-
1
CHAPTER 1
INTRODUCTION
1.1 Cancer and radiotherapy
Cancer is a term used for disease in which abnormal cells
divides
without control and are able to invade other tissue. The main
treatment
modalities include surgery, chemotherapy and radiotherapy.
Radiotherapy
or radiation oncology is the medical use of ionizing radiation,
generally as
part of cancer treatment to control or kill malignant cells.
Ionizing radiation
works by damaging the deoxy ribo nucleic acid (DNA) of exposed
tissue
leading to cellular death. Aim of radiotherapy is to give
maximum
radiation dose to tumor while minimizing radiation to normal
tissues to
reduce the complications. To spare normal tissues, shaped
radiation beams
are aimed from several angles of exposure to intersect at the
tumor,
providing a much larger absorbed dose there than in the
surrounding
healthy tissue. The three main divisions of radiation therapy
are external
beam radiation therapy or teletherapy, brachytherapy or sealed
source
radiation therapy, and systemic radioisotope therapy or unsealed
source
radiotherapy. The differences relate to the position of the
radiation source:
external is outside the body, brachytherapy uses sealed
radioactive sources
placed precisely in the area under treatment, and systemic
radioisotopes are
given by infusion or oral ingestion.
-
2
1.2 Radiotherapy machines and radiation treatment techniques
Therapeutic external radiation is given to the patients using
the
equipments such as ortho-voltage units, deep-therapy x-ray
machines, tele-
cobalt units and linear accelerators (linacs) which produce
megavoltage x-
rays (figure1.1 and figure1.2). In treating with linear
accelerators having
multileaf collimator (MLC), the treatment volume can be shaped
to
conform to the tumor volume through beam shaping (figure1.3)
and
shielding of normal tissues and critical organs.
Figure 1.1 A medical linear accelerator
-
3
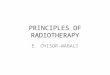
Figure 1.2 Medical linear accelerator and its components
Figure 1.3 Beam shaping with multi leaf collimators
-
4
The technique of radiotherapy with beam shaping and shielding
of
normal structures surrounding tumor volume is called as
3-dimensional
conformal radiation therapy (3-D CRT). Intensity modulated
radiation
therapy (IMRT) is an advanced form of 3-D CRT (figure1.4). In
IMRT,
customized radiation dose is intended to maximize tumor dose
while
simultaneously protecting the surrounding normal tissue. The
transition of
radiotherapy from IMRT to volumetric modulated arc therapy
(VMAT)
made treatment of cancer easier & beneficial (figure1.5). In
VMAT, three
parameters are changing simultaneously - Gantry speed of linac,
MLCs
shape, and dose rate, but in IMRT there is no movement of gantry
during
the treatment and there is no dose rate variation.
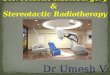
Figure 1.4 3DCRT and IMRT comparison
-
5
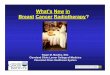
Figure 1.5 IMRT and VMAT comparison
1.3 Importance of accuracy in dose planning and delivery in
IMRT
It is well understood in radiation therapy that the
dose-response
curves are quite steep and there is clinical evidence that a
small change
(5%) in the dose to target volume can result in a change in the
tumor
control probability (ICRU 1976). Along the same argument,
similar dose
change may also result in a sharp change in the incidence and
severity of
radiation-induced morbidity, especially for serial critical
structures such as
spinal cord, optic chiasm, and brain stem. For IMRT and VMAT
the
accuracy in dose planning and delivery is even more important
because
even a small displacement of the delivered dose distribution can
result
changes in doses that exceed the tolerance values for critical
organs and
seriously under dose the tumor volume. Based on clinical
evidence on
effective and excessive dose levels, the consensus in radiation
therapy
community is that the dose delivered to the tumor volume should
be within
5% of the prescribed dose. Therefore, the guiding principle in
establishing
quality assurance (QA) test procedures and in defining tolerance
limits for
-
6
IMRT process is to minimize the overall uncertainty in delivered
dose to
less than 5%.
1.4 Overall process of IMRT, sources of errors and importance
of
patient specific QA
The IMRT process comprises of several steps: treatment
setup,
patient immobilization, computed tomography (CT) image
acquisition,
inverse treatment planning, plan acceptance, plan verification,
and the
actual treatment delivery. With multiple steps involved, there
remains a
large potential for random and systematic errors at each step
along the way.
Of these, the systematic errors are the most significant since
they can have
a huge impact on the final treatment outcome. In a clinical
scenario
therefore, every attempt should be made to reduce such
systematic errors.
The first logical step is to analyze the uncertainties in both
the components
of IMRT QA process – pertaining to machine (machine specific QA)
and
pertaining to individual patient treatment (patient specific
QA). In IMRT,
patient specific QA plays a crucial role because of the
complexities
involved in treatment plan, dose calculation and treatment
delivery.
1.5 Test tools and methods in IMRT patient specific QA
Commonly followed IMRT QA methods include point dose
measurements using a small volume ion chamber, planar dose
measurements using a film or a 2-D array detector, portal
dosimetry etc
[(wagter et al. (2004)]. In advanced QA systems, fluence
measured by a 2-
D array detector can be used to calculate dose to a 3-D volume.
This makes
possible comparison between treatment planning systems (TPS)
calculated
dose volume histogram (DVH) and QA system’s DVH.
-
7
1.5.1 Point dose measurement
Absorbed dose determination using calibrated ionization
chambers
in combination with a well established dosimetry protocol, such
as the
international atomic energy agency (IAEA) protocol, are
generally
assumed to be the gold standard in radiation dosimetry. Under
reference
conditions, the estimated combined standard uncertainty in
the
determination of absorbed dose in high energy photon beams
amounts to
about 1.5%.
As an initial step, during the commissioning of IMRT, the
solid
water phantom with ion chamber (figure1.6) has to be scanned and
the
image set has to be imported to the treatment planning system.
Patient
verification plans can be created in the treatment planning
system for the
absolute dosimetric measurement by exporting the patient
specific IMRT
plans on the image set of IMRT phantom, which saved in the
treatment
planning system. After the 3-D dose calculation, the dose at a
reference
depth in the phantom can be measured from the TPS created
verification
plan. These plans will be executed in the linear accelerator. To
measure the
absolute dose at the reference point, the IMRT water equivalent
phantom
should place on the treatment couch and the ion chamber has to
be inserted
at the level of reference point depth. The measured dose for
each IMRT
fields at reference point is then compared with the TPS
calculated absolute
dose at the same point and the % of variation will be calculated
[Mijnheer et
al. (2008)].
-
8
Figure 1.6 Solid water phantom, ion chamber and electro
meter for absolute point dose measurements
1.5.2 Film dosimetry
Radiographic films have been employed almost since the
discovery
of X-rays to measure radiation dose. The use of radiographic
films are
relatively easy, quick and cheap and therefore very often
applied for many
applications in radiotherapy. It provides data with a high
resolution and a
permanent record of the 2-D dose distribution in the plane of
irradiation.
There are, however, many parameters influencing the film
irradiation, film
processing and data analysis procedure that determine the
accuracy of the
final result. Simultaneous dosimetric measurements in more than
one point
have become an important need for quality assurance in
modern
radiotherapy. Such measurements are traditionally performed
with
radiographic films as a two-dimensional detector. However,
their
application is not straightforward due to many factors of
influence on the
optical density, such as energy and spectral composition, depth,
field size,
orientation, and processing conditions [Kapulsky (2002)].
Additionally, the
increasing number of IMRT patients suggests the use of faster
and more
-
9
efficient dosimetric tools. Finally, many hospitals are aiming
towards a so-
called “digital hospital”, where film-processing machines for
traditional
silver-halide films will not be available or easily accessible
in the near
future [Wiezorek et al. (2005)].
Radiochromic films, which are self-developing, almost tissue
equivalent and therefore shows little energy and directional
dependence,
represent an alternative to radiographic films but their use is
still limited
because they were until recently rather expensive [(wagter et
al. (2004)].
Other factors include cumbersome film handling, sensitivity
variations
across the film, and the low sensitivity to ionizing radiation
doses typically
used in radiation oncology. This prevented their use in external
beam
therapy, and their dominant application in radiation oncology
was limited
to brachytherapy. Figure1.7 shows the film dosimetry set up for
IMRT.
Figure 1.7 Film dosimetry set up for IMRT
-
10
1.5. 3 Portal dosimetry
On-line electronic portal imaging devices (EPIDs) have been
developed for acquiring megavoltage images during patient
treatment.
Megavoltage images, obtained in digital format with such a
device, are
then used for further analysis, mainly for determining set-up
errors. The
image information can, however, also be related to the dose
delivered to
the EPID, yielding dose information in a plane instead of in one
or few
points. EPIDs can serve for several purposes during the
verification
process of IMRT and are used: 1) to verify the leaf position
either during
static (step-and-shoot) or dynamic MLC (sliding window)
techniques; 2)
to check the correct transfer of the leaf sequencing file to the
treatment
machine; and 3) to measure the combined mechanical and
dosimetric
performance of the treatment unit [Prisciandaroo et al. (2004),
Fielding et
al. (2004), Yang et al. (2004)]. More recently the uses of flat
panel
imagers based on amorphous silicon (aSi) are becoming more
popular for
their use as 2-D dosimeters. Most new accelerators are
nowadays
equipped with aSi1000 EPID and it can therefore be expected that
the use
of these devices for IMRT verification will increase in the
future. Several
approaches have been described for the use of EPIDs for
pre-treatment
verification of IMRT delivery [Warkentin et al. (2003), Vieira
et al.
(2004), Budgel et al. (2005), Monti et al. (2006), Winkler et
al. (2006)].
More recently various groups have developed methods to translate
EPID
images into 2-D primary fluence maps, which are then used as
input in a
TPS to recalculate 3-D dose distributions using CT data of a
phantom or
patient. Generally these approaches are able to reconstruct the
3-D dose
distribution in phantoms with a high accuracy.
-
11
Figure 1.8 Linac with inbuilt aSi1000 EPID (black arrow)
The aSi1000 portal imager (figure1.8) is the most recent
detector
used for portal dosimetry. It is a flat panel X-ray imager with
large area
active matrix readout structure and is made up of phosphor or
photo
conductor. This detector is having four major parts- 1mm Cu
build up
plate, a scintillating Phosphor screen, Image forming sensitive
layer and
associated electronics. The Cu build up plate absorb the
incident photons
and emits recoil electrons and also it shields the scintillation
screen from
the scattered radiation. The recoil electrons from the build up
plate are
absorbed by the scintillating phosphor screen and convert it
into visible
light. The image forming layer is a 512 X 384 matrix deposited
on a glass
substrate. Here each pixel in the matrix is having 0.784 mm
pitch and
consists of aSi-n-i-p photo cathode to integrate the incoming
light in charge
capture and a thin film transistor (TFT). The associated
electronics with the
TFT switches enables the charge capture readout. The image
acquisition
system with fast readout electronics enable up to 30 frames per
second is a
-
12
major difference in aSi1000 EPID. The resolution of aSi1000 EPID
is upto
0.39 mm.
Before using the EPID for clinical purpose, the dosimetric
calibration and characteristics study of the portal imager has
to be
performed [Berger et al. (2006), McDermott et al (2006), Greer
et al.
(2007)]. For the IMRT patient specific QA, verification plans
are creating
in treatment planning system using PDIP (portal dose image
prediction)
algorithm. To measure the delivered dose the aSi1000EPID has to
be
placed at the calibrated distance from the source. The
verification plan is
then executed in linac through the networking platform and
control
console. The measured and TPS predicted planar doses for
individual fields
can be compare using the portal dosimetry analysis tool
(figure1.9).
Figure 1.9 Portal dosimetry work flow
-
13
1.5.4 2-D array system
The major benefit of dosimeter arrays are their simple handling
by
connecting them to a computer and the availability of on-line
information.
Two-dimensional (2-D) arrays are more practical as they allow
the
verification of a planar fluence or dose distribution. During
the last years
several systems became commercially available for 2-D dosimetry.
The
most commonly utilized dosimetric principles are ionization in
air or
ionization in semiconductor material, but other principles such
as
scintillation have been applied as well. Advantages of
ionization chambers
are the simple calibration, practically no dead time, which
allows real time
measurement, and no (significant) effect of radiation damage. In
general,
dosimetric properties are governed by the physics principle of
the detector.
The most important ones are dose linearity, energy dependence,
directional
dependence, dose rate dependence, source to detector distance
(SDD) field
size response and temperature response. The various
commercially
available 2-D arrays show differences in the number of
detectors, detector
spacing, detector shape, effective point of measurement,
water-equivalent
build-up layer, backscatter layer, and maximum field size
covered. Most of
these systems can be used for absolute dose measurement after
appropriate
individual calibration procedures to correct for response
variations across
the array. 2-D arrays mounted on the gantry enable IMRT
verification at
gantry angles identical to the ones applied in treatment plans.
For such
procedures detector misalignments and influences of gravity need
to be
considered carefully and corrected for if present.
The commercial 2-D arrays for dosimetric purposes come with
their
inherent evaluation software. It is generally possible to import
calculated
dose distributions from a planning system and to perform 1-D
dosimetric
analysis of profiles or a 2-D gamma evaluation using data of the
whole
-
14
array. The major limitation of 2-D array is it’s limited number
of detectors,
which impairs measurements in high dose gradient regions and in
small
fields. The usefulness of a gamma evaluation, based on
dosimetric
information with a limited spatial resolution is therefore
questionable.
Obviously the limited spatial resolution of the 2-D array
influences the
effectiveness of the verification at some points. For that
reason it is
recommended to combine the results of multiple measurements in
which
the array has been replaced over a small distance. Recently
transmission-
type radiation detectors have been developed that can be
positioned on the
radiation entrance side of the patient. These detectors are
multi wire or
multi-strip ionization chambers connected to a multi-channel
electrometer.
They are designed to be placed in dedicated holders or in
standard
accessory holders of the linear accelerator. As a consequence
the spatial
resolution depends on the mounting distance. Because of their
negligible
attenuation, transmission-type 2-D detectors can be permanently
installed
on accelerators primarily used for IMRT. They enable on-line
monitoring
of beam characteristics or leaf settings with and without the
patient in
place. However, when using such detectors the characteristics of
a certain
device need to be taken into account, including its specific
influences on
the overall QA procedures and dosimetry logistics. Moreover,
besides the
advantage of offering on-line information, 2-D detectors have
the potential
to increase the overall efficiency for IMRT QA. In addition,
these tools can
also be used for QA of linear accelerators used for conventional
treatments,
such as measurement of leaf position, output constancy, beam
symmetry
and field flatness.
There are different types of 2-D array systems available now
in
market for the IMRT patient specific QA. ImatriXX 2-D array
system of
IBA dosimetry, map check 2-D arrays of sun nuclear dosimetry
system, 2-
-
15
D arrays of PTW dosimetry system etc are the commonly using 2-D
array
systems.
ImatriXX 2-D array verification-process
The ImatriXX 2-D array system consists of 1020 parallel plate
ion chamber
arranged in a 32x32 grid, with an inter detector spacing of
7.619 mm. Each
detector is having a diameter of 4.5 mm, height 5 mm and chamber
volume
0.02 cc. To compare the TPS calculated planar dose with the
measured
planar dose the ImatriXX 2-D array system has to place on the
treatment
couch of the linac with the detector level at 100cm from the
source.
Sufficient backscatter is placing below the detector and build
up is placing
above the ImatriXX detector (figure1.10).
Figure1.10 ImatriXX 2-D array system- measurement set up
The TPS created verification plans will be executed in the
linac. The
measured and TPS calculated planar dose comparison can be
performed by
the IMRT QA software (figure1.11). The gamma evaluation can
be
-
16
performed and the % of pixels passing the specified gamma
criteria can be
obtained for every individual IMRT fields.
Figure1.11 ImatriXX 2-D array system – work flow
1.5. 6 Compass - DVH based verification system
Compass is a dose verification system of IBA and it is used
in
combination with MatriXX-Evolution detector (1020 pixels) for
pre-
treatment verification of conformal IMRT plans and with MatriXX
-
Evolution and gantry angle sensor for the verification of
rotational plans as
well as transmission detector (1600) pixels for online
verifications of
IMRT plans and rotational plans. Compass can determine the 3-D
dose
distribution in the patient anatomy, based on the measured beam
intensity
and it determines the fluence for all segments in a beam. As
this quantity
cannot be directly measured, Compass does first a calculation of
the
expected response of electrical signal for each segment based on
detector
pixel response, linac and detector models. After the
measurement, expected
-
17
and delivered responses are compared. The residual response is
then used
for computation of the really delivered fluence. The dose
computation in
Compass is a second independent step in which the resulting dose
to the
patient is determined based on a collapsed cone super position
algorithm.
For the commissioning of the Compass 3-D verification system
with
MatriXX-Evolution detector, the same data of TPS
commissioning
(profiles, depth dose curves, output factors, absolute dose
measurements)
are used. The primary quantity determined by Compass is the
fluence for
each segment. Discrepancies in delivery can be visualized as
difference in
the response patterns. The fluence determined in Compass is then
used as
input for the dose computation with the collapsed cone
algorithm. For the
conformal or IMRT plans, the Dicom RT plan, Dicom RT dose, Dicom
RT
structure and Dicom CT information etc are to be transferred to
the
Compass verification system. The Compass will compute using
collapsed
cone algorithm and compare the TPS calculated and compass
calculated
DVHs (dose volume histograms) and provide the differences.
1.6 Tolerance limits and Action levels for IMRT verification
Tests for IMRT verification can be separated into those for
verification of equipment for IMRT delivery, verification of
IMRT
treatment planning, and verification of patient-specific IMRT
techniques,
i.e., of the combined planning and delivery process of that
particular
patient treatment based on relative as well as absolute
dosimetry. Different
approaches exist for the comparison of sets of measured and
calculated
dose distributions [Mijenheer et al (2008)]. Each of these
approaches needs
well-defined criteria for acceptance of a plan and procedures if
these
criteria are not met. Tolerance and action levels can be used.
These
quantities can be defined in the following way: whenever a
parameter is
-
18
found in the range below the tolerance level, the equipment is
suitable for
high quality radiation therapy. If, however, a parameter exceeds
the action
level, it is essential that appropriate actions be taken as soon
as possible.
Consequently, tolerance levels are appropriate limits for
performance
specification and for acceptance testing procedures, while
action levels
might be regarded as more relevant values for use in ongoing
quality
control activities. If a parameter has a value between the
tolerance limit
and the action level, the responsible physicist will generally
decide to
continue with the treatment until a suitable moment for
further
investigation occurs. If such an investigation is not possible,
then high
quality treatments should no longer be performed with such
equipment.
Tolerance and action levels should now be defined for the
various tests to
compare measured with calculated dose distributions. The most
often
applied dose evaluation techniques comprise a direct comparison
of dose
differences (%dose difference), a comparison of distance to
agreement
(DTA) between measured and calculated dose distributions, and
a
combination of these two parameters: the gamma evaluation
method.
In the gamma evaluation, doses in the TPS calculated plan and
the
measured at the same pixel position are compared, and the
difference as a
percentage of the plan value is the percentage difference. In
high gradient
regions, one looks for the distance between a pixel in the plan
and a pixel
in the measured distribution, that have the same dose. This is
the distance
to agreement (DTA).
Differences of about 5% are generally significant for IMRT
verification [Mijenheer et al. (2008)]. Deviations larger than ±
5% should
therefore firstly result in a review of the complete dosimetric
procedure
taking into account the various factors influencing the
comparison result. If
no explanation for the observed discrepancy can be given,
the
-
19
measurement may be repeated. A possible recommendation might
then be
that a tolerance limit of ± 3% and an action level ± 5% should
be applied
for these types of point dose verifications. When the number of
comparison
points is large, simple methods of reporting deviations between
dose
measurements and calculations will collapse, and a method of
compiling
these deviations into a single number is required as a pass-fail
criteria.
Other methods have therefore been proposed, e.g., the use of the
quantity
“confidence limit” by Venselaar et al. (2001). The confidence
limit is
based on the average deviation between measurements and
calculations for
a number of data points in a comparable situation, and the
standard
deviation (SD) of the average of the differences. The confidence
limit is
then defined as the sum of the average deviation and 1.5 SD. The
factor 1.5
was based on experience and a useful choice in clinical
practice. A
multiplicative factor of 1.96 instead of 1.5 has later been
proposed by Palta
et al. (2003) for having 5% of the individual points exceeding
the tolerance
level. For both the verification of individual beams, as well as
for the
verification of patient-specific “hybrid” plans, Palta et al.
(2003) proposed
the set of values of confidence limits and action levels for
IMRT
treatments. An IMRT treatment plan should not be used clinically
if the
measured dose difference is more than the value given as the
action level,
which serves therefore as a pass-fail criterion. Application of
the gamma
evaluation method for selecting action levels is still in a
development stage.
Careful statistical analysis of patient specific verification
data might
reveal systematic uncertainties valid for the whole patient
group. The
statistical analysis of the results of a routine QA programme,
possibly
applied to a set of patients treated according to a class
solution, can be very
useful in defining appropriate tolerance/action levels taking
into account
the special aspects of IMRT relevant for a specific clinic.
Currently no
recommendations for 3-D dose evaluation are available and are
therefore
-
20
urgently needed. Biological considerations, combined with the
clinical
experience from the 3-DCRT era, may be required to develop
tolerance and
action levels for the evaluation of 3-D dose distributions for
an individual
patient.
If a gamma evaluation exceeds a certain action level for a
chosen
combination of dose-difference and DTA criteria, then possible
reasons for
discrepancies such as variation in phantom positioning and
linac
performance should first be investigated. If these
experimental
uncertainties are within accepted values, then it might be
useful to repeat
the experiment to confirm the observed discrepancies. If the
same areas of
the gamma maps fail the tolerance criteria again, then these
areas should be
compared with the corresponding regions in the patient dose
distribution,
and the implications of such a failure should be discussed with
the
responsible physicist and radiation oncologist. For each patient
a decision
should then be made if a new plan has to be generated or if the
differences
are clinically acceptable. It should be noted that such
patient-specific
action levels depend on many decisive factors, including the
position and
size of the area that failed to pass the evaluation criteria,
the dose level in
the PTV (planning target volume) or OAR (organ at risk), and
the
sensitivity of the plan for movement. Furthermore, gamma
evaluation is
currently mainly restricted to the dose delivered to the PTV,
whereas the
dose in an OAR is equally important. Extension of decision
protocols
including OAR is therefore urgently needed. The situation
becomes even
more complicated if dose distributions are evaluated in 3-D. It
should be
noted that tolerance limits and action levels have proven to be
very useful
in everyday quality control of accelerators, but some parameters
are not
easily and quickly corrected or repaired and some may almost
be
impossible or very expensive to restore. On very rare occasions,
it might
therefore be justified to use the radiation equipment
clinically, even if an
-
21
action level has been exceeded. The decision to clinically use a
treatment
unit, in spite of the fact that an action level has been
exceeded, has to be
discussed thoroughly and documented for every treatment
method.
1.7 Motivation for research and purpose of the thesis
Quality assurance in IMRT is mainly founded on quantitative
comparisons between computed and/or measured dose
distributions.
Differences between measurement and calculation are principally
caused
by errors in treatment planning, patient positioning, treatment
delivery and
radiation dose measurement technique. However a simple
agreement
between the two distributions cannot be held as a proof of
satisfying
quality. Indeed the distributions that are compared may contain
individual
uncertainties or bias such that the agreement seen is a chance
coincidence.
This consideration may serve as an argument to include many
degrees of
freedom in the QA measurement process, i.e. in terms of
measurement
points in the comparison, volume of detectors, resolution of
detectors, type
or complexity of plans, number of fields or arcs, movement of
carriage,
inclusion or exclusion of couch in the plan, mode of delivery
etc. The
proposed QA tolerance values found in some reports for these
parameters
should therefore be considered as general recommendations and
these may
not be always achievable in a clinical scenario.
Such guidelines for the IMRT QA are given in the American
Association of Physicists in Medicine- Task Group - 119 (AAPM-TG
119)
report [(Ezzell et al. (2009)] and in the European Society of
Radiotherapy
and Oncology (ESTRO) guidelines [(Mijenheer et al. 2008)]. But
a
comprehensive report that considers all possible influencing
parameters or
factors that affect QA results such as complexity of plans,
degree of
modulation, numbers of target volumes, numbers of fields or
arcs,
-
22
movement of MLC carriage, inclusion or exclusion of treatment
couch in
the plan, mode of delivery etc., is still to come. Because of
the nature of
complexity and the many steps involved, an optimized stringent
QA
protocol is essential to rule out all possible uncertainties and
errors. This
research work mainly aimed to study the influence of different
factors on
the optimization of patient specific QA in IMRT to adopt a
stringent QA
protocol.
1.8 Aims and objectives
The main objectives of this research work were as follows:
- To assess the beam stability of a Varian high energy medical
linear
accelerator; quantify MLC positional errors using ionometric
gravity test and dynalog file analysis.
- To establish the characteristics of the different QA systems
such as
aSi1000 based portal dosimetry and ImatriXX 2-D array
system.
- To study the angular response of the portal dosimetry and
ImatriXX
2-D array system.
- To optimize the patient specific QA measurements for IMRT
and
VMAT through the statistical analysis of the results.
- To examine the relationship and significance of different
parameters
such as detector systems, types of plans, their complexity,
number
of targets, movement of MLC carriage, number of fields or
arcs,
inclusion or exclusion of couch insert etc., on the selection of
pass-
fail criteria and action levels in patient specific QA.
- To examine whether the IMRT QA guidelines and published
reports
can be used for the VMAT QA analysis also or separate
optimization is needed or not.
- To validate the Compass 3-D verification system and to
optimize
patient specific QA for IMRT.
-
23
1.9 Hypothesis
Null Hypothesis (H0)
The null hypothesis was that the patient specific QA results are
not
influenced by the QA systems, type of plans, complexity of
plans, number
of fields or arcs, number of target volumes, movement of
carriage and
inclusion or exclusion of couch insert and there is no need for
institutional
local optimization of QA for IMRT and VMAT.
Alternate Hypothesis (H1)
The alternate hypothesis was that the patient specific QA
results are
influenced by the QA systems, type of plans, complexity of
plans, number
of fields or arcs, number of target volumes, movement of
carriage and
inclusion or exclusion of couch insert and institutional local
optimization
of QA for IMRT and VMAT is needed.