Embed Size (px)
Citation preview

CHAMPCHAMPChronic WoundsChronic Wounds
Miriam B. Rodin, MD, PhD, CMDMiriam B. Rodin, MD, PhD, CMD
University of ChicagoUniversity of Chicago

Learning objectivesLearning objectives
• Perform a competent bedside physical Perform a competent bedside physical examination for discovery and diagnosis of examination for discovery and diagnosis of woundswounds
• Incorporate knowledge of pathophysiology Incorporate knowledge of pathophysiology and wound healing into diagnostic and and wound healing into diagnostic and therapeutic assessmentstherapeutic assessments
• Appreciate the magnitude of the cost and Appreciate the magnitude of the cost and care burden of chronic woundscare burden of chronic wounds
• Incorporate evidence-based knowledge for Incorporate evidence-based knowledge for primary prevention and clinical management primary prevention and clinical management of woundsof wounds

Assess Learner’s OutcomeAssess Learner’s Outcome
• Attitudinal Attitudinal
– Believes that chronic wound care is an internal medicine Believes that chronic wound care is an internal medicine competencycompetency
• BehavioralBehavioral
– Performs wound evaluation at bedside on teaching Performs wound evaluation at bedside on teaching roundsrounds
– Puts wound care in the problem list and management Puts wound care in the problem list and management planplan
– Assists team to formulate an effective plan of care, Assists team to formulate an effective plan of care, including prognosis for healingincluding prognosis for healing
• Cognitive Cognitive
– Recognizes inappropriate, harmful or ineffective wound Recognizes inappropriate, harmful or ineffective wound managementmanagement

OutlineOutline
• Scope of the problemScope of the problem• PathophysiologyPathophysiology• Differential diagnosisDifferential diagnosis• ManagementManagement• PreventionPrevention• Geropardy: Name That WoundGeropardy: Name That Wound

Most pressure ulcers (PU) begin in acute care Most pressure ulcers (PU) begin in acute care hospitals.hospitals.
• Estimates of the scope of the problem Estimates of the scope of the problem flawed by methodological barriersflawed by methodological barriers
– Incomplete ascertainment Incomplete ascertainment – Confusion of incidence and prevalenceConfusion of incidence and prevalence– Incomparable study designsIncomparable study designs– Local institutional/population variabilityLocal institutional/population variability
• CMS guidelines define PU a reportable CMS guidelines define PU a reportable hospitalhospital patient safety event; quality patient safety event; quality indicator.indicator.

• Incidence 2.7% - 29.5%Incidence 2.7% - 29.5%• Prevalence 4% - 69% per bed-day Prevalence 4% - 69% per bed-day
or 3.5% - 29.5% per patient per bed-or 3.5% - 29.5% per patient per bed-dayday
• High risk patients:High risk patients:– QuadriplegicsQuadriplegics– NeurosurgeryNeurosurgery– Orthopedic..post-op hips..up to 66%Orthopedic..post-op hips..up to 66%– Critical care MICU/CCU/SICU…33% - 41%Critical care MICU/CCU/SICU…33% - 41%– Prolonged anaesthesia timeProlonged anaesthesia time– Debilitated AND age > 70Debilitated AND age > 70

Scope of the ProblemScope of the Problem
• Chronic wound care products: a $14B Chronic wound care products: a $14B industry.industry.
• Ischemic and diabetic leg ulcers are Ischemic and diabetic leg ulcers are the leading indication for the leading indication for revascularization and amputation. revascularization and amputation.
• Litigation against nursing homes: #1 Litigation against nursing homes: #1 Falls #2 Pressure ulcers. Largest Falls #2 Pressure ulcers. Largest settlements for PU (FL $92m, TX settlements for PU (FL $92m, TX $300m) and recently, hospitals.$300m) and recently, hospitals.

Human cost easier to Human cost easier to appreciateappreciate
• PainPain• AmputationAmputation• DisablementDisablement• Social costs (disfigurement, odors, Social costs (disfigurement, odors,
institutionalization)institutionalization)• Risk managementRisk management

OutlineOutline
• Scope of the problemScope of the problem• PathophysiologyPathophysiology• Differential diagnosisDifferential diagnosis• ManagementManagement• PreventionPrevention• Geropardy: Name That WoundGeropardy: Name That Wound

Site of the injurySite of the injury
Capillary closing pressure 32 mm/Hg
Venule closing pressure 6mm/Hg

Common pathway Common pathway Tissue ischemia and cell death due toTissue ischemia and cell death due to
• Extrinsic pressure >>Extrinsic pressure >>Pressure (Decubitus) Pressure (Decubitus) UlcerUlcer– Capillary closing pressure <30mm/Hg x 15 minCapillary closing pressure <30mm/Hg x 15 min
• Stasis >> Stasis >> Ulceration or DermatitisUlceration or Dermatitis– Obstructed outflow (Obstructed outflow (venous insufficiencyvenous insufficiency))– Obstructed clearance of extracellar fluid and debris Obstructed clearance of extracellar fluid and debris
((lymphatic insufficiency, sclerosislymphatic insufficiency, sclerosis))
• Arterial occlusive diseaseArterial occlusive disease– Tissue hypoxia Tissue hypoxia – Acute TE in small or terminal arteriolesAcute TE in small or terminal arterioles gangrene gangrene– Chronic PAD medium and large vesselsChronic PAD medium and large vessels ischemic ischemic
ulcers.ulcers.

The cause of the injury explains The cause of the injury explains the chronicity of the injurythe chronicity of the injury
• Increased duration of extrinsic pressure:Increased duration of extrinsic pressure:– Debilitated patients do not spontaneously Debilitated patients do not spontaneously
adjust position: neuropathy, sedation, adjust position: neuropathy, sedation, restraints, weaknessrestraints, weakness
• Loss of dermal collagen and fat support of Loss of dermal collagen and fat support of microcirculationmicrocirculation
• InflammationInflammation– Poor drainage inhibits clearance of bacteria, Poor drainage inhibits clearance of bacteria,
pro-inflammatory factors, necrotic tissue pro-inflammatory factors, necrotic tissue
• Tissue hypoxiaTissue hypoxia– Poor perfusion and anemia limit delivery ofPoor perfusion and anemia limit delivery of

OutlineOutline
• Scope of the problemScope of the problem• PathophysiologyPathophysiology• Differential diagnosisDifferential diagnosis• ManagementManagement• PreventionPrevention• Geropardy: Name That WoundGeropardy: Name That Wound

Differential diagnosis Differential diagnosis directsdirects
•Choice of therapyChoice of therapy•Choice of consultationChoice of consultation•Prognostication for healingPrognostication for healing

Pressure UlcerPressure Ulcer
• The usual pressure points: sacrum, The usual pressure points: sacrum, trochanters, heels, coccyxtrochanters, heels, coccyx
• Can develop on ANY part of the body: Can develop on ANY part of the body: nostrils from nasal cannula, DHT; nostrils from nasal cannula, DHT; scalp from immobilization on scalp from immobilization on ventilatorventilator
• In joint spaces of contracted limbsIn joint spaces of contracted limbs• Where body parts “kiss” (knees, Where body parts “kiss” (knees,
buttocks)buttocks)

PRESSURE ULCERS:PRESSURE ULCERS:
– Hypoxia induced cell death releases cytosolic Hypoxia induced cell death releases cytosolic factors into the microcirculationfactors into the microcirculation
– Provokes circulating macrophages to the wound, Provokes circulating macrophages to the wound, produce PMN chemotactic, proflammatory produce PMN chemotactic, proflammatory substances, collagenases and proteases.substances, collagenases and proteases.
– Tissue bound macrophages do not produce Tissue bound macrophages do not produce tissue growth factors in the presence of these tissue growth factors in the presence of these substances.substances.
– Fibroblasts will not migrate into the wound bed; Fibroblasts will not migrate into the wound bed; cell differentiation and proliferation will not cell differentiation and proliferation will not occuroccur

PRESSURE ULCER THERAPY PRESSURE ULCER THERAPY
• Relieve pressureRelieve pressure• Remove necrotic tissueRemove necrotic tissue• Protect clean wound baseProtect clean wound base• Be alert for secondary infectionBe alert for secondary infection

Bedside ApproachBedside Approach
• Trigger: Pressure points? Risk factors? Trigger: Pressure points? Risk factors? Immobility? ICU? Post-op?Immobility? ICU? Post-op?
• Pressure ulcerPressure ulcer• Stage it: Stage it:
– InspectInspect– PalpatePalpate– Debride UNLESS IT IS A DRY HEELDebride UNLESS IT IS A DRY HEEL– Probe for depth and tunnelingProbe for depth and tunneling

StagingStaging
• Stage 0Stage 0 red, blanching “post ischemic red, blanching “post ischemic hyperemia”hyperemia”
• Stage 1Stage 1 red, non-blanching, red, non-blanching, indurated*indurated*– ……Dark-skinned patients: no erythema, blue or purple Dark-skinned patients: no erythema, blue or purple
discoloration and boggy feel on palpation discoloration and boggy feel on palpation
– *Apoptotic cells are lysing, releasing chemotactic signals *Apoptotic cells are lysing, releasing chemotactic signals into interstitium, attracting macrophages. into interstitium, attracting macrophages.
– Macrophages release collagenases, proteases and Macrophages release collagenases, proteases and additional inflammatory intermediates (TNF, IL-2, IL-6). additional inflammatory intermediates (TNF, IL-2, IL-6).
• Keratinized layer intact. Intradermal edema.Keratinized layer intact. Intradermal edema.

Staging cont’dStaging cont’d
• Stage 2Stage 2 • Cell lysis extends into the dermis, a shallow Cell lysis extends into the dermis, a shallow
crater appears. “Partial thickness.”crater appears. “Partial thickness.”• Dermal thickness varies over body surface, Dermal thickness varies over body surface,
decreases with advancing age, photoagingdecreases with advancing age, photoaging
• FULL THICKNESS WOUNDS:FULL THICKNESS WOUNDS:• Stage 3 Stage 3 Injury extends into the subdermal tissueInjury extends into the subdermal tissue
• Stage 4Stage 4 Injury extends into muscle, bone, internal Injury extends into muscle, bone, internal structures (scrotum, rectum, visible tendons)structures (scrotum, rectum, visible tendons)
• UnstageableUnstageable:: Depth of wound cannot be Depth of wound cannot be determined and is presumably 3 or 4: Eschar, determined and is presumably 3 or 4: Eschar, heels heels

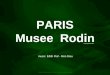
A decubitus ulcer in an elderly patient is seen on the left. A decubitus ulcer in an elderly patient is seen on the left. The ulcer is covered by fibrino-purulent exudate. The The ulcer is covered by fibrino-purulent exudate. The picture on the right shows the same wound after it has picture on the right shows the same wound after it has healed. Note the puckering scarhealed. Note the puckering scar

Stage 3 sacral PU with residual eschar,slough and secondary necrotic tissue

Stage 2 Sacral Pressure UlcerStage 2 Sacral Pressure Ulcer
Heel Unstageable, probable 4

ICEBERG principleICEBERG principle
• Pressure is distributed in a Pressure is distributed in a roughly upright cone, expanding roughly upright cone, expanding outward and down through the outward and down through the subdermal tissues:subdermal tissues:
• Eschar indicates Stage 3 or Eschar indicates Stage 3 or higherhigher
• Subcutaneous wound is larger Subcutaneous wound is larger than the visible area of escharthan the visible area of eschar

OutlineOutline
• Scope of the problemScope of the problem• PathophysiologyPathophysiology• Differential diagnosisDifferential diagnosis• ManagementManagement• PreventionPrevention• Geropardy: Name That WoundGeropardy: Name That Wound

Management of pressure Management of pressure ulcersulcers
• Explore open wound manually or with probe Explore open wound manually or with probe to determine extent of undermining and to determine extent of undermining and tunnelingtunneling
• Closed wound must be visually inspected Closed wound must be visually inspected daily for progressiondaily for progression
• Eschar: leathery black or brown covering is Eschar: leathery black or brown covering is NOT a scab NOT a scab – MUST be opened.. sharply scored and excised.* MUST be opened.. sharply scored and excised.* – Failure to do so will result in rapid wound Failure to do so will result in rapid wound
extension, anaerobic seeding and sepsis.extension, anaerobic seeding and sepsis.– *Except hard, dry eschar on heel *Except hard, dry eschar on heel

A pressure ulcer is not an A pressure ulcer is not an infection.infection.
• Foul, smelly gray and yellow gunk is what Foul, smelly gray and yellow gunk is what macrophages make while they are cleaning macrophages make while they are cleaning up dead tissue. It is NOT a sign of infection.up dead tissue. It is NOT a sign of infection.
• Signs of infection:Signs of infection:– Expanding red, warm, indurated halo around Expanding red, warm, indurated halo around
woundwound– Visible bone with disrupted periosteal membraneVisible bone with disrupted periosteal membrane– Exposed bone with surrounding granulation that Exposed bone with surrounding granulation that
will not cover the bone after 10-14 dayswill not cover the bone after 10-14 days– Deep tissue biopsy is confirmatory. Assume skin Deep tissue biopsy is confirmatory. Assume skin
flora, staph species for empiric treatment.flora, staph species for empiric treatment.
• NEVERNEVER swab a wound for culture. swab a wound for culture.

Non-healing PUNon-healing PU
• Should improve within 14 d. If not:Should improve within 14 d. If not:• Heavy “purulent” exudate: Heavy “purulent” exudate:
– gm+ colonization:gm+ colonization: absorbent dressingabsorbent dressing• Clean no exudate: Clean no exudate:
– gram-neg colonization: silvadene, other Ag+ impregnated gram-neg colonization: silvadene, other Ag+ impregnated dressingdressing
• Recurrent necrosis: Recurrent necrosis: – consider pressure ischemia: air fluidized bed (Level 3 consider pressure ischemia: air fluidized bed (Level 3
device).device).• Visible bone: Visible bone:
– Periosteum disrupted: bone bx for culturePeriosteum disrupted: bone bx for culture• Terminal ulcer: Terminal ulcer:
– multiple non-healing ulcers of various ages: (pre-death multiple non-healing ulcers of various ages: (pre-death marker, “Kennedy ulcer.” Medicare approved hospice marker, “Kennedy ulcer.” Medicare approved hospice diagnosis diagnosis

Decubitus Do’sDecubitus Do’s
StageStage 00 1 1 22 33 44Relieve pressure Relieve pressure xx x x x x xx xx
Avoid frictionAvoid friction xx x x x x xx xx
Inspect dailyInspect daily xx x x x x xx xx
Occlusive dressingsOcclusive dressings11 xx
Sharp debridementSharp debridement22 xx xx
Enzymatic debriderEnzymatic debrider33 xx xx
Moist gauze/gel packingMoist gauze/gel packing xx xx
Absorbent dressingsAbsorbent dressings44 xx xx
““Wet-to-dry” Wet-to-dry” 55
1. e.g. Hydrocolloid occlusive dressing 2. Remove eschar, soft 1. e.g. Hydrocolloid occlusive dressing 2. Remove eschar, soft debris 3. Removes adherent slough: yellow, brown, black material, debris 3. Removes adherent slough: yellow, brown, black material, e.g. collagenases enzymatic debriders 4. Removes non-adherent e.g. collagenases enzymatic debriders 4. Removes non-adherent exudate, e.g. Ca.alginate, Aquacel 5. Not recommended. exudate, e.g. Ca.alginate, Aquacel 5. Not recommended.

Common Decubitus ErrorsCommon Decubitus Errors
• Staging errors:Staging errors:– Occlusive dressing on a 3, 4 or closed unstageable: Occlusive dressing on a 3, 4 or closed unstageable:
creates anaerobic environment, prevents daily creates anaerobic environment, prevents daily inspection.inspection.
• Overly aggressive debridement:Overly aggressive debridement:– Sharply debride hard, dry eschar OR fluid-filled blister Sharply debride hard, dry eschar OR fluid-filled blister
on a heelon a heel– Recurrent trauma to a healing wound: e.g. wet-to-dryRecurrent trauma to a healing wound: e.g. wet-to-dry
• Use of –cidal agents on granulation tissue:Use of –cidal agents on granulation tissue:– Topical iodine, Dakin’s, peroxide on any clean wound.Topical iodine, Dakin’s, peroxide on any clean wound.
• Overuse of antibiotics:Overuse of antibiotics:– Creates multiply resistant organisms Creates multiply resistant organisms – Encouraged by inappropriate swab wound culturesEncouraged by inappropriate swab wound cultures– Systemic antibiotics without evidence of systemic Systemic antibiotics without evidence of systemic
infection (cellulitis, osteo, bacteremia) infection (cellulitis, osteo, bacteremia)

ISCHEMIC ULCERISCHEMIC ULCER
– Arterial occlusion prevents macrophage, Arterial occlusion prevents macrophage, fibroblast, growth factor migration to the fibroblast, growth factor migration to the wound. wound.
– Ischemic ulcer paradoxically clean and dry.Ischemic ulcer paradoxically clean and dry.– Gangrene is not an infection: Necrosis of fleshy Gangrene is not an infection: Necrosis of fleshy
soft tissue. soft tissue. – Treatment of wet vs dry gangrene: Treatment of wet vs dry gangrene:
• Wet early surgery for odors or painted with betadine Wet early surgery for odors or painted with betadine as a desiccant as a desiccant
• Dry allowed to auto-amputate.Dry allowed to auto-amputate.

Ischemic Ulcers: Ischemic Ulcers: Epidemiologic Risk FactorsEpidemiologic Risk Factors
• Classic CVD RF multiple longitudinal studies: Classic CVD RF multiple longitudinal studies: Framingham, Chicago Heart, Honolulu Heart, Framingham, Chicago Heart, Honolulu Heart, CHS, Rotterdam, WhitehallCHS, Rotterdam, Whitehall
– SmokingSmoking– HTNHTN– DMDM– Older ageOlder age– Male sexMale sex– HypercholesterolemiaHypercholesterolemia– Black raceBlack race– HHCHHC– CRPCRP– D-dimer.D-dimer.

ISCHEMIC ULCERISCHEMIC ULCER
• Approach to therapy:Approach to therapy:
• Protect at-risk watershed tissueProtect at-risk watershed tissue• Restore perfusionRestore perfusion• Manage pain Manage pain

Physical DiagnosisPhysical Diagnosis
• End arterial location, typically feetEnd arterial location, typically feet• Non-healing lower leg trauma. Non-healing lower leg trauma. • Clean (more or less), dry, no granulation Clean (more or less), dry, no granulation
tissue, edge may be heaped up.tissue, edge may be heaped up.• Signs of chronic ischemiaSigns of chronic ischemia
– Muscle wastingMuscle wasting– Cool extremitiesCool extremities– Dopplers ABI’sDopplers ABI’s– Blanching or incr pain on elevationBlanching or incr pain on elevation
• Arterial ischemic ulcerArterial ischemic ulcer

Non-healing ischemic ulcerNon-healing ischemic ulcer

GangreneGangrene

Diabetic UlcersDiabetic Ulcers
• Typically on the ball of the foot or other Typically on the ball of the foot or other weight-bearing pressure point.weight-bearing pressure point.
• Characteristic hard keratinized margin Characteristic hard keratinized margin with a small deep open center.with a small deep open center.
• Small vessel disease, neuropathySmall vessel disease, neuropathy• Debridement superficial only for Debridement superficial only for
comfort.comfort.• Probe for bone.Probe for bone.• Infection is more likely, empiric ABX Infection is more likely, empiric ABX
warranted .warranted .

Diabetic foot ulcerDiabetic foot ulcer

Stasis Ulceration and Stasis Ulceration and DermatitisDermatitis
– Pro-inflammatory cells and substances Pro-inflammatory cells and substances trapped in the tissue by venous, trapped in the tissue by venous, lymphatic incompetencelymphatic incompetence
– Back pressure impedes fibroblast and Back pressure impedes fibroblast and growth factor penetration of superficial growth factor penetration of superficial dermal layers. dermal layers.
– Unrelieved, eventually exceeds Unrelieved, eventually exceeds arteriolar, lymphatic closing pressures, arteriolar, lymphatic closing pressures, lymphatic capillaries sclerose.lymphatic capillaries sclerose.

Physical DiagnosisPhysical Diagnosis
• Lower leg circumferential or Lower leg circumferential or • Localized: perforator vein syndromeLocalized: perforator vein syndrome
– Pain improves with elevationPain improves with elevation
• Extensive: chronic edema, elephantiasis Extensive: chronic edema, elephantiasis (Milroy’s disease). (Milroy’s disease).
• Rarely extends completely through the Rarely extends completely through the dermisdermis
• Weeping. Bubbling. Secondary Weeping. Bubbling. Secondary inflammation. inflammation.
• May be visible, palpable varicosities.May be visible, palpable varicosities.

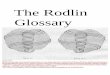
Ulceration due to rheumatoid vasculitis

Stasis Ulceration and Stasis Ulceration and DermatitisDermatitis
• Approach to therapy:Approach to therapy:• Reduce interstitial edema by Reduce interstitial edema by
compressioncompression• Clean superficial slough with Clean superficial slough with
dressings, gentle debridement e.g. 4-dressings, gentle debridement e.g. 4-layer dressing NO WET-TO-DRYlayer dressing NO WET-TO-DRY
• Treat co-existent cellulitisTreat co-existent cellulitis

Wound ConsultationWound Consultation
• Ostomy RNOstomy RN St 0-2; 3-4 after sharp debridement. St 0-2; 3-4 after sharp debridement. – Advantage: Will inspect & dress wound daily.Advantage: Will inspect & dress wound daily.
• General surgery:General surgery:– Advantage: Debride large woundsAdvantage: Debride large wounds
• Vascular surgeryVascular surgery for ischemic wounds for ischemic wounds– Advantage: Will take patient for revascularizationAdvantage: Will take patient for revascularization
• OrthoOrtho for wounds with visible bone for wounds with visible bone– Advantage: Can get bone and deep tissue biopsyAdvantage: Can get bone and deep tissue biopsy
• PlasticsPlastics if a possible candidate for flap or skin graft if a possible candidate for flap or skin graft• DermDerm for chronic stasis dermatitis, “unkowns” for chronic stasis dermatitis, “unkowns”
– Advantage: Outpatient follow up if ambulatoryAdvantage: Outpatient follow up if ambulatory• PTPT
– 4 layer & compression dressings, some sharp debridements4 layer & compression dressings, some sharp debridements– Dawn Piech 2-6891Dawn Piech 2-6891

OutlineOutline
• Scope of the problemScope of the problem• PathophysiologyPathophysiology• Differential diagnosisDifferential diagnosis• ManagementManagement• PreventionPrevention• Geropardy: Name That WoundGeropardy: Name That Wound

PreventionPrevention
• No A level recommendations No A level recommendations (ACHPR)(ACHPR)
• No A level evidence (ACHPR)No A level evidence (ACHPR)

OutlineOutline
• Scope of the problemScope of the problem• PathophysiologyPathophysiology• Differential diagnosisDifferential diagnosis• ManagementManagement• PreventionPrevention• Geropardy: Name That WoundGeropardy: Name That Wound

Hospital acquired pressure ulcer

High Transmetatarsal Amputation with pressure ulceration of protuberance

Gangrene with surrounding cellulitis

Ischemic foot ulcer

Stage 3 with surrounding cellulitis

Unstageable heel

AHCPR Clinical GuidelineAHCPR Clinical GuidelinePressure Ulcer PreventionPressure Ulcer Prevention
• A level recommendations*:A level recommendations*:– Education of staff, patient, family (content is B or C Education of staff, patient, family (content is B or C
level) level) *SEE AHCPR APPENDIX*SEE AHCPR APPENDIX
• B level recommendations:B level recommendations:– Avoid massageAvoid massage– Q 2hr repositioning in bed, q 1hr sitting (Recent Q 2hr repositioning in bed, q 1hr sitting (Recent
Swedish RCT does not support)Swedish RCT does not support)– Bed pressure reducing devices…see Lyder referenceBed pressure reducing devices…see Lyder reference
• C level recommendations:C level recommendations:– InspectInspect– Clean with mild soapClean with mild soap– Dry (absorbent, barrier)Dry (absorbent, barrier)– Body mechanics, frictionBody mechanics, friction– Nutritional supplements (macro or micro)Nutritional supplements (macro or micro)– MobilizationMobilization– Documentation Braden or Norton scoreDocumentation Braden or Norton score– Specific positioning devices, bunny boots etc.Specific positioning devices, bunny boots etc.– NO donut cushionsNO donut cushions

ReferencesReferences
1.1. Lyder CH. Pressure ulcer prevention and management. Lyder CH. Pressure ulcer prevention and management. JAMA 2003;289(2):223-6.JAMA 2003;289(2):223-6.
2.2. Perneger TV et al. Hospital-acquired pressure ulcers: risk Perneger TV et al. Hospital-acquired pressure ulcers: risk factors and use of preventive devices. Arch Internal Med factors and use of preventive devices. Arch Internal Med 1998;158 (17):1940-1945.1998;158 (17):1940-1945.
3.3. Schoonhoven L. Prospective cohort study of routine use of Schoonhoven L. Prospective cohort study of routine use of risk assessment scales for prediction of pressure ulcers. risk assessment scales for prediction of pressure ulcers. BMJ 2002;325(7368):797.BMJ 2002;325(7368):797.
4.4. Bates-Jensen BM. Quality indicators for prevention and Bates-Jensen BM. Quality indicators for prevention and management of pressure ulcers in vulnerable elders. management of pressure ulcers in vulnerable elders. Annals Internal Med 2001;135(8pt2):744-51.Annals Internal Med 2001;135(8pt2):744-51.
5.5. Lyder CH et al. Quality of care for medicare patients at Lyder CH et al. Quality of care for medicare patients at risk for pressure ulcers. Arch Internal Med. risk for pressure ulcers. Arch Internal Med. 2001;161(12):1549-54. 2001;161(12):1549-54.

AppendixAppendix
• Wound care vocabularyWound care vocabulary• AHCPR Clinical Guideline for PU AHCPR Clinical Guideline for PU
PreventionPrevention• AHCPR Clinical Guideline for PU AHCPR Clinical Guideline for PU
TreatmentTreatment

Wound vocabularyWound vocabulary
• EscharEschar ShearShear• SloughSlough ExcoriationExcoriation• GranulationGranulation GangreneGangrene• UnderminingUndermining CollagenaseCollagenase• NecroticNecrotic DebrideDebride• ColonizationColonization (Hydro)Colloid(Hydro)Colloid• CellulitisCellulitis OcclusiveOcclusive• AbcessAbcess

AHCPR Clinical GuidelineAHCPR Clinical GuidelinePressure Ulcer PreventionPressure Ulcer Prevention
• A level recommendations:A level recommendations:
– Education of staff, patient, family (content is B or C level)Education of staff, patient, family (content is B or C level)
• B level recommendations:B level recommendations:
– Avoid massageAvoid massage– Q 2hr repositioning in bed, q 1hr sitting (Recent Swedish RCT does not Q 2hr repositioning in bed, q 1hr sitting (Recent Swedish RCT does not
support)support)– Bed pressure reducing devices…see Lyder referenceBed pressure reducing devices…see Lyder reference
• C level recommendations:C level recommendations:
– InspectInspect– Clean with mild soapClean with mild soap– Dry (absorbent, barrier)Dry (absorbent, barrier)– Body mechanics, frictionBody mechanics, friction– Nutritional supplements (macro or micro)Nutritional supplements (macro or micro)– MobilizationMobilization– Documentation Braden or Norton scoreDocumentation Braden or Norton score– Specific positioning devices, bunny boots etc.Specific positioning devices, bunny boots etc.– NO donut cushionsNO donut cushions

AHCPR Clinical GuidelineAHCPR Clinical GuidelinePressure Ulcer TreatmentPressure Ulcer Treatment
• A level recommendations:A level recommendations:– Minimize bacterial colonization with recommended cleaning and Minimize bacterial colonization with recommended cleaning and
debridementdebridement– Consider a 2 wk trial of topical triple Abx or Silvadene for a Consider a 2 wk trial of topical triple Abx or Silvadene for a
clean non-healing wound or one that continues to produce think clean non-healing wound or one that continues to produce think exudate.exudate.
– Systemic Abx only for cellulitis, sepsis, osteomyelitisSystemic Abx only for cellulitis, sepsis, osteomyelitis– Assess daily for recurrent PUAssess daily for recurrent PU
• B level recommendations:B level recommendations:– Prevent malnutritionPrevent malnutrition– Avoid –cidal topical agents (povidone, betadine, Dakin’s, Avoid –cidal topical agents (povidone, betadine, Dakin’s,
peroxide)peroxide)– Irrigation with NS 4-15 psi for cleaningIrrigation with NS 4-15 psi for cleaning– Continuously moist dressing…no demonstrated difference Continuously moist dressing…no demonstrated difference
among many competing products and just NS and fluff gauze. among many competing products and just NS and fluff gauze. – NO wet-to-dry on clean wounds.NO wet-to-dry on clean wounds.– Consider nursing labor time needed for dressing planConsider nursing labor time needed for dressing plan– Trial of low voltage electro stimulant therapy for refractory Trial of low voltage electro stimulant therapy for refractory
woundswounds

AHCPR PU Guidelines AHCPR PU Guidelines Cont’d.Cont’d.
• C level recommendations:C level recommendations:– Initial standardized assessment, weekly reassessmentInitial standardized assessment, weekly reassessment– Reassess management if no healing of a clean wound within 2-4 weeksReassess management if no healing of a clean wound within 2-4 weeks– Complete H&PComplete H&P– Q 3 mo nutritional assessment, if p.o. intake is inadequate, consider TFQ 3 mo nutritional assessment, if p.o. intake is inadequate, consider TF– Vitamin and mineral supplements Vitamin and mineral supplements if deficiency confirmedif deficiency confirmed or suspected. or suspected.– Assess and manage painAssess and manage pain– Psychosocial (caregiver availability)Psychosocial (caregiver availability)– Set treatment goalsSet treatment goals– Positioning schedules, devices, Air-fluidized bed if Stage 3 or 4 non-Positioning schedules, devices, Air-fluidized bed if Stage 3 or 4 non-
healinghealing– Debride, sharp or chemical as appropriateDebride, sharp or chemical as appropriate– Moist dressingsMoist dressings– WhirlpoolWhirlpool– Loose packing of all wound cavitiesLoose packing of all wound cavities– No evidence for miscellaneous topical or systemic agents, hyperbaric, No evidence for miscellaneous topical or systemic agents, hyperbaric,
UV, IR, zinc, Vit C or US.UV, IR, zinc, Vit C or US.– Quantitative soft and bone biopsy culture for non-healing woundsQuantitative soft and bone biopsy culture for non-healing wounds– Observe clean body substance precautions, not sterileObserve clean body substance precautions, not sterile