Embed Size (px)
Citation preview

Challenging deep venous interventions: case review and
recorded cases
Prof. Nils Kucher University Hospital Bern
Switzerland [email protected]
nilskucher.com

Venous Intervention
Acute DVT treatment Catheter-directed thrombolysis
+/- Stenting
Chronic venous obstruction Endovascular reconstruction
Stenting

Venous Intervention
Acute DVT treatment Catheter-directed thrombolysis
+/- Stenting
Chronic venous obstruction Endovascular reconstruction
Stenting

Candidates for Endovascular Therapy:
Clinical & Anatomical Criteria
• Clinical criteria: Presence of the post-thrombotic syndrome – Venous claudication
– Skin changes (Varicosis, Hyperpigmentation, Lipodermatosclerosis)
– Ulcers
– Pelvic congestion symptoms
– Varicocele
– Recurrent thrombophlebitis
• Anatomical criteria: Occlusion of common femoral vein, or
Occlusion of iliac vein, or
Occlusion of inferior vena cava

Useful Tests prior to Venous Intervention
• Vein plethysmography (to verify chronic venous insufficiency)
• Exercise testing (to quantify venous claudication)
• Duplex sonography (access site femoral vs popliteal)
• MR or CT Phlebography (to quantify extent of venous occlusion)

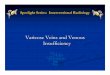
Author Nr limbs Technical success
Primary Patency % after month
Secondary Patency % after month
Nazarian et al 56 92 50 at 48m 75 at 48m
Raju et al 104 93 58 at 24m 82 at 24m
Knipp et al 58 100 38 at 60m 73 at 60m
Neglen et al 982 ns 67 at 72m 93 at 72m
Hartung et al 43 95 78 at 120m 90 at 120m
Hartung et al 46 100 86 at 42m 97 et 42m
Nazarian GK et al 1996, Radiology Raju S et al 2006, J Vasc Surg Knipp BS et al 2007, J Vasc Surg Neglen P et al 2008, J Vasc Surg Hartung et al 2008, Eur J Vsac Endovasc Surg
Studies including >40 patients
Patency after Endovascular Treatment
For Chronic Iliocaval Venous Obstructions


Iliofemoral Venous Intervention (male, 50 yrs B-F)
Infrarenal VCI occlusion
MR: chronic total occlusion of infrarenal IVC and iliac veins


Iliocaval Venous Intervention (male, 58 yrs W-U)

Iliocaval Venous Intervention (male, 58 yrs W-U)

Iliocaval Venous Intervention (male, 58 yrs W-U)

Challenge for stents to treat May Thurner (MT) syndrome
• The majority of iliofemoral DVTs are caused by iliac vein compression (May-Thurner Syndrome)
• Focal external compression and vicinity to the ilio-caval bifurcation hampers venous stenting using conventional stents.
Ideal MT stent: radial force at the compression site and flexibility to accommodate the
anatomy of the curved iliac vein.

Iliac vein anatomy: Lateral view 90 ° hip flexion
90° kinking VIC 90° kinking VIC

sinus-Obliquus® stent
Distal open cell design: • Provides flexibility and less radial force for
accomodating the curved anatomy of iliac veins during hip flexion
Proximal closed cell design: • Provides high radial force at compression site • Oblique design (35°) prevents jailing off the
contralateral iliac vein • 4 markers for correct rotational positioning

sinus-Obliquus® stent Visualized from behind

Implantation of sinus-Obliquus® stent

Implantation of sinus-Obliquus® stent

IVUS pre and post sinus-Obliquus Stenting
Pre Stenting Post Stenting
Left VIC compression (May Thurner)
sinus-Obliquus in left VIC (May Thurner) Right AIC
Right AIC

Bern Venous Stent Registry
• The Bern Venous Stent Registry is a prospective ongoing registry including >500 patients with venous stents at the University Clinic of Angiology in Bern, Switzerland
• Between December 2014 and July 2015
23 patients with common iliac vein compression were treated with sinus-Obliquus stent:® - 9 patients with acute iliofemoral thrombosis after catheter-directed thrombolysis - 10 patients with postthrombotic syndrome (PTS) - 4 patients with non-thrombotic iliac vein compression.

sinus-Obliquus® stent: Outcomes at 3 months
• Primary patency rate: 100% (23/23) • Clinical symptoms:
completely resolved in 39%, improved in 52%, unchanged in 9%
• In patients with postthrombotic Syndrome: Villalta score decreased by 4.7 ±3.5 points (P=0.002) Revised Venous Clinical Severity score (rVCSS) decreased by 2.7 ± 2.5 points (P= .007)
• No procedural complication 2 patients minor bleeding (popliteal hematoma, and hypermenorrhea)
*Stuck AK, Kunz S, Baumgartner I, Kucher N.: Short-term Patency Rates and Clinical Outcomes of Patients with Common Iliac Vein Compression Treated with a Dedicated Venous Self-expanding Oblique Hybrid Nitinol Stent; submitted 2016.

Venous Intervention
Acute DVT treatment Catheter-directed thrombolysis
+/- Stenting
Chronic DVT treatment (PTS) Endovascular reconstruction
Stenting
[email protected] nilskucher.com

Challenging deep venous interventions: case review and
recorded cases
Prof. Nils Kucher University Hospital Bern
Switzerland [email protected]
nilskucher.com






![Venous Interventions Presentation [Read-Only] · Oct;4(4):333-7 Axillary-subclavian venous occlusion: the morbidity of a nonlethal disease. Gloviczki P, Kazmier FJ , Hollier LH](https://img.pdfslide.us/doc/110x75/5fc305dffe95af280a6d6d61/venous-interventions-presentation-read-only-oct44333-7-axillary-subclavian.jpg)