Embed Size (px)
Citation preview

Changing Phenotype in Floating-Harbor Syndrome
Joseph H. Hersh,1* Kathleen R. Groom,1 Frank F. Yen,1 and Gerald D. Verdi2
1Child Evaluation Center, Department of Pediatrics, University of Louisville, Louisville, Kentucky2Department of Surgery, University of Louisville, Louisville, Kentucky
We report on a girl with Floating-Harborsyndrome, trigonocephaly due to metopicsuture synostosis, preauricular pit, hypo-plastic thumb, subluxated radial head, andSprengel deformity. A review suggests thattrigonocephaly may be an important cranio-facial manifestation in this syndrome that isrecognizable in infancy. With time, this find-ing appears to become less noticeable, andthe face develops a triangular shape, accen-tuated by a broad and bulbous nose. Am. J.Med. Genet. 76:58–61, 1998.© 1998 Wiley-Liss, Inc.
KEY WORDS: Floating-Harbor syndrome;trigonocephaly; short stat-ure; delayed bone age; bul-b o u s n o s e ; h y p e r n a s a lspeech; speech delay; me-topic synotosis; pseudoar-throsis of clavicle; celiac dis-ease; mental retardation; fa-cial anomalies
INTRODUCTION
Pelletier and Feingold [1973] and Leisti et al. [1974]each described a male with short stature, characteris-tic facial appearance, and delayed speech development.This entity was named Floating-Harbor syndrome(FHS) after the two hospitals where these two caseswere originally identified, Boston Floating Hospitaland Harbor General Hospital in Torrance, CA. Sincethen, 18 additional cases have been published [Robin-son et al., 1988; Majewski and Lenard, 1991; Patton etal., 1991; Chudley and Moroz, 1991; Houlston et al.,1994; Lacombe et al., 1995]. We report on a girl withFHS, review several manifestations not previously ob-served in this disorder, and describe a changing facial
phenotype that may assist in early recognition of thisentity.
CLINICAL REPORT
A 12-year-old girl was born at term following a preg-nancy in which maternal hypertension was treatedwith bed rest in the last gestational month. The motherwas 24 years old and the father 25 years old. Both wereof normal stature, and he had insulin-dependent dia-betes mellitus; a brother had normal growth and de-velopment. There was no consanguinity and a mater-nal aunt had Down syndrome. After an uncomplicatedvaginal delivery, weight was 2,860 g and length 52 cm.At age 4 1/2 months (Fig. 1), she was evaluated becauseof craniofacial anomalies and developmental delay.Her length was 58 cm (<5th centile, 50th centile for 21/2 months); weight 5,050 g (5th centile); and occipito-frontal circumference (OFC) 37.7 cm (<5th centile, 50thcentile for 2 months). She had apparent trigono-cephaly. The inner canthi were laterally displaced, andthe bridge of the nose was not prominent. The right earwas mildly abnormal with a preauricular pit. Therewas no murmur. She had clinodactyly of the fifth fin-gers. Mild metatarsus adductus deformities werenoted. On neurological examination, there was muscu-lar hypotonia. Chromosome analysis was normal(46,XX). Metopic suture synostosis was identified ra-diographically and surgically repaired at age 8 months.
Left esotropia was treated with patching of the righteye and glasses. A growth hormone evaluation waspursued at age 4 years (Fig. 2), because of short statureand a bone age of 2 4/12 years, with normal results.Radiographically she had evidence of a hypoplastic dor-sally subluxated left radial head.
Psychological evaluation at 4 2/12 years demon-strated average intellectual abilities in nonverbal skillswith a measured IQ of 95, but there was evidence ofsignificant expressive language deficits. At age 6 years,a pharyngeal flap procedure was performed due to aresonance disorder characterized by hypernasality,phonological deficits, and oral motor dysfunction.Speech improved, although she remained mildly hyper-nasal. She was treated with Ritalin for attention deficithyperactivity disorder.
At 12 2/12 years she was reevaluated (Fig. 3). Speechand language therapy had been received since early
*Correspondence to: Joseph H. Hersh, M.D., Child EvaluationCenter, 571 South Floyd Street, Suite 100, Louisville, KY 40202-3828.
Received 26 February 1997; Accepted 9 June 1997
American Journal of Medical Genetics 76:58–61 (1998)
© 1998 Wiley-Liss, Inc.

childhood, and she was receiving special educationalservices. Communication skills had improved, but shestill had speech deficits and hypernasality. Her heightwas 133 cm (<5th centile, 50th centile for 9 years);weight 29.3 kg (<5th centile, 50th centile for 9 years);and OFC 48.1 cm (<5th centile, 50th centile for 2years). She had a narrow forehead and nasal bridgewith a prominent nose and wide columella. The earswere relatively large and posteriorally angulated andthe right ear was abnormally modeled. There was aright preauricular pit. The midface and mandible weresmall. Palpebral fissures were slightly downslantingand eyelashes were long. The philtrum was short andsimplified and the mouth was small with a thin upperlip. The palate was intact and she had a pharyngealflap. There was a normal complement of teeth withtooth gaps. The neck was short with a normal hairlineand no webbing. There was no murmur. The left thumb
was mildly hypoplastic, and there was a contracture ofthe right fifth finger at the proximal interphalangealjoint with mild fifth finger clinodactyly bilaterally.
Radiographically, there was evidence of pseudoar-throsis of the right clavicle, abnormal rotation of theright scapula, hypoplastic left radius with dislocationof the radial head, and hypoplastic first metacarpal ofthe left hand. Fluorescence in situ hybridization(FISH) of chromosome 22 at band q11.2, using theD22S75 DiGeorge chromosome region probe, demon-strated two hybridization signals without evidence of amicrodeletion. There was no evidence of increasedchromosomal breakage with the addition of diepoxybu-tane and mitomycin C.
DISCUSSIONFHS comprises short stature with delayed bone age,
characteristic facial appearance, most commonly rec-
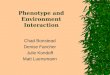
Fig. 2. Patient at 4 years. Thebridge of the nose is higher and thereis still evidence of mild trigono-cephaly.
Fig. 1. Patient at 4 1/2 months.Note the trigonocephaly and abnor-mally positioned and modeled rightear.
Floating-Harbor Syndrome 59

ognized in mid-childhood, and expressive language de-lay. Our patient represents the 21st report with thisdisorder (Table I). Structural abnormalities of majororgan systems are infrequent in FHS; however, celiacdisease [Robinson et al., 1988; Chudley and Moroz,1991] and genitourinary defects [Pelletier and Fein-gold, 1973; Leisti et al., 1974] have been described,each in two cases. Although neither problem was foundin our patient, she did have pseudoarthrosis of theclavicle, which has been reported in two other cases[Leisti et al., 1974; Patton et al., 1991].
Several additional clinical findings, previously notdescribed, were noted in our patient. These includedmetopic synostosis, subluxation of a hypoplastic radial
head, Sprengel deformity, preauricular pit, and hypo-plastic thumb. A duplicated thumb was reported in aprevious case [Patton et al., 1991]. Although theseanomalies have not been described in other affectedindividuals, we suspect that they may represent low-frequency associations in FHS.
In infancy, our patient had trigonocephaly, due tometopic suture synostosis. The face in FHS is describedas rounder with more prominent eyes in infancy [Pat-ton et al., 1991], and in childhood, is reported to have atriangular shape with deeper set eyes, a finding thathas been noted in eight cases [Leisti et al., 1974; Rob-inson et al., 1988; Patton et al., 1991; Chudley andMoroz, 1991; Houlston et al., 1994; Lacombe et al.,1995]. However, review of photographs from previouscase reports suggests to us that variable degrees oftrigonocephaly may be present in infancy, representinga more common early manifestation in this disorder[Pelletier and Finegold, 1973; Leisti et al., 1974; Rob-inson et al., 1988; Patton et al., 1991; Houlston et al.,1994]. Therefore, although the typical clinical findingsof FHS may not be as evident at a younger age, thepresence of trigonocephaly may represent a usefulearly diagnostic marker in this disorder. If it is lesssevere, trigonocephaly may actually spontaneously re-solve by mid-childhood, at a time when the facialchanges of FHS appear to be more easily recognizedand characterized by a triangular shape, and the typi-cal appearance of the nose dominates the facial pheno-type.
In general, cognitive abilities in affected patientshave ranged from normal intelligence to mild mentalretardation, with relative deficits in expressive lan-guage abilities. In our patient, intellectual abilitieswere in the average range, and she had evidence of anattention deficit hyperactivity disorder and a learningdisability. In addition to having expressive languagedelays, there was also severe hypernasality as the re-sult of velopharyngeal insufficiency requiring surgery.In addition to expressive language delays, a constantfinding in FHS, articulation deficits or nasal speechhas been reported in five previous cases [Pelletier andFeingold, 1973; Leisti et al., 1974; Patton et al., 1991;Houlston et al., 1994]. Thus, we suspect that in
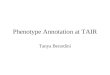
Fig. 3. Patient at 12 8/12 years.The face is now triangular in appear-ance. The nose has a ‘‘bulbous’’ shapewith a wide columella. Note thesmall midface, micrognathia, andcontinued evidence of an abnormalright ear.
TABLE I. Major Manifestations of FHS
Clinical findingsPrevious
casesPresent
case Total
Growth and developmenta. Low birth weight 8/17 − 9/17b. Low birth length 8/12 − 9/13c. Short stature 16/17 + 17/18d. Delayed bone age 16/16 + 17/17e. Delayed motor skills 4/17 − 4/18f. Speech delay 17/17 + 18/18g. Mild mental retardation 8/16 − 8/17
Craniofacial anomaliesa. Triangular face 8/16 + 9/17b. Deep-set eyes 13/16 − 13/17c. Long eyelashes 14/17 + 15/18d. Posteriorly angulated ears 10/16 + 11/17e. Bulbous nose 16/17 + 17/18f. Wide columella 16/17 + 17/18g. Short philtrum 14/17 + 15/18h. Thin lips 16/17 + 17/18i. Malocclusion 6/16 − 6/17
Other manifestationsa. Hirsutism 9/17 − 9/18b. Short neck 9/16 + 9/17c. 5th finger clinodactyly 13/17 + 14/18d. Brachydactyly 8/16 − 8/17e. Clubbed fingers 7/16 − 8/17f. Joint laxity 8/16 − 8/17g. Strabismus 2/17 + 3/18h. Celiac disease 3/17 − 3/18i. Genitourinary defect 3/18 − 3/19j. Pseudoarthrosis clavicle 2/18 + 3/19
60 Hersh et al.

patients with FHS, besides expressive language delays,a resonance disorder also represents a component ofthe developmental profile in this syndrome.
The phenotype of FHS resembles that seen in velo-cardio-facial syndrome (VCF) [Goldberg et al., 1993]. Infact, one of the cases reported with the former diagno-sis was challenged as representing the latter disorder[Lipson, 1991]. Similarities between the two conditionsextend beyond the facial appearance, with short stat-ure, cognitive deficits, speech delays, and hypernasal-ity being present in both syndromes. Therefore, FISHanalysis using a 22q11 probe, which demonstrates amicrodeletion in most instances of VCF [Lindsay et al.,1995], routinely should be performed in a patient witha clinical diagnosis of FHS. In the case of our patient, amicrodeletion of 22q11 was not demonstrated.
Although clinical variability in FHS exists, findingsin our patient may broaden the phenotype and lead toearlier recognition of this multiple organ system disor-der. Establishing a diagnosis primarily impacts onidentification of fairly typical growth and developmen-tal patterns in this disorder. Therefore, FHS repre-sents another example in which early recognition isimportant in providing developmental programs tomaximize an affected child’s prognosis.
ACKNOWLEDGMENTS
The authors are grateful to Jeanie Young for her sec-retarial assistance.
REFERENCES
Chudley AE, Moroz SP (1991): Floating-Harbor syndrome and celiac dis-ease. Am J Med Genet 38:562–564.
Goldberg R, Motzkin B, Marion R, Scambler PJ, Shprintzen RJ (1993):Velo-cardio-facial syndrome: A review of 120 patients. Am J Med Genet46:313–319.
Houlston RS, Collins AL, Dennis NR, Temple IK (1994): Further observa-tion on the Floating-Harbor syndrome. Clin Dysmorphol 3:143–149.
Lacombe D, Patton MA, Elleau C, Battin J (1995): Floating-Harbor syn-drome: Description of a further patient, review of the literature, andsuggestion of autosomal dominant inheritance. Eur J Pediatr 154:658–661.
Leisti J, Hollister DW, Rimoin DL (1974): Case report 2. In Bergsma D (ed):‘‘Syndrome Identification.’’ White Plains, NY: National Foundation—March of Dimes 2(1):305.
Lindsay EA, Goldberg R, Jurecic V, Morrow B, Carlson C, KucherlapatiRS, Shprintzen RJ, Baldini A (1995): Velo-cardio-facial syndrome: Fre-quency and extent of 22q11 deletions. Am J Med Genet 57:514–522.
Lipson A (1991): Letter to the editor: Floating-Harbor and the good shipShprintzen. J Med Genet 28:807–808.
Majewski F, Lenard H-G (1991): The Floating-Harbor syndrome. Eur JPediatr 150:250–252.
Patton MA, Hurst J, Donnai D, McKeown CME, Cole T, Goodship J (1991):Syndrome of the month: Floating-Harbor syndrome. J Med Genet 28:201–204.
Pelletier G, Feingold M (1973): Case report 1. In Bergsma D (ed): ‘‘Syn-drome Identification.’’ White Plains, NY: National Foundation—Marchof Dimes 1(1):8–9.
Robinson PL, Shohat M, Winter RM, Conte WJ, Gordon-Nesbitt D, Fein-gold M, Laron Z, Rimoin DL (1988): A unique association of short stat-ure, dysmorphic features, and speech impairment (Floating-Harborsyndrome). J Pediatr 113:703–706.
Floating-Harbor Syndrome 61