Embed Size (px)
Citation preview
VALVULAR HEART DISEASE
324
Malfunction of any of the cardiac valvesresults in a less efficient circulatory system.Valvular dysfunction causes work overload inone or both ventricles. In extreme cases, result-ant congestive heart failure can cause death.More information about etiology, pathogenesis,differential diagnoses, and diagnostic approach-es used for evaluation of valvular diseases canbe found in chapters 27–33.
BACKGROUNDBefore the discovery of penicillin, rheumat-
ic heart disease was commonplace. Physi-cians recognized that mitral valve stenosis fre-quently followed rheumatic fever. Thisobstruction to blood flow through the mitralvalve was not medically treatable however.For “stenosed” mitral valves, physiciansdescribed the need to relieve the obstructionsurgically. The first successful attempt at surgi-cal treatment involved incising the left atrialappendage, placing a finger through the inci-sion into the left atrium, feeling the stenoticmitral valve, and relieving the obstruction bysimple finger pressure. Soon after these initialtherapeutic approaches, special knives anddilators were developed to relieve mitralvalve stenosis. In the early days of cardiovas-cular surgery, these procedures were all per-formed on the beating heart.
The notion of using anticoagulant heparin toallow blood to circulate outside a patient’s vas-culature without clotting led to the develop-ment of cardiac and pulmonary bypass
machines in the 1950s. It was then possible tokeep the patient alive while stopping the heartfor surgical repair. The ability to stop the heart,examine valve pathology, and try to repair itstimulated surgeons’ collaboration withmechanical engineers in developing prostheticvalves to replace those that were too diseasedto repair. Initial attempts to duplicate valveleaflets with flexible, nonbiologic materialsfailed. The leaflets of these valves were too stiffin comparison with normal valve leaflets.
FIRST-GENERATION PROSTHETIC VALVES
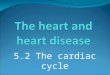
Attempts at using nonflexible leaflets by con-structing hinged valve leaflets resulted in hingethrombosis and malfunction. Design engineersthen focused on free-floating occluders, such asdiscs or balls retained in a cage-like housing. Thisgeneral valve design produced the first clinicallyuseful valves, including the Hufnagel, Starr-Edwards, Smeloff-Cutter, and Beall valves (Fig.34-1). In 1958, the Starr-Edwards valve was usedin the first clinically successful valve replace-ment.
Although these early designs functioned asintended, the first caged-ball valves had majorshortcomings: (1) they were bulky in design anddid not fit well into a small ventricle or aorta; (2)they had a small internal orifice, making themrelatively stenotic; and (3) they stimulatedthrombus formation, which precipitated throm-boembolic events, necessitating long-term anti-coagulation therapy.
Competency of the atrioventricular valves allows blood to enter the ventricles, where pressure isgenerated. When adequate systolic blood pressure (SBP) is generated, the aortic and pulmonaryvalves open, allowing the blood to enter the arterial system. The atrioventricular valves close, pre-venting the flow of blood into the atria. During diastole, the aortic and pulmonary valves close, theatrioventricular valves open, the ventricles fill and ultimately begin the cycle of pulsatile blood flowthrough the systemic and pulmonary vascular tree.
Peter J. K. Starek
Chapter 34
Surgical Treatment for Valvular Heart Disease
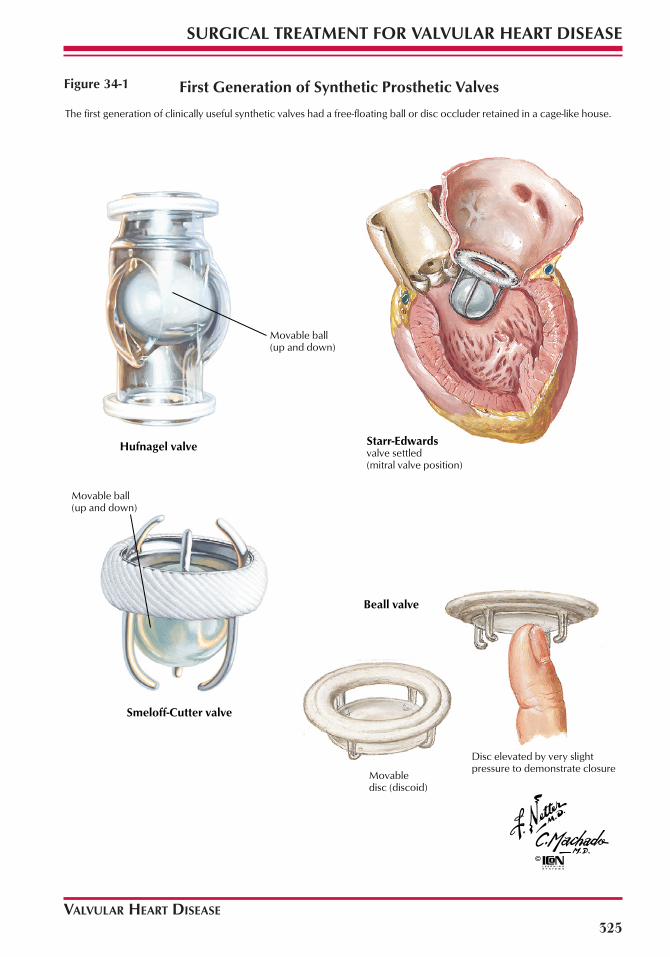
The first generation of clinically useful synthetic valves had a free-floating ball or disc occluder retained in a cage-like house.
Movable ball (up and down)
valve settled (mitral valve position)
Movable ball (up and down)
Movable disc (discoid)
Disc elevated by very slight pressure to demonstrate closure
Hufnagel valve Starr-Edwards
Smeloff-Cutter valve
Beall valve
First Generation of Synthetic Prosthetic Valves
VALVULAR HEART DISEASE
SURGICAL TREATMENT FOR VALVULAR HEART DISEASE
325
Figure 34-1
VALVULAR HEART DISEASE
SURGICAL TREATMENT FOR VALVULAR HEART DISEASE
326
SECOND-GENERATION PROSTHETIC VALVES
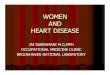
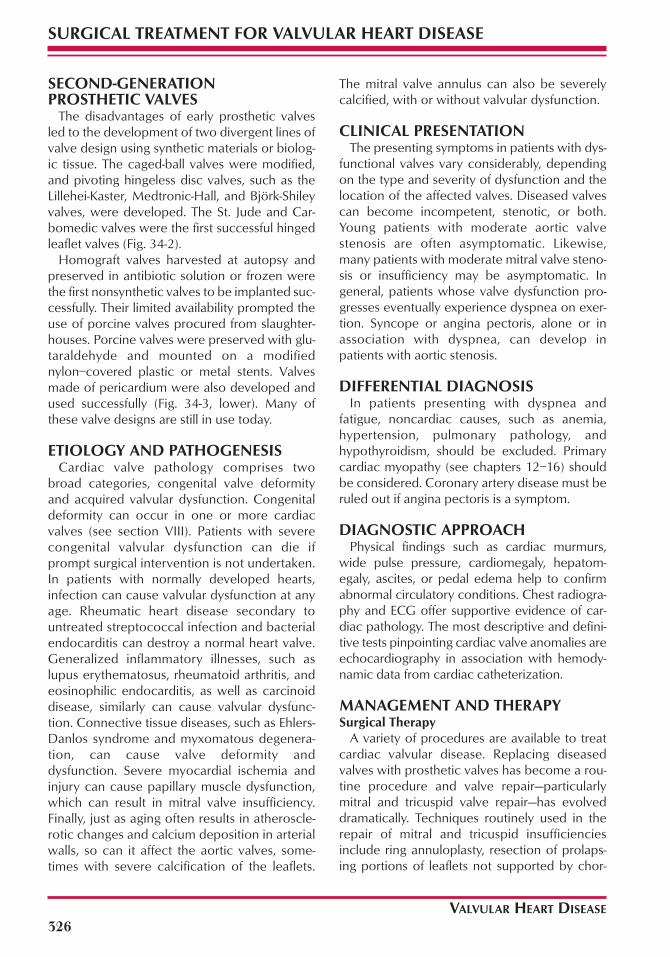
The disadvantages of early prosthetic valvesled to the development of two divergent lines ofvalve design using synthetic materials or biolog-ic tissue. The caged-ball valves were modified,and pivoting hingeless disc valves, such as theLillehei-Kaster, Medtronic-Hall, and Björk-Shileyvalves, were developed. The St. Jude and Car-bomedic valves were the first successful hingedleaflet valves (Fig. 34-2).
Homograft valves harvested at autopsy andpreserved in antibiotic solution or frozen werethe first nonsynthetic valves to be implanted suc-cessfully. Their limited availability prompted theuse of porcine valves procured from slaughter-houses. Porcine valves were preserved with glu-taraldehyde and mounted on a modifiednylon–covered plastic or metal stents. Valvesmade of pericardium were also developed andused successfully (Fig. 34-3, lower). Many ofthese valve designs are still in use today.
ETIOLOGY AND PATHOGENESISCardiac valve pathology comprises two
broad categories, congenital valve deformityand acquired valvular dysfunction. Congenitaldeformity can occur in one or more cardiacvalves (see section VIII). Patients with severecongenital valvular dysfunction can die ifprompt surgical intervention is not undertaken.In patients with normally developed hearts,infection can cause valvular dysfunction at anyage. Rheumatic heart disease secondary tountreated streptococcal infection and bacterialendocarditis can destroy a normal heart valve.Generalized inflammatory illnesses, such aslupus erythematosus, rheumatoid arthritis, andeosinophilic endocarditis, as well as carcinoiddisease, similarly can cause valvular dysfunc-tion. Connective tissue diseases, such as Ehlers-Danlos syndrome and myxomatous degenera-tion, can cause valve deformity anddysfunction. Severe myocardial ischemia andinjury can cause papillary muscle dysfunction,which can result in mitral valve insufficiency.Finally, just as aging often results in atheroscle-rotic changes and calcium deposition in arterialwalls, so can it affect the aortic valves, some-times with severe calcification of the leaflets.
The mitral valve annulus can also be severelycalcified, with or without valvular dysfunction.
CLINICAL PRESENTATIONThe presenting symptoms in patients with dys-
functional valves vary considerably, dependingon the type and severity of dysfunction and thelocation of the affected valves. Diseased valvescan become incompetent, stenotic, or both.Young patients with moderate aortic valvestenosis are often asymptomatic. Likewise,many patients with moderate mitral valve steno-sis or insufficiency may be asymptomatic. Ingeneral, patients whose valve dysfunction pro-gresses eventually experience dyspnea on exer-tion. Syncope or angina pectoris, alone or inassociation with dyspnea, can develop inpatients with aortic stenosis.
DIFFERENTIAL DIAGNOSISIn patients presenting with dyspnea and
fatigue, noncardiac causes, such as anemia,hypertension, pulmonary pathology, andhypothyroidism, should be excluded. Primarycardiac myopathy (see chapters 12–16) shouldbe considered. Coronary artery disease must beruled out if angina pectoris is a symptom.
DIAGNOSTIC APPROACHPhysical findings such as cardiac murmurs,
wide pulse pressure, cardiomegaly, hepatom-egaly, ascites, or pedal edema help to confirmabnormal circulatory conditions. Chest radiogra-phy and ECG offer supportive evidence of car-diac pathology. The most descriptive and defini-tive tests pinpointing cardiac valve anomalies areechocardiography in association with hemody-namic data from cardiac catheterization.
MANAGEMENT AND THERAPY Surgical Therapy
A variety of procedures are available to treatcardiac valvular disease. Replacing diseasedvalves with prosthetic valves has become a rou-tine procedure and valve repair—particularlymitral and tricuspid valve repair—has evolveddramatically. Techniques routinely used in therepair of mitral and tricuspid insufficienciesinclude ring annuloplasty, resection of prolaps-ing portions of leaflets not supported by chor-
VALVULAR HEART DISEASE
SURGICAL TREATMENT FOR VALVULAR HEART DISEASE
327
Second-generation synthetic prosthetic valves were hingeless pivoting disk valves and hinged bileaflet valves.
Tissue valves made of porcine aortic valves, pericardium, or cadaver homografts are also important in valve replacement surgical therapy.
Anterior mitral leaflet
Aorta artery wall
Medtronic-Hall pivoting disk valve
St. Jude bileaflet valve
Björk-Shiley valveCarbomedics bileaflet valve
Hancock porcine valve (closed)
Edwards-Carpentier valve (closed)
A Medtronic freestyle valve
Aortic homograft being settled
Second Generation of Synthetic Prosthetic Valves and Biologic Valves
Figure 34-2
VALVULAR HEART DISEASE
SURGICAL TREATMENT FOR VALVULAR HEART DISEASE
328
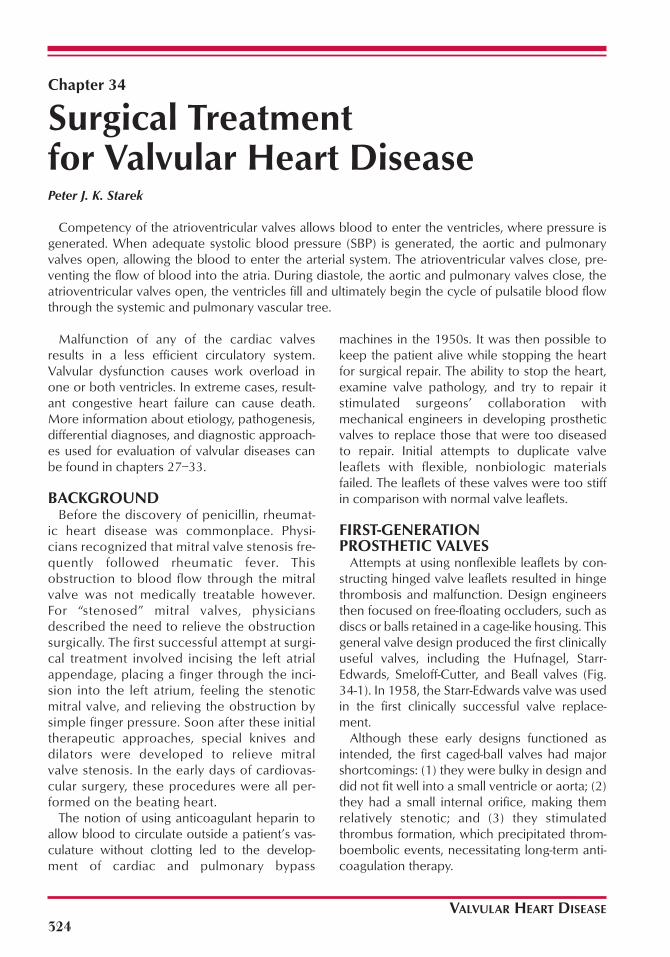
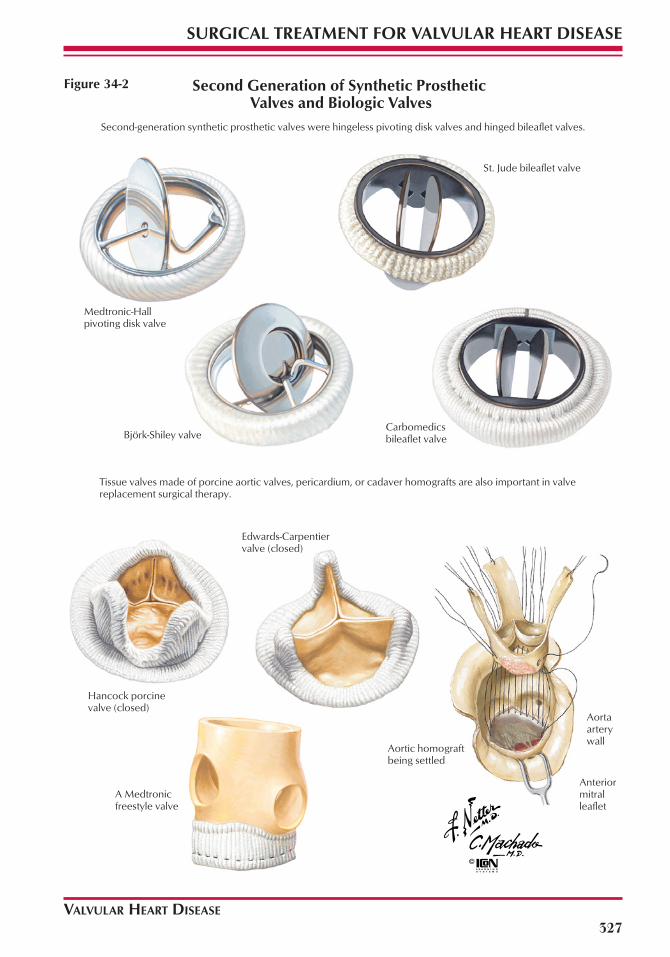
Torn anterior leaflet chordae
Ascending aorta wall
Anterior leaflet
Posterior leafletLeft atrium
Chordae
Left ventricle
Papillary muscles
Portion of the posterior leaflet, with chordae transferred to repair the anterior leaflet (Carpentier quadrangular technique)
In these views, the medial aspect of the mitral valve, chordae tendineae, and papillary muscles apparatus has been removed.
Anterior leaflet reconstructed
Cut for sliding annuloplasty technique
Insertion of a flexible annuloplasty ring may be indicated to reestablish the coaptation and strengthen the annular support.
In these views, the valvar apparatus is shown complete with chordae tendineae and papillary muscles.
Chordal Transfer, Sliding Annuloplasty, and Ring Annuloplasty
Figure 34-3

VALVULAR HEART DISEASE
329
SURGICAL TREATMENT FOR VALVULAR HEART DISEASE
dae, shortening or using artificial chordae, andincreasing or decreasing the leaflet area by slid-ing annuloplasty (Fig. 34-4). In patients whoneed aortic valve replacement, some surgeonsadvocate the Ross procedure, which entailstransplanting a patient’s pulmonary valve intothe aortic position. This provides the patientwith a living, durable, nonthrombogenic, andhemodynamically superior valve. The pul-monary valve is then reconstructed using a tis-sue homograft valve. The choice of proceduredepends on many factors, including thepatient’s valve pathology, age, and ability to tol-erate and comply with long-term anticoagula-tion.
Mitral and Tricuspid ValvesPatients with mitral and tricuspid valve pathol-
ogy should be considered for valve repair ratherthan replacement because the operative mortal-ity associated with repair of these valves is lowerthan that associated with their replacement.After surgery for either valve repair or replace-ment, patients need to receive anticoagulantsfor 3 to 6 months until the surgical site isendothelialized. Patients with repaired valves orvalves replaced with biologic tissue can then dis-continue anticoagulation if they remain in sinusrhythm. The long-term incidence of thromboem-bolic events is generally lower in patients withrepaired valves in comparison with patients withreplaced valves. This is one of the reasons thatvalve repair is preferable to valve replacement,when the repair is technically feasible.
Conditions precluding satisfactory repair ofthe mitral and tricuspid valves include severescarring and deformation by a disease processsuch as advanced rheumatic heart disease,advanced lupus, or another inflammatoryprocess involving the valve leaflets and destruc-tion of valve leaflets and annuli by endocarditis.Under these circumstances, the valve should bereplaced. Mitral valve replacement shouldinclude preservation of a portion of the sub-valvular chordae and papillary muscles to aid inpreserving normal ventricular contractility.
Aortic ValvesAdult patients with aortic valve pathology are
seldom candidates for valve repair; valve
replacement is usually necessary for significantaortic stenosis or regurgitation. The patient’sage, the patient’s lifestyle, and the preferencesof the surgeon and the patient dictate the typeof prosthetic valve replacement.
Patients with prosthetic valves made of bio-logic tissue have a lower incidence of bleedingbecause long-term anticoagulation is notrequired in patients in sinus rhythm. Unfortu-nately, all tissue valves eventually deteriorateand become insufficient. Deterioration of tissuevalves occurs at an accelerated rate in youngerpatients and in patients with end-stage renal dis-ease on hemodialysis. For older patients, partic-ularly those with a risk of falling, a tissue valvemay be the most appropriate choice. Youngerpatients, with a natural life expectancy exceed-ing 15 to 20 years, should have prosthetic valvesmade of durable synthetic materials, such aspyrolytic carbon, titanium, stainless steel, or acombination of these.
Postoperatively, all patients with prostheticheart valves must be anticoagulated untilendothelialization of the sewing ring is com-plete, as discussed previously herein. Use ofnon-tissue valves necessitates indefinite antico-agulation.
Issues With Prosthetic Valve ReplacementNontissue valves must have an appropriate
sewing ring sutured to the annulus of thepatient’s valve after the leaflets are excised.Sewing rings are usually circular and rigid andvary in thickness. The rigid sewing rings changethe natural shape of the valve annulus and,depending on thickness, decrease the size ofthe internal orifice of the prosthetic valve.Implanting a valve with a circular sewing ringinto a noncircular annulus can generate unnatu-ral tension between the valve annulus andsewing ring, which can lead to paravalvularleaks; the surgical approach in these instancesmust take this possibility into account.
The use of rigid circular sewing rings is unnec-essary in biologic tissue valves implanted in theaortic position. Freehand suturing is used toinsert autograft pulmonary valves into the aorticposition (the Ross procedure). It is also used inhomograft cadaver valve implantation and withnonstented freestyle porcine valves.
VALVULAR HEART DISEASE
SURGICAL TREATMENT FOR VALVULAR HEART DISEASE
330
SURGICAL TREATMENT FOR VALVULAR HEART DISEASE
330
Figure 34-4
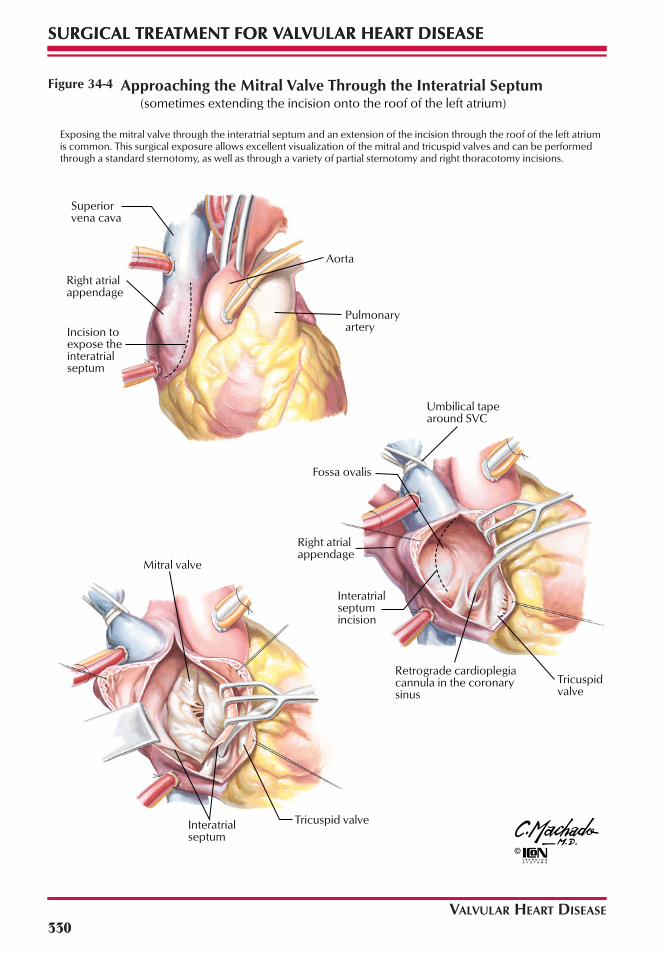
Exposing the mitral valve through the interatrial septum and an extension of the incision through the roof of the left atrium is common. This surgical exposure allows excellent visualization of the mitral and tricuspid valves and can be performed through a standard sternotomy, as well as through a variety of partial sternotomy and right thoracotomy incisions.
Tricuspid valve
Superior vena cava
Right atrial appendage
Aorta
Pulmonary arteryIncision to
expose the interatrial septum
Umbilical tape around SVC
Fossa ovalis
Right atrial appendage
Interatrial septum incision
Retrograde cardioplegia cannula in the coronary sinus
Tricuspid valve
Mitral valve
Interatrial septum
Approaching the Mitral Valve Through the Interatrial Septum(sometimes extending the incision onto the roof of the left atrium)

VALVULAR HEART DISEASE
SURGICAL TREATMENT FOR VALVULAR HEART DISEASE
331
Minimally Invasive TechniquesMinimally invasive coronary artery revascular-
ization surgery uses small incisions and there-fore is performed on a beating heart, obviatingthe use of cardiopulmonary bypass (CPB). Invalve repair and replacement procedures, theuse of smaller incisions is possible, but eliminat-ing CPB is not feasible with current techniquesand prosthetic valves.
Good visualization of the operative field is aprerequisite for proper valve repair or replace-ment. Smaller incisions limit visualization,although the use of miniature video camerasimproves the view of the operative field. Themitral valve is generally the most difficult to visu-alize, so many surgeons approach it through theintra-atrial septum, sometimes extending the inci-sion to the roof of the left atrium (see Fig. 34-4).
FUTURE DIRECTIONSRefinements in manufacturing synthetic pros-
thetic valves and their sewing rings will continueto decrease thromboembolic complicationswhile improving their hemodynamic characteris-tics. Better chemical preservation of tissuevalves will improve their longevity and resist-ance to deterioration and make tissue valves amore attractive choice for younger patients.
The teaching of valve repair techniques to sur-gical trainees is already becoming more stan-dardized. The appropriate surgical repair tech-
nique will be more predictable from the preoper-ative, noninvasive echocardiographic examina-tion and hemodynamic evaluation. Freehandvalve implantation techniques will find increaseduse in selected patients, particularly for patients inwhom the annulus is small and the valve sewingrings make the prosthetic valves too stenotic.Finally, with clinical acceptance of genetic engi-neering, farms of genetically altered pigs andbaboons might provide viable biologic leaflets,valves, and entire hearts for implantation.
REFERENCESCarpentier A. Cardiac valve surgery: The “French connec-
tion.” J Thorac Cardiovasc Surg 1983;86:323–337.Duran CG, Pomar JL, Revuelta JM, et al. Conservative oper-
ation for mitral insufficiency: Critical analysis supportedby postoperative hemodynamic studies in 72 patients. JThorac Cardiovasc Surg 1980;79:326–337.
Katholi RE, Nolan SP, McGuire LB. Living with prostheticheart valves: Subsequent noncardiac operations and therisk of thromboembolism or hemorrhage. Am Heart J1976;92:162–167.
Khan SS, Trento A, DeRobertis M, et al. Twenty-year com-parison of tissue and mechanical valve replacement. JThorac Cardiovasc Surg 2001;122:257–269.
Ross DN. Replacement of aortic and mitral valves with a pul-monary autograft. Lancet 1967;2:956–958.
Rozich JD, Carabello BA, Usher BW, et al. Mitral valvereplacement with and without chordal preservation inpatients with chronic mitral regurgitation: Mechanismsfor differences in postoperative ejection performance.Circulation 1992; 86:1718–1726.
Shumacker HB Jr. The Evolution of Cardiac Surgery. Bloom-ington: Indiana University Press; 1992:39.

BLANK