Embed Size (px)
Citation preview

Archives ofDisease in Childhood 1990; 65: 739-745
Changes in pulmonary circulation in severe
bronchopulmonary dysplasia
A Bush, C M Busst, W B Knight, A A Hislop, S G Haworth, E A Shinebourne
AbstractEight patients with severe bronchopulmonarydysplasia underwent cardiac catheterisation.Seven had a pulmonary vascular resistance>3 mm Hg.l-' min.m2 (mean 8-9, range 2-2-13-8). All had raised intrapulmonary shunts(mean 25-6%, range 5-4-50%, normal <5%).Two had a high alveolar dead space, and twohad unsuspected congenital heart disease.Epoprostenol (prostacyclin), but not 100%oxygen, caused a significant fail in pulmonaryvascular resistance. Death was associatedwith a high pulmonary vascular resistance anda high shunt. Morphometric studies in threecases showed normal numbers of airways, butincreased thickness of bronchial muscle. Thenumbers of alveoli were reduced and the wailsthickened. There was increased medial thick-ness in small pulmonary arteries with distalextension of muscle. In the oldest child somevessels were obliterated by fibrosis. Wespeculate that measurements of pulmonaryvascular resistance and shunt may have prog-nostic value; that a trial of pulmonary vasodi-lators other than oxygen might be worthwhilein patients with poor prognosis; and thatabnormalities of the pulmonary circulationcontribute to the difficulties of managingpatients with bronchopulmonary dysplasia.
Brompton Hospital,Fulham Road,London SW3 6HPA BushC M BusstW B KnightE A ShinebourneInstitute of Child Health,LondonA A HislopS G HaworthCorrespondence to:Dr Shinebourne.Accepted 28 February 1990
The aggressive treatment of low birthweight,premature infants with respiratory distress hasbeen extremely successful, but the cost has beenthat some survivors are left with chronic lungdisease. Bronchopulmonary dysplasia was firstdescribed in 1967,' and is now increasinglyrecognised as a major cause of respiratory dis-ability in infants.2 3 There have been manystudies of airway function4 5 and lung mecha-nics,6 7 but the cardiovascular consequences ofbronchopulmonary dysplasia have received lessattention,4 8-12 despite the recognition of theprognostic importance of cor pulmonale in theearliest descriptions of the disease.'The Brompton Hospital is a tertiary referral
centre for infants with severe bronchopulmon-ary dysplasia. Infants referred to the depart-ment of paediatric cardiology undergo cardiaccatherterisation, mainly to exclude clinicallyimportant cardiac structural defects. At thesame time we assess the response of the pulmon-ary circulation to vasodilators to see if theymight be beneficial. We describe here the pul-monary haemodynamics and the abnormalitiesin gas exchange in this selected group, correlat-ing them with quantitative lung morphologywhen possible.
Patients and methodsWe studied eight infants who met the standardclinical diagnostic criteria for bronchopulmon-ary dysplasia,'3 namely a respiratory disorderbeginning with acute lung injury in the first twoweeks of life; at least 28 days postnatal age; andappreciable clinical (tachypneoa, intercostalretraction), radiographic (hyperinflation, cysticareas, fibrotic strands), and functional (arterialoxygen pressure (PaO2) <8 kPa (60 mm Hg)or carbon dioxide pressure (PaCO2) >6 kPa(45 mm Hg) while breathing air) abnormalities.These patients were referred consecutively fromother hospitals during a three year period. Theindication for referral was failure to improveclinically. Monitoring and treatment withoxygen, digoxin, and diuretics had beendecided by the referring paediatricians andvaried among the different referring centres. Nopatient had systemic hypertension.'4 Informedconsent by proxy was obtained from the parentsin each case, and the procedures were approvedby the Brompton Hospital ethics committee.
PHYSIOLOGICAL STUDIESFull details of the methods have been publishedelsewhere.'5 16 Briefly, the infants were studiedwhile they were anaesthetised, paralysed, andventilated. We measured cardiac output by thedirect Fick principle, and calculated pulmonaryvascular resistance, wasted ventilation (alveolardead space), and wasted perfusion (anatomicalshunt). We assessed the fall in pulmonary vas-cular resistance in response to administration of100% oxygen and to prostacyclin given intrave-nously.
For the calculations of cardiac output, oxygenconsumption was measured by a mass spectro-meter (MGA 200) using the steady state, argondilution method.'5 Blood oxygen contents werecalculated from measured PaO2, pH, and baseexcess (Corning 170 blood gas analyser), usingKelman's subroutine and assuming the solubil-ity of free oxygen in blood to be 0-003 ml/100ml/mm Hg.'7 The mass spectrometer was alsoused to monitor end tidal gases to ensure arespiratory steady state was maintainedthroughout the study. End tidal PCO2 was cal-culated as the mean of at least eight measure-ments, which had to differ by less than 05 kPa(3-8 mm Hg).
Intravascular pressures were measured withfluid filled catheters introduced percutaneouslyinto the femoral artery and vein and screenedinto position in the aorta and pulmonary artery,respectively. Pulmonary vascular resistance wascalculated as (mean pulmonary artery
739
on 10 July 2019 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.7.739 on 1 July 1990. Dow
nloaded from

Bush, Busst, Knight, Hislop, Haworth, Shinebourne
pressure - mean left atrial pressure)/cardiacindex. Pulmonary capillary wedge pressure was
substituted for left atrial pressure where thiscould not be measured directly. In all cases thiswas less than 10 mm Hg, and did not changeappreciably during the study. We also calcu-lated the percentage of the alveolar deadspace-that is, that part of the alveolar tidalvolume (tidal volume minus the anatomicaldead space) that reached alveoli which were notperfused-an index of wasted ventilation. Thecalculation is based on the Bohr equation,which gives percentage alveolar dead spaceequal to [(1 - end tidal PCO2)/arterial PCO2x 100]. Wasted perfusion (anatomical shunt on
100% oxygen) was calculated from the shuntequation ([Cc'02 - CsaO2]/[Cc'02 -CpaO2])%where Cc'02, CsaO2, CpaO2 are the bloodoxygen contents of pulmonary end capillary,aortic, and mixed venous blood, respectively.Pulmonary end capillary P02 was assumed to bewithin 1-3 kPa (10 mm Hg) of alveolar P02,which was calculated from the measured endtidal PCO2 using the alveolar air equation.The initial measurements were made when
the infants were ventilated on air, or the lowestinspired oxygen concentration that was con-
sidered safe. Respiratory steady state was con-
firmed by monitoring end tidal gases. Thepatients were then switched to 100% oxygen,and the measurements repeated after not lessthan 10 minutes ventilation. All other ventilatorsettings were constant during the study. Ad-equacy of alveolar nitrogen washout (mixedexpired nitrogen <1%) was confirmed using themass spectrometer. If the pulmonary vascularresistance on 100% oxygen was appreciablyraised (>4 units), prostacyclin was given bycontinuous infusion into a peripheral vein, ini-
tially at a dose of 5 ng/kg/min. The measure-
ments were repeated at the end of five minutes.The dose was then increased by steps of 5 ng/kg/min, and measurements repeated after fiveminutes, until either a dose of 20 ng/kglmin hadbeen reached, or mean aortic pressure had fallenby 20 mm Hg. Finally the infusion was stopped,and diagnostic angiography carried out. We didnot do pulmonary wedge angiograms.
PATHOLOGICAL STUDIES ON THE LUNGLung tissue was obtained at necropsy fromcases 2, 3, 6, and 8. The initial necropsies were
carried out at the referring hospitals, and no
special preparation of the lungs was under-taken. The normal values were also taken fromlung tissue that had not undergone specialpreparation. In each case at least four blocks oftissue were taken from different parts of thelung, and 4 ,um paraffin embedded sectionswere stained with haematoxylin and eosin,periodic acid Schiff's reagent, and Miller's elas-tic stain counterstained with van Geison's stain.Microscopically, the diameter and thickness ofthe muscle wall of the respiratory unit arteriesand peripheral veins were measured with an
eyepiece graticule. 18 Percentage arterial wallthickness was calculated as: (twice the wallthickness/external diameter). The extension ofmuscle along the arterial pathway was deter-mined. For the airways, the diameter of smallbronchi and bronchioli was measured. Theamount of bronchial wall muscle was estimatedby planimetry using the Kontron MOP Video-plan image analyser, and expressed for each air-way as area in mm2/mm length of lumen. Thenumber of alveoli in the acinar region was esti-mated by calculating the Emery count.'9
ResultsThere were four boys and four girls, mean age
12 months, range 10 weeks to 3 years (table 1).At the time of cardiac catherisation, cases 1-7were being treated for cor pulmonale, whichhad been diagnosed on clinical grounds. Allwere receiving diuretics (frusemide and spir-onolactone) and cases 1-3 and case 5 were
receiving digoxin. There was only one long termsurvivor; cases 1, 2, 6, and 7 died of progressivecardiorespiratory failure associated with pre-sumed bronchopulmonary sepsis. In case 1,Candida albicans was isolated from the naso-
pharyngeal aspirate. In the other infants thediagnosis was a clinical one, but no pathogenicorganisms were isolated. Case 3 died after aspir-ating a feed, and case 4 died in the intensive careunit of intractable pulmonary hypertension.The deaths were attributed to the complicationsof bronchopulmonary dysplasia, not to thehaemodynamic studies. Case 8, whose mainproblem was congenital heart disease, had sur-
gical correction of the anomalous vena cava, butdied after a stormy postoperative course compli-cated by recurrent pulmonary oedema, infec-tion, and renal failure.
Table I Details of patients studied
Case Age Sex Weight Fractional inspired Electrocardiographic Echocardiographic Type of ventilationNo (years) (kg) oxygen concentration findings findings
I 1-1 Female 3-7 Air Right ventricular Right ventricular Spontaneoushypertrophy hypertrophy
2 0 5 Female 4-6 Low flow oxygen Right ventricular Right ventricular Spontaneoushypertrophy hypertrophy
3 3-5 Female 8-7 Air Right ventricular Right ventricular Spontaneoushypertrophy hypertrophy
4 0 5 Male 3-6 10 Right ventricular Right ventricular Intermittenthypertrophy hypertrophy positive pressure
5 0-8 Male 6-3 Low flow oxygen Right ventricular Right ventricular Spontaneoushypertrophy hypertrophy and
ventricular septaldefect
6 0-2 Male 2-3 0-6 Normal Normal Intermittentpositive pressure
7 0-2 Male 3-7 0-3 Normal Normal Spontaneous8 1-8 Female 7-9 Air Normal Normal Spontaneous
740
on 10 July 2019 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.7.739 on 1 July 1990. Dow
nloaded from

Changes in pulmonary circulation in severe bronchopulmonary dysplasia
PHYSIOLOGICAL STUDIESThe individual results are plotted in figs 1-3.For the baseline measurements, mean (SD)PaO2 was 6-61 (3 04) kPa and PaCO2 was 4 45(0-83) kPa. All patients had raised anatomicalshunts (mean 25-6%, range 5-4-50-0, normal5%). Two patients had high alveolar dead space,26% and 30%, respectively, the normal being5%. Seven patients had raised pulmonary vascu-lar resistance (mean 8-8 mm Hg.l-.min.m2,range 2-2-13-8, the normal being <3 units).There were cardiac structural lesions in two
80-
I
E 60-
C-
coc)0
a)
CucoC0E 20-L
Air °2
18-
16-Ca
= 14-
C.)- 12-
C4-o
- 10-
coCDco 8-
Cu
C 6-0E0- 4-
2-
1
5
2
_ 6
5 10 15 20
Prostacyclin (ng/kg/min)
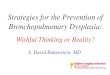
Figure I Individual changes in pulmonary artery pressurewith 100% oxygen (02) and prostacyclin. The numberscorrespond to the case numbers in table 1. The baselineforcases 6 and 7 was not air, butfractional inspiratory oxygenof0-6 and 0-3, respectively.
6-
4-
2-
7
8
/3
4gg~R> 516
Air 02 5 10 15 20
Prostacyclin (ng/kg/min)Figure 2 Individual changes in cardiac output with 1000/ooxygen (02) and prostacyclin. The numbers correspond to thecase numbers in table 1. The baselinefor cases 6 and 7was not air, butfractional inspiratory oxygen of0-6 and 0-3,respectively.
n :,;;
.53i
67
8
Air 02 5 10 15 20Prostacyclin (ng/kg/min)
Figure 3 Individual changes in pulmonary vascularresistance with 1000/o oxygen (02) and prostacyclin. Thenumbers correspond to the case numbers in table 1. Thebaselinefor cases 6 and 7 was not air, butfractionalinspiratory oxygen of0-6 and 0-3, respectively.
patients. Case 5 had a small ventricular septaldefect, which was haemodynamically unimpor-tant. Case 8 had anomalous drainage of thesuperior vena cava into the left atrium, whichalmost totally accounted for the systemic ar-terial desaturation.When switched to 100% oxygen, ventilation
was comparable (mean (SD) PaCO2 =4-43(1-25) kPa) and PaO2 rose to 25-51 (17-71) kPa.Mean pulmonary artery pressure showed littlechange except in case 3, in whom it fell by 18mm Hg. Cardiac output and pulmonary vascu-lar resistance rose in two patients and fell inthree others when they were given100% oxygen. Group mean pulmonary vascularresistance was unchanged (8-8 (4-2)). Whenprostacyclin was added, ventilation remainedcomparable (PaCO2=4-56 (1-47)). Cardiac out-put rose in five of six patients and pulmonaryvascular resistance fell in all patients. Thechanges in PaO2 are shown in fig 4. All patientsshowed rises when given 100% oxygen, but intwo patients there were marked falls when theywere given prostacyclin. These falls did notaffect the blood oxygen content significantly,because the starting PaO2 was so high.The group data are summarised in figs 5 and
6. These results were prepared by removing thebaseline variation and expressing the results asthe percentage change over the measurementwhen breathing air. We selected the dose ofprostacycin that caused the maximum reduc-tion in pulmonary vascular resistance. Thevalues of the other variables at this dose of pros-tacyclin were then compared with the baseline
N
E
1-
CL
co0.0
cUC)
a t...........t -----------r ...........r........11-4
usl -------;-------;--------........................
741
on 10 July 2019 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.7.739 on 1 July 1990. Dow
nloaded from

Bush, Busst, Knight, Hislop, Haworth, Shinebourne
Aortic Systemicpressure vascular resistance
Heart rate
* p< 0.05
Air °2 1 Air 02Prostacyclin Prostacyclin
Air 02 5 10 15 20
Prostacyclin (ng/kg/min)
Figure 4 Individual changes in systemic arterial oxygenpressure (PaO2) with 1000/o oxygen (02) and prostacyclin.The numbers correspond to the case numbers in table 1. Thebaselinefor cases 6 and 7 was not air, butfractionalinspiratory oxygen of0-6 and 0-3, respectively.
Air 02
Prostacyclin
Figure 6 Percentage changes over baseline (vertical axis) insystemic haemodynamics with 1000/o oxygen (02) and thedose ofprostacyclin resulting in the lowestpulmonaryvascular resistance. There was no significant change in aorticpressure: systemic vascular resistance fell, and heart rate rose,when prostacyclin was given. These results arefrom thefivepatients with complete datafor all doses ofprostacyclin (casenumbers 1-3, 5, and 6). Bars indicate mean (SEM) andsignificant differences are indicated.
Cardiac Pulmonaryoutput vascular
resistance
0
I,
* p<O.05L p<O.020 P<0.O1
t tAir 021
t t IAir 02Prostacyclin Prostacyclin Prostacyclin
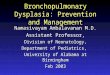
Figure 5 Percentage changes over baseline (vertical axis)in pulmonary haemodynamics with 100% oxygen (02) andthe dose ofprostacyclin resulting in the lowestpulmonaryvascular resistance. There was no significant change inpulmonary artery pressure; cardiac output rose, andpulmonary vascular resistance fell when prostacyclin wasgiven. These results arefrom thefive patients with completedata for all doses ofprostacyclin (case numbers 1-3, 5, and6). Bar indicate mean (SEM) and significant differences areindicated.
measurement. Figure 5 shows that there was no
significant change in pulmonary artery pressureat any time, and (for the group) no significantchange in any variable when breathing 100%oxygen. Cardiac output (mean (95% confidenceintervals)) rose by 30-8 (18-8 to 42-8)% whenprostacyclin was added to oxygen, and pulmon-ary vascular resistance fell by 23-2 (9-1 to37-3)%. Prostacyclin also had effects on the sys-
temic circulation (fig 6). There was no change inaortic pressure, but systemic vascular resistancefell by 38-8 (13-8 to 63 8)%, and heart rate roseby 11 0 (3-9 to 18-1)%, when prostacyclin wasadded to oxygen; from these data, there was noevidence for any selective effect on the pulmon-ary circulation.Of the six patients who died with severe bron-
chopulmonary dysplasia (cases 1-4, 6, and 7),two had pulmonary vascular resistance of morethan 7 units, two had anatomical shunts of morethan 30%, and two had both these abnormali-ties. Both patients with wasted ventilation ofmore than 25% died.
PATHOLOGICAL STUDIESIn cases 2, 3, and 6 the structure of the periph-eral airways and alveoli was abnormal, thealveoli varying in size and shape. The alveolarwalls were thickened with an excess of collagenand elastin, and in cases 2 and 3 capillarydensity seemed to be increased. In all threecases, an Emery count indicated a reduction inalveolar number (table 2). In the oldest, aged 3years, the alveolar count was similar to the nor-mal value at birth. The peripheral airways wereof normal size for age, but the amount of bronc-hial smooth muscle was increased. There wereno areas of extensive fibrosis. In the vascula-ture, pulmonary arterial smooth muscle wasincreased, as shown by a significant increase inmean percentage arterial medial thickness andby extension of muscle into more peripheralarteries than normal so that most of the alveolarwall arteries were completely muscularised(table 2, fig 7). Only the oldest case showed inti-mal proliferation, with hyalinisation of the
80-
60-
co5 40-
20-
1401
120-
100-
80-
60-
40-
20-
n%-.
Pulmonaryarterialpressure140-
120-
100-
80-
60-
40-
20-
t IAir 02
I]
n I I
f
742
2
7
5
1
3
4 ........... :::::::::::6............ ..........
*
on 10 July 2019 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.7.739 on 1 July 1990. Dow
nloaded from

Changes in pulmonary circulation in severe bronchopulmonary dysplasia
Table 2 Results of pathological studies
Case Age at Percentage arterial wall Percentage vein wall Emety Bronchial muscleNo death (years) thickness thickness (SO-100i) count (mmlmm length ol lumen)
<IOO,u >100y
2 1-3 17-9** 22 9**;' 5 0 5-0 0-0053 35 31-2'' 243*** 66' 57 00076 0-6 15*59*t* 96* 5*9* 4 7 0 01'3'8 2-0 l34** 94 6 3 7 4 0 003
Normal values:Babies born at full term 24.9I8 14.7I8 4.718 5.519 0-0015taged 0-24 hoursInfants aged 8 months 9.618 7 218 4-718 8 5'9 0-0045tto 3 years
*p<O-OS; **p<O-Ol; ***p<o-001 compared with normal range.tA A Hislop and S G Haworth, unpublished observations.
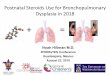
Figure 7 Photomicrograph ofnecropsy lung tissuefrom case 3 stained with Miller's elasticstain and van Gieson's stain magnificationx 720. A muscular pulmonary artery (wallthickness 30%/) is seen at thejunction ofalveoli. Abbreviations: cap=capillary, al=alveolus,and c=collagen.
media in some vessels. Cases 3 and 6showed an increase in vein wall thickness withtarterialisation'.20 In general the changes weremore severe with age, but the numbers are toosmall for statistical analysis.
Case 8, who had an anomalous insertion ofthe left superior vena cava to the left atrium,was thought to have severe bronchopulmonarydysplasia before the haemodynamic study. Atnecropsy, however, she had none of the patho-logical features. The Emery count indicatedthat the number of alveoli was within normallimits and the airways were of normal size andmuscularity (table 2). The significant increasesin pulmonary arterial and vein wall thicknesswere compatible with the cardiac anomaliespresent in this child.
DiscussionWe have reported eight patients who were sentto a- tertiary referral centre with a diagnosisof severe bronchopulmonary dysplasia. Onepatient (case 8) was cyanosed because of acardiac structural lesion, and histology of thelung confirmed only minor changes of broncho-pulmonary dysplasia. Similar diagnostic diffi-culties have been reported by others,9 and itmay be difficult to assess clinically the relative
severity of heart and lung disease. This patientis not discussed further. The main findings inthe other seven patients were increases inpulmonary vascular resistance (n=7), anatomi-cal shunt (n=2), and alveolar dead space (n=2).In this selected group of patients, prostacyclinwas a better pulmonary vasodilator thanoxygen. The patients with pulmonary vascularresistance of greater than 7 units, or anatomicalshunt of more than 30%, or both (n=6), diedfrom their disease. Quantitative histology (n=3)showed reduced numbers of alveoli with thick-ened walls. There was increased medial musclethickness in small pulmonary arteries, and dis-tal extension of smooth muscle. The changestended to be more severe with increasing ageand pulmonary vascular resistance, althoughthere were too few infants for statistical testing.The physiological study compared the pul-
monary vascular reactivity to oxgyen and pros-tacyclin. We chose prostacyclin because we hadpreviously shown it to be a safe pulmonary vaso-dilator in children with congenital heartdisease.16 Oxygen has been reported to lowerpulmonary vascular resistance in some butnot all patients with bronchopulmonary dys-plasia. 10 1 In our selected group of patients,oxygen had no acute effects on pulmonaryhaemodynamics, whereas prostacyclin caused apronounced fall in pulmonary vascular resist-ance. Other workers have reported falls in pul-monary vascular resistance in patients withbronchopulmonary dysplasia given hydrala-zine.12 We recommend extreme caution, how-ever, if prostacycin or other bloodborne pul-monary vasodilators are to be used. Case 4 wasunable to tolerate a dose higher than 10 ng/kg/min because of systemic hypotension. Prostacy-clin caused a fall in systemic vascular resistancein all patients, and a fall in PaO2 in two. Hydra-lazine may also cause adverse reactions inpatients with bronchopulmonary dysplasia. 12Under controlled conditions, bloodborne pul-monary vasodilators may be useful adjuncts tomanagement, and possibly allow reductions ininspired oxygen tension, one of the majoraetiological factors in bronchopulmonary dys-plasia.
The structural study showed that in threecases the abnormalities of the airways consistedof a failure of alveolar multiplication with anincrease in both the amount of bronchialsmooth muscle, and in the amounts of collagenand elastin within the alveolar walls. Theseabnormalities of airways were no more severe,
743
on 10 July 2019 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.7.739 on 1 July 1990. Dow
nloaded from

744 Bush, Busst, Knight, Hislop, Haworth, Shinebourne
however, than those reported, in a previousseries of children who also had neonatal respira-tory distress and who subsequently did notdevelop cor pulmonale.2' This difference innatural history is not explained by bronchoal-veolar changes alone. Neither group of patientshad the extensive fibrosis described in theclassic accounts of bronchopulmonary dys-plasia.' 22 Such severe damage is now rarelyseen, probably because of improvements inmethods of mechanical ventilation.Cor pulmonale is usually associated with
alveolar hypoxia in adults and children, but inour cases failure of alveolar development wasprobably an important additional factor. In nor-mal children new respiratory unit arteriesdevelop after birth as the alveoli multiply.23Failure of alveolar development therefore leadsto a reduction in the number of peripheral arter-ies, which would predipose to the developmentof cor pulmonale. Other predisposing factorsinclude a pronounced reduction in diameter ofthe lumens by excessive muscularisation ofsmall precapillary arteries, the probable obliter-ation of some alveolar wall arteries by fibrosis,and possibly also capillary distortion by abnor-mally shaped alveoli.
There are few published data correlatingpulmonary haemodynamics with lung morpho-logy in infants with bronchopulmonary dyspla-sia. A single premature infant with supra-systemic pulmonary artery pressures had ahypoplastic pulmonary circulation, but the cli-nical course had not been typical of bronchopul-monary dysplasia.24 A large pathological studyconfirmed that hypertensive pulmonary vascu-lar disease is common in bronchopulmonarydysplasia,25 but no haemodynamic data wereavailable. In contrast to our study and to thefindings of others,25 26 one group reportedincreased numbers of small pulmonary arterieswith medial wall thicknesses that were less thannormal27; we cannot account for these discre-pancies.
Although ours is a small series, the severity ofthe pulmonary arterial changes tended toincrease with age, as shown by the progressiveincrease in pulmonary vascular smooth muscle,and the presence of some hyalinised arteries inthe oldest child. Correlation between structureand function is difficult because of the smallnumber of cases and the relatively long timeinterval (up to nine months) between cardiaccatheterisation and death in these youngpatients. The wasted perfusion might be theresult of collagen deposition in the alveolarwalls, and possibly also in the blood gasbarrier.28 Wasted ventilation could be attri-buted to a reduction in peripheral pulmonaryarterial number and the diameters of thelumens.These data were obtained from a highly
selected subgroup of patients with bronchopul-monary dysplasia, but may have implicationsfor the outpatient treatment of less severelyaffected patients. The current mainstay of treat-ment is domiciliary oxygen.29 30 Treatmentwith an oral pulmonary vasodilator would bemuch more convenient than low flow oxygen.Theoretically it may even be safer, in that there
is some evidence that even modest increases ininspired oxygen tensions may be toxic.3' 32 Anyfall in PaO2 would be dangerous, however, inpatients who have arterial hypoxaemia whilebreathing air, because a large fall in bloodoxygen content would result. Possibly the com-bination of low flow oxygen and an oral vasodi-lator might be more useful than either alone. Ifthey are to affect the natural history of thedisease appreciably, however, they would prob-ably have to be given much earlier, before thepulmonary circulation became irreversiblydamaged. Any such treatment should be thesubject of a carefully controlled trial before itcould be recommended for general use.To summarise, we have reported the pulmon-
ary circulatory abnormalities in eight patientsreferred with a clinical diagnosis of bronchopul-monary dysplasia. In this selected group,pulmonary vascular disease showed itself phy-siologically by an increased pulmonary vascularresistance and by disturbances of ventilation toperfusion matching. The increases in pulmon-ary vascular resistance were reduced more by abloodborne vasodilator, prostacyclin, than by100% oxygen. In these patients the morphologi-cal counterpart was failure of alveolar multi-plication and consequent hypoplasia of thepulmonary circulation, extensive muscularisa-tion of precapillary arteries and peripheralveins, and some obliteration of vessels by fibro-sis in case 6. Most of these developmentalchanges are probably irreversible, although areduction in muscularity is possible. The reasonwhy some patients develop severe pulmonaryvascular disease secondary to bronchopulmon-ary dysplasia is not clear. We suggest thatcardiac catheterisation should be carried outmore readily in patients with bronchopulmon-ary dysplasia. It is important to exclude cardiacstructural lesions, and hyperinflation may makeechocardiography difficult. Cardiac catheterisa-tion may also help to choose the most effectivetreatment for the individual patient. In addi-tion, we need to increase our understanding ofthe role of the pulmonary circulation in thepathogenesis of this condition.AB, AAH, and SGH were supported by the British HeartFoundation.
1 Northway WH, Rosan RC, Porter DY. Pulmonary diseasefollowing respiratory therapy of hyaline-membrane disease.N Engi J Med 1967;276:357-68.
2 Greenough A, Roberton NRC. Morbidity and survival inneonates ventilated for the respiratory distress syndrome.Br Med J 1985;290:597-600.
3 Bancalari E, Gerhardt T. Bronchopulmonary dysplasia.Pediatr Clin North Am 1986;33:1-23.
4 Harrod JR, L'Heureux P, Wangenstein OD, Hunt CE.Long-term followup of severe respiratory distress syn-drome treated with IPPB. J Pediatr 1974;84:277-86.
5 Smyth JA, Tabachnik E, Duncan WJ, Reilly BJ, Levison H.Pulmonary function and bronchial hyperreactivity in long-term survivors of bronchopulmonary dysplasia. Pediatrics1981;68:336-40.
6 Bryan MH, Hardie MJ, Reilly BJ, Swyer PR. Pulmonaryfunction studies during the first year of life in infants re-covering from respiratory distress syndrome. Pediatrics1973;52:169-78.
7 Tepper RS, Pagtakhan RD, Taussig LM. Non-invasivedetermination of total respiratory system compliance ininfants by the weighted-spirometer method. Am Rev RespirDis 1984-130:461-6.
8 Berman W, Yabek SM, Dillon T, Burstein R, Corlew 5.Evaluation of infants with bronchopulmonary dysplasiausing cardiac catheterization. Pediatrics 1982-70:708-12.
9 Abman SH, Accurso FJ, Bowman CM. Unsuspected car-diopulmonary abnormalities complicating bronchopulmon-ary dysplasia. Arch Dis Child 1984-59:966-70.
10 Abman SH, Wolfe RR, Accurso FJ, Koops BL, Bowman
on 10 July 2019 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.7.739 on 1 July 1990. Dow
nloaded from

Changes in pulmonary circulation in severe bronchopulmonary dysplasia 745
CM, Wiggins JW. Pulmonary vascular response to oxygenin infants with severe bronchopulmonary dysplasia. Pediat-rics 1985;75:80-4.
11 Berman W, Katz R, Yabek SM, Dillon T, Fripp RR, PapilleLA. Long-term follow-up of bronchopulmonary dysplasia.J Pediatr 1986;109:45-50.
12 Goodman G, Perkin RM, Anas NG, Sperling DR, Hicks DA,Rowen M. Pulmonary hypertension in infants with bron-chopulmonary dysplasia. J Pediatr 1988;112:67-72.
13 O'Brodovich HM, Mellins RB. Bronchopulmonary dyspla-sia. Am Rev Respir Dis 1985;132:694-709.
14 Abman SH, Warachy BA, Lum GM, Koops BL. Systemichypertension in infants with bronchopulmonary dysplasia.J Pediatr 1984;104:929-31.
15 Davies NJH, Denison DM. The measurement of metabolicgas exchange by mass spectrometry alone. Respir Physiol1979;36:261-7.
16 Bush A, Busst CM, Booth K, Knight WB, Shineboume EA.Does prostacyclin enhance the selective pulmonary vasodi-lator effect of oxygen in children with congenital heartdisease? Circulation 1986;74:135-44.
17 Kelman GR. Digital computer subroutine for the conversionof oxygen tension into oxygen saturation. J Appl Physiol1966;21:1375-6.
18 Haworth SG, Hislop AA. Pulmonary vascular development:normal values of peripheral vascular structure. Am JCardiol 1983;52:578-83.
19 Emery JL, Mithal A. The number of alveoli in the terminalrespiratory unit of man during late intrauterine life andchildhood. Arch Dis Child 1960;35:544-7.
20 Wagenvoort CA. Morphologic changes in the intrapulmonaryveins. Hum Pathol 1970;1:205-13.
21 Hislop A, Wigglesworth JS, Dessai R, Aber V. The effects of
preterm delivery and mechanical ventilation on human lunggrowth. Early Hum Dev 1987;15:147-64.
22 Taghizadeh A, Reynolds EO. Pathogenesis of bronchopul-monary dysplasia following hyaline membrane disease. AmJ Pathol 1976;82:241-58.
23 Hislop A, Reid L. Pulmonary arterial development duringchildhood: branching pattern and structure. Thorax 1973;28:129-35.
24 Rendas A, Brown ER, Avery ME, Reid LM. Prematurity,hypoplasia of the pulmonary vascular bed, and hyperten-sion: fatal outcome in a ten month old infant. Am RevRespir Dis 1980;121:873-80.
25 Stocker JT. Pathologic features of long-standing 'healed'bronchopulmonary dysplasia. A study of 28 3- to 40-month-old infants. Hum Pathol 1986;17:943-61.
26 Sobonya RE, Logvinoff MM, Taussig LM, Theriault A.Morphometric analysis of the lung in prolonged broncho-pulmonary dysplasia. Pediatr Res 1982;16:969-72.
27 Tomashefski JF Jr, Opperman HC, Vawter GF. Bronchopul-monary dysplasia: a morphometric study with emphasis onthe pulmonary vasculature. Pediatr Pathol 1984;2:469-87.
28 Haworth SG, Hall SM, Patel M. Peripheral pulmonary vascu-lar and airway abnormalities in adolescents with rheumaticmitral stenosis. Int J Cardiol 1988;18:405-16.
29 Pinney MA, Cotton EK. Home management of bronchopul-monary dysplasia. Pediatrics 1976;58:856-9.
30 Campbell AN, Zarfm Y, Groenveld M, Bryan MH. Low flowtherapy in infants. Arch Dis Child 1983;58:795-8.
31 Boat TH, Kleinerman JI, Fanarff AA, Matthews LW. Toxiceffects of oxygen on cultured human neonatal respiratoryepithelium. Pediatr Res 1973;7:607-15.
32 Nunn JF. Oxygen - friend and foe. J R Soc Med 1985;78:618-22.
on 10 July 2019 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.7.739 on 1 July 1990. Dow
nloaded from