Embed Size (px)
DESCRIPTION
SPIE MI CAD Conference Poster presentation
Citation preview

Automated Lung Field Segmentation in CT images using Mean Shift Clustering and Geometrical Features
Automated Lung Field Segmentation in CT images using Mean Shift Clustering and Geometrical Features
Chanukya Krishna Chamaa, Sudipta Mukhopadhyaya, Prabir Kumar Biswasa, Ashis Kumar Dharaa,
Mahendra Kasuvinahally Madaiahb and Niranjan Khandelwalb
Lung field segmentation is the task of separating the lung region from other anatomical parts of the body in computed tomography (CT) scans of thorax
Automated lung field segmentation with a minimal amount of user interaction is a precondition for designing an efficient nodule and interstitial lung disease pattern detection system
Armato and Sensakovic[1] illustrated the importance of accurate segmentation as a preprocessing step in a computer aided diagnosis (CAD) system
Introduction
aDept. of Electronics & Electrical Communication Engineering, Indian Institute of Technology Kharagpur, W.B 721302, INDIA
This work has been supported by Department of Information Technology (DIT), Govt. of India. The authors are grateful to team of radiologists at PGIMER, Chandigarh, Dr. Pinakpani Bhattacharya, Quadra Medical Pvt. Ltd., Kolkata and Dr. Anup sadhu, EKO CT & MRI Scan Centre, Calcutta Medical College, Kolkata for providing chest CT data along with their radiology interpretations and Prof. R. M. Rangayyan at University of Calgary, Canada for valuable advice to our research work.
False Negative Reduction
False negatives are created due to high density abnormalities viz. consolidation, fibrosis, ground glass opacity, nodules etc
For the convex part of the lung, the convex hull is found and the MS clusters from the label map with more than 50% overlap are included to the lung region.
This operation is limited within 80% depth of the lung slice from the costal end. For this purpose, the cumulative positions inside the lung segmentation are employed as described in [3]
* If I am absent please find me at presentation no. 8670-108
[1] Armato III, S. G., and Sensakovic, W. F., “Automated lung segmentation for thoracic CT: Impact on computer-aided diagnosis,” Academic Radiology, 11(9), 1011 - 1021 (2004)[2] Lee, S. L. A., Kouzani, A. Z. and Hu, E. J., “Empirical evaluation of segmentation algorithms for lung modelling,” Proc. IEEE International Conference on Systems, Man and Cybernetics, 719 - 724 (2008)[3] Van Rikxoort, E. M., De Hoop, B., Viergever, M. A., Prokop, M., and Van Ginneken, B., “Automatic lung segmentation from thoracic computed tomography scans using a hybrid approach with error detection," Medical Physics, 36(7), 2934 - 2947 (2009)[4] Comaniciu, D., and Meer, P., “Mean shift: A robust approach toward feature space analysis," IEEE Trans. Pattern Analysis Machine Intelligence, 24(5), 603 - 619 (2002)[5] Hu, S., Hoffman, E. A., and Reinhardt, J. M., “Automatic lung segmentation for accurate quantitation of volumetric x-ray CT images,” IEEE Trans. Medical Imaging, 20(6), 490 - 498 (2001)
References
DiscussionsProposed mean shift clustering and geometric features based method is robust to high dense abnormalities viz. pleural nodules, consolidation and fibrosis and provides scope of improvement in case of severe abnormalities viz. pleural effusion, honey combing, severe fibrosis etc
Results
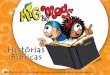
(f) (j)
(a) (b) (c) (d) (e)
(g) (h) (i)
Figure 2. Illustration of the proposed method, (a) Lung CT image, (b) Pseudo color MS label map, (c) MS segmentation, (d) Removal of objects connected to border, (e) MS segmented image with overlaid lung ROI, (f) MSR I mask, (g) convex hull of costal right lung, (h) convex hull of costal left lung, (i) MSR II mask, (j) Lung field contour (─ ─ ─ ─) and ground truth contour (─────) overlaid on input image
In case of fused lung (shown in Figure 3), fused lung separation is performed to eliminate pleura (FP’s) attaching both the lungs by iterative thresholding
The effect of lower threshold is limited to small rectangular region around vertical central line
Fused lung separation
Mean Shift Segmentation [2,4] is performed for edge preserving smoothing (with spatial bandwidth hs=5, range bandwidth hr=20 and minimum size of final output
regions M=30) to obtain an over segmented image and label map. Otsu thresholding [5] is performed on the image to create binary mask of lung.
Mean Shift Segmentation
Connected component labeling Connected component labeling (with 8-neighbours) is performed to find
number of objects present in binary mask and to calculate various features of those objects
Removal of bordering objects
Background objects (FP’s) connected to image border are removed. The result at the end of this stage will be referred as mentioned as MS result.
Detection of the objects with in lung ROI Detection of the objects with in lung ROI is performed to find the lung
objects (TP’s)
Detection of fused lung If the pleura between the two lungs are thin and low intensity, the two lungs
may be fused after the mean shift segmentation resulting FP
Figure 1. Flow of the proposed automated lung field segmentation algorithm
Figure 3. (a),(d) are Lung CT image; (b),(e) are MS Segmentation output of fused lungs and overlaid lung ROI; (c),(f) are MSR I mask
(d)
(a) (b) (c)
(e) (f)
False positive reduction In MS, FP occurs due to low intensity regions viz. bed, trachea, bronchus
and liver in the costal regions.
To eliminate the FP connected component labeling is performed on the above mask and for various objects, region features such as Eccentricity, Solidity, Area and Centroid are calculated.
Eccentricity is defined in terms of eccentricity of the ellipse that has the same second-moments as the object and is calculated as follows
where a is the length of semi-major axis and b is the length of semi- minor axis. The value of eccentricity is between 0 and 1. An ellipse whose eccentricity is
0 is a circle, while an ellipse whose eccentricity is 1 is a line segment.
Solidity is defined as the proportion of the pixels in the convex hull that are also in the object.
Solidity = (Area of the object) / (Convex area of the object)
The value of solidity is between 0 and 1. Any convex shape objects such as rectangle, circle without holes/concavities will have solidity of 1, while objects with spikes, holes and non-circular will have low solidity
Eccentricity feature (>0.9) within lung ROI is used to remove part of bed High solidity (>0.4) and small area (< 720 mm2) are used to remove trachea, bronchus, liver.
The result at the end of this stage will be referred as mentioned as MSR I (Mean shift segmentation result after FP reduction).
12
2b
ea
Figure 4. Illustration of costal lung convex hull generation. (a),(f) Lung CT image; (b),(g) MSR I segmented lung mask (c),(h) cumulative x-positions inside lung; (d),(i) costal lung; (e),(j) convex hull
(d)(a) (b) (c) (e)
(i)(f) (g) (h) (j)
The cumulative position of a point (x, y) inside a lung is defined as follows
where A is the total number of pixels in the lung, I is the lung mask which is 1 inside the lung and 0 elsewhere, and X, Y are dimensions of the image.
( , )x y
1( ) ( , )
0 0
x x I x y dx dyA
Y x
1( ) ( , )
0 0
y y I x y dx dyA
y X
Composition of Test database
Database Name Normal AbnormalSubjects Images Subjects Images
ILD Database 15 79 26 196LIDC-IDRI Database 17 54 17 100Total 32 133 43 296 Lung ROI is created using 281 images from 2 normal
subjects out of 435 images in LIDC-IDRI database which are not used for evaluation of proposed algorithm as shown in Figure 5.
Ground truth’s for quantitative evaluation of segmentation algorithms are prepared using human guided scribble based interactive segmentation tool
Figure 5. Lung ROI created from symmetric centroid map
Qualitative results of MS, MSR I, MSR II are shown in first, second and third column respectively. The segmented contour and ground truth contour are shown in green (─ ─ ─ ─) and red (─────) respectively. The results with 10 lung CT patterns corresponding to normal, excavated mass, pleural nodule, ground glass opacity (GGO) with mass, fibrosis, spicular solitary pulmonary nodule (SPN), cystic bronchiectasis, pleural effusion with septal thickening, septal thickening and fibrosis respectively are shown in (a)-(j)
Methods CategoryPerformance Metrics
MHD* (in mm) DSC** TPF*** Specificity
MS(Comaniciu et al. ‘02)
Normal 7.91 ± 7.89 0.9725 ± 0.0154 0.9759 ± 0.0134 0.9966 ± 0.0018Abnormal 10.66 ± 9.57 0.8747 ± 0.1486 0.8243 ± 0.1896 0.9955 ± 0.0047
MSR I Normal 2.91 ± 4.85 0.9833 ± 0.0288 0.9723 ± 0.0434 0.9993 ± 0.0011Abnormal 8.37 ± 8.76 0.8771 ± 0.1641 0.8158 ± 0.2037 0.9984 ± 0.0023
MSR II(Proposed method)
Normal 1.47 ± 4.31 0.9854 ± 0.0288 0.9771 ± 0.0433 0.9991 ± 0.0014
Abnormal 6.23 ± 9.00 0.8954 ± 0.1498 0.8468 ± 0.1908 0.9969 ± 0.0061
(http://kspace.cdvp.dcu.ie/public/interactive-segmentation)
Block Diagram
The flow of the proposed algorithm is shown in Figure 1. The description of each important steps are given below. *Modified Hausdorff Distance, **Dice Similarity Coefficient, ***True positive fraction
The result at the end of this stage will be referred as mentioned as MSR II (Mean shift segmentation result after FP reduction and FN reduction).
Aim of the paper
Automated lung field segmentation in CT images based on mean shift clustering and geometric features which is robust to high dense abnormalities attached to lung boundary
Lung region of interest (ROI) created from symmetric centroid map of two normal subjects, false positives (FP) reduction module (using eccentricity, solidity, area, centroid features) and false negatives (FN) reduction module (using overlap feature between clusters from MS label map and convex hull of costal lung) are used for accurate and automated segmentation.
Quantitative performance
Qualitative performance
Lu ng C Tim age
M ean shiftsegm entatio n
R em o val o fo bjects co nnectedto im age bo rder
F N redu ctio nLu ng fie ldim age
F u sedlu ngs ?
F u sed lu ngsseparatio n
F P redu ctio n
N o
Y es
C o nnectedco m po nent
labeling
D etectio n o fo bjects w ithin
lu ng R O I
Lu ng R O Iinfo rm atio n
b Dept. of Radiodiagnosis, Postgraduate Institute of Medical Education & Research, Chandigarh 160012, INDIA
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
(i)
(j)