Embed Size (px)
Citation preview

Changes of the speaking and singingvoice after thyroid or parathyroidsurgeryThomas J. Musholt, MD, Petra B. Musholt, MD, Jens Garm, Ulrike Napiontek, MD, andAnnerose Keilmann, MD, Mainz, Germany
Background. While permanent dysphonia is a rare complication of thyroid or parathyroid surgery,postoperative changes of the speaking and/or singing voice often remain unrecognized.Methods. In a prospective 4-arm study, vocal fold videolaryngostroboscopy and functional assessmentof pre- and postoperative vocal performance was used to evaluate voice disturbances in 120 patientsundergoing extended cervical surgery and in 19 patients with limited interventions for thyroid and/orparathyroid pathology.Results. Impairments, especially of the singing voice, were predominantly observed after extendedendocrine neck surgery. In women, the highest pitch of the singing voice (HPS) dropped from 651 Hzto 563 Hz (E5 to Csharp5, P � .001). In men, the HPS decreased to a lesser extent (423 Hz to 374Hz, (Gsharp4 to Fsharp4, P � .009). Covariant analysis of influencing factors revealed thepreoperative maximum frequency range and the HPS as predictors of the postoperative voice outcome.Conclusions. While alterations of the speaking voice after thyroid and parathyroid surgery usuallyremain subclinical, transient changes of the singing voice will matter to voice professionals.(Surgery 2006;140:978-89.)
From the Departments of Endocrine Surgery, Endocrinology, and Communication Disorders, Gutenberg University
Medical SchoolInjury to or accidental discontinuation ofthe recurrent laryngeal nerve (RLN) with subse-quent vocal cord paralysis represents the mostprominent complication in thyroid and parathy-roid surgery—especially in reoperations1,2—withpotentially serious implications for the patient’squality of life. In the recent past, the externalbranch of the superior laryngeal nerve has beenrecognized as an additional important neural struc-ture at risk,3,4 especially in patients professionallyusing their (singing) voice. However, the patho-physiology of postoperative dysphonia developingdespite normal respiratory vocal fold mobility andin the absence of intraoperative neural injuries isnot well understood. Multiple causes have been
Presented at the 27th Annual Meeting of the American Associ-ation of Endocrine Surgeons, New York, New York, May, 2006.
Reprint requests: Professor Thomas J. Musholt, MD, EndocrineSurgery, Dept of General and Abdominal Surgery, GutenbergUniversity Medical School, Langenbeckstr. 55101 Mainz, Ger-many. E-mail: [email protected].
0039-6060/$ - see front matter
© 2006 Mosby, Inc. All rights reserved.
doi:10.1016/j.surg.2006.07.041
978 SURGERY
hypothesized leading to objective postoperativevoice impairment such as discrete swelling oredema of the neural structures innervating themuscles necessary for phonation; division, intraop-erative fixation, or injury to the external laryngealmuscles and prelaryngeal strap muscles (sternohy-oid, sternothyroid) or development of adhesions tothese muscles5; and trauma attributed to endotra-cheal intubation (dislocation of the arytenoid car-tilage or compression of the anterior branch of theRLN in its intralaryngeal course).
Post-(para)thyroidectomy dysphonia may clinicallyimpose as hoarseness, voice fatigue, or voice weaknessbut may also present as a subclinical alteration that isobserved by comparison of pre- and postoperativefunctional voice assessment only. On the other hand,postoperative complaints or discomforts may be re-ported by a number of patients without objectivevoice changes. The incidence of voice impairmentsdirectly after thyroid surgery has been reported in41% to 84% of patients.3,5-14 Although voice changesin patients who underwent thyroid or parathyroidresections are mostly subclinical and transient, assess-ment of the pre- and postoperative vocal perfor-mance is recommended not only for medicolegal
aspects in patients with preoperative vocal cord le-
yperpa
Surgery Musholt et al 979Volume 140, Number 6
sions15 but for identification of individuals needingpostoperative voice rehabilitation to prevent perma-nent voice impairments.
We conducted a prospective 4-arm study of 139patients undergoing either limited or extended en-docrine cervical surgery for thyroid and/or para-thyroid pathology and evaluated pre- andpostoperative differences in vocal fold videolaryn-gostroboscopy and in objective vocal performance(speaking and singing voice).
MATERIAL AND METHODSPatients. Our prospective study included 139
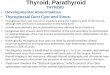
consecutive patients undergoing thyroid and/orparathyroid resections by a single endocrine sur-geon (T.J.M.) between April 2004 and December2005. Of these, 102 patients suffered from benignor malignant thyroid disease and 37 patients fromprimary (19) or secondary (18) hyperparathyroid-ism (HPT) (Table I). Nine patients had undergoneprevious neck surgery; 105 of 139 patients under-went thyroid resections, whereby 59 surgical proce-dures included parathyroidectomies (27), lymphnode dissections (11), or both (21). Isolated para-thyroid resection was performed in 30 of 139 pa-tients, and isolated lymph node dissection in 3 of139 cases (reoperations for thyroid carcinoma).One patient underwent systematic central and uni-lateral lymphadenectomy with resection of theright upper parathyroid gland for metastasizingfollicular thyroid carcinoma (Fig 1, Table II).
Although pre- and postoperative direct visualiza-tion of the vocal folds—by means of a rigid tele-scope performed by 1 of 3 ear, nose, and throatspecialists—is a routine procedure in our endo-crine surgery clinic, informed consent for the voiceassessments was obtained. Individuals with preop-erative vocal cord paralysis, speech disorders, my-asthenia gravis, and so forth, were considered
Table I. Indications leading to cervical surgery in
Extended cervical surger
Men(n � 40)
Wo(n �
pHPT 3sHPT 9MNG � HPT 1MNG 15 4Grave’s disease 3Thyroid carcinoma 9 1Total 40 8
HPT, Hyperparathyroidism; MNG, Multinodular goiter; pHPT, primary h
ineligible to our study. Two patients with signs of
postoperative unilateral vocal fold paralysis (no oronly minor respiratory mobility of the vocal corddespite of normal neuromonitoring of the RLN)were excluded from the statistical analysis.
The 139 patients studied were categorized ac-cording to extent of surgery and to gender into 4study arms (Tables I-IV). The extent of surgery wasdefined as follows: patients who underwent surgicalprocedures with moderate to high risk for a RLNinjury for predominant thyroid pathology (thyroid-ectomy; lobectomy; near-total thyroid resections;central lymph node dissections; reoperations in thecentral cervical compartment) or for predominantparathyroid pathology (parathyroidectomy for sec-ondary HPT, including 3 cases of additional thy-roid enucleations or subtotal unilateral resection).This group incorporates 7 thyroidectomies or com-
escribed patient cohort
Limited cervical surgery
TotalMen
(n � 9)Women
(n � 10)
6 7 190 0 182 1 101 2 630 0 90 0 209 10 139
rathyroidism; sHPT, secondary hyperparathyroidism.
3
1
11
46
2730
21
lymph node dissections
thyroidresections
parathyroid resections
Fig 1. The diagram depicts the overlap of thyroid andparathyroid surgical procedures as well as lymph noderesections in the patient cohort.
the d
y
men80)
3965610
pletion thyroidectomies with lymph node dissec-

980 Musholt et al SurgeryDecember 2006
tions for medullary thyroid carcinoma (MTC).Surgery with low risk to the RLN was defined asfollows: minimally invasive or open parathyroidec-tomy for primary HPT (thereof 8 cases with addi-tional minor thyroid resections) and enucleationsof thyroid nodules alone. Overlap of surgical pro-cedures performed (thyroid and parathyroid resec-tions, lymph node dissections) is demonstrated inFigure 1.
Surgery. Routine identification of the RLN wasperformed during all interventions classified asextended cervical surgery. The surgical proce-dure for lobectomy and thyroidectomy includedunilateral or bilateral exposure of the recurrentlaryngeal nerve(s) throughout the entire lengthin the tracheo-esophageal groove, starting frombelow the crossing of the nerve with the inferiorthyroid artery up to the cricothyroid muscle.
Table II. Surgical procedures, extent of cervical su
Extended cerv
Men(n � 40)
Thyroid resectionEnucleation 1Subtotal unilateral 0Lobectomy 8Bilateral subtotal 0Dunhill procedure 4Thyroidectomy 17Bilateral completionThyroidectomy 3No thyroid surgery 7
LymphadenectomyCentral 9Re-op central 4Lateral 1No lymphadenectomy 26
ParathyroidectomyUnilateral 7Bilateral 19Re-op 1No parathyroidectomy 13
Muscle divisionWithout division 33Sternohyoid and sternothyroid 5SCM 2
Tobacco useNonsmoker 18Former smoker 3�20 cig/d 10�20 cig/d 5Missing information 4
Cig, Cigarettes; re-op, reoperation; SCM, sternocleidomastoid muscle.
With the aid of magnification glasses, the paratra-
cheal tissue was dissected and the “dorsal limitinglamella” opened, especially if electromyographicnerve monitoring was utilized. The RLNs werevisually identified and preserved (but not skele-tonized!) and followed upward to the point ofentry into the subglottis behind the cricothyroidjoint. The superior thyroid vessels were carefullyfreed and ligated very close to the thyroid cap-sule, while care was taken not to damage theexternal branch of the superior laryngeal nerve.Routine positive identification of this neuralstructure was avoided. Meticulous hemostasis wasaccomplished with bipolar forceps, ligation ofsuperior thyroid vessels, and closure of small ves-sels with tiny titan clips—particularly in the areaof the ligament of Berry and in close proximity tothe RLN. Transverse division of 1 or several cer-vical muscles (sternothyroid, sternohyoid, omo-
, and smoking history
rgery Limited cervical surgery
Totalomen� 80)
Men(n � 9)
Women(n � 10)
1 1 2 51 2 1 4
19 0 0 270 2 0 2
13 0 0 1726 0 0 43
4 0 0 716 4 7 34
15 1 0 254 0 0 82 0 0 3
59 8 10 103
14 8 8 3722 0 0 410 0 0 1
44 1 2 60
71 9 10 1236 0 0 113 0 0 5
47 4 6 756 0 0 99 2 2 236 2 0 13
12 1 2 19
rgery
ical su
W(n
hyoid, sternocleidomastoid) was performed in

ging vo
Surgery Musholt et al 981Volume 140, Number 6
thyroid and parathyroid reoperations and incases of lateral lymph node dissections for thy-roid carcinoma.
Monitoring of the vagal nerve and RLN wasroutinely performed during extended surgery butnot used in every case because of system malfunc-tion. Suction drains were regularly placed and usu-ally removed at the first (rarely second)postoperative day. Diclofenac medication was rou-tinely administered for pain relief and anti-inflam-matory effects.
Assessment of vocal fold mobility and vocalperformance. The pre- and postoperative respira-tory vocal fold mobility was assessed by indirectvideolaryngostroboscopy (Figs 2A and 3). In addi-
Table III. Results of univariate analyses of selectedpaired samples
ExtMen (n � 40)
Preop Postop
PMean SD Mean SD
LPS 86.2 15.7 80.1 16.8HPS 423.4 143.5 374.0 153.4MFRS 337.2 143.8 294.0 151.7FFSp 132.2 29.0 123.7 22.5
LimMen (n � 9)
LPS 74.8 9.1 72.4 10.0HPS 420.0 134.5 420.9 192.5MFRS 345.2 132.0 348.4 187.7FFSp 123.3 23.2 125.1 38.6
FFSp: Mean, fundamental frequency of the speaking voice; HPS: mean, hMFRS: mean, maximum frequency range of the singing voice; postop, po*While no significant differences were observed after limited surgery, bosinging voice and the maximum phonational frequency range of the sin
Table IV. Prevalence of relative alteration of the hrange (MFRS) of the singing voice
Extended cervical surgery
Men (n � 40) Women (n � 80
HPS��0.5 0 2�0.5 to 0 13 320 to 0.5 25 45�0.5 2 1MFRS��0.5 2 4�0.5 to 0 10 260 to 0.5 23 44�0.5 5 6
tion, the maximum frequency range (in Hz) and
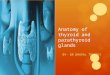
dynamic frequency range (in dB) were evaluated.These data were generated by digital tape record-ing of the patient’s voice with a high-fidelity micro-phone that was placed in a defined distance fromthe individual’s mouth under standardized condi-tions (Phonomat Spektra, Homoth, Hamburg, Ger-many)(Fig 2B). This machine records thefundamental frequency (Fo) of vibrations of thevocal folds in real-time by extracting cycle-to-cyclechanges with an accuracy of 1 Hz, and provides anobjective evaluation of pitch and voice quality thatis reliable and reproducible. The resulting data aredisplayed in a 2-dimensional plot (frequency [Hz]and loudness [dB]) representing a voice range pro-file or phonetogram (Fig 4). Each patient was en-
titative parameters using the Student t test for
cervical surgeryWomen (n � 80)
Preop Postop
P valueMean SD Mean SD
133.5 21.3 135.2 27.9 .524651.1 206.8 563.3 193.7 .000517.6 204.0 428.1 189.0 .000220.2 35.7 212.7 34.9 .44
rvical surgery*Women (n � 10)
138.4 14.2 135.5 19.0 .545643.5 242.2 646.0 229.9 .971505.1 242.8 510.5 231.2 .939226.3 17.3 225.7 25.7 .942
pitch of the singing voice; LPS: mean, lowest pitch of the singing voice;ive; preop, preoperative.and women displayed significant differences of the highest pitch of the
ice. Mean values and SD (standard deviation) are given in hertz (Hz).
t pitch (HPS) and of the maximum frequency
Limited cervical surgery
TotalMen (n � 9) Women (n � 10)
1 1 42 6 536 2 780 1 4
1 1 82 4 426 4 770 1 12
quan
ended
value
.001
.009
.019
.092ited ce
.529
.979
.921
.843
igheststoperatth men
ighes
)
couraged to maximum voice performance by a

of vid
982 Musholt et al SurgeryDecember 2006
professional instructor. The range of speaking Fo,the range of singing Fo, and the range of intensityof the speaking voice were evaluated. The usualspeaking Fo was defined as the frequency that was
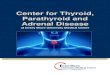
Fig 2. A) Indirect videolaryngostroboscopy enables thefold abduction and vibration (phonatoric mobility). B)fidelity microphone fixed to a headpiece which maintaiphonetogram of the singing and speaking voice. Each pathe test.
Fig 3. Freeze images of preoperative (upper row) and powho underwent a left-sided lobectomy. The images demonof the vocal cleft (the left vocal fold is on the right sidewith the preoperative situation can be observed whilesymmetrically (2nd images), but the left vocal cord premaabducted (3rd images), resulting in a discrete asymmetrythe vocal fold mobility can be detected only with the aid
used most often during speaking. The upper and
lower limits of the singing voice were defined as thelowest and highest recorded frequencies while sing-ing the scale. The range of the singing voice wascalculated as difference between the upper and
stration of the symmetry and discrete mobility of vocalal tape recording of the patient’s voice—using a high-efined mouth-to-microphone distance—to generate theas strongly motivated by a professional instructor during
rative (lower row) videolaryngostroboscopies of a patientin a sequence from left to right the opening and closureimage). After left lobectomy, no differences compared
cal folds are closed (left images). The vocal folds openswings back while the right vocal cord is still completelythe closing phase (4th images). These minor changes ofeostroboscopy and high-speed recording.
demonDigit
ns a dtient w
stopestrate
of thethe voturelyduring
lower limits of the recorded singing voice. The

Surgery Musholt et al 983Volume 140, Number 6
maximal and minimal loudness of the singing voicewas determined as well.
Moreover, the maximum duration holding a sin-gle tone (maximum phonation time) was assessedas a measure of the ability to regulate ventilatoryand laryngeal systems for voice production inde-pendent of a frequency or intensity target. Apartfrom these objective quantitative data, we classifiedthe quality of the voice with the attributes hoarse-ness, roughness, and breathiness that were subjec-tively assessed as semi-quantitative parameters.Preoperative videolaryngostroboscopy and evalua-tion of the vocal performance was done 1 to 28 daysbefore thyroid or parathyroid surgery. The postop-erative evaluation was performed up to 3 times atintervals of 2 to 15 days (mean, 3.9), 7 to 122 days(mean, 38.2), and 37 to 412 days (mean, 129.5)after cervical surgery. Limits of staff and clinicalresources forced us to perform repeated postoper-ative examinations only in cases with pathologicfindings at first visit after surgery. Although in-
Patient A
Patient B
pre-op
pre-op
frequency [Hz] 65 131 523
[dBC]
50
110
50
110
Fig 4. Two examples of preoperative and early postopera 2-dimensional plot. While the phonetograms in the usinging voice (dotted line) after thyroidectomy, the examplfrequency range of the speaking voice (continuous line) ais given in decibel C(dBC).
tended at the beginning of the study, standardized
schedules of the second and third postoperativeclinical examination could not be realized becauseof the patients’ personal schedules.
Statistical analysis. Statistical analysis was per-formed with the statistical software package SPSS,version 12.0 (SPSS Inc., Chicago, Ill) and SAS,version 9.1 (SAS Institute, Cary, NC). Analyses formen and women were performed separately be-cause the average speaking and singing voice ofmen is 1 octave lower than the voice of women. Pre-and postoperative differences of the vocal cordmobility were evaluated by the Student t test forpaired samples. In addition, analysis of covarianceusing the SAS procedure GLM was performed toassess the possible influence of different parame-ters (gender, extent of surgery, highest pitch of thesinging voice, maximum frequency range, trans-verse division of cervical muscles, smoking) on thepostoperative vocal performance. To investigatethe dependence of quantitative variables, linearregression models were used. The primary hypoth-
post-op
post-op
65 131 523
aximum phonational frequency ranges represented inw demonstrate a loss of the highest frequencies of the
n in the lower row demonstrates an unaltered phonationalging voice post-thyroidectomy. The sound pressure level
ative mpper roe givend sin
eses were detectable differences of the pre- and

scape
984 Musholt et al SurgeryDecember 2006
postoperative frequency range of the speaking andsinging voice (ie, 4 tests were performed). Multipletesting was taken into account by using the Bonfer-roni-Holm procedure. All other P values are de-scriptive and have been computed in exploratoryanalyses.
RESULTSEarly postoperative changes of the mean funda-
mental frequency of the speaking voice were ob-served in women (mean, 220 Hz [A3] to 212 Hz[Gsharp3]) and men (mean, 132 Hz [C3] to 123Hz [H2]) after extended cervical surgery (TableIII). However, the differences were not statisticallysignificant.
The singing voice, on the other hand, was almostundisturbed after limited cervical interventions,but was significantly altered in both genders afterextended surgery. In women, the mean highestpitch dropped from mean 651 Hz to 563 Hz (E5 toCsharp5, P � .001) accompanied by marked reduc-tion of the maximal sound pressure level (95.7 to92.1 dB, P � .001). In male patients, the meanhighest pitch of the singing voice decreased as well,but to a lesser extent (mean 423 Hz to 374 Hz,Gsharp4 to Fsharp4, P � .009) compared withwomen. As a result of the reduction of the highestpitch of the singing voice in both genders, therange of the singing voice was congruently re-duced. Significant differences of the lowest pitch ofthe singing voice were observed in only the groupof men who underwent extended surgery. Calcula-
-30 -20 -10 0 10 20 300
5
10
15
20
25
30
-300 -200 -100 0 100 200 30
5
10
15
20
25
30
LPS HPS Differences in men
Fig 5. Histograms depicting the prevalence of differencelowest pitch of the singing voice after extended cervical sto 50 Hz (for women) and 30 Hz (for men) of the lowobserved for the highest pitch of the singing voice, whicHz for men. Negative differences actually demonstrate athat patients learned the test procedures and lost their e
tion of the differences of the pre- and postoperative
highest and lowest pitch of the singing voice re-vealed that the frequencies were not always loweredpostoperatively, but also showed improvements (ie,negative values) in a number of patients (Fig 5).
Analyses of covariance and linear regressionmodels were used to explore possible influencingfactors on the postoperative vocal performance.Gender, extent of surgery, intraoperative divisionof cervical muscles, and tobacco use were consid-ered most important. However, analysis of covari-ance revealed that only the preoperative highestpitch of the singing voice remained of prognosticsignificance (P � .001) for the postoperative vocalperformance. The extent of surgery seemed tohave some influence but did not reach significantvalues (P � .142). Cigarette smoking, the time aftersurgery, the transversal division of the prelaryngealstrap muscles, and gender did not influence thepostoperative function of the vocal folds or thechange of the highest pitch of the singing voice,respectively.
Reexamination of the vocal performance of 38patients with observed early postoperative voice al-terations showed that the impairments of the sing-ing voice were reversible in all cases. The Student ttest revealed no significant differences in compar-isons of the second or third postoperative exami-nation with the preoperative data. Congruously,the relative change of the singing voice (calculatedby [preoperative value – postoperative value]/pre-operative value) declined to zero with increasing
-100 -50 0 50 -400 -200 0 200 400 600 8000
5
10
15
20
25
30
LPS HPS Differences in women
een the preoperative and early postoperative highest and. Both genders show only insignificant differences of up
itch of the singing voice. More evident differences areunts to –400 to � 800 Hz for women and –300 to �300perative improvement that may be explained by the factments.
000
5
10
15
20
25
30
s betwurgeryest p
h amoposto
time periods after surgery (Fig 6).

Surgery Musholt et al 985Volume 140, Number 6
DISCUSSIONAlthough vocal fold paralysis is considered the
most prominent complication after thyroid andparathyroid resection, the pre- and postoperativeassessment of the vocal performance as well as thedefinition of functional voice impairments as partof a postoperative quality control is a matter of
0 50 100 150
-1,0
-0,5
0,0
0,5
1,0
SPHextended
0 50 100 150
-1,0
-0,5
0,0
0,5
1,0
SPHlimited ce
Fig 6. Scattergram of the relative changes of the highestof the maximum frequency range of the singing voice (Mare displayed in the upper row, patients with limited cerviupper diagram and one in the left lower diagram) demonstraof more than 50%. In 12 patients (11 after extended surthe MFRS of more than 50% was observed. In all but 1 pat the second postoperative examination, and further desurgery.
ongoing debate. While some surgeons still do not
support routine preoperative and even postopera-tive indirect laryngoscopy in the absence of audiblechanges of the patient’s voice,16 it has been dem-onstrated that unilateral vocal cord palsy may becompletely asymptomatic.10,15 In Germany, pre-and postoperative assessment of the respiratory vo-cal fold mobility has become a kind of routine
0 50 100 150 days SRFM
al surgery
0 50 100 150 days SRFM
l surgery
of the singing voice (HPS, left) and the relative changesight). Men and women with extended cervical operationserventions in the lower row. Only 4 patients (3 in the leftlinically relevant, early postoperative decline of the HPSafter limited surgery), a clinically relevant reduction ofthe voice impairments decreased to subclinical findingsto normal within 50 to 150 days after extended cervical
-1,0
-0,5
0,0
0,5
1,0
cervic
-1,00
-0,50
0,00
0,50
1,00
rvica
pitchFRS, rcal intted a cgery, 1atient,clined
procedure in endocrine neck surgery not only for

986 Musholt et al SurgeryDecember 2006
medicolegal reasons. However, despite a normalintraoperative neuromonitoring signal and an un-remarkable post-thyroidectomy or postparathyroid-ectomy laryngoscopic result, patients mayexperience voice changes, or asymptomatic pa-tients may display impairments of the vocal perfor-mance that are detectable by extensive phoniatricevaluation only.
Our study prospectively evaluated the frequency,extent, variability, and course of postoperativevoice impairments (ie, impairments despite normalor negligibly changed respiratory mobility of thevocal folds) in 139 patients undergoing limited orextended endocrine cervical interventions using astandardized voice assessment protocol. In contrastto other studies, the surgical procedures were per-formed by a single endocrine surgeon, and patientswith limited cervical interventions—predominantlyparathyroidectomies for primary HPT—were in-cluded as a comparative group representing theinfluence of endotracheal intubation, limitedtrauma to the prelaryngeal strap muscles, and aneck wound. In addition, the evaluation was notrestricted to benign uncomplicated thyroid diseasebut encompassed patients with Graves disease (n �9), patients with previous neck surgery (n � 9), andpatients with thyroid carcinoma (n � 20) to ac-count for increasing surgical trauma in close prox-imity to the RLN as well as to the prelaryngeal strapmuscles.
A limitation of our study is the fact that not allpatients were reevaluated a second and third timeafter surgery, which relates first to the difficulty toconvince patients without clinical symptoms to un-dergo unpleasant examinations and second to thelimited resources of the phoniatric department.However, Stojadinovic et al9 showed that all pa-tients found to be asymptomatic 1 week post-thy-roidectomy remained symptom-free at 3-monthfollow-up. In addition, all patients with detectablevoice disturbances were reevaluated, demonstrat-ing that the detected voice changes were only tran-sient.
The described assessment of vocal performancein our study represents a restriction to simple-to-evaluate parameters that accurately and reproduc-ibly demonstrate voice impairments. Assessmentwith a Multi-Dimensional Voice Program (MDVP)software generates considerably more data thanpresented here, but the parameters assessed tendto be less reproducible and are more dependent onthe actual situation at time of examination (eg,patient motivation, time period after endotrachealintubation). It is well known, that even patients
who underwent no cervical surgery display consid-erable vocal fold pathology and therefore postop-erative voice changes.17
Among various quantitative and semi-quantita-tive parameters used to assess the voice perfor-mance, the highest pitch and the maximumfrequency range of the singing voice displayed dis-tinct differences expressing most accurately objec-tive impairments. As expected, no significantdifferences were observed in men and women afterlimited cervical operations, indicating that this mi-nor trauma to laryngeal structures is of inferiorimportance. In accordance with other authors,9
men and women displayed significant early postop-erative differences of the highest pitch and themaximum frequency range of the singing voicethat decreased with time. While univariate analysesimplied a relation of the postoperative alterationsto the extent of the cervical trauma, analysis ofcovariance revealed that, in contrast to this logicalassociation, only the preoperative maximum fre-quency range and the highest pitch of the singingvoice predict the postoperatively impaired voiceperformance. In other words, patients with excel-lent preoperative voice performances (eg, voiceprofessionals such as actors, singers, teachers, etc)are more prone to usually transient performancereductions. The extent of surgery seems to be ofsome influence; however, none of the factors clas-sifying this influence remained significant in themultivariate analysis.
To put this observation into perspective, one hasto consider that the measurement of the phona-tional voice range is highly dependent on the pa-tient’s motivation and that some reduction of thevoice performance may be expected early postop-eratively because of the patient’s anxiety and sorethroat. The comparison with the group of patientswho underwent limited surgery demonstrates thatthe resultant variability is limited, but extendedendocrine neck surgery may also intensify thesenon–surgery-associated but patient-dependent in-fluences.
Compared with other groups, the overall inci-dence of postoperative voice changes was low if a(surely arbitrary, but often used) cutoff value of50% is applied to differentiate clinically significantand nonsignificant findings. Only 4 of 139 (2.8 %)patients demonstrated a more than 50% reductionof the highest pitch of the singing voice, and 12 of139 (8.6%) patients displayed an equal loss of themaximum frequency range of the singing voice(Table IV).
Thirty-eight of 139 (27%) patients were selectedfor reevaluation because of postoperative voice im-
pairments. Considering the fact that up to 5% of
Surgery Musholt et al 987Volume 140, Number 6
patients may develop voice changes after endotra-cheal intubation, and with respect to the fact thathigh-risk patients (thyroid carcinoma and patientswith previous neck surgery) were also included inour study, the prevalence of postoperative voicechanges is markedly lower than in other studies,although all patients were thoroughly investigatedand our definitions of voice alterations did notdiffer significantly. The discrepancy may in part berelated to the surgical technique with meticuloushemostasis or to the difficulties to generate repro-ducible results during assessment of the voice per-formance as mentioned above.
Possible causes leading to postoperative voicechanges are multifaceted and complex in their in-teractions. The human voice is—apart from thefunction of the vocal cords—influenced by the ac-tion of the sternohyoid, sternothyroid, and omohy-oid muscles. Intraoperative mobilization or evendivision of these muscles or their innervatingnerves as well as postoperative adhesions to thelarynx or cervical trachea were hypothesized tocause impairments of phonation and swallowing. Incontrast, the present study was not able to demon-strate a statistically significant association. Neverthe-less, the documented postoperative voice changes arerelated to the type of cervical surgery. Dissection orthermal injury in close proximity of the RLNs, com-pression or traction of the nerve and laryngealstructures, as well as postoperative formation ofeven tiny hematomas close to the RLN may lead tooccult edema of the neural structure. Subsequentimpairments of the RLN function may be not clin-ically evident in patients who do not exploit theirfunctional voice capacity but may come to light inpatients who demonstrate excellent voice perfor-mance. That inflammation and postoperativeedema may be of clinical importance is also im-plied by a study from Wang et al18 who were able toinfluence the course of transient post-thyroidec-tomy RLN palsies by intraoperative administrationof corticosteroids.
Common surgical efforts during thyroidectomyto minimize postoperative dysphonia—ie, carefuldissection of the RLN, elaborate hemostasis, pres-ervation of the sternothyroid, sternohyoid, andomohyoid muscles, and so forth—did not pre-vent minor transient postoperative voice changes.Immediately after surgery, voice changes wereregularly observed in cases of intact RLN neuro-monitoring and laryngostroboscopically normalrespiratory vocal fold mobility. While alterations ofthe speaking voice were usually absent or remainedsubclinical, the changes of the singing voice—au-
dible even to untrained individuals—will matter tosingers or other voice professionals who are moreprone to postoperative dysphonia. Extended pre-and postoperative phoniatric workup may be indi-cated in this subgroup of patients who may needvoice rehabilitation to prevent permanent postop-erative impairments.
We thank Irene Schmidtmann, Department of MedicalBiometry, Epidemiology, and Informatics, for her sup-port of the statistical analysis.
REFERENCES1. Patow CA, Norton JA, Brennan MF. Vocal cord paralysis and
reoperative parathyroidectomy. A prospective study. AnnSurg 1986;203(3):282-5.
2. Moley JF, Lairmore TC, Doherty GM, Brunt LM, De-Benedetti MK. Preservation of the recurrent laryngealnerves in thyroid and parathyroid reoperations. Surgery1999;126(4):673-7; discussion 677-9.
3. Aluffi P, Policarpo M, Cherovac C, Olina M, Dosdegani R,Pia F. Post-thyroidectomy superior laryngeal nerve injury.Eur Arch Otorhinolaryngol 2001;258(9):451-4.
4. Bellantone R, Boscherini M, Lombardi CP, et al. Is theidentification of the external branch of the superior laryn-geal nerve mandatory in thyroid operation? Results of aprospective randomized study. Surgery 2001;130(6):1055-9.
5. Hong KH, Kim YK. Phonatory characteristics of patientsundergoing thyroidectomy without laryngeal nerve injury.Otolaryngol Head Neck Surg 1997;117(4):399-404.
6. Keilmann A, Hulse M. [Dysphonia following strumectomywith normal respiratory movement of the vocal cords]. FoliaPhoniatr (Basel) 1992;44(6):261-8.
7. Debruyne F, Ostyn F, Delaere P, Wellens W. Acoustic anal-ysis of the speaking voice after thyroidectomy. J Voice1997;11(4):479-82.
8. McIvor NP, Flint DJ, Gillibrand J, Morton RP. Thyroid sur-gery and voice-related outcomes. Aust N Z J Surg2000;70(3):179-83.
9. Stojadinovic A, Shaha AR, Orlikoff RF, et al. Prospectivefunctional voice assessment in patients undergoing thyroidsurgery. Ann Surg 2002;236(6):823-32.
10. Steurer M, Passler C, Denk DM, Schneider B, Niederle B,Bigenzahn W. Advantages of recurrent laryngeal nerve iden-tification in thyroidectomy and parathyroidectomy and theimportance of preoperative and postoperative laryngo-scopic examination in more than 1000 nerves at risk. Laryn-goscope 2002;112(1):124-33.
11. Yarbrough DE, Farley DR. I can’t sing anymore: voicechanges after thyroidectomy. Curr Surg 2003;60(6):554-60.
12. Sinagra DL, Montesinos MR, Tacchi VA, et al. Voicechanges after thyroidectomy without recurrent laryngealnerve injury. J Am Coll Surg 2004;199(4):556-60.
13. Hillel AD. Voice changes after thyroidectomy without recur-rent laryngeal nerve injury. J Am Coll Surg 2005;200(5):813.
14. Randolph GW, Kamani D. The importance of preoperativelaryngoscopy in patients undergoing thyroidectomy: Voice,vocal cord function, and the preoperative detection of in-vasive thyroid malignancy. Surgery 2006;139(3):357-62.
15. Farrag TY, Samlan RA, Lin FR, Tufano RP. The utility ofevaluating true vocal fold motion before thyroid surgery.Laryngoscope 2006;116(2):235-8.
16. Jarhult J, Lindestad PA, Nordenstrom J, Perbeck L. Routineexamination of the vocal cords before and after thyroid andparathyroid surgery. Br J Surg 1991;78(9):1116-7.
17. Kark AE, Kissin MW, Auerbach R, Meikle M. Voice changes

988 Musholt et al SurgeryDecember 2006
after thyroidectomy: role of the external laryngeal nerve. BrMed J (Clin Res Ed) 1984;289(6456):1412-5.
18. Wang LF, Lee KW, Kuo WR, Wu CW, Lu SP, Chiang FY. Theefficacy of intraoperative corticosteroids in recurrent laryn-geal nerve palsy after thyroid surgery. World J Surg2006;30(3):299-303.
DISCUSSIONDr Irving B. Rosen (Toronto, Ontario, Canada).
I would like to congratulate you on your presenta-tion. The really important aspect, it has legal im-plications obviously. I just want to ask you onequestion, though. Did you assess or analyze a con-trolled group of patients who had underwent pro-longed endotracheal intervention without really aneck procedure? Did you analyze a group of pa-tients who underwent surgery with a prolongedendotracheal intubation but did not have neck sur-gery or exposure of the recurrent nerve?
Dr Thomas J. Musholt. In the literature, dyspho-nia following endotracheal intubation for noncer-vical operations is described in 30% to 70% ofpatients, laryngeal trauma in about 6% of patients.In our study, we did not document the duration ofintubation for each patient. What we did is to clas-sify patients according to the extent of surgery; forexample, patients who underwent surgery for med-ullary thyroid carcinoma—usually operations last-ing 6 hours or more—were classified as extendedcervical cases. And these patients did not havemuch of a difference in postoperative dysphoniacompared to the patients who underwent limitedthyroid surgery.
Dr Gary B. Talpos (Detroit, Michigan). DrMusholt, this is very good. It is certainly helpful fora lot of us that see professional singers. The ques-tions I had: length of follow-up, for instance. Wewill frequently see individual singers that improve,and our voice people will tell neck surgery patients,whether it is endocrine or disk disease, it can takeup to 2 years for a voice to recover. Thankfully, Ihave not had to wait that long. The other question,what do you recommend in terms of voice exercise,voice rest, for your singers? Finally, do you usesteroids, or do you use laryngeal mask anesthesia?Have you studied those patients at all?
Dr Thomas J. Musholt. Last questions first: Wedo not routinely use laryngeal mask anesthesia orsteroids. I sometimes administer steroids when I amafraid that postoperative swelling of the vocal cordsmay occur, for example, in patients who underwenta previous neck operation with a lot of scar tissue.
We do not recommend any kind of specific voicetraining immediately following surgery. Only if wefind significant changes of the vocal cord mobility,
we refer the patient to a phonetician for voicetraining. In my experience, professional singersstart early postoperatively to independently assesstheir voice quality and to perform their own rou-tine voice exercises.
Dr Gary B. Talpos. In terms of follow-up, thelength—you said that most of your singers are backto normal within 6 weeks. Certainly we have seen ittake longer. And our voice specialists, our laryn-gologists will use a figure of 2 years.
Dr Thomas J. Musholt. We had no professionalsinger in this study group, but a lot of patients whoprofessionally talk a lot and thus were classified asvoice professionals. In our group, these patientsreported no voice impairments or other complaintsafter a period of 6 weeks. But we didn’t examineevery patient a second or third time postopera-tively, that is, 4 to 6 weeks and about 3 monthsfollowing neck surgery, respectively. So from the139 patients undergoing the first postoperativevoice assessment, we repeatedly examined onlythose that showed objective changes. That was thecase in 38 patients, equivalent to 27% of the pa-tients studied. All of these patients did not showclinically significant dysphonia at the 3-month fol-low-up assessment.
Dr Ashok R. Shaha (New York, NY). I think whatis important for all of us to appreciate: There is adifference between clinical dysphonia and voiceparameter analysis. We didn’t know much aboutthis 10 years back when we did not have videostro-boscopy, acoustic, and glottographic analysis. Whatwe are trying to do now is to analyze the voice. Andthere are minor changes. The changes that weshowed, 84% were by the analysis not clinical dys-phonia. These people have normal voice, normalvocal cord mobility. But when you analyze voice,there is a slight difference.
And I use the explanation that, as if we areopening a gift wrap, picking out a gift, you can’t putit back in the proper way. And I think that isprobably what happens in these patients. The mi-nor voice changes will persist. We saw the differ-ence from 84% to 14% changes after 3 months. Sothese people do improve in about 2 to 3 months.This is a very nice study.
Dr Thomas J. Musholt. I agree with you in theimportance of differentiation of minor objectivevoice changes from clinically significant voicechanges. But there are problems associated withvoice assessments: the more parameters you lookat, the more differences you will find. And you willfind those differences also in patients who didn’tundergo surgery at all. So if you test the sameproband 1 week and the next week, you will find a
slight difference in voice performance. Therefore,
Surgery Musholt et al 989Volume 140, Number 6
when studying postoperative dysphonia, one has todefine differences that really matter to the patients.And that cutoff level is completely unclear at themoment, I think.
Dr Greg Randolph (Boston, Mass). I think this isan excellent paper and a very interesting topic. Iwould like to just make a comment and then ask aquick question.
Yesterday, we saw a paper where the immediatevocal cord paralysis rate was 5% and in secondarythyroidectomy was 12%. So I think it is very impor-tant to look at your data and emphasize that voicechange assessment postoperatively is not the sameas laryngoscopic exam, and that for us to reallyunderstand what sort of surgery we are doing andwhat our outcomes are, we need to look at thelarynx at least with flexible fiberoptic endoscopy ifnot more advanced techniques like stroboscopy.This is especially important in the US, where pay-for-performance outcome measures are being ini-tiated, initiatives are being forwarded. So really toknow what rates of vocal cord paralysis exist, wecan’t ask the patient; there are voice changes thatoccur with and without vocal cord paralysis exist. Inmy mind, in our group, we think of voice changeswithout vocal cord paralysis in three categories.
One, those that are attributable to the endotra-cheal tube. Vocal cord edema, arytenoid cartilagedislocation are examples.
The second kind of category of voice changeswithout vocal cord paralysis would just be nonspe-cific surgical changes like strap muscle retraction,strap muscle division, and adhesions from surgery.Important in that category, I think, is probablycricothyroid muscle edema. You know, if you openup the thyroid bed 2 days after thyroidectomy, yousee this fibrinous soup that is right up against thecricothyroid muscle. This is a laryngeal muscle that
is on the outside of the larynx directly in the sur-gical bed, and even with preservation of the exter-nal branch it, I think, probably suffers a toxic insultfrom these thyroid bed inflammatory mediators fora period of time, even with preservation of the SLN.
Then the third category, which I think is prob-ably the most difficult to deal with, is voice changeswithout vocal cord paralysis; this category is unrec-ognized superior laryngeal nerve paresis or paraly-sis. Because, as you know, the endoscopic findingsthat correlate with that are very subtle and difficultto diagnose.
So the message I am taking from your study isthat voice changes and postoperative glottic func-tion are 2 separate things and that we really have tolook at the larynx postoperatively to know what ourrates of RLN paralysis are.
And I just wanted to ask, do you now routinelyuse laryngoscopy in all patients undergoing thy-roidectomy postoperatively? The second questionis, for those patients with upper register problems,do you do cricothyroid muscle EMG, which is kindof the gold standard in detection of SLN injuries?
Dr Thomas J. Musholt. I don’t perform cricothy-roid muscle EMGs because the patients do notconsent to that very unpleasant examination. At themoment, we routinely examine patients with video-laryngostroboscopy before and after thyroid andparathyroid surgery, but we don’t do routinely flex-ible fiberoptic endoscopy. We perform follow-uppostoperative stroboscopy in case that the phoniat-ric specialist recognizes differences between thepre- and postoperative status of the patient. So nowin daily routine we continue to select patients foradvanced diagnostic procedures and voice assess-ment following neck surgery. I strongly recom-mend laryngoscopic examination in every patientbefore and after thyroidectomy and parathyroidec-tomy, because—as you said— one cannot rely on
clinical voice assessment only.