimate of SIR corrected forselective attendance was 0.60, but, asmentioned above, it was affected bycontamination in the control population].
Manitoba, CanadaA province-wide cervical cytology screen-ing programme was initiated in Manitobain 1963, and included a screening reg-istry. Cases of cervical cancer wererecorded at the Manitoba CancerRegistry (Choi & Nelson, 1986).The dataon cancer incidence after a negativescreening test were included in the IARCstudy (see below; IARC, 1986).
SwedenFrom 1964 onwards, several countiesin Sweden gradually introduced
organized cytological screening pro-grammes for cervical cancer. Womenaged 30–49 years were targeted, witha four-year screening interval. The pro-gramme covered all of Sweden exceptthe municipality of Gothenburg by1973. All tests within the organizedprogramme were reported to theNational Board of Health and Welfare,where 930 127 women were registeredwith at least one test during the period1967–75. This cohort was followed upfor incidence of invasive cervical cancerto the end of 1980 (Pettersson et al.,1986). The data for women with a negative result at entry were included inthe IARC study (see below; IARC,1986).
In a later study, a cohort of 386 990women resident in Uppsala andGävleborg counties was followed up forinvasive squamous-cell cancer of thecervix (Sparén, 1996). The screeninghistories were derived from computer-ized registers including any cytologicaltests performed in the area. Recordlinkage allowed complete follow-up withregard to cancer incidence, migrationand deaths during 1968–92. The rela-tive risk of squamous-cell cervical can-cer incidence among ever- versusnever-screened women was 0.55 (95%CI 0.51–0.61). The lowest age-specificrelative risks among the screenedwomen were in the age group 40–59years (RRs from 0.27 to 0.38).
Østfold, NorwayA regional cervical cancer screeningprogramme was organized in ØstfoldCounty, Norway. The first round tookplace in 1959–65 and the last (fifth)round in 1974–77. A cohort follow-upstudy included all 45 960 women invi-ted to the first screening in the age-group 25–59 years and not previouslydiagnosed with cervical cancer. Thecohort was followed up to the end of1982, and the observed incidence andmortality were compared with those ofwomen in five neighbouring counties
172
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 172

which did not offer organized screening.During the period 1959–82, 267 newcases of invasive cervical cancer wereobserved in the Østfold cohort com-pared with 341.5 expected cases (SIR =0.78), and 103 deaths from cervical cancer were observed and 124expected (SMR = 0.83) (Magnus et al.,1987). Women not participating in thescreening programme had a 61% higherincidence of cervical cancer than thatobserved in the reference populationand a more than two-fold excess in themortality rate. Women with any negativetest in the programme had an incidenceof cervical cancer of 48% and those withfive negative tests 18%, compared withthe incidence expected from the coun-ties without organized screening. [Theefficacy estimate of SIR corrected forselective attendance was 0.77.]
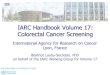
The quantitative results from thecohort studies are illustrated in Figure 50.Four of the cohort studies (in Canada,Denmark, Finland and Norway) allow anestimate of efficacy with presumably onlysmall bias. The results show large varia-tion in effect, with RRs from 0.17 in theBritish Columbia study to 0.77 in the
Østfold county study.Only part of the vari-ation can be accounted for by bias or ran-dom variation; most of it is likely to betrue.The screening programmes have aneffect that varies from close to eradicationof invasive disease to a marginal one,which further emphasizes the need fororganization and quality assurance, asoutlined in other chapters of this volume.
Case–control studiesCase–control studies do not measurethe impact of screening in relation tothe situation that would be expected inthe absence of screening in the popu-lation subjected to the screening pro-gramme. Instead they compare therisks among the screened to thatamong non-screened or never-screened groups. As the absolute risksremain unknown, it is not possible toadjust for selective attendance.Despite the inherent biases in theirdesign, resulting in overestimation ofefficacy, case–control studies, likecohort studies, have been crucial in theassessment of the efficacy of screen-ing. In 1986, the conclusions of theIARC Working Group on CervicalCancer Screening were based on a
review of studies performed in a num-ber of countries with widely differentapproaches (Hakama et al., 1986).Among these, the results of fivecase–control studies were analysed;two (Macgregor et al., 1985; Geirssonet al., 1986) were nested case–controlstudies within organized programmes(in Aberdeen, Scotland, and in Iceland)and three (Clarke & Anderson, 1979;Berrino et al., 1986; Raymond et al.,1984) in areas where screening was notcentrally organized (Toronto, Canada;Milan, Italy; Geneva, Switzerland).
The studies in Iceland and Aber-deen were designed to determine thereduction in risk of invasive cervicalcancer among women with a previousnegative test, in terms of time elapsedsince the smear was taken (Macgregoret al., 1985; Geirsson et al., 1986). Acombined analysis of the two studiesshowed a relative protection (RP) ofmore than ten-fold (RP = 11.1; 95% CI2.4–52.2) for women with their lastnegative test performed 0–11 monthsbefore the diagnosis of the case, com-pared with women who had had theirlast negative test ten or more yearsbefore (Moss, 1986). The other threecase–control studies were designed toevaluate the effects of cytologicalscreening for invasive cervical cancer.They differed in the criteria used forcase and control selection and in thedefinition of screening history, but theodds ratios (OR) observed for ever ver-sus never screened were similar, rang-ing from 0.26 to 0.37. Furthermore, theeffects were similar to those observedin the other studies when time elapsedsince the last screening and number ofprevious tests were taken into account.
Since the publication of the IARCmonograph (Hakama et al., 1986) onthe efficacy of cytological screening,several case–control studies havebeen carried out to evaluate screeningprogrammes and activities. Fourteenstudies published between 1986 and1998 were reviewed by Zappa and
173
Efficacy of screening
Figure 50 Forest plot of risk ratio estimates of incidence in cohort studies withinvitational screening
Study
Fidler et al. (1968)
Hakama & Räsänen-Virtanen (1976)
Magnus et al. (1987)
Sparén (1996)
Vikki et al. (1999)
Lynge (2000)
Relative risk(95%)
0.16 (0.09, 0.29)
0.22 (0.18, 0.27)
0.62 (0.52, 0.75)
0.55 (0.51, 0.61)
0.50 (0.40, 0.70)
0.53 (0.42, 0.67)
Relative risk
163-200 ( VOIR IMAGES) 27/01/05 16:10 Page 173

Ciatto (2000): three of these had beencarried out in North America, two inCentral America, four in Asia and five inEurope. Since then, another fourcase–control studies have reportedeffects of cytological screening byscreening status (screened versusnon-screened), in Mexico (Jiménez-Pérez & Thomas, 1999), Finland(Nieminen et al., 1999), Sweden(Andersson-Ellström et al., 2000) andSouth Africa (Hoffman et al., 2003).Table 60 summarizes the main charac-teristics and findings of these studies.
About half of the studies were carriedout within organized programmes orwith active invitation of women.Exposure was usually defined by thescreening (attendance) status, not byscreening invitation. It is also possiblethat there had been some screeningactivity among the ‘non-screened’groups, diluting the exposure contrastand affecting the rates. This might alsohave been the case in studies usingsmear archives and registers. In allstudies, cervical cancer incidence wasused as the outcome. Two studies alsoconsidered cervical cancer mortality inseparate analyses. Many studies lim-ited cervical cancers to the squamoussubtype, whereas two studies madeseparate analyses for squamous andadenocarcinomas (Herrero et al., 1992;Sato et al., 1997), while in others thehistological type of cervical cancer wasnot specified. In certain studies, atten-tion was paid to the stage of cervicalcancer and/or only advanced stageswere considered (van der Graaf et al.,1988; Zhang et al., 1989) or separateanalyses were carried out for differentgrades of invasion (Herrero et al.,1992). About half of the studies werepopulation-based and the others werehospital-based. In some studies, con-trols were selected from subjects with anegative test at the date of diagnosis ofmatched case (Macgregor et al., 1994);in another (Sobue et al., 1990), thecontrols for screen-detected cases
were selected among subjects with anegative test in the same year as thediagnosis of the respective case.Two ofthe studies were nested within cohortsof women invited to be screened(Zhang et al., 1989; Sato et al., 1997).
The proportion of controls 'everscreened' may give an idea of the cov-erage of cytological testing in the gen-eral population, although in most stud-ies controls were matched to cases forseveral co-variables, so that the actualcoverage cannot be directly estimated.Proportions tested differ substantiallyfrom one study to another. The propor-tion of ever-screened controls rangedfrom 20% in Osaka and 37% inBangkok to 88% in Miyagi and 93% inMaryland. Most studies tried to identifyand exclude tests performed becauseof symptoms by excluding those per-formed within 6 or 12 months beforethe index date.
In spite of the differences men-tioned in relation to eligibility criteria forcases and/or controls, methods of col-lection of screening history and adjust-ment for confounding variables, theresults from the review by Zappa andCiatto were quite similar, ORs rangingfrom 0.27 in the Danish study to 0.43 inthe Canadian study. Some results falloutside this range, with lower risks inthe studies in Miyagi, Japan and Jingan,China (OR = 0.16) and a higher riskobserved in Mexico City (OR = 0.76). Inthe latter study, the OR fell to 0.38 (95%CI 0.28–0.52) when only tests per-formed in the absence of gynaecologi-cal symptoms were considered.
Two fairly recent studies showsmaller impact of screening, with ORsin the range 0.5–0.8 (Nieminen et al.,1999 for opportunistic screening;Andersson-Ellström et al., 2000). In theFinnish study (Nieminen et al., 1999),there was a clear difference betweenself-reported screening in the organized programme and that inopportunistic screening. The OR ofcervical cancer was 0.25 (95% CI
0.13–0.48; all ages included) amongthose who participated in the orga-nized screening only (but who were notscreened in the spontaneous screen-ing modality) in comparison with thenon-screened; the corresponding ORwas 0.57 (95% CI 0.30–1.06) for thosewho had at least one test in the spon-taneous modality only (and did not par-ticipate in the organized programme).Most women had had tests in bothscreening modalities (OR = 0.27; 95%CI 0.15–0.49). The OR for women inboth screening modalities (organizedand spontaneous) versus those withspontaneous screening alone was 0.47(95% CI 0.29–0.75). This difference ineffect was obtained with less resourcesin the organized screening (seeChapter 3).
In the Swedish study (Andersson-Ellström et al., 2000), the effect ofscreening was estimated in compari-son with women who had not beentested during the last six years beforethe index date. Some of these mighthave been tested earlier, diminishingthe screening contrast. There was alarge proportion of cases, comparedwith controls, in whom carcinoma insitu or another (milder) lesion hadbeen previously treated (see Table 60).In only 18 cases (16%) had all the pre-vious tests been negative (the corre-sponding figure for controls was notgiven). [These findings suggest thatinadequacies in the management oftreatment may have, at least partly,accounted for the rather modest effectof screening; or that a fraction of thecase women had been tested in thecourse of management follow-up activity.]
Figure 51 presents a summary ofresults from the case–control studieson incidence included in Table 60. Forthe study by Hernandez-Avila et al.(1998), the results excluding tests per-formed on account of symptoms wereconsidered most relevant for the purpose of estimating efficacy in this
174
IIARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
163-200 ( VOIR IMAGES) 27/01/05 16:11 Page 174

diagram. From the study by Nieminenet al. (1999), only the results on orga-nized screening were included. Thestudy by Andersson-Ellstrom et al.(2000) was not included, as sympto-matic women may have been included.There was a strong indication of het-erogeneity in the results over all stud-ies reported in the table, reflecting themany differences in studies mentionedabove, whereas in the results selectedfor Figure 51, the heterogeneity is verymuch less (p = 0.288, calculated afterDer Simonian & Laird, 1986). Therewas indication of publication bias, how-ever (p = 0.023, calculated after Begg& Mazumdar, 1994). Most studiesreported large decreases in the cervi-cal cancer risk attributable to screen-ing, although because of the limitationsof and selection in the individual stud-ies, one needs to be cautious wheninterpreting the pooled point estimate(0.34) of the impact from thecase–control studies. A crude attemptto adjust for bias can be made byassuming that selection was the mostimportant source of bias and that itwas relatively constant over the stud-ies. The relatively high homogeneityover the case–control studies in theestimated ORs is another justificationfor such asn assumption. The ORs inthe cohort studies in risk between non-responders and controls (not non-responders) was about 1.5, which indi-cates that the non-responders mayhave an inherent risk up to two timesthat among responders. Such anadjustment would imply a true protec-tive effect in the populations subjectedto case–control studies of screeningof about 0.7. If the estimates of ORs inthe case–control studies were 0.6 orlarger, there is a possibility that theprogramme was practically withouteffect.
When death from cervical cancer istaken as the end-point, the protectiveeffect of screening tends to be slightlyhigher than estimated from the inci-
dence studies. In the Scottish study(Macgregor et al., 1994), the OR formortality was 0.25 (95% CI 0.11–0.48)and for incidence 0.35 (95% CI0.25–0.50), while in the Osaka study(Sobue et al., 1990) the correspondingfigures were 0.22 (95% CI 0.03–1.95)and 0.41 (95% CI 0.13–1.29). Most ofthe studies did not report impact onmortality.
Cervical cancer incidence afterscreening negativeThe IARC joint study on the incidenceof invasive cervical cancer by numberof previous negative tests (Day, 1986;IARC, 1986) was based on data fromten centres worldwide from which indi-vidual screening histories were avail-able and could be linked to cancer reg-istry data. Five were cohort studies,two nested case–control studies andthree population-based case–controlstudies. The cohort studies were thoselisted above from British Columbia(van Oortmarssen & Habbema, 1986),Manitoba (Choi & Nelson, 1986),Sweden (Petterson et al., 1986),Norway (Magnus & Langmark, 1986)and Denmark (Lynge & Poll, 1986a, b).The nested case–control studies(Macgregor et al., 1985; Geirsson etal., 1986) were carried out within orga-nized screening programmes inAberdeen and Iceland. The population-based case–control studies (Clarke &Anderson, 1979; Berrino et al., 1986;Raymond et al., 1984) were from areaswhere screening was not centrallyorganized (in Toronto, Milan andGeneva, respectively). In the case–control studies and in one of the cohortstudies (British Columbia), the refer-ence population was the potentiallyselected group of unscreened women;in the other cohort studies, theexpected incidence in the absence ofscreening was derived from corre-sponding population incidence rates ina period before mass screening wasstarted. A negative result was defined
in the IARC study as either aPapanicolaou group I result or one ortwo suspicious (group II) results fol-lowed by a group I result. The relativerisk of squamous-cell carcinoma of thecervix among women aged 35–64years, whose second negative testoccurred at age 35, by time since theindex negative smear is given in Table61. The risk estimates were 0.07 (95%CI 0.04–0.10) during the first year (12months), 0.08 (95% CI 0.05–0.13) dur-ing the second year, 0.13 (95% CI0.08–0.19) during the third year and0.36 (95% CI 0.25–0.53) during thefifth year since screening negative.These risks were used to calculate thecumulative percentage reduction inrisk of squamous-cell carcinoma of thecervix assuming different screeningintervals (see below).
One recent cohort follow-up study(Van den Akker-van Marle et al.,2003a) and two case–control studies(Miller et al., 2003; Sasieni et al., 2003)have also reported cervical cancerincidence rates after negative screen-ing results. These studies collecteddata on screening history from archivesources and followed cervical cancerincidence since time from the indexnegative smear.
Van den Akker-van Marle et al.(2003a) followed invasive cervical can-cer incidence among women whotested negative in the Dutch screeningprogramme during 1975–97. Data onscreening were derived from a nationalpathological archive, and informationon cervical cancers was obtained fromthe same source for the period1994–97. Incidence rates were calcu-lated for women aged 35–64 yearswith one and with two previous nega-tive tests. A negative screen wasdefined as an episode consisting of acytological or histological examinationwith a negative result, or a cytologicalexamination with a positive result butwithout histological confirmation ofinvasive cervical cancer or a precursor.
175
Efficacy of screening
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 175

176
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
Table 60. Main characteristics and results of case–control studies on cervical cancer screening published after1986 (modified and updated from Zappa & Ciatto, 2000)
Country (reference)
Bangkok, Thailand(Wangsuphachartet al., 1987)
Denmark (Olesen,1988)
Nijmegen,Netherlands (vander Graaf et al.,1988)
Maryland, USA(Celentano et al.,1988)
Washington, USA(Shy et al., 1989)
Jingan, China(Zhang et al.,1989)
Osaka, Japan(Sobue et al.,1990)
Osaka, Japan(Sobue et al.,1990)
Florence, Italy(Palli et al., 1990)
Bogota, MexicoCity, Panama,Costa Rica (Herrero et al.,1992)
Screeningmodality
Not invita-tional
Invitational
Invitational
Not invita-tional
Not invita-tional
Invitational
Invitational
Invitational
Invitational
Not invita-tional
Proportionsof cases/controls everscreened (%)
30/37
45/67
47/68
72/93
85/93
Not available
25/39 (within10 years)
7/20 (within10 years)
19/48
50/72
OR ever vsneverscreened
0.39(screenedevery 2–5 y vsnever)
0.27
0.22
0.29(screenedwithin 3 y vsnever)
0.21
0.16 (smearsperformedwithin last 2 yvs smears per-formed 6 ormore y earlier)
0.41(screenedwithin 10 y vsnot screenedwithin 10 y)
0.22(screenedwithin 10 y vs.not screenedwithin 10 y)
0.29
0.40
95% CI
0.21–0.74
0.18–0.42
0.1–0.81
0.15–0.58
0.09–0.50
0.05–0.58
0.13–1.29
0.03–1.95
0.15–0.55
0.31–0.48
Data source forscreening information.Notes
Questionnaire
Questionnaire to generalpractitioners
Questionnaire
Interview
Telephone interview.Smearscollected in the follow-upof an abnormal test or atthe cancer diagnosiswere excluded. OR esti-mate a re-calculation byZappa & Ciatto (2000).
Archive
Archive. Only negativetests included.
Archive. Includes diag-nostic smears
Archive
Interview
Outcome, period of obser-vation, number and sourceof cases and controls
Incidence (all histologicaltypes, ages 15–54 y),1979–83, 189/1023, hospitalrecords
Incidence (all histologicaltypes, mean age 52.6 y),1983, 428/428, cancer registry
Incidence (FIGO >1A, age<70 y), 1979–85, 36/120,cancer registry and regis-trar's office
Incidence (age 22–84 y),1982–84, 153/153, hospitaladmission records
Incidence (FIGO >1B-occult,ages 31–75 y), 1979–83,92/178, cancer registry
Incidence (FIGO >1A, squa-mous), 1965–74, 109/545,screening archive
Incidence (ages 30–79 y),1965–87, 28/272, cancerregistry and dwelling history
Mortality (age <80 y),1965–87, 15/150, cancerregistry and dwelling history
Incidence (age <75 y),1982–85, 191/540, cancerregistry and residents list
Incidence (age <70 y),1986–87, 759/1433, cancertreatment centres, hospitaladmission list and partly fromcensus list.
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 176

177
Efficacy of screening
Table 60 (contd)
Country (reference)
Manitoba, Canada(Cohen, 1993)
South-eastScotland, (Mac-gregor et al.,1994)
South-eastScotland, (Mac-gregor et al., 1994)
UK (Sasieni et al.,1996)
Miyagi, Japan(Sato et al., 1997)
Mexico City,Mexico(Hernandez-Avilaet al., 1998)
Guadalajara, Mexi-co (Jiménez-Pérez& Thomas, 1999)
Finland (Nieminenet al., 1999)
Värmland,Sweden(Andersson-Ellström et al.,2000)
Western Cape,South Africa(Hoffman et al.,2003)
Screeningmodality
Not invita-tional
Invitational
Invitational
Invitational
Invitational
Not invita-tional
Not invita-tional
Invitational
Not invita-tional
Any smears(about 50%of the testswere afterinvitation)
Not invita-tional
Proportions ofcases/controls everscreened (%)
76/87 (within 10y)
45/73
35/73
73/85
55/88
42/51
54/82
56/72 all ages68/88 ages 30–5964/66 all ages80/80 ages 30–59
61/65 (within 6 y)
83/88 in ages20–59 (within 6 y)
50/73
OR ever vsnever screened
0.43
0.35
0.25
0.26 (tests per-formed 24–35months before,vs not screenedor screened >66months before)
0.16 (screenedwithin 5 y vs notscreened within5 y)
0.76
0.3
0.360.320.730.85
[0.83]
[0.62]
0.3
95% CI
0.32–0.57
0.25–0.50
0.11–0.48
0.14–0.47
0.09–0.28
0.59–0.98
0.2–0.4
0.25–0.530.19–0.570.49–1.070.45–1.60
0.3–0.4
Data source forscreening informa-tion. Notes
Health care files
Cytopathology data-base
Cytopathology data-base
Archive. These datawere included in thelater study (Sasieni etal., 2003)
Interview and archive
Interview. OR = 0.38(95% CI 0.28–0.52)when tests due togynaecological symp-toms were excluded.
Interview
Questionnaire
Pathology database. 16cases (14%) and 4 (4%)controls had been previ-ously treated for carcino-ma in situ of the cervix (p< 0.01); 32 cases (29%)and 6 controls (5%) hadformer atypia (p < 0.001)
Interview. OR 0.2among those with atleast 3 tests; and 0.3among those with <10 ysince the last screen
Outcome, period of obser-vation, number andsource of cases and con-trols
Incidence (ages 25–64 y),1981–84, 415/29269, cancerregistry and residents list
Incidence (squamous CC),1982–91, 282/564, screeningrecords
Mortality (squamous CC),1982–91, 108/216, screeningrecords
Incidence (age >20 y),1992, 348/677, pathologylaboratories and registry oflocal health authority
Incidence (ages 35–79 y),1984–89, 119/218, screen-ing archive
Incidence, 1990–92,397/1005, hospital admis-sions records and sampleof residents
Incidence (age <70 y),1991–94, 143/311, hospitalrecords
Incidence, 1987–94,147/1098, hospital recordsand population files
Incidence (ages 20+ y),1990–97, 112/112, patholo-gy and population files
Incidence (stage >IA),524/1540, hospital records
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 177

The incidence expected in theabsence of screening was estimatedusing incidence data from threeregions during 1965–69 (the latestperiod before the screening pro-gramme was started) covering 8% ofwomen in the whole country. In addi-tion, age-period-cohort (APC) model-ling was used to refine the expectedincidence without screening, using thesame pre-screening period incidencedata as the input. The relative risk ofinvasive cervical cancer increasedfrom 0.13 in the first year after screen-ing to 0.24 after more than six yearsfrom screening for women with oneprevious negative screening (confi-dence intervals not available). These
figures decreased to 0.12 (95% CI0.08–0.17) and 0.06 (95% CI0.03–0.10) for 0–6 and 7–12 monthssince the last negative screening and0.18 (95% CI 0.11–0.30), respectively,for more than six years among womenwith two or more previous negativescreening results. The identificationand linking method used in the pathol-ogy register was not perfect (i.e., theidentification code consisted of thesame characters for two or morewomen); this was considered to haveproduced an upward bias in the inci-dence rate after a negative test. As aconsequence, the true reduction in rel-ative risk might have been somewhatlarger than reported. On the other
hand, the analysis using APC model-ling suggested overestimation of thebackground risk.
Miller et al. (2003) analysed nega-tive cytological histories within aselected group of women having con-tinuous participation in the KaiserPermanente medical care programmein northern California, USA, for at least30 months before the diagnosis date ofthe cervical cancer cases. The cases(N = 482), diagnosed between 1983and 1995, were drawn from the files ofthe medical care programme, SEERand the California cancer registry; con-trols (N = 934) were matched for age,length of membership and race. About92% of women aged 20 years or more
178
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
Figure 51 Forest plot of results from case–control studies with invitational and non-invitational screening, including apooled odds ratio estimate (incidence) using a random effects model (Der Simonian & Laird, 1986)
Odds ratio(95%)
Odds ratio0.1
163-200 ( VOIR IMAGES) 24/01/05 14:57 Page 178

had been screened at least once and89% within the last three years. A testwas defined as negative if the cytolog-ical result did not require a change inthe follow-up interval (i.e., no referral orcontrol test was required). In addition,there was a group of 'other smears'
including those for which the resultwas missing or unrelated to invasivecancer (e.g., atypical or dysplasticendometrial cells, atrophic changes,Trichomonas infection); and a group of'abnormal' results. For 32% of thecases and 10% of the controls, no neg-
ative results were available (indicatingeither that the women had beenscreened elsewhere or had not beenscreened at all, or that they had hadpositive or other smears). In the follow-up of the last negative test (irrespectiveof the other two groups in earlierscreenings), the OR for a two-year(19–30 months) versus one-year (0–18months) follow-up interval was 1.72(95% CI 1.12–2.64) and for a three-year (31–42 months) versus one-yearfollow-up interval 2.06 (95% CI1.21–3.50). Adjustment for ever havinghad an abnormal result before theindex test and for having at least oneprevious consecutive negative resultwithin 36 months before the index testdid not essentially change the results.For the sub-sample of women with atleast two consecutive negative results,the OR was 2.15 (95% CI 1.12–4.11)for the two-year follow-up and 3.60(95% CI 1.50–8.68) for the three-yearfollow-up, as compared with the one-year follow-up. [The study did not quan-tify the overall reductions in cervicalcancer attributable to screening. TheWorking Group noted that the baselinerisk with one-year follow-up was difficultto estimate and could be subject tobias; therefore the results of this studywere not included in the table.]
A study in the United Kingdom(Sasieni et al., 2003) used screeningdata on women registered within agroup practice drawn from a computer-ized database of the screening pro-gramme; information on cervical can-cer cases was obtained from pathol-ogy laboratories. There were 1305women aged 20–69 years, diagnosedbetween 1990 and 2001 with franklyinvasive cervical cancer, and 2532age-matched controls. It was not pos-sible to identify which cancers werescreen-detected, because some 50%of the women screened in England inthe mid-1990s did not attend inresponse to an invitation to the grouppractice. In all analyses, the date of
179
Efficacy of screening
Time interval since Relative risk (95% confidence interval)screening IARC (1986) a
years (months) Ages 35–64
1 (0–11) 0.07 (0.04-0.10)2 (12–23) 0.08 (0.05-0.13)3 (24–35) 0.13 (0.08–0.19)4 (36–47) 0.19 (0.13–0.28)5 (48–59) 0.36 (0.25–0.53)6 (60–71) 0.28 (0.17–0.48)7–10 (72–119) 0.63 (0.30–1.67)
Van den Akker-van Marle et al. (2003a) b
Ages 35–64
1 (0–6) 0.12 (0.08–0.17)1 (7–12) 0.06 (0.03–0.10)1–2 0.08 (0.06–0.12)2–4 0.15 (0.11–0.19)4–6 0.20 (0.14–0.29)6–10 0.18 (0.11–0.30)
Sasieni et al. (2003)c
Ages 20–39 Ages 40–59 Ages 55–69
1 (0–18) 0.24 (0.16–0.37) 0.12 (0.08–0.18) 0.13 (0.08–0.22)2 (18–30) 0.33 (0.21–0.51) 0.14 (0.08–0.22) 0.13 (0.07–0.23)3 (30–42) 0.67 (0.43–1.04) 0.25 (0.16–0.40) 0.15 (0.08–0.26)4 (42–54) 1.06 (0.65–1.72) 0.30 (0.18–0.50) 0.18 (0.09–0.34)5 (54–66) 1.40 (0.75–2.62) 0.61 (0.34–1.09) 0.28 (0.14–0.57)6 (66–78) 1.86 (0.88–3.93) 0.72 (0.36–1.43) 0.33 (0.14–0.79)>6 (>78) 2.37 (1.16–4.85) 0.69 (0.36–1.34) 0.55 (0.27–1.10)
a Including invasive squamous-cell carcinoma of the cervix uteri, since the last negativetest at ages 35–64 years, in comparison with expectation in the absence of screening.Assuming that a woman is screened negative at age 35 and that she had at least onenegative screen previously.b Invasive cervical cancer for 35–64-year old women since two or more previous negativescreenings, in comparison with expectation without screening.c Invasive cervical cancer in various age groups since the last operationally negativesmear.
Table 61. Relative risk of invasive carcinoma of the cervix within differentfollow-up windows since screening negative, in comparison with expec-tation in the absence of screening
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 179

diagnosis for a case was used as theindex date and in each case–controlstratum only the registered tests per-formed before that date were consid-ered. An operationally negative resultwas defined as a negative one not pre-ceded by an abnormal one (borderlineor worse) within the previous 12months. Overall, 66% of the cases and80% of the controls had at least onerecorded test (with any result); the fig-ures were 48% and 71% in age group55–69; 68% and 85% in age group40–54; and 80% and 83% in age group20–39 years. Compared with thosewho never had a negative test, theORs for invasive cervical cancer variedamong women aged 55–69 years from0.13 (95% CI 0.08–0.22) in the follow-up window of one year (0–18 months)since the last negative test to 0.28(95% CI 0.14–0.57) in that of fiveyears. The corresponding ORs amongwomen aged 40–54 years were from0.12 (95% CI 0.08–0.18) to 0.61 (95%CI 0.34–1.09) and among womenaged 20–39 years from 0.24 (95% CI0.16–0.37) to 1.40 (95% CI 0.75–2.62).The higher risk estimate of womenscreened negative as compared withnon-screened among the youngestage group might be related to selectionamong those who attended regularscreening.
Age to start screeningThe incidence of carcinoma of thecervix is very low in women aged lessthan 25 years, but then begins toclimb. However, in an extension of theBritish Columbia cohort study, the inci-dence of carcinoma in situ at age20–24 was of the order of 16 per 100 000 (Miller et al., 1991b), encour-aging a national workshop in Canadato recommend that screening shouldstart at the age of 20 years (Miller etal., 1991a). Similar conclusions havebeen drawn by other North Americanadvisory committees (e.g., Saslow etal., 2002).
Other countries have taken a differ-ent view. They have noted thatalthough young women below the ageof 25 or 30 have much higher rates ofcervical abnormality than olderwomen, the rise in cervical cancer inci-dence does not take place until thenext decade.While treatments are verysuccessful and have very low rates ofcomplications, the consequences for ayoung woman can be much greaterthan for an older woman, for whompreservation of fertility is not an issue.For younger women, the risk of harmmay be greater than the risk of benefit.
In Europe, the age to start screen-ing varies widely, with women inFinland and the Netherlands invited tothe organized programmes from theage of 30 years, while some countriesstart screening at much younger ages(Miller, 2002b). Sasieni et al. (2003), onthe basis of a study principallydesigned to determine the frequencyof re-screening, found that the effec-tiveness of cytological screening wasrelatively low in young women, butrose in older women (lower part ofTable 61). This led to the decision inEngland to move from a recommendedage of 20 years for starting screeningto the age of 25 years.
For developing and some middle-income countries, in order to maximizeuse of resources, and given the infrequency of cervical cancer belowthe age of 35 years, it is generally rec-ommended to start screening at 35years and only extend screening toyounger ages when resources permit(WHO, 1986). It has been pointed outthat age is the most important risk fac-tor forcervical cancer and that screen-ing should aim to target high-riskwomen. A good guide would be to takethe age at the beginning of the rise inincidence of cervical cancer and beginscreening five years before this age.In most countries, this would be atabout 30–35 years of age (Miller et al.,2000).
Frequency of re-screeningScreening programmes seek to maxi-mize the reduction in incidence of andmortality from disease, for a given levelof resources. The optimal screeninginterval is one that provides the mostfavourable ratio between degree of dis-ease control and cost of screening.The design of a screening programmedefines two key parameters for achievingthese objectives, the target populationand the screening interval. Compliancewith these parameters is crucial in main-taining the effectiveness of the pro-gramme and in measuring its cost-effec-tiveness in order that resources can beused to increase population coverage(see Chapter 3). Significant deviationfrom the recommended screening inter-val or target population may reduce theprogramme efficiency either by usingexcessive resources, as in the case ofannual re-screening for cervical cancer,or by allowing the disease to ‘escape’ theperiod at which early intervention canlead to treatment and/or cure. Modelscan facilitate decisions on the optimalperiodicity of screening.
Determining the frequency ofscreening is helped by understandingthe natural history of the condition tobe screened for, especially the dura-tion of the asymptomatic (latent)phase. A high frequency of screeningwill result in a low number of cases perscreen and thus a low predictive value.The reason for this is that the preva-lence of asymptomatic disease will below in the population if the screeningfrequency is high. On the other hand,screening too infrequently will leavemuch of the disease uncontrolled(Cole & Morrison, 1980).
An early evaluation of cervical can-cer screening in British Columbia usinga Markov–Chain model supported aprolonged natural history of carcinomain situ (an average sojourn time of atleast nine years) and suggested thatcytologically negative women shouldbe rescreened every five years (Shun-
180
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
163-200 ( VOIR IMAGES) 27/01/05 16:14 Page 180

Zhang et al., 1982).The IARC Working Group on
Cervical Cancer Screening Pro-grammes (IARC, 1986) established aproper approach to re-screening. Thisstudy showed that there was very littleevidence to support annual screeningand largely provided the basis for inter-national recommendations for three-yearly or even less frequent screening.It underlined the importance of con-centrating screening between the agesof 35 and 64 years, with almost asmuch benefit expected from three-yearly screening as from annual re-screening (Tables 61 and 62). Thesefindings have been reinforced by astudy in the Netherlands (Van denAkker-van Marle et al., 2003a; seeTable 61).
It is important to note that thegreatest percentage reduction incumulative incidence can be obtainedonly if a high proportion of the popula-tion complies with screening. However,even in the best of circumstances,experience in highly efficient cytologyscreening programmes of many coun-tries shows that no realistic screeningschedule results in the abolition ofinvasive cervical cancer.
Part of the reason for the imperfectoutcome of screening programmes isfailure of an essential component ofthe programme, which can occur at thelevel of the woman, her physician orthe laboratory examining the cytologi-cal smears (Miller, 1995). However,another reason is likely to be the vari-ability of the natural history in differentwomen. The models are based onaverages of transition probabilities,each with a different distribution orrange of time periods during whichsome lesions progress from one stageto the next, while others regress to nor-mal, and still others remain stable forlong periods of time. Some lesionsmay progress so rapidly that they can-not be found in a curable stage evenwith annual screening, and it seems
unlikely that the majority of suchlesions would be detected by more fre-quent screening. This does not meanthere are different types of cancer ofthe cervix, as suggested many yearsago (Ashley, 1966), just that the fast-growing lesions represent one extremeof the distribution of progression(sojourn) times.
Celentano et al. (1989) conducteda case–control study of 153 cases ofinvasive cancer, 153 case-nominatedcontrols and 392 randomly selectedcontrols. The results were largely con-gruent for the two sets of controls. Therelative protection after a self-reportednegative test was significant for 2–3years from the last negative test (OR =8.28; 95% CI 3.44–19.9 for case-nom-inated controls, OR 4.62; 95%2.04–10.5 for randomly selected con-trols) and some degree of protectionwas seen for 4–6 years (OR = 4.30;95% CI 1.46–12.7; 3.63; 95% CI1.38–9.57, respectively) after adjust-ment for a variety of confounders.
Herbert et al. (1996) studied the inci-dence of cervical cancer in a region ofthe UK after the introduction of the UKcomputerized call-and-recall system.The incidence of invasive cancer wassignificantly higher in women who hadnot been screened in the previous fiveyears than in those who had (RR = 2.6;95% CI 1.6–4.3); the incidence washigher in those with an interval of 3.5–5.5
years compared to 0.5–3.5 years (RR =2.2; 95% CI 1.3–3.8). The RRs werehigher when screen-detected cancerswere excluded. The authors concludedthat a five-year interval is too long.
Viikki et al. (1999) studied the riskof cervical cancer after a negative testin the context of the five-yearly orga-nized screening programme in Finland(see above). They found that the SIRwas low initially after screening andincreased gradually until the time thenext test was due. There was an esti-mated 3% annual increase in risk ofinvasive disease.The risk did not reachthe national average within the morethan 20 years of follow-up. They alsofound that the relative risk of a preinva-sive lesion after an initial negativeresult was decreased up to the secondrescreening round at 10 years andconcluded that the five-year screeninginterval applied in Finland was appro-priate.
Goldie et al. (2001) modelled thenatural history of cervical cancer usingpublished data on transition andregression rates, and data from astudy in Cape Town, South Africa.Theyconcluded that in developing countries,if the limited resources are such as toallow three screenings in a lifetime, itmay be more cost-effective to givethese tests every five years from theage of 35 or 40 years, rather than every10 years from the age of 35, as had
181
Efficacy of screening
Screening % reduction in the Number of testsfrequency cumulative rate*
1 year 93.5 302 years 92.5 153 years 90.8 105 years 83.6 610 years 64.1 3
* Assuming a screen occurs at age 35 years, and that a previous negative screen hadbeen performedFrom IARC (1986)
Table 62. Percentage reduction in the cumulative rate of invasive cervicalcancer over the age range 35–64 years, with different frequencies ofscreening
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 181

been modelled by the IARC (1986)study, and subsequently adopted as asuggested policy for South Africa(Provincial Administration WesternCape: Department of Health, 1995).
Miller et al. (2003) conducted acase–control study of cases of invasivecancer diagnosed between 1983 and1995 within the Kaiser Permanentemedical care programme (see above).The ORs for various intervals betweenscreens, with a one-year interval as thereferent, adjusted for ever having hadan abnormal cytological finding beforethe last negative result and for havingat least one negative result within 36months before the last negative one,increased to 2.24 (95% CI 1.28–3.92)at 2 years, 3.37 (1.97–5.76) at 3–5years and 5.72 (3.48–9.41) at 5–10years, although there was a lowabsolute risk of developing invasivecervical cancer within three years of aprevious negative result. [The WorkingGroup noted that the cited odds ratioswere entirely dependent on the validityof the estimated referent risk level.]
Sawaya et al. (2003) studied theprevalence of biopsy-proven cervicalneoplasia among 938 576 women under65 years of age. The prevalence of allgrades of CIN was highest in womenaged less than 30 years and muchhigher in those with no previous nega-tive cytological result than in those withone or more. No invasive cervical can-cers were detected in those who hadhad three or more previous negativetests. Using a Markov model, and various rates of progression andregression from the literature, theyestimated that for women aged 30–64years who had had three or more consecutive negative tests, extendingthe re-screening interval from one yearto every three years would result in an average excess risk of about 3 per100 000.
Sasieni et al. (2003) conducted acase–control study in the UnitedKingdom based on the screening his-
tories of 1305 women age 20–69 withstage 1B cancer of the cervix and2532 age-matched controls from therecords of the screening programme(Table 61). The OR for occurrence ofcervical cancer increased with timefrom last negative result; it reached 1.0(no protection) at three years forwomen aged 20–39, approached 1.0at six years for women aged 40–54and was still ~0.5 at six years forwomen aged 55–69 years.The authorsestimated the proportion of cervicalcancer that would be prevented by dif-ferent schedules of re-screening.These proportions varied by age. Forwomen aged 20–39, 30% would havebeen prevented by five-yearly, 61% bythree-yearly and 76% by annualscreening. The corresponding percent-ages for women aged 40–54 were73%, 84% and 88%, and for womenaged 55–69 were 83%, 87% and 87%,respectively. On the basis of theseresults, the authors recommendedthree-yearly screening for womenaged 25–49, five-yearly screening forwomen aged 50–64 and, for womenaged 65 or over, screening only ofthose who had not been screenedsince age 50.
Age to stop screeningMany countries recommend stoppingscreening or inviting women at aroundage 60 or 65 years, for a number ofreasons. For example, older womenhave tended to be poor attenders forscreening, and good-quality smearsare difficult to obtain in women so farpast the menopause. In addition, ifthey have had regular tests with a nor-mal outcome in the past, they are con-sidered to be at low risk of developingcervical cancer. However, in view of therelatively high age-specific incidencerates of invasive cervix cancer in allcountries in older women, there is aconsensus in developed countries thatwomen over the age of 60 years whohave never been screened or have not
been screened for many years shouldbe encouraged to have at least twotests, and only if both are negativeshould they stop screening (e.g., Milleret al., 1991a; Sasieni et al., 2003).However, in developing countrieswhere resources are limited but avail-able for some screening in olderwomen, it has been recommended thatwomen who have never previouslybeen screened and are older than 60years of age should have one test only(Miller et al., 2000).
Cecchini et al. (1996) revieweddata for women aged 60–70 yearsfrom the Florence screening pro-gramme and the Tuscany CancerRegistry. Only five of 242 women withinvasive cervical cancer had had twoor more negative results between 50and 60 years of age. However, of 11 342 women aged 58–60 who had anegative test between 1980 and 1987and were followed to December 1990,only one invasive cancer was diag-nosed, compared with 13.95 expectedfrom age-specific incidence data fromthe cancer registry (OR = 0.07; 95% CI0.002–0.39). The authors recom-mended reconsideration of continuingscreening after 60–64 years of age.
In North America, it is generallyrecommended that women who havebeen actively screened and alwaysbeen negative should cease screeningat 69–70 (Miller et al., 1991a; Saslowet al., 2002). In Europe, the guidelinesrecommend 64 years as the upper agelimit for active invitation for screening(Coleman et al., 1993).
There have been suggestions thatwomen who have been active partici-pants in screening but never had acytological abnormality could stopscreening at younger ages (e.g., 55 oreven 50 years) (Cruickshank et al.,1997). Flannelly et al. (2004) analysedscreening data for women aged 50years and over who had had a satis-factory result between 1988 and 1996(N = 36 512) from five regions in
182
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 182

England and Scotland. Women withprior dyskaryosis or borderline nuclearabnormalities had RRs for a positivetest after the age of 50 of 4.39 and3.08, respectively, compared withwomen whose screening historybefore the age of 50 was negative.However, 1.8% of women with a nega-tive screen history before the age of 50had dyskaryosis detected after the ageof 50 during a median duration of fol-low-up of 33.2 months.
Four screening techniques based onvisual inspection have been assessedfor early detection of cervical neopla-sia, mostly in low-resource settings:• Unaided visual inspection (also-
known as downstaging)• Visual inspection with 3–5% acetic
acid (VIA)• Visual inspection with acetic acid
using low-level magnification (VIAM)• Visual inspection with Lugol’s
iodine (VILI)Unaided visual inspection involves
naked-eye visualization of the cervix,without application of acetic acid, toidentify abnormal tissue harbouringcervical neoplasia, particularly inva-sive cancer. Cross-sectional studies inIndia have shown low sensitivity(30–50%) for unaided visual inspectionto detect cervical cancer precursorsand it is no longer considered a suitable screening test (Sankarana-rayanan et al., 1997; Basu et al.,2002). VIAM involves the use of low-level magnification (2–4 X) in visualiz-ing acetowhite lesions after applicationof acetic acid. The test characteristicsof VIA and VIAM have been evaluatedin cross-sectional studies in India andSouth Africa (Denny et al., 2000a,2002; Sankaranarayanan et al.,2004e). The results from these studiesindicate that magnification did notimprove the test performance over and
above that of naked-eye visualization.Low-level magnification is no longerwidely used for visualization afterapplication of acetic acid.
VIAVIA involves naked-eye inspection ofthe cervix one minute after applicationof 3–5% dilute acetic acid. VIA hasbeen widely investigated for its testcharacteristics in detecting CIN 2–3lesions and invasive cancer in severalcross-sectional studies, mostly indeveloping countries (Slawson et al.,1992; Cecchini et al., 1993; Megevandet al., 1996; Londhe et al., 1997;Sankaranarayanan et al., 1998b, 1999;University of Zimbabwe/JHPIEGOCervical Cancer Project, 1999; Dennyet al., 2000a; Cronje et al., 2001;Belinson et al., 2001; Denny et al.,2002; Rodriguez-Reyes et al., 2002;Ngelangel et al., 2003; Tayyeb et al.,2003; Cronje et al., 2003;Sankaranarayanan et al., 2004a). Therelative sensitivity of VIA to detecthigh-grade precancerous lesions andinvasive cervical cancer varied from29% to 95% and the specificity variedfrom 68% to 98% in cross-sectionalstudies suffering from verification bias(Slawson et al., 1992; Cecchini et al.,1993; Megevand et al., 1996; Londheet al., 1997; Sankaranarayanan et al.,1998b, 1999; Cronje et al., 2001;Tayyeb et al., 2003) (see Chapter 2,Table 26). In cross-sectional studieswith minimal verification bias, the sen-sitivity of VIA to detect CIN 2–3 lesionsvaried from 37% to 92% and the speci-ficity from 49% to 91% (University ofZimbabwe/JHPIEGO Cervical CancerProject, 1999; Denny et al., 2000a;Belinson et al., 2001; Singh et al.,2001; Denny et al., 2002; Rodriguez-Reyes et al., 2002; Ngelangel et al.,2003; Cronje et al., 2003; Sankara-narayanan et al., 2004a) (see Chapter2, Table 26). Conventional cytologywas concurrently evaluated in most ofthe above studies and the sensitivity of
VIA was found to be similar to or higherthan that of cytology as provided in therespective study settings, but thespecificity of VIA was consistenly lowerthan that of cytology (Londhe et al.,1997; Cecchini et al., 1993;Sankaranarayanan et al., 1998b, 1999;University of Zimbabwe/JHPIEGOCervical Cancer Project, 1999; Dennyet al., 2000a; Cronje et al., 2001;Denny et al., 2002; Cronje et al., 2003;Sankaranarayanan et al., 2004f) (seeChapter 2, Table 27). HPV testing wasconcurrently evaluated in cross-sec-tional studies in India, South Africa andZimbabwe and was found to have sen-sitivity similar to that of VIA (Denny etal., 2000a; Womack et al., 2000;Sankaranarayanan et al., 2004b) butsimilar (Womack et al., 2000) or higherspecificity than VIA (Denny et al., 2000a;Sankaranarayanan et al., 2004b).
VIA is being evaluated in three ran-domized intervention trials in India, toassess the reduction in incidence of andmortality from cervical cancer as com-pared to a control group with no screen-ing (Sankaranarayanan et al., 2003a, b,2004c, d). Early results in terms of par-ticipation, detection rates of cervicalneoplasia and stage distribution of inva-sive cancers detected have beenreported from two of these studies.
The impact of a single round ofscreening with VIA provided by trainednurses on cervical cancer incidenceand mortality as compared to a controlgroup with no screening is being inves-tigated in a cluster-randomized trial inDindigul district, south India(Sankaran-arayanan et al., 2003a, 2004d).Women aged 30–59 years living in 507villages grouped into 113 clusters wererandomized to VIA screening (57 clusters, 48 225 women) by nursesand to a control group (56 clusters,30 167 women). The early results fromthe study are given in Table 63. All thescreen-positive women were investi-gated with colposcopy by nurses andmost had biopsies taken.The detection
183
Efficacy of screening
Visual inspection
163-200 ( VOIR IMAGES) 27/01/05 16:15 Page 183

rates of lesions among screenedwomen were 5.8% for CIN 1, 0.7% forCIN 2–3 and 0.2 for invasive cancer.71% of women with CIN 1 and 80% ofthose with CIN 2–3 lesions acceptedcryotherapy provided by nurses andexcisional treatment by mid-level clinicians. Overall, 97 and 34 incidentcervical cancer cases were observedin the intervention and control arms,respectively, giving age-standardizedincidence rates of 92.4 and 43.1 per100 000 person-years, respectively, dur-ing 2000–03, the screening phase ofthe study. One third of the cases in theVIA group were diagnosed in stage I,while three quarters of those in thecontrol arm were diagnosed in stageIII; no stage I cases were detected inthe control group. The study groups arebeing followed up to monitor cervicalcancer incidence and mortality.
The impact of screening by VIA,cervical cytology or HPV testing (usingthe Hybrid Capture® 2 (HC 2) probe B
assay; see Chapter 2) on cervical can-cer incidence and mortality, as com-pared to a control group, is beinginvestigated in a cluster-randomizedcontrolled trial in Osmanabad district,India (Sankaranarayanan et al., 2003a;2004c). Women aged 30–59 years living in 52 clusters of 497 villages inrural Osmanabad District, were randomized to a single round ofscreening by either VIA (13 clusters,34 149 women) or cytology (13 clus-ters, 32 136 women) or HPV testing(13 clusters, 34 515 women) or to acontrol group (13 clusters, 30 378women). The early results are given inTable 64. Participation of eligiblewomen in screening was 78.4% in theVIA group, 79.5% in the cytology groupand 78.7% in the HPV group. The test-positive rates were 14.0% for VIA, 7.0%for cytology and 10.4% for HPV testing.Test-positive women were investigatedwith colposcopy and biopsy based oncolposcopy findings. Biopsies were
taken from 9.9% of screened women inthe VIA, 3.5% in the cytology and 4.3%in the HPV groups.
Low-grade lesions were detectedin 1068 (4.0%) screened women in theVIA group, 304 (1.2%) in the cytologygroup and 327 (1.2%) in the HPVgroup. VIA had a significantly higherrate for detection of low-grade lesionsthan cytology or HPV testing (p <0.001). The detection rates of CIN 2–3were 0.7% in the VIA, 1.0% in thecytology and 0.9% in the HPV groups.The detection rates of CIN 2–3 weresignificantly different between arms (p < 0.001); after adjustment for socio-economic factors affecting detectionrates, the detection rate of CIN 2–3 inthe VIA arm was significantly lowerthan in the cytology arm (OR = 0.7, p =0.005). During 2000–03, 121 women inthe VIA group, 131 in the cytologygroup, 100 in the HPV group and 59 inthe control group were diagnosed withinvasive cancer. In the interventiongroups, 70–74% of the cancers werescreen-detected, and 48–60% werediagnosed in stage I as opposed to24% in the control group. The prelimi-nary findings from this study indicatesatisfactory participation rates forscreening, diagnosis and treatment.VIA detected significantly fewer CIN2–3 cases than did cytology. The trialparticipants are being followed up todocument cervical cancer incidenceand mortality in the four groups.
The preliminary findings from theabove trials indicate that a VIA-basedscreening programme is feasible, safeand acceptable for a population in ruralsettings, and that it results in earlydetection of cervical neoplasia. VIA isassociated with high detection of low-grade CIN. The detection rates of CIN2–3 lesions by VIA were similar in boththe trials. While the detection rate ofCIN 2–3 lesions for VIA was constantin the Dindigul trial throughout recruit-ment, it declined from 1.0% at thebeginning to 0.5% at the end of recruit-
184
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
VIA-screened group Control group
Number of women 48 225 30 167Received screening 30 577 –Screened positive 2939 (9.6%)a –Number of screen-positive women 2939who had colposcopyNumber of women who received 2777biopsyCIN 1 1778 (5.8%)b –CIN 2–3 222 (0.7%)b
Number with invasive cancer 97 34Number with stage I cancer 34 (35.0%)c 0 (0.0%)c
Number with stage II cancer 18 (18.6%)c 6 (17.6%)c
Number with stage III cancer 45 (46.4%)c 26 (76.5%)c
Number with stage IV cancer 0 (0.0%) 2 (5.9%)
a Percentage of screened womenb Indicates detection rate of CIN per 100 screened womenc Percentage of all cancers
From Sankaranarayanan et al. (2004d)
Table 63. Initial results after the screening phase of the cluster-random-ized controlled trial of visual inspection for cervical cancer with aceticacid in Dindigul district, India
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 184

ment in the Osmanabad trial; withcytology, the rate remained constant inthe latter study. A high proportion ofinvasive cancers were diagnosed instage I in women screened with VIA.The ultimate efficacy of VIA in reducingcancer incidence and mortality willbecome clearer with follow-up for cancerincidence and mortality in these studies.
An innovative option taking advan-tage of the immediate availability oftest results with VIA is the screen-and-treat or single-visit approach, to ensurehigh treatment compliance amongscreen-positive women. This approachis based on the following premises:studies have reported high sensitivityfor VIA to identify precancerouslesions; the lack of or inadequate infra-structure and resources for diagnosticfacilities such as colposcopy andhistopathology in many low-resourcesettings; the possibility of high rates ofloss to follow-up associated with multi-
ple visits; and the potential for protec-tion against cervical neoplasia amongwomen who had ablation (with electro-coagulation or cryotherapy) of theectopic cervical epithelium and thetransformation zone (Vonka et al.,1984).
In the screen-and-treat approach,screen-positive women without clinicalevidence of invasive cancer and satis-fying the criteria for ablative therapyare immediately treated by cryother-apy, without confirmatory colposcopicor histological investigations. Thesafety, acceptability and feasibility ofsuch a single-visit approach combiningVIA and cryotherapy was assessed ina recent study in rural Thailand(RTCOG/JHPIEGO, 2003). Trainednurses tested 5999 women with VIAand 798 (13.3%) women were VIA-positive. Overall, 756 women receivedcryotherapy (either immediately orpostponed). No major complications
were recorded following cryotherapy;only 33 women (4.4%) of treatedwomen returned for a perceived prob-lem. At a one-year follow-up visit, theVIA test negative rate among treatedwomen was 94.3%.
The efficacy of the screen-and-treat approach with VIA as comparedto HPV testing and treatment in reduc-ing the frequency of high-grade CIN isbeing assessed in a randomized clini-cal trial in South Africa, which has notyet published any results.
In order to assess how screen-and-treat with VIA will perform in a routinehealth service setting, a large demon-stration project to screen women aged30–49 years has been launched in theSt Martin province of Peru. This pro-gramme aims to cover 80 000 womenin three years; no results have yet beenpublished.
A greater proportion of cervical can-cers detected by VIA were in stage I than
185
Efficacy of screening
Group screened Group screened Group screened Control groupwith VIA with cytology with HPV testing
Number of women 34 149 32 136 34 515 30 378Received screening 26 755 25 535 27 159 –Screened positive 3731 (14.0%)a 1790 (7.0%)a 2812 (10.4%)a –Number of screen positive 3682 1559 2475 –who had colposcopyNumber of women who 2528 828 1114 –received biopsyLow-grade lesions 1068 (4.0%)b 304 (1.2%)b 327 (1.2%)b –CIN 2 lesions 84 (0.3%)b 103 (0.4%)b 105 (0.4%) –CIN 3 lesions 112 (0.4%)b 162 (0.6%)b 138 (0.5%)b –Number with invasive cancer 121 131 100 59Number with stage I cancer 58 (47.9%)c 67 (51.2%)c 60 (60.0%)c 14 (23.7%)c
Number with stage II cancer 18 (14.8%)c 12 (9.2%)c 9 (0.0%)c 8 (14.9%)c
Number with stage III cancer 30 (24.8%)c 29 (22.1%)c 10 (10.0%)c 30 (50.9%)c
Number with stage IV cancer 5 (4.1%)c 1 (1.0%) c 1 (1.0%)c 3 (5.6%)c
a Percentage of screened womenb Indicates detection rate of CIN per 100 screened womenc Percentage of all cancers
From Sankaranarayanan et al. (2004c)
Table 64. Initial results after the screening phase of the cluster-randomized controlled trial of visual inspectionfor cervical cancer with acetic acid, cytology and HPV DNA testing in Osmanabad district, India
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 185

among cancers occurring in unscreenedcontrols. The long-term impact of VIAscreening in reducing cervical cancerincidence remains to be established.
VILIVisual inspection with Lugol’s iodine(VILI) involves naked-eye examinationof the cervix to identify mustard-yellowiodine-non-uptake areas after applica-tion of Lugol’s iodine. The test charac-teristics of VILI provided by nurses,midwives and trained non-medicalworkers have been studied in a set often cross-sectional studies, with a similar protocol, involving 49 080women aged 25–65 years conductedin Burkina Faso, Republic of Congo,Guinea, India, Mali and Niger(Sankaranarayanan et al., 2004a). VIAwas also simultaneously evaluated inall 10 studies, conventional cytology infive and HPV testing in three studies.No untoward reaction to iodine wasobserved. VILI had a significantlyhigher pooled sensitivity than VIA(91.7% versus 76.8%) but similarspecificity (85.4% versus 85.5%) indetecting CIN 2–3 lesions. VILI hadsignificantly higher pooled sensitivitythan cytology (83.9% versus 45.4%)but lower specificity (82.5% versus99.2%) in detecting histologically confirmed CIN 2–3 lesions (Sankaran-arayanan et al., 2004f).VILI had similarsensitivity to that of HPV testing, butlower specificity, to detect histologicallyconfirmed CIN 3 lesions in the pooledanalysis of three cross-sectional stud-ies (Sankaranarayanan et al., 2004b).There are no randomized trials evaluat-ing the efficacy of VILI in reducing cer-vical cancer incidence and mortality.
Almost all of the studies on HPV test-ing have focused on the sensitivity andspecificity of the test under various
conditions. No studies have prospec-tively investigated its impact on subse-quent cancer rates, but a few have retrospectively studied the detectabilityof HPV in archival smears which werenegative on cytology some yearsbefore a diagnosis of cancer. Issues ofthe persistence of HPV in high-gradelesions and the length of protection following a negative HPV test havebeen addressed in a few studies. Acomprehensive review of the role ofHPV testing in cervical screeningappeared in 1999 (Cuzick et al.,1999b) and several important studieshave been reported since then.
Relative sensitivity for CIN 2 or3 compared with cytologyMost of the recent screening studieshave used the Hybrid Capture™ 2 testfor high-risk HPV types, which is theonly test now commercially available. Itis clear that this test is more sensitivethan cytology for CIN 2 or 3 and forCIN 3, but it also has lower specificity(Table 65). The specificity improves iftesting is restricted to women over theage of 30 years.
Typically, HPV testing has a sensi-tivity of 95% for detecting CIN 2 orworse lesions compared with 75% forcytology at the borderline (ASCUS) orabove level and 70% for cytology at themild dyskaryosis (LSIL) level (i.e.,when the cytology threshold (or cut-off)is ASCUS or worse, or when it is LSILor worse). Thus, virtually all of thelesions detected by cytology wereHPV-positive, as were an additional25% which were negative on cytology.In women over the age of 30 years,specificity is about 93%, comparedwith 95% for cytology at the borderlinelevel and 98% at the mild level. Foryounger women, both tests havepoorer specificity. For example, in theEnglish screening programme, forcytology at the borderline cut-off,specificity is about 89% in womenaged less than 30 and 96% for older
women (NHS, 2003a). For HPV, thespecificity is about 85% for womenaged less than 30 and 93% for olderwomen. Where available, the studiesshow even greater sensitivity fordetecting CIN 3 (Table 65b)
Lower sensitivities of both HPVand cytological testing are seen indeveloping countries. In the three largeEuropean studies (Clavel et al., 2001;Petry et al., 2003; Cuzick et al., 2003),the sensitivity of HPV testing was uniformly high (97% or higher),whereas the sensitivity of cytology waslower and highly variable betweencountries.
Retrospective studies of HPVevaluationEleven published studies have evalu-ated HPV infection in stored material(Table 66). Seven used archivalsmears (de Roda Husman et al., 1995;Walboomers et al., 1995; Chua &Hjerpe, 1996; Wallin et al., 1999;Carozzi et al., 2000; Ylitalo et al.,2000a; Zielinski et al., 2001a), oneused previous biopsy specimens(Konno et al., 1992) and three testedfor HPV antibodies in stored serumsamples (Chua et al., 1996; Lehtinenet al., 1996; Dillner et al., 1997).
Two of these studies (Konno et al.,1992; de Roda Husman et al., 1995)did not include controls. They looked ata total of 15 women with invasive cer-vical cancer and five with CIN 3, andexamined smears and biopsies takenup to 10 years previously. All storedspecimens tested positive for HPV16,18 or an unknown type. Chua andHjerpe (1996) analysing archivalsmears, with two matched controls percase, obtained odds ratios of 16, 11and 18 for invasive squamous, adeno-carcinoma and carcinoma in situ of thecervix based on 18, 12 and 58 cases,respectively. Walboomers et al. (1995)used as controls women from a gynae-cological clinic, some of whom werebeing treated for CIN.They used general
186
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
Human papillomavirus testing
163-200 ( VOIR IMAGES) 27/01/05 16:16 Page 186

187
Efficacy of screening
(a) for CIN2+
Reference Sensitivity Specificity CommentsCytology ≥ LSIL HPV Cytology < LSIL HPV
Clavel et al. (1999) 85 100 95 85Cuzick et al. (1999a) 79 95 99 95 Age ≥ 35 yearsSchiffman et al. (2000) 78 88 94 89 Costa RicaRatnam et al. (2000) 40 90 77 51 69% HC-I, 31% HC-IIDenny et al. (2000a) 78 73 85 76 South AfricaDenny et al. (2000b) 82 72 93 86 South AfricaSchneider et al. (2000) 20 89 99 94 PCR with GP5+/6+Womack et al. (2000) 44 81 91 62 Zimbabwe – high HIV rateClavel et al. (2001) 68 100 95 86 Conventional
88 93 LBCPetry et al. (2003) 37 98 99 95 Age ≥ 30 yearsKulasingam et al. (2002) 36 63 96 83 Age ≥ 30 yearsCuzick et al. (2003) 70 97 99 93 Age ≥ 30 yearsSankaranarayanan et al. 37–72 46–81 87–98 92–95 3 centres with variable results(2004b)Salmeron et al. (2003) 59 93 98 92 Mexico. Cut-point for cytology
was ≥ ASCUSNieminen et al. (2004) 83 98 94 78 Hospital population
(b) for CIN3+
Reference Sensitivity Specificity CommentsCytology ≥ LSIL HPV Cytology < LSIL HPV
Cuzick et al. (1999a) 79 100 99 95 Age ≥ 35 yearsFerreccio et al. (2003) 63 85 94 88 Conventional
86 88 LBCSalmeron et al. (2003) 60 94 98 90 Mexico. Cut-point for cytology
was ≥ ASCUSPetry et al. (2003) 40 97 99 95 Age ≥ 30 yearsCuzick et al. (2003) 77 98 99 93 Age ≥ 30 yearsKulasingam et al. (2002) 57 91 90 73 All agesSankaranarayanan et al. (2004b) 80 77–89 95 92–95 3 centres with variable resultsNieminen et al. (2004) 86 100 93 78 Hospital population
Table 65. Relative sensitivity and specificity of Hybrid Capture (HC) 2 compared with cytology on biopsy in cross-sectional screening studies
primers to probe archival smears and,consistent with other studies from thisgroup, found a very strong associationwith high-risk HPV types. Sixteen ofthe 17 women with invasive carcinomahad HPV in archival smears comparedwith seven of the 50 controls, giving anodds ratio of 49. Further, all nine caseswith two archival smears had the sametype of HPV detected on both. Thesmears were taken between two
months and six years before cancerdiagnosis (median 1 year). By design,all smears were originally classed asnormal. On reanalysis, four of the 26archival smears from the cases weredeemed inadequate, and the restshowed severe dyskaryosis or worse.Wallin et al. (1999) compared archivalsmears, all of which had normal cytol-ogy, from 118 women with subsequentcervical cancer with those from 118
controls. The average durationbetween smears and cancer was 5.6years (range, 0–26 years). HPV wasdetected in 30% of the cases but only3% of the controls (OR = 16.4; 95% CI4.4–75). The PCR in this study usedboth MY09/MY11 and GP5/6 consen-sus primers.
Ylitalo et al. (2000a) reviewed allprevious smears in 484 cases of carci-noma in situ and 619 matched controls
163-200 ( VOIR IMAGES) 27/01/05 16:19 Page 187

in Uppsala, Sweden. Smears wereavailable for up to 26 years beforediagnosis. Only HPV16 was tested for.The case smears from 16–18 yearsbefore diagnosis were HPV-positive forabout 10% of women, which was simi-lar to controls, but the proportion roselinearly to 56% 2.3 years before diag-nosis, which was highly significant. Apositive HPV16 result on the two lastsmears before diagnosis was associ-ated with an odds ratio of 31.2 (95% CI10.6–91.8) for carcinoma in situ. Themean time from HPV positivity to diag-nosis was estimated to be between 7and 12 years.
Carozzi et al. (2000) assessedarchival smears classified as normalfrom 79 cases of CIN 2 or worse andmatched controls. They used a con-sensus system which detected HPVtypes 16, 18, 31, 33, 52 and 58. Anodds ratio of 64 (95% CI 31–133) forCIN 2 or worse was found for HPV-positivity in all smears, which rose to103 (95% CI 43–251) in smears takenless than four years before the lastcytological test; overall 77% of casesmears were HPV-positive comparedwith 5.1% of control smears.
Zielinski et al. (2001a) examinedthe last normal archival smear from 57women who later developed cancerand 114 control women, usingGP5+/6+ primers. HPV was detectedin 65% (37) of the smears from casescompared with 6% (7) of the controlsmears (OR = 28; 95% CI 11–72).Positivity was only slightly higher insmears taken within three years ofdiagnosis (76%) than in smears taken4–20 years previously (65%).
Three studies (Chua et al., 1996;Lehtinen et al., 1996; Dillner et al.,1997) looked for HPV16 (or HPV16and 18) antibodies in stored serumsamples, using a nested case–controldesign. All three found increased riskof cancer or carcinoma in situ inwomen with prior seropositivity toHPV16. The odds ratios associated
with HPV antibodies in these studiesranged from 3 to 13. A longer lag timefrom sampling of sera to diagnosis wasassociated with greater relative risk.Chua et al. (1996) estimated the pro-gression rates to cancer or carcinomain situ in women of different ages withand without HPV16 antibodies. Theincidence of cancer or carcinoma insitu decreased with age, as did the rel-ative risk associated with HPV16 anti-bodies, whereas seropositivityincreased with age in the controls. Apossible explanation of this finding isthat CIN is associated with an activeHPV infection and women who devel-oped antibodies some years earlier nolonger necessarily carry the virus. Thestudy also looked at antibodies forHPV18 and 33, but these were not significantly associated with disease.The largest of the studies (Dillner etal., 1997) combined cohorts fromFinland, Norway and Sweden andincluded 182 cases of invasive carci-noma. Overall, the relative risks were2.7 for HPV16 antibodies and 2.2 forHPV16, 18 or 33 antibodies. The rela-tive risk associated with HPV16 anti-bodies increased to 3.9 in thosewomen with a lag time of over fiveyears. The third study measuring anti-bodies (Lehtinen et al., 1996) included27 cases of invasive cancer and 25 ofcarcinoma in situ. Overall, the oddsratio for risk of developing cervical car-cinoma according to the presence ofHPV antibodies was 13.2. It was greaterfor invasive cancer (OR = infinite; 95%CI 2.0–infinite) than for carcinoma insitu (OR = 6.0; 95% CI 1.2–29.7) and forlag times of over five years (OR = 18;95% CI 2.3–142) compared with underfive years (OR = 8.6; 95% CI 1.0–75).[Due to the lack of sensitivity of serological tests (50% at best for somehigh-risk HPV types), odds ratios fromthese studies are inevitably much lowerthan for direct DNA testing in cervicalspecimens.]
Duration of protectionThe higher relative sensitivity of HPVtesting for CIN 2 or 3 compared withcytology suggests that it might be safeto lengthen screening intervals if HPVtesting were used. Two studies of thisissue have been reported (Bory et al.,2002; Sherman et al., 2003a) and others are in progress. Bory et al.(2002) found that among 2432 womenwho were negative for high-risk HPV,only two (0.08%) developed high-grade CIN after a median follow-up of27 months. Both cases were HPV-pos-itive at the time of diagnosis (after 18and 24 months). This was comparedwith 21.2% developing CIN 2 or 3among women who were initially HPV-positive but cytologically normal.
Sherman et al. (2003a) reported a 10-year follow-up of 20 810 womenscreened by cytology and HPV DNAtesting at Kaiser Permanente inPortland, Oregon. Cervical lavagespecimens were used for HPV testing.A total of 171 women were diagnosedwith CIN 3 or cancer on follow-up. HPVpositivity was more sensitive fordetecting CIN 3 on follow-up thancytology (89 versus 58 in the first 45months and 110 cases versus 59cases overall). Conversely, there werefewer cases in HPV-negative women(29 versus 60 in the first 45 monthsand 61 versus 112 overall). Detectionrates were similar between tests in thefirst nine months (15 cases in HPV-positive women, 15 cases in HPV-neg-ative women) but HPV negativity wasmuch more protective than cytologyafter that (14 versus 45 cases inmonths 10–45; 46 versus 97 in months10–112).
In addition, modelling studies havesuggested that the use of HPV testingcould safely allow the screening inter-val to be lengthened. Goldie et al.(2004) modelled the US data and recommended that women whoseresults are negative by both HPV DNAtesting and cytology should not be
188
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 188

189
Efficacy of screening
Reference Assay Follow-up Setting Age Case Control Material(years)
Konno et al. In situ hybridi- < 10 y Japan CIN 3 (5) Hysterectomy(1992) zation Microinvasive (2) sections
PCR of Invasive carcinoma negatives (1)
All with HPV16/18on hysterectomy section
HPV 16 found in all previous biopsy specimens
De Roda General primer 2–9 y; Netherlands Cervical cancer (12) None Archival Husman et al. PCR mean, Screening smears(1995) 5.8 y programme
HPV found in archival smears of all 12 cases. Same type found in smear and biopsy of tumour.
Walboomers GP5/6 2 mo–6 y; Netherlands 17 cancers with 50 controls from Archival et al. (1995) median, 1 y 3-yearly screening normal archival gynaecology clinic smears
programme smears including women with CIN
Archival HPVhr Total
+ - Women SmearsCase 16 1 17 26 Odds ratio,Control 17 43 50 88 49
All nine cases with two archival smears had the same viral type on bothOn rescreening 26 archival smears from the cases, four were inadequate and the rest (22) were all severe dyskaryosis or worse
Chua & PCR (nested): 2–7 y Sweden 17–68 Adenocarcinoma (12) No carcinoma in situ for 5 y ArchivalHjerpe (1996) (i) MY09/11 mean 3 y Squamous-cell (18) post-smear (but some history smears
(ii) GP5+/6+ Carcinoma in situ (58)of abnormaly) (age matched)
Case ControlNo. HPV + No. HPV+
(%) (%)Carcinoma in situ 58 71 58 12Invasive squamous- 18 67 18 11cellAdenocarcinoma 12 58 12 8
Chua et al. Serology L1 < 6.5 y; Sweden 27–61 CIN 2/3 (41) Population-based Sera(1996) and L2 capsids mean CIN 1 (10) Match on age, date of blood
for HPV16 anti- 3 y CIN not otherwise Probability of CIN within 3bodies specified (23) months given HPV seropositivity
No. Seropositive (%) Age (years) + –CIN 2–3 41 37 25–34 0.034 0.005CIN 1 10 20 35–44 0.016 0.006CIN not 23 43 45–64 0.002 0.002otherwisespecifiedControls 148 16
Table 66. Studies retrospectively analysing stored samples for HPV DNA or antibodies
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 189

190
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
Reference Assay Follow-up Setting Age Case Control Material(years)
Lehitinen HPV16 L1 and 0.7–22.8 y; Finland Mean, 27 invasive carci- 143 individually matched Stored seraet al. (1996) L2 capsid mean, 10 y 18 814 39 at nomas
antibodies women baseline, 25 carcinomas inflagged to 49 at situcancer diagnosisregistry
Dillner et al. L1 and L2 14% under Finland < 40 182 invasive ~ 3 matched controls per case Stored sera(1997) capsids to 1 y; 33% Norway (45%) carcinomas (total, 538)
HPV16, 18 over 5 y and > 45and 33 anti- Sweden (26%) No. HPV 16+ HPV 16, 18, 33+bodies population- Case 182 16% 37%
based Control 538 7% 19%serum Relative risk 2.7 2.2
For HPV16, relative risk increased with increasing lag time: 3.9 (95% CI 1.6–9.6) over 5 years
Wallin et al. MY09/11 and 0–26 y, Sweden 19–74, Cancers with prior 118 Archival(1999) GP5/6 median, mean negative smears smears
5.6 y 44 (118) (and biopsies)
HPV + HPV–Case 35 83Control 3 115
OR 16.4 (95% CI 4.4–75)
Ylitalo et al. PCR 0.26 y; Sweden 20–70 484 CIS (2228 619 matched controls Archival(2000a) HPV 16 median, 8 y median; smears) (1806 smears) smears
35 HPV+ HPV–Case 130 353Control 36 581
First smear: OR13 y prior, 3.6 (95% CI 1.2–11)1 y prior, 11.1 (95% CI 5.5–22.2)Last 2 smears postive:OR 31.2 (95% CI 10.6–91.8)Average time to CIS, 7–12 years
Carozzi et al. PCR (consensus0–6 y; Florence, 25–64 92 total smears 3 controls per case; total number Archival(2000) primers HR mean, Italy 15 CIN 2 of control smears, 332 smears
HPV) 2.5 y 59 CIN 3 All smears cytologically negative5 invasive
HPV+ HPV–Case 71 21Control 17 315
OR 64 (95% CI 31–133)For slides with latency < 4 years:OR 103 (95% CI 43–251)
Zielinski et GP5+/6+ 0–18 y Netherlands 57 cancers with 114 age matched controls Archivalal. (2001a) PCR 3-yearly normal smear smears
screening HPV+ HPV– Totalprogramme Case 37 20 57
Control 7 107 114OR 28 (95% CI 11–72)
CIS, carcinoma in situ; HR, high-risk; OR, odds ratio. Modifed and updated from Cuzick et al. (1999a)
Table 66 (contd)
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 190

re-screened before three years.Women with normal cytologicalresults, but who are positive for high-risk HPV DNA, are at relatively low riskof having high-grade cervical neopla-sia, and colposcopy should not be per-formed routinely in this setting.Instead, HPV DNA testing along withcervical cytology should be repeated inthese women after 6–12 months. If testresults of either are abnormal, col-poscopy should then be performed. Asa result of these recommendations, theAmerican Cancer Society and theAmerican College of Obstetricians andGynecol-ogists have approved theextension of screening intervals fromannually to three-yearly in women agedover 30 years, when HPV is added tocytology. [The Working Group notedthat modelling results are no substitutefor direct evaluation of this question.]
Cuzick et al. (2003) showed thatwomen who originally had negative orborderline cytology but were subse-quently found to have CIN 2 or worselesions remained HPV-positive. [TheWorking Group noted the importanceof persistence in determining the likeli-hood of underlying high-grade dis-ease, but that currently this could onlybe assessed by two tests less thanone year apart.]
Liquid-based cytology systemsIntroductionSeveral literature reviews and meta-analyses have been published com-paring the relative sensitivity andspecificity of liquid-based cytology sys-tems with those of conventional cervi-cal testing (see Chapter 2).
The comprehensive systematicreview and meta-analysis by Arbyn etal. (2004a) includes split-sample andmore recent direct-to-vial studies. Theauthors noted that early studies oftenyielded favourable results for LBC
when comparing test positivity rates forlow-grade abnormalities on cytologyonly, whereas in studies using detec-tion rates for biopsy-confirmed CIN 2or 3, no significant differences betweenconventional and liquid-based cytologywere found.
This meta-analysis showed thattest positivity was higher in direct-to-vial studies than in traditional testing,suggesting a bias in previous split-sample studies to the disadvantage ofLBC. In direct-to-vial studies, moreLSIL and HSIL lesions were identifiedin both ThinPrep and SurePath LBCsystems (Table 67) (Arbyn et al.,2004a). Identification of equivocalsamples (ASCUS) was similar. Theauthors were concerned thatincreased identification of cytologicalabnormalities (ratios >1) alone pro-vides insufficient evidence forimproved sensitivity of LBC in ascreening programme and that verifi-cation with a valid gold standard isneeded. Figures 52 and 53 show thetest positivity ratios from studies avail-able to the Working Group.
Only a few studies verified allcases (test positives and negatives)with a gold standard, allowing evalua-tion of sensitivity and specificy of bothLBC and conventional cytology withoutverification bias (see Table 68). Allthese studies used the split sampledesign and none showed a statisticallysignificant difference. In fact, the rela-tive sensitivity was somewhat lower forLBC than for conventional testing.
Consideration of the positive pre-dictive value (PPV) would allow deter-mination of whether higher cytologicalpositivity rates with LBC are due to anincrease in false-positive tests. As pos-itive predictive values for presence ofCIN 2+ pooled from studies with atleast an 80% gold standard verificationof test-positives by colposcopicallydirected biopsy did not significantly dif-fer from that of conventional cytology,this was probably true.
Evidence of efficacy from LBC in rou-tine cervical screening programmesExperience with LBC as the routinetest in screening programmes is rela-tively recent and there is no long-termfollow-up in terms of effects on inci-dence and mortality in the populationsserved. Thus the evaluation of efficacyhas been made in terms of short-termsurrogate markers such as relative sen-sitivity and specificity of LBC compared with those of high-qualityconventional cytology. Short-term evalu-ations of LBC as the routine test in cer-vical screening in England, Scotlandand Canada are described below.
A systematic review of the litera-ture and modelling of cost-effective-ness, commissioned in the UnitedKingdom by the National Institute forClinical Excellence (NICE) (Payne etal., 2000), concluded that, despite thelack of published studies providingdirect evidence regarding cost-effec-tiveness of LBC for cervical screening,it was likely that LBC would reduce thenumber of inadequate samples,reduce the number of false negativeresults and decrease the time requiredfor examination of specimens by cytol-ogists. NICE immediately commis-sioned a full cost-effectiveness trial ofLBC in a low-prevalence population forroutine screening. LBC was introduced,after a learning transition period of 3 to6 months in three selected laboratories,as part of a 12-month pilot project aim-ing at 100 000 routine screening tests.In two laboratories, the ThinPrep sys-tem was introduced and SurePath inanother. The cytological results of thefirst six months of the pilot period werecompared with the four previous yearswhere exclusively conventional cytol-ogy was used (Moss et al., 2003). Itwas noted that different samplingdevices were used before (woodenAylebury spatula) and after (Cervexbroom) the introduction of LBC, butthere is published evidence that thereis no statistical difference in sensitivity
191
Efficacy of screening
Other screening methods
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 191

192
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
ThinPrep SurePath
Test threshold Pooled estimate 95% CI No. of studies Pooled estimate 95% CI No. of studies
HSIL+ 1.72 1.42–2.08 21 1.47 1.14–1.89 7
LSIL+ 1.74 1.47–2.06 21 1.52 1.24–1.86 7
LSIL 1.80 1.52–2.12 21 1.54 1.25–1.90 7
ASC+ 1.23 1.07–1.40 19 1.19 0.96–1.46 7
ASC 0.95 0.84–1.09 19 0.93 0.67–1.31 7
From Arbyn et al. (2004a)
Table 67. Meta-analysis: pooled ratios of test positivity rates for liquid-based cytology (direct-to-vial studies) ver-sus conventional testing
Figure 52 Ratios of test positivity for HSIL+ in direct-to-vial studies with ThinPrep LBC, compared with conventionalPap cytology< > indicates the combined effect estimated by random-effects model
between these two devices (Buntinx &Brouwers, 1996).
The proportions of inadequate testsbefore and after conversion to LBC areshown in Table 69. The evaluationshowed an 80% reduction in the rate of
inadequate samples in all laboratoriesand in all age groups after introductionof LBC. The rate was lowest in theSurePath laboratory.The quality of con-ventional smears increased with age,but no age differential was observed
with LBC. The inadequate rate inEnglish laboratories is higher than inmany other countries (average 9%).
The relative changes in the identifi-cation of cytological abnormalities withLBC versus conventional testing by
163-200 ( VOIR IMAGES) 24/01/05 14:58 Page 192

age group and by laboratory areshown in Table 70. There was no sig-nificant increase in the rates of HSILwhen averaged across the three sites.However, in the ThinPrep laboratories,significantly more SIL and HSILlesions were found, and one of them(lab C) also found more borderlinelesions. In the laboratory whereSurePath was used, less HSIL andborderline lesions were detected. Thereason for this difference is not known.The increased identification of LSIL orworse lesions by SurePath was concentrated in the 20–34-year agegroup.
The reduction in inadequate rateshould lead to fewer tests being per-formed, with a resulting decrease inworkload for laboratories and primarycare as well as recall systems.
Referrals to colposcopy are likely to beaffected only if the overall reporting ofhigh-grade lesions increases. Com-paring the running costs of LBC withthose of conventional testing was com-plex since they utilize differentamounts of laboratory resources.
There was some debate in theUnited Kingdom on the extent to whichpublished differences between LBCand conventional cytology representeda true improvement (Herbert &Johnson, 2001, Moseley & Paget,2002); a more recent article (Coste etal., 2003) contradicted the NationalHealth Service pilot findings.
In another LBC pilot study, con-ducted by the Scottish CervicalScreening Programme (SCSP, 2002),four regional groups of smear-takerswere randomized into two groups, col-
lecting respectively conventional cervi-cal smears and ThinPrep preparationsfrom women attending for routine orfollow-up screening tests. ThinPrepalone was chosen as the LBC systemstudies, since Cytyc had a more estab-lished infrastructure to support the laboratories at the time and the num-bers in the study (30 000 LBC) wereinsufficient for evaluation of LBC withtwo systems. Smears and ThinPrepLBC vials were sent to four selectedlaboratories where cytotechnologistshad received training in the interpreta-tion of ThinPrep slides. The LBC samples were collected using the plas-tic cervix broom, while conventionalsmears continued to be collected by thewooden Aylesbury spatula. The results,summarized in Table 71, showed asharp reduction in the rate of unsatis-
193
Efficacy of screening
Figure 53 Ratios of test positivity for HSIL+ in direct-to-vial studies with AutoCyte Surepath LBC, compared with con-ventional Pap cytology< > indicates the combined effect estimated by random-effects model
Saurel, 1999
Vassilakos, 1999
Tench, 2000
Marino, 2001
Royer, 2001
Day, 2002
Moss, 2003
TriPath, 2003
Colgan, 2004
Combined
163-200 ( VOIR IMAGES) 24/01/05 14:58 Page 193

factory samples and a significantimprovement in the identification ofhigh-grade lesions (between 3 and 9women per 1000 tested). Reducedworkload and increased productivitywere also demonstrated in laboratories.
In Ontario, Canada, SurePath wasadopted for routine cervical screeningin large screening laboratories in 2001,after training of large numbers ofcytotechnologists. Almost one millionroutine cervical screening results were
reviewed using the Ontario Provincialdatabase. The results for 445 011SurePath samples reported betweenJanuary and June 2002 were com-pared with 445 225 conventional smearresults from the same period in 2001(Colgan et al., 2004; McLachlin et al.,2004). All slides had been screenedmanually. The SurePath cases showed21% higher reporting of LSIL+ but a15% decrease in HSIL detection.Assessment with the addition of colpo-scopic diagnostic rates is in progress todetermine the relative sensitivity andspecificity of the SurePath technologyas a routine screening test.
194
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
ThinPrep SurePath
95% CI No. of studies 95% CI No. of studies
Ratio of sensitivities (LBC/CP) 0.95 0.88–1.03 2 0.95 0.81–1.11 1
Ratio of specificities (LBC/CP) 1.08 0.90–1.30 2 0.94 0.87–1.01 1
Test threshold HSIL+Adapted from Arbyn et al. (2004a)
Table 68. Ratio of sensitivity and specificity for CIN 2+ of two liquid-based cytology systems (LBC) relative to theconventional Pap smear (CP), pooled from studies with complete verification by colposcopy and/or biopsy
Preparation system % inadequate 95% CI
Conventional Pap smear 9.7 9.4–10.0ThinPrep LBC 2.0 1.8–2.2SurePath LBC 0.9 0.8–1.1
Computed over four years of conventional cytology and the first six months’ use of LBCFrom Arbyn et al. (2004a), adapted from Moss et al. (2003)
Table 69. Prevalence of inadequate specimens by preparation system
Abnormal (≥ borderline) SIL (≥ mild dyskaryosis) HSIL (≥ moderate dyskaryosis)
Laboratory RR 95% CI RR 95% CI RR 95% CI
A 0.99 0.94–1.04 1.25 1.19–1.31 1.10 0.98–1.24B 0.94 0.90–0.99 1.00 0.93–1.08 0.85 0.75–0.96C 1.37 1.30–1.44 1.73 1.60–1.86 1.55 1.36–1.76
Age RR 95% CI RR 95% CI RR 95% CI
20–34 1.15 1.11–1.19 1.25 1.19–1.31 1.18 1.08–1.2835–49 0.96 0.91–1.02 1.03 0.94–1.13 1.01 0.87–1.1650–64 0.93 0.85–1.01 1.03 0.87–1.23 0.75 0.55–1.0120–64 (MH) 1.06 1.03–1.09 1.18 1.13–1.23 1.10 1.02–1.18
MH: overall Mantel–Haenzel-adjusted relative riskLaboratories A and C used Thin Prep; B used Sure PathFrom Arbyn et al. (2004a), adapted from Moss et al. (2003)
Table 70. Relative change in test positivity for abnormal results, SIL and HSIL in liquid-based cytology in com-parison with conventional cytology, by laboratory and by age (crude and weighted)
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 194

Use of liquid-based cytology systemsin cervical screening programmesIn May 1996, the ThinPrep T2000processor was approved by the USFood and Drug Administration (FDA)for use in cervical screening on thebasis of lower inadequacy rates andhigher identification of LSIL and HSILin comparison with conventional cytol-ogy and this was extended to the fullyautomated ThinPrep T3000 processorin May 2000. The SurePath approvalby FDA in June 1999 indicatedimproved specimen quality and equiv-alent identification of cytological abnor-malities to conventional cytology and inMay 2003 a claim for increased HSILidentification was approved by theFDA. These two LBC systems nowaccount for over 80% of cervicalscreening tests in the USA.
The Scottish Department of Healthdecided in 2002 that LBC should beimplemented as the routine screeningtest throughout Scotland, following theScottish LBC pilot project (see above).Scottish laboratories opted to use theThinPrep system and all laboratoriesare now fully converted. In Englandand Wales, the NICE (2003) recom-mended to the National Health Servicethat LBC be introduced as the primarymeans of processing samples in its
cervical screening programme. Healthtechnology assessments in severalother countries have not yet led toapproval of LBC, although it is alreadywidely used in the private sector inother parts of the world.
Other liquid-based systems are mar-keted, but there is little or no evidence inpeer-reviewed literature for their efficacy(Johnson et al., 2000; Bergeron &Fagnani, 2003; Alves et al., 2004).
Automation-assisted devicesAutomation-assisted screening isaimed at enhancing the performanceof manual microscopic screening byexcluding some of the normal slidesfrom manual screening or by relocatingthe most suspicious cells down themicroscope or collecting images into agallery for review on computerscreens. These technologies have thepotential to decrease the fatigue of theuser, allow 50% more slides to bereviewed per day, decrease thescreening false negative rate due tohuman error, with appropriate decisionsupport, identify morphological fea-tures that are not apparent in routinehuman review and, in particular, identi-fying small numbers of small abnormalcells, known to be very difficult to findin conventional screening.
Most of the automated scanningdevices are capable of processingeither conventional or liquid-basedsmears, potentially allowing their usein different kinds of screening pro-grammes. Since LBC systems depositcells onto a thin layer on a microscopeslide, problems of cell overlap andobscuring debris are mitigated andthus LBC facilitates the performance ofcomputer-assisted imaging (seeChapter 2)
Technological developments arevery rapid in this area and several newapproaches are emerging. A develop-ment of the FDA-approved AutoPap®system is the FocalPoint™ system,which is designed for use withSurePath (LBC) slides. The few pub-lished studies on the FocalPoint sys-tem suggest a performance equivalentto that of AutoPap (Cengel et al., 2003,Parker et al., 2004).
Another system that has becomecommercially available recently is theCytyc ThinPrep Imager. Again, only afew studies on the performance of thissystem have been reported, but theseshow statistically significant improve-ment in sensitivity of the Imager reviewmethod over the conventional manualreview for HSIL+. Specimen adequacycan be determined with the Imager
195
Efficacy of screening
Proportion Ratioa
Cytological category ThinPrep Conventional (ThinPrep/ conventional) 95% CI
Unsatisfactory 1.86% 8.00% 0.23 0.20–0.26Borderline 3.67% 4.35% 0.84 0.76–0.94Mild dyskaryosis 2.10% 1.09% 1.93 1.60–2.32Moderate dyskaryosis 0.97% 0.48% 2.01 1.52–2.66Severe dyskaryosis 1.09% 0.59% 1.84 1.42–2.38
a Confidence intervals are approximate. The SCSP report stated that in half of the total of 30 288 women a conventional Pap smearwas taken and in the other half a ThinPrep, so the calculation of confidence intervals was made assuming exactly 15 144 individualsin each group.From Arbyn et al. (2004a), adapted from SCSP (2002)
Table 71. Proportion of inadequate specimens and cytological abnormalities and ratios observed in two randomized groups of women from four Scottish areas
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 195

review method. Cytotechnicians wereable to double their daily work outputwhile maintaining the same quality(Biscotti et al., 2003; McKee et al., 2003).
A few randomized prospectivestudies using the obsolete Papnet sys-tem (Nieminen et al., 2003) (seeChapter 2) show that automation-assisted screening is feasible in routineprimary screening and that it performs inorganized screening programmes atleast as well as conventional manualmicroscopy. It is suggested that automa-tion-assisted screening would notimprove the outcome of an optimal cer-vical cytology service.
There are no data specifically on theefficacy of screening in HIV-positivewomen. In considering this group ofwomen, three aspects of screeningneed to be taken into account.• The accuracy of cytology as a
screening test in HIV-positive ver-sus HIV-negative women;
• The natural history of preinvasivedisease of the cervix in HIV-posi-tive versus HIV-negative women;
• The impact of anti-retroviral treat-ment on the natural history ofpreinvasive lesions of the cervix.
Accuracy of cytology in HIV-positive womenSeveral studies have addressed theaccuracy of the cytological test in HIV-positive women. Maiman et al. (1991)reported that the false negative rate ofcytology was significantly higher inHIV-infected women than in HIV-unin-fected women and recommended thatroutine colposcopy and histologicalsampling be performed in thesewomen. A follow-up study confirmedthe earlier findings (Maiman et al.,1998), based on an evaluation of 285HIV-infected and 685 HIV-negative
women, among whom 255 of the HIV-infected women underwent colposcopyand biopsy. Abnormal cytology detected62% of all biopsy-confirmed CIN and83% of all high-grade CIN in the HIV-infected women, but 38% of all CINdiagnosed would have been missedhad colposcopy not been performed.The false negative rate of cytology, how-ever, was not significantly different fromthat recorded in the HIV-negative group,reflecting the limitations of cervicalcytology as a screening test rather thana poorer performance of cytology inHIV-infected women.
Fink et al. (1994), in a cross-sec-tional analysis of 51 HIV-positivewomen examined by cytology, col-poscopy and biopsy, showed that therewas good reproducibility of cytologicalresults in HIV-infected women, but ahigh false negative rate for cytologycompared to colposcopy. For instance,of 29 women who had normal cytolog-ical findings, 24% had CIN on biopsy.The authors recommended that thishigh false negative rate of cytology andthe high prevalence of CIN in HIV-infected women warranted the inclu-sion of routine colposcopy for all HIV-infected women as a part of primaryscreening.
Korn et al. (1994) tested 52 HIV-positive women by cytology, col-poscopy and histology, and a group of85 women who self-reported HIV-neg-ative status. The prevalence of CINwas 50% in the HIV-infected group andthe sensitivity of cytology was 63%with a specificity of 84%. The perfor-mance of cytology in the control groupwas similar, however, and it was concluded that the accuracy of cytol-ogy was not significantly lower in HIV-positive women. The authors noted ahigh rate of loss to follow-up in HIV-positive women, as well as a signifi-cant incidence of concurrent lowergenital tract pathology, which may jus-tify initial colposcopic evaluation in thisgroup.
Spinillo et al. (1998) reported on across-sectional study of 241 HIV-posi-tive women and 991 controls (404known HIV-negative and 587 ofunknown HIV status). Among HIV-pos-itive women, the sensitivity of cytologywas 73% and the specificity 97%. Thecorresponding figures for the controlgroup were 84% and 99% and the dif-ferences were not statistically signifi-cant. However, the negative predictivevalue of cytology was significantlylower in the HIV-positive group. Theauthors suggested more frequentscreening of HIV-positive womenrather than primary screening withcytology, colposcopy and biopsy.
Goodman et al. (2000) undertook aprospective study of cytology and con-current colposcopically directed biop-sies in HIV-positive and -negativewomen to determine the accuracy ofcytology in the two groups. Among 82HIV-positive women, the prevalence ofCIN was 37%, compared with 17% inthe HIV-negative group; the false neg-ative rates of cytology in the HIV-posi-tive and -negative women were 37%and 21% respectively, if ASCUS find-ings on cytology were included amongthe negative results. These false nega-tive rates fell to 10% and 14%, respec-tively, if ASCUS was counted as a pos-itive result. The authors concluded thatASCUS diagnosis comprised themajority of false negative calls in HIV-positive women and they too recom-mended an initial screening col-poscopy to detect cases of CIN missedby cytology. Thereafter, they recom-mended six-monthly cytologicalscreening.
Boardman et al. (1994), who com-pared 41 HIV-positive women with 228HIV-negative and 409 women withunknown HIV status, also found no difference in the performance of cyto-logical testing between HIV-positivewomen and women of negative orunknown HIV status. With HIV-nega-tive women as the reference group, the
196
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
Efficacy of screeningamong HIV-positive women
163-200 ( VOIR IMAGES) 27/01/05 16:22 Page 196

relative risk of cytology–histology dis-crepancy was 1.1 for HIV-positivewomen compared with 1.5 for womenwhose HIV status was unknown.
Adachi et al. (1993) performed col-poscopy on 48 women with a cytologi-cal diagnosis of SIL, of whom 95% hadcolposcopic or histological findingsthat were no more severe than thecytological result. They concluded thatthe positive predictive value was high.Del Priore et al. (1995) also reported ahigh PPV of abnormal cytology to pre-dict disease in a series of 52 HIV-posi-tive women. The PPV of cytology was96% for HIV-positive women versus78% for HIV-negative women. The sensitivity of cytology among HIV-posi-tive women was only 57%, with a specificity of 92%. The authors con-cluded, however, that prediction of thepresence and degree of an intraepithe-lial lesion by abnormal cytology was noworse in HIV-positive than in HIV-nega-tive women.
Where colposcopy services arereadily available and accessible, an ini-tial colposcopy may be warranted, par-ticularly in women at greatest risk ofdisease, such as those with significantimmune compromise or borderlineabnormal cytology. Where such a ser-vice is lacking, more frequent cytologi-cal surveillance, e.g., six-monthly, hasbeen recommended, although with lit-tle supporting evidence.
Natural history of preinvasivecervical disease in HIV-positiveversus HIV-negative womenIt is now clear that women infected withHIV have a higher prevalence of infec-tion with HPV and are more likely todevelop persistent infection with multi-ple types of HPV, as well as having ahigher incidence and prevalence ofpreinvasive lesions of cervix, possiblya more rapid progression to cervicalcancer and a higher incidence of cervi-cal cancer (Schafer et al., 1991; Kleinet al., 1994; Wright et al., 1994; Sun et
al., 1997; Palefsky et al., 1999;Ellerbrock et al., 2000).
In 1992, the Centers for DiseaseControl and Prevention (CDC)included cervical cancer as an AIDS-defining disease, on the basis ofextrapolation of data on the higher fre-quency of CIN in HIV-positive than inHIV-negative women (Centers forDisease Control and Prevention,1992). A number of studies have sup-ported this view and shown that HIV-positive women generally present withmore advanced lesions and have apoorer prognosis than HIV-negativewomen (Maiman et al., 1993, 1997).
In a large population-based studyby the AIDS-Cancer Match RegistryStudy Group in the USA, Frisch et al.(2000) found that, compared with thegeneral population, HIV-infected indi-viduals were at considerably increasedrisk for all types of anogenital HPV-associated cancers and their precursorlesions. This elevated risk spannnedthe decade from five years before theonset to five years after the diagnosisof AIDS. The relative risks of in situcancer of the cervix (N = 722) (4.6;95% CI 4.3–5.0) and invasive cancer(N = 44) (5.4; 95% CI 3.9–7.2) weresimilar in women with HIV infection orAIDS.
In the population-based Cancerand AIDS Registry Linkage Study inItaly (Dal Maso et al., 2003), womenwith HIV infection or AIDS had a rela-tive risk of invasive cervical cancer (N = 18) of 21.8 (95% CI 12.9–34.6).
Lomalisa et al. (2000) presenteddata from South Africa on 60 HIV-seropositive and 776 HIV-seronegativewomen with newly diagnosed invasivecervical cancer. HIV-positive womenpresented with cervical cancer almost10 years earlier than HIV-negativewomen (mean age 44 years versus 53years), although the stage distributionwas not different in the two groups, afinding of particular importance forscreening programmes. In addition,
severely immunocompromised women(e.g., CD4+ counts below 200 cells/µL)were significantly more likely to haveadvanced-stage disease at initial diag-nosis than HIV-negative women.
A study in Senegal (Hawes et al.,2003) provided support for these con-clusions, showing that HIV infectionwas associated with increased rates ofcervical infection with high-risk types ofHPV and that high-grade cervical can-cer precursors and invasive cervicalcancer were significantly more com-mon in HIV-positive than in HIV-nega-tive women (OR = 8.0; 95% CI2.0–31.5). The degree of cervicalabnormality was related to increasedHIV viral load and increased immuno-suppression, as expressed by lowCD4+ cell counts.
Sitas et al. (2000) identified 167cases of invasive cervical canceramong HIV-positive South Africanwomen versus 1323 among HIV-nega-tive women (OR = 1.6; 95% CI1.1–2.3), suggesting an increased cer-vical cancer risk among HIV-positivewomen in a country with high rates ofcervical cancer and HIV seropositivity.
Numerous studies have indicatedan increased prevalence of preinvasivelesions of the cervix in HIV-positivewomen. Mandelblatt et al. (1992)reviewed 21 studies from 1986 to1990, and found five studies with suffi-cient data and a comparison group. Allfive studies showed a significant asso-ciation between HIV infection and CIN,with an odds ratio for HIV-positivewomen of 4.9 (95% CI 3.0–8.2) com-pared with HIV-negative women.
Wright et al. (1994) conducted across-sectional study of 398 HIV-posi-tive and 357 HIV-negative women;20% of HIV-positive women had colpo-scopically confirmed CIN, comparedwith 4% of the HIV-negative women.The sensitivity and specificity of cyto-logical testing did not differ significantlybetween the two groups and theauthors concluded that cytology was
197
Efficacy of screening
163-200 ( VOIR IMAGES) 27/01/05 16:22 Page 197

an effective screening test in HIV-posi-tive women. In addition, by multiplelogistic regression analysis, CIN wasfound to be associated with HPV infec-tion (OR = 9.8), HIV infection (OR =3.5), CD4+ T-lymphocyte count of lessthan 200 cells/µL (OR = 2.7) and agegreater than 34 years (OR = 2.0).
Delmas et al. (2000) reported onthe effect of immunodeficiency on theprevalence and incidence of SIL in 485HIV-positive women. Compared withwomen with CD4+ counts of over 500cells/µL, women with counts below 200had a two-fold increase in both theprevalence and incidence of SIL and innon-regression from untreated low-grade SIL. In addition, these womenhad a lower response rate to treatmentfor high-grade SIL.
In the Women’s Interagency HIV study(WHIS) (Massad et al., 1999), baselinecytology in 1713 HIV-positive women and482 high-risk HIV-negative women wasabnormal in 38% of HIV-positive womencompared with 16% of HIV-negativewomen. Risk factors for any abnormalcytology were CD4+ counts lower than200 cells/µL (OR = 2.13; 95% CI1.45–3.13), presence of HPV DNA andhistory of abnormal cytology.
Ellerbrock et al. (2000) showed thatthe prevalence of abnormal cytologicalfindings was 4.3-fold higher in HIV-infected than in uninfected women,confirming the findings of other studiesshowing abnormal cytology rates of23–60% (Provencher et al., 1988).HIV-positive women were 4.5 timesmore likely to have histologically con-firmed CIN at 54 months of follow-upthan HIV-negative women.
Ahdieh et al. (2000) followed 84HIV-negative and 184 HIV-positiveinjection drug users with six-monthlyvisits. Of the HIV-positive women, 70%were HPV DNA-positive at baselinecompared with 26% of HIV-negativewomen. Cervical abnormalities werefound in 13% of HIV-infected womenversus 2% of HIV-negative women.
Following treatment, HIV-positivewomen have generally shown highrecurrence rates ranging from 38% to62%, compared with 15–18% in HIV-negative women (Petry et al., 1994;Maiman et al., 1999; Chirenje et al.,2002).
Impact of anti-retroviral therapyon the natural history of preinvasive cervical lesionsThe use of anti-retroviral therapy (ART)for treatment of HIV-infected individu-als in developed countries has sub-stantially reduced the associated mor-bidity and mortality. The increase in lifeexpectancy may affect the burden ofcervical cancer in either direction,depending on the degree to which theimmune reconstitution allowed by ARTis sufficient to diminish the risk of cer-vical cancer. The InternationalCollaboration on HIV and Cancer(2000) found no change in the inci-dence of cervical cancer between1992–96 and 1997–99 (i.e., after theuse of ART had become widespread)in a reanalysis of cancer risk in 23cohort studies in developed countries.This contrasted with marked reduc-tions in the incidence of Kaposi sar-coma and non-Hodgkin lymphoma.
Recent studies have shown a ben-eficial impact of ART, with greaterregression of HPV-associated lesionsin treated women. In a cohort ofFrench women, the prevalence of cer-vical HPV infection among 34 HIV-pos-itive women remained unchanged at81% five months after the initiation ofART. However the prevalence of CINdecreased from 69% to 53% after amedian of five months (p = 0.04) and themean CD4+ cell count was higheramong women who regressed, suggest-ing that the loss of immune responseand ART-induced reconstitution ofimmunity may have played a role in pro-tecting against CIN (Heard et al., 1998).
In a long-term follow-up study(Heard et al., 2002) (median follow-up
17.7 months) of 168 HIV-positivewomen, 96 of whom were receivingART, regression of CIN (defined as aregression to normality or to a lowergrade of CIN) was seen in 40% of the168 women. In a multivariate analysis,the grade of the lesion and the use ofART were independently associatedwith regression of CIN, after adjust-ment for CD4+ cell count. The relativehazard of regression of CIN in womenreceiving ART was 1.93 (95% CI1.14–3.29; p = 0.01) compared withuntreated HIV-positive women. In addi-tion, a trend for a greater increase inCD4+ cell counts after six months ofART was observed in women whoregressed compared with those whodid not.
Minkoff et al. (2001) reported thatwomen on ART were 40% more likelyto show regression of cervical cytolog-ical abnormalities towards normality orlower-grade disease and less likely toshow progression (OR = 0.68; 95% CI0.52–0.88), after control for stage ofHIV disease and severity of cytologicalabnormality. Among HIV-infectedwomen, persistence of HPV infectionand high HIV viral load were associ-ated with cytological progression.Conversely, low HIV viral load and highCD4+ cell counts were associated withregression.
Moore et al. (2002) reported on 71HIV-positive women who were exam-ined by cytology, colposcopy andbiopsy before starting ART and had atleast one similar assessment sixmonths after starting ART. The base-line prevalence of cervical disease was55%, and at six months after startingART 13% of the women showedregression without treatment of thecervix. No individual factor (e.g., smok-ing, HIV viral load, stage of HIV dis-ease or CD4+ cell count) was signifi-cantly associated with regression,although a greater increase in CD4+cell count in women on ART was moststrongly associated with regression
198
IARC Handbooks of Cancer Prevention Volume 10: Cervix cancer screening
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 198

(OR = 1.66 per 50 cell increase, p =0.08).
These data suggest that the bestresponses of cervical disease inwomen on ART are seen amongwomen with higher CD4+ cell countsor that women who respond to ARTare those with the largest increase inCD4+ cell counts. It is important to
note, however, that progression fromCIN to cervical cancer occurs overmany years. Before ART was intro-duced, HIV-positive women most oftendied of other HIV-related diseases andthere was insufficient time for thedevelopment of cervical cancer. If ARTleads to prolongation of life, womenwith cervical disease may be at greater
risk of developing invasive cervicalcancer if they do not enter a screeningprogramme. Until a clear impact ofART on the regression and progres-sion of HPV-associated lesions of thecervix is confirmed, HIV-positivewomen being treated with ART shouldundergo cervical screening and beactively treated where appropriate.
199
Efficacy of screening
163-200 ( VOIR IMAGES) 24/01/05 11:09 Page 199