Embed Size (px)
Citation preview

Original release: April 1, 2017
COPe COurse iD:
53202-GL
last review: March 17, 2017
COPe COurse CategOry: GLAucoMA
exPiratiOn: March 16, 2020
in GlaucomaChallenging CasesManaging
The Pressure’s ON!
CE MONOGRAPH
Sponsored by
This continuing medical education activity is supported through an unrestricted educational grant from Bausch & Lomb Incorporated.
Visit http://tinyurl.com/ThePressuresOnCOPE for online testing and instant CE certificate.
Faculty
Murray Fingeret, ODBen gaDDie, OD
Administrator
Distributed with

2
learning MetHOD anD MeDiuMThis educational activity consists of a supplement and ten (10) study questions. The participant should, in order, read the learning objectives contained at the beginning of this supplement, read the supplement, answer all questions in the post test, and complete the Activity Evaluation/Credit Request form. To receive credit for this activity, please follow the instructions below in the section titled To Obtain CE Credit. This educational activity should take a maximum of 1 hour to complete.
COntent sOurCeThis continuing education (CE) activity captures content from a regional dinner meeting series.
aCtivity DesCriPtiOnDespite the variety of treatments available for glaucoma, some patients continue to have vision-threatening intraocular pressure (IOP) levels. New drugs, new fixed combinations of existing drugs, and new procedures constantly challenge the traditional treatment paradigm and are showing promise in lowering IOP and slowing disease progression by multiple mechanisms of action. The purpose of this activity is to update optometrists on the current state of the art and science for treating patients with glaucoma.
target auDienCeThis educational activity is intended for optometrists.
learning OBJeCtivesUpon completion of this activity, participants will be better able to:• Assess traditional and emerging risk factors, such as ocular perfusion pressure and cerebrospinal fluid pressure, in the global risk assessment of glaucoma• Describe the mechanism of action of current and emerging topical glaucoma therapies• Evaluate the clinical relevance of safety and efficacy data for emerging topical therapies for the treatment of glaucoma• Develop treatment plans to achieve evidence-based target IOP in patients with glaucoma
aCCreDitatiOn stateMentThis course is COPE approved for 1 hour of CE credit for optometrists.
COPE Course ID 53202-GLCOPE Course Category: GlaucomaAdministrator:
DisClOsuresMurray Fingeret, OD, had a financial agreement or affiliation during the past year with the following commercial interests in the form of Consultant/Advisory Board: Allergan; and Bausch & Lomb Incorporated.
Ben gaddie, OD, had a financial agreement or affiliation during the past year with the following commercial interests in the form of Consultant/Advisory Board: Aerie Pharmaceuticals, Inc;
Alcon; Allergan; Bausch & Lomb Incorporated; Diopsys, Inc; Marco; Reichert, Inc; TearLab Corporation; TearScience; and Zeiss.
David S. Greenfield, MD, had a financial agreement or affiliation during the past year with the following commercial interests in the form of Consultant/Advisory Board: Aerie Pharmaceuticals, Inc; Alcon; Allergan; Bausch & Lomb Incorporated; and Quark.
eDitOrial suPPOrt DisClOsuresTony Realini, MD, MPH, had a financial agreement or affiliation during the past year with the following commercial interests in the form of Consultant/Advisory Board: Alcon; Bausch & Lomb Incorporated; Inotek Pharmaceuticals Corporation; and Smith & Nephew; Contracted Research: Alcon; and F. Hoffmann-La Roche Ltd.
Diane McArdle, PhD; Cynthia Tornallyay, RD, MBA, CHCP; Kimberly Corbin, CHCP; Barbara Aubel; and Michelle Ong have no relevant commercial relationships to disclose.
DisClOsure attestatiOnThe contributing physicians listed above have attested to the following:1) that the relationships/affiliations noted will not bias or otherwise influence their involvement in this activity;2) that practice recommendations given relevant to the companies with whom they have relationships/affiliations will be supported by the best available evidence or, absent evidence, will be consistent with generally accepted medical practice; and3) that all reasonable clinical alternatives will be discussed when making practice recommendations.
PrODuCt usage in aCCOrDanCe witH laBelingPlease refer to the official prescribing information for each drug discussed in this activity for approved indications, contraindications, and warnings.
grantOr stateMentThis continuing education activity is supported through an unrestricted educational grant from Bausch & Lomb Incorporated.
tO OBtain Ce CreDitWe offer instant certificate processing and support Green CE. Please take this post test and evaluation online by going to http://tinyurl.com/ThePressuresOnCOPE. Upon passing, you will receive your certificate immediately. You must answer 7 out of 10 questions correctly in order to pass, and may take the test up to 2 times. Upon registering and successfully completing the post test, your certificate will be made available online and you can print it or file it. Please make sure you take the online post test and evaluation on a device that has printing capabilities. There are no fees for participating in and receiving CE credit for this activity. DisClaiMerThe views and opinions expressed in this educational activity are those of the faculty and do not necessarily represent the views of The State University of New York College of Optometry, MedEdicus LLC, Bausch & Lomb Incorporated, or Optometry Times. This CE activity is copyrighted to MedEdicus LLC ©2017. All rights reserved.

3
in GlaucomaChallenging CasesManaging
The Pressure’s ON! Faculty
Murray Fingeret, ODclinical ProfessorState university of New york college of OptometryNew york, New york
Ben gaDDie, ODOwner and DirectorGaddie Eye centerslouisville, Kentucky
introductionThe science of glaucoma evaluation and management is progressing. New drugs with novel mechanisms of action and promising phase 3 clinical data are poised for US Food and Drug Administration review in the near future. New risk factors to guide clinical decision-making are emerging. In this series of clinical cases, key decisions faced daily in the evaluation and management of patients with suspected or established glaucoma will be identified and discussed.
Case 1. Assessing the Need for Treatment in Ocular HypertensionFrom the Files of Murray Fingeret, OD
A 36-year-old African American male presents for a comprehensive eye examination complaining of blurred vision. His last eye examination was 2 years ago. His medical and family histories are unremarkable.
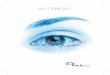
On examination, his visual acuity is 20/20 OU, with a -1.00 D spherical correction in each eye. Anterior segment examination is unremarkable. Goldmann tonometry at 9 am is 28 mm Hg in the right eye and 29 mm Hg in the left eye. Pachymetry reveals corneal thickness of 520 and 510 μm in the right and left eye, respectively. The angles are open on gonioscopy. Figure 1 shows his optic nerves, optical coherence tomography (OCT) imaging, and visual fields.
Q: What is glaucoma?Glaucoma is a difficult disease to diagnose, in part because it is difficult to define. The 2015 edition of the American Academy of Ophthalmology’s (AAO’s) Preferred Practice Pattern for Primary Open-Angle Glaucoma (POAG) defines POAG as “a chronic, progressive optic neuropathy in adults in which there is a characteristic acquired atrophy of the optic nerve and loss of retinal ganglion cells and their axons. This condition is associated with an open anterior chamber angle by gonioscopy.”1
This definition is noteworthy in several ways. First, the diagnosis of glaucoma is based solely on clinical findings; there is no laboratory test to give a positive or negative confirmation. This means that clinicians must have excellent clinical skills to detect glaucoma, and because it is typically asymptomatic until later stages, it must be looked for in every patient.
Q: How do we identify glaucoma in clinical practice?What should be looked for? What clinical skill is the most important to detect glaucoma? The optic nerve head (ONH) examination. The pathognomonic clinical finding in all forms of glaucoma is glaucomatous optic neuropathy, a nebulous term that is poorly defined and easily confused with normal anatomic variants of optic nerve appearance. The preceding definition is of little help to clinicians, hedging on precisely
Figure 1. Clinical data from the patient presented in Case 1. (A) Color optic nerve photographs. (B) Optical coherence tomography results. (C) Visual field results.Images courtesy of Murray Fingeret, OD
C
a
B

4
what they should be looking for. Describing glaucoma nerve damage as “characteristic acquired atrophy of the optic nerve”1 is only helpful if clinicians already know what they are looking for and assumes that they will know it when they see it.
Q: What does a glaucomatous optic nerve head look like?The classic finding in glaucomatous optic neuropathy is cupping of the ONH. Every ONH has 2 main components: the neuroretinal rim, which is made up of axons from retinal ganglion cells coursing through the scleral canal to form the optic nerve, and the physiologic cup, the leftover space not occupied by the neuroretinal rim. In glaucoma, the axons are lost, the rim becomes thinner, and the cup becomes enlarged over time.
On initial examination, however, whether a given cup is healthy and stable or has enlarged over time because of progressive rim loss cannot be known. Larger cups—above 0.5 or so—are more suggestive of glaucoma damage, but healthy eyes can have normal physiologic cups as large as 0.9. So how can a large cup be determined as glaucomatous or healthy?
One clue is disc size. The size of the ONH is determined by the size of the scleral canal (which is quite variable among eyes), whereas the amount of neuroretinal rim is determined by the number of retinal ganglion cells in the eye (which is fairly consistent among eyes). If the same number of axons pass through a large hole and a small hole, there will be more leftover space in the former and less in the latter. Therefore, larger-diameter ONHs tend to have larger physiologic cups, and smaller-diameter ONHs tend to have smaller physiologic cups. A moderate or large cup in a small ONH is potentially worrisome when evaluating for glaucoma. Physiologic cups tend to be round in shape, with an intact neuroretinal rim 360° around the cup. Also, in a healthy physiologic ONH, the ISNT rule often applies: the neuroretinal rim is thickest Inferiorly, then Superiorly, then Nasally, and finally Temporally. If this ISNT the case, then the ONH likely ISNT healthy.2
In addition to cupping, there are other ONH findings that suggest the diagnosis of glaucoma. One is focal rim notching. Often, in glaucoma, cupping is not concentric. The superior and inferior poles of the ONH have more axons bunched up than the nasal and temporal sectors of the ONH. These crowded regions tend to get preferentially damaged by glaucoma. As a result, the optic cup appears focally thinned in these regions. Damage to the superior or inferior neuroretinal rim typically appears as a focal notch in the rim. If both the superior and inferior rims are thinned, the cup appears vertically elongated.
Focal notching of the neuroretinal rim frequently produces another classic glaucoma sign: the nerve fiber layer bundle defect. These wedge-shaped defects can often be seen radiating from the ONH’s notched sector(s). Clinically, they are best observed under red-free illumination. Other ONH findings suggestive of glaucoma include disc hemorrhages and peripapillary atrophy of the retinal pigment epithelium (Figure 2).
Q: What role does optic nerve head imaging play in the diagnosis of glaucoma?Two forms of ONH imaging are of value in glaucoma: stereo disc photography and OCT imaging. Disc photographs capture the clinical appearance of the ONH at a moment in time—usually the baseline assessment at the time of diagnosis—to provide a basis for detecting change over time. Photographs may also provide better detection of
disc hemorrhages compared with the clinical examination.3 OCT imaging is best used to assess the status of the retinal nerve fiber layer (RNFL). Both diffuse and focal RNFL loss can be detected by OCT. Further, OCT can be helpful in distinguishing between physiologic and glaucomatous ONH cupping; a fully intact RNFL in an eye with a large round cup is suggestive of physiologic cupping. Both photography and OCT can assist in detecting progression over time. Serial ONH photographs must be manually compared, whereas serial OCT images can be automatically compared to detect changes over time.
Neither form of ONH imaging can or should replace a thorough clinical examination of the optic nerve. Universal OCT screening for glaucoma is inappropriate and will result in high rates of false-positive tests (so-called “red disease”), which generate unnecessary anxiety for patients and significant costs to the health care system for follow-up confirmatory tests that will ultimately rule out glaucoma. OCT imaging should be obtained only if the clinical examination suggests glaucoma.
Q: What role does perimetry play in the diagnosis of glaucoma?Glaucoma occurs in a continuum that begins with early axon loss that cannot be detected using current examination or testing techniques (Figure 3).4 Early glaucomatous ONH damage is typically insufficient to cause a measurable visual field defect using standard achromatic automated perimetry. Accordingly, visual field loss is not necessary to make the diagnosis of glaucoma. This is reflected in the preceding AAO definition of glaucoma, which makes no mention of visual field loss as a feature of the disease. Perimetry is useful in diagnosing and staging glaucoma. Early visual field defects generally appear with moderate ONH damage. The greater
Figure 2. Typical features of glaucomatous optic neuropathy. (A) Concentric enlargement of the cup resulting from diffuse axon loss. Note that this is easily confused with normal physiologic cupping. (B) Focal neuroretinal rim notching. (C) A nerve fiber layer bundle defect associated with a focal neuroretinal rim notch. (D) A disc hemorrhage. (E) Peripapillary atrophy of the retinal pigment epithelium.Images courtesy of Murray Fingeret, OD
a B
C D
e

5
Q: Should this patient be treated or not?There are benefits to treating this patient. If the patient has early POAG, treatment will reduce the risk of progression.7 If the patient has ocular hypertension, treatment will reduce the risk of developing POAG.8 There are also detriments to treating this patient. This patient may not have, and may never develop, POAG; thus, treatment may be unnecessary. All interventions to lower IOP, such as medications or laser or incisional surgery, have potential side effects, costs, and a negative effect on quality of life. Subjecting patients to risks without benefits should be avoided whenever possible.
With these considerations in mind, how can patients most likely to benefit from IOP-lowering therapy be identified? By identifying those at highest risk of developing visual disability from glaucoma and treating those patients preferentially. Global risk assessment in glaucoma can help identify high-risk patients. This process involves comprehensive assessment of all known and suspected risk factors for glaucoma, then synthesizing the results into an overall risk impression. Some risk factors are well established, including age, IOP, central corneal thickness, and a family history of glaucoma.1,9,10 Others are less clear, such as myopia,11 diabetes,12 and abnormalities on specialty perimeters like frequency-doubling technology13 or short-wavelength automated perimetry.14 Still others are only now emerging, and there are insufficient data to fully understand their effect on glaucoma risk. These include corneal hysteresis,15 ocular perfusion pressure (OPP),16 cerebrospinal fluid pressure,17 and obstructive sleep apnea.18
Several of these risk factors have been incorporated into a validated risk calculator developed from data collected in a pair of major clinical trials: the Ocular Hypertension Treatment Study9 and the European Glaucoma Prevention Study.19 The calculator considers the most well-established risk factors, weighs them accordingly, and generates the probability of progressing to POAG with reproducible visual field loss within 5 years.20 This tool is available without charge online at http://ohts.wustl.edu/risk/calculator.html. Expert consensus supports the following treatment guidelines based on risk level: if the risk is below 5%, observation is prudent; for a risk between 5% and 15%, the decision to treat or observe should follow an informed discussion with the patient; and for a risk in excess of 15%, treatment should be encouraged.4
Applying the risk calculator to the patient in Case 1 reveals an 18.5% probability that the patient will develop POAG within the next 5 years (Table 1). On this basis, treatment was recommended and the patient agreed.
the field loss, the more advanced the glaucoma. Perimetry is also useful in detecting progression of glaucoma over time. Simple manual review of serial fields over time will often demonstrate progression. Modern perimeters also feature advanced progression analysis software that can identify subtle changes over time and assist in differentiating between glaucomatous progression and field loss attributable to other causes, such as cataract progression.
As with ONH imaging, using perimetry to screen for glaucoma is inappropriate and ineffective. Perimetry is a subjective test and prone to false-positive results based on patient performance errors, especially on first attempts. Perimetry should be obtained only if the clinical evaluation suggests its value.
Q: What role does intraocular pressure play in the diagnosis of glaucoma?The AAO definition of glaucoma noted previously makes no mention of intraocular pressure (IOP) as a feature of the disease. Many patients with POAG do not have elevated IOP,5 and others may have elevated IOP only part of the time. Therefore, a normal IOP in no way rules out the presence of glaucoma. Conversely, the presence of elevated IOP does not mean that the patient has glaucoma. Up to 7% of healthy adults have IOP greater than 21 mm Hg and no glaucoma.5 However, population studies have demonstrated that the likelihood of glaucoma does increase with increasing IOP.5,6
The relevance of IOP to glaucoma is that IOP reduction is the only established method of reducing the risk of glaucoma progression over time. Regardless of the absolute level of IOP at the time of diagnosis, therapy should be instituted to achieve adequate IOP reduction to slow or halt the rate of progression over time.
Q: Does this patient have glaucoma?The patient described in Case 1 has elevated IOP, healthy-appearing optic nerves, normal OCT imaging of the RNFL, and an abnormal visual field in the right eye. However, this was the patient’s first visual field, and there is a learning curve for correctly performing perimetry. When the visual field was repeated, the results were normal in both eyes.
In this case, the differential diagnosis includes both ocular hypertension and early POAG, with insufficient damage for detection using standard methods (examination, perimetry, and OCT). At present, there is no easy way to differentiate between these 2 entities other than longitudinal follow-up; POAG will progress over time,7 whereas ocular hypertension will not.8
Figure 3. Glaucoma continuum covering the spectrum from early, undetectable disease to advanced disease with visual dysfunction4
Abbreviation: VF, visual field.
Reprinted from American Journal of Ophthalmology, 138, Weinreb RN, Friedman DS, Fechtner RD, et al, Risk assessment in the management of patients with ocular hypertension, 458-467, Copyright 2004, with permission from Elsevier.
unDe
teCt
aBle
Dise
ase
asyMPtOMatiC Disease
FunCtiOnal iMPairMent
FaCtOrs
Age 36 rigHt eye MeasureMents
leFt eye MeasureMents
1st 2nd 3rd 1st 2nd 3rduntreated Intraocular Pressure
(mm Hg)28 27 28 29 30 28
central corneal Thickness(μm)
520 522 516 510 505 505
Vertical cup to Disc Ratio by contour 0.45 0.45Pattern Standard DeviationHumphrey octopus loss variance (dB) (dB)
1.7 1.6 1.4 1.4
This risk assessment tool is available for use free of charge at http://ohts.wustl.edu/risk/calculator.html.
Reprinted with permission.
The patient’s estimated 5-year risk (%) of developing glaucoma in at least 1 eye18.5%
Table 1. Global Risk Assessment of the Patient Presented in Case 1

6
Case 2. Initial Therapy for Newly Diagnosed Primary Open-Angle GlaucomaFrom the Files of Murray Fingeret, OD
A 68-year-old Hispanic male with diabetes mellitus presents for an eye examination to screen for diabetic eye disease. He has no personal history of any eye problems. His family history includes a brother with open-angle glaucoma. His medical history is significant for type 2 diabetes mellitus diagnosed 10 years ago, which is well controlled with oral metformin; his recent HbA1c was 5.8%. He also has hyperlipidemia, which is controlled with simvastatin, and systemic hypertension, which is controlled with atenolol and hydrochlorothiazide.
On examination, his visual acuity is 20/20 in each eye, with a small hyperopic correction. Intraocular pressure is 17 and 16 mm Hg in the right and left eye, respectively, measured at 9 am with Goldmann tonometry. Central corneal thickness is 545 and 540 μm in the right and left eye, respectively. Gonioscopy revealed angles open to the ciliary body band in both eyes. Figure 4 shows his optic nerves, RNFL, OCT, and visual fields.
Q: What is the diagnosis?Careful inspection of the optic nerve photographs (Figure 4a) reveals thinning of the inferior neuroretinal rim in the right eye, with an associated RNFL bundle defect. A similar inferior RNFL bundle defect can be seen in the left eye. OCT imaging of the RNFL confirms thinning inferotemporally in both eyes (Figure 4B). The visual field in the right eye has a corresponding superior arcuate defect, whereas the left visual field remains essentially full. Thus, this patient has functional loss in the right eye that correlates with the structural damage evident both clinically and on OCT imaging. In the left eye, however, there is no evident visual field loss on standard automated perimetry. On the basis of these observations, the patient has POAG.
Intraocular pressure values for this patient are within the normal range. Historically, the classic findings of IOP in an eye with normal IOP would be considered normal-tension glaucoma (NTG). It is unclear, however, whether NTG is a distinct entity from POAG or simply a subset of POAG. Given that there is no pathognomonic finding other than IOP that distinguishes NTG from POAG, it is likely that they are the same disease and that POAG exists across the full spectrum of IOP.
This patient has been examined only once. Intraocular pressure is a dynamic biologic parameter and exhibits significant variation throughout the day and from day to day in both healthy and glaucomatous eyes.21,22 Unless the clinical setting necessitates urgent IOP reduction, there is value in delaying the initiation of therapy to more fully characterize IOP through multiple assessments. After initiating therapy, multiple on-therapy measurements may be necessary to fully characterize the therapeutic response to treatment.23
The patient was asked to return in 2 weeks for a repeat IOP assessment before starting therapy. At that visit, IOP was 17 mm Hg OU at 2 pm. The diagnosis of POAG with normal IOP was made. A target IOP of 13 mm Hg (25% reduction) was established.
Q: What is the best first-line therapy for this patient?The choice of therapy should consider treatment goals. The AAO Preferred Practice Pattern for POAG recommends an initial 25% IOP reduction for patients with early-to-moderate POAG, citing numerous lines of evidence that this degree of IOP lowering can slow the progression of disease.1 Other considerations when selecting therapy include safety, tolerability, convenience of dosing, and cost.
Prostaglandin analogues optimally provide the desired features of a first-line intervention. Topical beta-blockers represent an alternative medical option. Of note, topical beta-blockers have reduced efficacy in subjects on systemic beta-blockers (such as this patient), presumably because of a partial therapeutic effect from systemic administration.24 Selective laser trabeculoplasty (SLT) is an effective and safe alternative to daily medical therapy25 that minimizes issues related to side effects, daily dosing, and cost. In a retrospective analysis, SLT was shown to effectively reduce IOP and eliminate medication use in patients with ocular hypertension.26 Surgical interventions are very effective for
Figure 4. Clinical data from the patient presented in Case 2. (A) Right and left optic nerve photographs; green arrows indicate retinal nerve fiber layer bundle defects. (B) Optical coherence tomography images of the retinal nerve fiber layer. (C) Visual fields.
Images courtesy of Murray Fingeret, OD
a
B
C
SS 24-2 SS 24-2

7
instillation. Conjunctival or ocular hyperemia rates were similar between LBN (7%) and latanoprost (8.5%). A pair of phase 3 trials—APOLLO and LUNAR—compared the IOP reduction of LBN, 0.024%, with that of timolol, 0.5%, twice daily. In the APOLLO trial, LBN was superior to timolol, providing a significantly lower IOP at all 9 time points (8 am, 12 pm, and 4 pm at weeks 2, 6, and 12).33 In the LUNAR trial, LBN was found to be noninferior to timolol, lowering IOP significantly more than did timolol at 8 of the 9 time points.34 Across the 2 studies, mean IOP reduction ranged from 7.5 to 9.1 mm Hg with LBN and from 6.6 to 8.0 mm Hg with timolol. In a more recent study in Japanese subjects, LBN was shown to lower IOP by an average of 22% in eyes with low baseline IOP (mean, 19.6 ± 2.9 mm Hg before treatment).35 In an open-label extension study, LBN lowered IOP by 32% to 34%, and the mean diurnal decrease in IOP was 6.3% to 8.3% (Figure 5).36 LBN has also been shown to effectively lower IOP throughout the full 24-hour period, including at night.37 Other NO-donating molecules are in earlier stages of development, including formulations of bimatoprost38 as well as dorzolamide and brinzolamide.39
Another product in late-stage development is netarsudil mesylate, a drug that inhibits both rho-kinase and norepinephrine transporter. Inhibition of the enzyme rho-kinase results in both increased trabecular outflow and reduced episcleral venous pressure.40 Inhibition of norepinephrine transporter increases adrenergic activity, which in turn reduces the rate of aqueous production. All 3 of these actions contribute to IOP reduction. Phase 3 studies of netarsudil mesylate have produced mixed results and remain unpublished to date.41 Netarsudil is currently undergoing evaluation as a fixed combination with latanoprost.42 In a phase 2b study, the combination significantly lowered IOP compared with latanoprost or netarsudil alone (P < .0001). Hyperemia, reported as mild in severity, occurred in 40% of patients treated with netarsudil alone or in combination with latanoprost (Table 2).
Also in phase 3 evaluation is trabodenoson, an adenosine receptor agonist with high affinity and specificity for the adenosine A1 receptor. When activated, the A1 receptor lowers IOP in nonhuman primates, in part by regulating the composition of the extracellular matrix of the trabecular meshwork, resulting in increased aqueous outflow.43,44
achieving low IOP, but have a less favorable safety profile and are not typically considered for first-line therapy in early or moderate glaucoma.
In the current case, generic latanoprost was prescribed for dosing at bedtime OU. One month later, the patient returned with an IOP of 15 mm Hg OU. Intraocular pressure was rechecked 2 weeks later and was 16 mm Hg OU. The patient has suboptimally responded to prostaglandin analogue therapy.
Q: What is the next best therapeutic step?Should an additional medication be added to achieve a target IOP of 13 mm Hg? The decision to switch or add should be made on the basis of efficacy and safety. If the therapy was ineffective or poorly tolerated, it should be discontinued and alternative therapy should be implemented. If therapy was well tolerated and provided IOP reduction consistent with its known efficacy profile, it should be continued and adjunctive therapy should be added.
For patients who cannot tolerate or do not respond to a prostaglandin analogue, alternative therapies must be considered. Prostaglandin analogues have set the bar high as the gold standard first-line therapy for glaucoma, offering unrivaled efficacy and safety with convenient once-daily dosing. Topical beta-blockers can also be dosed once daily and can produce IOP reductions comparable to those of prostaglandin analogues,27 but with more contraindications, including bradycardia, heart block, and pulmonary disease.28
Also, as discussed previously, beta-blockers provide reduced efficacy in patients using systemic beta-blockers,24 such as this patient. SLT is also a reasonable option. Numerous studies have demonstrated that SLT provides IOP reduction comparable to that seen with prostaglandin analogue therapy.25,29 SLT has the added advantage of eliminating the need for daily adherence with medical therapy and has been shown to be more cost-effective than medications in a model of glaucoma.30
Q: What novel drugs are in the development pipeline?This case demonstrates a significant unmet need for medical therapies that provide equivalent or superior efficacy, safety, and dosing convenience compared with prostaglandin analogues for patients who have contraindications to, cannot tolerate, or exhibit suboptimal efficacy with prostaglandin analogues. Several promising drugs are in late-stage development and are expected to garner approval for use in the United States in the near future.
Among these is latanoprostene bunod (LBN), a nitric oxide (NO)-donating form of the latanoprost molecule. Nitric oxide plays key roles in both health and disease throughout the body, including the eye. The molecule relaxes smooth muscle, thus promoting vasodilation. Disease states in which NO is a therapeutic target include angina pectoris, pulmonary hypertension, erectile dysfunction, and, more recently, glaucoma. In the trabecular meshwork, NO activates the cyclic guanosine monophosphate signaling pathway, resulting in trabecular relaxation and increased trabecular outflow.31 Coupled with latanoprost’s effect on increasing uveoscleral outflow, LBN would be expected to provide greater IOP reduction than latanoprost alone. In the phase 2 VOYAGER trial comparing LBN in various doses with latanoprost in 413 subjects, LBN, 0.024%, once daily lowered IOP 1 to 1.5 mm Hg more than did latanoprost, 0.005%, once daily.32 The most common adverse event associated with LBN was pain upon
Figure 5. APOLLO/LUNAR open-label extension study.36 Follow-up times for APOLLO and LUNAR were 9 and 3 months, respectively.
APOLLO/LUNAR: Long-term Efficacy and Safety Open-label Extension StudyCombined number of subjects: 737Crossover from timolol to LBN allowed• Additional decrease in mean diurnal IOP: 6.3%-8.3%Mean reduction in IOP for all subjects: 32%-34% (P < .001 from baseline)Adverse events were primarily mild to moderate (> 99.5%)• Conjuctival hyperemia: 59%• Eye irritation: 4.6%• Eye pain: 3.5%
Intraocular PressureLatanoprost Netarsudil, 0.02% Fixed Combination*
N = 298 total
Baseline, mm Hg 26.0 25.4 25.1Final, mm Hg 18.4 19.1 16.5Reduction, mm Hg 7.6 6.3 8.6
* P < .0001 compared with both latanoprost alone or netarsudil alone
Table 2. Phase 2b Study of Fixed Combination Netarsudil/Latanoprost: Efficacy42

8
A topical ophthalmic formulation of trabodenoson is in clinical development for the reduction of elevated IOP in patients with ocular hypertension or POAG. In a dose-ranging phase 1/2 study, IOP reductions with the highest tested dose ranged from -4 to -7 mm Hg.45 In this study, the prevalence of conjunctival hyperemia did not increase from pretreatment baseline in any dose group. Phase 3 clinical development is under way.
Several novel delivery systems for existing glaucoma drugs are also in development. Among these are a punctal plug46 and an intraocular implant47 delivering travoprost, as well as an intraocular implant48 and a conjunctival ring49 delivering bimatoprost. Several of these products are in late-stage development, and the role of these products in current management practice patterns has yet to be established.
Case 3. Glaucoma Progression Despite Low Intraocular PressureFrom the Files of David S. Greenfield, MD
A 70-year-old white female with a 20-year history of POAG presents for a scheduled follow-up visit. She has advanced POAG and lost fixation in her right eye 10 years ago. Her current treatment regimen includes latanoprost OU at bedtime and dorzolamide OU twice daily. She reports excellent adherence to therapy. Her medical history is remarkable for migraine headache, hyperlipidemia controlled with simvastatin, and hypertension controlled with atenolol.
On examination, her visual acuity is counting fingers in the right eye and 20/40 in the left eye (due to moderate cataract). Her IOP is 13 mm Hg in the right eye and 14 mm Hg in the left eye. Of note, her pretreatment IOP level was 24 mm Hg in the right eye and 32 mm Hg in the left eye, and her IOP on therapy has never been above 15 mm Hg in the past 10 years. Her central corneal thickness in the right and left eye is 499 and 497 μm, respectively. Her angles are open on gonioscopy. Figure 6 shows the left optic nerve photograph, OCT, and visual field results that demonstrate progression.
Q: Why is this patient progressing with intraocular pressure in the low teens?When confronted with any patient with glaucoma whose disease is progressing, the first question is whether IOP has been adequately lowered from untreated baseline. In this case, the patient’s left eye IOP has been consistently reduced from 32 to 14 mm Hg, a 56% reduction. This magnitude of IOP reduction would be expected to halt, or at least dramatically slow, glaucoma progression. This is not the case, so alternative explanations must be considered.
An important consideration is whether the patient is adherent to therapy. Some patients use their medications only in the days preceding office visits, which presents a misleading appearance of adequate IOP control to the physician. The reasons for this behavior are poorly understood and likely complex. Such patients are probably unlikely to admit to such behavior, and physicians are generally unable to identify the patients who are most likely to be nonadherent.50 This patient consistently reports excellent adherence to therapy, but such behavior is difficult to verify objectively.
Central corneal thickness can contribute to artifact in the measurement of IOP by applanation tonometry. Specifically, thin corneas—which tend to be flatter and less rigid—applanate with less force than thicker corneas and can lead to underestimation of true IOP. This patient’s corneas are quite
thin—less than 500 μm—which is likely associated with a clinically relevant underestimation of IOP. Although the ocular hypotensive response to therapy appears to be adequate, her true absolute
Figure 6. Clinical data from the patient presented in Case 3. (A) Color optic nerve photograph. (B) Optical coherence tomography data showing a decline in retinal nerve fiber layer thickness over time. (C) Visual field data showing progression of visual field loss over time.
Images courtesy of David S. Greenfield, MD
C
a
B

9
IOP level may be considerably higher than the 14 mm Hg value measured with Goldmann tonometry, and a lower target IOP may be appropriate in light of her recent progression.
This patient’s IOP has consistently been 15 mm Hg or lower when measured during routine office hours, yet IOP tends to peak at night when lying down asleep. This is because IOP is higher in the supine position than in the sitting position and also because IOP tends to rise at night as part of its own circadian rhythm.51
Q: How can intraocular pressure be assessed outside office hours?Routine clinical assessment of 24-hour IOP is impractical because of a lack of safe, affordable, and user-friendly home tonometry devices. Recently, the US Food and Drug Administration approved the Triggerfish contact lens–based 24-hour IOP monitor. This device is worn like a regular contact lens and contains a strain gauge that detects changes in corneal curvature that are attributable to changes in IOP. This information is transmitted wirelessly to a receiver worn around the periocular region and is stored on a small data drive connected to the receiver by a wire. The device can record and store up to 24 hours of continuous IOP data. The contact lens has been shown to be well tolerated through 24 hours,52 but data—reported in mV and not mm Hg—are limited to relative changes in IOP curve shape and not to absolute IOP values over time. Optimal use of this device, including both patient selection and data interpretation, has not been described to date.
Q: Could the patient’s systemic hypertension be related to her glaucoma progression?Systemic blood pressure tends to dip at night.53 This can be particularly significant in patients who take blood pressure medications, especially those who dose their antihypertensive therapy in the evening before bed. The nocturnal concurrence of high IOP and low systemic blood pressure may result in a significant reduction in OPP. OPP is the difference between systemic blood pressure and IOP and represents the relative pressure of blood perfusing the eye. Numerous epidemiologic studies have demonstrated a higher prevalence of POAG in subjects with low OPP vs normal or high OPP.54-58 A role for OPP in the development of POAG is biologically plausible because low OPP indicates reduced perfusion of ocular tissues, which may contribute to hypoxia/ischemia of optic nerve tissue. Importantly, IOP is typically highest at night when systemic blood pressure is typically lowest, resulting in low OPP.53
Q: Is any additional work-up appropriate for this patient?This patient is progressing despite a 50% reduction in baseline IOP to the low teens. An additional diagnostic evaluation might be warranted. Ambulatory 24-hour blood pressure monitoring may reveal nocturnal dips. Nocturnal blood pressure dips might be mitigated by reducing the dose of systemic antihypertensive medication, using morning dosing rather than evening dosing, or having the patient ingest salty snacks (such as tomato juice or potato chips) before bed to raise blood pressure. There are no data from epidemiologic studies or trials to support salt loading in this setting. Likewise, 24-hour IOP monitoring using the Triggerfish system may reveal significant IOP elevations in the nighttime hours. Nocturnal IOP peaks may be reduced by sleeping with an extra pillow or 2 to elevate the head.59,60 Coupling 24-hour IOP and blood pressure monitoring can provide insight into circadian OPP and might reveal nocturnal dips in
OPP. OPP is potentially modifiable, most easily by adjusting antihypertensive medications to avoid periods of hypotension.
A simpler approach to 24-hour blood pressure assessment is to obtain blood pressure measurements during office-based glaucoma visits. Routine daytime blood pressure measurements in all patients is expensive, cumbersome, and may be of limited value. Selecting patients at high risk for progression (eg, patients who report a history of low blood pressure or eyes with optic disc hemorrhage) may provide a snapshot and reveal systemic hypotension, which may be more pronounced at night. These patients may benefit most from adjustment of the dose or time of administration of antihypertensive therapy by the primary care physician.
An additional consideration is the possibility that her optic nerve damage is unrelated to her glaucoma. Central nervous system lesions can mimic glaucoma and should be considered when the clinical scenario is atypical for glaucoma progression, such as this case of progression at low IOP. Neuroimaging can help identify potential lesions and should be considered in patients with other signs suggestive of central nervous system involvement, including optic disc pallor greater than cupping; visual field defects out of proportion to cupping; bitemporal, homonymous, or vertically aligned visual field defects; early loss of central visual acuity, early dyschromatopsia; or an afferent pupillary defect without asymmetric cupping.61
Q: What is the next therapeutic step for this patient?This patient is progressing by both structural and functional criteria, despite having an IOP in the low teens on 2 glaucoma medications (prostaglandin analogue and carbonic anhydrase inhibitor). Alternative likely explanations for her progression have been ruled out, and inadequately controlled glaucoma is the likely explanation. Additional IOP lowering is necessary to halt disease progression. A reasonable goal would be an additional 15% to 20% reduction in IOP (approximately 10-11 mm Hg). One therapeutic approach is to add a third topical medication, such as a beta-blocker or adrenergic agonist, to achieve the target IOP and continue close surveillance.
Other options include proceeding directly with laser trabeculoplasty or incisional surgery. Selective laser trabeculoplasty can lower IOP in patients on multidrug regimens.62 However, in patients with confirmed progression who require a very low target IOP, traditional glaucoma surgery, such as trabeculectomy or tube-shunt implantation, may be the preferred approach.63 Because this patient also has a visually significant cataract and is functionally monocular, she may be a candidate for a combined cataract and glaucoma procedure. Lastly, a new generation of minimally invasive glaucoma surgery has emerged in recent years, and these procedures may be acceptable in eyes with coexisting cataract and mild-to-moderate open-angle glaucoma. It should be noted that cataract surgery alone often lowers IOP by several points in eyes with elevated IOP.64-66
summaryGlaucoma evaluation and management are evolving. New risk factors enable better evaluation of the value of treatment in glaucoma suspects and better understanding of the complex pathophysiology of glaucoma. New treatments will soon come to market, offering novel ways to lower IOP. Each of these advances improves clinicians’ ability to ensure that their patients with glaucoma maintain their sight and preserve their quality of life.

10
1. American Academy of Ophthalmology. Preferred Practice Pattern®. Primary Open-Angle Glaucoma. San Francisco, CA: American Academy of Ophthalmology; 2015.2. Harizman N, Oliveira C, Chiang A, et al. The ISNT rule and differentiation of normal from glaucomatous eyes. Arch Ophthalmol. 2006;124(11):1579-1583.3. Budenz DL, Anderson DR, Feuer WJ, et al; Ocular Hypertension Treatment Study Group. Detection and prognostic significance of optic disc hemorrhages during the Ocular Hypertension Treatment Study. Ophthalmology. 2006;113(12):2137-2143.4. Weinreb RN, Friedman DS, Fechtner RD, et al. Risk assessment in the management of patients with ocular hypertension. Am J Ophthalmol. 2004;138(3):458-467.5. Sommer A, Tielsch JM, Katz J, et al. Relationship between intraocular pressure and primary open angle glaucoma among white and black Americans. The Baltimore Eye Survey. Arch Ophthalmol. 1991;109(8):1090-1095.6. Leske MC, Wu SY, Hennis A, Honkanen R, Nemesure B; BESs Study Group. Risk factors for incident open-angle glaucoma: the Barbados Eye Studies. Ophthalmology. 2008;115(1):85-93.7. Heijl A, Leske MC, Bengtsson B, Hyman L, Bengtsson B, Hussein M; Early Manifest Glaucoma Trial Group. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol. 2002;120(10):1268-1279.8. Kass MA, Heuer DK, Higginbotham EJ, et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120(6):701-713.9. Gordon MO, Beiser JA, Brandt JD, et al. The Ocular Hypertension Treatment Study: baseline factors that predict the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120(6):714-720.10. Tielsch JM, Katz J, Sommer A, Quigley HA, Javitt JC. Family history and risk of primary open angle glaucoma. The Baltimore Eye Survey. Arch Ophthalmol. 1994;112(1):69-73.11. Loyo-Berrios NI, Blustein JN. Primary-open glaucoma and myopia: a narrative review. WMJ. 2007;106(2):85-89, 95.12. Costa L, Cunha JP, Amado D, Pinto LA, Ferreira J. Diabetes mellitus as a risk factor in glaucoma’s physiopathology and surgical survival time: a literature review. J Curr Glaucoma Pract. 2015;9(3):81-85.13. Medeiros FA, Sample PA, Weinreb RN. Frequency doubling technology perimetry abnormalities as predictors of glaucomatous visual field loss. Am J Ophthalmol. 2004;137(5):863-871.14. Spry PG, Johnson CA, Mansberger SL, Cioffi GA. Psychophysical investigation of ganglion cell loss in early glaucoma. J Glaucoma. 2005;14(1):11-19.15. Mansouri K, Leite MT, Weinreb RN, Tafreshi A, Zangwill LM, Medeiros FA. Association between corneal biomechanical properties and glaucoma severity. Am J Ophthalmol. 2012;153(3):419-427.e1.16. Costa VP, Harris A, Anderson D, et al. Ocular perfusion pressure in glaucoma. Acta Ophthalmol. 2014;92(4):e252-e266.17. Berdahl JP, Allingham RR, Johnson DH. Cerebrospinal fluid pressure is decreased in primary open-angle glaucoma. Ophthalmology. 2008;115(5):763-768.18. Coleman AL, Kodjebacheva G. Risk factors for glaucoma needing more attention. Open Ophthalmol J. 2009;3:38-42.19. Miglior S, Pfeiffer N, Torri V, Zeyen T, Cunha-Vaz J, Adamsons I; European Glaucoma Prevention Study (EGPS) Group. Predictive factors for open-angle glaucoma among patients with ocular hypertension in the European Glaucoma Prevention Study. Ophthalmology. 2007;114(1):3-9.20. Gordon MO, Torri V, Miglior S, et al; Ocular Hypertension Treatment Study Group; European Glaucoma Prevention Study Group. Validated prediction model for the development of primary open-angle glaucoma in individuals with ocular hypertension. Ophthalmology. 2007;114(1):10-19.21. Realini T, Weinreb RN, Wisniewski S. Short-term repeatability of diurnal intraocular pressure patterns in glaucomatous individuals. Ophthalmology. 2011;118(1):47-51.22. Realini T, Weinreb RN, Wisniewski SR. Diurnal intraocular pressure patterns are not repeatable in the short term in healthy individuals. Ophthalmology. 2010;117(9):1700-1704.23. Realini T. Assessing the effectiveness of intraocular pressure-lowering therapy. Ophthalmology. 2010;117(11):2045-2046.24. Schuman JS. Effects of systemic beta-blocker therapy on the efficacy and safety of topical brimonidine and timolol. Brimonidine Study Groups 1 and 2. Ophthalmology. 2000;107(6):1171-1177.25. Katz LJ, Steinmann WC, Kabir A, Molineaux J, Wizov SS, Marcellino G; SLT/Med Study Group. Selective laser trabeculoplasty versus medical therapy as initial treatment of glaucoma: a prospective, randomized trial. J Glaucoma. 2012;21(7):460-468.26. Gandolfi SA, Ungaro N. Low power selective laser trabeculoplasty (SLT) repeated yearly as primary treatment in ocular hypertension: long term comparison with conventional SLT and ALT. Invest Ophthalmol Vis Sci. 2014;55(13):818.27. Watson P, Stjernschantz J. A six-month, randomized, double-masked study comparing latanoprost with timolol in open-angle glaucoma and ocular hypertension. The Latanoprost Study Group. Ophthalmology. 1996;103(1):126-137.28. Lama PJ. Systemic adverse effects of beta-adrenergic blockers: an evidence-based assessment. Am J Ophthalmol. 2002;134(5):749-760.29. McIlraith I, Strasfeld M, Colev G, Hutnik CM. Selective laser trabeculoplasty as initial and adjunctive treatment for open-angle glaucoma. J Glaucoma. 2006;15(2):124-130.30. Stein JD, Kim DD, Peck WW, Giannetti SM, Hutton DW. Cost-effectiveness of medications compared with laser trabeculoplasty in patients with newly diagnosed open-angle glaucoma. Arch Ophthalmol. 2012;130(4):497-505.31. Cavet ME, Vollmer TR, Harrington KL, VanDerMeid K, Richardson ME. Regulation of endothelin-1-induced trabecular meshwork cell contractility by latanoprostene bunod. Invest Ophthalmol Vis Sci. 2015;56(6):4108-4116.32. Weinreb RN, Ong T, Scassellati Sforzolini B, Vittitow JL, Singh K, Kaufman PL; VOYAGER Study Group. A randomised, controlled comparison of latanoprostene bunod and latanoprost 0.005% in the treatment of ocular hypertension and open angle glaucoma: the VOYAGER study. Br J Ophthalmol. 2015;99(6):738-745.33. Weinreb RN, Scassellati Sforzolini B, Vittitow J, Liebmann J. Latanoprostene bunod 0.024% versus timolol maleate 0.5% in subjects with open-angle glaucoma or ocular hypertension: the APOLLO Study. Ophthalmology. 2016;123(5):965-973.34. Medeiros FA, Martin KR, Peace J, Scassellati Sforzolini B, Vittitow JL, Weinreb RN. Comparison of latanoprostene bunod 0.024% and timolol maleate 0.5% in open-angle glaucoma or ocular hypertension: the LUNAR Study. Am J Ophthalmol. 2016;168:250-259.35. Kawase K, Vittitow JL, Weinreb RN, Araie M; JUPITER Study Group. Long-term safety and efficacy of latanoprostene bunod 0.024% in Japanese subjects with open-angle glaucoma or ocular hypertension: the JUPITER Study. Adv Ther. 2016;33(9):1612-1627.
36. Vittitow JL, Liebmann JM, Kaufman PL, Medeiros FA, Martin KR, Weinreb RN. Long-term efficacy and safety of latanoprostene bunod 0.024% for intraocular pressure lowering in patients with open-angle glaucoma or ocular hypertension: APOLLO and LUNAR studies. Invest Ophthalmol Vis Sci. 2016;57(12):3030.37. Liu JH, Slight JR, Vittitow JL, Scassellati Sforzolini B, Weinreb RN. Efficacy of latanoprostene bunod 0.024% compared with timolol 0.5% in lowering intraocular pressure over 24 hours. Am J Ophthalmol. 2016;169:249-257.38. Impagnatiello F, Toris CB, Batugo M, et al. Intraocular pressure-lowering activity of NCX 470, a novel nitric oxide-donating bimatoprost in preclinical models. Invest Ophthalmol Vis Sci. 2015;56(11):6558-6564.39. Huang Q, Rui EY, Cobbs M, et al. Design, synthesis, and evaluation of NO-donor containing carbonic anhydrase inhibitors to lower intraocular pressure. J Med Chem. 2015;58(6):2821-2833.40. Bacharach J, Dubiner HB, Levy B, Kopczynski CC, Novack GD; AR-13324-CS202 Study Group. Double-masked, randomized, dose-response study of AR-13324 versus latanoprost in patients with elevated intraocular pressure. Ophthalmology. 2015;122(2): 302-307.41. Katz LJ, Weiss MJ, Heah T, Kopczynski C, Novack GD. Two phase 3 studies of the efficacy and safety of AR-13324 ophthalmic solution 0.02%: in patients with open angle glaucoma and ocular hypertension. Invest Ophthalmol Vis Sci. 2016;57(12).42. Lewis RA, Levy B, Ramirez N, Kopczynski CC, Usner DW, Novack GD; PG324-CS201 Study Group. Fixed-dose combination of AR-13324 and latanoprost: a double-masked, 28-day, randomised, controlled study in patients with open-angle glaucoma or ocular hypertension. Br J Ophthalmol. 2016;100(3):339-344. 43. Shearer TW, Crosson CE. Adenosine A1 receptor modulation of MMP-2 secretion by trabecular meshwork cells. Invest Ophthalmol Vis Sci. 2002;43(9):3016-3020.44. Zhong Y, Yang Z, Huang WC, Luo X. Adenosine, adenosine receptors and glaucoma: an updated overview. Biochim Biophys Acta. 2013;1830(4):2882-2890.45. Myers JS, Sall KN, DuBiner H, et al. A dose-escalation study to evaluate the safety, tolerability, pharmacokinetics, and efficacy of 2 and 4 weeks of twice-daily ocular trabodenoson in adults with ocular hypertension or primary open-angle glaucoma. J Ocul Pharmacol Ther. 2016;32(8):555-562.46. Ocular Therapeutix, Inc. Phase 2b study evaluating safety and efficacy of OTX-TP compared to timolol drops in the treatment of subjects with open angle glaucoma or ocular hypertension. ClinicalTrials.gov Web site. https://clinicaltrials.gov/ct2/show/ NCT02312544. Updated December 13, 2016. Accessed March 9, 2017.47. Glaukos Corporation. Study comparing travoprost intraocular implants to timolol ophthalmic solution. ClinicalTrials.gov Web site. https://clinicaltrials.gov/ct2/show/ NCT02754596. Updated April 27, 2016. Accessed December 6, 2016.48. Allergan. Efficacy and safety of bimatoprost sustained-release (SR) in patients with open- angle glaucoma or ocular hypertension. ClinicalTrials.gov Web site. https://clinicaltrials. gov/ct2/show/NCT02247804. Updated January 20, 2017. Accessed March 9, 2017.49. Brandt JD, Sall K, DuBiner H, et al. Six-month intraocular pressure reduction with a topical bimatoprost ocular insert: results of a phase II randomized controlled study. Ophthalmology. 2016;123(8):1685-1694.50. Okeke CO, Quigley HA, Jampel HD, et al. Adherence with topical glaucoma medication monitored electronically the Travatan Dosing Aid Study. Ophthalmology. 2009;116(2): 191-199.51. Liu JH, Zhang X, Kripke DF, Weinreb RN. Twenty-four-hour intraocular pressure pattern associated with early glaucomatous changes. Invest Ophthalmol Vis Sci. 2003;44(4): 1586-1590.52. Mansouri K, Medeiros FA, Tafreshi A, Weinreb RN. Continuous 24-hour monitoring of intraocular pressure patterns with a contact lens sensor: safety, tolerability, and reproducibility in patients with glaucoma. Arch Ophthalmol. 2012;130(12):1534-1539.53. Costa VP, Jimenez-Roman J, Carrasco FG, Lupinacci A, Harris A. Twenty-four-hour ocular perfusion pressure in primary open-angle glaucoma. Br J Ophthalmol. 2010;94(10):1291-1294.54. Memarzadeh F, Ying-Lai M, Chung J, Azen SP, Varma R; Los Angeles Latino Eye Study Group. Blood pressure, perfusion pressure, and open-angle glaucoma: the Los Angeles Latino Eye Study. Invest Ophthalmol Vis Sci. 2010;51(6):2872-2877.55. Leske MC, Wu SY, Nemesure B, Hennis A. Incident open-angle glaucoma and blood pressure. Arch Ophthalmol. 2002;120(7):954-959.56. Bonomi L, Marchini G, Marraffa M, Bernardi P, Morbio R, Varotto A. Vascular risk factors for primary open angle glaucoma: the Egna-Neumarkt Study. Ophthalmology. 2000;107(7):1287-1293.57. Tielsch JM, Katz J, Sommer A, Quigley HA, Javitt JC. Hypertension, perfusion pressure, and primary open-angle glaucoma. A population-based assessment. Arch Ophthalmol. 1995;113(2):216-221.58. Quigley HA, West SK, Rodriguez J, Munoz B, Klein R, Snyder R. The prevalence of glaucoma in a population-based study of Hispanic subjects: Proyecto VER. Arch Ophthalmol. 2001;119(12):1819-1826.59. Buys YM, Alasbali T, Jin YP, et al. Effect of sleeping in a head-up position on intraocular pressure in patients with glaucoma. Ophthalmology. 2010;117(7):1348-1351.60. Malihi M, Sit AJ. Effect of head and body position on intraocular pressure. Ophthalmology. 2012;119(5):987-991.61. Greenfield DS, Siatkowski RM, Glaser JS, Schatz NJ, Parrish RK 2nd. The cupped disc. Who needs neuroimaging? Ophthalmology. 1998;105(10):1866-1874.62. Francis BA, Ianchulev T, Schofield JK, Minckler DS. Selective laser trabeculoplasty as a replacement for medical therapy in open-angle glaucoma. Am J Ophthalmol. 2005;140(3):524-525.63. Gedde SJ, Schiffman JC, Feuer WJ, Herndon LW, Brandt JD, Budenz DL; Tube Versus Trabeculectomy Study Group. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. Am J Ophthalmol. 2012;153(5):789-803.e2.64. Mansberger SL, Gordon MO, Jampel H, et al; Ocular Hypertension Treatment Study Group. Reduction in intraocular pressure after cataract extraction: the Ocular Hypertension Treatment Study. Ophthalmology. 2012;119(9):1826-1831.65. Poley BJ, Lindstrom RL, Samuelson TW, Schulze R Jr. Intraocular pressure reduction after phacoemulsification with intraocular lens implantation in glaucomatous and nonglaucomatous eyes: evaluation of a causal relationship between the natural lens and open-angle glaucoma. J Cataract Refract Surg. 2009;35(11):1946-1955.66. Shingleton BJ, Laul A, Nagao K, et al. Effect of phacoemulsification on intraocular pressure in eyes with pseudoexfoliation: single-surgeon series. J Cataract Refract Surg. 2008;34(11):1834-1841.
References

11
To obtain COPE CE Credit for this activity, read the material in its entirety and consult referenced sources as necessary. We offer instant certificate processing and support Green CE. Please take this post test and evaluation online by going to https://tinyurl.com/ThePressuresOnCOPE. Upon passing, you will receive your certificate immediately. You must score 70% or higher to receive credit for this activity, and may take the test up to 2 times.
Ce Post test Questions
For instant processing, complete the CE Post Test onlinehttp://tinyurl.com/ThePressuresOnCOPE
1. Which of the following is necessary to make a diagnosis of POAG? a. Elevated IOP b. Optic nerve damage c. Visual field loss d. All the above
2. When examining a patient’s ONH, which of the following findings is NOT suggestive of glaucoma? a. Disc hemorrhage b. Small optic nerve and cup c. Focal notching of the neuroretinal rim d. Vertical elongation of the optic cup
3. With which stage of glaucoma are early visual defects associated? a. Early b. Moderate c. Advanced d. End-stage
4. When evaluating a patient with suspected glaucoma, which component is the least valuable for assessing risk of future visual field loss? a. IOP b. Central corneal thickness c. Presence of diabetes d. Refractive error
5. You are considering the use of topical timolol to manage a patient’s glaucoma. When taking the patient’s medical history, use of which systemic hypertension medication might prompt you to select a different IOP-lowering agent? a. Angiotensin-converting enzyme inhibitor b. Beta-blocker c. Thiazide diuretic d. Angiotensin receptor blocker
6. In glaucoma, NO can lower IOP by: a. Increasing trabecular outflow b. Reducing aqueous production c. Increasing uveoscleral outflow d. Increasing episcleral venous pressure
7. Which of the following best describes latanoprostene bunod? a. Latanoprostene bunod lowers IOP better than timolol, but not as well as latanoprost b. Latanoprostene bunod only has a single mechanism of action c. The most common side effect of LBN is conjunctival hyperemia d. Latanoprostene bunod lowers IOP by 32% to 34%
8. When initiating IOP-lowering therapy in a newly diagnosed patient with early POAG and baseline IOP of 20 mm Hg, what is a reasonable target IOP? a. 15% reduction b. < 21 mm Hg c. 25% reduction d. < 18 mm Hg
9. Which is NOT generally an important consideration when selecting initial therapy for early-stage POAG? a. Dosing frequency b. IOP-lowering efficacy c. Mechanism of action d. Safety
10. In the phase 2b study of fixed combination netarsudil, 0.02%, plus latanoprost, the IOP reduction over baseline was: a. 6.0 mm Hg b. 8.6 mm Hg c. 5.8 mm Hg d. 9.1 mm Hg

in GlaucomaChallenging CasesManaging
The Pressure’s ON!
101D