Embed Size (px)
Citation preview

Dr. Beena E. Thomas
Social Scientist
Social & Behavioural Research
11th April 2016
Challenges of tuberculosis (TB) among tribals in India

Background – Tribal in India
• Tribal population constitutes 8.6% of the nation’s
total population (Census 2011)
– 11.3% of the total rural population in India
– 2.8% of the total urban population
• Information among this group is limited
particularly on their health status, health seeking
behavior, socio-cultural characteristics
• Limited information on TB situation among
the Tribal population.
Source: Tribal profile at a glance 2013 http://www.indiaenvironmentportal.org.in/files/file/tribal%20profiles%20at%20a%20glance.pdf

TB Prevalence among Tribal
• Wide variation in TB prevalence (133 – 3259 per 100 000
population with a pooled estimate of 703 per 100 000 which is
higher than that estimated for India (256 per 1 lakh)) (Beena
Thomas et.al., IJMR 2015; V.G.Rao et.al., 2015)
• MDR-TB is comparable with the non-tribal population (2.2% of
new cases and 8.2% among the previously treated case) (J.Bhat
et.al., IJMR 2015)
• TB studies among tribals are mainly on prevalence. Very few
studies on other aspects (V.G. Rao et.al., IJT – In press)

Prevalence of chest symptomatics
• General population – 3 to 5 %
• Adult OPD attendance – 3 to 5 %
• Among the tribal population
– Madhya Pradesh – 7.9% (2009)
– Car Nicobar – 9% (2004)
– Saharia tribe – 11.4% (2010)
TAP emphasizes on…
(a) Strengthening early reporting,
(b) Enhancing treatment outcomes, and
(c) Closer supervision of tribal areas
Action Plan proposed
Improve service coverage and provide quality RNTCP services
Improve accessibility and utilization of the services
Promote community participation and inter-sectoral coordination
RNTCP Tribal Action Plan (TAP)
Source: Tribal Action Plan 2005
RNTCP performance in tribal areas in India
• Poor performance in terms of case detection rate (CDR) in
tribal districts compared to other districts in India
• Among tribal districts
– 53 % in 2010, 45% in 2011 and 56% in 2012 had CDR of
new smear positive <70%
– 26% of tribal dominated districts had CDR of <51% in 2012
• More than 50% of tribal districts were not able to achieve
<85% of cure rate
Source: Muniyandi M et.al., IJMR 2015; Published as a news in ‘The Pioneer’ on June 2015

An ICMR Task Force study has been initiated to
Estimate the burden of TB among the tribal
population and develop an innovative health
system model to strengthen TB control

Objectives
Primary
• Estimate the prevalence of TB amongst tribal groups (TGs)
• To find out the health seeking behavior patterns of chest symptomatics
• Develop a tribal health system model with feasible interventions
Secondary
• Identify socio-cultural determinants as risk factors for TB
• To understand the knowledge, attitude and perceptions on TB among
tribal
• To review the functioning of RNTCP in DMCs, TUs and DTC in these tribal
areas
Methodology
Sequential phases which included…
• Situational analysis
– Social mapping, health facilities available, distances between health
facilities, staff structure of the facilities and profile of the tribal
population
• Qualitative assessment – to find out the gaps and barriers identified
among tribals
– FGDs and interviews with key informants
• Quantitative assessment (Multistage cluster sampling)
– General information-census of households
– Identify the chest symptomatics
– No. of TB patients

The study has been initiated in 6 states in India…
Name of the Institutes Proposed area for study States & No. of Clusters or Villages
Regional Medical Research Centre for Tribals(ICMR), Nagpur Road, Jabalpur – 482003 (MP)
Madhya Pradeshand Chhattisgarh
Madhya Pradesh-16Chhattisgarh-06
Regional Medical Research Centre, (ICMR),Chandrasekharpur, Nandankanan Road,Bhubaneswar – 751023
Odisha Odisha-06
Regional Medical Research Centre (ICMR), Post BagNo: 13, Port Blair 744 101. Andaman and NicobarIslands
Andaman and Nicobar group ofIslands
Andaman-03
Pondicherry Institute of Medical Sciences, (A Unitof Madras Medical Mission) Kalathumettupathai,Village No:20, Kalapet, Puducherry – 605014
Pondicherry and Tamilnadu Maharashtra-08
Rajendra Institute of Medical Sciences (RIMS),Department of PSM, RIMS, Bariatu, Ranchi –834009, Jharkhand
Jharkhand Jharkhand-09

Interim findings – Geographical area covered
• 40 villages in the 6 states have been covered thus far for the
The situational analysis
Social mapping
Qualitative data to assess the gaps and barriers
STATE_NAME SNO Village Name
ANDAMAN 1 Arong
2 Sawai
3 Harmender
CHHATTISGARH 4 Ratenga
5 Kargi Khu
6 Jenjra
7 Singhor
8 Baghmalla
JHARKHAND 9 Kolgi
10 Rampur/ Jura
11 Kundibart
12 Kuri /Hebrom
13 Sagipi
14 Murakanji
15 Tegra
16 Bundu
17 Ghutbahar

STATE_NAME SNO Village Name
MADHYA PRADESH 18 Chhulha
19 Mondra
20 Khuddurpa
21 Salaiya K
22 Sarmesar
23 Padaliya
24 Sarjpura
25 Kichkhidi
26 Urdani
STATE_NAME SNO Village Name
MAHARASHTRA 27 Ghoti
28 Chandsury
29 Pankheda
30 Sitarampu
31 Roshamal
32 Ekadare
33 Hanumantp
34 Kharpadi
ODISHA 35 Maghamara
36 Jantaribo
37 Penagaber
38 Bhadua
39 Gandirabe
40 Kasiabeda

The tribes in these areas
• Madhya Pradesh – Kol, Gond, Korku, Rathya, Bhumiya, Bhil, Sahariya, Baiga, Bhilal, Gwali
• Jharkhand – Oran, Lohra, Mahli, Chik Baraek, Santhal, Malpahadiya, Munda, Ho, Yadav-MOM-Tribal, Lohar-MOM-Tribal, Sourya Pahariya, Bhumij
• Maharashtra – Hindu-Mahadev, koli, Pawara, Bhil, Kokani, Mavachi, Bhil, Patil (OBC), Padavai, Hindu-Varli, Hindu-Kokna, Hindu-Koli, Hindu-Kokand
• Chhattisgarh – Muriya, Bhatara, Kunwar, Bhaina, Urao, Dhanwar, Sornta, Gond, Kawar, Binjwar, Biyar, Lohar, Khariwar, Mavar, Sanwar
• Odhisa – Juang, Munda, Kondha(Koi), Majhi, Dehuri, Kolha, Bhumija, Santal, Bhuyan
• Andaman & Nicobar – Nicobari

Realities: Challenges among tribals
• Difficult terrain, geographical location (forest, hilly regions)
– Inaccessibility to healthcare facilities
– Long distances between villages
– Very poor road condition and lack of transportation

Difficult terrain
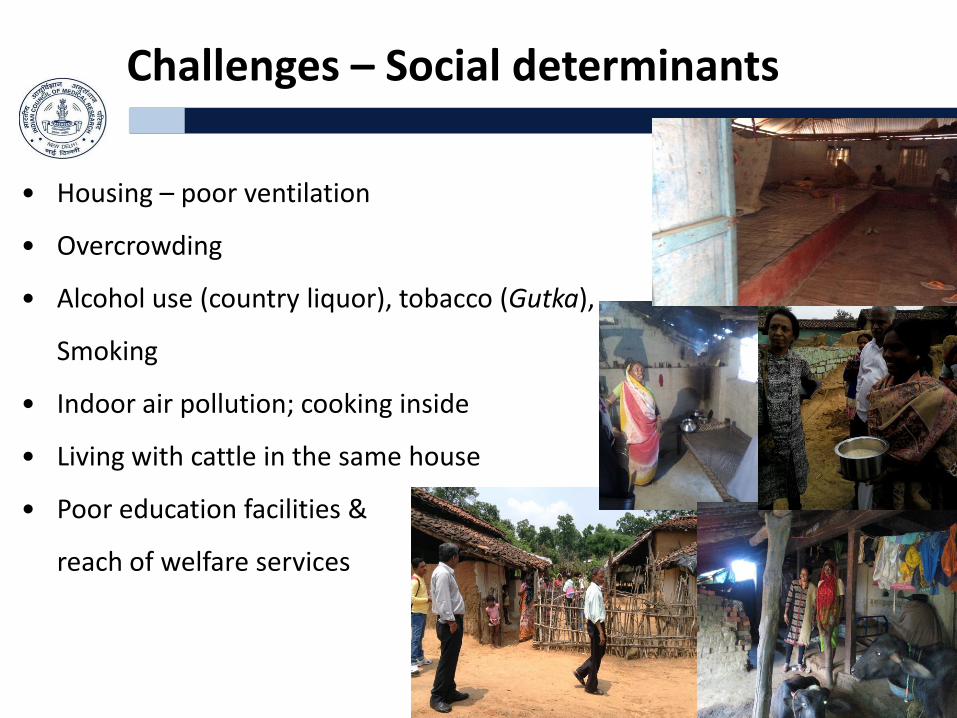
Challenges – Social determinants
• Housing – poor ventilation
• Overcrowding
• Alcohol use (country liquor), tobacco (Gutka),
Smoking
• Indoor air pollution; cooking inside
• Living with cattle in the same house
• Poor education facilities &
reach of welfare services

Challenges – Social determinants
• PDS supply erratic and delayed
• Poor nourishment among children
• No toilet facilities (open defecation)
• No electricity, poor water sources
• Gender discrimination
• Insufficient community involvement

Challenges – Health seeking behavior
• Delays in seeking care
• Low awareness on TB
• Misconceptions on TB
• Dependent on ‘Quack doctors’
• Traditional healing practices (Faith healers)
and cultural beliefs

Challenges – Health system barriers
• Lack of awareness on healthcare facilities / RNTCP
• Sub-centres closed / variations in timings
• Location of sub-centre (schools) – high chances of
transmission
• Long distance covered to reach DMC in collecting
sputum
• High cases of water borne disease & malaria
reported (Odhisa & Maharashtra)
• Lack of staffs or non-availability of doctors
– Pharmacist dispenses medical advice and Rx
– Exploitation by ‘Quack doctors’

Challenges – Health system related
• Poor attitude of staff
• Poor facilities for MDR-TB patients
• Over dependent on ASHAs
• Difficulties faced by ASHA workers, ANM (poor incentives for ASHA),
poor commitment due to lack of monetary rewards
• Lack of healthcare facilities
– Sputum collection
– Difficulties in Rx initiation
• Delays in informing investigation results
• Improper health facilities for technicians
• Inadequate contact screening and chemoprophylaxis

Progress thus far (Quantitative findings)
• Data available for 11 villages till date
• Total no. of households in all these areas
– 3747 households
– 11446 individuals
• No. of chest symptomatic identified – 537
• No. of sputum positive (TB) – 58

Progress thus far
Study area Total no. of
Villages
covered
No. of
individuals
No. of
Symptomatics
Total
positive
No. of
culture
positive
Andaman 1 1048 18 (1.72) 0 0
Chhattisgarh 2 3459 179 (5.2) 13(7.2) 0
Jharkhand 1 852 39( 4.6) 0 0
Madhya
Pradesh4 3676 254 (6.9) 38(15) 14
Maharashtra 2 1566 24 (1.5) 1(4.2) 0
Odisha 1 845 23 (2.7) 6(26.1) 0

The way forward – Possible solutions
• Interventions
» Strengthen access to RNTCP services in the tribal
population for early diagnosis and Rx)
» Active case finding( equipped mobile vans ,door to
door surveys )
» Ensure Patient-centered approach
• Better ward facilities for MDR patients
• Sensitization and training of HCPs
• Ensuring staff in all facilities

Possible solutions
• Ensure contact screening and prophylaxis
• Ensure that incentives reach the ASHA workers
• Explore possible DOTS providers, Family DOTS
• Improve awareness on TB and RNTCP services through community
based activities
» Community engagement – involvement of VHSC, traditional
healers, Panchayati Raj members, Anganwadi workers, ASHA &
ANM, outreach workers, community leaders, tribal youth,
educated members, women, teachers and school students
» Use of fairs, sports for TB sensitization
Possible solutions
• Community based Monitoring and evaluation ( community advisory
boards with representation from the tribal population)
• Provide evidence through Operational and Implementation research
• Sustained collaboration and dissemination of realities with
government and non government institutions at local and national
level for action and translation to policy
Holistic Multi-sectoral approach
• Encourage kitchen garden for better nutrition
• Better ventilated houses
• Nutritional support for children and pregnant
women
• Better sanitation and electricity
• Networking with research institutions, NGOs,
Government for translation
to program and policy

Holistic Multi-sectoral approach
• We need to work towards TB elimination and develop model districts where possible such as in the Car Nicobar Islands

“We need to wash away the scourge of TB…”

Thank You