Embed Size (px)
Citation preview
Chapter 32 Operating Room Fires and Personnel Injuries Related to Sources of Ignition P.908
Al though f lammable anesthet ics have disappeared from operating rooms,
perioperat ive f i res cont inue to occur. They can have devastat ing consequences,
precipi ta te legal act ion, and take a great psychological to ll on everyone involved.
They usua lly come as a comple te surprise to the staff (1,2,3,4).
Most operat ing room fi res are o f l i t tle consequence and are not reported, making
the actual inc idence dif f icul t to determine (2,5 ,6). Approx imately 10% to 20% of
reported f i res resu lt in serious patient injury (7,8). Fuels present in the operat ing
room include plast ics tha t produce dense black smoke when ignited. The smoke
may conta in toxins and may h inder safe evacuation of the pat ient and staff f rom the
room. Sudden igni tion can present secondary problems (9). It can cause a start le
ref lex , caus ing the surgeon's hand to je rk and potentially cut into unin tended t issue
or set other a reas of the surgical s ite on fi re .
The Fire Triangle For a f i re to occur, there must be three fac tors (f ire tr iangle or triad) p resent: an
igni tion source, a fuel , and an oxid izer to support combustion together in the proper
proport ions and under the right condi t ions (Fig. 32.1).
View Figure
Figure 32.1 Three things are necessary for a fire to occur: an ignition source, fuel, and an oxidizer.
Ignition Source There are a number of igni tion sources in the operat ing room. Most are under the
surgeon's control.
Lasers The acronym laser ( l ight ampl if ication by s timulated emission of radiat ion) def ines
the process by which a form of energy is converted into l ight energy
(10,11,12,13,14,15,16). The term can also refer to the device tha t produces the
l ight or to the l ight i tself .
Lasers use a col imated, coherent, monochromatic , intense beam of electromagnetic
radiation to cut, coagulate, or vaporize tissue.
The rate that the laser energy is delivered is ca lled power and is measured in
watts . The wattage is equal to the amount of energy, measured in joules, d iv ided by
the duration of exposure measured in seconds. Laser power density is the amount
of power d istr ibu ted wi thin an area and is indicated in watts per square cent imeter.
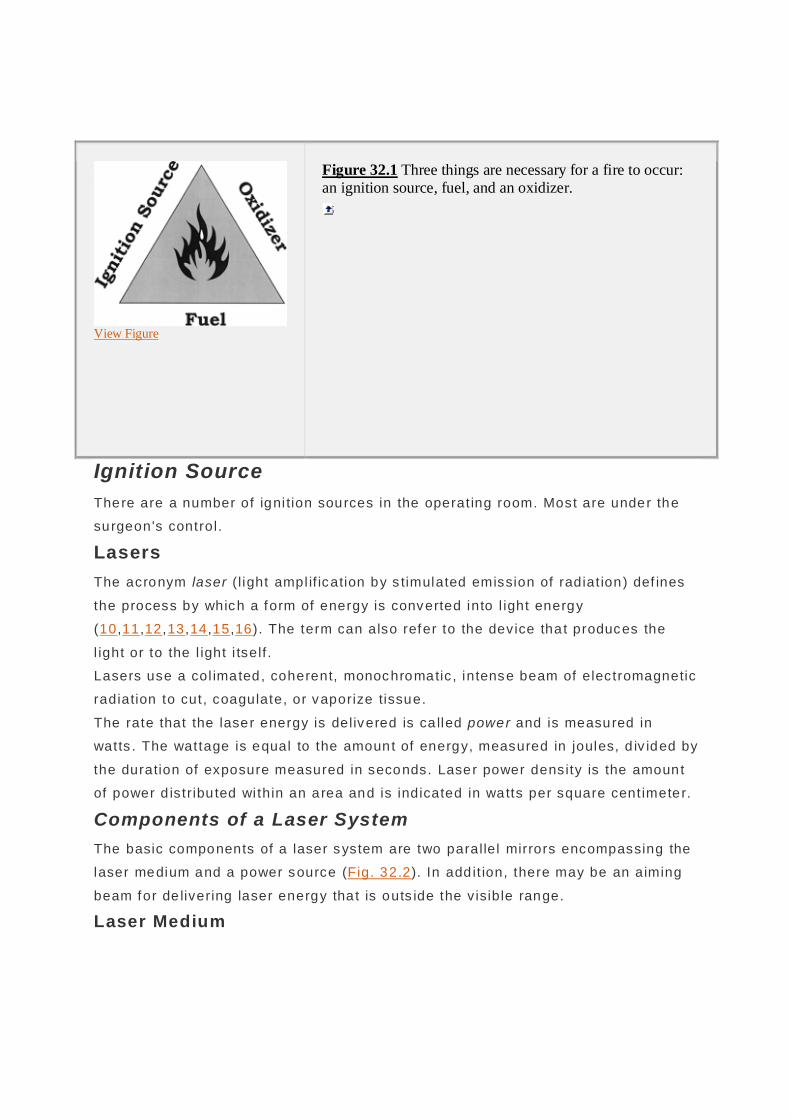
Components of a Laser System The basic components of a laser system are two parallel mirrors encompassing the
laser medium and a power source (Fig. 32.2). In add it ion, there may be an aiming
beam for de livering laser energy tha t is outs ide the v isible range.
Laser Medium

The medium (head) holds the subs tance energized to produce laser l igh t. The
medium, wh ich may be a solid, liquid, o r gas, determines the wavelength of the
emitted radiation . The laser is named for the material used as the medium.
Power Source The power (pumping, pump, exci ta tion) source supplies energy to the laser med ium
to c reate the l ight. When the power source is act ivated, energy is absorbed by
electrons of the atoms in the laser medium, which are e levated to energy levels
above their ground state. They then decay to lower energy levels and emit photons
that are not in phase with one another and travel in all di rections.
Optical Cavity The optical (resonator) cavi ty p rov ides the envi ronment in which the laser medium
is conf ined. Energy released from the medium travels in al l di rect ions. Mirrors are
used to ref lec t and increase the energy of emission. One of the mirrors is no t 100%
ref lec tive and allows a small port ion of the l ight to escape.
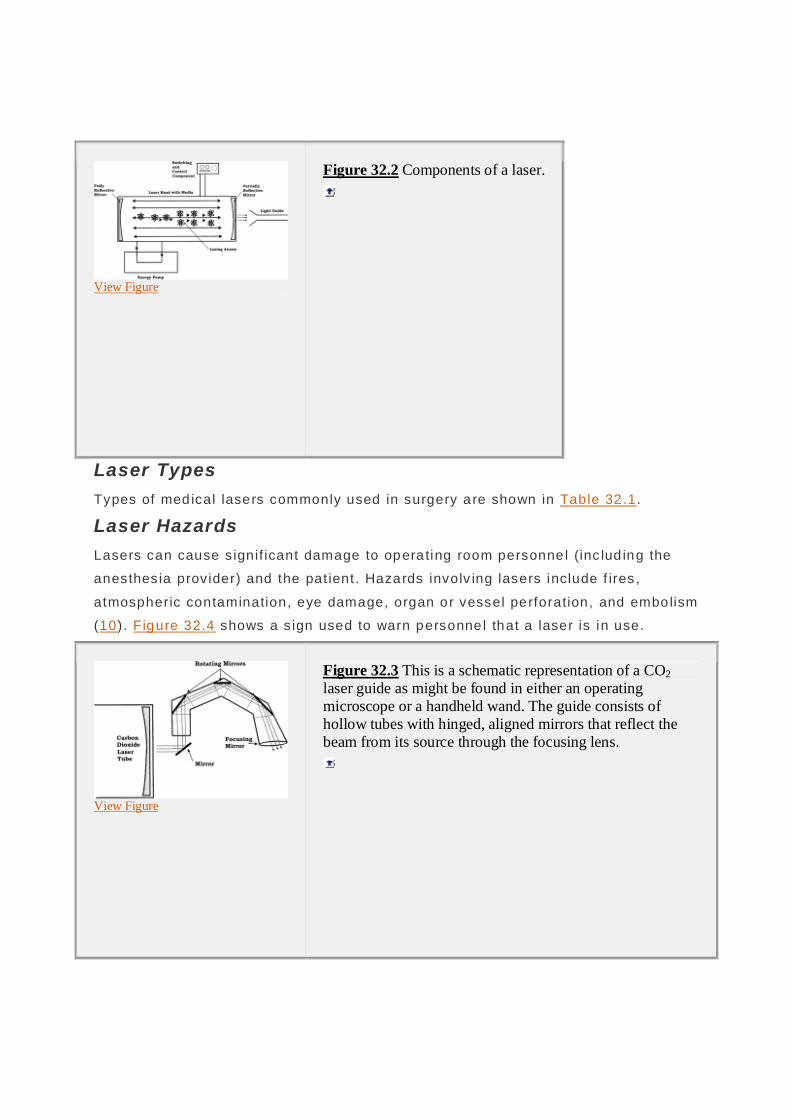
Light Guide A light guide (delivery system) di rec ts the laser beam to the surgical s ite (Fig.
32.3). Fiber-optic bundles are a convenient f lex ible condui t for some wavelengths .
Other lasers ut i l ize a hol low tube wi th mirrors aligned to reflect the beam f rom i ts
source through the focusing lens .
Aiming Beam With certa in lasers, it is necessary to use a low-powered v is ib le beam as a marker.
This is usua lly a helium-neon gas laser. I t passes th rough the same optical pa th as
the laser beam.
P.909
View Figure
Figure 32.2 Components of a laser.
Laser Types Types of med ical lasers commonly used in surgery are shown in Table 32 .1.
Laser Hazards Lasers can cause s ignif icant damage to opera ting room personne l (inc lud ing the
anesthesia provider) and the pat ient. Hazards involv ing lasers include f ires ,
atmospheric contamination, eye damage, organ or vessel perforation, and embolism
(10). Figure 32.4 shows a s ign used to warn personne l that a laser is in use.
View Figure
Figure 32.3 This is a schematic representation of a CO2 laser guide as might be found in either an operating microscope or a handheld wand. The guide consists of hollow tubes with hinged, aligned mirrors that reflect the beam from its source through the focusing lens.

A recurrent problem wi th lasers is that they may be activated when not in use
(22,23). Often, a foot switch accidentally act iva tes the laser. The laser may be in a
posit ion where this is not no ticed for some time. When the laser is not actually in
use, i t should be p laced in the STAND-BY mode.
A f i re may resu lt when a laser beam hits a fuel or the laser f iber becomes
damaged. Ign ition can be almost ins tan taneous. Whi le mos t ignition sources must
be in contact with a material to cause ign it ion, a laser can supp ly heat to a fuel
f rom a few centimeters to severa l meters away, so i t can ignite material c lose to the
t ip, at some d istance from the tip , or under several layers of o ther material . A
surface drape can be penetrated by the laser but not igni te . Materials under the
drape may then igni te and burn wi thout being not iced for several minutes (24). The
laser beam can be ref lec ted f rom a metal surface, causing a burn or ign it ing
material in a remote loca tion.
Laser Risk Classification A classif ication system ref lecting laser risk to the patient and personnel has been
developed (25,26,27). The higher the c lass, the more stringent the protec tion
needed.
P.910
TABLE 32.1 Commonly Used Lasers and Associated Personnel Hazards
Laser Medium
Features Potential Hazards to the Eye
Special Considerations
CO2 Readily absorbed by all biologic materials, independent of pigmentation. Tissue destruction is proportional to its water content. Produces a very superficial tissue effect.
Injury to the eye will be confined to the cornea. There is no risk to the retina. Since the laser is absorbed by plastic and glass, ordinary eyeglasses with sideguards can be used for eye protection.
Fires involving both tracheal tubes and supraglottic devices have been reported with this laser.
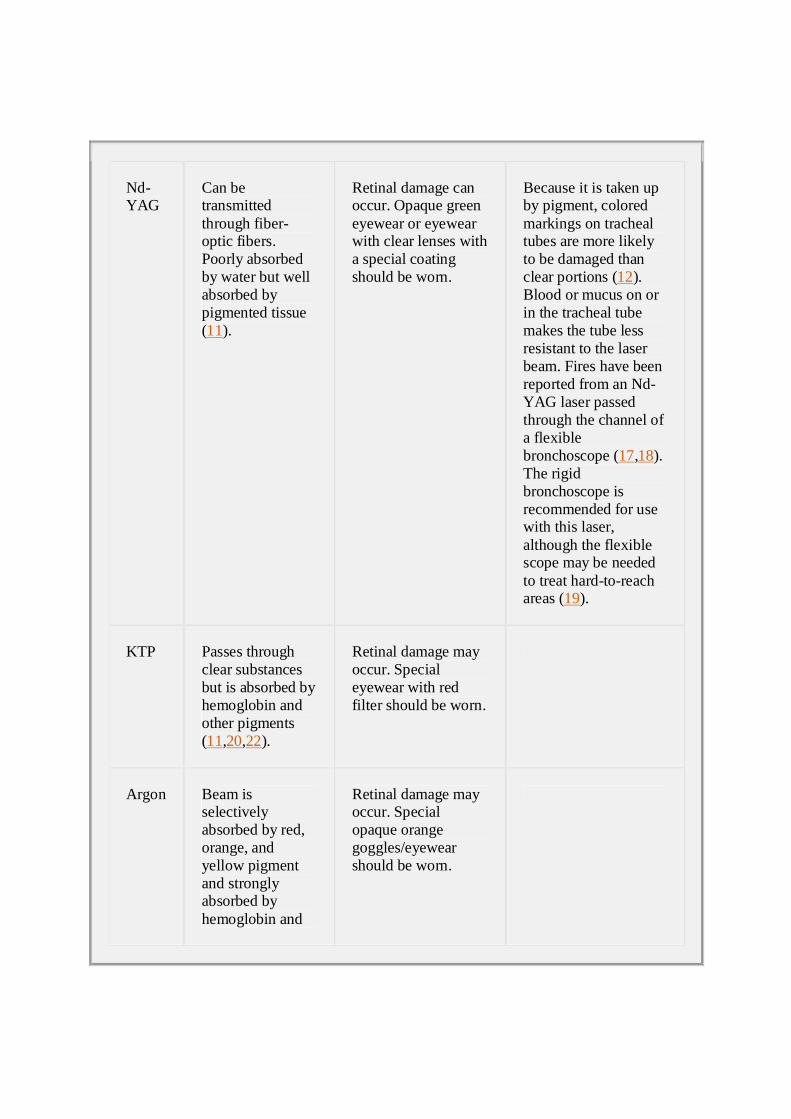
Nd-YAG
Can be transmitted through fiber-optic fibers. Poorly absorbed by water but well absorbed by pigmented tissue (11).
Retinal damage can occur. Opaque green eyewear or eyewear with clear lenses with a special coating should be worn.
Because it is taken up by pigment, colored markings on tracheal tubes are more likely to be damaged than clear portions (12). Blood or mucus on or in the tracheal tube makes the tube less resistant to the laser beam. Fires have been reported from an Nd-YAG laser passed through the channel of a flexible bronchoscope (17,18). The rigid bronchoscope is recommended for use with this laser, although the flexible scope may be needed to treat hard-to-reach areas (19).
KTP Passes through clear substances but is absorbed by hemoglobin and other pigments (11,20,22).
Retinal damage may occur. Special eyewear with red filter should be worn.
Argon Beam is selectively absorbed by red, orange, and yellow pigment and strongly absorbed by hemoglobin and
Retinal damage may occur. Special opaque orange goggles/eyewear should be worn.
melanin. Fiber-optic bundles can be used to transmit the laser beam.
From Klarr P. Laser complications. In: Atlee J, ed. Complications in Anesthesia. Philadelphia: WB Saunders, 1999:588–590.
Class 1 Lasers Lasers that are totally enclosed or that emit extremely low output fall into c lass 1.
These are safe to v iew.
Class 2 Lasers Low-risk lasers are in c lass 2. Their r isk is approximate ly equivalent to staring at
the sun or o ther brigh t lights that can cause centra l re tinal injury. These are not
hazardous unless someone overcomes their natura l aversion response to bright
l ight.
Class 3 Lasers Class 3 lasers operate at a power level above 1 mW. This is a hazard even if
v iewed only momentari ly . Class 3 lasers are subdiv ided into a and b subclasses .
The 3a subclass cons is ts of lasers in the 1 to 5 mw power range. These lasers pose
a moderate ocular hazard. Class 3b inc ludes lasers that emit between 5 and 500
mW of output power. Even momentary v iewing of these lasers is potential ly
hazardous to the eye. They may also be a hazard to skin.
P.911
View Figure
Figure 32.4 Note that the laser class is on the sign.
Class 4 Lasers Any cont inuous wave laser wi th a power output above 500 mW is in c lass 4 . These
lasers pose serious skin, eye, and f i re hazards.
Igni tion risk is re lated to a number of fac tors beside the laser c lassif ication . Class
3b and 4 lasers are cons idered to be igni tion hazards. The igni t ion risk of other
c lasses of lasers wi l l depend on how they are focused, the t ime of exposure, and
the oxidizers and fuels tha t are present.
Metal instruments can become overheated with pro longed laser use and could
cause a burn (28).
Electrosurgery Unit Electrosurgery (radio frequency) apparatus is so widely used that there is of ten
complacency about reading the instruct ion manual or following safe pract ices
(29,30). Electrosurgery units are the mos t common igni tion source in surgica l f i res
(6). The instruction manua l should be s tudied at the beginning of a tra ining program
and reviewed periodica lly. A brief set of operat ing instruc tions should be readi ly
availab le on the instrument (31).
Terminology The vocabulary concerning electrosurgery is somewhat confusing (32). This chapter
wi l l def ine e lec trosurgery devices as those that employ a h igh-f requency (radio
f requency) electric current passing through t issues to cut, coagulate, or prov ide a
blend of cutting and coagu lat ion. Elec trocautery ut i l izes a heated wire or blade,

usual ly at the end of a probe fo r coagulation . Most elec trocautery devices are
battery-opera ted.
Physics There are three modes avai lable on modern electrosurgery devices .
Cutting Mode The cutt ing mode uses a continuous s ine wave. Heating is rap id and produces h igh
temperatures that explode cel ls that come in contact wi th the electrode. This
produces a cut in the tissue.
Coagulation Mode The coagu lat ion mode features short bursts of a dampened s ine wave. Less heat is
produced s ince the current is not cont inuous. Tissue desiccat ion occurs , and the
ends of blood vessels are thermally sealed .
Blend Mode The blend (cut-coagulation) mode employs a waveform and voltage between tha t of
the cutting and coagu la tion cycle . The rela tive amount of cutting or coagulat ion
depends on the lengths of the bursts of voltage. Severa l blend se tt ings may be
availab le on an elec trosurgical uni t (33).
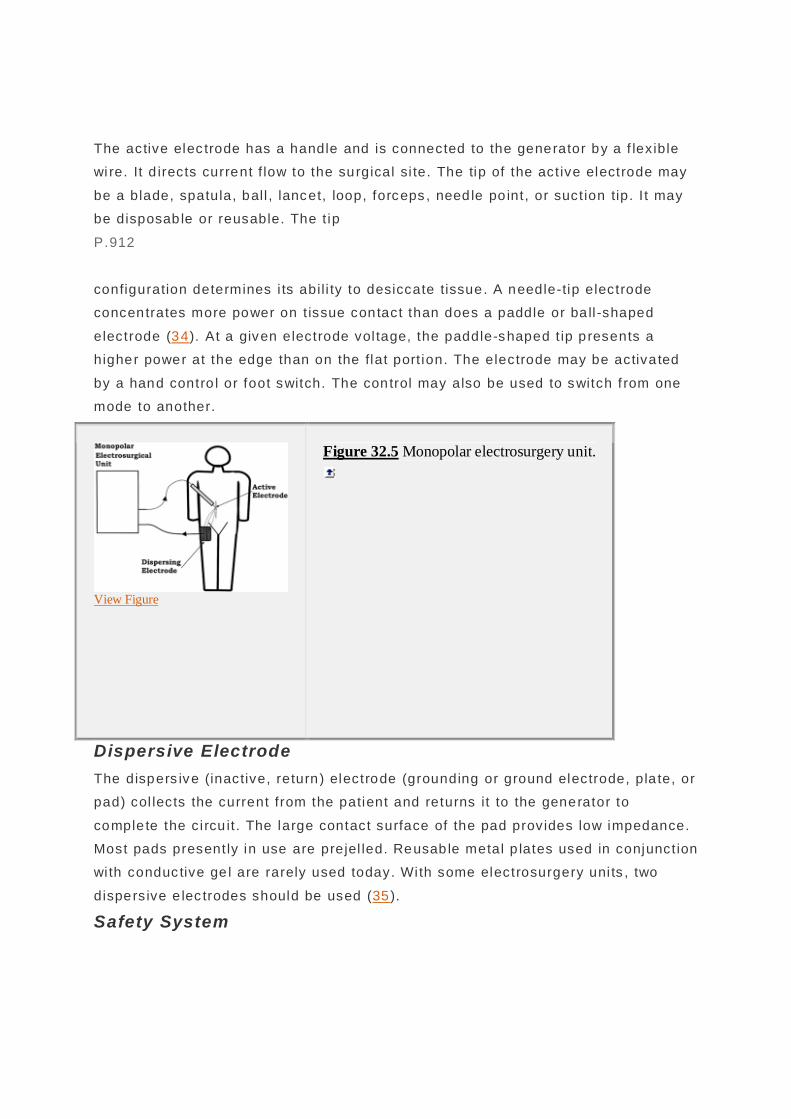
Types Monopolar With monopolar (unipolar) electrosurgery un its , e lectrons f low f rom the genera tor to
the act ive electrode and through the patient to the dispers ive (return , inact ive)
electrode, sometimes incorrect ly called the grounding pad (Fig. 32.5). The curren t
disperses from high densi ty at the tip of the act ive electrode to a lower dens ity v ia
the lowest impedance pathway tha t it can f ind .
Generator The elec trically powered generator (power uni t) c rea tes a radio frequency current
that passes through the active electrode. The effect on tissue depends on the
current intensi ty, the type of current employed, the durat ion of exposure to the
current, the hand piece used, and the dispers ive electrode (34). Coagulat ion
requires longer contact wi th the probe than cutt ing. As electrica l energy is appl ied
to the t issue, char forms. Since char has h igher impedance, more current d iss ipates
di rectly to the dispers ive elec trode and the ef fect is reduced (34).
Active Electrode
The active elec trode has a handle and is connected to the generator by a f lex ible
wi re. It d irects current f low to the surgical si te. The tip of the act ive electrode may
be a blade, spatula, ball , lancet, loop, forceps , need le po int, or suct ion tip. I t may
be disposab le or reusable. The t ip
P.912
configuration determines i ts abil i ty to desiccate tissue. A needle-tip electrode
concentrates more power on t issue contact than does a paddle or ba ll -shaped
electrode (34). At a given electrode vol tage, the paddle-shaped t ip p resents a
higher power at the edge than on the flat port ion. The electrode may be activa ted
by a hand contro l or foot switch. The control may also be used to switch f rom one
mode to another.
View Figure
Figure 32.5 Monopolar electrosurgery unit.
Dispersive Electrode The dispers ive (inactive, return) electrode (grounding or ground electrode, pla te, or
pad) col lects the current from the patient and returns it to the generator to
comple te the c i rcu it . The large contact surface of the pad provides low impedance.
Most pads present ly in use are prejel led. Reusab le metal p lates used in conjunct ion
wi th conduc tive ge l are rarely used today. With some electrosurgery uni ts , two
dispers ive e lec trodes should be used (35).
Safety System

Modern electrosurgical uni ts possess a return e lec trode (contac t quali ty) moni to ring
system. This ensures tha t the patient is connec ted to the return e lec trode (34,36).
Current f lowing to the ac tive electrode is measured and compared with current
returning f rom the d ispers ive electrode. If the curren ts are not ba lanced, the uni t is
deactivated. A more recent innovation is active electrode monitoring (AEM)
(37,38,39,40). This continuously moni tors the electrical c ircui t and automatically
shuts down the generator and sounds an ala rm if dangerous e lectrical leakage
occurs. Newer generators can sense dramatic changes in t issue impedance or
temperature changes at the return electrode (33,41). Some modern electrosurgery
machines are equipped wi th “spl i t pads” (42). The uni t wi l l not func tion unless both
halves of the pad are in contact wi th the patient.
Bipolar The bipo lar electrosurgery unit is composed o f a generator and two electrodes
located wi th in mill imeters of each other. The energy f low is be tween the two
electrodes , and no current f lows through the patient 's body. This al lows the energy
to be local ized more precise ly. The current densi ty in the t issues surrounding the
ac tive electrode is substant ially less than that for monopolar elec trodes, and
deeper t issue layers are preserved wi th lower vol tage and power requirements. This
type of e lec trosurgery un it can coagulate even when the tip is immersed in b lood.
Bipolar units cannot be used fo r cutting .
Bipolar elec trodes are produced in a variety o f conf igurat ions: hooks , spatulas ,
sc issors, forceps , and needles (29 ,43). Of ten, these devices are batte ry-opera ted.
There are reports that the ON-OFF swi tch on one of these dev ices did not always
deactivate the dev ice when it was set aside (44 ,45). The hot t ip could then set
drapes on f i re. At least one device could be act ivated by another device's wire less
remote-control uni t or by f luorescent room l ights (46).
Hazards Associated with Electrosurgery Mishaps with the elec trosurgery uni t of ten involve faul ty re turn electrodes, improper
electrode placement, or al te rnate low-impedance outlets. Insuff ic ient contact wi th
the dispersive pad can resul t in pa tient burns and/or burns to others who are in
contact wi th the pat ient. Among the low-impedance al te rnatives are
electrocardiogram (ECG) monitoring elec trodes, temperature probes, urinary
ca theters, metall ic parts of surgica l tables, heating pads, and oximeters (47).
About 68% of reported surgical f i res involve e lectrosurgical equ ipment (48). Fires
associated wi th the electrosurgery unit are of ten associated with an oxidizer-

enriched atmosphere. When the electrosurgery uni t is used, heat vaporizes t issue
or expels tissue embers from the t ip. In room air, t issue vapors do not igni te, and
embers are quick ly extinguished. In an oxidizer-enriched atmosphere, the vapors
can ignite into a brief f lame, and embers can fly several inches and burn unt i l they
are consumed. A f la re of evolved gases can d irectly ignite any convenient fuel . The
electrical wires associa ted wi th the electrosurgery electrode may develop a short
c i rcui t, wh ich could resul t in a f ire (49).
During laparoscopic surgery, burns that are sometimes fatal can occur ou tside the
surgeon's v iew when using an elec trosurgery uni t (14,29,33,38,40,50,51,52). These
are usua lly caused by insu lat ion fai lure, di rect coupling, or capacit ive coup ling.
I f a defect occurs in the active electrode's insulation , current can f low through the
defec t. Defec ts can resul t f rom improper handling or damage to both reusable and
disposable electrodes . A number of devices are avai lable to detect insula tion
defec ts (33,40,51). Act ive electrode monitoring cont inuously monitors the elec trical
c i rcui t and automatical ly shuts down the generator and sounds an alarm if
dangerous elec trical leakage occurs (37,38,39,40).
Capaci ta tive coupling occurs when the electrosurgical current induces s tray
currents on other nearby conductors . It can occur even through intact insulat ion . It
occurs as a result of the active e lectrode contacting or coming into very c lose
proximity to a non-insula ted metal ins trument (such as a laparoscope) in the
surgical field. If the electrical ly-energized laparoscope has been placed through a
metal cannula, the current wi l l s imply f low to the pat ient's abdominal wal l . However,
i f the laparoscope has been placed th rough a nonconduct ive cannu la, the current
cannot f low to the abdomina l wal l. In th is case, any piece of bowel o r other internal
t issue touch ing the laparoscope can be burned. Capaci tative coupling is always
present and cannot be to tal ly eliminated.
Argon Beam Coagulator The argon beam (enhanced) coagulator (ABC) is solely a coagu la ting instrument.
Rad io f requency monopo lar curren t is delivered through a f low of ionized argon
gas.
P.913
The f low is al te red as the power is changed. The t ip does not touch the tissue. I f
the tip is greater than 1 cm from the t issue surface, only a gent le s tream of argon
wi l l f low. When the tip is 1 cm or less f rom the tissue surface, the ac tive mode
occurs. If the nozzle t ip glows red, the tip is too close to the t issue or the power
se tt ing is too high.
Fiber-optic Illumination System A f iber-optic i l luminat ion system consis ts of a l ight source and l ight-transmitting
cable . The cable is connected to an endoscope or headligh t. The term cold l ight ,
used to describe l ight f rom a f iber-opt ic source, is incorrec tly assumed by many to
mean that heat is not generated. Actual ly co ld l ight refers to l ight in which the
amount of inf ra red radiat ion has been reduced (53). These light sources can
provide several hundred watts of v is ible, infra red, and ul trav iolet light. Al though
some of these wavelengths can be f i l tered out, the power is typical ly focused into a
f iber-opt ic cable of smal l d iameter tha t can deliver a h igh-power densi ty .
A number of f ires have been igni ted when the unprotected end of the f iber-optic
cable was allowed to res t on a drape (6 ,49 ,53,54,55,56,57). The cable end can
reta in a signi ficant amount of heat a fter be ing d isconnected from the l ight source.
Defibrillator When a def ibri l la tor is act ivated, a spark may be generated if insuff icient force is
applied to the paddles; if the paddle pad is too smal l; if paddles are applied over an
i rregular surface or bony prominence or near an ECG electrode; when insuff ic ient,
excess or the wrong kind of gel is used; or if there is another conductive medium
between the paddles (6 ,58 ,59). I f disposable def ibri l la tion pads are used to
increase e lec trical conduction between the paddle and the patien t, an arc can occur
i f the surface of the paddle is not comple tely on the pad, if the pad is smal ler than
the padd le, if there is a fold in the pad, o r if the pad is dry.
Pressure Regulators When gas is al lowed to f low f rom a high-pressure to a low-pressure chamber,
recompression can cause a rap id rise in temperature. Materials that cannot
wi thstand both 100% oxygen and high temperatures wil l igni te . This hazard is
associated mostly with aluminum oxygen regula tors (60,61,62,63,64,65,66,67,68).
Another cause of heat in a pressure regu la tor is part ic le impact f rom contaminants.
Tef lon tape, chips f rom seal materials , or hydrocarbon contaminants may be
present (69).
Surgical Lights Surgical l ights can be a source of igni tion. I f the light does not have the proper
mechanism to diss ipa te inf rared radia tion or i f that mechanism fails , the patient o r
personnel envi ronment can be exposed to energy levels high enough to cause
burns or f i res (70,71). The heat f rom a surgical l ight can contac t and rupture a hose
f rom the medical gas pipel ine system (72).
Electrical Faults An electrica l f i re can occur in any env ironment where there is electrical equipment.
A short c i rcui t can occur in an anesthesia mach ine (73,74,75). In one reported
case, a short circu it in a laryngoscope wi th a rechargeable handle caused f lames to
shoot f rom the charging end of the handle (76). Elec trical arc ing in surg ical booms
has been reported to cause fi res (77,78).
Other Ignit ion Sources Other reported sources of ignit ion in opera ting room f i res include resectoscopes,
heat lamps, heated probes , pneumatic tourniquets, denta l and orthopedic burs and
dril ls , heated-wire breath ing tubes, and humid if ie rs (1,79,80,81,82,83,84).
Fuels Fuels abound in the operating room. A fuel is anything that can burn, inc luding
most things tha t come in contact with pat ients as we ll as the patients themselves.
Tracheal Tubes The risk and characteris t ics of a tracheal tube f ire wil l depend on the type of tube
used. In most cases , igni tion requires the tube to be penetra ted (85). The f ire
begins on the ins ide rim of the penetrat ion area and then spreads both wi th and
against the flow of ox id iz ing gas.
Polyvinyl Chloride Tubes Polyv inyl ch loride (PVC) tubes are combus tible in an ox idizer-enriched atmosphere
wi th a carbon d ioxide (CO2) laser. Once igni ted and penetrated, a PVC tube can
susta in a torchlike f lame. PVC tubes wi thout markings are re lat ively res is tant to the
Nd-YAG laser, but mark ings inc rease the risk (86). I f there is blood, mucus , or
sa liva on the tube, the risk of f i re is inc reased. The inju ries associated wi th PVC
tube f i res are more severe than wi th other types of tubes (87,88).
Red Rubber Tubes Red rubber tubes are combus tible with the CO2 , potassium t itanyl phosphate (KTP),
and Nd-YAG lasers (86,87,88,89,90). A major p rob lem is the inabil ity to see
through the tube. Should an intraluminal f i re develop, it may go undetec ted for a
longer period of time than with other tubes .
Damage to the tracheobronchial tree af te r an in traluminal f ire may be less severe
wi th a red rubber tube than a PVC tube (87). Red rubber tubes are less l ikely to
soften, deform, or fragment if ignited than are o ther tubes. Another advantage is
that they can be quickly
P.914
removed f rom the pat ient (91). The high pressure in the cuff causes it to def late
more quickly than is possible with a low-pressure cuff .
Silicone Tubes A sil icone tube is more resistant to penetration by a CO2 laser than other tubes
(87). If ign ited, a s i l icone tube rapidly becomes a bri tt le ash tha t crumbles eas ily
and may be aspira ted , ra is ing the possibil i ty of future problems with s il icosis
(87,90,92,93). However, the acute injuries are less severe than with red rubber and
PVC tubes (88).
Laser-resistant Tubes A number of ready-to-use laser-resistant tubes and tube wraps are avai lable and
are desc ribed in Chapter 19. They should meet the requirements of Inte rnational
Standards Organ ization (ISO) 14408 (93). It is importan t to remember tha t laser-
resistant does not mean laser-proof . Laser-resistant tubes can igni te, especial ly i f
manufac turer's warnings, precautions, or directions fo r use are not followed. If a
laser tube is used with a laser other than that for wh ich i t was designed or a
f lammable part such as the cuf f is exposed, it wi l l catch f ire (92 ,94). Laser-resistan t
tubes are usually not res is tan t to other heat sources such as an electrocautery
penci l.
Supraglottic Airway Devices The relative resistance o f suprag lott ic ai rway dev ices depends on their
composi tion . Those devices tha t are made of s i licone rubber such as the LMA-
Classic, LMA-Flexible , and LMA-ProSeal are s ign if icant ly more resis tant to the CO2
laser than are PVC tracheal tubes (95). Many disposable supraglottic dev ices are
made of PVC and are probably as suscept ible to fi res as tracheal tubes of the same
composi tion .
Surgical Products Surgical drapes, towe ls , and dressings are common fue ls for opera ting room f i res .
Of ten , the drape is igni ted f rom another f ire (24). Whi le many drapes are resis tan t
to ignit ion in room a ir, the oxidizer-enriched a tmosphere that is often present may
cause them to burn with v igor (49,96,97,98,99,100,101,102,103,104).
Disposable drapes may be part icularly diff icul t to deal wi th during a f i re because
they are water repellen t. Addi tion of water may even spread the f lame. Laser-
resistant drapes are avai lab le . Some synthetic drapes wi l l mel t away f rom the laser
rather than igni te (103).
There are numerous reports of surgical sponges, gauze pads, and swabs being
igni ted (49,105,106,107,108,109,110,111,112,113). Wet sponges may be used to
protect a tracheal tube from a laser beam. However, if they are allowed to dry out,
they become f lammable.
Adhesive Substances Adhesive tape can be the fuel for a fi re (114). Co llodion and benzo in are
f lammable .
Skin Preparatory Solutions Flammable volat i le organic so lut ions are often used to prepare the sk in prior to
surgery. If the l iqu id or vapor is contacted by an igni tion source , a flame can resu lt
(1,101,115,116,117,118,119,120,121). Alcohol-based solut ions are espec ia lly
f lammable . They can also in fi l t rate and pool under the drapes. When this happens,
they are slow to dissipate. Alcohol-based f ires have a f lame tha t is d if f icult to see.
Of ten , the result of the f lame is the f i rs t thing not iced.
Intestinal Gases Gases that accumulate in the bowel (especial ly hydrogen, hydrogen sulf ide , and
methane) can be the fuel for a fi re o r exp los ion if an elec trosurgery uni t is used to
open the bowel (105). Proper bowel preparation may prevent this (122). Suff ic ient
oxygen to support combustion is normally not present in intestina l gas . However,
ni trous oxide may diffuse into the intest inal lumen, c reating a f lammable mixture.
Oxygen Cannulas Oxygen cannulas are made of plas tic that can burn . They carry 100% oxygen. If
touched by a hot e lec trosurgery probe or a laser beam, they burn readily. Even if
not di rec tly contac ted, the area around them may be so oxygen-rich that a smal l
spark can turn in to a burning ember tha t can igni te the cannula.
Lubricants and Ointments
Petro leum-based ointments that are used in an oxidizer-enriched a tmosphere wi l l
igni te when enough heat is present to cause vaporizat ion (105,123,124). Water-
based lubricants wi l l not burn and can be used to coat ha ir to make i t f i re -resistant.
Body Hair Body hair, including eyelashes, moustaches, and beards can be involved in a f i re
(105,106,125,126). Coating the hair with a water-based lubricant wil l decrease the
risk .
Surface flame propagation occurs where there are fine surface f ibers of fabric o r
body hair (127). In the presence of an ox id izer, these f ine f ibers can be igni ted.
Of ten , the skin or underlying fabric is not burned. The surface f i re races in the
di rection of the oxygen source, where the oxygen supply tubing may be ignited
(58).
Other Combustible Substances A number of artic les used in or near the patient can serve as the f lammable
material . These include (but are not l imited to ) oxygen tubings, endoscopes, smoke
evacuator hoses, esophageal s te thoscopes, breath ing tubes, reservoir bags, eye
patches, s ten ts , masks, nasogastric tubes, en teric feeding tubes, rubber and plas tic
nasopharyngea l ai rways, covers, paper products, blood pressure cuffs , aeroso l
adhesives, tourniquets, gloves, s tethoscope tubing , th roat packs, eggcrate foam
P.915
mattresses, bandages, stockinettes, d ressings, pil lows, glue, gowns, straps, caps
and hoods , rubber elec trosurgica l uni t probe sheaths, shoe covers, loca l anesthetic
spray, and organic gas f rom a necro tic tumor
(106,116,128,129,130,131,132,133,134,135,136,137).
Alcohol-based hand sani tizers (gels, foams, and liqu ids ) are h ighly f lammable
(138). They shou ld be stored in a cabinet that is designed fo r flammable materials .
However, a study pub lished in 2003 found no fi res attribu tab le to hand sanit izers,
and the National Fire Protec tion Associat ion now a llows alcohol-based hand
sanit izer d ispensers in corridors and other public a reas, provided certain
restric t ions are observed (139). I f a dispenser is mounted in a hallway, the corridor
must be at leas t 6 fee t wide. The dispenser can project up to 6 inches f rom the wal l
and mus t be instal led above handrai l height.
Oxidizers
With an oxidizer-enriched atmosphere , a f i re igni tes easier, burns more v igorously,
spreads more rapidly, and is more d if f icu lt to extinguish . The oxidizers of g reates t
inte res t are oxygen and ni trous oxide. Ni trous oxide supports combustion and in the
process releases the energy of i ts formation, providing increased heat. Thus , any
mixture of oxygen and ni trous oxide wil l support combustion. Air wi l l a lso support
combustion, because it contains oxygen.
Because oxygen is heavier than ai r, i t collec ts in low-lying areas, inc lud ing drape
folds. Some materia ls such as drapes and towels absorb oxygen and reta in i t fo r
some t ime (1,127). Tenting drapes wi l l al low oxygen to dra in off toward the f loor
and be d iluted by ai r c i rculation.
Common Scenarios
Airway Fires During airway surgery, all of the th ree necessary components are in close
proximity: a combus tible subs tance (trachea l tube, gauze, etc.), an igni t ion source
(laser or e lectrosurgery apparatus), and gas to support combustion (oxygen wi th or
wi thout ni trous oxide). An ai rway f i re is part icularly serious because a considerab le
amount of heat is genera ted in a smal l area, and the smoke and gases f rom such
f ires can be b lown deep in to the pat ient's lungs .
Using Electrosurgery during Tracheostomy Many a irway f i res have occurred while using the electrosurgery uni t during
tracheos tomy
(9,105,128,130,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154).
Of ten , the patien t is being given 100% oxygen in ant ic ipa tion of interrupted
venti lation and/or because of the underly ing c linical cond ition. If the tracheal tube
or cuff is contacted, an oxidizer wi l l be released. Current ly , there is no tracheal
tube that is safe for use wi th electrosurgical devices or electrocautery, al though
some are more resistant to igni tion than others (155).
Using Electrosurgery in the Mouth Using electrosurgery in the oral cavi ty may resul t in a f i re
(6,156,157,158,159,160,161,162). The tracheal tube is of ten the fuel , but o ther
i tems such as sponges or patient t issue may be involved. Of ten, wet gauze is used
in the throat to catch sec ret ions or to pro tect the tracheal tube. If there is a leak
around the tube, the gauze can becomes oxidizer-enriched and dry ou t more
quick ly.
Laser-induced Tracheal Tube Fires The l ikelihood that a laser wil l contact the tracheal tube during ai rway procedures
is high (163). Cuffed tubes are more l ikely to be contacted than noncuffed tubes.
The tube may be exposed to ei ther the di rec t or ref lec ted laser beam. Flaming
t issue in c lose proximity to the tube may cause it to ignite (164).
In addi tion to local damage in the larynx, injury can occur to the lower a irway and
the parenchymal t issue in the lung. The products of combustion may be b lown into
the lungs.
The cuff is the most vulnerable part of the tracheal tube. It cannot be wrapped, and
laser-resistan t tubes do not have laser-res is tan t cuffs .
Wet cotton sponges are of ten used around the tube to protect the cuff f rom the
laser beam. If these dry out, they can become fuel for a f ire (165). Tape that is
used to secure the tube can igni te.
During lower ai rway surgery using a laser, the cable may be passed through the
inside of a tracheal tube. The tracheal tube should be placed just below the vocal
cords so that the t ip is as fa r away f rom the operat ive s ite as possible.
Other Head and Neck Fires Head and neck f i res can occur during local anesthes ia procedures when
electrosurgery apparatus is used (6,49,56,126,166,167,168,169,170,171,172,173).
Of ten , oxygen is being administe red, and i t may diffuse into the surg ical area. Any
f lammable i tem in the v ic ini ty can catch f ire.
Fires Involving Pressure Regulators While no t a frequent occurrence, a f ire in a regulator can be d isastrous (174).
These fi res may resul t f rom adiabat ic compress ion or partic le ignit ion in which
debris is b lown f rom the cyl inder into the regulator wi th suffic ient energy to cause
igni tion. Improper pressure regulator assembly may also cause a f i re.
P.916
Regula tors wi th aluminum components are more l ike ly to burn than other
regulators . The Food and Drug Adminis trat ion (FDA) and the National Ins ti tute for
Occupational Safe ty and Heal th (NIOSH) now recommend that aluminum regulators
be replaced wi th ones wi th brass components (64,66). A number of aluminum
oxygen regulators have been recalled (67).
Intraperitoneal Fires Severa l explosions have been reported during laparoscopy when nitrous oxide was
used as the insuff lating gas (122,175,176,177). Ni trous oxide in the inspired gases
wi l l dif fuse into the peritoneal cavi ty and may reach a high enough concentrat ion to
support combustion (178,179). Fires have also resul ted f rom inf lat ing the peri tonea l
cavity wi th an oxygen-CO2 mixture instead of pure CO2 (180,181). The Pin Index
Safety System (Chapter 1) wi l l not p revent this error, because the index ho les for
tanks wi th 100% CO2 are the same as for any tank wi th greater than 7% CO2 .
Fires during Defibrillation Oxygen is always used during resusci tation, and the source is of ten disconnected
and p laced near the head (58,182,183). This may allow oxygen to f low over the
defibri l la tion electrodes (184). A spark caused by placement of the def ibri l lato r
paddle or electrode close to an ECG elec trode or poor contact be tween the
patient 's sk in and the def ibri l lator paddle or electrode may ignite hair or other
combustible materials in the area (183,185).
Fires in Canisters Fires in CO2 absorbent canisters have been reported
(186,187,188,189,190,191,192,193). These are d iscussed in more detail in Chapter
9.
Personnel Risks
Smoke Hazards Potent ial ly hazardous ai rborne contaminants are formed from tissue vaporization
when a laser is used. These by-products have the potent ial to be mutagenic,
carc inogenic, teratogenic, or a vector for v iral infect ion (10,194). Elec trosurgery
devices and bone saws also produce vaporized f ragments that have the same
hazards (25).
Inhaling potent ia lly hazardous ai rborne contaminants can be kept to a minimum by
scavenging the smoke. This wi l l help to give the surgeon a c learer v iew o f the
surgical field and removes o ffensive and irrita ting odors. Various smoke evacuators
are avai lable (103,195). To be most effect ive, the evacuator nozzle should be
posit ioned as c lose as possible to the operative f ie ld and be func tiona l before,
during and for 30 seconds after t issue is vaporized (196).
Personnel masks should be removed and discarded as soon as poss ib le af te r use
(196). Standard surgical masks f i l ter ou t partic les down to about 3 microns in
diameter. The laser plume has partic les as small as 0.31 microns . High-eff ic iency
masks can f il te r partic les down to 0.30 mic rons, bu t they are dif f icul t to breathe
through and lose their eff iciency when wet (10,103).
Ocular Injuries The laser beam may be di rected over some distance. The area of hazard may not
be l imi ted to the immediate surgical area and may present risk to operating room
personnel (25). The surgeon is not highly susceptible to injury because of the
safety dev ices bui lt into the ins trument. However, if the ins trument is accidental ly
ac tivated, he is exposed to the same hazards as other personnel .
The eye is especially vulnerable to injury. Because CO2 laser beams are absorbed
wi th in the fi rs t 200 µm of t issue, they are a hazard to the cornea (197). Argon, KTP,
and Nd-YAG lasers are more like ly to cause damage to the retina . The ex tent of
damage wil l depend on wh ich part of the retina is affected. Permanent v isual loss
may resul t (25).
All personnel in the area where a laser is used should wear appropriate protect ive
eyewear. This may inc lude goggles, face shields, spectacles , or presc ription
eyewear using special materials or reflec tive coatings (or a combination of both),
se lec ted to reduce the potent ial ocular exposure. The safety eyewear should be
marked according to the wavelength (laser type) (Fig. 32.6). I t should be noted that
laser safety eyewear is not des igned fo r looking di rectly at a laser beam (16). The
patient 's eyes should be c losed and covered wi th saline-soaked gauze or a
nonshiny metal shield . Awake patients should wear goggles specif ic for the laser
being used. Windows in the room should be covered and a warning sign placed
P.917
on the operat ing room door at eye level (Fig. 32.4). Spare eyeware should be
availab le at a ll entrances.
View Figure
Figure 32.6 All laser-protective eyewear should be clearly and permanently labeled.
Electrical Shock Another concern is electrical shock from the e lec trosurgery device. A common
pract ice among surgeons is to al low an assistant to touch the dista l end of a
forceps wi th the act ive electrode f rom the electrosurgery apparatus. This act ion
makes the forceps the active electrode. A glove may not offer suffic ient p rotec tion
f rom the electrical c ircui t . Holes appear in as many as 15% of g loves.
There are ways to minimize the shock potential wh ile using electrosurgery. The
ac tive electrode should be f irmly in contact wi th the forceps before i t is energized.
The person holding the forceps should try to contact i t in as large an area as
possible to spread the concentration of the charge.
Fire Prevention The best way to deal with fi res is to prevent them f rom start ing (127,198). Fi res can
be avoided by not allowing the th ree elements of the f ire tr iangle to come together
at the same t ime.
Controlling Ignition Sources One way to reduce f ires is to properly use equipment that might ac t as an igni tion
source. I t is important to read instruct ion manuals and to alter techniques to f i t
these instructions.
Lasers
Personnel who use lasers should take a cert if ied laser course (6,23,26,103). They
should practice their techn ique on inanimate ob jec ts and gain experience a t the
hands of an experienced c linic ian. Specif ic personnel should be designated to
moni tor and prevent laser hazards.
A laser protocol should be developed and fo llowed. Lasers should be test f ired onto
a safe surface before use to ensure tha t the beams are properly al igned. Lasers
should always be kept in the standby mode except when needed. The lowest power
densi ty and shortest pu lse dura tion that wi l l do the job should be used. The laser
should be activated only when the tip is under the surgeon's d irect v is ion. The laser
should be placed in standby mode before removing i t f rom the surg ical s i te.
Laser f ibers should not be c lipped to drapes because the f ibers may be broken. The
laser fiber should be careful ly passed through an endoscope before in troducing the
scope into the pat ient to minimize the risk of f iber damage. The f iber's funct ionali ty
should be verif ied before insert ing the endoscope into the pat ient.
I f a laser contact t ip is used, the t ip wil l remain hot for several seconds. Bl ind entry
into cavi ties wi th this tip should be avoided (199). The risk of tracheal tube igni tion
wi l l be lowered if the laser is activated during the expiratory pause (200).
Electrosurgery Unit The elec trosurgery uni t should not be used during tracheostomy
(31,34,50,111,171,201,202,203,204). Bleeding should not be trea ted wi th
electrosurgery af ter f lammable dressings have been appl ied.
A bipolar electrosurgery uni t should be used whenever possible . This wi l l reduce
the curren t densi ty in the t issues surrounding the ac tive electrode and minimize the
potential for di rect coupl ing. Bipolar units work at lower voltages and are not
associated wi th insulation fai lure .
Monopolar un its should have a means to moni tor the return electrode or ac tive
electrode. Us ing active e lec trode monitoring wi l l min imize the risk of s tray
electrosurgical burns (38). Before each use, the electrosurgery uni t and assoc ia ted
safety features should be inspected for s igns of damage and tested to ensure that
the uni t is functioning correct ly. If i t is not work ing properly or is damaged, the
electrosurgical apparatus should be immediately removed f rom serv ice. The uni t
should be pro tec ted f rom sp il ls . Unintentional act ivation may occur i f f lu ids enter
the generator. The alarm system should be checked prior to applying the dispers ive
electrode. The act ive electrode should have a t ip that is secure, because a loose
t ip may cause a spark. Prejel led dispers ive electrode pads should be checked for

uniform gel dis tr ibution and absence of exposed wires before being applied to the
patient. Outdated or previously opened but unused dispers ive e lectrode pads
should not be used, because the gel can undergo electrolys is and/or desicca tion. If
a dispers ive elec trode pad requiring gel is used, the pad shou ld be checked
careful ly to identify any dry spots on i ts surface before it is placed on the patient.
Af ter the patient has been posi tioned, the connect ion between the pat ient and the
unit should be establ ished by p lac ing the dispers ive electrode on a nonhairy a rea of
c lean, dry sk in. The dispers ive electrode should be the appropria te s ize for a
patient ( i.e. , neonate, infant, ped iatric , adult) and never be cu t to reduce its size.
The dispers ive electrode should be app lied to c lean, dry skin over a large, wel l-
perfused muscle mass as c lose to the operative s i te as practica l, avoiding bony
prominences, scar t issue, skin over a metal prosthesis, o r dis tal to a tourniquet.
Excessive hair shou ld be removed before apply ing the dispers ive e lec trode,
because hair wil l insu late the pad from the patient. The pad's ent ire surface area
should main tain uniform body contact. There should not be any ten ting, gaping, o r
moisture under the pad. This wil l interfere with adhesion to the sk in and decrease
the contac t surface. The dispers ive electrode
P.918
should not be moved to another s i te a fter ini tial appl ication. The status of the
dispers ive e lec trode should be checked if any tension is applied to the cord or i f
the pat ient is reposi tioned after the pad is appl ied. A used dispers ive electrode
should not be reapp lied.
Electrocardiographic electrodes should be placed as far as possible from the
operative si te to minimize the alternate f low o f current through the electrodes and
moni tor to g round.
I f insulated electrosurgical elec trode probes are required, only commercial ly
availab le insulated probes should be used (9). Insulating s leeves cut f rom catheters
or o ther materials shou ld no t be used to sheathe probes.
The lowes t power settings tha t are effective for the surgical procedure , as
determined by the surgeon in conjunc tion wi th the manufacturer's recommendation,
should be used. The ent i re ci rcui t should be checked if the operator requests higher
power sett ings because of ineffectual results .
The elec trosurgery uni t should be act ivated only when the tip is under the
surgeon's direc t v ision and only by the person using i t . Cords shou ld no t be
c lamped with or wound around any objec ts . The electrosurgery probe should be
kept c lean to minimize the risk of adherent t issue incandescing or f laming. The
electrosurgical penc il should be placed in a holster when i t is not in act ive use. The
electrosurgical uni t should be placed in s tandby mode whenever i t is no t in active
use. Unnecessary foo t swi tches should be removed so that they are not
accidentally ac tivated .
During laparoscopic surgery, all-metal or a ll-p lastic cannulas should be used and
not a hybrid cannula system (i.e. , a combination of plastic and metal cannulas )
(37). Electrosurgery elec trodes should not be used ins ide metal suct ion i rrigators.
The elec trosurgica l uni t should be deac tivated before removing it f rom the surgical
s i te. Even after deact ivation , the probe t ip may retain enough heat for a few
seconds to mel t plast ics or igni te some fuels, so it shou ld be placed ins ide a c lean,
wel l -insulated holder or broken off . In addi tion to protecting the t ip, this makes i t
more dif f icult to acc identally ac tivate the switch . The t ip should be broken, and a
safety cover should be placed over the tip and act ivation swi tch before the device
is discarded (205).
Argon-enhanced Coagulation All safety measures observed for the electrosurgical unit shou ld be observed for
argon-enhanced coagulation (31). The electrode should not be placed in di rect
contact wi th t issue. The hand piece should be moved away f rom the pat ient's t issue
af te r each activation. The argon gas f low and the argon coagu lator should be
ac tivated simul taneously. The argon gas l ine should be purged of ai r before each
procedure and by act ivat ing the system after moderate delays between act ivat ions.
Fiber-optic Light Sources All connec tions should be made before the l ight source is activated, because the
end of the cable can cause a f i re (53). An act ive f iber-optic cable should not be
placed on flammable material . The l ight source shou ld be turned OFF before
disconnecting the cab le. The end of a f iber-optic cable can retain a signif icant
amount of heat after be ing disconnected from the l ight source (206). Therefore, i t is
importan t to be careful where one places the end of a f iber-op tic cord.
Heated Humidifiers Only a breath ing tube and heat ing ci rcu it labeled for use with a spec if ic humid if ier
should be used (207). Heated breathing c i rcui ts should not be covered wi th sheets,
blankets, towels, clothing, o r other material. They should not rest on surfaces such
as the patient, operat ing table, blankets, o r medical equipment. Instead, a boom
arm or tube tree shou ld be used to support them. A heated-wire breathing ci rcui t
should not be turned ON before f low has been ini tiated. I f there is no f low (as
during cardiopulmonary bypass ), the heater should be turned OFF (208).
Defibrillators When us ing a defibri l lato r, care should be taken to hold the paddles f i rmly and
posit ion them properly. Disposable conduc tive pads should be larger than the meta l
surface of the paddle and be wi thin their expiration date. This wil l prevent arc ing
when the paddles are activa ted (58). ECG electrodes should be appl ied as far as
possible f rom the def ibri l lat ion pads.
Electrical Faults All electrica l cords should be regularly inspec ted for cuts and nicks in the
insulat ion, f rayed insulat ion, and loose connections at the plug or receptac le ends
(209). Al l plugs should be pushed completely in to the receptacles to prevent p rong-
to-prong arc ing (210).
Managing Fuels Tracheal Tubes
Non-intubation Techniques Since the tracheal tube is of ten the fuel for the f i re , anes thetic techn iques that do
not require a tracheal tube wi l l el iminate one component of the f i re triad (92).
These inc lude apnea, jet vent i lat ion, and spontaneous breathing.
Apnea With the apneic technique, the pat ient is vent i lated by us ing a mask or tracheal
tube, and these are withdrawn as the laser is used (92,93,211). Af ter a period of
t ime, vent i lat ion is reinstated. This is repeated as long as needed to perform the
surgery.
Insufflation Patients may be al lowed to spontaneously breathe a combinat ion of oxygen and
anesthet ic agents whi le laser procedures are undertaken. The gases are
administered through a catheter or hook in the
P.919
corner of the mouth tha t is wel l out of the way of the laser beam. The suc tion
channe l of a laryngoscope may be used to insuff late oxygen. Operat ing room
pollut ion wi th anesthet ic agents may be high wi th this technique. Oxidizers should
be used as sparingly as possible s ince the insuff lated gas cou ld support
combustion.
Jet Ventilation Jet vent i la tion techniques ei ther v ia a metal bronchoscope or a catheter inserted
through the crico thyroid membrane may be used (212). A h igh-veloci ty jet of oxygen
or helium and oxygen can be di rec ted into the ai rway above or below the glo tt is by
us ing various apparatus (21,92,93,196,213,214).
There has been a f i re reported with th is technique (215). An errant laser strike
igni ted the surgeon's glove. The resul tan t burning vapors were entra ined into the
patient 's airway. The patient's mustache was also igni ted , and the pat ient suffered
fac ial burns .
Filling the Cuff with Saline The cuff is the most vulnerable part of the tracheal tube, regardless of the tube or
cuff materia l. If a laser beam penetrates an ai r-f i l led cuff , gas can leak in to the
operative field, and if the oxygen concentrat ion is high, the risk of f i re is great.
Fluid in a cuf f ac ts as a heat s ink and makes the cuff less easy to perforate
(216,217). Fi l ling the tracheal tube cuff wi th a l idocaine jelly-plus -saline mixture no t
only prevents the cuff f rom being igni ted but may plug small holes in the cuff
resul ting f rom a laser h it (218).
I f the cuff is perfora ted, a je t of f lu id may ex tingu ish the f ire. If perfo rated, fluid-
f il led cuffs reta in their shape longer than a ir-f i l led cuffs . Care must be taken to
remove all ai r f rom the cuff , because any remaining ai r wil l sett le in the most
superior part of the cuff , which is the part most l ikely to be h it by the laser beam.
Addit ion of methylene blue or o ther biocompatible and highly v isible dye to the
sa line wi l l help the surgeon to recognize a perforated cuff . Some surgeons object to
the addi t ion of methylene blue because if the cuff is punc tured, the color of the
t issues is al tered, making it dif f icu lt to recognize pathology.
Protective Wrappings The tube can be covered wi th a protective wrapping. These are discussed in
greater de tai l in Chapter 19.
Merocel wrap (Laser-GuardTM) was found to be acceptable for surg ical levels of
CO2 , KTP, and Nd-YAG lasers (219,220,221,222). Merocel-wrapped tubes are not
more combus tible if they are coated with blood (223). Reflec ted laser beams have
not been a problem with th is wrap (224). This product is easier to apply than
metall ic tapes (225).
Aluminum and copper tapes are effective for use with the CO2 and Nd-YAG lasers if
the tube is meticulously wrapped (226,227,228). However, a f i re can occur if the
laser contacts part of the tube that is not wrapped (229,230). A wrapped red rubber
tube does not offer protection f rom the KTP laser (86). The adhesive backing or
surface coating of some tapes can be ign ited by laser beams (92). The presence of
blood on the surface of foi l-wrapped tubes makes combustion more l ikely to occur
(223). Tape-wrapped tubes may unravel, leaving portions of the tube exposed. I f
the wrapping is dislodged, i t could obstruct the airway. A wrapped tube may catch
f ire (231,232). Meta ll ic tapes may ref lect the laser to nontargeted areas (224).
Spiral wrappings may cause the tube to k ink . Any wrapping adds thickness to the
tracheal tube, which could be a problem for the surgeon.
Protecting the Cuff with Wet Covers As a fu rther p recaut ion, moist cottono ids, sponges, or pledgets can be placed on
the cuff (92,233,234). Cotton gauze is a good choice because i t s tays wet longer
than other covers and has low energy transmission (235). Wet gauze wi l l also
protect the shaft (236). These have been found to be especial ly help ful with the
CO2 laser (234). The Nd-YAG, KTP, and argon lasers may allow some energy to
penetrate the pledget and rup ture the cuff (235).
I t is important that wet covers be kept moist. Laser beam h its may dry them, and if
that happens, they lose their protect ive effect. Further hi ts can cause the
co ttonoids and/or cuff to ign ite. Al l these must be retrieved af ter surgery.
Special Tracheal Tubes Ready-to-use laser-resis tant tubes are discussed in Chapter 19. Laser res istant
means tha t the material can wi thstand l imi ted laser energy wi th l i tt le o r no damage.
The use of a special laser tube does not necessari ly prevent a f ire during laser
surgery (237). Even though the tube is labeled laser-resistant, the cuff wi l l not be
resistant, and special p recautions need to be taken to protect it . A fi re may occur i f
the pro tec tive wet gauze over the cuff dries or is displaced.
No laser-resistant tracheal tube is completely safe f rom all types of lasers under all
condi tions . All of these tubes can be damaged or igni ted by lasers for which they
are not intended or by high laser energies (238,239). Some are made more
combustible by blood (223). Tubes sold for use with lasers should indicate the type
of laser fo r which they are sui ted as we ll as the condi tions (power, power densi ty,

spot s ize, oxygen concentra tion) under which the tube is safe to use. Stric t
adherence to manufacturer's warnings and d irections is essential .
I f the Nd-YAG laser is used through a f iber-optic bronchoscope passed th rough a
tracheal tube, i t is best to use an unmarked PVC tube (240). The tracheal tube
should be placed just below the vocal cords so tha t the t ip is as far away from the
operative si te as possible. I t should be remembered tha t the cover on the f iber-
optic endoscope is plast ic and can burn.
Some laser-res is tan t tubes are more resistant to f i re than conventiona l tracheal
tubes when contacted by elec trosurgical instruments (155).
P.920
When laser contac t tips are used, there is an even greater opportuni ty for igni tion .
They can get hot enough to melt and burn plast ics even when the laser is inac tive
(241).
Double-cuff tubes are not more resistant to leaks that wil l occur af ter cuff puncture
but do al low a sea l to be maintained if one cuff remains intact. The second cuff is
s t i l l vulnerable to puncture (239).
There are disadvantages assoc ia ted wi th laser-resis tant tubes . They are more
expensive than PVC and red rubber tubes. Since these tubes are often used for
patients who have had previous laryngeal surgery, the anatomy may be dis to rted,
making intubat ion diff icult . Some laser-resistant tubes are so st if f that i t is dif f icult
to pass a stylet or use wi th a specia lized laryngoscope such as the Bu llard
laryngoscope (Chapter 18). Therefore , a diff icult intubation may become even more
challenging when these tubes are needed.
Using Smaller Tracheal Tubes Smal l -diameter trachea l tubes require higher power densit ies fo r ignit ion than
large-d iameter tubes because the higher gas f low cools smaller tubes more quick ly
than larger tubes. Also, the smal le r the tracheal tube, the less l ikely i t is to be hi t
by an igni t ion source.
Making the Tracheal Tube Easy to Remove The tube should be f ixed so that it can be removed rapidly, if necessary. If the tube
is to be removed, th is should be done immediately after igni tion to minimize
damage to the ai rway and lungs. If the tube continues to burn, i t may be very
diff icul t to remove. Some tracheal tubes break apart as they burn . If the tube is
wrapped, the wrapping may break in to pieces tha t could lodge in the airway.
Some tubes are easier to remove than others (91). PVC tubes wi th sal ine-f il led
cuffs are more diff icult to remove than red rubber tubes . The fastest way to deflate
a fluid-f i l led cuff is to remove the contents wi th a syringe rather than cu tt ing the
pi lot bal loon. Unclamping the inf lation tube on a red rubber tube wi l l result in rapid
release of the cuff contents.
Wetting Fuels The use of wet towe ls , packers, or sponges around the surgical s ite can prevent
igni tion of materials near the s i te . Gauze or sponges used with uncuffed tracheal
tubes to minimize gas leakage in to the pharynx and sponges , gauze, and pledges
(and their s tr ings) used to protec t the tracheal tube cuff should be moistened and
not allowed to dry.
Hair that is near the opera tive si te (e.g., eyebrows, beards , and moustaches)
should be made nonflammable by coating i t thoroughly wi th a water-soluble
lubricating jelly .
Proper Preparation Practices Water-based solut ions should be used to decontaminate the skin prior to surgery
whenever possible . If a lcohol-containing solut ions must be used, a minimum of the
agent should be used and appl ied l ike paint, no t in a thick, runny coat. The so lu tion
should not be applied in a manner tha t allows dripping, pooling, or wicking. I f
so lut ion drips away from the surgica l s i te , it should be immediate ly blotted with a
gauze sponge before it can soak into any absorbent material . Any soaked materials
should be removed. Daubing of p rep pooled on skin (in the umbil icus or c ricoid
notch) may be needed. Draping should be delayed to al low the solution to fully
vaporize and become d iluted in room air. Th is could take 10 minutes or longer
(1,117). Incise (adhesive, occ lus ive) drapes should be used, if possible, to iso late
head and neck inc is ions from oxygen-enriched atmospheres and from flammable
vapors beneath the drapes (120). I f the incise material does not adhere to the
patient, the prep is l ikely s ti ll wet, and the pat ien t should be redraped once the
prep is ful ly d ry.
Correct Product Choices I t is important to consider the f i re potent ial when choosing equipment. The
anesthesia provider should be aware of the c i rcumstances under which a f i re can
occur and strive to use the product that wi l l have the lowest flammabil ity under
condi tions where i t wi l l be used.
Fi re /laser-res is tan t drapes should be used when exposure to igni tion is poss ib le. It
is important that the drape is tested with the type of ignit ion source that is to be
used. A standard for testing drapes using the CO2 laser has been published (242).
Laser-resistant anesthes ia c i rcui t protectors and drapes are available. These are
aluminized to def lec t the laser beam. There is sti l l the possibi l i ty tha t the beam may
be reflec ted onto a flammable surface and start a f ire (243).
The use of a metall ic Y-piece and elbow wi l l ensure tha t tracheal tube combus tion
wi l l not spread to the anes thesia breathing system (244).
Other Measures A number of other measures may be benef ic ial in preventing a f ire. The tracheal
tube should be withdrawn to above the s i te of surgery during tracheotomy. The use
of posi tive end-expira tory pressure (PEEP) may decrease the risk of a irway f i re in
some cases (245,246). Nurs ing personnel can reduce the combustible load in the
room by removing disposable paper wrappers and covers before the start of the
case. Not only does this reduce the fuel in the room, bu t it a lso reduces the waste
that mus t be disposed as “red bag” wi th i ts higher disposal costs (2).
Minimizing Oxidizer Concentrations The f ire risk can be reduced by remov ing or iso la ting the oxidizer f rom the surgical
area or minimizing i ts concentrat ion.
P.921
During def ibri l lat ion, all sources of oxygen should be comple tely removed f rom the
area around the pat ient.
Oxygen should be adminis te red only when indicated and in no h igher concentration
than is needed (as gu ided by oxygen saturat ion monitoring).
There are several ways of supp ly ing a gas with an oxygen concentra tion greater
than 21% but less than 100% to the pat ient. An oxygen and an ai r f lowmeter can be
connec ted by using a Y-piece (Fig. 32 .7), or a blender can be used. If the machine
has an a ir f lowmeter, a mixture of oxygen in a ir can be set and del ivered to
common gas outlet (247). If the common gas outlet can be accessed, a nasal
cannula can be mated to the outlet by using a 5-mm tracheal tube connector. I f the
common gas outlet cannot be accessed, a ci rc le sys tem can be attached to the
machine, the adjustable pressure l imi ting (APL) va lve c losed, and the selector
swi tch set to BAG. A nasal cannula can then be attached to the Y-piece. This
arrangement may cause the cont inuous positive pressure alarm to be activated. A
forced-air convect ion machine can be used to prov ide a high f low o f ai r around the
patient 's head whi le a nasal cannu la delivers a low f low of 100% oxygen to the
patient.
View Figure
Figure 32.7 Gas from an oxygen flowmeter and an air flowmeter can be connected to produce a gas with an oxygen concentration of less than 100%.
I f possible , the oxygen flow should be discont inued for at leas t 1 minute before
heat-produc ing surg ical instruments are used (248,249). When the heat source is
no longer used and any t issue embers are ext inguished, oxygen administra tion can
be resumed.
During head and neck surgery, a barrier should be established between the oxygen-
enriched atmosphere beneath the drapes and the surgica l field, if possible. Th is
can often be accompl ished wi th an adhesive (incise, occlusive) drape (2,117).
When gas is used to venti late the area under the drapes and prevent CO2
accumulat ion, the lowest acceptab le concentrat ion of oxygen should be used (250).
Forming an open tent wi th the drapes wil l prevent gases from collecting and allow
oxygen to diss ipate (56 ,170). Since oxygen is s light ly heav ier than room air as long
as there is some way for the oxygen to get in and out of a space, i t wi l l tend to f low
toward the f loor. Actively scavenging the space beneath drapes wi th a suct ion
device wil l lower oxygen concentrat ions s ign if icant ly (251). Dev ices that combine
oxygen de livery wi th suction to prevent oxygen bui ldup under the drape have been
described (252,253). A fan can be used to blow the accumulated oxygen away f rom
the pat ient. Direct ing the f low o f nasa l oxygen through a nasal ai rway wil l lower the
oxygen concentration a t the sk in (254).
Hea lth care ins ti tu tions should consider purchasing anesthesia workstat ions tha t
include internal pipel ines and f lowmeters for ai r (248). This makes it easy to switch
patient venti lat ion beneath the drapes f rom oxygen to air before the use of heat-
producing surgical instruments. An ex ternal f lowmeter can be added to an
anesthesia mach ine if piped air is available (Fig. 32.7).
Ni trogen, ai r, o r hel ium may be used to reduce the inspired oxygen concentrat ion to
the lowest level that wi l l provide acceptable patien t oxygenation. Nitrous oxide
supports combus tion and should not be used as the di luent gas (255,256,257).
Helium is a good heat conduc tor and may offe r a s ligh t pro tective effect wi th the
CO2 bu t not the KTP laser (258,259). The use of hel ium may decrease the
resistance of the gases passing through the tracheal tube (260,261).
P.922
Ni trogen insuff lation can s ignif icantly reduce the inc idence of laser-induced
tracheal tube cuff f i res (262). This can be accompl ished by attaching a catheter
covered with a laser-resistant wrap to the tracheal tube. Ni trogen is then insuff lated
through the catheter. This technique should be undertaken wi th caut ion, as a
hypoxic mix ture may possibly be adminis te red.
Al though using lower inspired oxygen concentrat ions wi l l reduce the risk of igni t ion ,
i t wi l l not tota lly prevent it . If there is a s igni ficant leak around the tracheal tube
cuff , the anes thesia prov ider may f i l l the reservoir bag by pushing the oxygen f lush .
This wi l l result in an elevated oxygen concentra tion. A more appropria te response
wou ld be to inc rease the f resh gas f low wh ile main ta ining the same inspired oxygen
concentration or to replace the tracheal tube.
When elec trosurgery is used in the oral cavity , the use of a cu ffed tracheal tube wi l l
minimize the oxidizer level . Leaks around the tube may result in f ires (161,263). I f
an uncuf fed tube mus t be used, an occlusive pharyngeal pack moistened with a
nonf lammable l iquid wi l l reduce the gas f low into the oral cavi ty (264). Insuff la ting
the mouth with gases such as helium, CO2 , or n itrogen wi l l reduce the oxidizer
concentrat ion . The oropharynx can be scavenged wi th separate suct ion.
Pneumatic power tools shou ld be opera ted wi th n itrogen or ai r. Inf latable
tourniquets should be inf la ted wi th ai r or nitrogen but not oxygen or ni trous oxide
(56,79,265). Ni trous ox ide should not be used for insuff la ting the abdominal cav ity
during laparoscopy (266,267,268).
Preventing Pressure Regulator Fires Fires in regulators can be minimized by not al lowing them to become contaminated
wi th oi l , grease, or other combus tible materials o r c leaned with a f lammable agent
such as alcohol (122,269). Before a regula tor is f it ted to a cyl inder, partic les should
be cleared f rom the cylinder ou tlet by remov ing the protect ive cap or seal and
s lowly and briefly opening (“cracking”) the valve wi th the port pointed away f rom
the user and any other persons . A cyl inder valve should always be opened slowly to
al low heat to be dissipated as the gas is recompressed. Consideration should be
given to rep lacing aluminum regulators with those made f rom brass. Rules for
handling cylinders are discussed in Chapter 1.
Fire Plan Each heal th care fac il i ty should formulate a plan for deal ing quickly wi th an
operating room f ire (1 ,6,56,58,127,171,202,206,240,270,271,272,273,274). Surgica l
teams should be trained in and prac tice dri l ls for keeping minor f i res f rom gett ing
out of control and manag ing f ires that do get out of control . They should know the
locat ion and proper use of a larm boxes, gas shut-o ff valves, and fi re extinguishers.
Evacuation procedures should be reviewed periodically.
I t is important to immediately cal l for help, decide who is going to f ight the fi re ,
when i t wi l l be appropriate to leave the room, and how to care for the pat ient during
the f i re .
Burning material on or in the pat ient of ten can be ex tingu ished effec tively and
safely by hand or wi th a nonflammable liqu id (e .g ., saline f rom a bas in on the scrub
table) or wet c loth. With laser surgery in the a irway, a t least two syringes f il led with
sodium chloride should a lways be available to ex tingu ish the f ire (275). Larger
areas can be smothered with a blanket or wet towe l. Fi re b lankets are not
recommended (8 ,276). If the drape is water-resis tant, water poured on i t wi l l be
ineffective (277). The f ire wi l l burn on the unders ide. The only effect ive technique
is to pul l the burning materials from the patient.
Fires tha t involve electrica l components are best handled by disconnect ing the
device from i ts electric power supply and removing the dev ice f rom the room.
The f low o f oxygen, n itrous oxide, or ai r to any involved equipment should be
turned OFF, if this can be accompl ished wi thout injury to personnel or the pat ient.
Most pat ients can tolerate short periods of oxygen deprivation . The patient should
be venti lated with ai r and intravenous agents used to mainta in anesthesia unt i l all
possible sources of f i re or reigni t ion are suppressed. It may be necessary to c lose
the oxygen and ni trous oxide shut-off valves to the affected room (58,278,279).
Cyl inder valves should be c losed and all cylinders removed from the area. If
supplemental oxygen is necessary to oxygenate the pat ient, the patient should be
moved to the nearest area where oxygen can be safely used (56).
I f an ai rway f i re occurs, the breath ing system shou ld be disconnected from the
tracheal tube to stop gas f low. If this s i te is not easi ly accessible or the operator
may be burned in the process o f disconnecting the tube, the breathing system can
be disconnected at the absorber (280).
The trachea l tube should no t be unduly secured so that i t can be removed quick ly.
Al though immediate removal of the tracheal tube and protective devices is usua lly
recommended wi th an ai rway f i re , th is may not always be the bes t course of act ion
(148,281). The risk:benefi t ratio of extubat ion needs to be considered. A stylet or
ai rway exchange catheter can be used to subst i tute a new tube the burned tube for.
I f the decis ion to remove the tube has been made, sal ine-f i lled cuffs on plast ic
tubes can be def la ted faster by aspira ting the f luid than by cutt ing the p ilot tube
(91). With red rubber tubes, unclamping the pilot tube is fastest.
P.923
The airway should be re-establ ished and the patient vent ilated wi th ai r unt i l i t is
certain that nothing remains burning . Then, 100% oxygen should be administered.
A search for f ragments tha t remain in the trachea and assessment of damage to the
larynx and tracheobronchial tree shou ld be made.
Extinguishing a Fire Although mos t operat ing rooms have a sprink ler system, sprinklers are frequently
not effec tive wi th operat ing room f ires (206). This is because the sprink le rs are
rare ly located over the operating room table and are heat ac tivated. Operating room
f ires tend to give off a lot of smoke and tox ic produc ts bu t not necessarily enough

heat to immediately activate the sprinklers . Therefore, i t is important the all
operating room personnel are fami liar wi th f i re extinguishers .
Location Strategically placed portable fi re ext inguishers are an important part of any f ire
protect ion program (1 ,282,283). They shou ld be located in conspicuous, readi ly
access ib le loca tions that a re known by al l operat ing room staff (F ig. 32.8).
Hands-on experience with f i re ex tingu ishers is essent ial to a f ire safety education
program (284). Sett ing up real f i res in a park ing lot and prov iding practice wi th
ex tinguishers can have valuable payoffs during an actual f i re.
Use Use of any f ire extinguisher can be recalled by the acronym, pass . Pul l the p in. Aim
the horn or nozzle a t the base of the f ire. Squeeze the trigger o r handle wh ile
holding the ext inguisher upright. Sweep the ext inguisher from side to side, covering
the area of the f i re. Ins truct ions are found on the f ire ext inguisher (F ig. 32.9). The
pin and hose are shown in F igures 32.10 and 32.11.
Choice of Extinguisher The choice of ex tingu isher should be based on the pred ic ted f ire risk for that
locat ion (282,285,286). Fi res are c lassif ied according to their fuel. Class A f i res
include small masses of ordinary combus tibles—-c lo th, paper, and most plas tics.
Fi res involv ing f lammable l iqu ids or grease are in c lass B. Electrical ly energized
f ires are c lass C. Two standard sets of f i re c lass labels exist: a tradi tional le ttering
system and a newer universal pictograph system tha t does not require the user to
be famil iar wi th the alphabet f ire c lass codes (F ig. 32.9).
View Figure
Figure 32.8 Fire extinguishers should be in conspicuous locations, well known to all operating room staff.
Halogenated Agents Halogenated ext inguishing agents are l iquids that upon discharge under relatively
high pressure surround a f ire with a combinat ion of vapor and l iquid droplets (mist).
Halogenated agents are ideal ly sui ted for f ighting f ires involv ing electronic
equipment and f i res in areas where electrical or electronic equipment is nearby.
Halon was the agent of choice fo r operating room f ires fo r many years (202). I t has
the abi li ty to penetrate burning material and to smother and cool the chemical
react ion of the fi re . While usual ly marked for c lass B and C f ires, i t is also effec tive
against class A f ires found in the opera ting room. Unfortunately, because of
environmental concerns, halon ext inguishers are no longer avai lable . If present in
an opera ting room, they may be used but cannot be recharged. The National Fi re
Protect ion Association requires that nonrechargeable
P.924
P.925
ex tinguishers be removed from serv ice 12 years from the date of manufacture

(287). In response to the prohibi tions on the use of ha lon , a number of
ex tinguishing agents have been developed to rep lace it (282,288,289) (Fig. 32 .12).
View Figure
Figure 32.9 The instructions for using the fire extinguisher are printed on the extinguisher.
View Figure
Figure 32.10 The pin that needs to be pulled to activate the extinguisher is in the handle at the top of the extinguisher. The hose is normally attached to the side of the extinguisher. This figure also shows the pressure gauge, which indicates that the extinguisher is usable, and the monthly checkout list, which shows that the extinguisher has been checked, the extinguisher and hose is undamaged, and the pressure is in the use range.

View Figure
Figure 32.11 Close-up of pin and pressure gauge at top of extinguisher.
View Figure
Figure 32.12 There are several substitutes for halon available.
Carbon Dioxide CO2 ex tinguishers emit a fog of CO2 gas with l iquid and solid partic les that rapidly
vaporize to cool and smother a f i re. Although they carry a B and C rat ing, they can
be used to ex tinguish small class A fi res. CO2 f ire ext inguishers are heav ier and
bulk ier than halon-type devices . CO2 ext inguishers do not leave a residue but do
emit l iquid and sol id components that rap idly vaporize . This causes rapid cool ing
that might cause f reezing i f i t comes into contact wi th exposed skin or internal
organs (283,290).
Water Pressurized-water ext inguishers are chiefly ef fec tive against c lass A f ires . They are
more dif f icult to use than CO2 and halon-type extinguishers. To put ou t fi res on
water-repel lant d rapes, a f inger mus t be placed over the nozzle to produce a f ine
spray. A s tream or splash of water could fan the f i re (1). A non-magnetic water mis t
ex tinguisher is avai lable for use in the MRI unit magnet room.
View Figure
Figure 32.13 All operating room personnel must know where the fire alarm is located. The instructions for activating it are printed on the fire alarm.
I f the f i re starts to get out of control , the f i re alarm (Fig . 32.13) should be sounded,
and the f ire department should be not if ied to give f iref igh ters ample time to respond
(1). F iref igh ters would ra ther f ind that a small f i re has been ext inguished than see
smoke bil lowing out of a bui ld ing—especially in a health care faci l i ty .
The patient and staff should be evacuated if the f i re and smoke are excessive
(210). In some s i tua tions , however, it may be more hazardous to move the pat ient
than to a ttempt to ext inguish or contain the f i re. The attending physician must
determine which would present the lesser hazard .
The doors should be c losed to contain the smoke and isola te the f i re . Wet sheets or
towels can be stuffed under the doors to reduce the spread of smoke f rom the
room.
Whatever steps are necessary should be taken to protect or evacuate pat ients in
adjacent a reas.
Af ter the f ire, involved materials and dev ices should remain in place for the f ire
department invest igators . Notes should be made as soon as poss ible af te r the f ire
and an inc ident report comple ted.
P.926
References 1. Anonymous. Understanding the f i re hazard. Techno l Anes th 1992;12(9):1–6.
2. Lees DE. Opera ting room f i res : s t i l l a problem? ASA Newslett 2002;66:33–34.
3. Anonymous. JCAHO warns about surgical f ires . Outpat ien t Surgery Magazine
2003;4:8 .
4. Nationa l Fi re Protect ion Association. Fi re safety in heal th care fac il i t ies. Quincy,
MA: Author, 2003.
5. Rodriguez JG, Satt in RW. Injuries as an adverse react ion to c l inical ly used laser
devices. Lasers Surg Med 1987;7:457–460.
[CrossRef]
[Med line Link]
6. Anonymous. A c l inician's guide to surgica l f i res. How they occur, how to prevent
them, how to put them out. Hea lth Devices 2003;32:5–24.
7. Wolf GL. Danger from OR f ires st i l l a serious problem. J Clin Monit Comput
2000;16:237–238.
[CrossRef]
[Med line Link]
8. Wasek S. Preventing surgica l f i res. Outpat ient Surgery Magazine 2003;4:28–
35.
9. Anonymous. E lec trosurgica l fi res sti l l a hot topic. Technol Anesth 1996;17(4):1–
2.
10. Rampi l IJ . Anesthet ic considerat ions for laser surgery. Anesth Analg
1992;74:424–435.
[Fu ll text Link]
[CrossRef]
[Med line Link]
11. Garry B, Bivens HE. Laser safety in the operating room. I. Admin istering
anesthesia. Cancer Bul le tin 1989;441:219–223.
12. Sosis MB. Hazards of laser surgery. Seminars in Anesthesia 1990;9 :90–97.
13. Van Der Spek AFL, Spargo PM, Norton ML. The physics of lasers and
implica tions for their use during ai rway surgery. Br J Anaesth 1988;60:709–729.
[CrossRef]
[Med line Link]
14. Bal l KA. Lasers. The periopera tive challenge. St. Louis : Mosby, 1995.
15. Absten GT. The fundamentals of medical laser technology. Biomed Instrum
Technol 2002;36:203–207.
[Med line Link]
16. American National Standards Inst i tute. Safe use of lasers in health care
fac i li t ies (ANSI Z-136.3). New York: Author, 2005.
17. Denton RA, Dedhia HV, Abrons HL, e t al . Long-term surv ival af ter
endobronchial f i re during trea tment of severe malignant ai rway obs truct ion with the
Nd:YAG laser. Ches t 1988;94:1086–1088.
[CrossRef]
[Med line Link]
18. Krawtz S, Mehta AC, Wiedemann HP, et a l. Nd-YAG laser-induced
endobronchial burn. Management and long term follow-up. Chest 1989;95:916–
918.
[CrossRef]
[Med line Link]
19. Brut inel WM, Cortese DA Edel l ES, et al. Compl icat ions of Nd:YAG laser
therapy. Chest 1988;94:902–903.
[CrossRef]
[Med line Link]
20. Lobraico RV. Laser safe ty in heal th care faci l i ties. Am Col l Surg Bul l
1991;76:16–22.
[Med line Link]
21. Sosis M. Anesthesia for laser surgery. Clin Anes th Updates 1993;4(5):1–12.
22. Anonymous . The devastat ion of pat ient f ires. Heal th Dev ices 1992;21:3 .
23. Brodman M, Port M, Friedman F, et al. Opera ting room personne l morbidity from
carbon d ioxide laser use during preceptored surgery. Obstet Gyneco l 1993;81:607–
609.
[Fu ll text Link]
[Med line Link]
24. Anonymous . Laser igni tion of surgical drapes . Heal th Devices 1992;21:15–16.
[Med line Link]
25. Sliney DH. Laser safety. Lasers Surg Med 1995;16:215–225.
[CrossRef]
[Med line Link]
26. National Fi re Protection Assoc ia tion. Standard for laser f i re p rotec tion (NFPA
115). Qu incy, MA: Author, 2003.
27. National Fi re Protection Assoc ia tion. Standard for laser f i re p revent ion (NFPA
115). Qu incy, MA: Author, 2003.
28. Asai T. Burn in the mouth during oral laser surgery. Anaesthesia 1997;52:806–
807.
[Fu ll text Link]
[Med line Link]
29. Tucker RD, Voyles CR. Laparoscopic e lec trosurgical compl icat ions and their
prevention. AORN J 1995;62:52–78.
30. Pfenninger J. ABCs of electrosurgery. Outpat ient Surgery Magazine 2004;5:45–
50.
31. Anonymous . Recommended pract ices for electrosurgery. Ci ty, STATE:
Associat ion of Operat ing Room Nurses, Inc., 1999.
32. Kle in SL, Leonard PF. Buzz ‘em or burn ‘em. Anes th Ana lg 1991;73:358–359.
[CrossRef]
[Med line Link]
33. Lee J. Update on electrosurgery. Outpatient Surgery Magazine 2002;3:44–53.
34. Bel l AF, Shagets FW, Barrs DM. Princ iples and hazards of elec trocautery in
otolaryngology. Otolaryngol Head Neck Surg 1986;94:504–507.
[Med line Link]
35. Anonymous . Prevent ing pat ient burns at the return-electrode s i te during high-
current elec trosurgical procedures . Heal th Devices Alerts 2005;29:1–3.
36. Meltzer B. Issues in electrosurgery. Outpatient Surgery Magazine 2001;11:51–
61.
37 . Dennis V. Pref l ight ing your act ive e lectrodes. Outpat ient Surgery Magazine
2003;4:62–68.
38. Dennis V. Protect ing pat ien ts f rom laparoscopic burns. Outpatient Surgery
Magazine 2004;5:84–85.
39. Dennis V. 7 ho t spots in e lectrosurgery. Outpatien t Surgery Magazine
2005;6:49–53.
40. Dennis V. Toward safer laparoscopic electrosurgery. Outpat ient Surgery
Magazine 2006;7:38–40.
41. Anonymous . Return-elec trode-s i te burns assoc ia ted wi th Ri ta Medical Systems
Mode l 1500 and 1500X radio-frequency generators . Heal th Devices Alerts 2005;29:
3–4.
42. Gross JB. Less jo lts from your vol ts—elec trical safe ty in the opera ting room
(ASA Refresher Course #126). Park Ridge, IL: ASA, 2005.
43. Lohmann G. Faul t wi th an Ohmeda Excel 410 machine. Anaesthesia
1991;46:695.
[CrossRef]
[Med line Link]
44. Bortolussi ME, Hunter JG. Fi re hazard of the ophthalmic cautery. Plast
Reconstr Surg 1989;83:753.
[Fu ll text Link]
[CrossRef]
[Med line Link]
45. Curt in JW. The disposable cautery: a f ire hazard . Plast Recons tr Surg
1989;84:853.
[Fu ll text Link]
[CrossRef]
[Med line Link]
46. Anonymous . Hazard report. Fluorescent l ights can ac tiva te Val ley Forge
Scien tif ic Mal is CM CIII bipolar e lectrosurgica l uni t . Heal th Devices 1999;28(5–
6):230–231.
[Med line Link]
47. Ashman MN, Mathasko MJ. E lec trical and fi re safety in the operat ing room.
Seminars in Anesthesia 1993;12:276–281.
48. Anonymous . Tra ining paramount in reducing risk o f surgical f i res . Technol
Anesth 2003;24:5–7.
49. Mil l iken RA, Bizzarri DV. Flammable surgical drapes—a pat ient and personnel
hazard. Anesth Analg 1985;64:54–57.
[Fu ll text Link]
[CrossRef]
[Med line Link]
50. Tucker RD. Laparoscopic electrosurg ical injuries : survey resul ts and their
implica tions . Surg Laparosc Endosc 1995;5:311–317.
[Med line Link]
51. McKee K. A gu ide to tes ting your electrosurgery ins truments. Outpatien t
Surgery Magazine 2001;11:59–64.
52. Dennis V. Choosing your act ive electrodes wi th care. Outpatient Surgery
Magazine 2003;4:65–67.
53. Anonymous . OR f ires caused by f iberopt ic i l lumination sys tems. Heal th Devices
1982;11:148–149.
54. Taylor IR. Hazards of laparoscopic surgery. Br J Anaesth 1999;82:651.
[Med line Link]
55. Eggen MA, Brock-Utne JG. Fiberoptic i lluminat ion systems can serve as a
source o f smoldering f i res. J Cl in Moni t 1994;10:244–246.
[Med line Link]
56. Anonymous . OR f ires : preventing them and putting them out. Heal th Devices
1986;15:132–136.
57. Anonymous . Laparoscopy l ight cable ign ites opera ting room f ire. Biomed Safe
Stand 1994;24:162–163.
58. Anonymous . Fires f rom def ibri l la tion during oxygen administration. Techno l
Anesth 1994;15:1–2.
59. Anonymous . Safety notice . Anaesthesia 1995;50:581.
60. Anonymous . Oxygen regula tor fi re caused by use of two yoke washers. Technol
Anesth 1990;11:1–2.
61. French Minis try of Employment and Solidari ty . Withdrawal f rom the market of
some pressure regula tors fo r medical use. September 1 , 1998.
62. Anonymous . High-pressure gas regulators . Technol Anesth 1999;19(10):8–9.
63. Anonymous . High-pressure gas regulators . Technol Anesth 1999;19(11):6.
64. Anonymous . Are aluminum regulators safe? Technol Anesth 1999;11(11):4–5.
65. Explosions and f i res in aluminum oxygen regulators . FDA and NIOSH Publ ic
Hea lth Advisory, 1999.
66. Anonymous . Alert . www.hosmat.com, 2000.
67. Anonymous . Fires , explos ions lead to recall of aluminum oxygen regula tors.
Biomed Safe Stand 1999;29:57–58.
68. Anonymous . Withdrawal f rom the market of some pressure regulators for
medical use. www.hosmat.com, 2000.
69. Anonymous . “The patien t is on f i re! ” A surgical f i res primer. Heal th Dev ices
1992;21:19–23.
70. Eisenbaum SL. Facial burns as a complicat ion of of fice surgery l ighting . Plast
Reconst Surg 1989;83:155–159.
[Fu ll text Link]
[CrossRef]
[Med line Link]
71. Bourke DL, Yee K, Mark L . Severe burn caused by an opera ting room l ight.
Anesthesiology 1993;79:171–173.
[Fu ll text Link]
[CrossRef]
[Med line Link]
72. Anderson EF. A potent ia l ignit ion source in the operating room. Anesth Analg
1976;55:217–218.
[CrossRef]
[Med line Link]
73. Rogers S, Dav ies MW. My anaesthes ia machine's on f i re . Anaesthesia
1997;52:505.
[Fu ll text Link]
[Med line Link]
74. Anonymous . Anes thesia machine f i re hazard update . Biomed Safe S tand
2003;33: 73–74.
75. Usher AG, Cave DA, Finegan BA. Cri tical inc ident with Narkomed 6000
anesthesia mach ine. Anesthesiology 2003;99:762.
[Fu ll text Link]
[CrossRef]
[Med line Link]
76. Alexander PD, Meurer-Laban M. Rechargeable optima laryngoscopes. Br J
Anaesth 1995;74:724–725.
[CrossRef]
[Med line Link]
77. Anonymous . Risk of f ire in surgical booms. Heal th Devices Alerts 2005;29.
78. Anonymous . Risk of f ire in surgical booms. Technol Anesth 2005;25:5–6.
79. Anonymous . Overv iew of pneumatic tourniquets. Technol Anesth 2001;22(4):1–
3.
80. Rita L, Seleny F. Endotracheal tube ignition during la ryngea l surgery with
resec toscope. Anesthesiology 1982;56:60–61.
[Fu ll text Link]
[CrossRef]
[Med line Link]
81. Cel inski M. Explosions in anaesthesia. Br J Anaes th 2005;94:691–692.
[Fu ll text Link]
[CrossRef]
[Med line Link]
82. Anonymous . Incompatibi li ty of disposable heated-wire breathing ci rcu its and
heated-wire humid if ie rs. Technol Anesth 1993;14:4–5.
83. Anonymous . Anes thesia breathing ci rcuits any overheat & melt tub ing . Biomed
Safe Stand 1994;24:85.
84. Anonymous . Fisher & Paykel—Dual-heated adul t resp iratory vent i lator ci rcui ts :
r isk of fi re . Heal th Devices Alerts 2006;30:4.
85. Gaba DM. More on ni trous oxide and laser surgery. Anesth Analg 1988;67:488–
489.
[Fu ll text Link]
[CrossRef]
[Med line Link]
86. Geff in B, Shapshay SM, Bellack GS. Flammabi li ty of endotracheal tubes during
Nd-YAG laser appl ica tion in the ai rway. Anesthesiology 1986;65:511–515.
[Fu ll text Link]
[CrossRef]
[Med line Link]
87. Ossoff RH, Duncavage JA, Eisenman TS, et al . Comparison of tracheal damage
f rom laser igni ted endotracheal tube f ires. Ann Oto l Rhinol Laryngol 1983;92: 333–
336.
[Med line Link]
88. Duncavage JA, Ossoff RH, Rouman WC, et al. Injuries to the bronchi and lungs
caused by laser-igni ted endotracheal tube fires. Otola ryngol Head Neck Surg
1984;92:639–643.
[Med line Link]
89. Patel KF, H icks JN. Prevention of f i re hazards associated with use of carbon
dioxide lasers. Anesth Analg 1981;60:885–888.
[Fu ll text Link]
[CrossRef]
[Med line Link]
90. Fried MP, Mal lampati R, Caminear DS. Compara tive analysis of the safety of
endotracheal tubes with the KTP laser. Laryngoscope 1989;99:748–751.
[Fu ll text Link]

[CrossRef]
[Med line Link]
91. Sosis MB, Braverman B. Advantage of rubber over plas tic endotracheal tubes
for rapid extubat ion in a laser f ire. J Cl in Laser Med Surg 1996;14:93–95.
[Med line Link]
92. Anonymous . Guidance on airway management during laser surgery of upper
ai rway. Technical Report ISO TR 11991, 1995.
93. Anonymous . Upper airway management guide provided for laser ai rway surgery.
APSF News le tt 1993;8:13–16.
94. Anonymous . Endotracheal tube mel ts and ignites inside pat ient 's trachea.
Anesthesia Malpractice Prevention 2001;6:9–14.
95. Brimacombe J. The incendiary characteris tics of the laryngeal and reinforced
laryngea l mask ai rway to CO2 laser strike—a comparison wi th two polyv inyl chloride
tracheal tubes. Anaes th In tens Care 1994;22:694–697.
[Med line Link]
96. Galapo S, Wolf GL, Sidebotham GW, et al . Laser igni tion of surgical drapes in
an oxygen enriched atmosphere. Anesthes io logy 1998;89:A560.
97. Anonymous . Fire! Technol Anesth 1996;16:4–5.
98. Gibbs JM. Combustib le plast ic drape. Anaesth Intens Care 1983;11:176.
[Med line Link]
99. Lazard JL , Wolf GL, Charchofl ieh J, et al. Surg ical drape combustion in FIO2-
0.21, FIO2-0.50 and FIO2-0.95. Pos ter presentat ion, ASA Meeting, New Orleans,
2001.
100. Lazard JL, Wolf GL, Charchaf lich J, e t al . Surgical d rape combus tion in FIO2-
0.21, FIO2-0.50 and FIO2-0.95. Pos ter presentat ion, American Soc iety of Crit ical
Care Anes thesiologists , New Orleans, 2001.
101. Barker SJ, Polson JS. Fi re in the opera ting room: a case report and laboratory
study. Anes th Ana lg 2001;93:960–965.
[Fu ll text Link]
[CrossRef]
[Med line Link]
102. Ott AE. Disposable surgical d rapes—a potent ial f ire hazard. Obstet Gynecol
1983;61:667–668.
[Fu ll text Link]
[Med line Link]

103. Domin MA. Safety precaut ions fo r laser surgery. J Heal thc Mater Manage
1991(June);9:20–25.
104. Wolf GL, Sidebotham GW, Lazard JLP, e t al . Laser igni tion of surg ical drape
materials in air, 50% oxygen, and 95% oxygen. Anesthesiology 2004;100:1167–
1171.
[Fu ll text Link]
[CrossRef]
[Med line Link]
105. Anonymous . Surgical f i re case summaries. Hea lth Devices 1992;21(1):31–34.
P.927
106. Axe lrod EH, Kusnetz AB, Rosenberg MK. Operat ing room f ires init iated by hot
wi re cautery. Anes thesiology 1993;79:1123–1126.
[CrossRef]
[Med line Link]
107. Bennett JA, Agree M. Fi re in the ches t. Anesth Analg 1994;78:406.
[Med line Link]
108. Ortega RA. A rare cause o f fi re in the operating room. Anesthesiology
1998;89:1608.
[Fu ll text Link]
[CrossRef]
[Med line Link]
109. Lai A, Ng KP. Fi re during thoracic surgery. Anaesth Intens Care 2001;29:301–
303.
[Med line Link]
110. Blanchard DL. Fi re in surgery. Ophthal Plast Reconstr Surg 1987;3 :59.
[CrossRef]
[Med line Link]
111. Stouffer DJ. Fi res during surgery: two fatal incidents in Los Angeles. J Burn
Care Rehab il 1992;13:114–117.
[CrossRef]
[Med line Link]
112. Wood DK, Ho ll is R. Thermocautery causes a gauze pad f ire. JAMA
1993;270:2299–2300.
[CrossRef]
[Med line Link]
113. Katz JA, Campbel l L. F ire during thoracotomy: a need to control the inspired
oxygen concentration. Anesth Analg 2005;101:612.
[Fu ll text Link]
[CrossRef]
[Med line Link]
114. Santos P, Ayuso A, Luis M, et al . Ai rway ign it ion during CO2 laser la ryngeal
surgery and high f requency je t venti la tion. Eur J Anaesthesiol 2000;17:204–207.
[CrossRef]
[Med line Link]
115. Anonymous . $200,220 awarded in pat ient burn case. Biomed Safe Stand
1995;25:133.
116. Anonymous . Use of acetone & “eggcrate” mattress c ited in operating room fi re .
Indiana hospi ta ls advised to review in ternal pol ic ies. Biomed Safe Stand
1989;19:26.
117. Anonymous . Fi re hazard c reated by the misuse of DuraPrep solut ion . Heal th
Dev ices 1998;27(5):400–402.
[Med line Link]
118. Plumlee JE. Operat ing-room f lash f i re f rom use of cautery af ter aerosol spray:
a case report. Anesth Analg 1973;52:202–203.
[Fu ll text Link]
[CrossRef]
[Med line Link]
119. Sebben J. Fi re hazard and electrosurgery. J Dermatol Surg Oncol
1990;16:421–424.
[Med line Link]
120. Anonymous . Improper use of alcoho l-based skin preps can cause surgical
f ires. Tech Anesth 2003;24:3–6.
121. Prasad R, Quezado Z, St. Andre A, et al . Fi res in the operat ing room and
intensive care uni t : awareness is the key to prevention. Anesth Analg
2006;102:172–174.
[Fu ll text Link]
[CrossRef]
[Med line Link]
122. Macdonald AG. A brief his to rical rev iew of non-anaesthet ic causes of f i res and
explosions in the opera ting room. Br J Anaesth 1994;73:847–856.
[CrossRef]
[Med line Link]
123. Green JM, Sonbol ian N, Gonzalez RM, et al . CO2 laser res is tance of various
ointments and tapes. Anes thesiology 1991;74:964–965.
[Fu ll text Link]
[CrossRef]
[Med line Link]
124. Datta TD. Flash f i re hazard with eye ointment. Anesth Analg 1984;63:700–
701.
[Fu ll text Link]
[CrossRef]
[Med line Link]
125. Ches tler RJ , Lemke BN. Intraoperat ive f lash f ires associated wi th disposab le
cautery. Ophthal Pl Reconst Surg 1989;5 :194–195.
126. Martin L, Dolman P. Fi re! Can J Anaesth 1994;46:909.
127. de Richmond AL, Bruley ME. Head and neck surgica l f i res. In: Eisele DW, ed.
Compl icat ions in Head and Neck Surgery. St. Louis: Mosby–Year Book, 1993;311–
312.
128. Mandych A, Mickelson S, Amis R. Operat ing room f i re . Arch Otolaryngol Head
Neck Surg 1990;116:1452.
[Med line Link]
129. Anonymous . Infant dies af te r operat ing room flash f i re. Biomed Safe Stand
1988;18:154.
130. Bowdle TA, Glenn M, Cols ton H, et al . Fi re fol lowing use of electrocautery
during emergency percutaneous trans tracheal venti lat ion. Anesthesiology
1987;66:697–698.
[Fu ll text Link]
[CrossRef]
[Med line Link]
131. Anonymous . Laser-igni ted latex glove causes airway f ire. Biomed Safe Stand
1992;22:51.
132. Simpson JI, Wol f GL. F lammabili ty of esophageal s tethoscopes, nasogastric
tubes , feeding tubes, and nasopharyngeal ai rways in oxygen- and ni trous oxide-
enriched atmospheres. Anesth Analg 1988;67:1093–1095.
[Med line Link]
133. Demos JE. Fi re in the opera ting room. Plast Recons tr Surg 1995;95:419–
420.
[Fu ll text Link]
[CrossRef]
[Med line Link]
134. Bropuwers JW. Collodion and electrocautery do not mix . Anes th Analg
1998;67:718.
[Fu ll text Link]
[CrossRef]
[Med line Link]
135. Carter R, Smith JS. Oesophagea l prosthetic igni t ion following accidenta l
exposure to the Nd. YAG laser—a rea l or po tential hazard. Lasers in Medical
Science 1988;2:229–232.
[CrossRef]
136. Anonymous . Anesthesia f i re burns young boy. Biomed Safe Stand 2003;33:65–
66.
137. Kanno TA, Aso C, Saito S, et a l. A combustive des truct ion of exp irat ion valve
in an anes thetic ci rcu it . Anesthesiology 2003;98:577–579.
[Fu ll text Link]
[CrossRef]
[Med line Link]
138. Mayworm D. How to prevent infect ion from surg ica l instruments . Outpatient
Surgery Magazine 2002; Special edi tion:38–44.
139. Barlas S. TIA c leans up hand-sani tizer controversy. NFPA J 2004;98:36.
140. Anonymous . Venti la tor & ESU involved in electrosurgical f i re. Biomed Safe
Stand 1991;21:114–115.
141. Rogers SA, Mi l ls KG, Tufa il Z . Case report. Airway f ire due to d iathermy
during tracheostomy in an intens ive care pat ien t. Anaesthesia 2001;56:441–446.
[Fu ll text Link]
[CrossRef]
[Med line Link]
142. Lim HJ , Mil ler GM, Rainbird A. Airway f ire during e lec tive tracheotomy.
Anaesth Intens Care 1997;25:150–152.
[Med line Link]
143. Bai ley MK, Bromley HR, All ison JG, e t al . Electrocautery-induced ai rway f i re
during tracheostomy. Anesth Analg 1990;71:702–704.
[Fu ll text Link]
[CrossRef]
[Med line Link]
144. Aly A, McIlwa in M, Duncavage JA. Elec trosurgery-induced endotracheal tube
igni tion during tracheotomy. Ann Otol Rhinol Laryngol 1991;100:31–33.
[Med line Link]
145. Lew EO, Mitt leman RE, Murray D. Endotracheal tube igni tion by elec trocautery
during tracheostomy: case report wi th au topsy f ind ings. J Forensic Sci
1991;36:1586–1591.
[Med line Link]
146. LeClai r J , Gartner S, Halma G. Endotrachea l tube cuff igni ted by
electrocautery during tracheostomy. J Am Assoc Nurs Anesth 1990;58:259–261.
147. Thompson JW, Colin W, Snowden T, et a l. F ire in the operat ing room during
tracheos tomy. South Med J 1998;91:243–247.
[Fu ll text Link]
[Med line Link]
148. Chee WK, Benumof JL. Airway f i re during tracheos tomy: extubation may be
contraindicated. Anes thesiology 1998;89:1576–1578.
[Fu ll text Link]
[CrossRef]
[Med line Link]
149. Marsh B, Ri ley RH. Double-lumen tube f i re during tracheostomy.
Anesthesiology 1992;76:480–481.
[Fu ll text Link]
[CrossRef]
[Med line Link]
150. Michels AMJ, Stott S. Explosion of tracheal tube during tracheostomy.
Anaesthesia 1994;49:1104.
[CrossRef]
[Med line Link]
151. Wilson PTJ, Igbaseimokumo U, Martin J. Igni t ion of the tracheal tube during
tracheos tomy. Anaesthesia 1994;49:734–735.
[CrossRef]
[Med line Link]
152. Bowdle TA, Glenn M, Cols ton H, et al . Fi re fol lowing use of electrocautery
during emergency percutaneous trans tracheal venti lat ion. Anesthesiology
1987;66:697–698.
[Fu ll text Link]
[CrossRef]
[Med line Link]
153. Baur DA, But le r RC. Electrocautery-ign ited endotracheal tube f i re: case report.
Br J Oral Maxil lofac Surg 1999;37:142–143.
[CrossRef]
[Med line Link]
154. Awan MS, Ahmed I. Endotracheal tube f i re during tracheos tomy: a case report.
Ear Nose Throat J 2002;81:90–92.
[Med line Link]
155. Sos is MB, Braverman B. Prevent ion of cautery-induced a irway f ires wi th
special endotracheal tubes. Anesth Analg 1993;77:846–847.
[Fu ll text Link]
[CrossRef]
[Med line Link]
156. Gupte SR. Gauze f i re in the oral cavi ty: a case report. Anesth Analg
1972;51:645–646.
[Fu ll text Link]
[CrossRef]
[Med line Link]
157. Simpson JI, Wol f GL. Endotracheal tube fi re igni ted by pharyngeal
electrocautery. Anesthesio logy 1986;65:76–77.
[Fu ll text Link]
[CrossRef]
[Med line Link]
158. Kel ler C, El l iot t W, Hubbel l RN. Endotracheal tube safety during
electrodissection tonsi l lectomy. Arch Oto laryngol Head Neck Surg 1992;118:643–
645.
[Med line Link]
159. Collee GG. A f i re in the mouth. Anaesthesia 1984;39:936.
[CrossRef]
[Med line Link]

160. Macdonald MR, Wong A, Walker P, et a l. Elec trocautery-induced ign ition of
tonsi l la r packing. J Oto la ryngol 1994;23:426–429.
[Med line Link]
161. Kaddoum RN, Chidiac EJ, Zestos MM, et al. Elec trocautery-induced f i re during
adenotons il lectomy: report of two cases. J Cl in Anesth 2006;18:129–131.
[CrossRef]
[Med line Link]
162. Mattucci KF, Mil i tana CJ. The prevention of f i re during oropharyngeal
electrosurgery. Ear Nose Throat J 2003;82:107–109.
[Med line Link]
163. Pashayan AG, Gravens tein N. High incidence of CO2 laser beam contac t with
the tracheal tube during operat ions on the upper ai rway. J Clin Anes th 1989;1:354–
357.
[CrossRef]
[Med line Link]
164. Hirshman CA, Smith J. Ind irect igni t ion o f the endotracheal tube during carbon
dioxide laser surgery. Arch Oto laryngol 1980;106:639–641.
[Med line Link]
165. Cozine K, Rosenbaum LM, Askanazi J , et al . Laser-induced endotracheal tube
f ire. Anesthesiology 1981;55:583–585.
[Fu ll text Link]
[CrossRef]
[Med line Link]
166. Eade GG. Hazard of nasal oxygen during aesthet ic facial operations . Plast
Reconstr Surg 1986;78:539.
[Fu ll text Link]
[CrossRef]
[Med line Link]
167. Brechtelsbauer P, Carrol l W, Baker S. Intraopera tive f i re with electrocautery.
Otola ryngol Head Neck Surg 1996;114:328–331.
[CrossRef]
[Med line Link]
168. Chang BW, Petty P, Manson PN. Patient fi re safety in the operat ing room.
Plast Reconstr Surg 1994;93:519–521.
[Med line Link]
169. Reyes RJ, Smith AA, Mascaro JR, e t al . Supp lemental oxygen: ensuring i ts
safe del ivery during facial surgery. Plast Reconstr Surg 1995;95:924–928.
[CrossRef]
[Med line Link]
170. Anonymous . Fi res f rom oxygen use during head and neck surgery. Heal th
Dev ices 1995;24:155–157.
[Med line Link]
171. Anonymous . Preparing for and manag ing surgical f ires. Heal th Dev ices
1992;21(1):24–31.
[Med line Link]
172. Aston SJ, Bornstein SJ . An unusual compl icat ion associa ted wi th
blepharoplasty. Aes thetic Plast Surg 1978;2:451–453.
[CrossRef]
173. Lederman IR. Fi re hazard during ophthalmic surgery. Ophthalmic Surg
1985;16:577–578.
[Med line Link]
174. Garf ield JM, Al len GW, Si lverstein P, et al . Flash f ire in a reducing valve.
Anesthesiology 1971;34:578–579.
[Fu ll text Link]
[CrossRef]
[Med line Link]
175. Gunatilake DE. Case report: fata l intraperi toneal explosion during
electrocoagulat ion v ia laparoscopy. Int J Gynaecol Obste t 1978;15:353–357.
[Med line Link]
176. El-Kady AA, Abd-El Razek M. Intraperitonea l exp losion during female
steri l izat ion by laparoscopic elec trocoagulation. A case report. In t J Gynaecol
Obs tet 1976;14:487–488.
[Med line Link]
177. Robinson JS, Thompson JM, Wood AW. Fire and explosion hazards in
operating theatres : a reply and new evidence. Br J Anaesth 1979;51:908.
[CrossRef]
[Med line Link]
178. Diemunsch PA, Torp KD, Van Dorsselaer T, e t al . Ni trous ox ide f raction in the
carbon d ioxide pneumoperitoneum during laparoscopy under general inhaled
anesthesia in pigs . Anesth Analg 2000;90:951–953.
[Fu ll text Link]

[CrossRef]
[Med line Link]
179. Neuman GG, Sidebotham G, Negoianu E, et a l. Laparoscopy explosion
hazards with ni trous oxide. Anesthesiology 1993;78:875–879.
[Fu ll text Link]
[CrossRef]
[Med line Link]
180. Anonymous . Use of wrong gas in laparoscopic insuff lator causes f i re. Heal th
Dev ices 1994;23:55–56.
[Med line Link]
181. Gre il ich PE, Greil ich NB, Froel ich EG. Intraabdominal f i re during laparoscopic
cholecys tec tomy. Anesthesiology 1995;83:871–874.
[Fu ll text Link]
[CrossRef]
[Med line Link]
182. Anonymous . Def ib ri llator sparks f lames in ambulance. Hea lth Devices Alerts
2004;28:1–2.
183. Anonymous . Using ex ternal def ibri llators in oxygen-enriched atmospheres can
cause f ires. Heal th Dev ices Alerts 2006;30:1–2.
184. Robertshaw H, McAnul ty G. Ambient oxygen concentrat ions during s imulated
cardiopu lmonary resusci tation. Anaes thesia 1998;53:634–637.
[Fu ll text Link]
[CrossRef]
[Med line Link]
185. Anonymous . Pat ient se t af ire by def ib ri l lator paddles. Biomed Safe Stand
2004;34:25.
186. Cas tro BA, Freedman A, Craig WL, et a l. Explosion wi thin an anesthesia
machine: Baralyme, h igh f resh gas f lows and sevof lurane concentrat ion.
Anesthesiology 2004;101:537–539.
[Fu ll text Link]
[CrossRef]
[Med line Link]
187. McKeskey CH. Letter to hea lth care professionals. 2003.
188. Las ter M, Roth P, Eger EI. Fi res from the inte rac tion of anesthetics wi th
desiccated absorbent. Anesth Analg 2004;99:769–774.
[Fu ll text Link]
[CrossRef]
189. Wu J, Previte JP, Adler E, e t al . Spontaneous igni t ion , exp losion, and f i re wi th
sevof lu rane and barium hydroxide l ime. Anesthesiology 2004;101:534–537.
[Fu ll text Link]
[CrossRef]
[Med line Link]
190. Olympio MA, Morell RC. Canister f ires become a hot safety concern. APSF
News le tt 2004;18:45–48.
191. Anonymous . Anesthesia carbon dioxide absorber f ires . Technol Anesth
2003;24:1–3.
192. Fatheree RS, Leighton BL. Acute respiratory distress syndrome after an
exothermic Baralyme-sevoflurane react ion. Anesthesiology 2004;101:531–533.
[Fu ll text Link]
[CrossRef]
[Med line Link]
193. Holak EJ, Mei DA, Dunning MB, et al. Carbon monoxide production f rom
sevof lu rane breakdown: mode ling of exposures under c linical condit ions. Anes th
Analg 2003;96:757–764.
[Fu ll text Link]
[CrossRef]
[Med line Link]
194. Gatti JE, Bryant CJ, Noone RB, et a l. The mutagenici ty of electrocautery
smoke. Plast Reconstr Surg 1992;89:781–784.
[Fu ll text Link]
[CrossRef]
[Med line Link]
195. Bal l K. No smoking in the OR. Outpatient Surgery Magazine 2003;4:62–67.
196. American Society of Anesthesiologists. Recommendations for infection control
for the practice of anes thesiology. Park Ridge, IL : ASA, 1998.
197. Paes ML. General anaes thesia for carbon dioxide laser surgery wi thin the
ai rway. Br J Anaesth 1987;59:1610–1620.
[CrossRef]
[Med line Link]
198. Anonymous . The elements of surgical f ires . Technol Anesth 2003;23:1–7.
199. Anonymous . Laser contact t ips and tracheal tubes. Health Devices
1992;21:18.
[Med line Link]
200. Wolf GL, Sidebotham GW, Stern JB. Intraluminal f lame spread in tracheal
tubes . Laryngoscope 1994;104:874–879.
[Fu ll text Link]
[CrossRef]
[Med line Link]
201. Moak E. E lec trosurgica l uni t safety. AORN J 1991;53:744–752.
[CrossRef]
[Med line Link]
202. McCranie J. Fi re safe ty in the opera ting room. Today's OR Nurse 1994;16:33–
37.
[Med line Link]
203. Anonymous . Laser starts f ire in OR. Technol Anesth 1988;8:3–4.
204. Denn is V. Improving your electrosurgery safety. Outpat ient Surgery Magazine
2003;4:44–48.
205. Anonymous . Electrocautery uni ts : improper disposal can cause f i res. Health
Dev ices Alerts 2005;29.
P.928
206. Ehrenwerth J . A f i re in the opera ting room: i t can happen to you (ASA
Ref resher Course #144). Park Ridge, IL: ASA, 2005.
207. Anonymous . FDA issues safety a lert on heated-wire breath ing c ircui t hazards.
Biomed Safe Stand 1993;23(19):146–147.
208. Gowardman JR, Moriarty B. Explosion and f i re in the expiratory l imb of a
Fisher and Paykel “three in one” respiratory care system. Anaesth In tens Care
1998;26:427–430.
[Med line Link]
209. Sommers JR. Flammabil i ty s tandards for surg ical drapes and gowns. Pas t,
present, and fu ture. Surgical Serv ices Management 1998;4 :41–44.
210. McCranie J. Fi re safe ty in the opera ting room. Todays OR Nurse 1992;14:33–
37.
211. Hawk ins DB, Joseph MM. Avoiding a wrapped endotracheal tube in laser
laryngea l surgery: experiences with apne ic anesthes ia and metal Laser-Flex
endotracheal tubes. Laryngoscope 1990;100:1283–1287.
[Fu ll text Link]
[CrossRef]
[Med line Link]
212. Kwan A. The use of Storz bronchoscope in prevention of airway f ire. Anaesth
Intens Care 2004;32:720.
[Med line Link]
213. Kjeldsen L, Andersen APD, Hjorth A. Laser surgery in the ai rway. Anaesthes ia
1986;39:1146.
[CrossRef]
[Med line Link]
214. Hunsaker DH. Anesthesia for microlaryngeal surgery: the case fo r subglo ttic
jet venti lation . Laryngoscope 1994;104:1–30.
[Med line Link]
215. Wegrzynowicz ES, Jensen NF, Pearson KS, e t al . Ai rway f i re during jet
venti lation for laser excision of voca l cord papi l lomata . Anes thesiology
1992;76:468–469.
[Fu ll text Link]
[CrossRef]
[Med line Link]
216. Sos is MB, Di l lon FX. Sal ine-f i l led cuffs help prevent laser-induced
polyv inylchloride endotrachea l tube f i res. Anesth Analg 1991;72:187–189.
[Med line Link]
217. LeJeune FE, Guice C, LeTard F, e t al . Heat s ink pro tec tion against lasering
endotracheal cuffs . Ann Oto l Rhinol Laryngo l 1982;92:606–607.
[Med line Link]
218. Walsh M, Schubert A, Al Haddad S. The addi t ion of lidocaine je lly to saline in
the cuff of the endotracheal tube during laser surgery of the airway. Am J Anesth
1997;24:189–193.
219. Sos is MB, Di l lon F. Prevention of CO2 laser-induced wi th the Laser-Guard
protect ive coat ing. J Cl in Anesth 1992;4:25–27.
[CrossRef]
[Med line Link]
220. Sos is MB. Evaluat ion of foil coverings for protect ing p las tic endotracheal
tubes f rom the potassium-ti tanyl-phosphate laser. Anesth Analg 1993;77:589–591.
[Fu ll text Link]
[CrossRef]
[Med line Link]
221. Sos is MB. Why is the Laser-guard protec tive coating better than the foil
tapes? In response. Anesth Analg 1994;78:1030.
[Fu ll text Link]
[CrossRef]
222. Van De Merwe W. Silver p rotec tive tape resis ts burning better than aluminum.
Cl in Laser Mon 1989;7:21–22.
223. Sos is MB, Pri tikin JB, Caldarel l i DD. The effect of blood on laser-resistant
endotracheal tube combus tion. Laryngoscope 1994;104:829–831.
[Fu ll text Link]
[CrossRef]
[Med line Link]
224. Sos is M, Dil lon F. Reflec tion of CO2 laser radia tion f rom laser-resistant
endotracheal tubes. Anesth Analg 1991;73:338–340.
[CrossRef]
[Med line Link]
225. Sos is M, Dil lon F. Prevent ion of CO2 laser tracheal tube f i res with the Laser-
Guard protective coat ing. Can J Anaesth 1989;36:S88–S89.
226. Sos is M, Dil lon F. What is the safes t fo il tape for endotracheal tube protection
during Nd-YAG laser surgery? Anesthesiology 1990;72:553–555.
227. Sos is MB. Which is the safest endotracheal tube for use with the CO2 laser? A
compara tive study. J Clin Anesth 1992;4:217–219.
[CrossRef]
[Med line Link]
228. Walker P, Temperley A, Thelfol S, e t al . Avoidance of laser igni tion of
endotracheal tube by wrapping in aluminum foil tape. Anaesth Intens Care
2004;32:108–112.
[Med line Link]
229. Kuo CH, Tan PH, Chen JJ, et al. Endotrachea l f i res during carbon dioxide
laser surgery on the larynx—a case report. Ac ta Anaesthesiol Sin 2001;39:53–56.
[Med line Link]
230. DeVane CC. Laser ini tiated endotracheal tube explosion. AANA J
1996;58:188–192.
231. DeVane GG. Case report: laser ini tiated endotracheal tube explosion. J Am
Assoc Nurs Anesth 1990;58:188–192.
232. Ko C-H, Tan P-H, Chen J-J, e t al . Endotracheal tube f ires during carbon
dioxide laser surgery on the larynx—a case report. Ac ta Anaesthes iol Sin
2001;39:53–56.
[Med line Link]
233. Fontenot R, Bailey BJ, Stiernberg CM, et al . Endotracheal tube safety during
laser surgery. Laryngoscope 1987;97:919–921.
[Fu ll text Link]
[CrossRef]
[Med line Link]
234. Sos is MB. Sa line soaked pledgets prevent carbon dioxide laser-induced
endotracheal tube cuff inf lat ion. J Clin Anesth 1995;7:395–397.
[CrossRef]
[Med line Link]
235. Anonymous . Do pledgets protect the tracheal tube cuff f rom lasers? Heal th
Dev ices 1992;21:17.
236. Mil ler G, Limb R. The CO2 laser and latex armoured tube (le tter). Anaesth
Intens Care 1995;23:517–518.
[Med line Link]
237. Ses terhenn AM, Dunne AA, Braulke D, et al . Value of endotracheal tube safety
in laryngeal laser surgery. Lasers Surg Med 2003;32:384–390.
[CrossRef]
[Med line Link]
238. Anonymous . Laser-resistant trachea l tubes. Heal th Dev ices 1992;21:4–14.
[Med line Link]
239. Anonymous . Laser-resistant endotracheal tubes and wraps . Heal th Devices
1990;19:112–139.
240. Ehrenwerth J . Fi re safety in the operating room (ASA Refresher Course). Park
Ridge, IL: Author, 2002.
241. Anonymous . Airway f i res : reducing the risk during laser surgery. Technol
Anesth 1990;11:1–3.
242. Inte rnational Standards Organization. Lasers and laser-related equipment: tes t
method for determining the CO2 laser res istance of surgica l drapes and/or pat ient
protect ive covers (ISO 11810). Geneva, Swi tzerland: Author, 2002.
243. Sos is M. Evaluat ion of a new laser-resistant anesthesia ci rcui t protector.
drape and patien t eye shie ld. J Cl in Moni t 1991;7 :132.
244. Sos is M, Braverman B, Ivankov ich AD. Meta l anesthesia c i rcu it components
stop laser f i res . Anes thesiology 1991;75:A396.
[Fu ll text Link]
[CrossRef]
245. Anonymous . Increased PEEP levels may reduce laser-induced tracheal tube
f ire risks . Biomed Safe Stand 1993;23:123.
246. Pashayan AG, San Giovanni C, Dav is LE. Posi tive end-exp iratory pressure
lowers the risk of laser-induced po lyv inylchloride tracheal-tube f i res.
Anesthesiology 1993;79:83–87.
[Fu ll text Link]
[CrossRef]
[Med line Link]
247. Lampotang S, Gravenste in N, Paulus DA, et al. Reducing the incidence of
surgical fi res: supplying nasal cannulae wi th sub-100% O2 gas mixtures f rom
anesthesia mach ines. Anesth Analg 2005;101:1407–1412.
[Fu ll text Link]
[CrossRef]
[Med line Link]
248. Anonymous . Reducing the risk of f ires during head and neck surgery. Technol
Anesth 2002;22:1–2.
249. Lowry RK, Noone RB. Fi res and burns during plastic surgery. Ann Plast Surg
2001;46:72–76.
[Fu ll text Link]
[CrossRef]
[Med line Link]
250. Greco RJ, Gonzalez R, Johnson P, et a l. Potential dangers of oxygen
supplementat ion during fac ial surgery. Plast Recons tr Surg 1995;95:978–984.
[Fu ll text Link]
[CrossRef]
[Med line Link]
251. Barnes AM, Frantz RA. Do oxygen-enriched a tmospheres exis t beneath
surgical drapes and contribute to f ire potentia l in the operat ing room? AANA J
2000;68:153–161.
252. Ramanathan S, Capan L, Cha lon J , et al . Minienvi ronmental contro l under the
drapes during opera tions on the eyes of conscious patien ts. Anesthesiology
1978;48:286–288.
[Fu ll text Link]
[CrossRef]
[Med line Link]
253. Rinder CS, Dabu-Bondoc S, Salgar V. A dev ice to reduce O2 accumulat ion and
reduce f i re hazard during MAC anes thesia. Anesthesiology 2005;103:A804.
254. Borkowski RG, Meneghett i C, Morgan MM, e t al . A comparison of methods for
delivering supplementa l oxygen during plastic surgery. Anes thesiology
2005;103:A841.
255. Sos is M. Ni trous oxide is contraindicated in endoscop ic surgery. Can J
Anaesth 1987;34:539.
[Med line Link]
256. Sos is M. Ni trous oxide shou ld no t be used during laser endoscop ic surgery.
Anesth Analg 1987;66:1054–1055.
[Fu ll text Link]
[CrossRef]
[Med line Link]
257. Shapiro JD, El-Baz NM. N2O has no p lace during oropharyngeal and
laryngotracheal procedures. Anesthes iology 1987;66:447–448.
[Fu ll text Link]
[CrossRef]
[Med line Link]
258. Simpson JI, Schiff GA, Wolf GL. The effect of hel ium on endotracheal tube
f lammabili ty . Anes thesiology 1990;73:538–540.
[Full text Link]
[CrossRef]
[Med line Link]
259. Alhaddad S, Brenner J. Hel ium and lower oxygen concentrat ions do not
prolong tracheal tube ign it ion t ime during potassium t i tanyl phosophate laser use.
Anesthesiology 1994;80:936–938.
[Fu ll text Link]
[CrossRef]
[Med line Link]
260. Rampi l IJ . He lium and gas f low. Anesth Analg 1993;76:S453.
261. Eisenk raft JB, Barker SJ . Hel ium and gas flow. Anesth Analg 1993;76:452–
453.
[Med line Link]
262. Sos is MB. Evaluat ion of a technique of nitrogen insuff lat ion to decrease
plast ic endotracheal tube cuff f lammabi li ty during carbon d ioxide laser surgery. J
Cl in Anesth 1993;5:468–470.
[CrossRef]
[Med line Link]
263. Pashayan AG, Gravens tein JS. Airway f i res during surgery wi th the carbon
dioxide laser. Anesthes iology 1989;71:478.
[Fu ll text Link]
[CrossRef]
[Med line Link]
264. Sommer RM. Prevent ing endotracheal tube f i re during pharyngeal surgery.
Anesthesiology 1987;66:439.
[Fu ll text Link]
[CrossRef]
[Med line Link]
265. Inappropriate use of oxygen to inf late or power medical devices . Heal th
Dev ices 1983;3:3.
266. Coral l IM, E lias JA, Strunin L. Laparoscopy explosion wi th n itrous oxide. Br
Med J 1975;1 :288.
[Med line Link]
267. Robinson JF, Thompson JF, Wood AW. Laparoscopy explosion with ni trous
ox ide . Br Med J 1975;3 :764–765.
[Med line Link]
268. Robinson JS, Thompson JM, Wood AW. Laparoscopy explosion hazards wi th
ni trous oxide. Br Med J 1975;4:760–761.
[Med line Link]
269. MDA SN 2000(07), Medical gas cylinders : risk of f i re. MDA Adverse Incident
Center, aic@medica l-devices.gov.uk/sn2000(07).htm
270. Moxon MA, Reading ME, Ward MB. Fi re in the opera ting theatre. Evacuat ion
pre-planning may save l ives. Anaesthesia 1986;41:543–546.
[CrossRef]
[Med line Link]
271. Weston CJ. The operat ing theatre's on f i re . Heal th Serv Manage
1988;84(3):20–23.
[Med line Link]

272. Fennell M. A multidisc iplinary approach to intraoperat ive f i re safety. AORN J
1995;62:636–637.
[CrossRef]
[Med line Link]
273. Vidor K, Puterbaugh S, Will is C. Fire safety training: a program for the
operating room. AORN J 1989;49:1045–1049.
[CrossRef]
[Med line Link]
274. Anonymous . Recognizing and extingu ishing medical gas fi res. Health Devices
Alerts 2003;27:5.
275. Lierz P , Heinatz A, Gustorff B. Management o f in tratracheal f i re during laser
surgery. Anesth Analg 2002;93:502.
[Fu ll text Link]
[CrossRef]
[Med line Link]
276. Anonymous . Fi re blankets in the OR? Technol Anesth 2000;20:3.
277. Bruner JMR. Fire in the operat ing room. ASA Newslett 1990;54:22–25.
278. Anonymous . Responding to fi res in areas of oxygen use. Heal th Dev ices
1994;23:306–309.
[Med line Link]
279. Anonymous . Recognizing and extingu ishing medical gas fi res. Health Devices
Alerts 2003;27(A14):5.
280. Deboer GE. Endotracheal tube f i res . Can Anaesth Soc J 1993;40:1003–1004.
281. Wolf G, Sidebotham GW. Endotracheal tube f i re: comments on the advisab il i ty
of not ex tubating . Anes thesiology 1999;91:888.
[Fu ll text Link]
[CrossRef]
[Med line Link]
282. Nat ional F ire Protect ion Associat ion . NFPA guide to portable f i re
ex tinguishers . Quincy, MA: Author, 2003.
283. Anonymous . Talk to the specialis t . Techno l Anes th 1996;17(4):3–4.
284. Finnegan J. Staff educat ion can prevent OR f i res . Todays OR Nurse
1994;16(3):24–26.
[Med line Link]
285. Nat ional F ire Protect ion Associat ion . Standard fo r portab le f ire ext inguishers
(NFPA 10), 2002 ed. www.nfpacatalog.org. Quincy, MA: Author, 2002.

286. Nat ional F ire Protect ion Associat ion . Standard fo r portab le f ire ext inguishers
(NFPA 10), 2002 ed. Quincy, MA: NFPA, 2002.
287. Anonymous . 10 quest ions about NFPA 10. What you might want to know about
maintaining and using portable fi re ex tingu ishers. NFPA J 2001;95:26, 92 .
288. Freestone A. Finding a halon alternat ive. NFPA J 2002;96:68–73.
289. Gibson J. Finding a halon alternative. NFPA J 2002;96:18, 20.
290. Anonymous . Select ing fi re extinguishers for the opera ting room. Hea lth
Dev ices 1996;25:261, 263.
P.929
Questions For the fol lowing quest ions, select the correct answer
1. The percentage of operating room fires that result in patient injury is A. 10% to 20%
B. 20% to 30%
C. 30% to 40%
D. 40% to 50%
E. 50% to 75%
View Answer2. Which of the following is most commonly involved in operating room fires? A. Lasers
B. Elec trosurgery equipment
C. Argon beam coagula tors
D. Fiber-opt ic i l luminat ion systems
E. Def ibri l la tors
View Answer3. Which type of tracheal tube will cause the most severe damage to the tracheobronchia l tree if i t catches fire?
A. Red rubber
B. Si l icone
C. Laser resistant
D. PVC
View Answer4. In order to filter out potentia l airborne contaminants, the surgical mask must be able to fi lter particles of which size? A. 30 microns
B. 3 microns
C. 0.3 mic rons
D. 0. 03 mic rons
E. 0.003 microns
View Answer5. Wet cotton gauze will protect the shaft and cuff of a tube best w ith which laser?
A. Argon
B. KTP
C. Nd-YAG
D. CO2
View Answer6. A clear, unmarked PVC tube is relatively resistant to be used with which laser?
A. Argon
B. KTP
C. Nd-YAG
D. CO2
View AnswerFor the following quest ions, answer
• i f A, B, and C are correct
• i f A and C are correct
• i f B and D are correct
• i f D is correct
• i f A, B, C, and D are correct.
7. The factors necessary to start a fire include
A. Igni tion source
B. Fuel
C. Oxidizers
D. Lasers
View Answer8. The characteristics of laser l ight inc lude
A. Coherency
B. Monochromatic i ty
C. Coll imated
D. Ul trav iolen t
View Answer9. Which factors determine the ignition risk with a laser? A. Laser medium being used
B. How the laser is focused
C. Class of laser
D. Exposure t ime
View Answer10. Common errors when using e lectrosurgical equipment include A. Improper p lacement of dispers ive elec trode
B. Insuff ic ient dispers ive elec trode contact
C. Faulty re turn electrode
D. Insu lat ing the patien t from the opera ting room table
View Answer11. Measures to minimize the risk of a tracheal tube fire from a laser include A. Fil l ing the cuf f wi th saline
B. Minimiz ing the laser power densi ty and durat ion
C. Us ing a laser-resis tan t tube
D. Us ing low oxygen concentrations in the inspired gas
View Answer12. Concerning laser-induced tracheal tube fires A. The tube may be contacted by a ref lec ted laser beam
B. The cuff is laser-resis tant
C. Cotton sponges that p rotect the cuff may dry ou t
D. Use of an uncuffed tube increases the risk
View Answer13. Which laser(s) is (are) l ikely to damage the retina?
A. KTP
B. Nd-YAG
C. Argon
D. CO2
View Answer14. Which laser(s) is (are) l ikely to damage only the cornea? A. KTP
B. Nd-YAG
C. Argon
D. CO2
View Answer





























