Embed Size (px)
DESCRIPTION
Chapter 16. Dr. D. Washington. Respiratory Physiology. The term respiration includes three separate but related function: A. Ventilation (breathing): mechanical movement of air between nose and alveoli of the lungs - PowerPoint PPT Presentation
Citation preview

Chapter 16
Dr. D. Washington

Respiratory Physiology
The term respiration includes three separate but related function:
A. Ventilation (breathing): mechanical movement of air between nose and alveoli of the lungs
B. Gas exchange: between the air and the blood; and between the blood and tissues
C. Oxygen utilization: cellular metabolism

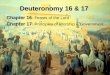
E.R. Weibel’s Model of the Human Airways (Morphometry of the Human Lung)
Trachea
Bronchus
Terminal bronchioles
Terminal bronchioles
Alveolar ducts
Alveolar sacs
Co
nd
uctive Z
on
eT
ran
sin
on
al o
rR
es
pira
tory
Zo
ne
Bronchioles
T
Br
BL
TBL
RBL
AD
AS
Zone
1234
1718
21
23
0

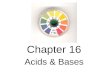
Functional Unit of the Lungs
Surfactant decreases the surface tension of fluids linings the alveoli.
Law of LaPlace: the distending pressure (P) in a distensible, hollow object is equal at equilibrium to the tension (T) in wall divided by the 2 principal radii of curvature of the objects (R1 and R2). P
T
v
Alvelus
Secretory cells (type II)(Surfactant)
Squamous cells (type I)Interstitium basement membranes ofcapillary & alveolus
Surface tension causedby the cohesive forcesof water molecules
Air pressure inside the alveolus

Surfactant Effects
Without Surfactant
The clamps represent the forces of surface tension. The greater pressure on the small alveolus would cause it to collapse. With Surfactant
The pressure on the small alveolus is reduced.

.50 _
.25_
Lu
ng
Vol
. Ch
ange
(li
ters
)
expiration
inspiration
Intrapleural pressure (cm H20) (pressure around the lungs)Intrapulmonary pressure Negative pressure = subatmospheric pressure
Pressure - Volume Curve(Compliance)
-4 -5 -6 -7+3 0 -3 -4

Changes in Compliance
A. Decrease (increased resistance)
1. Aleolar edema: decrease caused by increase in pulmonary venous pressure
2. Atelectasis: partial or complete collapse of lungs
3. Pulmonary fibrosis: infiltration or connective tissue
B. Increase (decrease resistance)
1. Age: loss of elastic tissue
2. Emphysema: destruction of alveolar tissue

When the pressure inside the jar isreduced below atm. Pressure, the lung expands.
Elastic Properties of the Lungs
Excised dog lung
(vol. measuredon spirometer)
pump

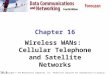
Lung Volumes
500 ml
3,000 ml
1,000 ml
1,000 ml
150 ml Dead spaceResidual volumeExpiration Reserve volumeTidal volumeInspiration Reserve volume

Lung Capacities(combination of volumes)
TLC - total lung capacity VC - vital capacity IC - inspiration capacityFRC - function residual capacity
TLC VC
RV
IC
FRC
IRV
TVERVRV

Note: If the anatomical dead space is 150ml, and the tidal volume is 500 ml;the percentage of fresh air reaching the alveoli is 350/500 X 100% = 70%
Inspiration Reserve volume
Tidal volume
Expiration Reserve volume
Residual volume
Lung Compartments

Composition of Gases at Sea Level
PP = Partial Pressure
OxygenPP %
CO2
PP %Water
PP %
Nitrogen &rare gasesPP %
Inspirated air 158 21. 0.3 0.04 8 1. 594 78 (20oC; 50%Sat.)
Moist tracheal 149 19.6 0.3 0.04 47 6.2 564 74 air (saturated)
Alveolar air 104 13.7 40 5.3 47 6.6 569 75
Arterial blood 100 13. 40 5.3 47 6.2 573 75
Venous blood 40 5.6 46 6.5 47 6.7 573 81
Expired air 116 15.2 29 4 47 6.2 568 75

Partial Pressure in the BodyInspired Air O2 = 158CO2 = 0.3H20 = 8N2 = 594
Expired Air O2 = 116CO2 = 29H20 = 47N2 = 568
Right Heart O2 = 40CO2 = 46H20 = 47N2 = 573
Left Heart O2 = 100CO2 = 40H20 = 47N2 = 573
Capillaries O2 = 40, CO2 = 46, H20 = 47, N2 = 573
Alveoli O2 = 104CO2 = 40H20 = 47N2 = 569
Veins Arteries
Dead space

Coordination of Ventilation & Perfusion The efficiency of gas exchange in the
lungs is dependent on the adequacy and uniformness of ventilation and perfusion.
Inspired gas and pulmonary blood flow are unevenly distributed.
Ventilation-perfusion ratio inequality is the most common clinical cause of arterial hypoxemia.

Ventilation-Perfusion Ratio VA/Q = 0.8 in a normal person at rest Volume of blood perfusing the lungs
is 1.2 times greater than the Volume of air ventilating the lungs
Coordination of Ventilation & Perfusion

Pathological causes for Non- Uniform Distribution of Ventilation1. Regional Elasticity of Changes
(pulmonary fibrosis)
2. Regional Obstruction of Airways
3. Intrathoracic fluid Accumulation
Coordination of Ventilation & Perfusion

Coordination of Ventilation & Perfusion
Pathological causes for Non- Uniform Distribution of Perfusion1. Compression of Blood Vessels Caused
by Intrathoracic P.
2. Embolism
3. Regional Vasoconstriction (ANS)

Regulation of Respiration
I. IntrinsicMedulla of Respiratory Center found
in the brain stem

Regulation of Respiration
II. Extrinsic
A. Chemoreceptors1. Peripheral
carotid and aortic bodies
2. Central Nervous System (Medulla) 70 - 80% main cause for change

Regulation of Respiration
II. Extrinsic
B. The Hering-Breuer reflexesMaintains normal tidal volume.
(more important in infants)
1. H-B inflation reflex
2. H-B compression reflex

Respiratory CenterCortical & midbrain stimuli
glassopharyngeal glassopharyngeal & vagus& vagus
Cord facillatoryCord facillatoryimpulsesimpulses
PneumotaxicPneumotaxicinhibits respirationinhibits respiration
ApneusticApneusticstimulates respirationstimulates respiration
MedullaryMedullaryrythmicity centerrythmicity center
Impulses Impulses toto respiratory respiratory
musclesmuscles

Rhytmic Oscillation in the Respiratory Center
inspiratory expiratory
I Eneurons neurons
muscles of muscles ofinspiratory expiratory

Respiration neurons in Brain StemDorsal View; Cerebelium removed
D
A
B
C
Vagi intact
Vagi cut
All transected in A & B
IX
X
XI
XII
Parabrachials N.(pneumotaric center)
Middle cerebellar peduncle
Apneustic centerin 4th ventrical
Dorsal grouprespiratory neurons
Ventral grouprespiratory neurons

Respiration neurons in Brain StemDorsal View; Cerebelium removed
Effects of Transection
A. Above pons - regular breathing continues
B. Below pneumotaxic area - inspiratory neutrons fire continuously (sustained inspriation -apneusis. However, if the However, if the vagus is intact respiration continues (effects from lungs).vagus is intact respiration continues (effects from lungs).
C. Below apneustic area - gasping type irregular respiration continues with or with our vagus
D. Below medulla - respiration stops (phrenic nerve cut)(phrenic nerve cut)

Increased ventilation
Increased arterial Pco2
Plasma CO2Blood pH
BloodCSF
Chemoreceptorsin medulla oblongata
Respiratory centerin medualla oblongata
Chemoreceptorsin aortic &
carotid bodies
Sensory neurons
Spinal cordmotor neurons Negative
feedback
Respiratorymuscles
Decreased ventilation

Effects of Po2, Pco2 + ph on Alveolar Ventilation
Fluctuation of one variable at a time
Co2
phO2
Pco2 35 40 45 50 55Po2 120 100 80 60 40ph 7.5 7.4 7.3 7.2 7.1
Alv
eola
r V
enti
lati
on
(b
asal
rat
es) 7
6543210

Effects of Po2, Pco2 + ph on Alveolar Ventilation
Free Fluctuation Co2
ph
O2
Pco2 40Po2 100ph 7.4

Oxygen SolubilityHenry’s Law
The concentration of a gas dissolved in a fluid is directly proportional to the partial pressure of that gas.
Solubility Coefficients of O2 in blood =
24cc/L/atmos.
Arterial Po2 = 100mmHg
therefore,
dissolved O2 = = 3/15cc/l100mmHg x 24cc/L
760 mmHg

CH2
CH2
COOH
C
C
HemeCH3
CH3
CH3
CH3
CH2
CH2
CH2
CH2
CH
CH
CH
COOH
HC
C
HC
C
CC
C
C
C
C
C
CC
C CN
N
N
NFeC
C

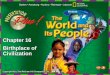
Effect of Changes inPo2 on Blood
Oxyhemoglobin Saturation and Oxygen Content (figure 15.34)
Po2
Amount of O2
unloaded to Tissues
Pe
rce
nt
oxy
hem
og
lob
in s
atu
rati
on
Ozy
ge
n c
on
ten
t
(ml O
2/10
0 m
l blo
od
)(mm Hg)
Veins(at rest)
Arteries
100
80
60
40
20
00 20 40 60 80 100
20
15
10
5
0

Oxygen Dissociation
half saturations myglobin = 6mm Hg
hemoglobin = 24 mm Hg
O2 pressure mmHG
% S
atu
rati
on
0 20 40 60 80 100
hemoglobin
myglobin100
80
60
40
20
0
507%
38%
dis
soci
ated

Th O2 dissociation curve for myoglobin follows the law of mass action
with a dissociation constant of 3.3, the Po2 has to fall almost to 0 before the O2 is releases to the cells
Oxygen Dissociation
Mb +Po2K =Mbo2

Bohr Effect(effect of pH on O2 Dissociation)
0 20 40 60 80 100
100
80
60
40
20
0
Po2
% O
2 sa
tura
tio
n
pCO2 = 40pCO2 = 80pCO2 = 20
pCO2 = 20 high pH, shift left
pCO2 = 80 low pH, shift right
A drop in pH at any pO2, causes an In O2 Dissociation.

Bohr Effect(effect of pH on O2 Dissociation)
Factors affecting O2 Dissociation
1. pH (or Co2 ) - deoxyhemogloblim binds H+ more actively then oxyhemogloblim
2. Temperature - effects metabolic rate
[CO2]
CO2+ H20 H2O H2CO3 H+ + HCO3
3. 2,3 - DPG (diphosphoglycerate) of RBC.

Carbon Dioxide Transport the Chloride Shift in Tissue Capillaries
Plasma
Tissue CellsTissue Cells
Carbonic anhydrase
CO2+ H2O H2CO3
H2CO3 H++HCO3 -
H+ combines with hemoglobin
CO2 combined with
hemogloblin to form carbaminohemoglobin
(20%)
CO2CO2 dissolved in plasma (10%)
Red blood cellsHCO 3 - (70%)Cl- Chloride shift