Embed Size (px)
Citation preview

CHAPTER
3 ORBITAL SURGERY
J C van der Meulen, PH Gilbert, R Roddi
EVALUATION
Orbital abnormalities can be appreciated only by those who are familiar with what is normal, and who are therefore aware of the importance of symmetry, balance and harmony. Not surprisingly we owe our knowledge first to artists, such as Leonardo da Vinci, and to anthropologists who studied the facial proportions and established the following relationships.
0RBITOFACIAL RELATIONSHIP
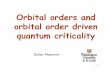
The rule of thirds The rule of thirds divides the face in three equal superposed levels - the upper, middle, and lower thirds (3.1). The upper and lower borders of the orbit are found respectively in the lower one-third of the upper level and the upper third of the middle level.
An ideal brow level for a fema le is well above the supraorbital margin with the lateral part slightly more elevated. For the male it
2/3 Menton
3.1 The frontal view of the face in aesthetic proportion. The face is roughly divided into thirds by division made at the points shown (the rule of thirds).
31
is at or close to the supraorbital rim. The brow itself is somewhat arched and, when the medial and lateral end are connected by a horizontal line, the point of maximal brow elevation is found at a line tangential to and vertical to the lateral limbus (3.2). The lateral brow ends on an oblique line passing from the ala of the nose and touching the lateral canthus (see 3.2). The lateral canthus is 1-2 mm higher than the medial canthus in occidentals and often higher than that in Asians. It is 5 mm from the orbital margin and 1 em from the fronrozygomatic suture. Its angle is acute and in contact with the globe. The medial canthus is rounded and separated by the lacus lacrimalis.
The upper eyelid covers the iris by 2-3 mm, and the lower eyelid is at a tangent to the iris. The upper lid crease is 8-12 mm from the eyelid rim. With the eye open, the loose septal skin overhangs the eyelid crease, forming the upper eyelid fold. The distinctive appearance of the Asian eyelid results from a smaller and lower upper lid crease than in Occidentals and a very full and prominent upper lidfold that very often hangs over and obliterates the upper lid crease .
I I
-------'------1 I
~:2~~-</ I I
/ /I
I I
I I
I I
I I
I
r
(~ ~j,// ....___. I
3.2 The f emale brow in relation to the nose and eye. The female brow lies wel l above the orbital rim.

ORBITAL SURGERY
The rule of fifths The rule of fifths breaks down the full face sagittally into five equal parts betweeen the two helices. Each of the five segments should be the equivalent of one eye's width (3.3 ). A study of this rule shows that the oral commissure is found at a line tangential to and vertical to the medial limbus (see 3.3 ).
The golden rule The dimensions, configuration, and position of the interorbital and orbital skeleton are intimately related, and alterations in size, shape, and site of one o f t hese structures may therefore affect this relationship (3.4) (Ricketts, 1982; Pacioli, 1509 ). Quite natura lly, human vision is offended by any abnormality in this particular relationship, but precise measurement has always been difficult.
CANTHI
Abnormalities may be due either to a change in the distances between the canthi or to a change in their level.
Currarino Hansman
Johr Laestadius
Johr Laestadius
I year old
3.3 The rule of fifths -there are five average 'eye widths' across the f ace.
I.O Ad~~-- \ :::-;_.- - ,.,
1 \,~ I~::.:-~ I I 1?:-_,-:- -- - -:-. .:::<f I
"'-:"':------ .,.,...""' I I : : ~----· I I I I I I I I I I
r.c-:::-c-:::-::--i I I I I I I
I I I I
I 8,3 I
I 11,3
3.5 The intercanthal relation. Assessment of distances in the orbital region by different authors. OOD - outer orbital distance; OCD - outer canthal distance; lCD - inner canthal distance; IDD- inner dacryal distance.
32
Intercanthal distances An abnormally wide distance between the medial canthi may be observed, and telecanthus must be differentiated from teleorbitism and hypertelorism. Telecanthus is produced by an abnormal insertion or length of the medial canthal tendons, whereas teleorbitism signifies that the distance between the dacrya has increased for some reason.
Measurements of the intercanthal distance do not always reflect the position of the orbit and the globe in patients with telecanthus. Gunther (1993 b) examined the normal distance between the dacrya and fou nd an upper limit of 30 mm. T his figure corresponds to a canthal index of 38 when the distance between the inner canthi is compared with the distance between the outer canthi and the result is expressed as a percentage.
Romanus (1953) advocated the use of an outer orbital (eyespan) to intercanthal (eyespace) index to measure the relationship. Dividing the external biorbita l diameter measured between the most lateral points on the temporal margin of the orbital wall (OOD) by the diameter joining t he inner canthi (ICD ), he arrived at a normal value of 40.
3 .4 The golden rule.
~ ~'\)
Mongoloid slanting
~
~) Antimongoloid slanting
3.6 The canthal level.
\
( ~

EVALUATION
Tessier stressed the point tha t objective measurements of the interorbital distance (IOD) should be taken between the lacrimal crests (the 'dacryons'), recognizing that the value thus obtained may be 7-8 mm greater than that of the more posterior measurements obtained by Gunther (1933b).
Average values for the distance between the dacryons, the canthi and the lateral orbital wall are presented in 3.5 .
The term teleorbitism or hypertelorism is used when there is an interorbita l distance of more than 30 mm and a canthal index over 42.
Along with Giinther, Tessier (1972) distinguishes between degrees of hyperrelorism: • 1st degree hyperrelorism - 30-34 IOD. • 2nd degree hypertelorism- 34-40 IOD. • 3rd degree hypertelorism- over 40 IOD.
Classifying hyperrelorism with its different aetiologies and varied appearances is not as simple as one might believe, but accurate differentiation is important if the type of malformation and its correction are to be matched. It should be based on the consideration that hypertelorism does not represent a syndrome but is rather only one of the signs that may be observed in this area. An abnormally wide interorbital distance is not automatically associated with divergence of the orbital axes and the lateral orbital walls.
It is therefore suggested that distinction is made between orbital hypertelorism (teleorbitism), in which there is true la teralization of the orbits, and interorbital hypertelorism, in which there is no observable lateralization of the orbits.
A: Euophthalmus
B: Enophthalmus
D: Enorbitism
Interorbital hypertelorism is present when the IOD is increased and the distance between the ectocanthia is normal. This anomaly is observed in patients with encephalocoeles or pneumatocoeles. Orbital hypertelorism (teleorbitism) exists when both distances are increased .
Canthal level (3.6) Cranial displacement of the lateral canthi (mongoloid slanting) is seen in Down's syndrome. Caudal displacement of the lateral canthi (anti-mongoloid slanting) is symptomatic of malar dysplasia. W idening may be seen in rare malformations such as Goldenhar's syndrome.
Alterations in the position of the medial canthi following trauma may occur in every direction - posterior and anterior, cranial and caudal, medial and lateral. Medial displacement of the lateral canthus may have been caused by trauma but more often it is iatrogenic, following eyelid reconstruction. Lateral displacement of the medial canthus may be due to rare skeleta l diseases such as fibrous dysplasia or craniotubular dysplasia. More commonly, however, it is caused by cysts and tumours of different origin.
EYE EXPOSURE
The amount of exophthalmus or enophthalmus is determined by the relation between the volume of the orbital contents and the volume or shape of the orbit itself (3.7).
C: Exophthalmus
E: Exorbitism
3.7 The orbito-ocular re lation . a Euophthalmus; b enophthalmus; c exophthalmus; d enorbitism; e exorbit ism.
33

ORBITAL SURGERY
~: ~ ~Normal )
~1~.'.~ (f
· i~-~'-<~/h/ ~ I
I I I I
=========,_ ___ --
I / I
I / A<C~
! (~ I I
/~~-~-l'\ " ~il~ .. -I II I 1 ~11 I
I ~~~-~_ . . : I ~~ ~--·~. ·- ~~--~_ ,_ , ,_ ,_ ~"_ ·· . . I -~ih~ ··-~r I I -., · I · •
(: ~ I . · ,f!· I ) (' I -\ . ·· . I 1~1 )
/~ (~ ;:
~Short ~ssure ) : : ~Long fissure , : : ~Long and wide , t -I I
I
:~T~-,A ~W -
I 1 ~ 1 1 ~11 I
1 1if ~,, ;;I ~{!2· I I ~/~:;,-• ·'' ' I ~- "''£_ . _ I 1 /j'(ti2 ""-~ - .,- I I ~ · I ~ I - _.,:: I I~ :) : (~ I ... - 1)
I I
/~ ~ - I I ~~~ )
{$)Wide fissure : I . . I I . .
1 (!)Short and wide . 1 1 (!)Long and narro~ I I
3.8 Dimensions of the eyelid fissure.
Exophthalmus due to alteration of orbital shape or reduction in orbital volume is seen in various synostosis syndromes, such as Aperr's syndrome and Crouzon's syndrome. When it is due to an increase in volume of the orbital contents, it may be caused by buphthalmia, orbital cysts and tumors, and retrobulbar haematoma. Most frequently it is related to thyrotoxicosis.
Enophthalmus may be observed in patients with microphthalmia or Treacher-Collins syndrome, after fractures of the orbital walls, or as a result of fat atrophy.
Exophthalmus and enophthalmus can be measured with an exophthalmometer, but more accurate information is provided by CT scanning. Exophthalmus should be distinguished from inferior scleral show. This can be due to retrusion of the orbital floor, lid retraction, or lagophthalmus.
Eyelids Texture and structure of eyelids can be described in a variety of ways. The tissues may be called slack, soft, thin, smooth, loose and redundant or tight, firm, thick, scarred, adherent, or deficient.
Deficiency of tissue Diffuse deficiencies of tissues of skin conjunctiva are seen in blepharophimosis, certain diseases (psoriasis, ichthyosis, pemphigus, trachoma), and burns. As a result, sympblepharon, entropion, or ectropion can occur in these patients.
Circumscribed deficiencies are seen in congenital anomalies such as ectropion, euryblepharon, epicanthus, and colobomata, and in traumatic lesions.
Traumatic lesions in particular require a detailed analysis involving several questions concerning location and penetration of the wound or the configuration and direction of scars. For example: • Does the lesion involve the lacrimal apparatus or levator muscle? • Is the lesion linear or more complex? • Does the scar run parallel to the palpebral fold or tension lines? • Is the lesion associated with a deficency of tissue causing either
entropion or ectropion?
Redundancy of tissue Redundancy of skin or conjunctiva is observed in a variety of tumours, including haemangiomas, lymphangiomas, and neurofibromatosis. Much more common, however, is redundancy caused by degeneration. Blepharochalasis, ptosis, entropion and ectropion are some of the abnormalities caused by old age.
-------~================~
34
I I
Eyelid fissure An abnormal dimension may be symptomatic for a series of conditions (3.8 ): • A short fissure may be due to myocutaneous contraction to global
retrusion or to canthal and skeletal anomalies. • A long fissure may be observed in myocutaneous laxity, in global
protrusion, and in skeletal anomalies. • A narrow fissure may be seen in myocutaneous hypertrophy
rigidity or contraction, in neuromuscular anomalies, in global retrusion, and in skeletal anomalies.
• A wide fissure may be a sign of myocutaneous deficiencies of neuromuscular anomalies and global protrusion. Many combinations are possible. A short or long fissure may also
be narrow or wide. Both eyelids or canthi may be involved or only one. Each combination can be associated with mongoloid or antimongoloid slanting.
Eyelid function Ptosis of the eyelid is usually congenital. More rarely it is caused by lesions of the oculomotor nerve to the levator muscle or by degeneration of the levator aponeurosis.
Lagophthalmus may be produced by hypoplasia of the orbicular muscle, as seen in euryblepharon, or by facial paralysis. Entropion and ectropion are caused by structural differences between the inner and outer lamina, caused by deficency or redundancy of tissues.
SURGICAL PRINCIPLES
PROTECTION FROM EXPOSURE
Protecting the cornea Hidden between the walls of the orbit and covered by the eyelids, the eye is normally well protected. H owever, the cornea, being the interface between the brain and the outside world, is extremely vulnerable. It is easi ly damaged by desiccation and irritation, and trauma, in whatever form, should therefore at all costs be prevented.
Protection of the cornea is urgent in two groups of patients: • The group with exophthalmus, caused by Crouzon's syndrome,
Apert's syndrome, etc. • The group with lagophthalmus, caused mainly by colobomata or
trauma. In these cases there is a constant threat to the eye, and this
becomes particularly dangerous when exposure of the cornea persists during sleep, in spite of a normal upward rotation.

SURGICAL PRINCIPLES
Protecting the conjunctiva The conjunctiva, although less vulnerable, may also suffer from exposure, but the consequences are never so dramatic as with the cornea and bealing is usually complete. Protection of the conjunctiva is frequently indicated in patients with entropion and ectropion, in which chronic irritation may be a source of complaint.
Methods of protection Correction of the anomaly is of course the best way to protect the eye. However, there may be circumstances that necessitate temporary measures being taken. Such temporary measures include: • Partial tarsorraphy. • An hourglass bandage, maintaining a humid climate over the eye
surface. • Various ocular unguents and liquids.
PREPARATION
When preparing the patient for an elective procedure, a clean operative field can be best obtained with a betadine solution, which does not irritate the conjunctiva. However, for emergency treatment following trauma a different approach is indicated. The orbital area and its surroundings are washed gently with copious amounts of a saline solution. All foreign material is then removed, if necessary with a small brush, and the depth of the wound is explored, taking care not to dissect or undermine excessively All devitalized tissue and small areas of tissue irregularities are then resected.
This must be done very carefully, because small fragments of skin and conjunctiva may remain viable and their resection may cause a secondary deformity. Meticulous haemostasis is performed either by prolonged compression of bleeding spots or by careful use of the thermocautery.
PROCEDURE
Following inspection and analysis of the abnormalities that can be seen, a strategy for correction should be outlined. This strategy has only one goal- the realization of a perfect result or, in other words, a function and appearance that are as normal as possible. To achieve this goal, a balance must be struck between the demands that are made by the receptor area and the solution offered by the donor areas.
Receptor areas A correct inventory and analysis of the abnormalities that are present is of utmost importance. Without this, the choice of the best procedure becomes a gamble. This means that an inventory must be made of the existing abnormalities analysed before considering what to do next.
Donor areas Following this analysis and inventory, a survey is made of the quality and quantity of the tissues that are available for correction. In general, preference should go to tissues that match the normal colour and texture of the receptor area as much as possible. In this respect there is no better substitute than tissues from the eyelid itself.
If this is not an option, other donor areas will have to be considered. There are many possibilities. If skin is needed, it can be transported as a flap or as a graft. If mucosa is needed a graft is the best solution.
The donor areas should of course be repaired in such a manner that they are barely noticeable.
35
3.9 Incisions of tissues- facial incisions should correspond with Langer's lines.
Just as there are many roads that lead to Rome, there are also many ways to be successful in ophthalmic plastic surgery. Each surgeon has to decide for himself or herself which procedure is going to give the best result.
This chapter will not provide any easy answers to difficult questions. It has only one purpose and that is to create a solid foundation of principles from which the surgeon can choose according to his or her needs and the needs of the patient. 'The principle is the point and the variation a necessity.'
The correction of a deformity usually involves three steps:
1. The incision of tissues. 2. The fixation of tissues. 3. The redistribution of tissues by various means, such as apposi
tion, transposition, or transplantation.
Incision of tissues All scars contract but some do so more than others. The degree of contraction is difficult to predict. Some of the factors involved are of an individual nature; they are not known and are therefore difficult to control. One factor, however, is known and always ready for inspection- the direction of the scar.
The direction of the scar affects healing in such a way that severe contraction is produced whenever it runs at right angles to the course of the relaxed skin tension lines, which in the eyelids correspond with that of the orbicularis muscles. Contraction becomes more evident when the scar is long and when the deeper layers are involved. It is particulary pronounced when it cuts across the eyelid rim.
The implications of this are clear. Incisions should follow the course of the orbicularis muscles and be made as near parallel as possible to the direction of the palpebral fissure (3.9).
Although it is true that scars soften and contractures frequently becomes less severe with time, why rely on nature when it shows time and time again that it can be very capricious?

ORBITAL SURGERY
Fixation of tissues H ealing in the orbital area is excellent and the most important advice is that sutures should never interfere with healing. A strangulating suture does more harm than one that is omitted, as does every suture that irritates the sclera or cornea.
A few inverted 6.0 catgut sutures for fixation of conjunctiva, a mucous membrane graft or subcutis and a few interrupted 6.0 monofilament sutures or a running suture for the skin are usually all that is needed. Even a steristrip may be sufficient.
REDISTRIBUTION OF TISSUES
Approximation of tissue The term 'apposition' is used to indicate a situation in which the edges of a wound can be apposed without further release or mobilization of tissues: i.e. the creation of a flap.
Apposition is the simplest form of closure, and it is performed when there is no or little loss of tissue. It is the procedure of choice in wounds that run parallel to the eyelid rim because it leaves a minimum of scarring and is least time consuming.
It may also be indicated in wounds that run at right angles to the eyelid rim but only as an emergency and only with the thought in mind that secondary correction of scar contraction may have to fo llow at a later date.
It is not indicated when reposition will hold the wound edges under unpermissable tension, because tension of the wound edges and attendant disturbances of these edges will cause dehiscence, extra loss of tissue, and secondary deformities due to traction and contraction.
Transposition of tissue Transposition of tissue occurs when a partially detached piece of skin is moved from one donor position to another receptor position. Transposition is direct when donor and receptor site are in continuity with each other and correction is obtained in one session . Transposition is indirect when donor and receptor site a re separated and correction is obtained in two sessions- a first session, in which the flap is transported and receptor and donor site are connected by the pedicle of the transposed flap, and a second session, in which the integrity of donor and receptor site is restored.
The transposition of flaps taxes the ingenuity of the ophthalmic plastic surgeon because the objective is to obtain an optimal correction of the ma lformation in a minimum of time, using a minimum of tissue and leaving a minimum of scarring. In order to obtain this goal a thorough knowledge of the different fl aps and of their possibilities and limitations is required.
Flaps may be differentiated according to composition, configuration, vascularization, and range of motion.
COMPOSITION OF FLAPS
Depending on the nature of the tissues that are incorporated in a flap, distinction can be made between cutaneous flaps, mucosal flaps, and composite flaps. Composite flaps consist of skin and conjunctiva. The tarsus may be included. Cutaneous flaps are frequently ra ised in combination with some muscle fibres and are sometimes called myocutaneous flaps.
CONFIGURATION OF FLAPS
In textbooks, flaps are frequently referred to as transposition flaps, rotation flaps, or advancement flaps. However, such a distinction
U - flap V- flap
C- flap 0- flap
3 .10 Configuration of flaps.
makes no sense. All flaps are transposed, as their use involves a change of position, and all flaps can be rotated or advanced (translated). Indeed, the flap that rotates less than any other flap is called a rotation flap (3.10).
Since there are no such flaps as transposition, rotation, or advancement flaps, it would be much better to characterize the different flaps by their shape, because this is the dominant quality. Flaps may be designed in a lmost any shape but the design is usually based on a form that may be symbolized by a letter, such as U, C, 0 , or V. In this chapter these flaps will therefore be called Uflaps, C-flaps, 0-flaps (or island flaps} and V-flaps (see 3.10).
The decision to use a particular design for transplantation is made only after carefu l evaluation of its origin, viability, mobility, and utility.
VASCULARIZATION AND VIABILITY OF FLAPS
The question of whether a flap will survive is not determined by the ratio of its length to its width. The critical factor is the number and type of blood vessels located in its pedicle. Based on this criterion, distinction can be made between: • Random flaps, which are nourished by an unknown vascular
supply (e.g. cutaneous flaps that survive by perfusion through the dermal-subdermal plexus, and myocutaneous flaps supplied by musculocutaneous arteries that enter from muscle). In the periorbital and orbital area the blood supply is excellent and the length of flaps may be several times their width.
• Axial flaps, which are vascularized by a recognizable artery.
MOBILITY OF FLAPS
When used to cover a defect the flap is either translated (moved in a direction perpendicular to its base) or rotated (moved laterally). Certa in flaps a re used for direct transposition whereas others are specially designed for an indirect transposition procedure.

SURGICAL PRINCIPLES
!
~~ ~ ~ ~ ~ _iJ j_J
·~ ) -- ( ...
! ~ ~· ~~
3.11 U-flaps, when advanced, tend to produce dog-ears that require correction.
® '\
I J
3.12 Combinations of V-flaps andY-flaps: a V- Y-flap; b Y-V-flap.
Translation Translation or advancement has important disadvantages. The range of translation of a flap depends on the elasticity of the tissues it contains and on the extent to which its base is able to follow the translation. In general, the range of movement is rather limited, and part of the gain that has been obtained may become undone as a result of scar contracture. This is particularly so when the axial direction of the flap was designed at right angles to the eyelid fissure.
Further problems are that the redistribution of skin and the quality of scar formation are less than optimal.
U-flap If aU-flap (3.11) is advanced in the direction of its distal end, closure of the defect will be associated with the formation of two 'dog ears' that flank the base of the flap. Correction of these dog ears
37
c~ ~
~ \
requires reduction and therefore loss of skin. In addition, the angular or rounded scars at the tip of the flap will tend to contract and cause a ' trapdoor effect'.
V-flap If a V-flap is advanced in the direction of its base, the V-incision tS
turned into a Y-incision, which may be closed without loss of skin but at the cost of a complex scar (V- Y-plasty}.
If the V-flap is advanced in the direction of its tip and a Y-Vplasty is performed, two lateral folds tend to be produced at both sides of its base (3.12). Reduction of this surplus will be associated with the formation of scars at right angles to its axial direction. A Y-V-plasty may be indicated in the correction of canthal malformations but the deformity has a tendency to recur.

ORBITAL SURGERY
0-flap In comparison with the U-flap and the V-flap, the 0-flap has a wider range of motion. No lateral excess of tissue is produced and scar contraction has little effect on its position. To avoid a trapdoor effect the flap must, however, be designed in a more elliptical fashion. In general, we see very little use for translation of skin and mostly rely on the rotation of flaps.
®
®
-
' I @ I
~ I
-t~
© I
I /
0 - t
~
3.14 C-flap rotations: a plain C-flap rotation; b C-flap rotation facilitated by first Z-plasty; (c) C-flap rotation f acilitated by second Zplast y.
Rotation of flaps The range of motion of a rotated flap is determined by the ratio of its length to its width. The longer the flap and the narrower its base, the wider the range will be. The shorter the flap the more restricted rotation becomes, unless its base is partially narrowed by a backcut, as in a C-flap, or totally cut except for its subcutaneous pedicle, as in the 0-flap.
3.13 U-flap rotation always leaves a substant ia l defect that may have t o be closed with a graft.
3.1 5 0-flap. (Courtesy of B Haeseker.)

SURGICAL PRINCIPLES
The value of a rotation flap lies in its potential to close defects within a wide perimeter, and in this respect there is a great deal of similarity between the basic U, C, 0 and V types of flaps . Differences become apparent in the way the flap is placed into the receptor site and the way the resulting donor site is closed.
U-flap AU-flap (3.13) ca nnot be advocated for the purpose of rotation, since there is always the risk of producing a trapdoor effect and its donor site is less easily closed. The wound has to be turned into a V-shaped defect in order to have a linear scar, and the flap has therefore no merit over the V-flap, unless two U-flaps are raised in continuity with each other, creating a visor flap. By this technique, tissues can be safely transposed directly as well as indirectly to the area where they are needed.
C-flap The C-flap (3.14) requires the undermining of a large surface in order to close a relatively small receptor site. Its rotation is facilitated by a backcut, creating a donor defect that can be closed by advancement of the edges or by transposition of a V-flap as a Zplasry. Indications for the C-flap are, however, limited. Owing to its shape, planning is difficult and the direction of the final scar at the receptor site may turn o ut to be at right angles to the eyelid rim. This problem can be solved by the incorporation of a second Zplasty, as advocated by the first author. A 'derotation' effect is thus produced.
0-flap The 0-flap (3.15 ) undoubtedly has the widest range of motion . Raising it requires attention to detail and good knowledge of the vascularization. The flap is best designed in an elliptical fashion if scarring in donor and receptor sites is to be minimized.
V-flap A V-flap obviously has the best chance of success. It blends well with the receptor site and the donor site is easily closed. While generally transposed directly, the flap may occasionally be used in an indirect transposition procedure.
The composite arterial flap that remains attached to the eyelid rim on one side of its base is an example of such a V-flap. Since it is rotated over 180°, it can close a defect in the other eyelid; its pedicle is severed after sufficient time has elapsed. Its value and versatility are best illustrated by the technique that never ceases to intrigue a plastic surgeon, the Z-plasty.
TECHNIQUES OF Z -PLASTY
The Z-plasty is one of the best weapons in a battle for perfection. It enables the redistribution of tissue by the transplantation of two symmetrical or asymmetrical flaps and the reorientation of a scar within tension lines by elongation, fragmentation, and rotation. The ease with which a flap can be rotated and tissue can be redistributed is determined by the initial orientation of its base in relation to the lines of tension and the size of its apical angle.
Equal Z-plasty In its most practical form a Z-plasty is performed by the juxtaposition of two V-shaped flaps with equal limbs and equal apical angles of 60° (3.16). Together these flaps form a rhombus with diagonals that cross at right angles, the long diagonal joining the extremities
39
of the lateral limbs and the short diagonal, which is 73% shorter than the long one, coinciding with the common central limb.
After transposition of two flaps at 60°, this orientation will differ by 30° from its original direction, and a gain in length of the short diagonal or central limb will be obtained at the expense of the long diagonal. The result is a new rhombus identical in form but with a different orientation because of the interchange of the two diagonals.
The Z-plasry with 60° flaps is the only one in which the direction of shortening is at right angles to the direction of the lengthening. In every other Z-plasry the diagonals are askew. The transposition of fl aps with an angle size beyond 60° will result in a greater gain in length bur the mobility of the fl aps will be less. In contrast, transposition of equal flaps with angles of less than 60° will produce progressively less gain.
Unequal Z-plasry In a design with unequal angles, t he behaviour o f the numerous angle combinations is dictated by the mobility of one or both flaps (3 .17). The narrower the base of a flap and the smaller its apical angle, the greater its mobility. The broader a flap, the more immobile it becomes. When the angle of one flap reaches 90°, shortening and lengthening will totally depend on the mobility of the other flap.
- -
3.16 Equal Z-plasty.
3.17 Unequal Z-plasty.

ORBITAL SuRGERY
Multiple Z-plasty A combination of smaller flaps instead of one large Z-plasty offers the advantage that tissue is borrowed more diffusely from the surrounding areas (3.18). However, the degree of shortening and lengthening produced by these techniques is similar.
Bisected Z-plasty Interchange of flaps with angles of 90° or more is impossible, owing to their lack of mobility. One way to overcome this problem and use flaps with angles up to 120' is to bisect the two flaps into four with equal angles of 60', which can then be transposed with more ease (3.19).
Opposing Z-plasty The use of two opposing Z-plasties (3.20) may be indicated in areas where particular attention needs to be paid to the direction of the resulting scars in relation to the lines of tension. The possibility of using one common lateral limb in Z-plasties with unequal angles is an important advantage of this technique.
While the mathematical indices throughout the whole range of variations and combinations are well known, they are of little practical value. The qualities of skin and particularly of scarred skin are not the same as those of paper, and the knowledge that the expected gain in length with a Z-plasty can be found by calculating the difference between the short and the long diagonal is not really helpful.
-
3.18 Multiple Z-plasties.
There are, however, some guidelines for optimal planning. 1. The first and most important is that the direction of the lateral
limbs should follow the tension lines as much as possible. If this is done correctly, at least two of the three scars will be in an optimal position in spite of some changes in orientation. The third will run in an acceptable direction.
2. The second guideline is that for the formation of these limbs, use should be made, if possible, of already existing scars.
3. The third guideline is that the flaps should be planned within a certain region to avoid dislocation of landmarks.
When planning is difficult, it is better to raise one flap first and to transpose it in the required direction before deciding on position and direction of the second lateral limb.
INDICATIONS FOR Z-PLASTY
The closure of a defect In the planning of a Z-plasty for closing a defect, several aspects must be considered. 1. The shape of the defect. A wide variety of defects may be
observed, but in the context of resurfacing procedures, the rhomboidal and triangular defects are the most important.
3.19 Bisected Z-plasty. 3.20 Opposing Z-plasties.
40

SURGICAL PRINCIPLES
2. The form and size of the flap in relation to the defect which must be obliterated.
3. The degree and direction of the distortion that is produced by the redistribution of tissues and its effect on the position of the adjacent landmarks.
4. The number and length of scars and their orientation in relation to the tension lines.
Rhomboidal defects After resection of a tumour, the defect to be closed will quite frequently be shaped as a rhombus with its long diagonal within the direction of the tension lines. Such a defect can be closed in several ways .
A well-known technique is to design a Z-plasty with its central limb in continuity with the short diagonal of the rhombus and one lateral limb parallel to one of the edges of the defect. The rhomboidal flap so planned will provide accurate closure of the defect, but some distortion in the direction of the tension lines will occur and the orientation of two of the resulting scars will inevitably cross the lines of tension.
Theoretically, malorientation of scars can be prevented by the use of another principle described by Limberg for the correction of a contracture, in which a Z-plasty is bisected with two obtuse angles of 120° (see 3.19), but this procedure has not been recorded as having been applied for the closure of a defect.
A better procedure, because the skin is more evenly distr ibuted, is to close the rhombus with the double Z-rhombic technique (3.21). Perfect obliteration with an acceptable orientation of the scars can then be achieved. Unfortunately it is not possible to use two opposing Z-plasties when the position of the rhomboidal defect is close to the eyelid rim.
In such a situation, tissue can be borrowed from only one site, forcing the surgeon to use the Z-plasty with the incorporated rhombic flap.
Triangular defects Triangular defects or colobomas are among the most common defects in the orbital region. They may be caused by the removal of tissue or by the contracture of a scar. In the presence of a scar contracture, the position of the Z-plasty is more or less directed by that of the contracture, but in the absence of such a scar the same principle as used in the resurfacing of a rhomboidal defect can be applied (3 .22), because it is made of two triangular defects.
b - b
3.21 Closure of rhomboidal defect.
41
Of the three alternatives that have been discussed, one in particular is useful - the Z-plasty with its central limb marked as an extension of one of the sides of the triangle. One lateral limb is formed by the other side and the second lateral limb determined by the form of the defect. This alternative has several advantages -the transposed flap fits perfectly into the defect and there is no distortion in the direction of the tension lines. The orientation of the scars remains acceptable.
The correction of contractures Contractures are a frequent phenomenon in the orbital region. They may be caused by the redistribution of tissue, producing relaxation in the direction of the contracture, or by the reorientation of the scar within the tension lines. The original scar is in fact broken up into three smaller scars producing lower contractile force.
A scar that crosses the tension lines at right angles or at an angle or more than 60° can best be improved by flaps angled at 60°, with the postoperative central diagonal placed in an optimal position (parallel to the tension lines), at the same time producing an important gain of length.
If the angle between tension lines and scar is 60° or less, the lateral limb should follow these lines as closely as possible. Depending on the type of scar, the following modifications of a Z-plasty can be applied: • Multiple Z-plasties achieve a more diffuse redistribution of tis
sues and are therefore useful in long scars. • Unequal Z-plasties are indicated when tissue on one side of a scar
is contracted while being loose on the other side. • The shorter side can then be lengthened by an incision almost
at right angles to the central limb of the Z-plasty. The resulting defect can be closed with a more acutely angled V-flap from the other long side.
• Bisected Z-plasties may show their value when there is severe contracture. Redistribution of tissue is however extreme, entailing a distinct risk of distortions.
• Opposing Z-plasties are indicated when correction of a semicircular scar, fold, or plication is indicated.
The relocation of a landmark The use of Z-plasties is also effective in the relocation of landmarks. Displacement of the canthi may be corrected by transposition in a cranial, caudal, medial, or lateral direction and similar procedures may be indicated for the treatment of a dystopic eyebrow.
-
3.22 Closure of triangular defect.

ORBITAL SURGERY
TRANSPLANTATION AND T RANSPOSITION OF TISSUES
Tissue grafts may be used for two purposes: • For resurfacing of a cutaneous or mucosal defect. • For resroration of a skeletal defect. Skin grafts are best harvested in the upper eyelid or in the rerroauricular area (3.23 ). Full thickness grafts have an excellent colour match and contraction is minimal. Full thickness grafts have been shown to be excellent material for resurfacing of fornices and socket defects. Contraction is minimal.
In general, split thickness grafts should not be used in the orbital area, since discoloration and contraction tend ro be severe. However, in major defects caused by burns, thick split thickness grafts may be indicated .
Mucosal grafts are best raised in the buccal area (3 .24). Cartilage grafts provide optimal tissue for the augmentation of
volume defects. Resorption is virtually non-existent. The ribs offer the best donor sire (3.25).
Bone grafts can be harvested from several areas, the skull and the iliac crest being most commonly used.
3.23 Retroauricular skin graft.
3.25 Cartilage graft.
========-- --
Split thickness skull grafts (3.26) are nowadays advocated by many craniofacial surgeons but resorption of bone can be significant and donorsite morbidity occurs not infrequently.
Donor areas Optima l reconstruction of a defect requires replacement of the lost parts with tissues that match these in quality and quantity. Replacement should not be associated with loss of function, distortion of landmarks, or conspicuous scarring in the donor site. This means that tissue should be borrowed only from donor sites with a relative surplus and that priority should always be given to sires with the best quality match. In this respect the eyelid itself cannot be surpassed. But if this donor sire is not available, the following tissues should be considered: • The frontal skin. • The galea. • The subgaleal fascia. • The temporalis fascia. • The temporalis muscle. • The retroauricular skin.
3.24 Buccal mucous me mbrane graft.
3.26 Split sku ll graft.

SURGICAL PRINCIPLES
®
© @
\ 3 .27 Forehead flaps: a Superficial temporal artery nourishing island f lap; b Sickle flap; c Scalping fl ap; d Median forehead flap.
Frontal skin The forehead (frontal skin) (3.27) has been used in a number of ways for lid and socket reconstruction. As originally described by Esser and later by McGregor, virtually the whole of the forehead can be elevated based on one superficial temporal artery. However, a flap that includes half of the forehead and that is based on the contralateral superficial temporalis artery is long enough to reach the orbita l area. The scalping flap of Converse (3.27c) provides an example of this technique. Alternative procedures are the sickle flap first reported by New and the island flap advocated by Esser.
Major disadvantages of using frontal skin are its thickness and lack of pliability, the possible damage caused to the frontalis branch of the facial nerve, and the fact that it is a conspicious donor area.
The flap described by Leonard preserves frontalis action and cosmesis as well as making for a thinner more pliable flap. The median forehead flap, based on the supraorbital and supratrochlear artery, can be used for smaller defects, but the amount of skin available, unless pre-expanded, is limited.
The galea The galea (3.28) is the layer immediately below the cranial dermis, to which it is intimately interconnected with fibrous septa. Strictly, the name 'galea' should be reserved for its central part- the aponeurosis between the fronta l and occipital muscles. Its lateral part has had several names applied to it, the temporoparietal fascia and the
\ 3.28 Galea flap.
43

ORBITAL SURGERY
® Temporalis muscle --~
1-\-----T emporo-parietal fascia
Line of fusion ----1
Deep layer----l
Superficiallayer -----+t""'-:1
Temporal fat pad Superficial -----tf':c'l
Deep from buccal fat---+
Posterior masseteric fascia
Frontal branch of facial nerve
Zygomatic arch
Fascia
Parotid-masseteric
3.29 Temporal is branch of facial nerve. a Lateral view (modified after Zide and Jelks: Surgical Anatomy of the Orbit. New York: Raven Press, 1985). b Path of dissection advocated by Stuzin (1989).
superficial temporal fascia being the most important. Abdul Hassan has described the anatomy of the fascial layers well. The temporoparietal fascia is supplied by the superficial temporal artery, which runs on its surface.
The flap is large and pliable and can easily be transposed to the orbital region. Its elevation is tedious, requiring great care but donor site morbidity is minimal.
Technique The course of the superficial temporal artery and its main branches is established by palpation and Doppler ultrasound. An incision 12-14 em long is then made parallel to the course of the vessels, taking care to protect them. The edges of this incision are adequately undermined at a level just below the hair follicles, exposing the fascia.
An axial pattern flap 4-5 em wide is then demarcated and incised down to the level of the pericranium in the distal part of the flap and down to the level of the temporalis fascia in its proximal part. Extension of the flap beyond the midline is possible. The flap is mobilized. A tunnel is made between the donor and recipient sites and the flap pulled through. The distal part of the flap is inserted into the orbital defect and the scalp incision is sutured.
In order to preserve the seventh nerve, which travels within and along the undersurface of the temporoparietal fascia, Ellis et at. advocate a superficial and lateral tunnel or a deep and medial tunnel since the nerve runs from a deep tissue plane at the zygomatic arch to a superficial plane at the lateral orbital rim . Dissection in the plane between the temporal fascia and the loose areolar subgaleal fascia affords maximal protection to the frontal branch of the facial nerve.
The nerve is at greatest risk of injury when subperiosteal exposure of the arch is required. In such cases, Stuzin et at. recommended a safer alternative by placing the plane of dissection beneath the superficial layer of the temporal fascia (3 .29).
44
The subgaleal fascia The loose areolar layer beneath the temporoparietal fascia has been shown to exist as a separate vital structure that can be dissected from the adjacent superficial and deep layers. Like the temporoparietal fa scia, the subgaleal fascia receives its blood supply from the main blood vessels that enter the scalp at its periphery and divide proximally (the supratrochlear artery, the supraorbital artery, and the superficial temporal artery).
Because of this, its potential as an independent donor site to be used separately or in combination with adjacent layers (bilaminar or trilaminar) has been recognized, though unfortunately there are still drawbacks. The dissection is difficult and in their quest for bulk and safety, most surgeons will choose to harvest a compound fascial flap that includes tissue from both the temporoparietal and the subgaleal fascias.
The temporalis fascia The temporalis fascia (3.30) overlies the temporalis muscle. Superiorly it blends with the pericranium. Inferiorly, at the level of the superior orbital margin, it divides into two layers- a superficial layer attaching to the lateral border of the zygomatic arch and a deep layer attaching to the medial border.
The temporalis fascia is supplied by the middle temporal artery. It is much more readily elevated than the temporoparietal flap. However, it is not so large and rotation is cumbersome. Therefore it is to be used only as a donor site for grafts.
Technique An incision approximately 6-10 em long is made within and parallel to the hairline, anterior to and above the ear. The wound is deepened and its edges are raised sufficiently widely to expose the temporalis fascia. An outline of the graft is drawn- a piece mea-

SURGICAL PRINCIPLES
Temporal musc le and fascia
3 .30 Temporal is fascia flap.
suring 6 em x 3 em is needed to cover an 18 mm implant. When used as a patch, a surface of 2.5 em x 1.5 em is required. The graft is easily dissected and the wound closed in layers.
Temporalis muscle The temporalis muscle (3.31) is supplied from its deep surface by the deep temporal artery. It is a large muscle that is readily elevated and has sufficient bulk to be brought through the lateral wall of the orbit for volume filling following exenteration. Its arc of rotation makes it unsuitable for eyelid reconstruction.
Technique A hemicoronal incision is made and deepened to expose the temporalis muscle lying deep to temporal fascia, the superolateral rim of the orbit, and the zygomatic arch. The temporalis fascia is separated from the temporal crest and the lateral rim of the orbit, leaving a margin of pericranium for future attachment.
Both sides of the lateral orbital wall are then exposed and a hole drilled in its lateral aspect to create an opening behind the lateral orbital rim. The periorbita is incised in a direction parallel to the lateral orbital rim.
The temporal muscle flap is then divided into anterior and posterior segments. The anterior segment is pulled through the defect in the lateral orbital wall, into the orbital cavity. Excess tension and compression should be avoided. To prevent hollowness of the temporal donor site, the posterior segment of the temporal muscle is attached to the lateral orbital rim.
Retroauricular flap Washio based his technique on the existence of a watershed between two major blood supplies. The ingenious flap that he described allows the transport of postauricular hairless skin to the facial
45
3.3 1 Temporalis muscle flap.
region. The quality and quantity of skin available is excellent; however, it is a multi-staged technique and it gives the patient a very bizarre appearance after the first stage.
The donor site requires a skin graft. Island flaps have been described by Guyuron (one stage) and van der Meulen (two stage). Unfortunately, the vascularity of these flaps is not sufficiently reliable because the retroauricular portion of the flap has a random vascularity.

ORBITAL SURGERY
Technique FIRST STAGE
First, the course of the superficial temporal artery and its posterior branch must be established by palpation and by Doppler study. The steps are illustrated in 3.32. Measure the distance from point A directly in front of the tragus to the medial canthus. This is usually approximately 12 em. Then draw a semicircle over the temporal area with point A as its centre and half the distance between A and the medial canthus (approximately 6 em) as its radius.
Mark a point B where the semicircle crosses the hairline. The base of the flap is the line AB.
A line is then drawn in the preauricular and supra-auricular folds, starting at point A and extending in a cephalad and slightly posterior direction. The point at which this line crosses the semicircle already marked is designated point C, thereby forming an equilateral triangle with CB as base, and AC and AB as sides. Washio considered these three points, A, B and C, to be the key in designing his flap.
A second semicircle is drawn in the supra-auricular area with point Cas its centre and a radius of again 6 em by placing D equidistant from B and C. A second equilateral triangle is thereby formed, with CB as base and BD and CD as sides.
Turn the second semicircle into a question mark and delineate the borders of the retroauricular portion of the flap. Incise the margins of the fiap and raise it by carefui dissection between the pericranium and the galea in the supra-auricular area and by elevation of the skin with the underlying fascia in the retroauricular area.
Injury to the superficial temporal artery is avoided by continuous inspection while the flap is being lifted.
The pedicle of the flap is fo lded twice: first along the line AB, turning its raw surface outward, then along the line BC, resulting in the formation of a tube with D covering A and its direction pointing forward. The extremity of the flap should reach beyond the medial canthus to avoid tension.
... - ... ...
~~ d----+-~d
3.32 Retroauricular flap (Washio's procedure).
--------o==========e=-
SECOND STAGE
The pedicle is separated in the hair-free border at the level of the lateral orbital rim, unfolded and returned to its original position. The split skin area that is covered by the flap is resected and the flap is sutured to the edges of the defect.
Retroauricular island flap (3.33) First establish the course of the superficial temporal artery and its posterior branch by means of palpation and Doppler ultrasound. A retroauricular flap with a surface as large as 6 em x 5 em is then designed. Cephalad to this design a triangular scalp area is delineated and depithelialized, thereby exposing the galea while preserving the posterior branch of the superficial temporal artery. The base of this triangle, made about 3 em wide, marks the upper border of the retroauricular flap. The length of the triangle is approximately 6-7 em.
The retroauricular skin flap and the depithelialized scalp area are raised at the subfascial level and the pretriangular and preauricular skin are carefull y incised and elevated over the course of the superficial temporal artery, permitting the dissection of the retroauricular flap to be continued. This dissection should include the nourishing vessels together with a safe margin of fascia approximately 2 em wide. A cephalad cutback directly above the helix and 2 em long makes it possible to increase the length of the pedicle.
Injury to the posterior branch of the superior temporal artery should of course be avoided. The flap is deiivered to the orbital area through a subcutaneous tunnel.
ORBITAL OSTEOTOMIES
Deliberate osseous sections serve a dual purpose. They can be used to provide temporary access to a cavity or they can be performed to correct an abnormal contour. Their effect is then of a permanent nature. The bones are cut with saws (reciprocating or oscillating), osteotomes or chisels. Rigid fixation of the mobilized portions of bone is essential for good consolidation .
3.33 Retroauricu lar island flap (Guyuron's procedure).
=:F===========-- - --

SURGICAL PRINCIPLES
Approach The bicoronal subperiosteal dissection defined as la route panoramique by Tessier gives excellent access to the orbital contours. Only the exposure of the inferior orbital margin and of the orbital floor is difficult with this approach, and a direct approach through the lower eyelid is generally combined to achieve a safe and complete dissection of the inferior part of the orbit. Detachment of the lateral and medial canthal ligaments permits a complete exposure.
Access Craniotomy The temporary removal of a bony plate exposes the dura mater and provides access to the anterior cranial fossa. The plate may be mobilized as a bone graft or as a flap pedicled on the ipsilateral temporal muscle in order to preserve its blood supply via the pericranium.
Orbitotomy Temporary removal of a part of the orbital wall is a very old practice. It can be used to provide better access to the posterior part of the orbit in trauma or tumor surgery.
Contour correcting osteotomies The cranial vault Orbital malformations are frequently associated with anomalies of the vault. To correct these, cranial segments can be raised, permitting mobilization in every spatial direction. Transposition, rotation, and reversal of the bony parts make it possible to give a deformed portion of the vault a normal curvature.
The orbitofrontonasal band (3.34) After the craniotomy the osteotomy continues lateral to the frontomalar junction with the formation of a tongue in groove, a spur or a Z-plasty in the frontosphenoidal area. These extensions provide stability and the use of a bone graft can thus be avoided. After traversing the smaller wing of the sphenoid and the orbital roof in
3.34 Frontonasal band.
47
its posterior third, the cut curves forward, avoiding the olfactory groove and passing the midline at the level of the foramen caecum. A horizontal frontonasal section extending in the medial orbital walls to join the cut in the orbital roof completes the osteotomy.
Mobilization of the band requires special attention -laterally, in the orbital pillar, the temporal lobe must be protected; medially, the integrity of the nasal lining and the olfactory tracks must be preserved.
The design of the osteotomy permits much freedom. The superior orbital rim may be removed or remodelled. The band may be moved forward or rotated downwards. It may be split in the middle to permit differential movement of each lateral part and it may be bent to correct abnormal contour using multiple cuts.
Total orbital osteotomies (3.35) Osteotomies of the orbit involve only its anterior ring (the 'movable orbit' or orbit utile described by Tessier). Mobilization is performed at two different levels: one anterior osteotomy around the orbital rim and one posterior inside the cavity. Anteriorly the cut is made horizontally in the supraorbital region. It runs parallel to the inferior edge of the craniotomy and extends somewhat laterally. The bar thus preserved later serves as a line of reference and a site of fixation for the transposed orbit. The malar bone is cut vertically or obliquely to a point slightly below the level of the infraorbital foramen. The incision is continued horizontally in the maxillary body towards and into the pyriform aperture below the inferior concha. It is completed by a second vertical cut through the nasal roof and through the frontal sinus.
At a posterior level the movable orbit is mobilized by a circular osteotomy, which starts in the inferior orbital fissure and is carried up into the anterior cranial fossa. At the pterion, the cut is divided into an external cut, which joins with the lateral extension of the supraorbital osteotomy to form a spur, and an internal cut, which runs across the orbital roof and continues downwards in the medial wall.
This part of the osteotomy is completed by a cut that traverses the orbital floor to join the inferior infraorbital fissure.
3.35 Total orbitotomy.

ORBITAL SURGERY
®
@
3.36 Partial orbitotomy.
Partial osteotomy (3.36) The movable orbit can be divided into four segments: • Mediofrontal segment; • Laterofrontal segment; • Maxillary segment; • Malar segment. These segments can be moved separately or in combination. The term 'one-quadrant osteotomy' is applied when one of these fragments is mobilized. AU-osteotomy or two-quadrant osteotomy may be used when two adjacent quadrants are moved as one unit.
There are four types of U-osteotomies: • Cranial or superior; • Subcranial or inferior; • Nasal or medial; • Temporal or lateral.
Interorbital osteotomy (3.37) Movement of the orbits towards the midline requires the removal of a segment of bone in the frontonasal area. This segment is more often triangular than rectangular.
A superior horizontal cut is first made in continuity with the supraorbital osteotomy. Inferiorly and medially directed oblique cuts pass through the frontal sinuses in their upper part, entering the cranial fossa. In their lower part they cut through the nasal bones and the ethmoid sinus.
An inferior horizontal dissection is carried out between the rim of the nasal bones and the triangular cartilages. This serves to sep-
®
3.37 Interorbital resection .
arate the mucosa from the nasal roof anterior to the olfactory tracts. The nasal bones are removed, exposing and preserving the mucous domes.
The central bony block can then be mobilized by a transverse cut through the floor of the anterior cranial fossa at the site of the fron-

SURGICAL PRINCIPLES
3.38 Orbitomaxillary osteotomy: different varients proposed by Tessier.
toethmoidal junction and through the septum. The exenteration of the interorbital region is completed by the resection of the deformed part of the septum and the ethmoid sinus. The integrity of the olfactory nerves is preserved.
Orbitomaxillary osteotomy (Lefort Ill) A coronal incision is the principal route of access for the orbitomaxillary osteotomy (3.38). Additional routes are provided by bilateral inferior palpebral incisions. The dissections expose the malar bones, the orbits, and the nasal roof. Detachment of the medial canthal tendon may therefore be required.
Access to the pterygomaxillary junction is obtained via vestibular or palatine incisions. The lateral wall of the orbit is divided transversely at the frontomalar suture line. Posteriorly the line of osteotomy is carried downwards into the infraorbital fissure.
Sectioning is then continued in two directions: medially the osteotomy traverses the orbital floor and the medial wall of the orbit behind the lacrimal fossae to reach the frontonasal suture; laterally and downwards, it runs across the posterolateral wall of the maxilla into the pterygoid groove area, where disjunction may be performed in a variety of ways. Position and direction of the cut in the malar area are dictated by the specific requirements of the case.
In the sagittal plane, the perpendicular plate of the ethmoid and the vomer are severed with the osteotome through the transverse cut at the nasofrontal junction. While performing these steps, it is extremely important to keep clear of the cribriform plates. The mobilization manoeuvres are performed with disimpaction forceps.
49
3.39 Frontofacial osteotomy.
The frontofacial monobloc osteotomy The frontofacial monobloc osteotomy (3.39) was first advocated by Ortiz-Monasterio in 1978. With this procedure it is possible to advance the maxillomalar complex and the orbitonasofrontal band as a single unit.

ORBITAL SURGERY
3.40 Facial bipartition (split-face osteotomy).
To avoid communication of the cranial with the nasal cavities and adjacent sinuses and to prevent infection by maintaining the integrity of the anterior cranial fossa and supraorbital bar, the original technique was modified in 1983 by Ander!, who advocated differential advancement of the forehead and maxilla.
The hemifacial monobloc osteotomy (3.40) This technique, known by the name of medial faciotomy (facial bipartition, or split face), was first described by van der Meulen in 1976 and 1979. A completely midpalatal osteotomy enables the surgeon to advance and rotate one or both facial halves and thus correct orbital hypertelorism at the same time.
MEDIAL CANTHUS
The medial canthus is where the upper and lower eyelid meet each other in one important anatomical structure, the medial canthal tendon. This band is anchored to the anterior crest of the lacrimal fossa covering and protecting the lacrimal sac. The course of this anatomical landmark may vary from one that is strictly lateromedial to one that runs in a more posteroanterior direction over the surface of the nasal bone. The fixation of the eyelids to the bone by this structure is enforced by a second band that is located behind the lacrimal sac, inserting more posteriorly.
The area superior to the medial canthus is characterized by a valley (the superiomedial angle) which separates the adherent skin over the nasal skeleton from the looser skin covering the superior part of the upper eyelid.
The intimate relationship of the structures that make up the medial canthal region is reflected in the variety of deformities that may be
so
observed. In principle, these can affect the maso-orbital skeleton, the medial canthal tendon, the nasal skin, and the lacrimal apparatus.
Reconstruction of the medial canthal area by means of a canthopexy is complicated by several factors . First, there is the difficulty involved in the reinsertion of the medial canthal tendon in its proper position, i.e. deep behind a line connecting the corneas. Accuracy is most important here and failure to achieve a good result is mainly due to technical problems.
The position of the canthal insertion makes it awkward to burr a transnasal tract from one side of the nose to the other through these areas, and pressure on the eye may be difficult to avoid with the apparatus that is normally used. Many surgeons therefore perforate the nasal bone and septum with an awl- a somewhat gruesome procedure.
The second complicating factor is the tendency of the canthal insertion to become detached. This phenomenon probably has its origin in the continuous traction of the orbicularis muscle. This traction will have linle effect when the canthopexy is performed according to the principles outlined here but fa ults in technique will inevitably result in telecanthus. The procedure is as follows (3.41).
A hole is bored at the site of insertion of the canthal tendon or more posteriorly with a diameter sufficiently wide to allow the tendon to enter as deeply as possible. The tendon is identified and secured with a monofilament ethylon 3-0 suture, leaving both ends long.
Two holes are drilled on the contralateral side parallel to and just below the bridge of the nose. The direction of the canals should be such that the tip of the burr becomes visible in the hole that was previously made.
Two hollow needles are passed through these canals, which serve as guides for the ends of the sutures. The needles are then withdrawn and the procedure is concluded by tying a firm knot.
The third complicating factor is the problem associated with the reconstruction of the upper canthal sulcus. Separating the skin and periosteum or the periosteum and bone by sharp dissection or avulsion may have important consequences for the integrity of this area. The following chain of events may be observed.
Once healing is in progress, the lateral traction of the orbicularis muscle will cause remodelling of scar tissue and loss of adherence between the tissues covering the nasal skeleton. The lateral pull of the orbicularis muscle may join forces with the downward pull of gravity, causing even more relaxation of tissues. The production of fibrous tissue may be enhanced by this traction, and occasionally in young children new bone may even be formed between periosteum and skeleton. Inevitably the upper inner canthal valley will disappear, causing important asymmetry.
THE LATERAL CANTHAL AREA
In contrast to the complexity of the medial canthal area, where three different anatomical planes meet each other at varying angles, there is only one such plane in the lateral canthal area. This simplicity is reflected in the severity of the abnormalities in this region, which, like those in the medial canthal region, may affect the skeleton, the canthal tendon, and the skin, but which are usually easier to correct.
Like its medial counterpart, the lateral canthal tendon consists of a deep and a superficial bundle. The deep bundle runs intraorbitally and has its insertion in the periosteum of Whitnall's tubercle immediately behind the orbital rim. The superficial bundle extends more anteriorly and attaches to the periosteum of the frontal process of the malar bone and the temporal aponeurosis.

SURGICAL PRINCIPLES
®
3.41 Medial canthopexy.
If the insertion of the lateral canthal tendon is disrupted by dissection of the periorbit or by a canthotomy in eyelid reconstruction, medial dislocation and rounding of the lateral canthus may result. The same deformity may be seen when the lateral canthal area has been reconstructed following its avulsion or resection but no canthopexy has yet been performed. The distortion is either caused or maintained by the traction of the orbicularis muscle and it may be so severe that vision in a lateral direction is prevented. It must therefore be corrected.
The procedure is as follows (3.42). Two small holes are drilled in the lateral wall of the orbit, directly behind the rim at a site opposite Whitnall's tubercle. The lateral canthal tendon is secured with a monofilament ethylon 3-0 suture and both ends are left long. Two hollow needles are passed through the holes that have been made and the ends of the tendon suture are inserted in the tips of these needles. The needles are withdrawn as soon as the ends of the tendon suture become visible at the other end of the needle. The procedure is concluded with a firm knot. 3.42 Lateral canthopexy.
SI

ORBITAL SURGERY
Temporal sagging caused by laxity of the lateral canthal tendon or the eyelid itself is a deformity commonly seen in patients with a loss of muscular tonus. It also occurs as a result of pressure when a prosthesis is worn. Correction of the laxity and restoration of the canthus can be obtained by resection of a small edge from the eyelid rim and a transosseous canthopexy, as described above.
However, similar results may be obtained when the eyelid rim is fixed to the periosteum orbital of the wall with a small tarsal strip or held in position by the transposition of a small periosteal flap raised over the lateral orbital wall.
BIBLIOGRAPHY
EVALUATION
GUnther H. Hypertelorismus. Endokrinologie. 1933a;13:61-72. GUnther H. Konstitutionelle anomalien des augenabstandes und des interor
bitalbreite. Virschows Archiv Abteilung 1933b;A 290:373. Hansman CF. Growth of interorbital distance and skull thickness as observed
in roentgenographic measurements. Radiology 1966;86:87. Johr P. Tableaux de mensurations des distances oculaires et craniennes.journa/
de Genetique Humaine 1953;2:247 Laestadius ND, Aase JM, Smith DW. Normal inner canthal and outer orbital
dimensions. Journal of Pediatrics 1969;74:405 Pacioli L. Divine Proportione. Venice: Paganini. della Porta GB. De hunana physiognomonia. Vico Equense: Cacchio. Ricketts RM. Divine proportion in facial esthetics. Clinics in Plastic Surgery
1982;9A01. Roman us T. Interocular-biorbital index. A gauge of hypertelorism. Acta
Genetica 1953;4:117.
SOFT TISSUES
Abdul-Hassan HS, von Drasek Ascher G, Acland RD. Surgical anatomy and blood supply of the fascial layers of the temporal region. Plast Reconstr Surg 1986;77;17-28.
Antonyshyn 0, Gruss JS, Birr JD. Versatility of temporal muscle and fascial flaps. Br J Plast Surg 198 8;4 );118-131.
Argenta LC, Friedman RJ, Dingman RO, Duus EC. The versatility of pericranial flaps. P!ast Reconstr Surg 1985 ;76:695-702.
Avelar JM, Psillakis JM. The use of galea! flaps in craniofacial deformities. Ann Plast Surg 1981;6A64-469.
Bakamjian VY, Souther SG. Use of temporal muscle flap for reconstruction after orbito-maxillary resections for cancer. Plast Reconstr Surg 1975;56:171.
Baker DC, Conley]. Avoiding facial nerve injuries in rhytidectomy: anatomic variations and pitfalls. Plast Reconstr Surg 1979;64:781.
Beare RLB. Flap repair following exenteration of the orbit. Proc Royal Soc Med 1969;62;1087.
Becker FF. Rhomboid flap in facial flap in facial reconstruction. Arch Otolaryngol1979;105;569.
Borges AF. Elective Incisions and Scar Revision. Boston: Little, Brown, 1973. Borges AF. The rhombic flap. Plast Reconstr Surg 1981;67:458. Borges AF, Alexander JE. Relaxed skin tension lines, Z-plasties on scars and
fusiform excision of lesions. Br J Plast Surg 1962;15:242. Borges AF, Alexander JE, Bvlock Ll. Z-plasty as an adjunct to straight advance
ment flaps.] /nt Call Surg 1965;44;198. Brent B, Upton], Acland RD, et al. Experience with the temporoparietal fascial
free flap. Plast Reconstr Surg 1985;76:177. Byrd HS. Temporoparietal (superficial temporal artery) fascial flap. In: Strauch
B, Vasconez LO, Hall-Findlay EJ (eds). Encyclopedia of Flaps, Volume 1. Boston: Little, Brown, 1991:27-31.
Carstens MH, Greco RJ, Hurwitz D], Tolhurst DE. Clinical applications of the subgaleal fascia. Plast Reconstr Surg 1991;87:615-626.
52
Medial and lateral canthus Loss of the muscular tonus or persistent pressure of the prothesis on the lower eyelid may cause sagging.
Correction can be achieved by a small variety of suspension procedures. A temporal fascial strip, a dermal or tendon graft or even a myocutaneous flap from the upper eyelid is used to shorten the distance between the canthi and to tighten the lid.
Casanova R, Cavalcante D, Grotting ]C, Vasconez LO, Psillakis JM. Anomatic basis for vascularized outer-table calvarial bone flaps. Plast Reconstr Surg 1986;78;300.
Chayan D, Nathan H. Anatomical observations on the subgaleotic fascia of the scalp. Acta Anat 1974;87:427.
Chiarelli A, Baldelli A, DiVincenzo A, Martine G. Utilization of the superfacial temporoparietal fascia in reconstructive plastic surgery. Ophthalmic Plast Reconstr Surg 1989;5:274.
Correia PC, Zani R. Surgical anatomy of the facial nerve as related to ancillary operations in rhytidoplasty. Plast Reconstr Surg 1973;52:549.
Cullen KW, Meyer M. Eyelid reconstruction using temporalis fascia. Ophthalmic Plast Reconstr Surg 1989;5:271.
Cuono CB. Double Z-plasty repair of large and small rhombic defects: the double-Z rhomboid. Plast Reconstr Surg 1983;71:658.
Cutting CB, McCarthy JG, Berestein A. Blood supply of the upper craniofacial skeleton; the search for composite calvarial bone flaps. Plast Reconstr Surg 1984;74o603-608.
Dufourmentel C. Le fermeture des pertes de substance cutanee limitees. Le lambeau de rotation en L pour losange, dit 'LLL'. Ann Chir Plast 1962;7:61.
Ellis DS, Toth BA, Stewart WB. Temporoparietal fascial flap for orbital and eyelid reconstruction. Plast Reconstr Surg 1992;89:606-612.
Esser A Rotation der Wange und allgemeine Bemerkungen bei chirurgischen Gesischtsplastik. Leipzig: Vogel, 1918.
Fonseca]. Use of pericranial flaps in scalp wounds with exposed bone. Plast Reconstr Surg 1983;72:786-790.
Fukuta K, Jackson IT, Coli ares MV, et al. The volume limitation of galea temporalis flap in facial augmentation. Br] Plast Surg 1991;44:281-284.
Furnas DW. Landmarks for the trunk and the temporofacial division of the facial nerve. Plast Reconstr Surg 1965;52:694.
Gahlos NF, Cuono, CB. Double-Z rhombic technique for reconstruction of facial wounds. Plast Reconstr Surg 1989:869-877.
Guyuron B, Labandter HP, Berlin AJ. Fasciocutaneous flap, secondary axial pattern flap and micro-vascular free flap in socket reconstruction. Ophthalmology 1984;91:94.
Gustafson J, Larrabee WF Jr, Borges AF. Experimental analysis of the adjunctive Z-plasty in the closure of fusiform defects. Arch Otolaryngol 1984;110Al.
Har-Shai Y, Fukuta K, Collares MV, et al. The vascular anatomy of galea! flap in the interparietal and midline regions. Plast Reconstr Surg 1992;89;64-69.
Holmes AD, Marshall KA. Uses of the temporalis muscle flap in blanking out orbits. Plast Reconstr Surg 1979;63:336.
Holt JE, Holt GR, Van Kirk M. Use of temporalis fascia in eyelid reconstruction. Ophthalmology 1984;91;89.
Horowitz, JH, Persing JA, Nichter LS, Morgan RF, Edgerton MT. Galeal-pericranial flaps in head and neck reconstruction: anatomy and applications. Am J Surg 1984;148A89.
Jackson IT, Adham MN, Marsh WR. Use of the galea! frontalis myofascial flap in craniofacial surgery. Plast Reconstr Surg 1986;77:905.
Jervis Wet al. Further applications of the Limberg and Dufourmentel flaps. Plast Reconstr Surg 1974;54:335.

BIBLIOGRAPHY
Kaplan IB, Gilbert DA, Terzis JK. The vascularized fascia of the scalp.] Reconstr Microsurg 1989;5:7-15.
Leonard AG. The forehead flap: minimising the secondary defect by preservation of the frontalis muscle. Br J Plast Surg 1983;36:322-326.
Liebman EP, Webster RC, Berger AS, Della Vecchia M. The frontalis nerve in the temporal brow lift. Arch Otolaryngoll982;108:232.
Limberg AA. Design of local flaps. In: Gibson T (ed). Modern Trends in Plastic Surgery, 2nd edition. London: Butterworths, 1966:38-61.
Limberg AA. Panimetrie und Stereometric der Hautplastik. Jena: Fischer, 1967. Limberg AA. Plastic interchange of triangular flaps. Odontol Stomatal
1928;L74. Limberg AA. Mathematical Principles of Local Plastic Procedures on the Surface
of the Human Body. Leningrad: Medgiz, 1946. Lister GD, Gibson T. Closure of rhomboid skin defects: The flaps of Limberg
and Dufourmentel. Br] Plast Surg 1972;25:300. McCarthy JG, Zide BM. The spectrum of calvarial bone grafting: Introduction
of the vascularized calvarial bone flap. Plast Reconstr Surg 1984;74:10. McGregor IA. Fundamental Techniques of Plastic Surgery. Edinburgh:
Livingstone, 1960. McGregor lA. The temporal flap in intra-oral cancer: its use in repairing the
post-excisional defect. Br J Plast Surg 1963;16:318. .Mercer DM. The cervicofacial flap. Br J Plast Surg 41:470--474. Mitz V, Peyronie M. The superficial musculo-aponeurotic system in the parotid
and cheek area. Plast Reconstr Surg 1976;58:80. Montandon D, Marty FD, Gumener R, et al. Subcutaneous tissue in the scalp:
anatomical, physiological and clinical study. Ann Plast Surg 1986;16;368-376.
New GB. Total rhinoplasty using a forehead flap. Plast Reconstr Surg 1946;1;271.
Ozersky D, Baek SM, Biller HF. Percutaneous identification of the temporal branch of the facial nerve. Ann Plast Surg 1980;4:276.
Pitanguy I, Silviera Ramos A. The frontal branch of the facial nerve: the importance of its variations in face lifting. Plast Reconstr Surg 1966;38:352~356.
Psillakis JM, Grotting JC, Casanova R, Cavalcante D, Vasconez LO. Vascularized outer-table calvarial bone flaps. Plast Reconstr Surg 1986;78309.
Robbins TH. The protection of the frontal branch of the facial nerve in face-lift surgery. Br J Plast Surg 1981;34:95.
Roggendorf E. The oblong parallelogram-shaped 'Schwenklappen' plasty. Plast Reconstr Surg 1980;65:635.
Rose EH, Norris MS. The versatile temporoparietal fascial flap: adaptability to a variety of composite defects. Plast Reconstr Surg 1990;85:224.
Shagets FW, Panje WR, Shore JW. Use of the temporalis muscle flaps in complicated defects of the head and face. Arch Otolaryngol Head Neck Surg 1986;112;60.
Smith RA. The free fascial scalp flap. Plast Reconstr Surg 1980;66:204-209. Stewart WB, Levin PS, Toth BA. Orbital surgery: the technique of coronal scalp
flap approach to the lateral orbitotomy. Arch Ophthalmof 1988;106:1724. Stuzin JM, Wagstrom L, Kawamoto HK, Wolfe SA. Anatomy of the frontal
branch of the facial nerve: The significance of the temporal fat pad. Plast Reconstr Surg 1989;83:265.
Tegtmeier RE, Gooding RA. The use of a fascial flap in ear reconstruction. Plast Reconstr Surg 1977;60:406.
Tolhurst DE, Carstens MH, Greco RJ, Hurwitz DJ. The surgical anatomy of the scalp. Plast Reconstr Surg 1991;87:603.
Tremolada C, Candiani P, Signorini M, Vigiano M, Donati L The surgical anatomy of the subcutaneous fascial system of the scalp. Ann Plast Surg 1994;32;8-14.
Washio H. Retroauricular-temporal flap. Plast Reconstr Surg 1969;43:162-166. Wilson JSP, Westbury G. Combined craniofacial resection for tumour involv
ing the orbital walls. Br] Plast Surg 1973;26:44. Wolfe SA. The utility of pericranial flaps. Ann Plast Surg 1978;1:146-152.
SOLID TISSUES
Anderl H, MUhlbauer W, Twerdy K and Marchac D. Frontofacial advancement with bony separation in craniofacial dysostosis. Plast Reconstr Surg 7];303,1983.
53
Converse JM and Wood-Smith DAn Atlas and Classification of Mid-Facial and Craniofacial Osteotomies. In Transactions of the Fifth International Congress of Plastic and Reconstructive Surgery, Melbourne, 1971. Melbourne: Butterworths, 1971. Pp. 931-962.
Converse JM, Ransohoff J, Mathews ES, Smith B, Molenaar A 1970 Ocular hypertelorism and pseudohypertelorism. Advances in surgical treatment. Plastic and Reconstructive Surgery 45: 1
Converse JM, Smith B 1962 An operation for congenital and traumatic hypertelorism. In: Trostman RC, Converse JM, Smith B (eds) Plastic and Reconstructive Surgery of Eye and Adnexa. Butterworth, Washington DC.
Converse JM, Telsey D 1971 The tripartite osteotomy of the midface for orbital expansion of the deformity iri craniostenosis. British journal of Plastic Surgery 24: 365.
Firmin F, Coccaro PJ, and Converse JM. Cephalometric analysis in diagnosis and treatment of craniofacial dysostoses. Plast Reconstr Surg 54: 300, 1974.
Gillies HD and Harrison SH. Operative correction by osteotomy of recessed malar maxillary compound in a case of oxycephaly. Br] Plast Surg. 2: 123, 1950.
Jackson IT 1984 Orbital hypertelorism. In: Serafin D, Georgiade NG (eds) Pediatric plastic surgery. Mosby, StLouis, pp. 467--498 .
Jackson IT, Munro IR, Salyer KE, Whitaker LA 1982 Atlas of craniomaxillofaciaf surgery. Mosby, StLouis.
Marchac D 1978 Radical forehead remodelling for craniostenosis. Plastic and Reconstrructive Surgery 61: 823.
Marchac D and Renier D. Early Monobloc Frontofacial Advancement. In Proceedings of the First International Congress of the International Society of Craniomaxillofacial Surgery, La Napoule, 1985. Berlin: Spinger-Verlag, 1987.Pp. 130-136.
Marchac D, Cophignon ], Achard E eta!. 1977 Orbital expansion for anophthalmia and micro-orbitism. Plastic and Reconstructive Surgery 59:486.
Marchac D, Dufourmentel C 1974 A propos des osteotomies d'advancement du crane et de la face. Annales de Chirurgie Plastique 19:311.
Marchac D, Renier D 1979 Le front flottant. Trraitement prCcoce des faciocdniostenoses. Annales de Chirurgie Plastique 24: 121.
Marchac D, Renier D 1982 Craniofacial surgery for craniosynostosis. Little, Brown, Boston, p.114.
McCarthy J G, Coccaro P J, Wood-Smith D, Converse J M 1979 longitudinal cephalometric studies following surgical correction or orbital hypertelorism: a preliminary report. In: Converse J M, McCarthy J E, WoodSmith D (eds) Symposium and diagnosis and treatment of craniofacial anomalies. Mosby, StLouis, 229.
McCarthy], Coccaro P J, Epstein F, Converse J M 1978 Early skeletal release in the infant with craniofacial dysostosis. Plastic and Reconstructive Surgery 62; 335.
McCarthy JG and Cutting CB. The timing of surgical intervention in craniofacial anomalies. Clin Plast Surg, 17:161, 1990.
McCarthy JG, LaTrenta GS, Breitbart AS, Zide BM and Cutting CB. Hypertelorism correction in the young child. Plast Reconstr Surg 1990;86.1: 214-225.
Motoki DS, Altobelli DE and Mulliken JB. Enophthalmos following orbital transposition for craniofacial malformations. Plast Reconstr Surg 1993; 91.1;416-422.
Muhlbauer W, Anderl Hand Marchaac D. Complete Frontofacial Advancement in Infants with Craniofacial Dysostosis. In Transactions of the Eighth International Congress of Plastic and Reconstructive Surgery, Montreal, 1983. Pp. 318-320.
Munro IR, Chir B, Das SK 1979 Improving results in orbital hypertelorism correction. Annals of Plastic Surgery 2: 6.
Murray JE and Swanson LT. Midface osteotomy and advancement for craniosynostosis. Plat Reconstr Surg 41: 299, 1968.
Ortiz-Monasterio F, Fuente del Campo A and Carrillo A. Advancement of the orbit and the midface in one piece, combined with frontal repositioning for the correction of Crouzon's deformities. Plast Reconstr Surg 61: 507, 1978.
Psillakis JM, Zanini SA, Godoy R, Cardim VLN 1981 Orbital hypertelorism: modification of the craniofacial osteotomy line. Journal of Maxillofacial Surgery 9: 10.
Stricker M, eta!. Craniofacial Malformations. New York: Churchill Livingstone, 1990.

ORBITAL SURGERY
Tessier P 1972 Orbital hypertelorism. I. Successive surgical attempts, material and methods, causes and mechanism. Scandanavian Journal of Plastic and Reconstructive Surgery 6: 135.
Tessier P 1973 The definitive treatment of orbital hypertelorism by craniofacial or extra cranial osteotomies. Scandanavian journal of Plastic and Reconstructive Surgery 7: 39.
Tessier P, Guiot G, Rougerie J, Delbet ]P, Pastoriza] 1967 Osteomies crania nasa orbito faciales- Hypertelorism. Annales de Chirurgie Plastique 12.
Tessier P. Dysostoses Cranio-Faciales. In Transactions of the Fourth International Congress of Plastic and Reconstructive Surgery, Rome, 1967. Pp. 774-783.
Tessier P. Osteotomies totales de la face: Syndrome de Crouzon, syndrome d' A pert. Oxycephalies, scaphocephalies, turricephalies. Ann Chir Plast 12: 273, 1967.
Tessier P. The definitive plastic surgical treatment of the severe facial deformities of craniofacial dysostosis Crouzon's and Apert's diseases. Plast Reconstr Surg48' 419,1971.
van der Meulen JC The Pursuit of symmetry in craniofacial surgery. British journal of Plastic Surgery 1976;29: 85~91.
54
van der Meulen JC Medical faciotomy. British Journal of Plastic Surgery 1979; 32,339.
van der Meulen JC and Vaandrager JM. Surgery related to the correction of hypertelorism. Plast Reconstr Surg 1983;71:6.
van der MeulenJC, Hauben DJ, Vaandrager JM, Birgenhager-Frenkel DH 1984 The use of a temporal osteoperiosteal flap for the reconstruction of malar hypoplasia in Treacher Collins syndrome (Vol 74, No.5), pp 687-693.
van der Meulen ]C. Discussion of hypertelorism correction in the young child. Plast Reconstr Surg 1990;86.1: 226~228.
van der Meulen JC, Zonneveld FW. Discussion of enophthalmos following orbital transposition for craniofacial malformations. Plast Reconstr Surg 1993; 91.1A23-428
Whitaker LA, Bartlett SP, Schut Land Bruce D. Craniosynostosis: An analysis of the timing, treatment, and complications in 164 consecutive patients. Plast Reconstr Surg 80: 195, 1987.
Whitaker LA, Katowitz ]A, Jacobs WE 1979 Ocular adnexal problems in craniofacial deformities. Journals of Maxillofacial Surgery 7: 55.