Embed Size (px)
Citation preview
Surgical Oncology
Liver and Pancreas Surgery
Bernardo Franssen M.D.
Changes in Management of Select Cancer Scenarios
Disclosures
• No conflict of interest
• Nothing to disclose
Specialist and SubspecialistDifferent point of view
Surgeon Oncologist
Radiation Oncologist
Anesthesiologist
Primary Care
Whole – Environment – Family
* Multidisciplinary Conferences
Overview
• Three topics where the management paradigm has shifted since most of us trained.
1) Pancreas Cancer treatment strategy
2) Metastatic Colorectal Cancer to Liver
3) Minimally Invasive Surgery – Specifically of the Liver and Pancreas.
Goals
• Be part of a comprehensive team that provides great care and gives hope to patients
• Identify patients who might benefit from these evolving strategies
• Timely referral to a specialist (or several): multidisciplinary approach
Pancreatic Cancer
Quick Overview
• Ductal adenocarcinoma
• 55,000 new cases/yr USA
• Mets to LN, liver, peritoneum, lung are common
• Only 15-20% are resectable at time of presentation
• Surgery prerequisite for cure
Quick Overview
• 20% of the unresectable cases are locally advanced at presentation.
- arteries are involved (SMA, celiac artery)
- other organs (stomach, aorta, vena cava)
• Borderline resectable: < 50% of an artery is abutted, or a vein is taken or abutted.
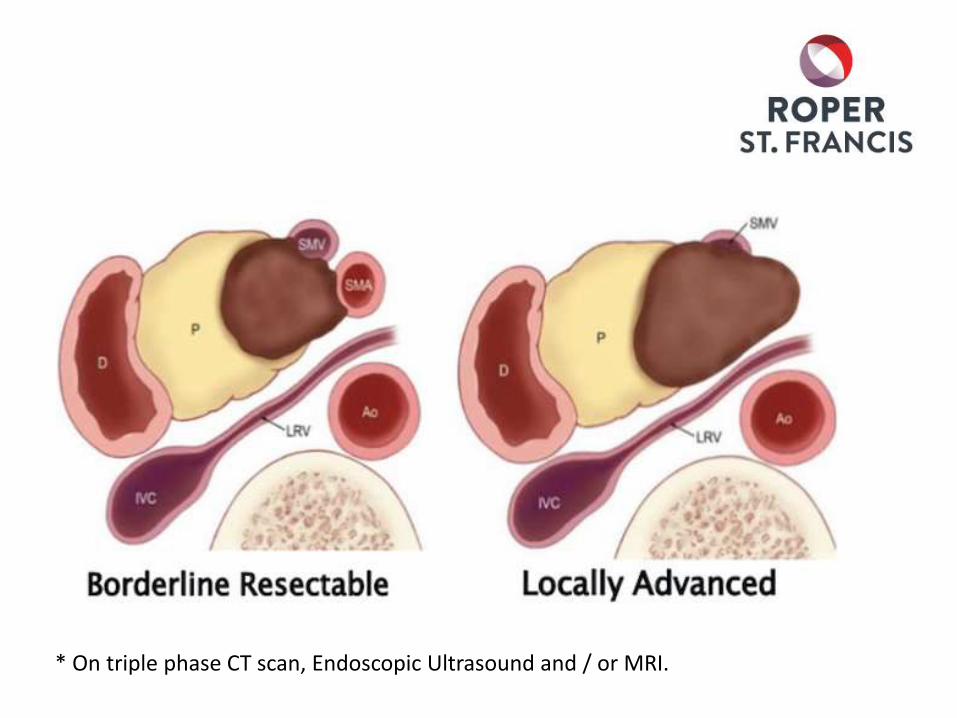
* On triple phase CT scan, Endoscopic Ultrasound and / or MRI.
Classic Clinical Scenario
• 67 M smoker
- Worsening diabetes (2 months)
- 15 pound weight-loss and loss of appetite.
- Painless Jaundice
CA-19-9: 405, expected alterations in LFT’s, rest of labs are normal
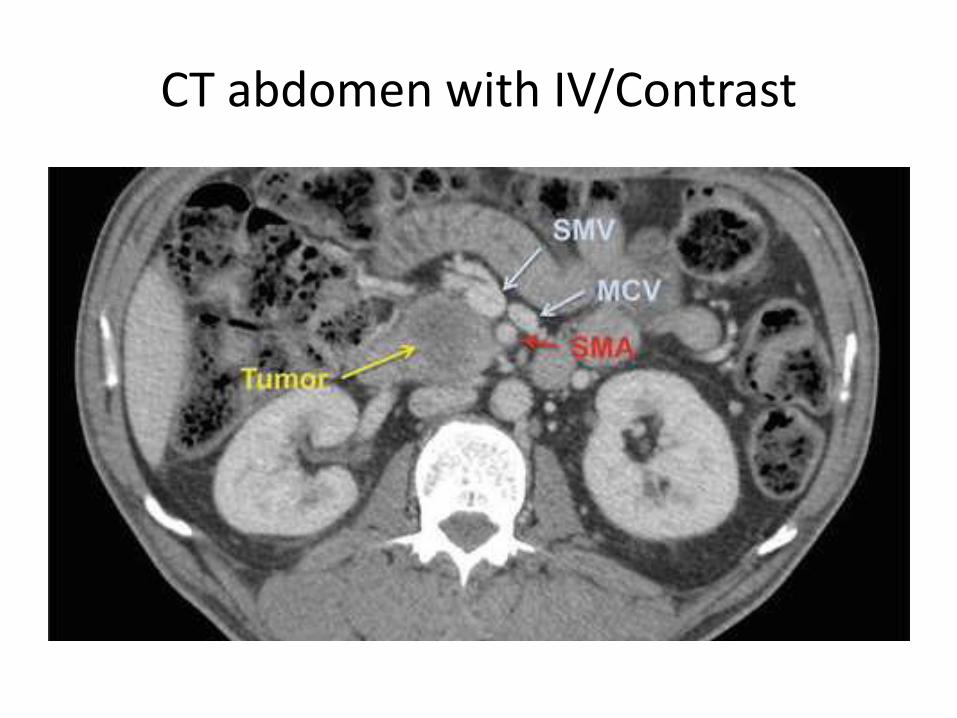
CT abdomen with IV/Contrast
What we used to do
• If good functional status:
Resection ASAP!
• Otherwise: Palliative Gemcitabine
What were the outcomes of surgery?
• 20-30 % aborted surgeries due to peritoneal or liver mets
• Another 20% Unresectable
• High rate of marcoscopic and microscopic positive margins ( as high as 60%)
• Early recurrence (R1,R2)
• Many patients never got adjuvant chemotherapy after surgery. Specially if complications
Foundation for Neoadjuvant Therapy
• Newer more effective regimens
• Response rates: in the 23-30% range compared to Gemcitabine 5-7%. (triple!)
• Survival doubled compared to Gemcitabine alone. (6 months to 11.3 months)
N Engl J Med. 2011;364(19):1817. N Engl J Med. 2013;369(18):1691
Neoadjuvant ProtocolsBorderline
• Why not give the chemotherapy and maybe even radiation before surgery?
• Conditions needed to proceed as per NCCN guidelines.
– Need a pathologic diagnosis (EUS guided biopsy is preferred)
– Long term (up to 6 months) biliary decompression
What's the Rationale
• Improve the selection of patients for whom resection will not offer a survival benefit
• Increase rates of margin-negative resections. Major goal of surgery!
• Early treatment of micrometastatic disease.
Current Results
• No Randomized controlled trials.
• Series proving substantial benefit
MD Anderson series:
- 160 patients
- 125 Completed neoadjuvant therapy
- 79 remained resectable after chemo or chemo-rads
- 66 were resected
- 62 had negative margins. (38% of original cohort)
- Median Survival:: 20 months. - if resected 40 months - if not resected 11 months.
- 5 year survival: 36% (In those that completed therapy)
- 27 patients remain free of disease at last check (Cured?)
Katz,et al. J Am Coll Surg. 2008;206(5):833. Epub 2008 Mar 17.
Best case scenario in pancreas cancer
✓ You never have metastases (tumor biology)
✓ Your tumor responds well to a multidrug chemo regimen (before or after surgery)
✓ You get a complete resection with negative margins (R0 resection)
✓ Your CA-19-9 normalized after treatment
>40% chance of 5 year survival and possibly cure!
Colorectal Cancer
with Liver Mets
Quick Overview
Colon Cancer: second cause of cancer death in both genders
In 2014 there were 130,000 cases diagnosed
The most common site of metastasis is the liver
1/3 of patient present with liver only disease.
Classic Clinical Scenario
• 64 year old male
• Presents to you with several months of constipation and reduced caliber stools, weight-loss and is anemic.
• Staging CT with multiple liver lesions on the right and three on the left. No extra-hepatic disease.
Who you gonna call ?
• Oncologist, Colorectal Surgeon, Liver surgeon.
• If colonic obstruction – Colorectal surgeon first
• Otherwise Oncologist first (chemo is a given) and liver and colorectal surgeon close second.
• Timing of procedure is individualized
Liver metastasis: What we used to do
• 20 years ago: Stage IV disease =
Palliative Chemo
• Much better chemo treatments (still not great)
- 5 year OS: 10% with 1/5 sustained response
Liver metastasis: What we used to do
• 15 years…. And if we take it out? Yes but….
- Unilobar disease only
- Resection margin > 1cm
- No pulmonary mets
- Adequate liver remnant volume
- Synchronous lesions only
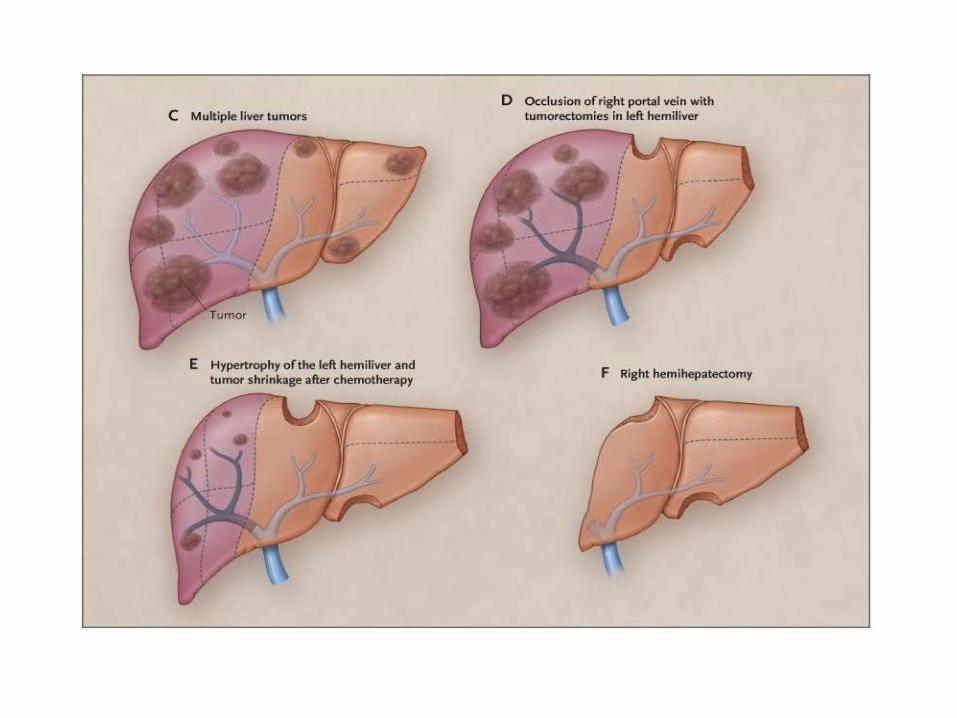
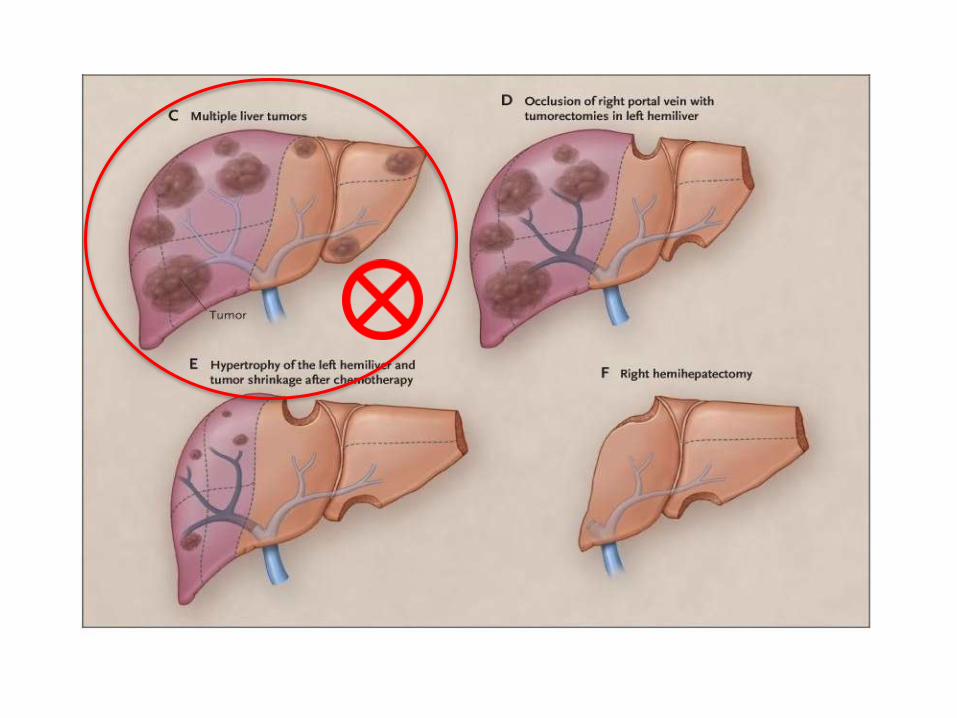
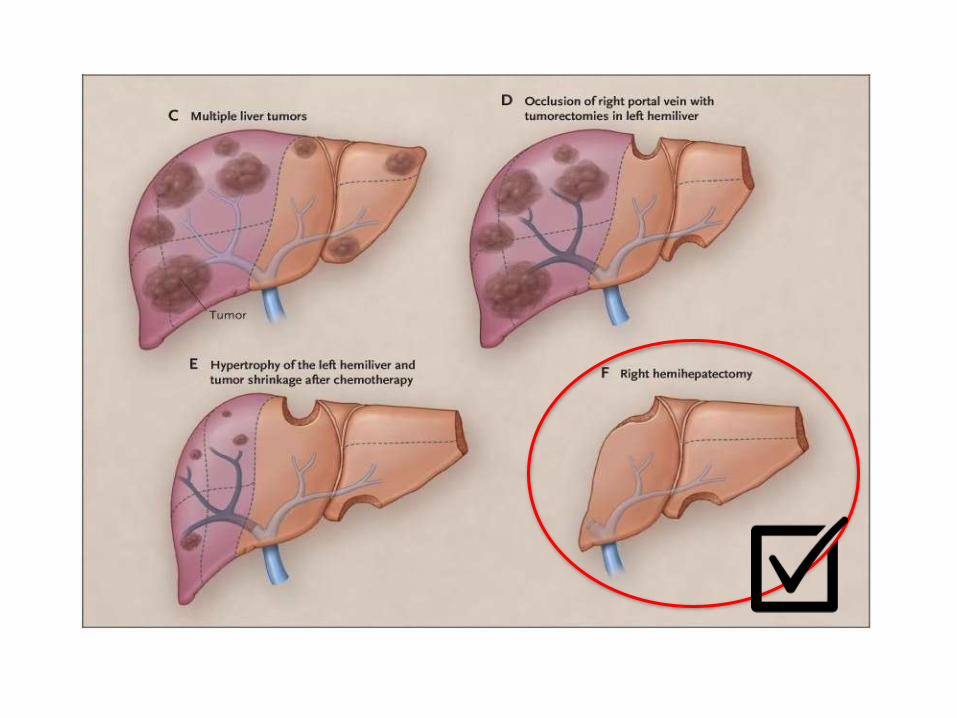
Resectability today
• Tumors that can be resected completely, leaving an adequate liver remnant.
– Can be bilobar
– Can be multiple lesions
– No size restriction
– Can be combined with Radiofrequency ablation
– Can be after liver remnant growth from Portal Vein Embolization (PVE)
– Can have lung mets (when resectable)
Outcomes
• Mortality < 5%
• Five year survival average 40% (11% with best chemo regimen) 4X!
• Well selected patients
• Adequate chemo
• Right timing
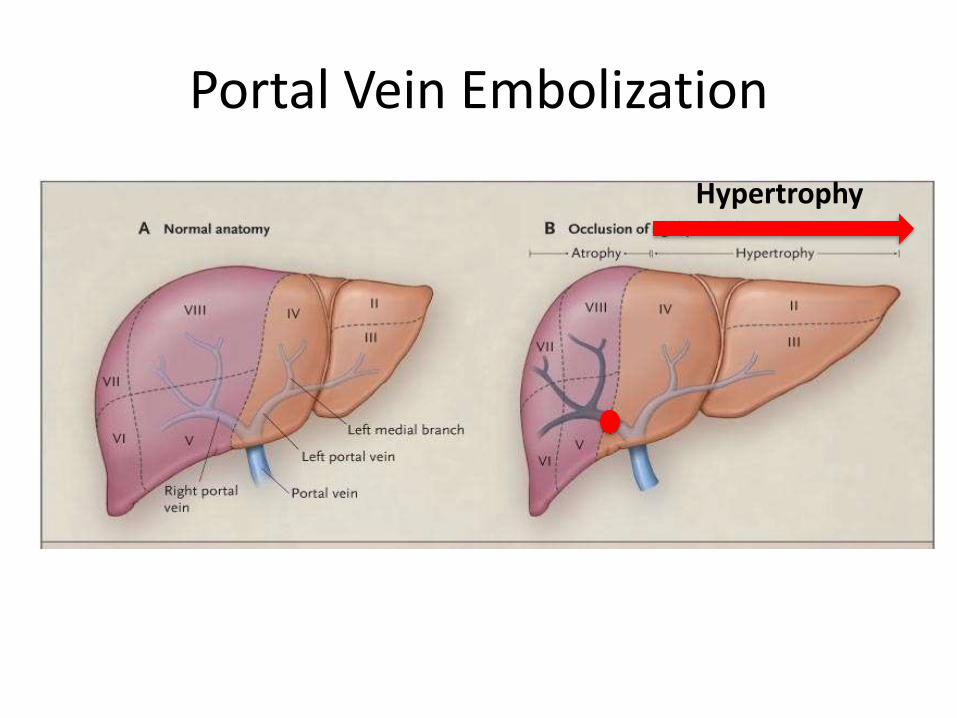
Portal Vein Embolization
Hypertrophy
Combine with otherloco-regional treatments
• Radiofrequency ablation
• Y-90: Beads of radiation injected selectively through the hepatic artery
• Maybe: Chemoembolization (TACE): Occludes arterial flow to tumor
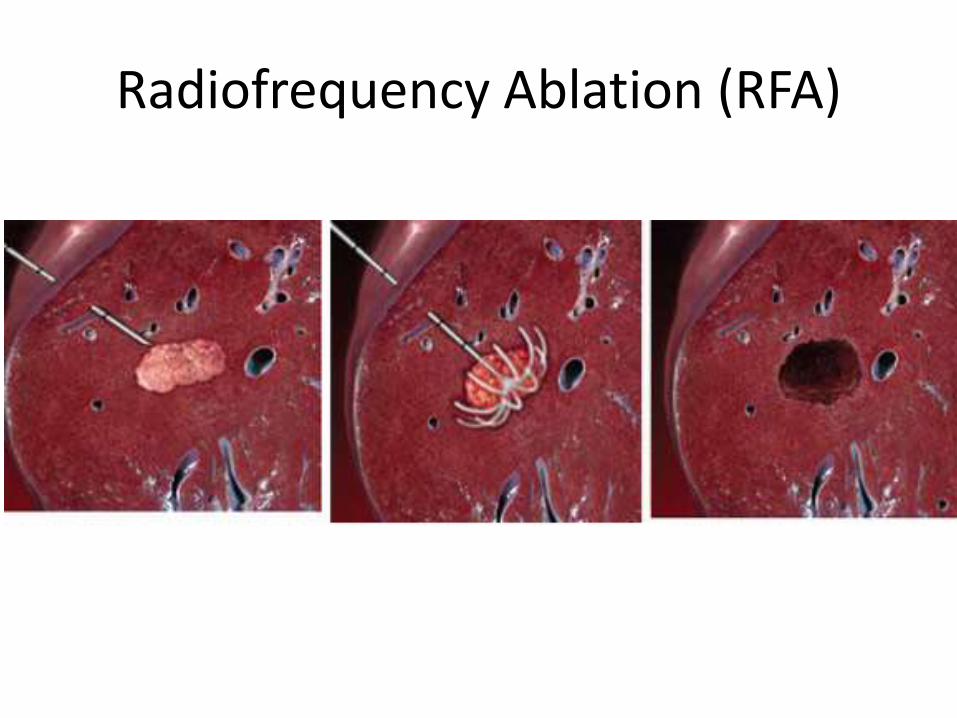
Radiofrequency Ablation (RFA)
Yttrium-90 in CRLM
• General Principles.
Aim: “selectively target all tumor in the liver with high doses of radiation regardless of the cell of origin or location yet limiting radiation of the normal liver to tolerable levels”
FDA approved in combination with chemotherapy.
- More complete response
- Same survival
Kennedy, Am J Clin Oncol 2012;35:91-99
Conclusion
• Best chance of cure with CRLM to liver is with effective chemotherapy and surgical removal .
4X more 5 year survival than chemo alone!
• Send patient to Liver Surgeon / Surgical Oncologist early for planning and best timing
MIS ≠ Specialty
The Brave
• Early 90’s
• No formal training
• Limited specialized equipment
• High conversion rate
• Resistance / Controversy
• Questionable results.
Gagner M et al. Laparoscopic partial hepatectomy for liver tumor (abstract) Surg Endosc. 1992;6:99.
Gagner M, Pomp A. Laparoscopic pylorus-preserving pancreatoduodenectomy.Surg Endosc. 1994;8:408–10
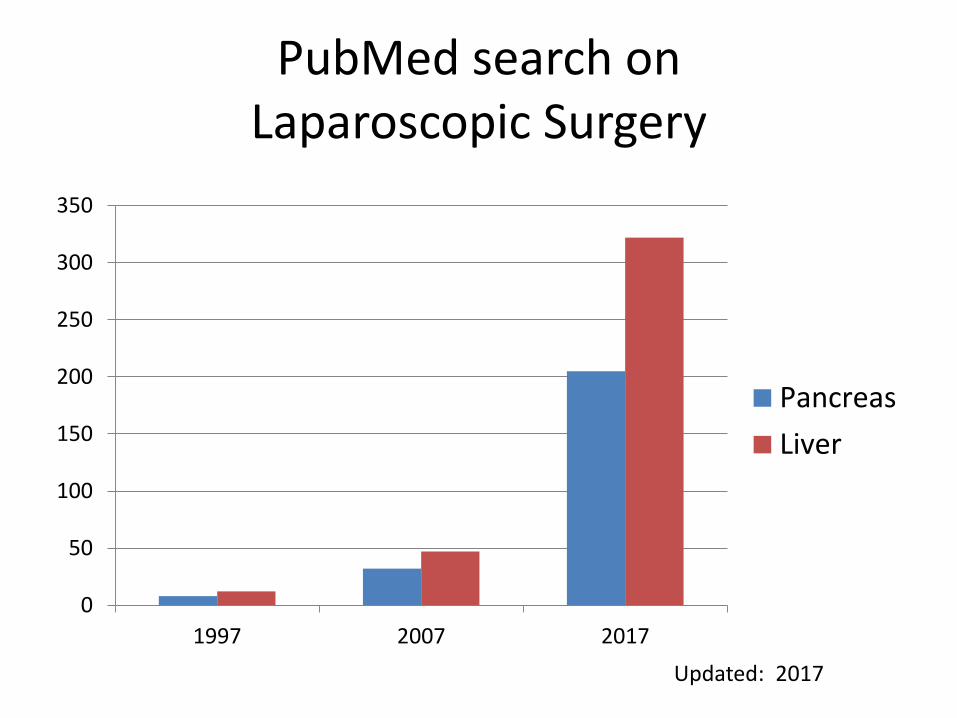
PubMed search on Laparoscopic Surgery
0
50
100
150
200
250
300
350
1997 2007 2017
Pancreas
Liver
Updated: 2017
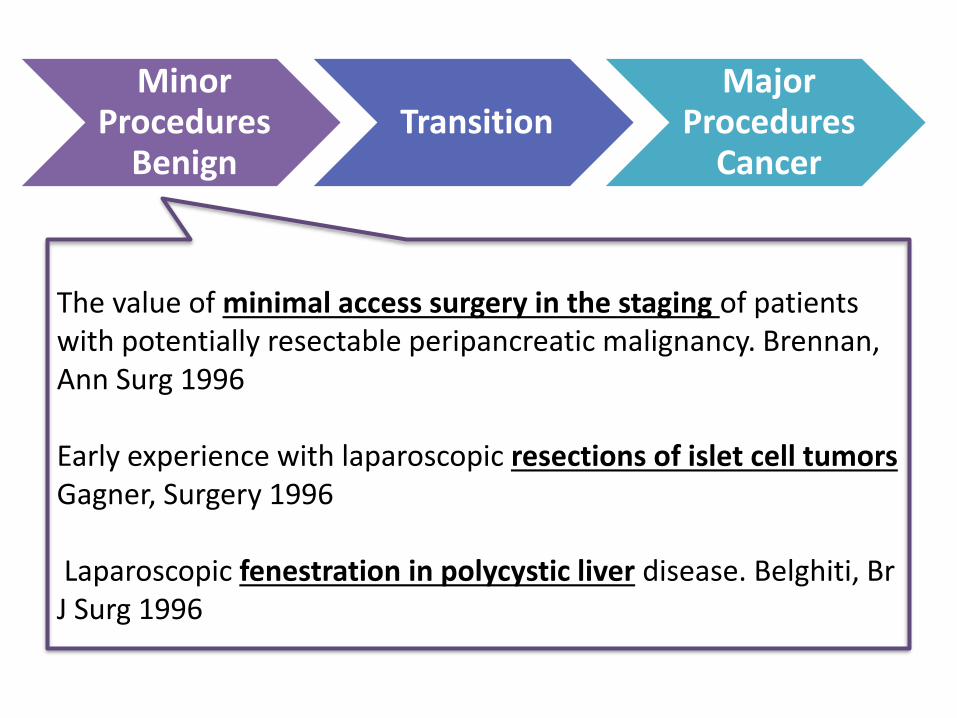
The value of minimal access surgery in the staging of patients with potentially resectable peripancreatic malignancy. Brennan, Ann Surg 1996
Early experience with laparoscopic resections of islet cell tumors Gagner, Surgery 1996
Laparoscopic fenestration in polycystic liver disease. Belghiti, Br J Surg 1996
Minor Procedures
BenignTransition
Major Procedures
Cancer
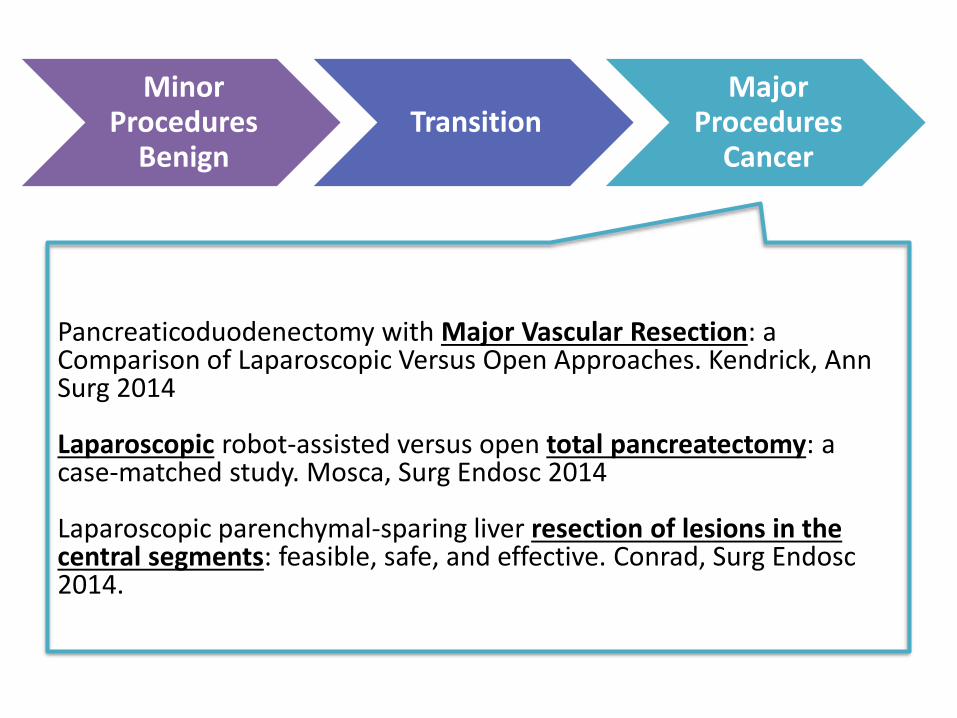
Minor Procedures
BenignTransition
Major Procedures
Cancer
Pancreaticoduodenectomy with Major Vascular Resection: a Comparison of Laparoscopic Versus Open Approaches. Kendrick, Ann Surg 2014
Laparoscopic robot-assisted versus open total pancreatectomy: a case-matched study. Mosca, Surg Endosc 2014
Laparoscopic parenchymal-sparing liver resection of lesions in the central segments: feasible, safe, and effective. Conrad, Surg Endosc2014.
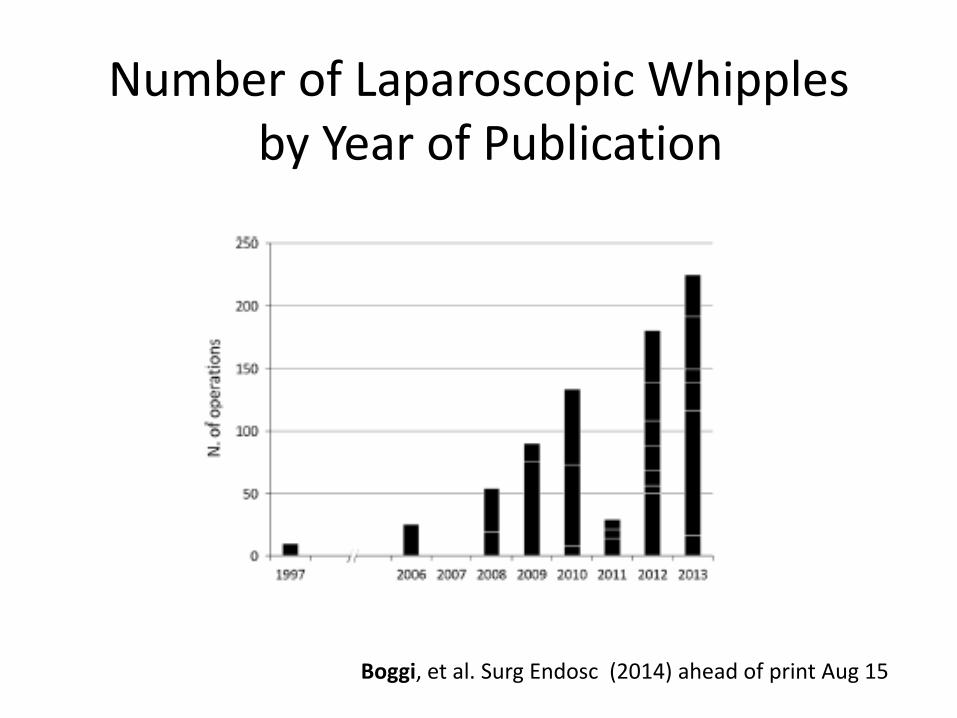
Number of Laparoscopic Whipplesby Year of Publication
Boggi, et al. Surg Endosc (2014) ahead of print Aug 15
MIS: Standard of Care in HPB
• Distal Pancreatectomy
• Lateral Sectionectomy
Mesleh, et al. J Hepatobiliary Pancreat Sci (2013) 20:578–582
Buell, et al. Ann Surg 2009;250: 825–830
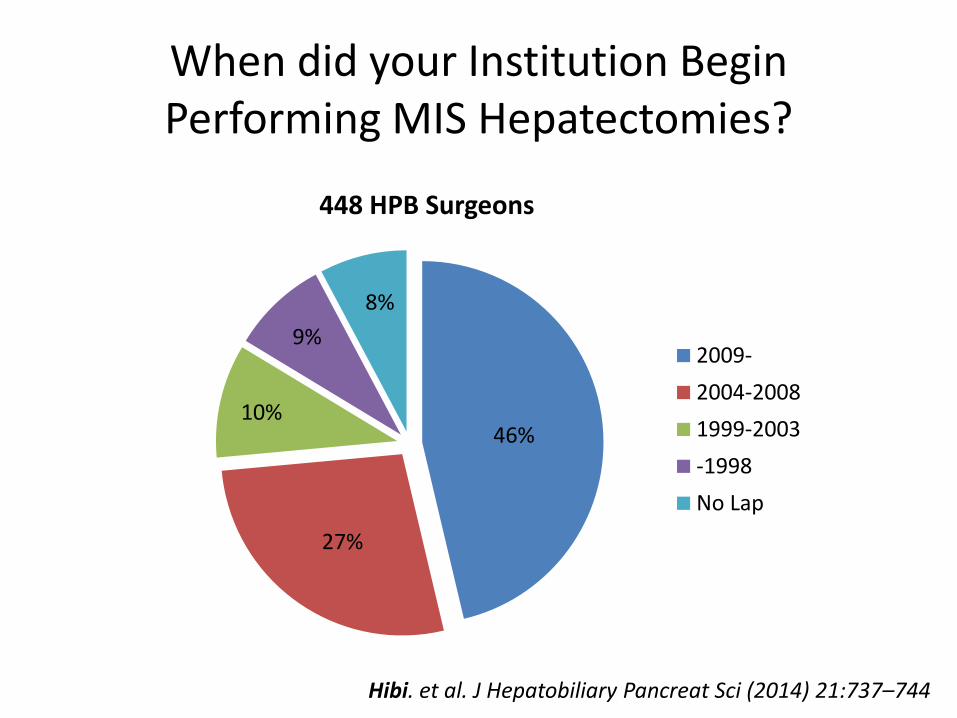
When did your Institution Begin Performing MIS Hepatectomies?
46%
27%
10%
9%
8%
448 HPB Surgeons
2009-
2004-2008
1999-2003
-1998
No Lap
Hibi. et al. J Hepatobiliary Pancreat Sci (2014) 21:737–744
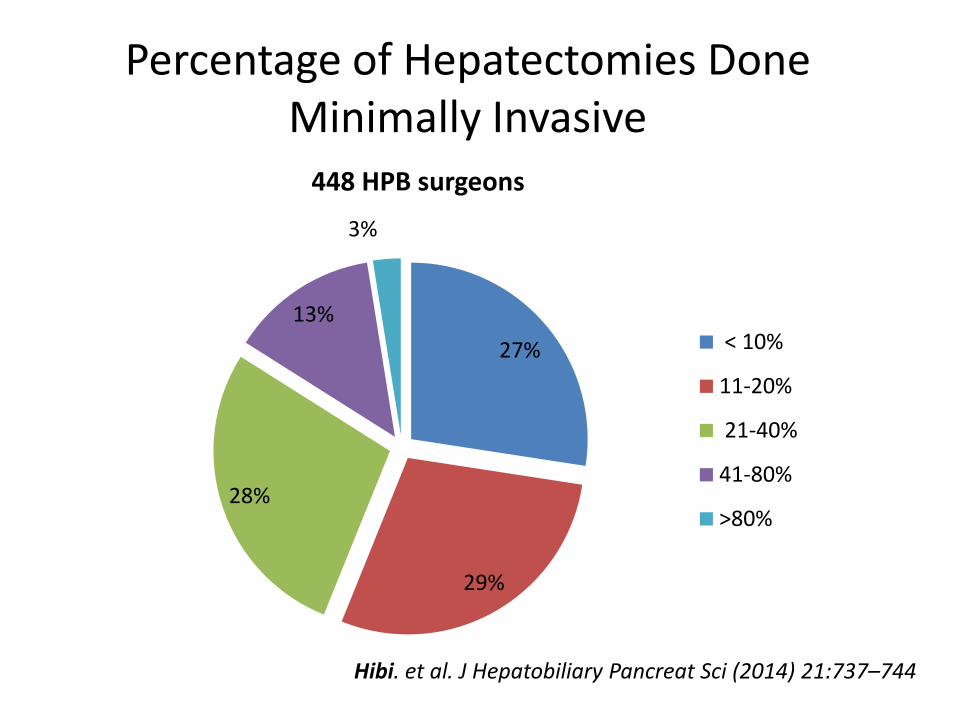
Percentage of Hepatectomies Done Minimally Invasive
27%
29%
28%
13%
3%
448 HPB surgeons
< 10%
11-20%
21-40%
41-80%
>80%
Hibi. et al. J Hepatobiliary Pancreat Sci (2014) 21:737–744
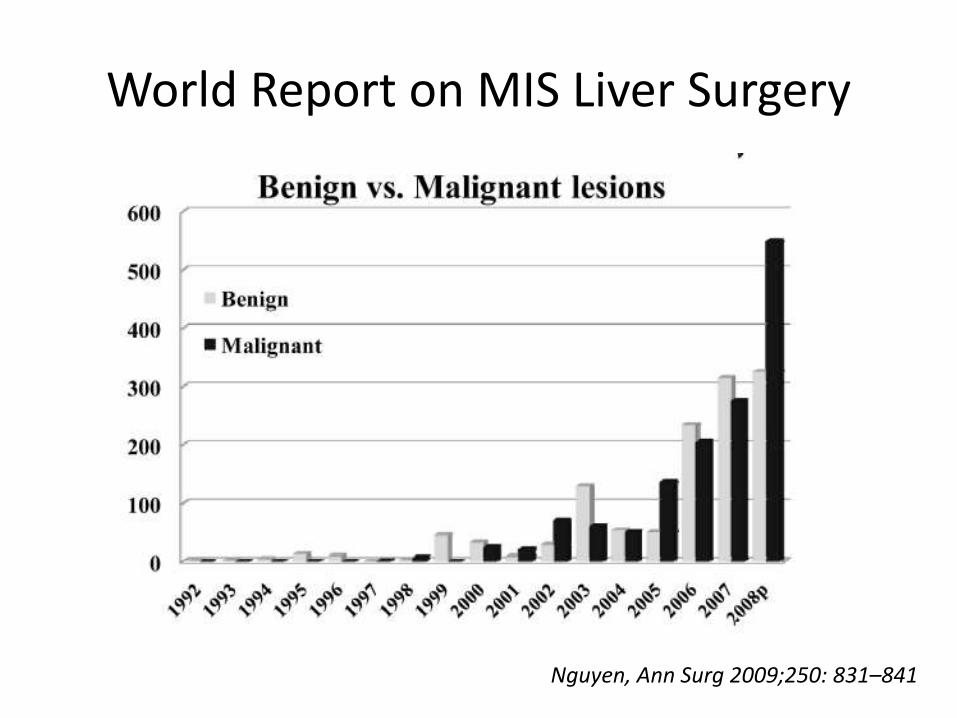
World Report on MIS Liver Surgery
Nguyen, Ann Surg 2009;250: 831–841
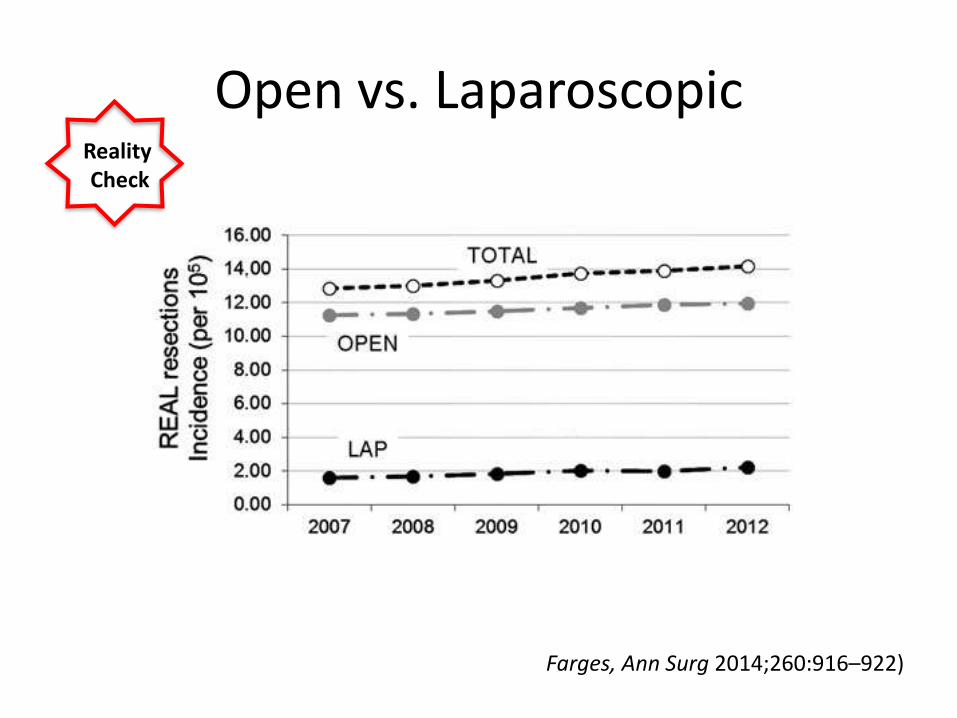
Open vs. Laparoscopic
Farges, Ann Surg 2014;260:916–922)
Reality Check
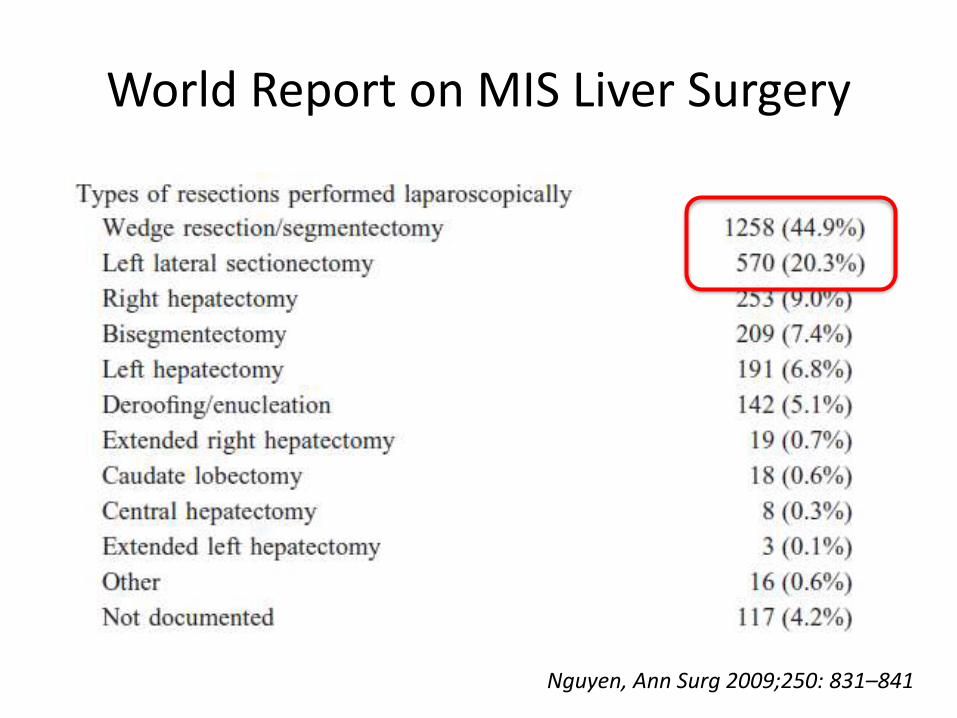
World Report on MIS Liver Surgery
Nguyen, Ann Surg 2009;250: 831–841
International Consensus2008 Louisville
• Experience in HPB surgery and MIS essential
• Equivalent or improved outcomes for minor resection (Except VII, VIII)
• Caution for major resections or posterior resections
• Laparoscopy as the standard for lateral sectionectomy
Buell, Ann Surg 2009;250: 825–830
International Consensus
2014 Morioka
• Equivalent or improved outcomes in both major and minor resections. (Publication bias, low level of evidence)
• Lateral Approach for posterior tumors
• Caution for major resection although feasible.
Wakabayashi, Ann Surg 2015;261:619–629
Laparoscopic Liver Surgery
Advantages
- CO2 Pneumoperitoneum likely reduces venous bleeding
- Visualization and reach through the caudal approach
Disadvantages
- Loss of tactile sensation
- Restricted capacity to manage bleeding.
- Need for specialized equipment
Wakabayashi, Ann Surg 2015;261:619–629
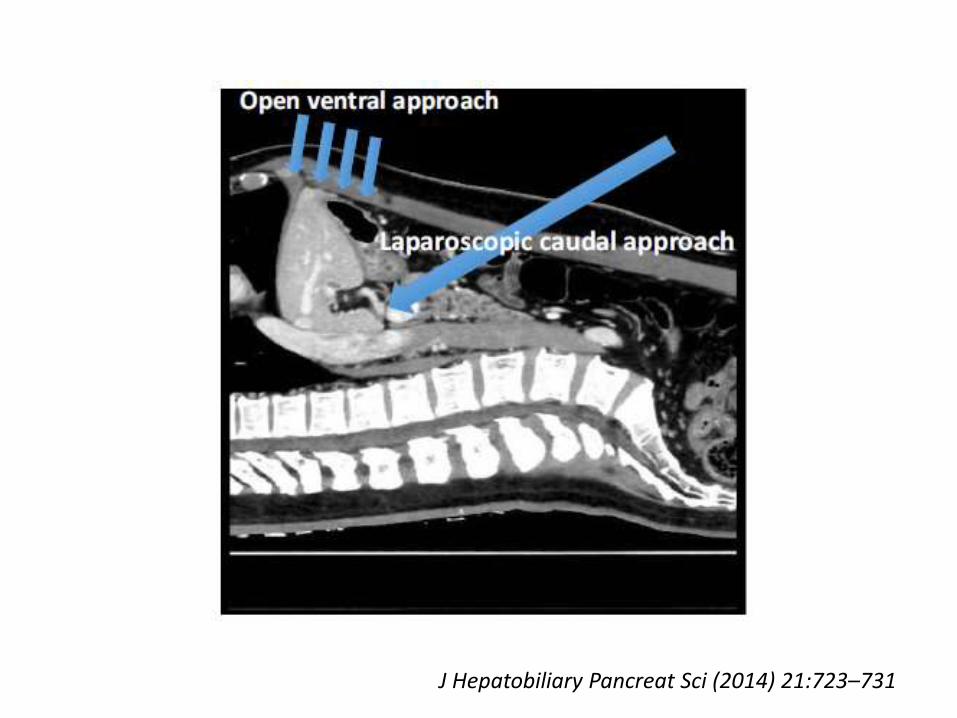
J Hepatobiliary Pancreat Sci (2014) 21:723–731
Technology Driven Operation
Mbah, et al. HPB 2012, 14, 126–131
• Staplers • US • Indocyanine injection / Infra-red light• Sophisticated 3D imaging assessment
• Transection devices– Clamp Crushing – Ultrasonic Dissection, Water Jet, Harmonic Scalpel,
Ligasure, Tissue-Link, Radiofrequency-assisted liver transection.
• Surgeons Choice
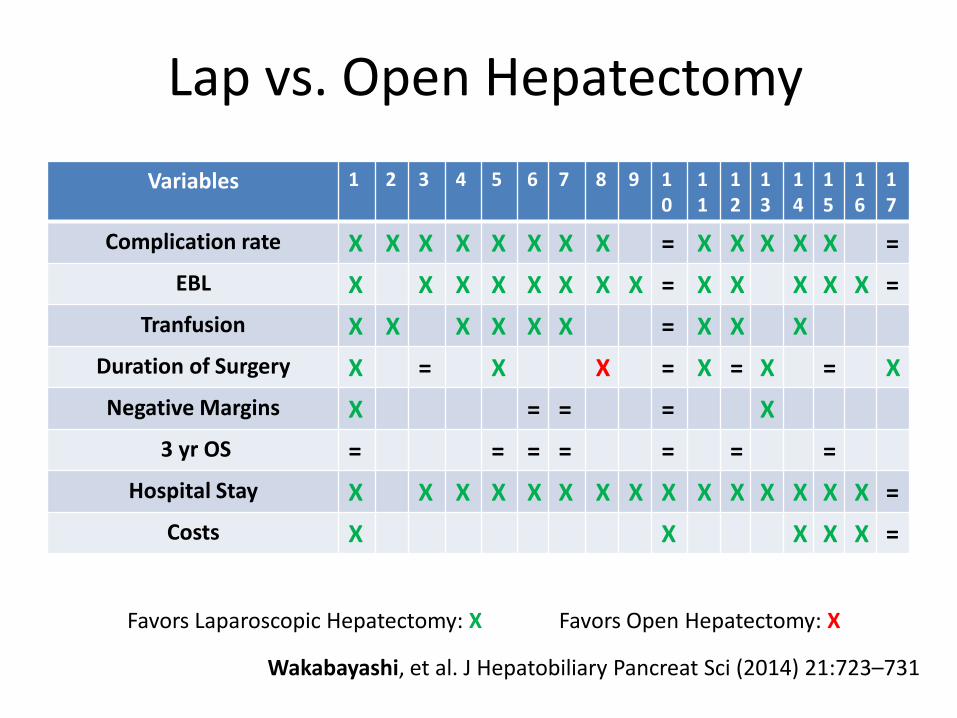
Lap vs. Open Hepatectomy
Variables 1 2 3 4 5 6 7 8 9 10
11
12
13
14
15
16
17
Complication rate X X X X X X X X = X X X X X =
EBL X X X X X X X X = X X X X X =
Tranfusion X X X X X X = X X X
Duration of Surgery X = X X = X = X = X
Negative Margins X = = = X
3 yr OS = = = = = = =
Hospital Stay X X X X X X X X X X X X X X X =
Costs X X X X X =
Wakabayashi, et al. J Hepatobiliary Pancreat Sci (2014) 21:723–731
Favors Laparoscopic Hepatectomy: X Favors Open Hepatectomy: X
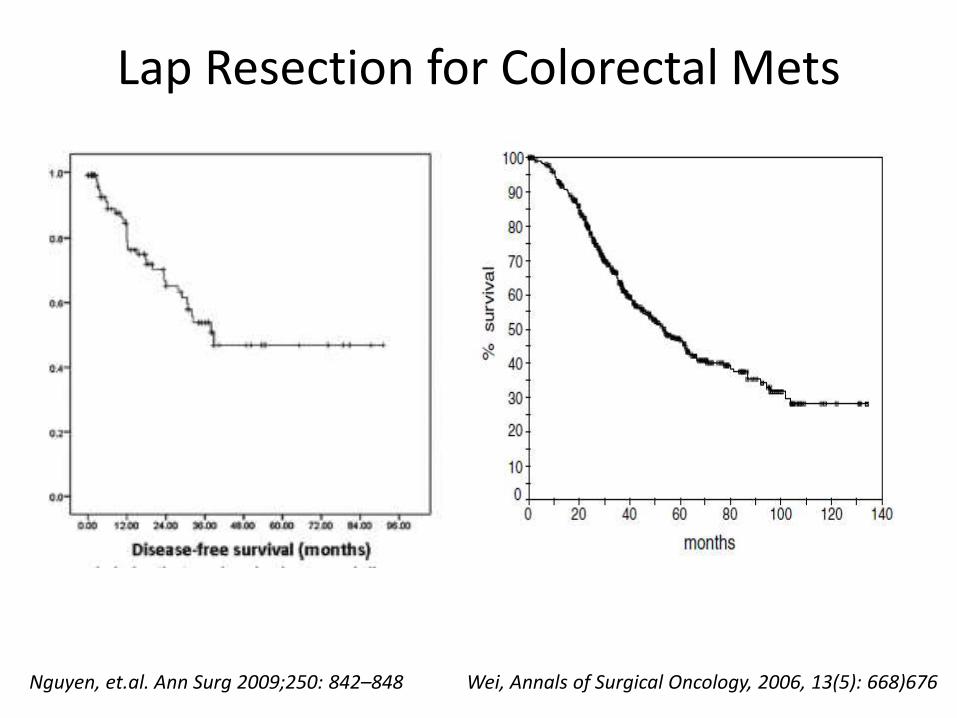
Lap Resection for Colorectal Mets
Nguyen, et.al. Ann Surg 2009;250: 842–848 Wei, Annals of Surgical Oncology, 2006, 13(5): 668)676
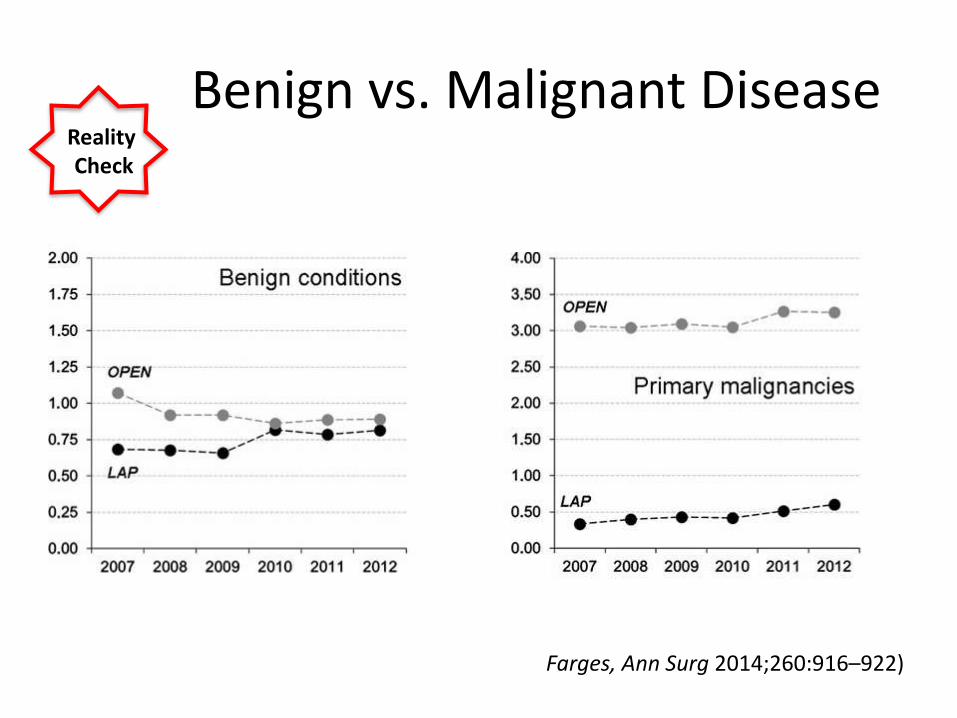
Benign vs. Malignant Disease
Farges, Ann Surg 2014;260:916–922)
Reality Check
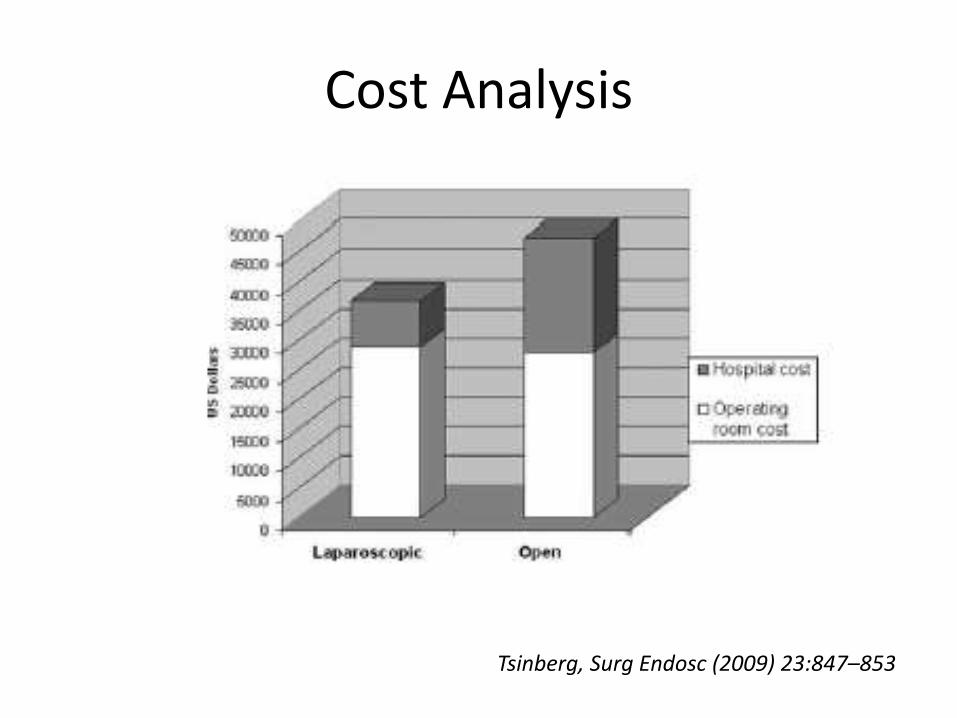
Cost Analysis
Tsinberg, Surg Endosc (2009) 23:847–853
Conclusion
Minimally Invasive Liver Surgery
• Its feasible and safe in expert hands
• Offers clear advantages: EBL, Hospital stay, Minor Complications.
• Equivalent oncologic results and costs
• Major Resections should only be performed by experts in specialized centers
• Lacking level I evidence
Thank you!




























