Embed Size (px)
Citation preview

5
Chapter 2: Mechanical Circulatory Support Systems, a review
Abstract Congestive Heart Failure (CHF) is a major health problem with a high mortality rate. Its ultimate therapy, heart transplantation, is limited by the shortage of donor hearts. Since decades researchers have been working to solve this problem by developing Mechanical Circulatory Support Systems (MCSS) that can replace or assist the failing heart.
Short-term and intermediate-term ventricular assist devices are used nowadays frequently to bridge patients with severe heart failure to recovery. Long-term ventricular assist devices (VADs) and Total Artificial Hearts (TAHs) are used increasingly as a bridge to heart transplantations or as permanent circulatory support in patients with end-stage heart failure that are contraindicated for heart transplantation. The early TAHs and VADs were mainly driven from an external pneumatic drive unit. The latest generation TAHs and long-term assist devices are electrically powered, ultracompact, totally implantable, and have small wearable drive/control consoles, allowing patients to return to their daily activities.
The article categorizes and reviews the development of MCSS, highlights the medical indications and contraindications of pump implantation, advantages and disadvantages of the various systems, and results of animal and clinical studies.
Technology and Health Care (submitted)

Chapter 2
6
Introduction Congestive Heart Failure (CHF) affects about 4,600,000 people in the United States1. It is marked by an extraordinary poor prognosis: median survival, following onset of CHF, is 1.7 years for men and 3.2 years for women2. Heart transplantation, the most effective therapy for end-stage heart failure, is limited due to the shortage of donor hearts. It is estimated that in the United States yearly 20,000 patients need heart transplantation while only 2,000 donors heart become available3. As a consequence, about 90% of these patients cannot be transplanted. Moreover, the heart condition of some patients may worsen so badly, while they are in the waiting list, that they may develop a multi-organ failure, which makes them contraindicated for heart transplantation. Nowadays, the period a patient needs a donor heart and the moment a donor heart becomes available can be bridged with Mechanical Circulatory Support Systems (MCSS). During those mechanical bridging the condition of the patient can be stabilized or even be improved4. On the other hand, the increased duration of MCSS implantation suggests that this could be an alternative to the heart transplantation. MCSS avoid the risks associated with immunosuppression and rejection, and could be produced in the quantities required to treat all the patients who might otherwise die before receiving a donor heart5.
Many patients that suffer from left ventricle heart failure (LVHF) and who do not respond sufficiently to pharmacological therapy still have the potency to recover from their illness. This group includes patients that went into cardiogenic shock after heart surgery or after myocardial infarction. They represent 2-6 % of all patients who undergo an open-heart surgery6. MCSS assist the pump function of the heart, unload the left ventricle, and generate enough blood flow to guarantee adequate organ perfusion to maintain organ functions of these patients. Recent experience showed evidence for myocardial recovery after prolonged LV mechanical assist in patients with end-stage heart failure7-9. Those results suggest that the LV assist is not only an established mechanical support for the failing ventricle, but may become an alternative therapy for management of the heart failure as well.
This article is mean to give a review of the development of MCSS, from experimental developments to clinical applications, in order to emphasize the possibilities that these devices can offer to the clinicians to treat patients with end-stage heart failure.
MCSS can be divided into several groups according to the type of assist (left, right, or biventricular assist), quality of generated flow (pulsatile or non-pulsatile), time-

MCSS
7
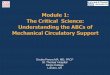
limitation (short-term, medium-term, or long-term), work-principle (electrohydraulic, pneumatic), etc. The easiest way to categorize MCSS is based on the need of native heart replacement. Therefore the MCSS are divided into two categories (Fig. 1): Total Artificial Heart (TAH) and Ventricular Assist Devices (VADs).
1.1. Pneumatic TAH 1.2. Electric TAH
1. Total Artificial Heart (TAH)
2.1. Intra-Aortic Balloon Pump
2.2.1. Roller pumps
2.2.2. Centrifugal pumps
2.2.3. Axial pumps
2.2. Non-pulsatile VADs
2.3.1. Pneumatic
2.3.2. Electric
2.3. Pulsatile VADs
2. Ventricular Assist Devices (VADs)
Mechanical Circulatory Support Systems (MCSS)
Fig. 1. Classification of Mechanical Circulatory Support Systems
1. Total Artificial Heart The TAH consists of two blood pumps that are implanted orthotopically, i.e., positioned in the place of the patient’s native heart within the pericardium. Because the device replaces the native heart, it can either be used temporary as a bridge to transplantation or permanent as a real artificial heart. The required cardiac replacement is the major difference between a TAH and VADs. When a VAD fails, the limited pump function of the native heart could still keep the patient alive. If a TAH fails however, the patient has a great chance to die within minutes.
The first experimental TAH implantation was reported by Akutsu and Kolff in 195810. Their pneumatically driven TAH was able to keep a dog alive for a period of six hours. In 1969 Cooley introduced the concept of a two-staged cardiac replacement and performed the first clinical TAH implantations as a bridge to transplant11. Fourteen years later, in 1983, first implantation of TAH as a permanent replacement of the native human heart was reported12. From 1969 to 1991 a number of 230 Total Artificial Hearts (TAHs) were implanted at 39 centers worldwide, using eleven different devices13. Nowadays the use of TAH as a mechanical circulatory support has become an established procedure for bridging patients with cardiomyopathy to cardiac transplantation. In patients with contraindications for heart transplantation the TAH serves as a permanent heart replacement.
The first generation TAHs were all pneumatically driven and possessed similar design characteristics6. They consisted of two blood pumps, each composed of a rigid blood chamber and an air chamber. The membrane, separating the blood from the air, was moved by air derived from an external drive unit. The air tubes

Chapter 2
8
that connect the TAH with the driver pass through the skin. Artificial valves, positioned in the inflow and outflow tract, ensure unidirectional flow.
To implant a TAH a sternotomy and cardiopulmonary bypass are required. The native ventricles are separated from their atria by cutting through the atrioventricular groves14. The aorta and pulmonary artery are cut just distal to the semilunar valves. Quick connectors are sutured to the remains of the native atria, aorta and pulmonary artery, both pumps are carefully de-aired, and the TAH is brought into place. When the TAH is started the cardiopulmonary bypass is decreased gradually. After a pump rate of about 80 beats per minute is reached the cardiopulmonary bypass is stopped.
1.1. Pneumatic Total Artificial Hearts
Until 1990 the Jarvik 7 was the most widely used TAH. With this device, named for its designer Robert Jarvik, a patient was kept alive for 620 days6. However, due to mismanagement and a high incidence of thromboembolic complications Jarvik 7 was withdrawn from the market in the early nineties15. Currently CardioWest (CardioWest, Tucson, AZ, USA) has taken over the production of the Jarvik 7. The pump is marketed as CardioWest TAH and has now become the only pneumatic TAH that is still used in the USA as a bridge to transplantation6. The CardioWest TAH has been implanted in 79 patients for up to 186 days, demonstrating a survival rate of 91% of the patients who reached transplantation16. However, to receive the CardioWest TAH as a bridge to transplant, the company handles strict criteria. The patients should not be younger than 18 or older than 59 years, possess a body surface area ≥ 1.7 m2, and a cardiac index < 2.0 L/min/m2. Moreover, the patients should be supported with two inotropic agents or one inotropic agent plus Intra Aortic Balloon Pump17.
1.2. Electric Total Artificial Hearts
In general pneumatic assist devices show a high incidence of infections, mainly caused by the percutaneous drivelines, which makes this devices unsuitable as a permanent artificial heart. Therefore, the second generation of TAHs was focused on the realization of a totally implantable, wireless electrically powered TAH. However, with existing techniques the electric TAH requires a minimum energy supply of 14 watts, which cannot be provided by implantable batteries yet6. For that reason new developments are aimed at improvement of rechargeable battery techniques and a wireless energy transmission. With wireless energy transmission the electrical energy is transferred from a primary (external) coil to a secondary (internal) coil with 70% efficiency and with no open connection through the skin15.

MCSS
9
In this way the implanted rechargeable battery will be used only as a back-up power source for about 40-60 minutes. An external console ensures device control.
In 1993 the US National Institutes of Health (NIH) granted a program for the development of an electrically powered TAH. The centers involved include Abiomed (Abiomed, Inc., MA, USA) in conjunction with the Texas Heart Institute, Nimbus (Nimbus, Inc., Rancho Cordova, CA, USA) with the Cleveland Clinic Foundation, and Sarns (Sarns 3M Health Care, MI, USA) with the Pennsylvania State University15.
The Abiomed/Texas Heart Institute TAH, known as AbioCor™ (Abiomed, Inc., MA, USA), uses a high-speed brushless direct-current motor that powers a unidirectional centrifugal pump15. A rotary valve ensures that the fluid of this electro-hydraulic device actuates first the right ventricle and then the LV, thus generating an alternating emptying of the blood chambers. A small chamber placed in line between the left atrial cuff and the inflow valve manages the physiologic left-right flow difference18. The thermal, physiologic, and hematological compatibility of the system was verified during long-term animal studies (> 100 days), which also demonstrated that the Abiomed TAH could provide cardiac output greater than 10 L/min19.
The Nimbus/ Cleveland Clinic Foundation TAH uses also a high-speed brushless direct-current motor and hydraulic actuator to drive two diaphragm-type blood pumps20. The space between the two artificial ventricles, containing the pump control electronics, is vented to an air-filled compliance chamber placed between the lung and the chest wall. Pericardial tissue valves and biolized blood-contacting surfaces potentially eliminate the need for anticoagulation20. The device, tested in calves for a period of up to 120 days, has a maximum output of 9.5 L/minute21.
The Sarns/Pennsylvania State University TAH uses a low-speed high-torque brushless direct-current motor and a dual pusher plate roller screw energy converter15. The blood pumps consist of highly smooth segmented polyurethane sacs with Björk-Shiley Delrin disk inlet and outlet valves. The gas-filled compliance chamber is similar to that used in the Nimbus/ Cleveland Clinic Foundation TAH. Used as a complete heart replacement, the device was capable to keep experimental animals alive for more than 13 months15.
2. Ventricular Assist Devices The VADs are mechanical blood pumps that can support or replace the function of the failing left ventricle, right ventricle, or both ventricles. The VADs do not require removal of the native heart and therefore can be used as a bridge to

Chapter 2
10
transplantation as well as a temporary support system in patients with expected myocardial recovery.
Left ventricular assist with a roller pump was introduced by Dennis in 196222. In 1971 DeBakey reported successful LV assist of patients who could not be weaned from the heart-lung machine23. Nowadays the mechanical assist of the failing ventricle is commonly used in patients with cardiogenic shock. The indications for mechanical circulatory support are hemodynamic deterioration before transplantation (i.e. bridge to transplantation), acute myocardial infarction, postcardiotomy cardiogenic shock, transplanted heart failure, or cardiac rejection24.
As mentioned before, according to the supported site, the VADs can be divided into three main groups: • Left ventricular assist devices (LVADs): blood is withdrawn from either the
pulmonary veins, left atrium or the apex of the LV and returned to the ascending aorta. Atrial cannulation is easier to perform and is less traumatic for the heart in comparison to the apical cannulation. Therefore the left atrial cannulation is preferred for a temporary LV support. However, a LV cannulation via the apex provides better LV unloading and better VAD performance25. For that reason the apical cannulation is preferred for LV assist as a bridge to transplantation.
• Right ventricular assist devices (RVADs): blood is withdrawn from the right atrium and returned to the main pulmonary artery.
• Biventricular devices (BiVADs): the BiVADs are actually a combination between LVAD and RVAD, and could be seen as a functional heart replacement.
Additionally, the VADs can be categorized into Intra-Aortic Balloon Pump (IABP), non-pulsatile and pulsatile VADs (Fig. 1).
The type of ventricular support as well as the device used differs from patient to patient according to the experience and individual preference of the surgical team and the perspective for ventricular recovery. Except the IABP, the most frequently implanted devices in Europe are the pneumatic VADs, followed by TAH, centrifugal pumps, and the electromechanical VADs24.
The main complications during the mechanical assist are bleeding and infection. Other complications include renal failure, respiratory failure, neurological impairment, and embolic events24.

MCSS
11
2.1. Intra-Aortic Balloon Pump
The Intra-Aortic Balloon Pump (IABP) is the most commonly used assist device for temporary support of the failing left ventricle after cardiac surgery26. The method, based on initial studies from Kantrowitz and Kantrowitz27, was described by Moulopoulos in 196228. The first successful clinical application of an IABP was reported by Kantrowitz at al. in 196829. The applicability of the IABP was significantly improved by the development of a percutaneous insertion technique for the balloon30. This technique made the IABP insertion possible not only in the operating room, but also in ICU and cardiac catheterization lab.
The IABP consists of a catheter-mounted polyurethane balloon connected to a driving system. The catheter is introduced percutaneously into the descending thoracic aorta via the femoral artery, with balloon positioned just distal (approximately 2 cm) to the left subclavian artery. The balloon can be introduced also directly into the aorta if the chest is open, e.g., during heart surgery. The device works on the principle of counterpulsation, i.e., assisting the heart in series synchronously with the patient’s ECG. The balloon is automatically inflated during begin of diastole, increasing the diastolic aortic pressure which in turns increases the coronary flow. During the systole the balloon is deflated, decreasing LV afterload, which in turns decreases the myocardial oxygen consumption, and increases cardiac output. Helium is chosen as driving gas because its low viscosity allows rapid movement and therefore fast inflation and deflation of the balloon.
LV support with IABP is indicated for treatment of cardiogenic shock in acute heart failure or after myocardial infarct31, and for treatment of heart failure after open-heart surgery32. IABP could be used as prophylaxis preoperative in high-risk patients undergoing coronary artery bypass grafting33, during high-risk percutaneous transluminal angioplasty (PTCA)34, or as intraoperative LV support for patients with cardiac disease undergoing noncardiac surgery35. LV assist with IABP is contraindicated if aortic valve insufficiency or aortic dissection is present.
Despite the superiority of VADs in terms of circulatory support, IABP remains the clinician's first choice in postcardiotomy low output syndrome either alone or in combination with VAD36. IABP is available almost everywhere and the balloon can be inserted into the aorta within minutes. The insertion as well as the removing of the balloon does not require major surgery. The device is easy to control, thus a specialized personnel is not needed to operate and control the system. IABP increases coronary artery perfusion and reduces ischemic ventricular dysfunction, mitral regurgitation, and the pulmonary capillary wedge pressure6. Early use of IABP reduces significantly mortality and morbidity in both cardiac surgery and

Chapter 2
12
cardiology patients36. A preoperative insertion of the IABP in high-risk elderly patients undergoing coronary artery bypass grafting led to results comparable to those in lower risk patients33. IABP therapy, used as an adjunct to conventional medical treatment, can give in properly selected young children with low cardiac output syndrome after heart surgery more than 50% chance of long-term survival37.
However, the IABP has disadvantages as well. Severe kinking or arteriosclerosis of the iliac or femoral artery could make the insertion of the balloon impossible. In such a case the subclavian artery could be used as an alternative introduction place38 or the IABP could be inserted into the ascending aorta. Vascular complications include perforation of the aortic wall39,40, aorto-iliac dissection38, limb ischemic complications39,41 leading to above-knee amputations32, etc. Infectious and bleeding complications were reported as well42. Unlike the true blood pumps, the IABP depends on residual LV function and therefore has only minor effects in patients with profound hemodynamic compromise43. Last, it should be kept in mind that IABP works properly only if the patient’s ECG is optimal. As a result, the system fails during severe arrhythmia or during fibrillation. In such a case the IABP could be synchronized with the aortic pressure instead of patient’s ECG.
2.2. Non-pulsatile Ventricular Assist Devices
According to the mechanical characteristics, the non-pulsatile VADs can be divided into 3 categories: roller pumps, centrifugal pumps, and axial pumps (Fig. 1).
2.2.1. Roller pumps
The roller pumps are similar to the pumps used for cardiopulmonary bypass. The inflow and outflow cannula are connected by tubing made partially of silicone rubber. The silicone part is placed in a head with rotating occlusive rollers. During the head rotation, the tubing is compressed repeatedly by the rollers and a unidirectional non-pulsatile blood flow is generated.
The roller pumps are simple to use and are relatively inexpensive devices. There are available in every cardiac surgery [e.g., Stöckert roller pump (Stöckert Instrumente GmbH, München, Germany)] and the cannulas used are the same as those used for cardiopulmonary bypass. However, the roller pumps have some major disadvantages: requirement of systemic anticoagulation, blood trauma leading to hemolysis, tubing spallation and fatigue, non-pulsatile or low-pulsatile flow, requirement of constant supervision, etc. Those limitations preclude use of the roller pumps beyond few hours or days6.

MCSS
13
2.2.2. Centrifugal pumps
Centrifugal pumps consisted of non-occlusive pump head positioned within a rigid pump housing. The rotating head consists of a various number of impeller blades that generate a non-pulsatile unidirectional flow by creating a vortex. Centrifugal pumps do not require artificial valves. The most used centrifugal pumps worldwide are the BioPump (Medtronic BioMedicus, Inc., Eden Prairie, MN, USA), the Sarns centrifugal pump (3-M Health Care, Ann Arbor, MI, USA), and the St. Jude Medical Lifestream centrifugal pump (St. Jude Medical, Chelmsford, MA, USA). The Carmeda BioPump (Medtronic BioMedicus, Inc., Eden Prairie, MN, USA), also known as BioActive BioPump, has the same appearance as the BioPump, but has heparin covalently bonded to the blood exposed surfaces.
Centrifugal pumps, like the roller pumps, are simple to use and inexpensive. In contrast to the roller pumps however, the centrifugal pumps are pressure limited, virtually eliminating the potential for air aspiration or tubing disruption6. Moreover, the centrifugal pumps are less destructive to blood cellular elements and cause significantly lower hemolysis, when compared with the roller pumps44,45. As a consequence, the centrifugal pumps have replaced roller pumps in 30% of routine cardiac surgery procedures, especially for procedures that are more prolonged46. The centrifugal pumps are currently used for a short-term mechanical cardiac assist, often as RVAD in combination with a pulsatile LVAD47. However, experimental studies demonstrated that some centrifugal pumps could be used beyond this period as well. For example, one of the most advanced centrifugal magnetically suspended impeller pump, the Terumo-Akamatsu device, has been functioning well in a sheep for over two years48.
The major disadvantage of the centrifugal pumps is the non-pulsatile flow, which is less desirable than the pulsatile flow49 and the relatively low pressure difference that can be bridged50.
2.2.3. Axial blood pumps
Hemopump
The Hemopump (Medtronic, Inc., Minneapolis, MN, USA) is a catheter-mounted transarterial transvalvular LVAD that can be used for short-term LV support. The device, described in 1988 by Wampler et al51, works on the principle of the Archimedes screw, rotating at up to 25,000 rotations/minute. The impeller, integrated into the aspiration cannula, is activated by a flexible cable connected to an external high-speed electromotor. The tip of the cannula is positioned into the LV via the femoral artery or via the ascending aorta. Blood is withdrawn from the

Chapter 2
14
LV and discharged into the descending aorta, providing non-pulsatile flow. For that reason, during the assist, the arterial pressure curve became flat52.
The Hemopump has been available in three variants: a 14-French version for percutaneous insertion, a 21-French version for introduction via graft anastomosed to the femoral artery, and a 26-French version (Sternotomy Hemopump) for direct introduction into the ascending aorta. The 14-French variant is designed for LV support during high-risk PTCA and allows flows up to 1.5 L/min. The 21-French variant allows flows up to 3.5 L/min. The sternotomy variant (26-French) allows flows up to 4.5 L/min. The last variant is useful in patients who cannot be weaned from cardiopulmonary bypass or in patients with severe peripheral vascular disease.
Hemopump is indicated as a short-term LV support of patients in cardiogenic shock after open-heart surgery52 and for performing coronary artery bypass graft operation on the beating heart without cardiopulmonary bypass53. The devise was used in the past as a LV support in patients undergoing high-risk coronary angioplasty as well43. Contraindications for Hemopump implantation include the presence of an artificial aortic valve as well as the presence of thrombi in the LV.
The Hemopump combines the direct LV unloading, typical for LVAD, with the fast and simple transarterial implantation of the IABP. In contrast to IABP, the Hemopump is not synchronized with the patients ECG and therefore works properly even during severe arrhythmia or cardiac fibrillation. Many physicians are concerned about the possibility of severe hemolysis during the Hemopump assist. The level of plasma free hemoglobin indeed increases during the initial period of assistance, but within the first 24 hr decreases and stabilizes near normal54.
Like the IABP, the percutaneous implantation of the Hemopump could be problematic in patients with severe peripheral arteriosclerosis or kinking, especially if a larger cannula is used. For example, Wiebalck at al. reported unsuccessful effort to insert 21-French Hemopump via the femoral artery in 6 out of 18 patients55. However, in 4 of these 6 patients an IABP was successfully inserted. Last suggests that an implantation of the 14-French Hemopump could be successful. The major complications during the assist are related to mechanical pump failure, such as fracture of the drive cable and expulsion of the cannula out of the ventricle55. The Hemopump, if not running, can induce substantial regurgitation through the pump into the left ventricle.
Although still used clinically in Europe, the Hemopump is not longer in production and is not currently available in the United States56.

MCSS
15
MicroMed DeBakey VAD™
The MicroMed DeBakey VAD™ (MicroMed Technology, Inc., Houston, TX, USA) is an axial flow pump jointly developed with Dr. Michael DeBakey and the National Aeronautics and Space Administration (NASA). The pump is 86-mm long, 25-mm wide (about the size of an AA battery), and weighs 95 grams57. Because of its small size, the device may be used both as a LVAD and RVAD.
The inflow cannula of the pump is attached to the ventricle or placed into or through the atrium. The outflow cannula (Dacron graft) is attached to the ascending aorta or pulmonary artery respectively. The only moving part of the device is an inducer-impeller. The pump can produce up to 6 L/minute flow at about 10,000 rotations/minute, and requires less than 10 W of power57. DeBakey VAD™ was tested in calves for up to 145 days58. From November 1998 to December 1999 the device was implanted in 19 patients with end-stage heart failure at six clinical trial sites in Europe. In February 1999 the company announced the first successful heart transplantation after 75 days of DeBakey VAD™ implantation.
Jarvik 2000 Heart
The Jarvik 2000 Heart (Jarvik Research, Inc., New York, NY, USA), named for its designer Robert Jarvik, is a compact axial flow impeller pump. The device is inserted through a sewing cuff into the left ventricle via the apex. The outflow Dacron graft is anastomosed to the descending thoracic aorta. The pump is 25 mm in diameter, 55 mm long, weights 85 gram, has a displacement volume of 25 ml, and provides up to 8 L/minute blood flow at 8,000 to 12,000 rotations/minute9. The rotor, positioned in a titanium shell, is suspended in each end by tiny, blood-immersed ceramic bearings. The pump has an energy requirement of 7 to 10 watts, delivered from external batteries. A percutaneous titanium pedestal transmits the electrical wires trough the skin of the scalp59. Jarvik 2000 heart was tested in sheep for up to 198 days demonstrating negligible hemolysis9.
Impella Pump
Impella intracardiac pump (Impella Cardiotechnik AG, Aachen, Germany) is designed for use in coronary bypass surgery, eliminating the need of heart-lung machine. The device can be used for complete bypass of the left ventricle, right ventricle, or both ventricles for a maximum period of 6 hours. The pump has an internal diameter of 6.4 mm and can be inserted directly, or through the peripheral vessels. Impella pump has a capacity of 4.5 L/minute at physiological pressures. Pump control is simplified by means of a touch-screen in combination with a multi-function key. Surgery data are recorded and are subsequently available at an external PC.

Chapter 2
16
Nimbus Innovative Ventricular Assist System (IVAS)
The Nimbus IVAS (Nimbus Inc., Rancho Cordova, CA, USA, a wholly owned subsidiary of Thermo Cardiosystems, Inc.) is an axial flow blood pump jointly developed with Nimbus Inc. and the University of Pittsburgh under a five-year contract funded by the National Institute of Health. The system, now designated as HeartMate II, uses a transcutaneous energy transformer system (TETS) and a diagnostic telemetry system60. The inflow cannula is inserted into the LV through the apex. The outflow cannula is positioned into ascending aorta. In order to minimize the requirements for anticoagulation, all blood-contacting surfaces of the pump are textured, like the pneumatic and electric versions of HeartMate (Thermo Cardiosystems, Inc., Woburn, MA, USA). The pump, tested in calves for up to 226 days, demonstrated basic reliability and biocompatibility and did not produce significant alterations in the mechanical properties of blood or animal health status61.
2.3. Pulsatile Ventricular Assist Devices
All pulsatile pumps are basically membrane pumps in which the membrane is moved by air, liquid or by a pusher-plate. The driving source (air, water or electricity) reaches the pump via a tube trough the skin. The most often used indication of these devices is bridging to transplantation62. Pulsatile pumps operate in various pump modes: ECG synchronous, ECG asynchronous, and a fulfill-full empty mode. During the ECG synchronous mode, the pump action is synchronized with the heart action by a R-wave detector. This allows the device to eject the aspirated blood into ascending aorta during the diastolic phase, thus increasing aortic diastolic pressure, coronary flow, and myocardial perfusion. During the ECG asynchronous mode the device operates in a fixed pump frequency.
Pulsatile pumps show many advantages to other pump systems. First, these devices generate a pulsatile flow. The pulsatile flows reduce sympathetic nerve activity and peripheral vascular resistance, thus improving the microcirculation as well as organ function50. Most pulsatile devices do not require continuous supervision from a technician. Furthermore, the pulsatile VAD cause less blood trauma then both roller and centrifugal pumps6.
The major disadvantages of the pulsatile pumps are the high cost, due to the required heart valves and the high cost of the driving system, and complexity of the pump design.

MCSS
17
2.3.1. Pneumatic Pulsatile Ventricular Assist Devices
Abiomed BVS 5000
The Abiomed Biventricular Support (BVS) 5000 (Abiomed, Inc., Danvers, MA, USA) is an external cardiac support system that can be used for short-term left, right or biventricular support. The device consists of an automated driving console and disposable dual-chamber blood pumps. The pumps contain a filling chamber (artificial atrium) and a pumping chamber (artificial ventricle), situated between two trileaflet polyurethane valves63. The first valve is positioned between the artificial atrium and artificial ventricle. The second valve is between the artificial ventricle and the outflow graft. Each chamber contains a 100-ml polyurethane blood sac. The artificial atrium, positioned at the top of the pump, fills passively during pump diastole and systole. The artificial ventricle, positioned at the bottom of the pump, is emptied by compressed air. One drive console can support one or two ventricles. The device operates in asynchronous full-to-empty mode with a maximum stroke volume of 82 ml63. To prevent thrombus formation, systemic anticoagulation is required.
Abiomed BVS 5000 is completely automatic and therefore does not require trained personnel to control the pump continuously. Food and Drug Administration (FDA) approval has been granted for the device to be applied in patients with postcardiotomy heart failure. Used in more than 500 patients worldwide Abiomed BVS 5000 demonstrated improved wean rate and discharge rate when compared with a non-pulsatile device64. The device can provide complete cardiac support allowing full myocardial recovery and has the potential to improve the survival rate of patients with reversible acute myocardial damage63,65.
HeartMate 1000 Implantable Pneumatic (IP)
The HeartMate 1000 IP (Thermo Cardiosystems, Inc., Woburn, MA, USA) is a totally implantable pneumatically driven blood pump designed for left ventricular support only. The pump consists of titanium housing (10.2 cm in diameter, 5.1 cm thick) with a flexible polyurethane diaphragm inside bonded to a rigid pusher plate. Blood is withdrawn from the LV via the apex and is returned to the ascending aorta. Porcine valves are placed in the inflow and outflow conduits to ensure unidirectional blood flow. A percutaneous air driveline connects the pump to an external console. The pump can operate either in a fixed-rate mode (20-140 beats/minute) or in an automatic mode. In the automatic mode, the device ejects when the pump is 90% full. When the patient’s activity increases, the pump fills faster and the pump-rate automatically increases, resulting in an increase in pump output5. A maximum stoke volume of 83 ml allows a pump output of up to 10 L/min.

Chapter 2
18
The HeartMate is implanted in a pocket in the left upper quadrant of the patient’s abdomen or abdominal wall.
A major advantage of the HeartMate is that the pump requires only antiplatelet agents (e.g., dipyridamole plus aspirin) instead of systemic anticoagulation, due to unique textured blood-contacting surfaces66. HeartMate 1000 IP received approval from FDA in 1994 for use as a bridge to transplantation. The system is also approved for use in Canada, Europe and Asia. Clinical experience demonstrated successful use of HeartMate 1000 IP as a long-term LV support (237 days mean support time) to bridge patients with LVHF to transplantation67.
Thoratec Ventricular Assist Device
The Thoratec VAD (Thoratec Laboratories Corp., Berkeley, CA, USA), based on a design developed at Pennsylvania State University by Pierce and Donachy, can be used as LVAD, RVAD, or BiVAD. The pump is paracorporeally placed and consists of polysulfone case and polyurethane made blood sac. Two mechanical valves insure unidirectional blood flow. The pump is connected to a pneumatic drive console, which like the Abiomed console can support one or two mechanical ventricles. As most of the VAD, the Thoratec VAD requires also systemic anticoagulation.
The prosthetic ventricle has a stroke volume of 65 ml and can operate in fixed-rate mode, ECG synchronous mode, and in full-to-empty mode. The last mode maximizes cardiac output by allowing the VAD pump rate to be determined by the preload6. The system received approval from FDA to be applied in patients with postcardiotomy heart failure as well as a bridge to transplantation. Used as a long-term ventricular support (BiVAD or LVAD) in 154 transplant candidates, an 84% early post-transplantation survival and a 54% overall survival was found68.
MEDOS/ Helmholtz Institute Aachen (HIA) Ventricular Assist Device
MEDOS/HIA Ventricular Assist Device (MEDOS Medizintechnik GmbH, Aachen, Germany) is a pneumatically driven pulsatile assist device developed at the Helmholtz Institute Aachen (HIA) in Germany, which can be used as LVAD, RVAD, or BiVAD. The device consists of a paracorporeally placed membrane pump, inflow and outflow cannulas, and a driving system. Three-leaflet polyurethane valves, placed in the inflow and outflow tract of the membrane pump, ensure unidirectional flow. The membrane pump, the valves, and both the inflow and the outflow cannulas are Heparin coated. The device can operate in ECG synchronous as well as in asynchronous mode. The MEDOS/HIA is indicated as a bridge to myocardial recovery as well as a bridge to transplantation. After extensive animal tests, performed at the University of Groningen, the Netherlands69, the system has been

MCSS
19
introduced into clinical settings since February 1994 and has been used on 217 patients until the end of 199770.
PUCA pump
The Pulsatile Catheter (PUCA) pump (BioMedical Engineering, University of Groningen, The Netherlands) is a transarterial transvalvular blood pump that can be used as LVAD. The device consists of a large-bore reinforced Tecothane® (Thermedics, Inc., Woburn, Mass., USA) catheter connected to an extracorporeally placed, pneumatically driven single-port membrane pump71. The pump can be activated by UTAH Heart driver (Artificial Heart Research Laboratories, Salt Lake City, USA), Intra-Aortic Balloon Pump driver (Datascope Corp., Oakland, N.J., USA), or by MEDOS VAD driver (MEDOS Medizintechnik, Stolberg, Germany). A miniaturized combined inflow/outflow valve positioned 12 cm from the distal end of the catheter guides the blood from the left ventricle towards the membrane pump during pump aspiration, and from the membrane pump towards the aorta during pump ejection. The 18 French (Fr) version is designed to operate under closed chest conditions and has to be introduced via the axillary artery. This version can generate a pump flow of up to 3 L/min. The 24 Fr version, designed to be used under open chest conditions, can be inserted directly into the aorta and can generate a pump flow of up to 5 L/min. Using unique technique, the tip of the catheter could be positioned into the LV without X-ray control72. The PUCA pump is ECG triggered. In case of severe cardiac arrhythmia or signal disorders, the pump driver switches automatically to an untriggered mode.
The PUCA pump in fact combines the direct LV unloading effect of the Hemopump with the counterpulsation effect of IABP, a combination that has proven to provide an excellent support for the ischemic, failing heart73. However, due to the presence of the combined inflow/outflow valve, the PUCA pump could be temporary switched off and kept in place without backflow from aorta to LV. If the Hemopump is switched off a backflow occurs73.
Results obtained from animal experiments demonstrated that both asynchronous and ECG-synchronous assists with the PUCA pump reduced significantly LV myocardial oxygen consumption and that the generated the pump flow is enough to maintain the systemic circulation74.
Enabler Circulatory Support System
The Enabler circulatory support system (HemoDynamics LTD, Upper Yoqneam, Israel) is a catheter-pump that expels blood from the left or right ventricular cavity and ejects it in the ascending aorta or in the pulmonary artery respectively. The disposable catheter (diameter 16-30 Fr, length 30-110 cm) is connected to a

Chapter 2
20
hydraulically driven membrane pump, connected to a bedside driving console. Two one-way valves positioned respectively in the distal part and in the aortic part of the catheter direct the blood flow. The device is ECG-triggered and operates in counterpulsation base. The Enabler was tested during non-failing, moderately failing, and severely failing heart conditions in sheep75. During the experiments the device provided up to 3.5 L/minute blood flow.
The Enabler catheter-pump design is obviously based on the PUCA-pump concept published in 199371. The position of the Enabler catheter into the LV is verified by a pressure measurement, a technique developed for the PUCA-pump introduction as well72. However although older as a concept, the PUCA-pump seems to be more advanced due to the presence of only one valve and catheter wall-thickness of 0.3 mm.
2.3.2. Electric pulsatile VAD
Novacor N 100
Novacor N100 (Novacor, Baxter Healthcare Corp., Berkeley, CA, USA) is an electromechanical totally implantable pump designed for left ventricular support only. The device contains a polyurethane blood sac that is compressed by a dual symmetrically opposed pusher plates6. The pump, implanted in a pocket in the left upper quadrant of the abdominal wall, is connected to the LV apex and ascending aorta with respectively inflow and outflow grafts both passing the diaphragm. Bovine pericardial valve-prostheses are incorporated into the grafts to ensure unidirectional blood flow. Percutaneous leads connect the pump to an extracorporeal controller unit and to a battery pack, both positioned in a shoulder bag. Novacor can operate either in a fixed-rate mode or in an automatic mode. In the automatic mode, the device ejects when the pump is 90% full. When the patient’s activity increases, the pump fills faster and the pump-rate automatically increases, resulting in an increase in pump output5. The Novacor pump has a maximum stroke volume of 67 ml6. The device is ECG synchronized and creates pulsatile flow on counterpulsation basis. To prevent thrombus formation, systemic anticoagulation is required. Novacor N 100 was introduced in Europe in late 1993 and received FDA approval in 1995. The device was used in Europe as a bridge to transplantation for up to 585 days; 33% of patients returned home supported by the system 76. Dohmen et al. reported recently a LV support with Novacor N 100 in a man with severe congestive heart failure for more than 3 years without serious complications77. The patient returned home three months after the device implantation, and is presently in NYHA class I, drives a car, and travels abroad for vacation.

MCSS
21
HeartMate 1000 Vented Electric (VE)
HeartMate 1000 VE (Thermo Cardiosystems, Inc., Woburn, MA, USA) is similar to the pneumatically driven version (HeartMate 1000 IP), but the pusher plate is driven by a low-speed torque motor instead of air. Percutaneous leads connect the pump to an external console and battery pack. The device can operate either in a fixed-rate mode (50-120 beats/minute) or in an automatic mode Like the pneumatic variant, the HeartMate 1000 VE has a maximum stroke volume of 83 ml and is designed for left ventricular support only. The pump received approval from FDA in 1998 and was successfully used for up to 604 days in patients awaiting cardiac transplantation78.
Conclusions Substantial progress has been made in the development of Mechanical Circulatory Support Systems during the past decades. The development of MCSS has been directed towards two major research areas: development of Total Artificial Heart and development of Ventricular Assist Devices.
Major breakthroughs have been made in the development of TAH. The first significant step forward has been the introduction of the two-stage cardiac replacement concept by Cooley in 1969. The concept launched the idea that the TAH could be used not only as a permanent cardiac replacement device, but also as a bridge to transplantation in patients with severe heart failure. The second breakthrough has been made in materials science, the change from pneumatic into electric TAH. The bulky drive consoles and the high incidence of infections, caused by the percutaneous drivelines, made the pneumatically driven TAHs unsuitable for long-term use. The new generation electric TAHs are expected to be compact, totally implantable, and will use wireless percutaneous energy transmission. The implanted rechargeable batteries are used only as a back-up power source. Also the use of titanium instead of stainless steel made the devices lighter. The highly smooth segmented polyurethane replaced the silicon rubber improving significantly the biocompatibility of the devices. Pericardial tissue valves and biolized blood-contacting surfaces may eliminate the need of systemic anticoagulation.
Major breakthroughs have been made in the development of VADs as well. The development of a percutaneous insertion technique for the Intra-Aortic Balloon Pump allowed fast device application without major surgery and made the IABP the most used device for temporary support of the failing left ventricle. The Hemopump was the first transarterial blood with a high pumping capacity. The minor hemolysis developed by the Hemopump stimulated researchers to develop new high-speed axial pumps for short-term and intermediate-term use. The most

Chapter 2
22
advanced axial pumps are magnetically suspended, ultracompact, and practically noise-free. Essential mechanical and material improvements have been made in the VADs as well. Like the new generation TAHs, the long-term VADs are nowadays totally implantable, compact, and electrically powered. The use of textured blood-contacting surfaces as well as porcine/bovine valves allowed antiplatelet agents to be used instead of systemic anticoagulation. The use of sophisticated electric motors resulted in a low incidence of device failure. Wearable drive/control units allow patients to perform their daily life activities.
References 1. American Heart Association. 2000 Heart and Stroke Statistical Update. Dallas,
Texas: American Heart Association, 1999.
2. Framingham Heart Study. National Heart, Lung, and Blood Institute (NHLBI).
3. Braunwald E. Heart Failure. In: Fauci AS, Braunwald E, Isselbacher KJ, Wilson JD, Martin JB, Kasper DL, Hauser SL, Longo DL, eds. Harrison's Principles of Internal Medicine. New York: McGraw-Hill; 1998:1287-1298.
4. Mancini D, Goldsmith R, Levin H, Beniaminovitz A, Rose E, Catanese K, Flannery M, Oz M. Comparison of exercise performance in patients with chronic severe heart failure versus left ventricular assist devices. Circulation 1998;98:1178-1183.
5. Goldstein DJ, Oz MC, Rose EA. Implantable left ventricular assist devices. N Engl J Med 1998;339:1522-1533.
6. Richenbacher WE, Pierce WS. Assisted Circulation and the Mechanical Heart. In: Braunwald E, ed. Heart Disease: a Textbook of Cardiovascular Medicine. Philadelphia: W.B. Saunders Company; 1997:534-547.
7. Dipla K, Mattiello JA, Jeevanandam V, Houser SR, Margulies KB. Myocyte recovery after mechanical circulatory support in humans with end-stage heart failure [see comments]. Circulation 1998;97:2316-2322.
8. Lee SH, Doliba N, Osbakken M, Oz M, Mancini D. Improvement of myocardial mitochondrial function after hemodynamic support with left ventricular assist devices in patients with heart failure. J Thorac Cardiovasc Surg 1998;116:344-349.
9. Westaby S, Katsumata T, Houel R, Evans R, Pigott D, Frazier OH, Jarvik R. Jarvik 2000 heart: potential for bridge to myocyte recovery. Circulation 1998;98:1568-1574.
10. Akutsu T, Kolff WJ. Permanent substitutes for valves and hearts. Trans Am Soc Artif Intern Organs 1958;4:230.
11. Cooley DA, Liotta D, Hallman GL, Bloodwell RD, Leachman RD, Milam JD. Orthotopic cardiac prosthesis for two-staged cardiac replacement. Am J Cardiol 1969;24:723-730.

MCSS
23
12. Joyce LD, DeVries WC, Hastings WL, Olsen DB, Jarvik RK, Kolff WJ. Response of the human body to the first permanent implant of the Jarvik-7 Total Artificial Heart. Trans Am Soc Artif Intern Organs 1983;29:81-87.
13. Johnson KE, Liska MB, Joyce LD, Emery RW. Registry report. Use of total artificial hearts: summary of world experience, 1969-1991. ASAIO J 1992;38:M486-M492.
14. DeVries WC. Surgical technique for implantation of the Jarvik-7-100 total artificial heart. JAMA 1988;259:875-880.
15. Pierce WS, Sapirstein JS, Pae-WE J. Total artificial heart: from bridge to transplantation to permanent use. Ann Thorac Surg 1996;61:342-346.
16. Arabia FA, Copeland JG, Smith RG, Sethi GK, Arzouman DA, Pavie A, Duveau D, Keon WJ, Masters R, Foy B, Carrier M, Dembitsky W, Long J, Kormos R. International experience with the CardioWest total artificial heart as a bridge to heart transplantation. Eur J Cardiothorac Surg 1997;11 Suppl:S5-10.
17. Arabia FA, Copeland JG, Smith RG, Banchy M, Foy B, Kormos R, Tector A, Long J, Dembitsky W, Carrier M, Keon W, Pavie A, Duveau D. CardioWest total artificial heart: a retrospective controlled study. Artif Organs 1999;23:204-207.
18. Kung RT, Yu LS, Ochs B, Parnis S, Frazier OH. An atrial hydraulic shunt in a total artificial heart. A balance mechanism for the bronchial shunt. ASAIO J 1993;39:M213-M217.
19. Kung RT, Yu LS, Ochs BD, Parnis SM, Macris MP, Frazier OH. Progress in the development of the ABIOMED total artificial heart. ASAIO J 1995;41:M245-M248.
20. Massiello A, Kiraly R, Butler K, Himley S, Chen JF, McCarthy PM. The Cleveland Clinic-Nimbus total artificial heart. Design and in vitro function. J Thorac Cardiovasc Surg 1994;108:412-419.
21. Harasaki H, Fukamachi K, Massiello A, Chen JF, Himley SC, Fukumura F, Muramoto K, Niu S, Wika K, Davies CR, et a. Progress in Cleveland Clinic-Nimbus total artificial heart development. ASAIO J 1994;40:M494-M498.
22. Dennis C, Carlens E, Senning A. Clinical use of a cannula for left heart bypass without thoracotomy: Experimental protection against fibrillation by left heart bypass. Ann Sur 1962;156:623.
23. DeBakey ME. Left ventricular bypass pump for cardiac assistance. Clinical experience. Am J Cardiol 1971;27:3-11.
24. Quaini E, Pavie A, Chieco S, Mambrito B. The Concerted Action 'Heart' European registry on clinical application of mechanical circulatory support systems: bridge to transplant. The Registry Scientific Committee. Eur J Cardiothorac Surg 1997;11:182-188.

Chapter 2
24
25. Lohmann DP, Swartz MT, Pennington DG, McBride LR, Reedy JE, Miller L. Left ventricular versus left atrial cannulation for the Thoratec ventricular assist device. ASAIO Trans 1990;36:M545-M548.
26. Kantrowitz A, Bridgewater B, Au J. Intra-Aortic Balloon Pumping for Assisted Circulation: New Techniques and New Prospects. In: Ungar F, ed. Assisted Circulation. Berlin: Springer; 1995:12-35.
27. Kantrowitz A, Kantrowitz AR. Experimental Augmentation of Coronary Flow by Retardation of the Arterial Pressure Pulse. Surgery 1953;34:678-687.
28. Moulopoulos SD, Topaz SR, Kolf WJ. Extracorporeal assistance to the circulation and intaaortic balloon pumping. Trans Am Soc Artif Intern Organs 1962;8:85-89.
29. Kantrowitz A, Tjonneland S, Freed PS, Phillips SJ, Butner AN, Sherman-JL J. Initial clinical experience with intraaortic balloon pumping in cardiogenic shock. JAMA 1968;203:113-118.
30. Bregman D, Nichols AB, Weiss MB, Powers ER, Martin EC, Casarella WJ. Percutaneous intraaortic balloon insertion. Am J Cardiol 1980;46:261-264.
31. Kumbasar SD, Semiz E, Ermis C, Yalcinkaya S, Deger N, Pamir G, Oral D. Effect of intraaortic balloon counter-pulsation on QT dispersion in acute anterior myocardial infarction. Int J Cardiol 1998;65:169-172.
32. Davidson J, Baumgariner F, Omari B, Milliken J. Intra-aortic balloon pump: indications and complications. J Natl Med Assoc 1998;90:137-140.
33. Gutfinger DE, Ott RA, Miller M, Selvan A, Codini MA, Alimadadian H, Tanner TM. Aggressive preoperative use of intraaortic balloon pump in elderly patients undergoing coronary artery bypass grafting. Ann Thorac Surg 1999;67:610-613.
34. Schreiber TL, Kodali UR, O'Neill WW, Gangadharan V, Puchrowicz-Ochocki SB, Grines CL. Comparison of acute results of prophylactic intraaortic balloon pumping with cardiopulmonary support for percutaneous transluminal coronary angioplasty (PCTA). Cathet Cardiovasc Diagn 1998;45:115-119.
35. Siu SC, Kowalchuk GJ, Welty FK, Benotti PN, Lewis SM. Intra-aortic balloon counterpulsation support in the high-risk cardiac patient undergoing urgent noncardiac surgery. Chest 1991;99:1342-1345.
36. Mehlhorn U, Kroner A, de Vivie ER. 30 years clinical intra-aortic balloon pumping: facts and figures. Thorac Cardiovasc Surg 1999;47 Suppl 2:298-303.
37. Akomea AC, Kejriwal NK, Franks R, Booker PD, Pozzi M. Intraaortic balloon pumping in children. Ann Thorac Surg 1999;67:1415-1420.
38. Murai N, Kaneko T, Oobayashi T, Sato Y, Ogata T, Anno M, Nakajima T. [Left subclavian artery approach for insertion of IABP]. Kyobu Geka 1998;51:579-582.

MCSS
25
39. Arafa OE, Pedersen TH, Svennevig JL, Fosse E, Geiran OR. Vascular complications of the intraaortic balloon pump in patients undergoing open heart operations: 15-year experience. Ann Thorac Surg 1999;67:645-651.
40. Barnett MG, Swartz MT, Peterson GJ, Naunheim KS, Pennington DG, Vaca KJ, Fiore AC, McBride LR, Peigh P, Willman VL, et a. Vascular complications from intraaortic balloons: risk analysis. J Vasc Surg 1994;19:81-87.
41. Gol MK, Bayazit M, Emir M, Tasdemir O, Bayazit K. Vascular complications related to percutaneous insertion of intraaortic balloon pumps. Ann Thorac Surg 1994;58:1476-1480.
42. Kantrowitz A, Wasfie T, Freed PS, Rubenfire M, Wajszczuk W, Schork MA. Intraaortic balloon pumping 1967 through 1982: analysis of complications in 733 patients. Am J Cardiol 1986;57:976-983.
43. Scholz KH, Figulla HR, Schweda F, Smalling RW, Hellige G, Kreuzer H, Aboul HW, Wampler RK. Mechanical left ventricular unloading during high risk coronary angioplasty: first use of a new percutaneous transvalvular left ventricular assist device. Cathet Cardiovasc Diagn 1994;31:61-69.
44. Curtis JJ, Walls JT, Wagner-Mann CC, Schmaltz RA, Demmy TL, McKenney CA, Mann FA. Centrifugal pumps: description of devices and surgical techniques. Ann Thorac Surg 1999;68:666-671.
45. Oku T, Harasaki H, Smith W, Nose Y. Hemolysis. A comparative study of four nonpulsatile pumps. ASAIO Trans 1988;34:500-504.
46. Golding LAR, Smith WA. Centrifugal Pumps - Now and Future. In: Ungar F, ed. Assisted Circulation. Berlin: Springer; 1995:142-151.
47. Mandarino WA, Winowich S, Gasior TA, Pham S, Griffith BP, Kormos RL. Assessment of timing right ventricular assist device withdrawal using left ventricular assist device filling characteristics. ASAIO J 1997;43:M801-M805.
48. Olsen DB. Rotary blood pumps: a new horizon [editorial]. Artif Organs 1999;23:695-696.
49. Anstadt MP, Tedder M, Hegde SS, Perez TR, Crain BJ, Khian HV, Abdel AS, White WD, Lowe JE. Pulsatile versus nonpulsatile reperfusion improves cerebral blood flow after cardiac arrest. Ann Thorac Surg 1993;56:453-461.
50. Fukae K, Tominaga R, Tokunaga S, Kawachi Y, Imaizumi T, Yasui H. The effects of pulsatile and nonpulsatile systemic perfusion on renal sympathetic nerve activity in anesthetized dogs. J Thorac Cardiovasc Surg 1996;111:478-484.
51. Wampler RK, Moise JC, Frazier OH, Olsen DB. In vivo evaluation of a peripheral vascular access axial flow blood pump. ASAIO Trans 1988;34:450-454.
52. Dreyfus GD. Hemopump 31, the sternotomy Hemopump: clinical experience. Ann Thorac Surg 1996;61:323-328.

Chapter 2
26
53. Lonn U, Peterzen B, Carnstam B, Casimir AH. Beating heart coronary surgery supported by an axial blood flow pump. Ann Thorac Surg 1999;67:99-104.
54. Wampler RK, Frazier OH, Lansing AM, Smalling RW, Nicklas JM, Phillips SJ, Guyton RA, Golding LA. Treatment of cardiogenic shock with the Hemopump left ventricular assist device. Ann Thorac Surg 1991;52:506-513.
55. Wiebalck AC, Wouters PF, Waldenberger FR, Akpinar B, Lauwers PM, Demeyere RH, Sergeant PT, Daenen WJ, Flameng WJ. Left ventricular assist with an axial flow pump (Hemopump): clinical application. Ann Thorac Surg 1993;55:1141-1146.
56. Sweeney MS. The Hemopump in 1997: a clinical, political, and marketing evolution. Ann Thorac Surg 1999;68:761-763.
57. DeBakey ME. A miniature implantable axial flow ventricular assist device. Ann Thorac Surg 1999;68:637-640.
58. Fossum TW, Morley D, Benkowski R, Tayama E, Olsen DB, Burns G, Miller MW, Franks J, Martinez E, Carroll G, Edwards J, Vinnerqvist A, Lynch B, Stein F, Noon GP, DeBakey ME. Chronic survival of calves implanted with the DeBakey ventricular assist device. Artif Organs 1999;23:802-806.
59. Westaby S, Katsumata T, Evans R, Pigott D, Taggart DP, Jarvik RK. The Jarvik 2000 Oxford system: increasing the scope of mechanical circulatory support. J Thorac Cardiovasc Surg 1997;114:467-474.
60. Thomas DC, Butler KC, Taylor LP, le Blanc P, Rintoul TC, Petersen TV, Griffith BP, Kormos RL, Borovetz HS, Litwak P, Kameneva MV, Choi S, Burgreen GW, Wu Z, Antaki JF. Progress on development of the Nimbus-University of Pittsburgh axial flow left ventricular assist system. ASAIO J 1998;44:M521-M524.
61. Kameneva MV, Watach MJ, Litwak P, Antaki JF, Butler KC, Thomas DC, Taylor LP, Borovetz HS, Kormos RL, Griffith BP. Chronic animal health assessment during axial ventricular assistance: importance of hemorheologic parameters. ASAIO J 1999;45:183-188.
62. Unger F. Ventricular Assist Devices: Clinical reality. In: Unger F, ed. Assisted Circulation. Berlin: Springer; 1995:55-58.
63. Everts PAM, Schonberger JPAM, Peels CH. The Abiomed BVS 5000 for Treatment of Postcardiotomy Cardiogenic Shock. In: Ungar F, ed. Assisted Circulation. Berlin: Springer; 1995:87-100.
64. Jett GK. ABIOMED BVS 5000: experience and potential advantages. Ann Thorac Surg 1996;61:301-304.
65. Sato M, Katayama Y, Higuchi S, Kosako Y, Ohtsubo S, Itoh T. [Initial clinical experiences of the ABIOMED BVS SYSTEM 5000 in Japan]. Nippon Kyobu Geka Gakkai Zasshi 1998;46:236-242.
66. Rose EA, Levin HR, Oz MC, Frazier OH, Macmanus Q, Burton NA, Lefrak EA. Artificial circulatory support with textured interior surfaces. A counterintuitive approach to minimizing thromboembolism. Circulation 1994;90:II87-II91.

MCSS
27
67. Koul B, Solem JO, Steen S, Casimir AH, Granfeldt H, Lonn UJ. HeartMate left ventricular assist device as bridge to heart transplantation. Ann Thorac Surg 1998;65:1625-1630.
68. Farrar DJ, Hill JD. Univentricular and biventricular Thoratec VAD support as a bridge to transplantation. Ann Thorac Surg 1993;55:276-282.
69. Rakhorst G, Hensens AG, Verkerke GJ, Blanksma PK, Bom VJ, Elstrodt J, Magielse CP, van der MJ, Eilers R, Reul H. In-vivo evaluation of the "HIA-VAD": a new German ventricular assist device. Thorac Cardiovasc Surg 1994;42:136-140.
70. Reul H. The MEDOS/HIA system: development, results, perspectives. Thorac Cardiovasc Surg 1999;47 Suppl 2:311-315.
71. Verkerke B, de Muinck ED, Rakhorst G, Blanksma PK. The PUCA pump: a left ventricular assist device. Artif Organs 1993;17:365-368.
72. Mihaylov D, Kik C, Elstrodt J, Verkerke GJ, Blanksma PK, Rakhorst G. Development of a new introduction technique for the pulsatile catheter pump. Artif Organs 1997;21:425-427.
73. Meyns B, Nishimura Y, Racz R, Jashari R, Flameng W. Organ perfusion with Hemopump device assistance with and without intraaortic balloon pumping. J Thorac Cardiovasc Surg 1997;114:243-253.
74. Mihaylov D, Verkerke GJ, Elstrodt J, Blanksma PK, De Jong ED, Rakhorst G. Evaluation of the Optimal Driving Mode during LV Assist with PUCA Pump in Calves. Artif Organs 1999;23:1117-1122.
75. Nishimura Y, Meyns B, Ozaki S, Racz R, Dohmen P, Flameng W. The enabler cannula pump: a novel circulatory support system. Int J Artif Organs 1999;22:317-323.
76. El Banayosy A, Deng M, Loisance DY, Vetter H, Gronda E, Loebe M, Vigano M. The European experience of Novacor left ventricular assist (LVAS) therapy as a bridge to transplant: a retrospective multi-centre study. Eur J Cardiothorac Surg 1999;15:835-841.
77. Dohmen PM, Laube H, de Jonge K, Baumann G, Konertz W. Mechanical circulatory support for one thousand days or more with the Novacor N100 left ventricular assist device. J Thorac Cardiovasc Surg 1999;117:1029-1030.
78. DeRose-JJ J, Umana JP, Argenziano M, Catanese KA, Gardocki MT, Flannery M, Levin HR, Sun BC, Rose EA, Oz MC. Implantable left ventricular assist devices provide an excellent outpatient bridge to transplantation and recovery. J Am Coll Cardiol 1997;30:1773-1777.

28