Upload
macon824
View
238
Download
0
Embed Size (px)
Citation preview
8/10/2019 Chapter 15 Stomach
1/129
8/10/2019 Chapter 15 Stomach
2/129
8/10/2019 Chapter 15 Stomach
3/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 3/
Schematic representation of positional changes of stomach. A, B,Rotation of stomach along longitudinal axis (anterior view). C, D,Effect of rotation onperitonea l attachments (transverse s ection). (Based on Sadler TW. Langman's Medical Embryology, 5th Ed. Baltimore: Williams & Wilkins, 1985.)
The anteroposterior axis rotation (Fig. 15-2) changes the position of the gastric cardia and fundus, as well as the position of the pylorus andgastroduodenal junct ion. Therefore, the dorsal midline becomes the greater curvature and the ventral midline becomes the lesser curvature (F igs.15-1C and 15-3). At the fourth fetal month the concavity of the lesser curvature is obvious and, at the eighth month, the fundic outgrowth (Fig.15-4). This is because the ventral border (lesser curvature) of the future stomach grows more slowly than its dorsal border (greater curvature).
Fig. 15-2.
8/10/2019 Chapter 15 Stomach
4/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 4/
Schematic drawings of rotation of stomach around anteroposterior axis. Note change in position of pylorus and cardia. (Based on Sadler TW. Langman'sMedical Embryology, 5th Ed. Baltimore: Williams & Wilkins, 1985.)
Fig. 15-3.
8/10/2019 Chapter 15 Stomach
5/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 5/
Cross-sectional diagrams through the embryonic stomach during the seventh week illustrating two hypotheses for the rotation of the stomach. A,Classic
concept: dorsal border rotates to left to become greater curvature. B,Concept of Dankmeijer and Miete.352 Left side becomes greater curvature as resultonly of increased growth. No actual rotation occurs.
Fig. 15-4.
Shape of stomach in prenatal stages and in adult. (Redrawn from Lewis FT. The development of the stomach. In: Keibel WP, Mall FP (eds). Manual ofHuman Embryology. Philadelphia: JB Lippincott, 1912; with permission.)
The human hand is used frequently as a mnemonic aid to instruct students about specific anatomic entities. To teach the embryology of thestomach, we use the left hand held in such a way that the hypothenar and fifth finger touch the epigastric area (Figs. 15-5, 15-6). With rotation,the palm touches the epigastrium; the hypothenar and fifth finger touch the greater curvature; and the thenar and thumb touch the lessercurvature. Remember that with further development, the proximal part of the st omach moves t o the left producing the permanent fundus, and thedistal part moves to the right producing the pylorus.
Fig. 15-5.
Location of left hand at embryonic foregut (beginning of dilated stomach). (Modified from Skandalakis JE, Gray SW (eds). Embryology for Surgeons, 2nd Ed.Baltimore: Williams & Wilkins, 1994; with permission.)
Fig. 15-6.
8/10/2019 Chapter 15 Stomach
6/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 6/
Use of left hand to demonstrate embryogenesis of stomach. Hypothenar and fifth finger touch the epigastrium vertically. If the same hand now turns sothat the fifth finger and the hypothenar touch in a transverse way, the epigastrium and the palm in toto touch the epigastrium; then the fifth finger andhypothenar represent the greater curvature, and the thumb and index represent the lesser curvature. (Modified from Skandalakis JE, Gray SW (eds).Embryology for Surgeons , 2nd Ed. Baltimore: Williams & Wilkins, 1994; with pe rmission.)
Some authors believe that positional rotational changes of the stomach do not take place. The gastroesophageal junction may be seen after
augmentation of the fundus from the body of the stomach. O'Rahilly and Mller2write about intrinsic growth changes in both gastric curvatures.They report that there is no evidence of gastric rotation. The embryologic enigma continues. But most likely O'Rahilly and Mller are right.
The rugae appear by the eighth week. The muscularis emerges between the eighth and 14th weeks.
The first glandular pits appear on the lesser curvature between the sixth and ninth weeks and by the tenth week are all over the stomach (Fig. 15-7). At birth approximately 200,000 pits and 500,000 glands may be found in the entire stomach. Parietal cells may be recognized at approximatelythe 11th week, and chief cells around the 12th week. At the same time mucous cells are found; pepsin is present in the mucosa by the last half ofthe sixth month.
Fig. 15-7.
8/10/2019 Chapter 15 Stomach
7/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 7/
, a ern o appearance o gas rc p s y wee s o em ryonc eve opmen . , a ern o ma ura on o gas r c sur a ce ep e um y wee s odevelopment. (Data from Salenius P . On the ontogenesis of the human gast ric epithelial cells: a histologic and histochemical study. Acta Anat [Basel]1952;50 [Suppl 46]:1-76.)
Congenital Anomalies
The anomalies of the stomach are presented in Table 15-2. In Figure 15-8A their chief locations are shown; Figures 15-8B through 15-8K depict theanomalies. We describe here only some of the most important anomalies. The interested student will find more information in Embryology for
Surgeonsby Skandalakis and Gray.3
Table 15-2. Anomalies of the Stomach
Anomaly Prenatal Ageat Onset
FirstAppearance
Sex ChieflyAffected
RelativeFrequency
Remarks
Agastria and microgastria Week 4 Infancy ? Very rare Many associated gastrointestinal tract and splenic anomalies
Malposition Week 10 Any age Males Rare May be associated with diaphragmatic eventration or hernia
Atresia and stenosis ? Infancy toadulthood
? Rare Maternal hydramnios familial occurrence (?)autosomal recessiveassociated with epidermolysis bullosa
Membranous partial Infancy toadulthood
Membranous entire ? Infancy toadulthood
Complete (solid) Weeks 6-7
Gastroduodenaldiscontinuity
?
Luminal with microscopiccanal ?
Typical stenosis withperforated membrane(s)
Hourglass stomach ? Any age ? Rare Usually not congenital
Congenital pyloric stenosis Postnatalweek 2
2-4 weeks Male Verycommon
Not a true anomaly
Infantile
Adult
Congenital muscular defect Weeks 8-10 Infancy ? Rare May not be congenital
Diverticula ? 40-70 yr Equal Rare May not be congenital
Duplicationdouble pylorus Week 3 Any age Female Rare Faulty separation of endoderm and notochordal plate
Mucosal heterotopia Weeks 4-5 Adhesion or metaplasia
From other organs tostomach
Pancreas
Small bowel
Others
From stomach to otherorgans
Congenital arteriovenousmalformations
? Adult Male Rare May not be congenital
Teratoma Infancy toadulthood
Male Rare Benign (usually)
Gastroduodenal adhesions ? ? ? ? ?
Source:Skandalakis JE, Gray SW (eds). Embryology for Surgeons, 2nd Ed. Baltimore: Williams & W ilkins, 1994; w ith permission.
Fig. 15-8.
8/10/2019 Chapter 15 Stomach
8/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 8/
8/10/2019 Chapter 15 Stomach
9/129
8/10/2019 Chapter 15 Stomach
10/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 10/
8/10/2019 Chapter 15 Stomach
11/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 11/
8/10/2019 Chapter 15 Stomach
12/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 12/
8/10/2019 Chapter 15 Stomach
13/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 13/
A,Chief locations of congenital anomalies of stomach. B,Five types of gastric atresia. (a),Membranous atresia; (b),Perforated membrane (stenosis); (c),Luminal atresia w ith microscopic endodermal canal; (d),Complete solid atresia; (e),Complete atresia with discontinuity. C,Two explanations of gastricatresia. (a),Redundant endodermal lining. Cauda l slippage of endoderm forms circular fold. Fold may or may not retain a central opening. (b),Attenuationof endoderm. Proliferation of endoderm fails to keep up with elongating foregut. Atresia or even complete discontinuity results. D,Rammsted tpyloromyotomy for infantile pyloric stenos is. E,Locations of 342 diverticula of stomach. Most are located on posterior wall of upper part of stomach. F,Duplication of the stomach. Those in top row are probably more common. G,Location of spontaneous rupture through congenital defects of gastricmusculature. Numbersindicate order of frequency; over half occur on greate r curvature. H,Inversion of stomach. Tracings from radiographs o f 65-year-oldwoman. A, Antrum; B, Body; C, Cardia; F, Fundus. I,Sources of heterotopic tissues found in stomach. Thickness of arrows indicates relative frequency. J,Distribution of hete rotopic pancreatic tissue in stomach. K,Location of heterotopic gastric mucosa in other organs of body. Thickness of arrows indicatesrelative frequency. (A-G, I-Kmodified from Skandalakis JE, Gray SW (eds). Embryology for Surgeons, 2nd Ed. Baltimore: Williams & W ilkins, 1994; w ithpermission. E,Data from Palmer ED. Gastric diverticula. Surg Obstet Gynecol 1951; 43:432-443. H,Modified from Rhinehart BA, Rhinehart DA. Congenitalabnormalities of the stomach. Radiology 1926;7:492-497. J,Data from Palmer ED. Benign intramural tumors of the stomach: a review with special referenceto gross patho logy. Medicine 1951;30:81-86; with permission.)
8/10/2019 Chapter 15 Stomach
14/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 14/
Microgastria and Agastria
Only in nonviable monsters is the stomach ever completely absent. Microgastria is an extremely rare congenital anomaly (fewer than 30 cases
reported)4and may be present as a small, tubular stomach which is associated with incomplete gastric rotat ion and megaesophagus. If conservativmedical att empts such as total parenteral nutrition or continuous nasogastric feedings are not successful, the treatment is surgical. Jejunal reservo
was reported by Gerbeaux;5gastrojejunostomy by Blank and Chisholm.6
The surgeon should be aware of further anomalies associated with microgastria and agastria: these include cardiac defects, asplenia,megaesophagus, and others.
Atresia and Stenosis
Gastric atresia (Fig. 15-8B and Fig. 15-8C) is limited to the antrum and pyloric region and, in most cases, is usually produced by a membranousmucosal diaphragm. This diaphragm may be perforated. If an antral or pyloric ulcer is present we conclude that atresia and stenosis is notcongenital, but ac quired.
The three cardinal symptoms in infants are persistent bile-free vomiting, upper abdominal distention, and decreasing quantity of stools.
The t reatment of choice is surgery (excision of the diaphragm or gastroduodenostomy) before the 10th day of life.
Hourglass Stomach
Hourglass stomach is a division of the two gast ric chambers by a constricting ring that may be of congenital origin. If symptomatic, surgery includesremoval of the ring and gastrogastrostomy or gastrojejunostomy of the proximal chamber.
Congenital (Infantile Hypertrophic) Pyloric Stenosis
The c linical entity of hypertrophy and hyperplasia of the muscularis of the pyloric canal appears early in postnatal life. This may be why it is
considered a congenital anomaly. Acc ording to McMullin,7the incidence of infantile hypertrophic pyloric stenosis is approximately 2.4 per 1000 livebirths, and does not appear to be a seasonal variation by month of birth.
Pyloromyotomy (Rammstedt's procedure) (Fig. 15-8D) is the operation of choice. It is a simple longitudinal incision of the pyloric musculature leavingthe mucosa intact . The muscularis must be incised without injury to the mucosa. The incision is not sutured. Balloon dilatation of the pyloric c anal i
also reported to be successful.8
Congenital True Gastric Diverticula
Most cases of congenital true gastric diverticula are located in the upper posterior wall (Fig. 15-8E). All layers of the gastric wall are present, butthere is no evidence of organic disease. If symptomatic, diverticulect omy or segmental gastric resect ion is performed.
Duplication of the Stomach
Duplicat ions of the alimentary tract are named for the structures with which they are assoc iated rather than for the mucosal lining within them.These rare lesions differ widely, so that few generalizations are possible. Most gastric duplications are located in the greater curvature of the
stomach (Fig. 15-8F). If symptomatic, removal of t he entire duplication is the ideal treatment.
Congenital Defects of the Gastric Musculature
Congenital defects of the gastric musculature are caused by failure of myoblast formation. The greater curvature is most frequently affected (Fig.15-8G). With gastric perforation, the treatment of choice is surgery.
Malposition of the Stomach
The most dramatic form of malposition of the stomach is assoc iated with situs inversus viscerum (Fig. 15-8H). Gastric volvulus associated with
wandering spleen secondary to an absence of ligamentous connections of stomach, spleen and posterior abdominal wall has been reported.9Ifgastric volvulus occ urs, emergency surgery is necessary.
Gastric Mucosal Heterotopia: Recipient and Donor
The stomach can be the recipient and the donor of gastric mucosa, which is the most peripatetic entity of the GI tract. Figs. 15-8I and 15-8Jillustrate the stomach as the recipient; Fig. 15-8E, as the donor. If symptomatic, c onservative surgery should be performed.
Gastric Teratoma
Gastric teratoma is a very rare benign lesion. In 1964 Skandalakis, one of the authors of this chapter, and his colleagues10reported the 13th caseof gastric teratoma. They reported that in all cases in which specific data had been available the patients were males and the teratomas werebenign. Subtotal gastrectomy or excision is the treatment of choice.
Lingawi and Filipenko11reported gastric outlet syndrome secondary to a benign hamartoma of Brunner's gland.
SURGICAL ANATOMY
The stomach is a pouch connecting the abdominal esophagus and the f irst part of the duodenum. Gahagan12speaks of the "termination of a tube,the esophagus, and the beginning of a pouch, the stomach." From a surgical standpoint, however, we will include the gastroesophageal junct ion anthe first portion of the duodenum with the stomach. These are the proximal and distal gastric connections. They are part of the "surgical stomach"which includes the cardiac orifice and the pyloric canal.
8/10/2019 Chapter 15 Stomach
15/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 15/
Topography and Relations
Few abdominal organs are as mobile as the stomach. Its position depends on the position of the individual, the degree to which the stomach is filledthe degree to which the intestine is filled, the tone of the abdominal wall, and the habitus of the patient. The stomach is higher in broad, stockyindividuals than in slender ones. Anatomic characteristics (e.g., shape and size), pathologic disorders (e.g., diaphragmatic hernia), and excessivelylarge meal consumption are factors that can play a role in the genesis of gast ric volvulus.
The only fixed point of reference is the gastroesophageal junction, which lies to the left of the midline behind the seventh costal cartilage at thelevel of the tenth thoracic vertebra. Some authors consider the retroperitoneal duodenum a second fixation because it has lost its primitive dorsalmesentery. However, 1 inch (2.54 cm) of the first part of the duodenum retains both primitive ventral and dorsal mesenteries; this may represent asecond fixation. For the remainder of the stomach there is no single "normal" projection.
Anteriorly, the stomach is in contac t with the liver, diaphragm, and anterior body wall. Posteriorly, in the recumbent cadaver, the stomach lies in abed formed by the diaphragm, spleen, left kidney and adrenal gland, pancreas, t ransverse mesocolon, and splenic flexure of the c olon. The positionand extent of the areas of contact of the stomach with these organs will vary in life.
The c lose proximity of the stomach t o other organs, the sharing of its blood supply with these organs, and its lymphatic system all dictate rules andregulations to the surgeon so that anatomic c omplicat ions can be avoided during gastric surgery. For example, the inflammatory process of a benigngastric ulcer can be responsible for fixation of the posterior wall of the stomach to the transverse mesocolon. A careless separation of the twostructures could jeopardize the blood supply of the transverse colon by injuring the middle colic artery. Another example of possible danger is injuryto the spleen from avulsion of its c apsule during gastric surgery.
Maingot13studied the direct invasion of gastric cancer to the neighboring organs. The most frequently involved organs are the colon, pancreas,liver, gallbladder, spleen, duodenum, and upper proximal jejunum. The authors of this chapter have seen direct invasion of the left hemidiaphragm,left adrenal, left kidney, and falciform ligament. Also, other organs such as the panc reas (Table 15-3) are responsible for direct invasion or lymphatispread to the stomach as well as to other anatomic entities.
Table 15-3. Pancreatic Carcinoma
Tr, Transverse; Reg LN, Regional nodes.
*Data from Cubilla AL, Fitzgerald PJ. Metastasis in pancreatic duct carcinoma. In: Day SB, Meyers WPL, Stanley P (eds). Cancer Invasion and Metastasis:Biologic Mechanisms and Therapy. New York: Raven Press, 1977, pp. 81-94.
**Data from Howard JM, Jordan JL Jr. Cancer o f the pancreas. Curr Probl Cancer 1977;2:25.
It is our opinion that esophageal and duodenal involvement from gastric c ancer is an established fact , and the distal esophagus and proximalduodenum should be treated accordingly (Fig. 15-9). In 1967 Paramanandhan14stated that gastric lesions invade the duodenum by directextension, or lymphatic spread, or both. We agree.
Fig. 15-9.
8/10/2019 Chapter 15 Stomach
16/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 16/
Direct extens ion of gastric cancer.
Stomach and Peritoneum
The stomach is c overed completely by the peritoneum, except in two small areas at the posterior surface of the cardia and at the proximal half ofthe first part of the duodenum. If we want to be more anatomically correct, the lesser and greater curvatures of the stomach are not covered byperitoneum. We see this during superselective vagotomy at the lesser curvature and during the ligation of the short gastric vessels at splenectomyThe two peritoneal layers are present anterior and posterior to the vessels.
Peritoneal Reflections
DERIVATIVES OF THE VENTRAL MESENTERY
Only the cranial portion of the embryonic ventral mesentery persists in the adult. The anterior part of this mesentery is represented by the falciformligament (F ig. 15-10) between the liver and the anterior body wall. The posterior part of the ventral mesentery becomes the hepatogastric andhepatoduodenal mesenteries that form the lesser omentum.
Fig. 15-10.
8/10/2019 Chapter 15 Stomach
17/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 17/
Peritonea l reflections and ligaments of s tomach. (Modified from Skandalakis JE, Gray SW, Rowe JS Jr. Anatomical Complications in Gene ral Surgery. NewYork: McGraw-Hill, 1983; with permission.)
Falciform and Coronary Ligaments
The falciform ligament, a remnant of the embryonic ventral mesentery, extends from the abdominal wall to the diaphragm and anterior surface of thliver. The free edge of the ligament contains the round ligament (the obliterated left umbilical vein).
The leaves of the falciform ligament separate as they reach t he liver to form the anterior, superior, and posterior (inferior) layers of the coronary
ligament. Laterally, these layers reunite to form the right and left triangular ligaments. On the left, the anterior and posterior layers of the c oronaryligament are almost in apposition until they reach the abdominal esophagus. On the right, the layers diverge as they approach the inferior venacava. Their wide separation is characteristic of the "right coronary ligament."
In reality the so-called right and left coronary ligaments do not exist as separate entities, but for descriptive purposes it is convenient for thesurgeon to use these terms for naming the left and right parts of the coronary ligament. From a surgical standpoint, the division of the left triangulaand left c oronary ligaments as a unit is anatomically justified for the exposure of the gastroesophageal junction. The surgeon must be careful toavoid the left hepatic vein, which is situated in the upper part of the left segmental fissure. (Our advice: After the left triangular ligament andlateral half of the left coronary ligament are cut by scissors, approach the gastroesophageal junction by finger dissection.)
Hepatogastric Ligament (Lesser Omentum)
The hepatogastric ligament is the proximal part of t he lesser omentum. It extends from the porta hepatis to the lesser curvature of the stomach anupward as the ventral mesentery of the abdominal esophagus. The ligament regularly c ontains the left gast ric artery and vein, hepatic division ofthe anterior vagal trunk, anterior and posterior gastric divisions of the vagal t runks (nerves of Latarjet), and lymph nodes and vessels. Also, in abouone-quarter of individuals, one can encounter an aberrant left hepatic artery in the proximal part of the hepatogastric ligament. Distally, and to the
right, the hepatogastric ligament contains branches of the right gast ric artery and vein. In this region also are the common hepatic artery and portavein; here they rise ventrally to gain their positions in the hepatoduodenal segment of the lesser omentum.
Hepatoduodenal Ligament
The hepatoduodenal ligament is the dextral part of the lesser omentum, extending from the liver to the first 2.5 cm of the duodenum. The free edgeenvelops the hepatic triad, which includes the proper hepatic artery, portal vein, and extrahepatic biliary ducts, in addition to the hepatic plexusand lymph nodes. By definition, the proper hepatic artery is the part of the artery distal to the origin of the gast roduodenal artery. An aberrant righ
hepatic artery, arising most commonly from the superior mesenteric artery (18-20%),15,16may ascend toward the liver on the deep, or posterior,aspect of the structures within the hepatoduodenal ligament.
Weiglein17studied the topography of the arteries in the lesser omentum in 138 cadavers. Only 9% had "normal" anatomy; the rest exhibited one ormore of the following variations (Figs. 15-11, 15-12, 15-13 and Tables 15-4, 15-5, 15-6):
Aberrant hepatic arteries, 37%
Artery in border of hepatoduodenal ligament, 19%
Right hepatic artery crossing porta l vein posteriorly, 4%
Right hepatic artery entering triangle o f Calot ante riorly, 29%
Right hepatic artery entering triangle o f Calot pos teriorly, 7%
Accessory left gastric artery branching off left hepat ic artery, 2%
Table 15-4. Variations of Arteries in the Lesser Omentum
8/10/2019 Chapter 15 Stomach
18/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 18/
NORM = incidence of no rmal anatomy, AGAS = incidence o f accessory left gas tric artery, CALOT = incidence of right hepatic arte ry crossing the commonhepatic duct arteriorly or never, LIG = incidence of an artery in the free border of the hepatoduodenal ligament, AHA = incidence o f aberrant hepatic arteries
Source:We iglein AH. Variations and topography of the arte ries in the less er omentum in humans. Clin Anat 9:143150, 1996; with permission.
Table 15-5. Incidence of Aberrant Hepatic Arteries
NORM = right and left hepatic artery branching off the proper hepatic artery, AHAD = aberrant right hepatic artery, AHAS = abberant left hepatic artery, AHAD+ AHAS = aberrant right and le ft hepat ic arteries.
Source:We iglein AH. Variations and topography of the arte ries in the less er omentum in humans. Clin Anat 9:143150, 1996; with permission.
Table 15-6. Variations of the Right Hepatic Artery in the Triangle of Calot
POST = right hepatic artery crossing the common hepatic duct po steriorly (normal ana tomy), ANT = right hepatic artery crossing the common hepatic duct
=
8/10/2019 Chapter 15 Stomach
19/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 19/
, .
Source:We iglein AH. Variations and topography of the arte ries in the less er omentum in humans. Clin Anat 9:143150, 1996; with permission.
Fig. 15-11.
8/10/2019 Chapter 15 Stomach
20/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 20/
Variations of arteries in les ser omentum. A,Normal patte rn. B,Aberrant right hepatic artery (replacing type). C,Aberrant right hepatic artery (accessorytype). D,Aberrant right hepatic artery (anastomosis w ith common/left hepat ic artery). E,Right hepatic artery to right of bile duct. F,Cystic artery to right ofbile duct. G,Right hepatic artery branching off gastroduodenal artery to right of bile duct. H,Right hepatic artery crossing porta l vein posteriorly. I,Aberrant left hepa tic artery (replacing type): hepatos plenic trunk and isolated left gastric artery. J,Aberrant left hepa tic artery (accessory type). K,Aberrant left and aberrant right hepatic artery: gastrosplenic trunk and hepatic artery branching off superior mesenteric artery. L,Triple vascularization:aberrant left, aberrant right, and proper hepatic artery. M,Accessory left gastric artery branching off left hepat ic artery. N,Triangle o f Calot: right hepaticartery dorsa l to hepatic duct (64%). O,Triangle of Calot: right hepatic artery ventral to hepatic duct (29%). (Modified from Weiglein AH. Variations andtopography of the arte ries in the less er omentum in humans. Clin Anat 9:143-150, 1996; with permission.)
Fig. 15-12.
Aberrant left hepa tic artery (L) branching off top of left gastric artery (G). Aberrant left hepatic artery gives rise to e sophagea l branches, celiac trunk,splenic artery (S), and common hepatic artery (H). (From Weiglein AH. Variations and to pography of the arteries in the lesse r omentum in humans. Clin Ana9:143-150, 1996; with pe rmission.)
Fig. 15-13.
8/10/2019 Chapter 15 Stomach
21/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 21/
Triple vascularization of the liver. Parts of the liver supported by a separate liver artery are broken apart. A,Aberrant right hepatic artery branching off
superior mesenteric artery. B,Proper hepatic artery branching off common hepatic artery. C,Aberrant left hepa tic artery branching off left gas tric artery.(From Weiglein AH. Variations and topography of the arte ries in the less er omentum in humans. Clin Anat 9:143-150, 1996; with permission.)
DERIVATIVES OF THE DORSAL MESENTERY
The primitive dorsal mesentery gives rise to three structures in the upper part of the abdomen (Fig. 15-10): the gastrocolic ligament (not shown),gastrosplenic ligament, and gastrophrenic ligament.
Occasionally in the operating room and in the anatomic laboratory especially with fresh cadavers one of the authors of this chapter (JES) hasseen several inconstant, or anomalous, peritoneal folds (derived from lesser omentum) which extended between the gallbladder and the duodenum,colon, or stomach in that order of frequency (Fig. 15-14). It is uncertain whether there is a relationship between these folds and the correspondingfistulous tracts of gallstone ileus; however, it is possible that these folds predispose to gastric, duodenal, and right colonic fistulae. This ishypothetical, of c ourse, and reminds us of the gubernaculum test is with its t ails (which of course do not exist) and its physiologic (normal orabnormal) destiny during the testicular descent .
Fig. 15-14.
8/10/2019 Chapter 15 Stomach
22/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 22/
Inconstant peritoneal folds of gallbladde r to duodenum, colon, or stomach (in order of frequency). (Modified from Skanda lakis JE, Gray SW. Surgicalanatomy of intestinal obst ruction. In: Fielding LP, We lch J (eds). Intestina l Obstruction. New York: Churchill Livingstone, 1987; with pe rmission.)
Gastrocolic Ligament
The gastrocolic ligament is a portion of the greater omentum. It passes from the greater curvature of the stomach and the first part of theduodenum to the transverse colon, to which it is fused. On the left and craniad, it is continuous with the gastrosplenic ligament.
The gast rocolic ligament c ontains the right and left gastroepiploic (gast roomental) arteries and veins. If the recess of the omental bursa passesdownward into the sac of the apronlike omentum, the gastrocolic ligament is said to be absent .
Gastrosplenic Ligament
The double-layered gastrosplenic ligament (Fig. 15-10) attaches to the greater curvature of the stomach. It is a downward continuation of thegastrophrenic ligament, or perhaps the gast rophrenic ligament is a cont inuation of the gast rosplenic ligament. Both are parts of the dorsalmesentery.
Michels15showed that only the anterior leaf of the dorsal mesentery becomes entirely free to form the gast rosplenic ligament. The posterior leafdoes not reach the gastroesophageal junction, so that there is a small "bare area" on the posterior wall of the st omach. The bare area lies over theleft c rus of the diaphragm, and is easily separated from it by t he surgeon's index finger. The left adrenal gland and the left gastric artery and vein lclose to this area.
Within the gastrosplenic ligament are:
Upper part: Short gastric arteries and veins and lymph nodes
Lower part: Left gastroepiploic artery and vein, terminal branches of the splenic artery, and lymph nodes
Gastrophrenic Ligament
The gastrophrenic ligament (Fig. 15-10) is continuous with the hepatogastric ligament to the left, or perhaps, opposite the esophagus. It has anavascular area through which the surgeon's finger can safely pass and through which a Penrose drain can be inserted around the cardia to pull dowthe esophagus. This is a useful maneuver in vagotomy.
Within the lower part of the gastrophrenic ligament are short gastric arteries and veins and lymph nodes. The upper part is avascular.
PHRENOESOPHAGEAL LIGAMENT
The esophagus is attached to the diaphragm at the hiatus by a strong, flexible, "airtight" seal known as the phrenoesophageal ligament (F ig. 15-15)The pleura and peritoneum ensure that the seal is "airtight," while collagen and elastic connective-tissue fibers provide strength and flexibility.
Fig. 15-15.
8/10/2019 Chapter 15 Stomach
23/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 23/
Coronal section through gastroesophageal junction and esophageal hiatus of diaphragm. (Modified from Skandalakis JE, Gray SW, Rowe JS Jr. AnatomicalComplications in Gene ral Surgery. New York: McGraw-Hill, 1983; with pe rmission.)
The fibers arise from the endoabdominal fascia of the diaphragm, pass through the hiatus, and insert into the adventitia and intermuscular
connective tissue of the esophagus 1 or 2 cm above the hiatus.18,19A second leaf of the fascia turns downward and inserts into the adventitia ofthe abdominal esophagus and stomach. A much weaker and less constant component arises from the endothoracic fasc ia and passes upward to join
the f ibers of the endoabdominal fascia.20,21The fibers allow about 2 cm of vert ical movement of the esophagus.22
The phrenoesophageal ligament is best seen in infants and children. With age, the esophagus is less firmly fixed in the hiatus, the ligament becomesless definitive, and fat appears between the surviving fibers. In our experience, by middle age the ligament has lost much of its identity. For all
practical purposes, it does not exist in patients with longstanding hiatal hernia.23
GREATER OMENTUM
From a surgical standpoint the greater omentum can be divided into two parts: an upper part, the gast rocolic ligament (desc ribed previously), and alower part, the true "greater omentum" or fat apron. The greater omentum is formed by four peritoneal layers, two anterior and two posterior, whichusually fuse together during development and growth (Fig. 15-16). Another late development is the fusion of the posterior layer to the transversecolon and the mesocolon, forming the "transverse mesocolon," which therefore also has four peritoneal layers.
Fig. 15-16.
8/10/2019 Chapter 15 Stomach
24/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 24/
Formation of greater omentum. A,After rotation of stomach and formation of omental bursa . B,First fusion of posterior wall of omental bursa to transversecolon and mesocolon. C-D,Second fusion or atta chment of anterior and pos terior walls of omental bursa to form adult omentum. S, Stomach. P, Pancreas.C, Colon.
In infancy and childhood, the omentum is small and not well developed. The width and length of the adult omentum differ from individual toindividual.
The greater omentum serves as the "policeman" of the peritoneal cav ity, exhibiting protect ive act ion in inflammatory processes. It also serves as a
depository for tumor metastases in ovarian carcinoma. Fukatsu et al.24stated t hat the greater omentum may play an important role in host defenseas a source of exudative neutrophils.
Blood Supply of the Greater Omentum
The blood supply of the greater omentum is presented very well by our late respect ed friend, Charles A. Griffith, in Surgery of the Esophagus,
Stomach, and Small Intestine.25We highly recommend this chapter.
The right gastroepiploic (gastroomental) branch of the gast roduodenal artery (Fig. 15-17) and the left gast roepiploic branch of the splenic arteryusually anastomose along the greater curvature of the stomach. The right and left gastroepiploic arteries form the arc of Barkow through their rightand left epiploic (omental) branches in the posterior omental layer. The arc of Barkow is reinforced by anterior epiploic arches which spring from theright and left gastroepiploic arteries and from posterior epiploic branches from the panc reatic vessels.
Fig. 15-17.
8/10/2019 Chapter 15 Stomach
25/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 25/
Arterial supply to greater omentum.
To maintain the viability of the omentum in surgery, the arc of Barkow can be preserved by several techniques.
For mobilization of the right side of the omentum:
1) transect the gast rocolic ligament inferior to the right gastroepiploic artery
2) ligate the anterior epiploics or the right gast roepiploic artery distal to the origin of the right epiploic vessels
For mobilization of the left side of the omentum:
1) ligate only the gastric branches of the left gastroepiploic arches
2) do not ligate the left epiploic arteries
Surgical Applications
Be aware of the relationships among the greater omentum, gastrocolic ligament, and transverse mesocolon. Remember the following:
The two-layer gastrocolic ligament (see "Embryogenesis" in chapter on peritoneum and omenta), whether short or long, is the best pathway for lesser saexploration, especially close to the greater curvature.
Be careful with the 6-layer gastrocolic ligament. All the layers are fused and the middle colic artery as well as other omental vessels may be the cause ofcomplications.
Gastric Divisions
The two well-defined borders of the stomach are the lesser and greater curvatures. Five arbitrarily defined regions are the:
cardia
fundus
8/10/2019 Chapter 15 Stomach
26/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 26/
body
antrum
pylorus
In many anatomy texts, the pylorus is subdivided into the pyloric antrum, pyloric canal, and pyloric sphincter. The antrum is the funnel shapedsubdivision of the pylorus which leads into the pyloric canal. T he canal leads to the pyloric sphincter, which is more uniform in diameter. Often,"pylorus" is used synonymously to indicate that which is referred to in textbooks as the pyloric canal, or to the area of the pyloric sphincter.
The stomach is subdivided into its parts by lines (Fig. 15-18A) that very oft en are more imaginary than real:
A horizontal line passes from the cardiac orifice to the greater curvature, separating the fundus from the body, or corpus
An oblique line begins at the angular notch, and traverses the stomach roughly perpendicular to the greater curvature, thereby separating the corpus fromthe pyloric antrum
An oblique line extends superiorly from the sulcus intermedius of the greater curvature to the lesse r curvature, separating the pyloric antrum from thepyloric canal
Fig. 15-18.
8/10/2019 Chapter 15 Stomach
27/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 27/
Morphologic and physiologic presentations of stomach. A,Three imaginary lines subdivide stomach. The first separates fundus from body, secondseparates body from pyloric antrum, third separates pyloric antrum from pyloric canal. B,Distribution of parieta l (acid-secreting) cells in the areas of the
stomach, each relative to the other. Percentages indicate that the maximal concentration of cells is in the body; in the fundus the concentration is abouthalf that of the body; along the lesser curvature, about three-fourths. C,The area in which gastrin is produced by the pyloric glands; and the areas (cardia,pylorus, and proximal duodenum) in which mucus is produced . In the proximal duodenum, the mucus is secreted by the Brunner's glands. (Data in Band Cfrom Berger EH. The distribution of pa rietal cells in the s tomach: a histotopographic study. Am J Anat 54:87, 1934.)
Neither in the operating room nor in the anatomy laboratory do we regularly find the angular notch and the sulcus intermedius. Thegastroesophageal junction, lesser and greater curvatures of the stomach, and gastroduodenal junction with the prepyloric vein of Mayo as anadditional landmark if present are the only visible landmarks. Therefore, for all practical purposes, there are no clear external landmarks to help the
surgeon or anatomist acc urately define the funct ional subdivisions of the stomach. We therefore agree with Griffith26that histologic and physiologicstudies are necessary for the delineation of the several parts of the stomach.
Morphology of the Stomach
In the ancient fable, several blind men encountered and touched an elephant, each touching a different part. Each then proceeded to describe theform of the elephant as he perceived it. The one who had felt the tail thought the elephant to be much like a snake; the second, who had felt the
belly of the huge beast, described the animal as seeming like a wall; to the third, who had felt a leg, it seemed like a tree; and so on. In somewhatsimilar fashion, the stomach has been desc ribed from different points of view in textbooks and other literature.
The embryologist describes the stomach as a fusiform dilatat ion of the foregut, beginning at the gast roesophageal junction and ending at thegastroduodenal junction.
The anatomist describes the stomach in terms of its several parts, such as the gast roesophageal junction, cardia, fundus, body, antrum, pyloriccanal, and sphincter, but also accepts the stomach as a distinct entity, a well-defined organ that is easily visualized, dissected, and demonstrated.
The physiologist and gast roenterologist desc ribe the endocrine and exocrine stomach, t reating the organ as two units, proximal and distal:
Proximal stomach. The proximal stomach (fundus and body) (Fig. 15-18A) receives and temporarily stores gastric contents. It is the home of the parieta lcells (Fig. 15-18B) which secrete acid and intrinsic factors, as well as the home of the cells that produce Group 1 pepsinogen.
Distal stomach. The distal stomach (antrum and pylorus) (Fig. 15-18A) mixes and p ropels gastric contents. It also contains the area of the pyloric glandswhich produce the hormones gastrin and somatostatin (Fig. 15-18C).
Chang et al.27reported that the distal stomach plus pylorus are likely to exert an important inhibitory mechanism in the regulation of gastrointestinamovement; vasoactive intest inal peptide was not found to be a major mediator of motility.
Relative to the maximal concentration of ac id cells existing in the corpus (Fig. 15-18B), the concentration of acid cells in the fundus is approximatel
one-half; along the lesser curvature, about three-fourths.28Both units proximal and distal work to produce Group II pepsinogens and
bicarbonate. Debas29states, "In truth, the entire stomach functions as both an endocrine and exocrine organ."
The pathologist recognizes three subdivisions of the stomach: the fundus, body, and antrum. These provide the basis for descriptions of localizedgross pathology.
The radiologist, in practical terms, locates the gastroesophageal junction just "below the junction," and refers to the first part of the duodenum asthe duodenal bulb.
From the surgeon's viewpoint, the stomach is part of two almost-separate organ systems, each with its special pathology and surgical approach.
" "
8/10/2019 Chapter 15 Stomach
28/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 28/
e rs o ese sys ems can e ca e e proxma gas rc un g. - , an con a ns e proxma s omac , s a esop agus, anesophageal hiatus of the diaphragm. The second is the "distal gastric unit" (Fig. 15-20), and includes the gast ric antrum and pylorus, together withthe first part of the duodenum.
Fig. 15-19.
Proximal gastric surgical unit (shaded area). (Modified from Skanda lakis JE, Gray SW, Rowe JS Jr. Anatomical Complications in General Surgery. New York:McGraw-Hill, 1983; with permission.)
Fig. 15-20.
Distal gast ric surgical unit (shaded area). Most gas tric surgery takes p lace in this area. (Modified from Skandalakis JE, Gray SW, Rowe JS Jr. AnatomicalComplications in Gene ral Surgery. New York: McGraw-Hill, 1983; with pe rmission.)
Proximal Gastric Surgical Unit
As noted above, t he proximal gastric unit (Fig. 15-19) consists of the distal esophagus, esophageal hiatus, and proximal stomach. The esophagus
joins the stomach in the abdomen, just below the diaphragm. The length of the abdominal esophagus is from 0.5 to 2.5 cm.30,31Allison32haspointed out that, by taking the level of the lowest connective tissue fibers attaching the esophagus to the diaphragm as the inferior limit of themediastinum, there is technically no "abdominal" esophagus. In spite of this view, the surgeon has ac cess to an appreciable length of esophagusbelow the diaphragm.
The abdominal esophagus lies at the level of the 11th or 12th thoracic vertebra, perhaps lower in tall, asthenic subjects, and higher in short
subjects.31Its relationships to surrounding structures are:
Anterior: Posterior surface of left lobe of liver
Pos terior: Right crus of diaphragm, aorta
8/10/2019 Chapter 15 Stomach
29/129
8/10/2019 Chapter 15 Stomach
30/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 30/
. - .
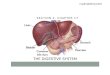
Relation of stomach to other organs in cadaver. A,Anterior relations. B,Pos terior relations. Remember: in a living patient, these re lations are highly
variable. (After Anson BJ (ed). Morris' Human Anatomy, 12 thEd. New York: Blakiston Division, McGraw-Hill, 1966, Fig. XI-52.)
Posterior relations are with the upper part of the lesser sac, the aorta and celiac axis and its branches, and the celiac ganglion and plexus.
Anteriorly the proximal unit is related to the anterior abdominal wall, left hepatic lobe and anterior segment of the right lobe, and diaphragm.
Remember
Anterior and posterior relations are quite variable.
The most important relation of the proximal gastric unit is with the left gastric artery, which should be ligated at its origin to include the lymph nodesassociated w ith it and the celiac axis.
Distal Gastric Surgical Unit
From an embryologic, physiologic, and certainly a surgical viewpoint, the gastric antrum, pylorus, and first portion of the duodenum form a unit
-
8/10/2019 Chapter 15 Stomach
31/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 31/
. - . ,to the general surgeon) than the proximal gastric unit.
GASTRIC ANTRUM
In the opened stomach, the antrum is easily distinguished from the body of the stomach by its mucosa, which is flatter and without rugae. The
antrum (Fig. 15-18A) begins just distal to the t ermination of the gast ric canal.45It is also histologically distinct, being without chief or parietal(acid-producing) cells.
The margin of the antrum is irregular, but definite. Externally, the antrum is difficult to demarcate. The boundary on the lesser curvature usually lies
at t he incisura angularis, usually found in textbook drawings, but inconstant and oft en absent in the operating room. We agree with Griffith25that"in the operating room this landmark either cannot be found or can be only vaguely located."
If the surgeon is not planning a gastrotomy to locate the antral margin, he or she can use the "crow's foot" of the anterior descending vagal trunkas a landmark (see "Anterior Gastric Division" under "Gastric Innervation" below). The antrum can be expected to begin 3 to 4 cm cranial to the"crow's foot," about 8 to 10 cm proximal to the pylorus. There is no good landmark on the greater curvature. In most cases the boundary extendsfrom a point on the lesser curvature two-fifths of the way from the pylorus to the esophagus to a point on the greater curvature one-eighth of thedistance from the pylorus to the esophagus.
PYLORUS
The pylorus (Fig. 15-18A) is a region of the stomach variously c alled the pyloric canal, pyloric ring, and pyloric valve. Proximally, it merges into thegastric antrum without a definite external boundary; distally, it ends abruptly at the thin-walled duodenum. At its narrowest point, the luminal
diameter never exceeds 19 mm.46,47The size is important in estimating the optimal size of artificial openings, such as in gastrojejunostomies orpyloroplasties.
At t he pyloroduodenal junct ion, the continuity of the c ircular musculature is interrupted by an anular septum that arises from the connect ive tissueof the submucosa. Proximal to this ring, the c ircular muscle layer is thickened to form the pyloric sphincter (Fig. 15-22). Distal t o the ring, the
circular muscle coat at the duodenum is thinner. The sudden decrease in wall thickness as one passes from the pylorus to duodenum results in an"os pylorus," surrounded by a duodenal "fornix."48The existence of this fornix must be kept in mind when performing pyloromyotomy.
Fig. 15-22.
8/10/2019 Chapter 15 Stomach
32/129
8/10/2019 Chapter 15 Stomach
33/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 33/
Gastric Wall
The gastric wall consists of the serosa, the muscular layer, the submucosal layer, and the mucosal layer.
Serosa
The serosa is nothing more than the peritoneum, a thin layer of loose connective tissue underlying a layer of simple squamous mesothelium.
Muscular Layer
The st ructure and arrangement of the muscular layer will differ, depending on the type of specialization of the person who speaks of it; each will be
correct. The anatomist describes the three well-known layers of musculature: an outer longitudinal layer, middle circular layer, and inner obliquelayer. The surgeon considers the three layers as one in the operating room. An investigator or a researcher sees that the muscular layer and the
formation of gast ric and duodenal ulcers might be related (a concept postulated by Oi50-54and discussed in this chapter under "Oi Concept").
The outer longitudinal layer of muscle is present along the lesser and greater curvatures. Its fibers are arranged into two groups. The first set iscont inuous with the outer smooth muscle layer of the esophagus. The f ibers are best developed along the curvatures, ending proximal to the pyloricregion. The second set begins in the body and passes to the right, with the f ibers becoming thicker as they near the pylorus. Some of the moresuperficial longitudinal muscle fibers are continuous with those of the duodenum. As noted previously, other longitudinal fibers turn inward at thesphincter, becoming interlaced with its circularly arranged muscle layer.
The middle circular layer rather uniformly encircles the entire stomach and "is the principal part of the muscular coat," according to Woodburne.55
This layer becomes thicker at the pylorus, most distally forming the pyloric sphincter. The c ircular muscle bundle is cont inuous with the c ircular
muscle layer of the esophagus, but is separated from that layer of the duodenum by a septum of connect ive tissue.56
The inner oblique muscle layer, internal to the circular layer, is limited to the body of the stomach and is most developed near the cardiac orifice.These f ibers sweep away from the c ardiac orifice (many are nearly parallel with the lesser curvature) forming a rather distinct edge to this layer tothe left of the lesser curvature. Other fibers, passing to the left, blend with the circular fiber layer as they approach the greater curvature.
The muscle layers of t he stomach are responsible for gastric motility.
We quote from Sun et al.:57
[I]n adults who have had pyloromyotomy for infantile hypertrophic pyloric stenosis in infancy, patterns of pyloric motility are abnormal; pylorictone is higher, whereas the number and amplitude of phasic pyloric pressure waves are less...the stomach has the capacity to compensatefor changes in pyloric motility to minimize effects on gastric emptying.
Submucosal Layer
The submucosa is composed of loose, areolar connective tissue which connects the mucosa to the external musculature. It can be called the"vascular layer" (both arterial and venous) of the gastric wall. It houses plexuses that have rich anastomoses through extensive ramifications thatform excellent collateral flow. All the parts of the gastric mucosa receive blood from these submucosal plexuses except the lesser curvature, which
receives blood from the right and left gastric arteries. Griffith25describes the submucosal plexus very well in his chapter on anatomy of the stomachand duodenum.
Mucosal Layer
Griffith's organization of t he layers of the wall of the stomach is very practical and very "surgical."25,26Following here, interspersed withmodifications, is a summary of that organization which includes the distal esophagus, cardia, fundus and body, antrum, and proximal duodenum.
The distal esophagus is lined by stratified squamous epithelium, with mucous cells in the abdominal esophagus. Some esophageal mucosal glands(which are called cardiac glands because of their resemblance to others in the cardiac portion of the stomach) are located in the lamina propria.
These secrete too little mucus to be protective against acid reflux from the stomach, however.58
A study by Fass and Sampliner59found that squamous cell extension into the proximal stomach is a newly recognized mucosal abnormality withpresently unknown clinical significance. This mucosal abnormality may represent an esophageal mucosal response to proximal gastric injury.
The cardia contains simple columnar cells. There is some minimal mucus production at the cardia. The small mucus-secreting, simple and branchedtubular glands of the cardia contain a variable number of the ac id-producing parietal c ells.
The fundus and body contain two types of cells: parietal (oxyntic) acid-secreting cells and chief pepsin-secreting cells.
The lamina propria of the fundus and body is filled with branched, tubular gastric glands. The neck and base of these glands contain parietal, c hief(zymogenic), and enteroendocrine cells.
The cytoplasm of the parietal cells is very rich in mitochondria. According to Debas,29this is indicative of the high energy requirement of acidsecretion. The parietal cells may also produce gastric intrinsic fac tor, which is extremely important in the absorption of vitamin B12, significant in
preventing pernicious anemia. Parietal cells also produce histamine, which is a strong stimulus for acid secretion.
The chief cells contain the inactive enzyme pepsinogen and also produce the enzymes pepsin and lipase. When pepsinogen is released into the ac id
environment of the stomach, it converts into the highly active proteolytic enzyme pepsin.60
The enteroendocrine cells produce serotonin and endorphin, which ac t not only as gast rointest inal hormones, but also as neurotransmitters in the
8/10/2019 Chapter 15 Stomach
34/129
8/10/2019 Chapter 15 Stomach
35/129
8/10/2019 Chapter 15 Stomach
36/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 36/
An algorithm of suggested selective treatment of a duodenal ulcer that has perforated. Asteriskindicates future consideration of elective ulcer-definitivesurgery. (Modified from Donovan AJ, Berne TV, Donovan JA. Perforated duodenal ulcer: An alternative therapeutic plan. Arch Surg 1998; 133:1166-71; withpermission.)
Chang et al.82reported that patients who underwent part ial duodenectomy with highly select ive vagotomy for obst ructing duodenal ulcer gainedweight. Further, the surgery was successful in restoring gastric emptying almost to normal.
Uravic et al.83advocated that the treatment of choice for duodenal obstruction secondary to chronic pancreatitis is vagotomy andgastroenterostomy.
Peptic Ulcer Disease
Any discussion of pept ic ulcer disease encompasses issues of anatomy, histology, and physiology. There are also questions of terminology andnomenclature for the condition itself. Is the term "peptic ulcer" correct? Maybe not. The terms "gastric" and "duodenal" are more exact .
What anatomic ent ity or physiologic act ion is responsible for the genesis of gastric and duodenal ulcers? Is the muscular network, the mucosal layeror both, responsible for the production of peptic ulcer disease?
It is known that the ulcer (Fig. 15-24) always occurs at the alkaline side of the gastroesophageal junction. It is known that excess formation ofhydrochloric acid and pepsin is responsible for the genesis of peptic ulcer disease, together with a lack of protection of gastric and duodenalmucosa.
Fig. 15-24.
8/10/2019 Chapter 15 Stomach
37/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 37/
Ulcers always form on alkaline side of junction in peptic ulcer disease.
Lu and Schulze-Delrieu84stated that the most common site for peptic lesions in the pyloric segment was the protuberance of the lesser curvaturecalled the pylorus torus. Many torus lesions extended into the destroyed distal pyloric muscle loop, c ausing widening of the gast ric outlet andincreased duodenogastric reflux.
Sometimes we are also confused by the so-called postbulbar ulcer. Is that ulcer located distal to the junction of the first and second parts of theduodenum, or is it located just distal to that part of the duodenum that is covered c ompletely by the peritoneum? Remember, the f irst part of theduodenum is covered with peritoneum; the second part is located retroperitoneally. In other words, is the diagnostic "fleck" of the radiologist bulbarpostbulbar, or just duodenal? Is the duodenal bulb or cap the first part of the duodenum in toto, and, if so, where is the normal or abnormal "fleck"located? Does that "fleck" appear to represent the presence of an ulcer when it ac tually is just a "normal" collection of barium between rugae at theapex of the bulb? We don't know. We are c onfused, and we are afraid that our radiologists may be uncertain also.
In this region, the anatomy of the duodenal mucosa must be interpreted by the sixth sense of the radiologist. Where exactly does the duodenalmucosa change from the "antral-like mucosa" to the parallel plicae mucosa of the small bowel? Does this happen at the middle of the bulb or at theend of the bulb? Radiologists, at least in conference, do not agree.
According to Portis and Jaffe,85the postbulbar ulcer is located 5 cm distal to the pyloric ring. If we accept the number that represents theaccepted length of the first part of the duodenum, then when we say postbulbar, we mean the area between the first part and the second part ofthe duodenum.
Duodenal Ulcer: Contributing Factors/Pathophysiology
High HCl
High pepsin
Low o r abnormal mucus
Low a lkaline pancreatic juice
Low bile
Hereditary factors
High stimulation of the vagus ne rves
In 10% of cases,86there is no duct of Santorini. Maybe this is an additional cause for the genesis of duodenal ulcer.
Gastric Ulcer: Contributing Factors/Pathophysiology
Normal, or low HCl
Low resistance of the gastric mucosa
Drug induced
Bile gast ritis
Remember
For all practical purposes, the gastric mucosa is covered by mucus secreted by the mucus-secreting cells. The parietal cells, forming the tubulargastric or oxyntic glands, secrete hydrochloric acid, pepsinogen, intrinsic factor, and mucus. The pyloric glands secrete mucus, gastrin, andpepsinogen.
Of the four types of mucosa in the stomach, according to Griffith,26the esophageal squamous epithelium is least resistant to ac id-pepsin ulcerat ionFollowing the esophageal squamous epithelium, in order of increasing resistance, are the duodenal mucosa, the antral mucosa, and the parietalmucosa. Because parietal mucosa is the most resistant to acid-peptic ulceration, gastric ulcers are rare there.
Hurwitz et al.87reported that gastric hypoacidity is not directly associated with aging. Their study of elderly white persons indicated that sequelaeof ac hlorhydria, including bacterial overgrowth or malabsorption of drugs, should not be expected.
Sadchikov et al.88believe that gastric ulcers should be regarded as a precancerous condition. Data by LaVecchia et al. 89confirm that the risk ofgastric cancer increases in the presence of gastric ulcer.
8/10/2019 Chapter 15 Stomach
38/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 38/
oncep
In 1959, Oi presented his classic work about locations of gastric, duodenal, and esophageal ulcers. He wrote about the association of esophageal,
gastric, and duodenal ulcers,50the location of gastric ulcer,51and the location of the duodenal ulcer.52Dual control of peptic ulcers by both the
gastric mucosa and musculature was described in 1966,53and a possible dual control mechanism in the origin of peptic ulcer was described in
1969.54Wastell stated,90"Oi's theory is interesting, and it probably largely explains the localization but not the c ause of some duodenal ulcers."
Wastell contends that the distinct ion between gastric and duodenal ulcers "is becoming somewhat blurred" due to evidence that H. pyloriis an
etiological factor for gastric ulcer and gastritis, as well as duodenal ulcer.91
Indicat ions and corresponding operative procedures for ac ute gastritis, gast ric ulcer, duodenal ulcer, and Zollinger-Ellison syndrome are shown inTable 15-8.
Table 15-8. Choice of Operative Procedure Based on Indication
Indication Procedure
Acute gastritis Vagotomy and pyloroplasty with oversewing of erosions or near-total gastrectomy
Gas tric ulce r Subtotal gastrectomy w ith ulcer e xcis ion
Duodenal ulcer
Intractable pa in Pa rieta l ce ll va gotomy
Perfora tio n Simple closure or closure and pa rie ta l ce ll vagotomy
Bleed ing Vagotomy and antre ctomy w ith suture ligatio n of bleeding vessel or
Vagotomy and pyloroplasty with suture ligation
Obstruction Vagotomy and antrectomy
Zollinger-Ellison syndrome Tumor resection or parietal cell vagotomy or total gastrectomy
Source:Ashley SW, Cheung LY. Gastritis and peptic ulceration. In: Miller TA (ed). Physiologic Basis of Modern Surgical Care. St. Louis: CV Mosby, 1988, pp.292-309; with permission.
Helicobacter pylori
The finding in the latter part of the twentieth century that H. pyloricauses ulcer disease is a very significant breakthrough in the field of
gastroenterology. In 1997 Breuer et al.92wrote that at least half of the world's population is infected with H. pylori. Blecker93stated thatcolonization with H. pyloriis determined by childhood factors. Most people infected with H. pylorido not develop peptic ulcers, according to
Wallace,94so it is reasonable to assume that other factors in addition to the bacterium are necessary for the pathogenesis of peptic ulcer disease.
Blum's95historical overview of at tempts to understand helicobact er-assoc iated disorders records the following conflict ing findings. In 1928 Konjetznreported an association between gastritis and gast ric ulcer. But Bchner, in 1927 and 1931, and Schindler, in 1946, reported no assoc iation betweethem. The controversy raged for many years.
It is now well accepted that H. pyloriis associated with peptic ulcer disease and gastritis. Epidemiologic data strongly support an association
between the bac terium and gastric cancer and lymphoma92(Fig. 15-25). In 1983 Isaacson and Wright96concluded that the development of gastriclymphoma originates from mucosa-associated lymphoid tissue (MALT).
Fig. 15-25.
Acquisition of H. pyloriinfection. Association of bacterium, gas tric cancer, and lymphoma. (Modified from Ernst PB, Michetti P, Smith PD (eds). TheImmunobiology of H. pylori: From Pathogenesis to P revention. Philadelphia: Lippincott-Raven, 1997; with permission.)
Stephens and Smith97reported that there is strong evidence that primary gastric lymphoma is assoc iated with H. pylori, and they advised that
8/10/2019 Chapter 15 Stomach
39/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 39/
. .
Yamamoto et al.98stated that there is a relation between residual gastritis and H. pyloriinfection. They also believe that H. pyloriis not the solecause of residual gastritis after partial gastrectomy.
According to Ota and Genta,99H. pyloricolonizes the antral mucosa, oxyntic mucosa, and mucosa of the gastric cardia with equal frequency. A
severe and active inflammation of the entire stomach is called pangastritis. According to Breuer et al.,92duodenal ulcer is assoc iated with an antrapredominant form of gast ritis that leaves acid sec retion from the c orpus intac t. In contrast, progressive multifocal gastritis with at rophy and
intestinal metaplasia is an outcome associated with gastric cancer (Fig. 15-26). Xia et al. 100reported that with H. pyloriinfection, atrophic gastritiand intestinal metaplasia occurs primarily at the gast ric antrum and incisura. Antralization of the gastric incisura in infected pat ients is assoc iatedwith a greater risk of these two conditions.
Fig. 15-26.
Hypothetical natural history of H. pylorigastritis. DU, Duodenal ulcer. GU, Gastric ulcer. MALT, Mucosa-associated lymphoid tiss ue. (Modified from Ernst PB,Michetti P, Smith PD (eds). The Immunobiology of H. pylori: From Pathogenesis to P revention. Philadelphia: Lippincott-Raven, 1997; with permission.)
In the preface to The Immunobiology of H. pylori: From Pathogenesis to Prevention,101the authors write, "Some of the results to date in animalmodels have been so impressive that a vac cine seems to be tantalizingly c lose to reality."
Sontag102advises biopsy and histologic examination of the ulcer. He thinks that a gast ric ulcer may be cured with a regimen of antibiotics, ranitidinbismuth citrate, bismuth, and proton pump inhibitors. Sontag prophesies that gastric ulcer disease will soon be "history."
Feldman et al.103found that serologic testing indicating undetectable antibody levels is a reliable indicator of cure of H. pyloriinfection in patientstreated with antimicrobial drugs for more than one year.
Pernicious Anemia
A study by Hsing et al.104confirmed that patients with pernicious anemia are at risk of developing gastric cancer and several other types of cancer
El-Newihi et al.105presented a c ase of gastric adenocarcinoma assoc iated with pernicious anemia. Sculco and Bilgrami106collected data about 136
patients with pernicious anemia assoc iated with gastric c arcinoid tumors. Becker and Gabriel107reported that gastric carcinoids may develop inpatients with chronic atrophic gastritis with and without pernicious anemia.
Vascular Supply of the Stomach
It is well known that the stomach is among the best vascularized of organs (Fig. 15-27). Not only is it served by many arteries, but its wall alsocontains a rich anastomotic network of vessels extrinsically and intrinsically. General surgeons are well aware of this "friendly enemy" that may workfor them, or against t hem. They know that the stomach c an survive after ligation of all but one of its primary arteries, and that extragastric ligationwill not control bleeding from a gastric ulcer.
Fig. 15-27.
8/10/2019 Chapter 15 Stomach
40/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 40/
Arterial supply to s tomach. L Inf Ph, Left inferior phrenic arte ry. SG, Short gastric artery. LGE, Left gastroepiploic artery. RGE, Right gastroepiploic artery. S,Splenic artery. GP, Great pancreatic artery. Inf P, Inferior pancreatic arte ry. PD, Pancrea ticoduodena l artery. DP, Dorsal pancreatic artery. GD,Gastroduodenal a rtery. RG, Right gastric artery. H, Hepatic artery. CT, Celiac trunk. LG, Left gastric artery. Post G, Posterior gastric artery. (Modified from
Skandalakis JE, Gray SW, Rowe JS Jr. Anatomical Complications in General Surgery. New York: McGraw-Hill, 1983; w ith permission.)
Following is a listing, or summation, of all the arteries that supply the stomach. Each of the principal arteries of supply originates from the celiactrunk.
Left gastric
ascending branch (gives rise to esophageal)
descending branch (gives rise to gastric)
Hepatic
right gast ric
gastroduodenal
anterior superior pancreaticoduodenal
retroduodenal
posterior superior pancreaticoduodenal
supraduodenal
right gastroepiploic (major branches)
Splenic
poste rior gastric
short gastrics
left gastroepiploic (major branches)
Arteries
LEFT GASTRIC ARTERY
In approximately 90% of individuals, the left gastric artery (Fig. 15-27) is a branch of the celiac axis. However, it may arise as an independent unitfrom the common hepatic artery, splenic artery, aorta, or superior mesenteric artery. In 4% it arises from a gastrosplenic trunk; in 3% it has a direc
aortic origin; in 2% the left gast ric is a branch of a hepatogast ric trunk.108Yildirim et al.109reported a case of left gastric artery originating directlyfrom the aorta.
The left gastric artery travels upward and to the left retroperitoneally to the proximal one-third of the lesser curvature of the stomach. Here, in
8/10/2019 Chapter 15 Stomach
41/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 41/
about 95% of cases, it provides esophageal branches. According to Swigart et al.,110it provides origin to 1-3 ascending esophageal branches in78%, and t o a cardioesophageal branch which supplies the esophagus, cardia, and fundus.
The left gastric artery commonly divides into an anterior and a posterior branch before attaining the lesser curvature111and, in such cases, theesophageal and cardioesophageal arteries may arise, variably, from either of those vessels; more commonly, however, the cardioesophageal arteryarises f rom the anterior gastric branch.
After its cardioesophageal branch the left gastric artery usually curves downward to the right and thereafter descends along the lesser curvature.As it desc ends, it bifurcates into an anterior branch which sends branches to the anterior gastric wall, and a posterior branch which, similarly,
supplies the posterior gastric wall. In 25 of 60 specimens, El-Eishi et al.108found both anterior and posterior branches. A smaller continuation of t heleft gastric artery continued along the lesser curvature.
The esophageal branches tend toward rather distinct anterior and posterior distributions toward the dextral side of the esophagus, which are not
associated with the locations of the vagal trunks.108An aberrant left hepatic branch from the left gastric artery occurs in about 30% of cases. 111
The esophageal and cardioesophageal arteries oft en arise from it.108,110,111
Although the esophageal arterial supply is segmental in nature between its cervical and abdominal portions,110anastomoses are rich between
esophageal and gastric branches.111The presence of such anastomoses between intercostal esophageal, left inferior phrenic (Fig. 15-28), and leftgastric branches can result in troublesome retrograde bleeding from these branches on the posterior side of the esophagus.
Fig. 15-28.
8/10/2019 Chapter 15 Stomach
42/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 42/
Arteries of distal esophagus and proximal stomach. A,Inferior phrenic artery supplies margin of hiatus. Esophageal branch of left gastric artery suppliesdistal esophagus a nd passes through hiatus to anas tomose with thoracic esophagea l arteries. B,Branches of inferior phrenic and left gastric arteries
supply distal esophagus with no thoracic anastomoses. C,Branches of inferior phrenic artery supply distal esophagus with thoracic anastomoses (rare).(Modified from Skanda lakis JE, Gray SW, Rowe JS Jr. Anatomical Complications in General Surgery. New York: McGraw-Hill, 1983; w ith permission.)
From its origin, the anterior branch of the left gastric artery angles rather obliquely across the body of the stomach toward the greater curvature. Iends in numerous small ramifications and forms a vascular "crow's foot" (of Payne) similar to the anterior gastric nerve of Latarjet. The anterior
branch terminates about 4-6 cm proximal to the pylorus, about 1 cm from the lesser curvature, by piercing the muscular coat .108
In most cases, the posterior branch follows the lesser curvature a centimeter or two from its edge until it anastomoses with the right gastric artery
When the left gastric artery cont inues along the lesser curvature after providing origin to the anterior and posterior branches, it typically ends as abranch at t he angular notch, and usually anastomoses with the right gastric artery. The first ramus of the posterior branch is relatively large andextensive in distribution, providing supply to the c ardia and proximal posterior part of the c orpus of the stomach.
The anterior and posterior gastric branches may possess direct interconnections with one another or with the continuing segment of the parent left
gastric artery.108
RIGHT GASTRIC ARTERY
The right gastric artery (F ig. 15-27) is a small branch which arises most commonly from the proper hepatic artery (50-68%), left hepatic artery
(28.8-40.5%), common hepatic (3.2%), or other, less frequent sources, as noted by Eckmann and Krahn,112and summarized by Van Damme and
Bonte111and Lippert and Pabst.113Often, the novice student cannot find this thin, tiny artery, which avulses and disappears during dissection.
Some of the discrepancies in description of the usual origin of the right gastric artery are attributable to confusion in the nomenclature of thecommon hepatic and proper hepatic artery. Authors have often used the term "hepatic," without designating whether they are speaking of the
common hepatic artery or its proper hepatic branch.
The right gastric artery gives origin to one or more suprapyloric branches. Anterior and posterior branches from these anastomose with infrapyloricvessels and with the supraduodenal artery, providing for the distal gastric unit (antrum, pyloric canal, first inch (2.54 cm) of the first part of theduodenum). The right gastric passes along the lesser curvature for about 4 to 6 cm, about 0.5 c m from the lesser curvature, before anastomosing
with the left gastric.108In about 13% of individuals, the right gastric artery provides origin for the supraduodenal artery. 111
Several authors, including Wilkie,114Reeves,115Barlow et al.,116Nakayama,117,118and Womack119have studied the blood supply of the lessercurvature, distal stomach, and the f irst part of the duodenum. The reader can refer to their various works for discussions of questions pertaining toadequacy of blood supply, anastomoses, end arteries, and the relations of duodenal ulcer to arterial circulation.
GASTRODUODENAL ARTERY
The gastroduodenal artery (Fig. 15-27) arises as one of the two terminal branches of the common hepatic artery branch of the celiac trunk. Shortlyafter it arises from the c ommon hepatic artery branch, the gastroduodenal artery gives origin to the supraduodenal, retroduodenal, and posteriorsuperior pancreaticoduodenal arteries. The supraduodenal and retroduodenal arteries arise, variably, as branches of the posterior superior
pancreaticoduodenal artery. The gast roduodenal artery ends by dividing into the right gastroepiploic and anterior superior pancreaticoduodenalarteries.
Splanchnic artery aneurysms of the gastroduodenal artery are very rare, and are often missed preoperatively. Konstantakos et al.120reportedobstruct ive jaundice in a pat ient with gast roduodenal artery aneurysm.
RIGHT GASTROEPIPLOIC ARTERY
The right gastroepiploic artery (Fig. 15-27) is a branch of the gastroduodenal artery (or its continuation) in most cases. It occasionally arises fromthe superior mesenteric artery or from the anterior superior pancreaticoduodenal artery. Aft er giving origin to an infrapyloric branch, the arterypasses along the greater c urvature of the distal gastric surgical unit within the gastrocolic ligament. It gives origin to 8-18 singular or paired anterioand posterior branches for the gastric wall.
The gast ric branches of the right gast roepiploic artery pass mostly undivided in a submucosal position about one- fifth of the distance from the
greater curvature. They anastomose extensively with branches from the left gastric artery.108If t he first infrapyloric branch is particularly large, thfirst following gastric branch tends to take its origin further around the greater curvature. In about 75% of individuals, the right gastroepiploic arter
clearly anastomoses with the left gastroepiploic,111although not so profusely as is seen in the anastomoses with the left gastric artery.
We quote from Sakamoto et al.,121who reported an anomalous right gastroepiploic artery arising from the superior mesenteric artery:
The gastroduodenal artery ran in front of the common bile duct and descended along the posterior surface of the head of the pancreas(posterior superior pancreaticoduodenal artery). The enlarged pancreatic branch arising from the superior mesenteric artery mainly suppliedthe anterior surface of the head of the pancreas and then continued to become the right gastroepiploic artery.
For omental viability during distal gastrec tomy, the right gast roepiploic artery should be preserved by one of the following methods: ligating itsgastric branches; ligating the anterior epiploic; or ligating the right gastroepiploic distal and c lose to the origin of the right epiploic. One of theauthors of this chapter (JES) prefers to ligate the gastric branches and to imbricate the greater curvature with continuous absorbable suture at its"nude," not resected part.
LEFT GASTROEPIPLOIC ARTERY
Accordin to Michels15
the left astroe i loic arter Fi . 15-27 is a hi hl variable arter . It arises in most cases 72% from the distal s lenic
8/10/2019 Chapter 15 Stomach
43/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 43/
inferior splenic terminal, middle part of the splenic trunk, or superior splenic terminal. The observations of Van Damme and Bonte 111differ ratherwidely from those of Michels. They state that the left gast roepiploic arises from the splenic direct ly in only 26% of individuals. In 66% it t akes originfrom the splenic artery by a common stem with the inferior polar splenic branch.
The left gastroepiploic artery is the largest branch of the splenic artery.56It reaches the stomach at a point about halfway along the greatercurvature, aft er it has already delivered several rather long branches to the more proximal part of the greater curvature. These branches reach thestomach by way of the gast rosplenic ligament.
The left gastroepiploic artery gives off t he left epiploic and the anterior epiploics. Together with similar branches of the right gast roepiploic, theyform the arc of Barkow (Fig. 15-17), which is reinforced also by t he posterior epiploic branches of the inferior pancreatic artery (see "Blood Supplyof the Greater Omentum" in this chapter).
In splenectomy, ligation of the splenic artery and vein should be located distal to the origin of the left gastroepiploic vessels. Better still, thesurgeon should ligate the splenic vessels very c lose to their entrance into the spleen. This avoids the postoperative bleeding which follows ligationproximal to the origin of the left gastroepiploic artery.
SHORT GASTRIC ARTERIES
Approximately five to seven short gast ric arteries (Fig. 15-27) arise from the terminal branches of the splenic artery or from the left gastroepiploicartery. They may appear to emerge from the substance of the spleen at its hilum, having arisen from terminal splenic branches within the organ. Thshort gastric vessels take care of the arterial blood supply of the fundus and upper part of the body of the stomach. Although their branches aredistributed both to the anterior and posterior surfaces, they appear to supply somewhat more of the posterior surface than the anterior.
The first short gastric artery reaches the greater curvature about 2-6 cm to the left of the esophagogastric junction. 108Some short gastric arterieare quite short; some are long. The shorter vessels are the troublemakers in splenectomy, and careful ligation is a must. Imbrication of the greatercurvature is a safety measure, not only to avoid bleeding, but also to avoid possible necrosis with perforation. The short gastric arteries alone areinadequate to supply the distal part of the proximal gastric surgical unit.
Read an Editorial Comment
POSTERIOR GASTRIC ARTERY
An additional artery may arise variably from the proximal, middle, or distal segment of the splenic artery. It travels upward, posterior to the stomachto vascularize the distal esophagus, cardia and fundus. This is the posterior (or dorsal) gastric artery (Fig. 15-27).
Acc ording to DiDio et al.,122the posterior gastric artery was discovered by Walther in 1729123and named by Haller in 1748. Its presence wasoverlooked by anatomists and surgeons alike for many years. This artery has received greater attention in recent years, particularly because of itspotential c linical significance. Inadvertent ligation or division of the artery can c ause complicat ions including focal necroses and postoperativehemorrhage.
The posterior gastric artery has also been referred to as the accessory left gastric artery or ascending posterior esophagogastric artery.15The
artery is of significant size in one-half to two-thirds of patients.124The posterior gastric artery alone is incapable of supplying the distal part of the
proximal gastric unit.
Estimates of the frequency of appearance of the posterior gastric artery vary widely (Table 15-9), from about 12.7% to 99% of cases, most
commonly ranging from 48% to 68%.124Differences in the data are att ributable in some measure to whether the vessel is identified withangiography or by dissect ion. The c riteria for identification of the vessel differ also. In some studies, an artery was determined to be t he posterior
gastric only if it provided no supply to the spleen.111In others, even if a branch to the superior pole left the vessel before it reached the fundic
region, it might be considered to be a posterior gastric artery if it arose from the splenic artery prior to its distal terminal major splenic branches. 125
Table 15-9. the Posterior Gastric Artery: Frequency of Incidence by Radiography or Dissection
Anatomic Dissections
Year Name of Author %
1910 Piquand 99
1983 Wald and Polk 88
1962 Aboltin 77
1963 Tanigawa (fetal studies) 67.8
1959 Chiarugi 66
1932 Versari 66
1904 Rossi and Cova 65.8
1967 Delteil et al. 64.3
1978 Suzuki et al. 62.3
1968 Levasseur and Couinaud 50
1912 Rio-Branco 50
1957 Weisz and Bianco 48
1991 Berens et al. 48
http://windowreference%28%27editorialcomment%27%2C%27editorialcomment.aspx/?aID=71870&comment_aID=72169%27);http://windowreference%28%27editorialcomment%27%2C%27editorialcomment.aspx/?aID=71870&comment_aID=72169%27);8/10/2019 Chapter 15 Stomach
44/129
5/23/2014 Print: Chapter 15. Stomach
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2015_%20Stomach.htm 44/
.
1985 Trubel et al. 37.5
1967 Kupic et al. 36.8
1963 Tanigawa (adult studies) 36
1988, 1990 Van Damme and Bonte 36
1988 Trubel et al. 27.7
1928 Adachi 21.6
1915 Helm 16
1907 Leriche and Villemin 12.7
1972 Laude et al. 4.0
Source:Data from Berens AS, Aluisio FV, Colborn GL, Gray SW, Skandalakis JE. The incidence and significance of the posterior gastric artery in humananatomy. J Med Assoc Ga 80(8):425-428, 1991; with permission.
The posterior gastric artery arose from the proximal part of the splenic artery and was independent of splenic supply in 46% of cases in radiographic
studies by DiDio et al.124In dissection studies by Berens et al.,126the vessel was found in 36 of 75 specimens (48%) (Table 15-10). It arose from
the first three centimeters of the splenic artery. In studies by Van Damme and Bonte111using combined techniques of radiography, corrosion, anddissection, the posterior gastric artery was found in only 36% of cases. This excluded any cases in which any branch passed to the spleen.
Table 15-10. Reported Incidence of Posterior Gastric Artery
Year Authors Incidence Breakdown
1729 Walther N/A N/A
1745 Haller N/A Origin-Midportion
1796 Sommerring "Sometimes" N/A
1873 Hyrtl "Inconsistent" N/A
1901 Haberer "In most cases" N/A
1904 Rossi and Cova 65.8% 2.5 cm from celiac
1907 Leriche and Villemin 12.7% Origin-Distal
1910 P iquand 99.0% Origin-Distal
1912 Rio-Branco 50.0% Origin-Proximal
1915 Helm 16.0% Origin-Proximal
1928 Adachi 21.6% 3-5 cm from celiac
1931 Testut and Latarjet N/A N/A
1932 Versari 66.0% N/A
1952 Franchi and Stuart