Embed Size (px)
Citation preview

Changing Paradigms in Aortic Dissection
Ali Azizzadeh, MD, FACS
Director, Vascular Surgery
Vice Chair, Department of SurgeryAssociate Director, Heart Institute
Cedars-Sinai Medical CenterLos Angeles, CA
Controversies & Advances inthe Treatment ofCardiovascular Disease
11/16/18

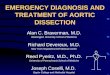
Classifications of Dissection:Stanford and DeBakey

Epidemiology
10-15 cases/100,000adults/year
2/3 type A
1/3 type B
Acute Type B Acute Type B
30% Cx
70% UnCx
Male: Female 2-5:1

Paradigm Shift

Management of Type B Aortic Dissection
OR / TEV AROR / TEV ARCX
TYPE BTYPE B
OMTOMTUNCX
TYPE BTYPE B
+ TEV AR+ TEV AR

TYPE B Aortic Dissection
R ecom m endationsforT EVA R Class L evel
A cuteT ypeB Dissection
Ischem ia I A
S T S ExpertConsensusDocum ent2008T reatm entofDescendingT horacicA orticDisease
10585286 DOC
S venssonL G,etal.Ann Thorac Surg, 2008;85:S 1-41
Ischem ia I A
N oIschem ia IIb C
ClassIIb:usefulness/efficacy islessw ellestablished by evidence

TYPE B Aortic Dissection
R ecom m endations Class L evel
Inuncom plicated T ypeB AD,m edicaltherapy shouldalw aysberecom m ended.
I C
ES C Guidelines2014R ecom m endedT reatm entofA orticDissection
10585286 DOC
Inuncom plicatedT ypeB A D,T EVAR shouldbeconsidered. IIa B
Incom plicatedT ypeB A D,T EVAR isrecom m ended. I C
Incom plicatedT ypeB AD,surgery m ay beconsidered. IIb C
ClassIIa:w eightofevidenceisinfavorofusefulness/efficacy
ErbelR ,etal.Eur Heart J.2014 N ov1;35(41):2873-926.

Treatment of ATBAD
3° Referral Center
Multi-specialtyteam: CT, Vasc Surg
Critical care
Consultants
Advanced imaging: Advanced imaging: CT, MR, IVUS, TEE
Hybrid OR’s
Monitoring MEP,SSEP
Full spectrum ofopen/endovascularprocedures

Admit CVICUCVC, arterial line, UOP
Admit CVICUCVC, arterial line, UOP
Anti-impulse TherapySBP<120, HR<60
Anti-impulse TherapySBP<120, HR<60
B-Blocker
Ca+2 Blocker
B-Blocker
Ca+2 BlockerRespiratory
DVT prevent
Respiratory
DVT prevent
Protocol
SBP<120, HR<60Control pain
SBP<120, HR<60Control pain
Ca+2 Blocker
Nitroglycerin
Nitroprusside
Ca+2 Blocker
Nitroglycerin
Nitroprusside
DVT prevent
Nutrition
Mobilization
DVT prevent
Nutrition
Mobilization
Reassessment
Blood pressure
Pain
Reassessment
Blood pressure
Pain

Percutaneous InterventionSurgical Intervention
Percutaneous InterventionSurgical Intervention
Protocol
Rupture/ LeakMalperfusion (renal, visceral, peripheral)
Acute ExpansionRefractory Symptoms
Rupture/ LeakMalperfusion (renal, visceral, peripheral)
Acute ExpansionRefractory Symptoms

UT Houston Series
2000 to 2014
1079 pts AD
532 ATBAD
60% Male
Mean age 60.6 ± 13.6 yrs
Median age = 60.5 yrs
Range 16 –98 yrs
Average Follow up: 3.7 yrs

Aortic Dissection
1079 DISSECTIONS

Aortic Dissection
535 532
1079 DISSECTIONS
535TYPE A
532TYPE B

Aortic Dissection
535
294UNCOMPLICATED
1079 DISSECTIONS
535TYPE A
238COMPLICATED

Complicated ATBAD
Rupture
Malperfusion: Neurologic
Spinal Cord Spinal Cord
Visceral (Celiac, SMA)
Renal
Lower Limb
Refractory Pain & HTN

• In-hospitalm ortality significantlyhigherw ithm edicalm anagem ent
• 2/3rd m edicalrx deathsduetorupture
• R efractory pain/HT N independent
refractory pain/HTN
Refractory Pain and HTN
• R efractory pain/HT N independentpredictorofin-hospitalm ortality
• Interventionassociatedw ithim provedoutcom esoverm edicalm anagem entforrefractorypain/HT N
Medical Management: In-hospital mortality
No pain/HTN
Circulation2010;122:1283-9

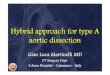
Types of Malperfusion
DynamicObstruction:• Prolapsed septum
into ostium duringcardiac cyclecardiac cycle
Static Obstruction: Dissection extends
into branch vessel

Dynamic Obstruction

Static Obstruction
Selective angiogram
Measure pull backpressures
Adjunctive stenting
Extend stent into TL
Williams DM, Patel HJ. Endovascular Therapy for Malperfusion in Acute Type B AorticDissection. Operative Techniques in Thoracic and Cardiovascular Surgery. p 2-11. 2009
Extend stent into TL

Static Obstruction: SMADissection

Static Obstruction: Left RenalArtery Dissection

Goals of TEVAR for cATBAD
Seal off proximal entry tear
Alleviate malperfusion
Expand compressed truelumenlumen
Induce false lumenthrombosis
Prevent/treat rupture

TEVAR DON’TS
Oversize >10%
Balloon Angioplasty
Place distal device first

IVUS Adjunct to CTA,
angiogram andTEE
Wire placementin true lumen
Assesses Assessesadequacy oftreatment
Guide additionaltherapy
Diagnosecomplications

True Lumen Compression

IVUS after TEVAR

Aortic Remodeling

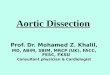
Mortality by Management Strategy
Total = 444Uncomplicated
N=271
C o m p l i c a t e d ( N = 1 7 3 )OR,
p-valueMedN=69
OpenN=52
TEVARN=37
Other CVN=15
Mortality5
1.9%13
18.8%6
11.5%5
13.5%3
20%* 8.8, 0.0001
* Uncomplicated compared to complicated type b aortic dissection

Survival at 5 yrs foruATBAD was 76.6%


Overall Survival: Max Aortic Diameter

uATBAD High Risk Criteria
Aortic diam e te r>44m m is a predictorof mortality after adjustment forsignificant risk factors.
Decreased intervention-free survivalin those with FL>22m m and/or m axin those with FL>22m m and/or m axaortic diam e te r>44m m onadmission.
Age >60 y e arsis a risk factor formortality.

Incidence of Risk Factors in AUTBAD
Risk Factors
TAD >44mm / FLD >22 / Age >60
1 Risk Factor 44%
2 Risk Factors 19%
3 Risk Factors 6%
Total 69%

The Fate of the 31%:uTBAD & no high-risk criteria
OMT 5% mortality / year
10% intervention / year
OMT + TEV AR 5-10% procedural morbidity and
mortality
Aortic stabilization

INSTEAD XL: 5 Year Analysis

INSTEAD XL: 5 Year Extended Follow-up
Clin
icalEvide
nce
O M T +T EVAR :N om id-orlate-term Aortic
O M T O nly:S ignificantm id-andlate-term term Aortic
m ortalityandlate-termm ortality


Complicated ATBAD
75 yo female with chestand back pain
CTA: ATBAD with aortoiliacthrombosis
On exam, mottled from the On exam, mottled from theumbilicus down
No motor or sensation inthe lower extremities

CTA

3D reconstruction

OR
Open right femoralaccess (no pulse)
Diagnostic angiogram
Glide catheter/ glidewire access toascending aortaascending aorta
IVUS confirmedplacement of the wirein the true lumen fromRCFA to ascendingaorta


Planned LSCA coverage

Abdominal Aortogram


Management RLE ischemia
Remove sheath
Open repair of RCFAarteriotomy
RLE angiogram?
Explore abdomen? Explore abdomen?
RLE fasciotomy?

Completion angiogram after open repair RCFA/SFA

HPI
P M H: Ascendingaorticaneurysm com plicatedby acutetypeA aorticdissection,P araparesis,N eurogenicbladder,Intracranialhem orrhage,T IA w ithsym ptom sofaphasia,Chronicleftfrontallobeinfarct,Chronicm icrovascularchanges,Hypertension,Hyperlipidem ia.
P S H: AscendingAortaR eplacem ent,Appendectom y,T onsillectom y.
• 72 y/om alereferredforsurgicalevaluationof6.8cm DT AA.
M edications: Glycolax,Florinef,Zetia,Ecotrin,Bystolic,P epcid,L asix,M ulti-vitam ins,M icro-K,Vitam inC,N eurontin,N orco,Caltrate,P lavix.
Allergies: N KA
FH: Father:history ofCAD,M aternalgrandfather:diedat43
S H: S m okingstatus:never,Alcohol:rarely

Consult: 07/05/2018
Surgical evaluation: enlarging 6.8cm DTAA
Vitals
P hysicalExam
General: Aw ake,Alert,O riented
HEEN T : N orm ocephalic,atraum atic,scleraeareanictericBP : 123/70
P ulse: 75
R R : 18
T em p: 97.4
HEEN T : N orm ocephalic,atraum atic,scleraeareanicteric
N eck: S upple,nom asses
L ungs: Cleartoauscultation
Cardiac: R R R ,norub,m urm urorgallop
Abdom en: S oft,nondistended,nontender,bow elsoundspresent
Incisions: W ell-healedm ediansternotom y andrightinfraclavicularincision.S ternum stable.

CTA

Problem list
Ascending aortic pseudoaneurysm
Residual arch and type B dissection
6.8 cm DTAA
CAD
Cerebrovascular disease Cerebrovascular disease
Solution?

Procedure 7/30/18
Repair of ascending aorta pseudoaneurysm and hemiarchreplacement
Ascending aorta to innominate artery bypass
CABG
DHCA with RCP DHCA with RCP

CTA

CTA
Video

CTA
Video

CTA
Video

CTA
Video

CTA
Video

CTA
Video

Residual 7 cm DTAA: Solution?

Arch Debranching
RCCA to LCCA to LSCAbypass
LSCA dissection with flow tofalse lumenfalse lumen

TEVAR: Zone 0
RAO
Markers for origin of aorto-innominate bypass

Procedure: TEVAR
Device #1: covered theorigin of the innominate, leftcarotid and left subclavianarteries (zone 0).
Device #2: overlap tocover zones 2 and 3.
Device #3: deployedabove the celiac artery.

Completion Angiogram
Successful exclusion of theextensive aortic aneurysmwith coverage of the nativewith coverage of the nativeinnominate, left commoncarotid and left subclavianarteries.

Type 2 endoleak: LSCA origin with dissection
Management?
Amplatzer plug 14mm

14mm Amplatzer Plug

Hospital course
Patient tolerated the procedure well.
Oriented, sensory and motor function intact, noneurological issues.neurological issues.
Lumbar drain removed: 09/23/2018
Discharge from hospital: 9/26/18

Conclusion
Paradigm shift in therapy for TBAD
All CTBAD should undergo TEVAR as first linetherapy
UTBAD patients with high risk criteria (2/3 of thecohort): TAD >44, FLD>22, Age >60 arecohort): TAD >44, FLD>22, Age >60 arecandidates for OMT+TEVAR
UTBAD patients with no high risk criteria (1/3 ofthe cohort): should be counseled about therisk/benefits of OMT vs. OMT+TEVAR

Thank You