Embed Size (px)
Citation preview

Challenges of Accurately Measuring and Using BMIand Other Indicators of Obesity in Children
abstractBMI is an important indicator of overweight and obesity in childhoodand adolescence. When measurements are taken carefully and com-pared with appropriate growth charts and recommended cutoffs, BMIprovides an excellent indicator of overweight and obesity that is suffi-cient for most clinical, screening, and surveillance purposes. Accuratemeasurements of height andweight require that adequate attention begiven to data collection andmanagement. Choosing appropriate equip-ment and measurement protocols and providing regular training andstandardization of data collectors are critical aspects that apply to allsettings in which BMI will be measured and used. Proxy measures fordirectly measured BMI, such as self-reports or parental reports ofheight and weight, are much less preferred and should only be usedwith caution and cognizance of the limitations, biases, and uncertain-ties attending these measures. There is little evidence that other mea-sures of body fat such as skinfolds, waist circumference, or bioelectri-cal impedance are sufficiently practicable or provide appreciableadded information to be used in the identification of children and ad-olescents who are overweight or obese. Consequently, for most clini-cal, school, or community settings these measures are not recom-mended for routine practice. These alternative measures of fatnessremain important for research and perhaps in some specializedscreening situations that include a specific focus on risk factors forcardiovascular or diabetic disease. Pediatrics 2009;124:S3–S22
CONTRIBUTOR: John H. Himes, PhD, MPH
Division of Epidemiology and Community Health, University ofMinnesota, School of Public Health, Minneapolis, Minnesota
KEY WORDSbody mass index, overweight, obesity, child obesity,measurement
ABBREVIATIONSCDC—Centers for Disease Control and PreventionIOTF—International Obesity TaskforceWHO—World Health OrganizationCI—confidence intervalBIA—bioelectrical impedance analysis
www.pediatrics.org/cgi/doi/10.1542/peds.2008-3586D
doi:10.1542/peds.2008-3586D
Accepted for publication Apr 29, 2009
Address correspondence to John H. Himes, PhD, MPH, Universityof Minnesota, School of Public Health, Division of Epidemiologyand Community Health, 1300 S 2nd St, Suite 300, Minneapolis,MN 55454. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2009 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The author has indicated he has nofinancial relationships relevant to this article to disclose.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 124, Supplement 1, September 2009 S3 by guest on December 10, 2020www.aappublications.org/newsDownloaded from

BMI (weight [kg]/height [m2]) hasprobably become themost common in-dicator used to assess overweight andobesity in a wide variety of settings,including clinical, public health, andcommunity-based programs. Althoughit is certainly not a perfect surrogatefor total body fatness and not withoutits technical limitations,1 BMI has beenrecommended as the most appropri-ate single indicator of overweight andobesity in children and adolescentsoutside of research settings.2–4
One of the attractive features of BMI isthat it is derived from measurementsof height and weight. These 2 anthro-pometric dimensions are the onesmost commonly collected on childrenworldwide. These 2measurements arenoninvasive, relatively inexpensive toobtain, and relatively easily under-stood by health practitioners, the indi-viduals being measured, and theirfamilies.
Mentioning child measurements ofheight and weight, individuals may bereminded of their own marks on thedoor sills and the bathroom scales oftheir childhood homes. So, althoughwide familiarity with height and weightenhances the use and understandingof a measure such as BMI, it also maydesensitize health professionals to theneed to give adequate attention toissues concerning how height andweight data are collected. Accordingly,one may hear the comment, “Anyonecan measure height and weight.” Al-though one must actually agree withthe language, if not the intent, of thiseasy declaration, many health profes-sionals are unaware that there areconsequences for the usefulness andaccurate interpretation of BMI datathat follow from decisions made con-cerning data collection.
In this article, challenges surround-ing the measurement of BMI in USchildren (2–18 years of age) and theimplications of these issues for the
appropriate collection, use, and inter-pretation of BMI as it is used as an in-dicator of child and adolescent over-weight and obesity are considered.Also, chief measurement issues re-lated to other selected anthropometricindicators of overweight and obesityare briefly discussed.
SOME BASIC CONCEPTS FROMMEASUREMENT THEORY
Classical measurement theory in-cludes some concepts that are helpfulfor understanding issues surroundingmeasurement of height, weight, and,therefore, BMI. Detailed explanationsof measurement theory are availablein standard textbooks concerningmeasurement and psychometrics.5,6
Different academic disciplines mayuse different terms to refer to thesame concepts, but for the present dis-cussion the terms usually found in thebiomedical and epidemiologic litera-ture will be used.
It is important to know that all mea-surements are imperfect and alwaysmeasured with some error, whetherthe measurements be height, weight,skinfolds, or bioelectric impedance.Accordingly, an index such as BMI,which is derived from 2 other mea-surements, will include the compo-nents of measurement error inherentin the constituent height and weightmeasurements. The nature andmagni-tude of these measurement errorshave some fairly predicable conse-quences related to the usefulness andinterpretation of the measurements.
Some measurement errors are ran-dom, with the same probability of be-ing smaller than or greater than thetrue value (a theoretical value mea-sured without error). Consequently,the average or mean of random errorsacross a series of measurements is 0.For example, nurse Brown measuredheights on a group of 4-year-old girlson Monday, and the mean height was
100 cm. She measured the same chil-dren a second time on Tuesday, againwith a mean height of 100 cm. Never-theless, for some girls there weresmall differences in height measure-ments between Monday and Tuesday,although the mean height of all girlsremained the same for the 2 days.The differences between measuredheights onMonday and Tuesday for theindividual girls are examples of ran-dom errors of measurement.
Random errors of measurement are aconcern, because they always add tothe variability of the true measure-ments; their presence and extent areusually considered the measure-ment’s “reliability.” Poor measure-ment reliability is a concern because itmay cause incorrect clinical judg-ments for individual children (misclas-sification) and alter conclusions forstatistical analysis for groups of chil-dren. Because most inferential statis-tical tests use a measure of variation(eg, SD) as a denominator, statisticaltests of differences between means,analysis of variance, correlations, re-gressions, and odds ratios are all at-tenuated (ie, less statistically signifi-cant) as the measurement reliabilitydecreases and the variability term inthe denominator increases. Randomerrors are usually reported in terms ofa measurement error variance or ameasurement error SD, or summa-rized in reliability coefficients (inter-class or intraclass correlations) fromreplicate measurements of the samechildren.
In a second example, nurse Brownmeasured the same group of girls onMonday, again with a mean height of100 cm. This time on Tuesday nurseJones measured them for a secondtime and recorded heights exactly1.0 cm taller than did nurse Brown forevery girl. Now the mean height for allthe girls on Tuesday was 101 cm. If weconsider nurse Brown to be our gold
S4 HIMES by guest on December 10, 2020www.aappublications.org/newsDownloaded from

standard of measurement, this sys-tematic measurement error (ie, all in 1direction) of nurse Jones is an exam-ple of measurement bias.
Measurement bias is a concern be-cause it may causemisclassification ofindividual children or groups of chil-dren. Nevertheless, as long as the biasis not differential among groups, puremeasurement bias will not affect theresults of statistical tests between oramong groups, such as differences be-tween means, analysis of variance,correlations (interclass), regressions,and odds ratios. In practice, differ-ences between individual observerswho measure the same children willalso have a component of randommeasurement error between them.Not surprisingly, observers tend tomeasure more like themselves thanlike others, so interobserver errorsare almost always larger than intra-observer errors.
Measurement theory usually specifiesthat measurement errors are inde-pendent and additive, that is, that thetotal measurement error variance isthe sum of error variances from allsources.5 Also, when increments or dif-ferences between successive mea-surements are used, the measure-ment errors attending each of the 2constituent measurements are in-cludedwith the increment. So an incre-ment has twice the random measure-ment error (variance) of an attainedvalue and lowermeasurement reliabil-ity. Obviously, if measurement biaseschange over time, the accuracy of in-crements becomes questionable.
CHIEF SOURCES OF MEASUREMENTERRORS FOR HEIGHT AND WEIGHT
When a child’s height and weight aremeasured, there are several pos-sible sources of measurement error.A simplified theoretical model wouldsay that the total variance of mea-surement error is the sum of that
associated with the instrument usedto measure, that associated with thechild being measured, and that associ-ated with the observer(s) doing themeasuring. In most settings, however,errors associated with the child andwith the observer(s) are the chiefsources ofmeasurement error inmea-surements of height and weight. Obvi-ously, it is still important to have ap-propriate measuring equipment, butonce they are installed and calibrated,little measurement error usually isdue to the instruments per se.
Measurement Errors Due toChild Variation
The normal day-to-day variation withina child leads to a component of mea-surement error. This variation proba-bly results from many sources includ-ing hydration, gastrointestinal andurinary bladder contents, diurnal hor-monal fluctuations, saltatory growth,fidgeting, alterations in position, andfatigue.7,8
As early as 1724, Wasse recognized ap-preciable variation in stature duringthe day and concluded that “[t]he al-teration in the human stature . . . pro-ceeds from the yielding of the carti-lages between the vertebrae to theweight of the body in an erect pos-ture.”9 MRI studies have since con-firmed that the diurnal variation instature primarily results from in-creases in water content in the softcentral portion of the intervertebraldiscs (nucleus pulposus) while at restand water loss while standing or dur-ing other weight-bearing activities.10
For children, one can expect a meanheight difference of �1.5 cm (SD:0.46 cm) between rising and late after-noon,11 with most of the change prob-ably occurring during the first 2 to 3hours of the day.12
In practice, it is helpful to understandthe expected diurnal variation in childheight but probably impractical to try
to time height measurements to ac-commodate it, unless one is engagedin a rigorous research protocol thatrequires serial measurements on asmall number of individual children.For the data included in the 2000 Cen-ters for Disease Control and Preven-tion (CDC) growth charts,13 heightswere measured frommornings throughevenings so that the reference percen-tiles represent something like heightsaveraged throughout the day, and theassociated within-child variation is in-cluded in the total variance in heightcaptured in the published percentilesor z scores at an age.
For body weight, the within-child varia-tion is related to the size of the childand should usually be within 1.5% ofthe measured weight (SD: 0.5%).14 Ac-cordingly, the expected maximumwithin-child weight variation for chil-dren whoweigh 25 and 50 kg should be�375 g (0.83 lb) and 750 g (1.65 lb),respectively. In practice, it is difficult tostandardize this physiologic within-child weight variation when childrenare measured, so it is usually ignoredfor most purposes.
Seasonal Variation
It has been known for a long time thatin some environments children maygrow differentially according to sea-son of the year.15 It is important, how-ever, to understand the contexts ofthese findings to determine the impli-cations for current studies of height,weight, and BMI.
In developing countries with prevalentpoverty, undernutrition, and infection,reduced seasonal patterns of aver-age growth in height and weight areoften linked to the rainy season(s),along with accompanying factors in-cluding reduced food availability andincreased infection.16,17 In developedcountries the evidence is mixed, butwhen seasonal patterns are present,they usually indicate relatively greater
SUPPLEMENT ARTICLE
PEDIATRICS Volume 124, Supplement 1, September 2009 S5 by guest on December 10, 2020www.aappublications.org/newsDownloaded from

growth in height and linear dimen-sions during the spring and summerand relatively greater growth inweightand fatness during the fall and win-ter.18,19 When seasonal fluctuations ex-ist in developed countries, they aresmaller and less common than thoseseen in children living in developingcountries.
In studies in both Japan20 and theUnited States,21 seasonal fluctuationsin growth were observed in earliergenerations of children but disap-peared within the same populationsover 20 to 40 years because generalhealth and nutrition conditions im-proved through time. Accordingly, foralmost all children now living in theUnited States, there should be little ifany seasonal variation in growth thatwould require accounting for it in thedesign of studies or data-collectionprotocols.
Excess growth in BMI has been ob-served over summer vacation be-tween kindergarten and first gradefor children in the Early ChildhoodLongitudinal Survey.22 Nevertheless,this should probably be viewed as aschool/no-school effect rather thanseasonal variation per se.
Measurement Errors Due toObserver Variation
An important goal in measurement ofheight and weight should always be tocollect the data with as little measure-ment error as possible, given the prac-tical and financial constraints of thelocal situation.
In a highly controlled research labora-tory with experienced anthropom-etrists, the mean interobserver (abso-lute) differences for standing heightand weight are 0.3 cm and 0.02 kg, re-spectively, with corresponding SDs of0.2 cm and 0.03 kg.23 These valuesshould be viewed as close to the mini-mum values possible using currentmethods. In most situations there is
more concern about observer reliabil-ity in measurements of height ratherthan weight, because height measure-ments include more “opportunities”for within-child and observer variationthan do weight measurements.
Often, height and weight measure-ments for BMI are collected in clinicalor other settings in which data col-lection may be hurried and observ-ers may not have been trained asrigorously as observers in researchsettings. Actually, there are few stud-ies available concerning measure-ment variation among those who prob-ably collect most of the data used forBMI evaluation and screening. Ahmedet al24 evaluated the measurementvariation among 2 sets of health visi-tors who each measured each of 10children at ages 3 and 4.5 years 3times with a portable stadiometer. Theaverage value for the SD of measure-ment was 0.47 cm. In a small compari-son trial on height of 5- and 6-year-oldBritish children, school nurses had apooled interobserver measurementSD of 0.32 cm, which compared favor-ably to that of a trained auxologist(0.35 cm) on the study.25 The nurses inthis study had been trained in measur-ing height. Importantly, training canimprove the precision of length andheight measurements.8,26
Given the above-listed principles, it fol-lows that when a large number of datacollectors are required the interob-server measurement errors increaseas well.27 Consequently, one would pre-fer to have as few individuals measur-ing height and weight as is practicablein the particular setting, especially ifthe resulting data will be used for re-search purposes or if serial measure-ments on the same children are beingmade.
Another strategy for reducing mea-surement errors is to take the mea-surements more than once and thenuse the mean of the replicates. The
theory here is that a mean of repli-cates is a better estimate of the “true”measurement, because the randomerrors of measurement are reduced.28
The usefulness of taking replicatemeasurements depends on the reli-ability of the single measurement inquestion and how the data will beused.
Routinely obtaining replicates benefitsmost those measurements that havethe lowest initial reliability, and thecorresponding improvements in reli-ability are predictable.28 Measurement-reliability coefficients (R) express thepercentage of the total observed vari-ation that is captured by the “true”measurement variation. For singlemeasurements of height and weight ina nonresearch setting, a reasonableexpectation for values of R should be�0.93 and 0.97, respectively. At theselevels of measurement reliability, col-lecting a second measurement andusing the mean raises the values ofR to 0.963 and 0.984, respectively.These are not dramatic improvementsin measurement reliability using a du-plicate, because the initial levels ofmeasurement reliability started outrather high.
Contrast these possible improvementswhen using replicate measurementswith those for skinfold thicknesses, forwhich the measurement reliability fora single measurement in nonresearchsettings is probably�0.8. For succes-sive numbers of replicate skinfoldmeasurements and using the mean,the R values would be 0.88 for 2 mea-surements, 0.92 for 3 measurements,and 0.94 for 4 measurements.
The errors of measurement with lowmeasurement reliability are usuallyassumed to be largely random. Conse-quently, how the data are to be used isa consideration in deciding whetherthe extra time and trouble should bespent routinely collecting replicatemeasurements. Purely random errors
S6 HIMES by guest on December 10, 2020www.aappublications.org/newsDownloaded from

will not affect the group means ofheight, weight, and BMI, although theywill increase the SDs because of theadded error variance. Similarly, theprevalence of children with a BMIabove percentile cutoffs for age andgender will not be affected by theadded random error because as manychildren should bemisclassified aboveand below the cutoff value. If the BMIdata are to be used for these pur-poses, routinely taking replicate mea-surements is probably not worthwhile.
For some uses of BMI data, however,routinely taking replicate measure-ments is recommended. If the BMI datawill be used to make clinical decisionsregarding treatment or referral of in-dividual children, or for assessingchanges in individuals over time, asecond measurement of height andweight will reduce misclassification ofcurrent status and increase the abilityto detect changes from one occasionto another. In research settings thatinclude height, weight, and BMI as im-portant variables, duplicate measure-ments of height and weight are recom-mended. If the height and weightreplicates are averaged before calcu-lating BMI, the latter calculation onlyneeds to occur once.
CHALLENGES OF USINGAPPROPRIATE REFERENCE DATAAND CUTOFFS
Which Reference Data?
Usually, BMI will be evaluated in chil-dren relative to reference data orgrowth charts. The main challenge tothe investigator is to choose the setof growth charts that is most ap-propriate for the intended purposesfor which the BMI data will be used.For height, weight, and BMI, US in-vestigators have the benefit of re-cent recommendations from an expertcommittee.4,29
For most purposes, US children aged2 to 18 years should be evaluated
relative to the 2000 CDC growthcharts.13 These are high-quality growthcharts that present selected percen-tiles and allow calculation of z scoresof attained height, weight, and BMI forage and gender and in metric and En-glish units. The primary data were col-lected in national surveys by using rig-orous measurement protocols, andstate-of-the-art statistical methodswere used to derive and smooth thepercentiles and z scores across theages. More detailed technical informa-tion on methods and development areavailable elsewhere.13 Earlier sets ofBMI reference data for US children (eg,Must et al30) should not be used be-cause the cutoff values are slightly dif-ferent, which will serve to complicatecomparisons across studies.
Some other countries have developedand use their own growth charts, but 2sets designed for international appli-cations should be briefly mentioned,particularly relative to BMI. The Inter-national Obesity Taskforce (IOTF) spon-sored a workshop with a goal of estab-lishing a standard definition for childoverweight and obesity worldwide.31
As a result, high-quality BMI data from6 countries (Brazil, Great Britain, HongKong, Netherlands, Singapore, and theUnited States) were combined to de-velop age- and gender-specific cutoffsfor children (birth to 20 years of age)corresponding to the locations of theBMI values of 25 and 30 kg/m2 in thestatistical distribution of adults.19
These latter BMI cutoffs are the con-ventional criteria that identify over-weight and obesity in adults.32
The IOTF cutoffs that define overweightand obesity correspond approximatelyto percentiles 82 to 84 and 96 to 97,respectively, on the 2000 CDC growthcharts for BMI for age, not very differ-ent from the 85th- and 95th-percentilecutoffs used customarily in the UnitedStates. Prevalences of overweight andobesity in children in countries outside
the United States are now being re-ported in the literature rather fre-quently using the IOTF criteria,33,34
which has been useful in standardizingBMI criteria. Nevertheless, it should benoted that the IOTF charts contain nopercentile or z-score curves other thanthe 2 cutoff lines, because they werespecifically designed for reportingpopulation prevalences of overweightand obesity. Accordingly, the IOTFcharts should not be used to monitorBMI growth in individual children.
In 2006 the Department of Nutritionand Health at the World Health Organi-zation (WHO) released a new growthstandard for children from birth to 5years of age based on longitudinal andcross-sectional data collected in 6countries (Brazil, Ghana, India, Nor-way, Oman, and United States).35 Thenew attained growth curves, includingBMI, were designed to represent howall children ought to grow under idealcircumstances. Accordingly, the moth-ers and children were carefully se-lected so that there were no knownconstraints to healthy growth, includ-ing exclusive breastfeeding and appro-priate introduction of solid foods.36 Be-cause of the homogeneous nature ofthe WHO samples and some choicesmade to exclude the heaviest children,the upper BMI percentiles and z scoresare somewhat restricted (ie, nar-rower) at an age compared with thosein the 2000 CDC growth charts. Conse-quently, using the same percentile cut-off for BMI at an age (eg, �95th), theWHO standards will yield a higher prev-alence of children than if the �95thpercentile for age were used from the2000 CDC growth charts.37 The oppo-site is true at the other end of the BMIdistribution so that thinness definedby a low BMI percentile on the WHOstandards will identify fewer childrenwith low BMI compared with using thesame percentile cutoff on the 2000 CDCgrowth charts.38
SUPPLEMENT ARTICLE
PEDIATRICS Volume 124, Supplement 1, September 2009 S7 by guest on December 10, 2020www.aappublications.org/newsDownloaded from

One concern about using these newWHO growth standards is the interpre-tation in terms of the health or growthof children who are in the extremes ofthe percentiles (eg, �5th, �95th) onthe basis of a standard that purport-edly only included healthy children.Nevertheless, the WHO standards areso new that there are no data docu-menting whether the new cutoffs arebetter at identifying children at healthrisk than the 2000 CDC growth charts.
In 2007, the WHO released a growth ref-erence for height, weight, and BMI forchildren aged 5 to 19 years that wasdesigned to align with the 2006 WHOgrowth standards at 5 years and tobe used internationally.39 The WHO re-analyzed the data comprising the USNational Center for Health Statisticsgrowth curves, published in 1977,40
and proposed that they be used as asingle growth reference for screening,surveillance, andmonitoring of school-aged children worldwide. As with chil-dren older than 24 months included inthe new WHO birth to 5 years refer-ence,35 BMI values of �2 SDs were ex-cluded as unhealthy for the 2007 5 to19 years reference.39 Because theheaviest children were excluded, theupper percentiles of BMI for the WHO2007 reference are substantially be-low the corresponding levels for the2000 CDC growth charts, especially inlater adolescence when high BMI val-ues are more common.
There has been much informal dis-cussion about the use of the IOTF andWHO references. Unfortunately, therehave been no formal recommenda-tions from agencies or professionalorganizations in the United States re-garding their routine or partial use(eg, at certain ages or for certain pur-poses). This institutional silence is un-fortunate, because it will likely lead toat least ambiguity and perhaps evenconfusion among health practitionersand in the scientific literature.
As a personal recommendation forhealth practitioners in the UnitedStates, the 2000 CDC growth chartsshould be used for routine screening,surveillance, and monitoring of BMIbecause they have been widely evalu-ated and adopted, and they have beenrecommended by recent expert com-mittees.4,29 If investigators wish tocommunicate with international col-leagues in presentations and in thescientific literature by citing the IOTFor WHO criteria, they should also in-clude at least prevalence results rela-tive to the 2000 CDC growth charts sothat their findings can be comparedwith those of other US studies. Hope-fully, as further research becomesavailable, more specific recommenda-tions can be made on the basis ofstudies of sensitivity/specificity anddifferential risk among the variousBMI criteria currently available.
A Rose by Any Other Name
Before 1994 the scientific literature onoverweight and obesity included awide range of defining criteria (eg,percent ideal weight, skinfold thick-ness, ponderal index, BMI) and manydescriptive names to refer to the chil-dren and adolescents who were con-sidered the fattest. This variation in re-porting made it difficult to comparefindings because different indicatorsmay actually identify different childrenas the fattest,41 and the differences interminology were sometimes confus-ing. An expert committee consideredthese issues, and their proceedings,published in 1994,2 had considerableeffect toward standardizing the crite-ria (BMI for age) and the nomenclaturefor referring to the fattest childrenand adolescents. Subsequently, thesedefinitions became preferred in de-scribing weight status.3,42,43
In the 1994 report,2 children with a BMIthat exceeded 30 kg/m2 or�95th per-centile for age and gender (whichever
was smaller) were considered over-weight. Children or adolescents with aBMI at �85th percentile but �95thpercentile were considered at risk ofoverweight. At that time, the term“obese” was avoided, because obesitywas technically defined in terms ofbody fat per se, and BMI was derivedonly from height and weight.
In 2005, the Institute of Medicine (IOM)consciously departed from the termi-nology discussed above and elected todefine children with at BMI at �95thpercentile for age and gender as obeserather than overweight.44 The IOM re-port expressed the seriousness, ur-gency, and medical nature of child-hood obesity and deliberately soughtto express this concern by using theterm “obese” to refer to the childrenand adolescents with the highest BMI.A recent expert committee endorsedthe IOM position and recommended toreplace the terms “at risk of over-weight” and “overweight” with theterms “overweight” and “obese,” re-spectively.4,29 Accordingly, the expertcommittee recommended that individ-uals 2 to 18 years of age with a BMI of�30 kg/m2 or �95th percentile forage and gender (whichever is smaller)should be considered obese. Individu-als with a BMI at�85th percentile but�95th percentile or 30 kg/m2 (whichever is smaller) should be consideredoverweight.
The expert committee believed that theterms “overweight” and “obese” betterconvey the seriousness and impor-tance of the obesity epidemic to healthproviders, parents, and children and ina less ambiguous manner than theprevious terms, although no specificliterature was cited to support thisview. Because BMI identifies the fattestindividuals with acceptable accuracy,especially at the highest levels ofBMI,45,46 the expert committee believedthat choosing more direct terms thatmay provide additional impetus for
S8 HIMES by guest on December 10, 2020www.aappublications.org/newsDownloaded from

treatment and change was to be pre-ferred to parsing technical conceptsthat would be unlikely to aid under-standing. Finally, the new terminologycomports with that from the IOTF BMIcriteria for children and adolescents,47
with conventional terminology foradults,32,48 and with the InternationalClassification of Diseases, 9th Revi-sion, Clinical Modification (ICD-9-CM).
Nomenclature really does matter; it is asine qua non with standardized defi-nitions of health conditions. Standard-ized nomenclature increases precisionin scientific and public communicationand provides improved understandingin health guidance.
Precision of Percentile Estimates
Often, health providers and research-ers use the exact BMI-for-age cutoffsthat define overweight and obesity asironclad diagnostic criteria. Althoughstandardized definitions are essential,as discussed above, the actual mea-surements on the child will alwaysvary somewhat as a result of child andobserver factors. In addition, the ac-tual percentile cutoffs themselves arestatistical estimates of points that arealso subject to errors.
Let us assume that the basic data thatwere used to construct the 2000 CDCgrowth charts13 are truly representa-tive of the US population of childrenand adolescents, and that the statisti-cal procedures used to smooth thepercentile values across age were ap-propriate and unbiased. There still re-mains a degree of uncertainty regard-ing the point estimates of the finalpercentile values related to the num-ber of children that were included inthe samples within each 6-month agegroup used to estimate the percen-tiles. Simply put, the larger the sample,the more precise the percentile esti-mates, especially at the extremes ofthe distribution.
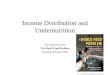
As an example, Fig 1 presents the 85th,95th, and 99th percentiles of BMI forgirls as straight lines and the respec-tive 95% confidence intervals (CIs) cal-culated by using the method of Wil-son49,50 and the unweighted samplesizes within age groups (15–20 years)used for the 2000 CDC growth charts.13
At younger ages the sample sizesrange from 400 to 639, and the 95% CIsare quite stable and similar to those at15 and 16 years. The sample sizes andcorresponding 95% CIs for boys aresimilar to those for girls. The 99th per-centile of BMI for age was not origi-nally published with the growth chartsbut has been suggested as a usefulcutoff for identifying children at addedhealth risk.51
On the basis of sample sizes, the 95%CIs around the 85th BMI percentiles in-clude values approximately betweenthe 81st and 88th percentiles until�17.5 years, when the sample sizesdecrease and the 95% CIs becomewider. These CIs mean that at 20 yearsof age (the most extreme case), a girlwhose BMI percentile corresponds tothe 85th percentile on the CDC chartmay actually have a BMI anywhere be-tween the 78th and 90th percentilesbecause of the imprecision the of per-centile estimates.
For the 95th BMI percentile estimatesbefore �17.5 years, the 95% CI range
from approximately the 92nd to the 97thpercentiles but increase in spread,reaching from the 90th to 98th percen-tiles at the older ages. The 95% CIsaround the 99th BMI percentiles forgirls include from approximately the97th to effectively just less than the100th percentiles (because no pointcan exceed percentile 100).
After�18 years of age, the upper 95%confidence limit for the 85th percen-tiles and the lower 95% confidencelimit for the 95th percentiles are ap-proximately coincident, and the upperlimit of the 95th and the lower limit ofthe 99th percentiles actually overlap.This means, for example, that a 19-year-old girl with a BMI identified asbeing at the 99th percentile by the2000 CDC growth charts (or by com-puter programs that calculate the ex-act percentiles) will probably have aBMI somewhere between the 96th and100th percentiles.
The precision of the upper percentilecutoffs for BMI can be viewed from sev-eral different perspectives. First, thesamples and CDC growth charts are asthey are, and no revisions are antici-pated in the near future. Consequently,those who use the growth charts shouldunderstand their limitations in inter-preting findings and not wait for moreprecise estimates. Actually, additionalimprecision beyond that related tosample size probably also occurs atsome ages in adolescence because ofdifferences in maturational status.52
Given the range of CIs surrounding theBMI percentiles at all ages, health pro-viders and investigators should be alittle less stringent in defining the ex-act location of a child or groups of chil-dren in the BMI distribution relative tothe growth charts. Accordingly, BMIvalues just below or just above recom-mended cutoffs should be interpretedas only 1 indicator and not the only di-agnostic criterion for clinical deci-sions. Follow-up visits and repeated as-
FIGURE 1The 85th, 95th, and 99th percentiles for BMI ingirls (straight horizontal lines) and 95% CIs cal-culated from the number of subjects included ateach age in the 2000 CDC growth charts.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 124, Supplement 1, September 2009 S9 by guest on December 10, 2020www.aappublications.org/newsDownloaded from

sessments on other occasions shouldreduce the uncertainty of the child’sBMI status.
The fairly wide confidence limitsaround the percentiles do not invali-date the recommended BMI cutoffs forstandardized reporting of populationprevalences or for analyses of theassociated risk profiles of groups ofchildren.51 Nevertheless, investigatorsshould be cautious drawing inferencesfrom risk ratios comparing the ob-served and expected prevalences be-yond a given BMI cutoff because of theimprecision of the percentile cutoffs.
When Should z (SD) ScoresBe Used?
A BMI z or SD score is the BMI of a childtransformed into a scale comprisingthe number of SD units it is away fromthe mean of the referent population ofthe same age and gender. The 2000CDC growth charts13 were constructedin such a way to allow calculation of zscores for BMI.
There are several advantages to usingz scores compared with using the cor-responding percentiles, although theyboth describe a child’s status relativeto the same reference data set. The pe-diatric applications of z scores thatare most common are probably in en-docrinology or nutrition where chil-dren who are very small relative to thegrowth charts are seen and z scoresprovide a more useful and manage-able metric than percentiles to evalu-ate and monitor status or treat-ment.53,54 For example, a 3-year-old boywith a height-for-age z score of �3.6has a height that is 3.6 SDs lower thanthe age- and gender-specific mean forhim on the growth charts; his corre-sponding height-for-age percentile is0.013.
When a high proportion of childrenhave heights and weights less than thelowest percentiles (eg, 3rd, 5th), asfound in many developing countries,
the percentile charts cease to be use-ful for differentiating their growth sta-tus. Accordingly, cutoffs of less than�2 z for height for age and weight forage have become conventional defini-tions for stunting and wasting,respectively.53
In a similar fashion, for overweightand obesity in children and adoles-cents, z scores can be useful for char-acterizing individuals with a high BMIthat exceeds the percentile levelsavailable on the growth charts. For ex-ample, if the progress of a girl with aBMI that far exceeds the 97th percen-tile for age (currently the highest per-centile available on the CDC charts) ismonitored, her attained BMI on thegrowth chart is difficult to evaluateand impossible to meaningfully quan-tify. On the other hand, by convertingher BMI to a z score, her progress canbe monitored and changes in subse-quent z scores have a direct interpre-tation relative to the referent popula-tion of her age. Because z scores arecalculated relative to age, noting achange in z score is an appropriateway to evaluate changes in BMI acrossages relative to what is expected in thereferent population.
An alternative to using z scores toevaluate change in individual childrenwith elevated BMI is to just use changein BMI itself. These changes are un-derstandable to practitioners, adoles-cents, and families, and they allow set-ting of goals andmonitoring of progress.
Using z scores is currently the onlyappropriate way available to quantifythe severity of obesity in children whohave BMI levels that exceed the avail-able percentiles for age and gender.Unfortunately, z scores require a com-puter program to calculate themreadily, and the SD-related metric isnot familiar to many practitioners. Be-cause the total variation in BMI (eg, thedistance between the 5th and 95th per-centiles) progressively increases with
age, calculating the percentage excessof a BMI value or percentage over-weight beyond a percentile value is in-appropriate, because it will have in-consistent meaning from age to age.
CHALLENGES OF MEASURINGHEIGHT, WEIGHT, AND BMI
Summary reminders concerning datacollection and management are listedin Table 1. The particular setting inwhich data for BMI assessments willbe collected has implications for howor whether the recommended prac-tices can be implemented.
Equipment and Space
If possible, height should be measuredto the nearest 0.1 cm (1⁄4 in) by usinga stadiometer mounted on the wall ora portable stadiometer that allowsthe child to be positioned properlywith his or her back against a verticalsurface. A second choice are modelsthat measure the child freely stand-ing, but the measurement errors forthese latter instruments tend to belarger than when the measurementsare taken with the child standingagainst a surface.55 The height mea-surements for the 2000 CDC growthcharts13 were taken by using wall-mounted stadiometers. Many brandsof acceptable stadiometers are avail-able, and searching on-line will pro-vide several good choices. Stadiom-eters attached to scales that do notallow the child to be positioned cor-rectly are not recommended.
Weight should be measured by using agood-quality scale to the nearest 100 g(1⁄4 lb). In the past, balance-beam scaleswere routinely recommended becausethe only alternatives were spring scalesthat were less dependable. Now thereare many good electric scales avail-able that are also quite portable. Themore expensive scales have multiplepressure transducers under the weigh-ing platform, so they are less sensitive
S10 HIMES by guest on December 10, 2020www.aappublications.org/newsDownloaded from

to variation in the child’s position andshifting of weight from one leg to theother. Again, an Internet-based searchwill yield many good alternatives.
In a research setting, obviously, thebest-quality equipment should bechosen for maximum consistency overtime and for reliability among observ-ers taking the measurements. In clini-cal or community settings, cheaper al-ternatives are often used, but giventhe heavy utilization in a busy clinic, forexample, investing in sturdy anthropo-metric equipment that can be cali-brated if necessary will prove worth-while and increase confidence in themeasurements. Cheaper models ofstadiometers tend to have less-rigidparts that wobble or bend with fre-quent use.
With repeated use or if equipment ismoved about fairly often, stadiometersand scales should be checked to deter-mine if they are calibrated correctly.It is important to develop a regularschedule for calibration (eg, daily inresearch, weekly in clinic) and assignsomeone to be responsible for theseduties. Depending on the installation,good stadiometers usually can be cal-
ibrated by using a metal rod of a fixedlength.
Good electric scales can be calibratedor “zeroed.” In most areas of theUnited States, state agencies in de-partments of commerce, standards, oragriculture have representatives whocalibrate and certify scales in grocerystores and in other commercial ven-ues. In some cases, these representa-tives can be called on to routinelycheck and calibrate scales at perma-nent sites. Alternatively, scales can becalibrated by using weights of knownsize. If models of electric scales areused in clinic or in the field, ensuringthat a supply of batteries of appropri-ate size should be on the checklist forroutine equipment maintenance.
Often, in busy clinic or school situa-tions, stadiometers and scales are rel-egated to hallways or even receptionareas. Children and adolescents mayfind it embarrassing to be measured,and even more so to have witnesses tothe procedures.56 Having a private orpartially screened area for the heightand weight measurements will in-crease child cooperation and enhance
the patient confidentiality sought by in-stitutional human subjects committees.
Measurement Protocols
Because health providers and otherswho use BMI data will almost alwayscompare them to the growth charts, itmakes sense to strive to collect theheight and weight measurements thatcomprise BMI by using protocols thatmatch those used in the referencedata as closely as possible. The mea-surement procedures used in the col-lection of the height, weight, and BMIdata for the 2000 CDC growth charts13
are currently available as a download-able file at the CDC National Healthand Nutritional Examination Survey(NHANES)Website(www.cdc.gov/nchs/data/nhanes/bm.pdf). These measure-ment protocols follow closely those rec-ommended by a US consensus group.57
This publication has become the gold-standard reference in the United Statesfor anthropometry methods related tohealth issues, although slight differ-ences exist for some measurementscustomarily used internationally.58
It is important to train data collectorsin the appropriate methods for mea-suring height and weight. Again, thegoal is to use the same measurementprotocols that were used for the deri-vation of the growth charts. Some-times, experienced clinic staff maytake offense because they have beenmeasuring height and weight for along time. Often, however, “the way wedo it here” includes some bad habits ordeviations from the prescribed proto-cols. Standardizing all data collectorsto a gold-standard trainer ensuresthat a single protocol is followed andthat departures from the trainer arewithin acceptable limits.59
For extended research protocols orfor ongoing surveillance or clinicalactivities, having a gold-standardtrainer periodically visit and observemeasurements or take some replicate
TABLE 1 Data-Collection and Management Practices for Reducing Errors for Height, Weight, andBMI
Equipment and spaceChoose appropriate equipmentCheck and calibrate equipment regularlyKeep extra batteries for scalesProvide a private area for child measurements, if possibleMeasurement protocolsChose a protocol that matches that used in the growth chartsHave written copies of measurement protocols available for reviewTrain and standardize data collectorsMake sure data are recorded in the appropriate units (eg, kilograms, pounds)Make sure data are measured and recorded to the nearest unit specified in the protocol (eg, 0.1 cm forheight, 0.1 kg for weight)Collect some replicate measurements for assessment of reliability, if feasiblePersonnelUse as few observers as is feasible to take measurements, especially for research studiesIdentify observers on data-collection forms or data-entry programsData managementUse as exact ages as possibleHave unique identifiers for childrenCalculate BMI, percentiles, and z scores by using tables or computer programs
SUPPLEMENT ARTICLE
PEDIATRICS Volume 124, Supplement 1, September 2009 S11 by guest on December 10, 2020www.aappublications.org/newsDownloaded from

measurements will help prevent “drift”in the measurement techniques. Also,these opportunities can be used to cor-rect and recertify data collectors, ifnecessary.
Laminated copies of the measurementprotocols on-site provide a readilyavailable reminder for data collectorsconcerning child position, measure-ment landmarks, and local policiesregarding calibration, clothing, exclu-sion criteria, data recording, dataflow, etc.
In research settings a certain propor-tion of the measurements should berepeated to evaluate measurementreliability. The proportion required de-pends on the number of different ob-servers concerned, the number of chil-dren usually measured, and the periodover which reliability will be assessed.In general, there should be enoughreplicates to capture the variationamong data collectors and study de-sign features and to capture a fairlystable estimate of the mean differ-ences between replicates and the ac-companying SD. The SD of differencesbetween replicates is really a measureof variance, and the CIs for a variancebegin to stabilize at sample sizeslarger than 20 (in our case, 20 pairs ofmeasurements).60
As an example, for a hypothetical studyin school-aged children, a 3-personmeasurement team will visit 4 differ-ent schools during a month of datacollection. Each school has an averageof 30 children, and the team will aver-age �10 children measured per day.So, each school will require 3 days ofdata collection, and �120 childrenwill be measured. If a target of 25 rep-licates is sought for assessing mea-surement reliability, that amounts toan �20% sample. One simple ap-proach is to specify that the data col-lectors remeasure 2 children per dayand that a different data collector fromthe one who measured the child the
first time take the measurements.Over the course of the month of datacollection, the variation among observ-ers, schools, and any study drift willbe captured in the final reliability sam-ple, which should include data on�25children. For complicated protocolsthat involve many measurements oradministration of other instruments,children may contribute only a repli-cate for one of the measurements sothat the burden on any one child issmall and the total of 25 replicatesmay represent many more individualchildren. The calculation of the rele-vant measurement-reliability statis-tics has been explained elsewhere.27,61
If the measurement protocols specifythat duplicate measurements be rou-tinely collected for all subjects (as rec-ommended above), then these repli-cates can be used for assessingmeasurement reliability as long as allthe different data collectors involvedin the study take the replicates. If themean of replicate measurements willbe used in statistical analyses, themeasurement reliability should takethis into account.61 If different data col-lectors usually work on different days,then special scheduling may be re-quired to accommodate fully captur-ing the interobserver variation in thereliability sample.
Personnel
Experience shows that an advancedformal education is not required totake high-quality anthropometric mea-surements. Willing adults who willgive adequate attention to detail andwho meet the requirements for em-ployment are usually satisfactory.Members of the community who arefamiliar with the local ethos and jar-gon may be excellent data collectors.In some situations, like-gender ob-servers may make children and ado-lescents more comfortable with the
touching required for anthropometricmeasurements.
As mentioned previously, having asfew data collectors as is feasible forother practical demands will minimizeinterobserver measurement variation.Ensuring that unique observer codesare included on the data-collectionforms or data-entry computer pro-grams will aid in quality-assurance ac-tivities and can even be used in the sta-tistical analyses if consistent observermeasurement bias becomes apparent.
Data Management
Having chronological ages as exact aspossible is important for the accuratecalculation of percentiles and z scores,and they will aid in minimizing age-related variance in statistical analyseswhen children are grouped accordingto age. Chronological ages in years ex-pressed to at least 2 decimal pointsare sufficient for most applications;this will capture exact ages to thenearest 3 days. For children less than 5or 6 years of age it may be more con-venient to express age in months to 1decimal point, or in exact days.
Actual values for BMI, BMI percentiles,and BMI z scores are best calculatedby using computer programs to avoidcomputational errors. There are manyWeb sites with BMI calculators thatcan be found easily by using Internetsearches, including those providedby the CDC (http://apps.nccd.cdc.gov/dnpabmi/Calculator.aspx) and NationalInstitutes of Health (www.nhlbisupport.com/bmi/bminojs.htm).
In some settings where immediate pa-tient feedback or charting are con-ducted, calculating BMI by using tablesmay be preferred. Again, many Websites provide such tables; the only cau-tion is that some BMI tables are de-signed for adults and may not includethe low heights and weights observedin children.2
S12 HIMES by guest on December 10, 2020www.aappublications.org/newsDownloaded from

Exact BMI percentiles and BMI z scorescan be calculated by using Epi Info, afree, user-friendly and downloadablecomputer program developed by theCDC (www.cdc.gov/epiinfo). At the CDCWeb site, researchers can downloada program for SAS statistical analysissoftware that generates a data set con-taining the percentiles and z scores forall the anthropometric measurements(including BMI) in the 2000 CDC growthcharts (www.cdc.gov/nccdphp/dnpa/growthcharts/resources/sas.htm).
SELF-REPORTED HEIGHT, WEIGHT,AND BMI
Having older children and adolescentsreport their height and weight ratherthan having someone directlymeasurethem is attractive economically andlogistically. Costs of direct anthropo-metric measurements include addi-tional time, personnel, training, andequipment. Logistically, direct mea-surements require an in-person ex-amination, space, and additional timefor participants. If direct measure-ments of height and weight are re-quired, some study designs and data-collection strategies are summarilyinadequate or eliminated (eg, mailsurveys, classroom surveys, telephonesurveys). Of course, the appropriate-ness of using self-reports of height,weight, and BMI depends on the reli-ability, bias, validity, and specific ap-plications of these measures. In somecases, self-reported data may be all thatexist, so it is important to understand
when and how such data might beused appropriately.62
Measurement Reliability
No published data are available on re-liability in self-reported height andweight as narrowly defined previously(ie, the random error associated withthe same measurement being re-peated). Such data would comprisethe same children being asked fortheir reported height and weight atleast twice over a period of time insig-nificant for growth.
Reliability in self-reports has beenevaluated in adolescents, consideringreliability as the random errors asso-ciated with the differences betweenself-reported height, weight, and BMIand the corresponding measured di-mensions. A good summary measureof this reliability is the Pearson orinterclass correlation coefficient.
Correlation coefficients between re-ported and measured height, weight,and BMI are presented in Table 2 forsome selected studies that reportedthe correlations according to gender.Overall, the correlations for reportedand measured dimensions are rela-tively high, indicating that self-reportedvalues are generally reasonable prox-ies for the corresponding measuredvalues. On the basis of the correlationcoefficients, boys generally do a littlebetter than girls, and weight is usuallymore reliably reported than is height.Because self-reported BMI combines
the random errors in both height andweight, self-reported BMI generallyhas lower correlations with measuredBMI than corresponding associationsobserved for reported and measuredheight and weight.
The youngest-aged children includedin these studies were 11 to 12 yearsold, and correlations between self-reported and measured dimensions,especially height, are usually lowerat these ages than they are later inadolescence.64,70,71
A slightly different concern aboutyoung adolescents is that they are of-ten unable or decline to report theirheights andweights.62,72 In a study basedon US national-level data, 41% of 12-year-olds and 25% of 13-year-olds hadmissing data for weight.64 These ratescompared with 4% missing reportedweights in 15- and 16-year olds. It maybe that for youth aged 11 to 13 yearstheir height has not yet become asimportant to them as it will be as theyget older, and they may not have regu-lar opportunities to have their heightmeasured.
Measurement Bias
Although Pearson correlation coeffi-cients are useful indicators of relia-bility, they only provide average asso-ciations, and they only account forrandom errors between reported andmeasured values. Pearson correla-tions are blind to systematic errors orbias. Several different sources of bias
TABLE 2 Selected Studies With Interclass Correlation Coefficients for Reported and Measured Height, Weight, and BMI According to Gender
Source Group/Location Age or Grade Level n, Male/Female Height r Weight r BMI r
Male Female Male Female Male Female
Davis and Gergen63 Mexican American/US 12–19 y 392/437 0.86 0.86 0.95 0.93 0.87 0.85Himes and Faricy64 All/US 12–16 y 759/876 0.89 0.79 0.97 0.93 0.93 0.87Himes and Story65 American Indian/Minnesota 12–19 y 41/28 0.91 0.71 0.96 0.91 0.90 0.80Hauck et al66 American Indian/US 12–19 y 536 0.83 0.62 0.95 0.90 0.88 0.79Brener et al67 20 states/US Grades 9–12 957/1075 0.87 0.82 0.92 0.94 0.89 0.89Himes et al68 Minnesota/US 12–18 y 1936/1861 0.90 0.80 0.96 0.94 0.89 0.85Tsigilis69 Trikala, Greece Middle and high schools 141/159 0.94 0.93 0.97 0.97 0.90 0.94Median r 0.89 0.80 0.96 0.93 0.89 0.85
SUPPLEMENT ARTICLE
PEDIATRICS Volume 124, Supplement 1, September 2009 S13 by guest on December 10, 2020www.aappublications.org/newsDownloaded from

in self-reports of height and weighthave been investigated, and they wererecently reviewed for studies on USadolescents.62
For our discussion, it is important torecognize that the mean values of self-reported height are usually overesti-mated by �1 to 2 cm, and meanself-reported weight is usually under-estimated by 2 to 4 kg, especially soin girls.62,72 Thus, with overestimatedheight and underestimated weight,mean BMI values calculated from theself-reported data are usually less by2 to 3 BMI units (kg/m2) than if theywere measured.
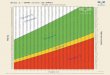
Another source of bias that is impor-tant for understanding how self-reported data might be used in evalu-ating overweight and obesity is relatedto the body size of the children and ad-olescents providing the self-reports.Themean differences for self-reportedvalues less measured values forheight, weight, and BMI are presentedin Fig 2 relative to categories of themeasured dimensions for a sampleof 3797 Minnesota youth aged 12 to18 years.68
For height, the errors in self-reportingare largely positive because most ofthe youth overestimated their heights(mean differences: boys, 1.2 cm; girls,2.4 cm). Nevertheless, a strong nega-tive relationship between the errorsin reporting height and the actualmeasured heights is evident so thatthe only group actually underestimat-ing height was the very tallest boys.For self-reported weight and BMI, theerrors in self-reports became increas-ingly negative (indicating underesti-mates) as categories of measuredweight and BMI increased, with steeperslopes in girls than in boys.
This pattern of underestimation meansthat the greatest impact of the biasin self-reported BMI will be to un-derestimate prevalences of over-weight and obesity defined by the
upper percentiles (eg, 85th, 95th). Forexample, in a separate study of highschool students by Brener et al,67 theprevalences for overweight (�85thpercentile) were 47.4% for directlymeasured BMI and 29.7% for self-reported BMI. Corresponding preva-lences for obesity (�95th percentile)were 26.0% for measured BMI and14.9% for self-reported BMI. Unfortu-nately, there is no easy conversionfrom a prevalence based on self-reported BMI to what it would have beenif height and weight were measured.
The biases in self-reports are entan-gled in idiosyncratic differences amongsamples in gender, age, underlyingdistributions of BMI, and perhapsrace, mental health, and socioeco-nomic status.62,68
Measurement Validity
From the evidence for bias discussedabove, it is not surprising that consid-erable misclassification occurs whenchildren and adolescents are identi-fied as overweight or obese on thebasis of self-reports and the BMI-percentile criteria. In the Brener et al67
study, the sensitivity and specificityof self-reported BMI for identifyingoverweight adolescents were 60.5%and 98.0%, respectively. Correspond-ing values for sensitivity and specific-ity for identifying obese individualswere 54.9% and 99.2%, respectively.So, as few as 55% (positive predictivevalue) of those who are truly over-weight will be correctly identified assuch when using BMI calculated fromself-reported heights and weights. Re-sults from other studies of validity arenot much more encouraging.62
The validity of BMI using self-reporteddata relative to total body fat has notbeen evaluated. Nevertheless, giventhe modest validity relative to mea-sured BMI, BMI derived from self-reported data must be even poorerthan measured BMI in its ability to cor-rectly identify the fattest individuals onthe basis of laboratory methods.
When Is It Appropriate to UseSelf-reported BMI?
In some situations, BMI derived fromself-reported data are the only dataavailable (eg, the CDC Youth Risk Be-havior Surveillance System,73 whichcollects data through telephone inter-views from a national sample). In othercases, the complexity and size of thesurvey make direct measurements im-practical.74 Nevertheless, any use of
FIGURE 2Mean differences between self-reported andmeasured body size adjusted for age, socio-economic status, and race/ethnicity, plottedagainst categories of the measured dimension:A, height; B, weight; C, BMI.68
S14 HIMES by guest on December 10, 2020www.aappublications.org/newsDownloaded from

self-reported height, weight, and BMIshould be done with an understandingof their limitations and biases despitethe obvious logistic and economic ad-vantages. Interpretation of findingsneeds to be couched accordingly.
For surveillance purposes, prevalencesof child and adolescent overweightand obesity are important for describ-ing the nature and extent of problems,monitoring trends or changes overtime, and comparing communities orregions for program priorities. An im-portant notion to understand here isthat prevalences of overweight andobesity based on self-reported BMIdata will almost certainly be under-estimates of the true prevalences, al-though to an unknown degree. Conse-quently, prevalences based on self-reported data should not be the basisof determining the extent of local prob-lems compared with prevalences re-ported in the scientific literature de-scribing national patterns and trendsand based on measured height andweight.
Although there are no specific datato elucidate whether biases in self-reports are fairly stable over time, it isnot unreasonable to assume that fac-tors related to reporting biases shouldnot dramatically change within thesame group over relatively short timeperiods (eg, 1–2 years). Consequently,with that assumption, it should be ac-ceptable to use prevalences from self-reported data to assess changes overtime within groups. When using thesame rationale, self-reported data maybe acceptable to use in some programevaluations, provided that interven-tions do not include behavioral or psy-chological components that may alterbody awareness or self-image thatmay be related to the biases in childreporting.75
Comparing prevalences of overweightor obesity among different locationsor groups by using self-reported data
are problematic, because the compar-ison assumes that all the possible fac-tors that contribute to the biases inreporting are the same, including theunderlying distribution of measuredBMI. Hence, if one concludes that thereare meaningful differences in preva-lences of child obesity on the basis ofself-reports, one had to arrive at thatconclusion by assuming that the un-derlying distribution of BMI was thesame.
Self-reported height, weight, and BMIshould not be used to assess body sizein clinical settings where diagnosticand therapeutic decisions are made.The individual variation in self-reportedvalues is impossible to predict, andthe consequences of misclassificationmay be serious. Certainly, for most re-search protocols, directly measuredheight, weight, and BMI are stronglyrecommended because they increasethe precision and accuracy of the esti-mates and they avoid the need to makeassumptions regarding BMI status dueto unmeasured factors.
PARENT-REPORTED HEIGHT,WEIGHT, AND BMI
If parents were able to accurately re-port the height and weight of theiryoung children, it would have many ofthe economic and logistic advantagesproposed for self-reports in older chil-dren. Unfortunately, there are far fewerdata directly evaluating the validity ofparental reports of child height andweight compared with those availablefor self-reports, and the results aremore difficult to generalize because ofdiffering study protocols and analyses,disparate child ages, and sometimesconflicting or even confusing results.
For parents to have reasonably accu-rate knowledge of their child’s heightand weight usually requires that theyhave either measured the child them-selves or been informed from theschool or clinic where someone else
measured them. Obviously, the morerecently the measurements weretaken, the more accurate the parentreports should be.
The fact that children continue to growafter the most recent measurement athome or clinic has lead some to con-clude that parental reports will alwaysunderestimate the measured heightand weight of children. Nevertheless,for most studies that make direct com-parisons, the mean parent-reportedchild height and weight were close tothe corresponding measured means,usually within �1 cm or �1 kg,76–80
and reasonably represented by under-estimates and overestimates of themeasured means. There are, however,exceptions. Mexican American moth-ers who participated in the US His-panic Health and Nutrition Examina-tion Survey (HHANES) consistentlyunderestimated the mean measuredheight of their children (6months to 11years) by 6 to 9 cm while reportingmean weight within 1 kg of the meanmeasured weight.63 Almost one fourthof the Mexican American mothers saidthat they did not know their child’sheight and weight and, thus, were un-able to report it. For a sample of 818Spanish children aged 6 to 8 years,mean parental-reported child heightwas 2.4 cm taller than the mean mea-sured height,81 and mean measuredweight was slightly overestimated but,again, within 1 kg.
The net effect on mean BMI calculatedfrom parental reports compared withthe mean of measured BMI in the avail-able studies is accordingly usuallysmall and within�1 kg/m2, except forthe Mexican American mothers in theUS Hispanic Health and Nutrition Exam-ination Survey, who substantially un-derestimated child height in their re-ports and, therefore, overestimatedthe mean BMI calculated from mea-sured height and weight.63
SUPPLEMENT ARTICLE
PEDIATRICS Volume 124, Supplement 1, September 2009 S15 by guest on December 10, 2020www.aappublications.org/newsDownloaded from

Although the average biases in paren-tal reports of height, weight, and BMItend to be rather small, there couldstill be systematic biases in parentalreports according to the measuredsize of the children, as occurs withself-reports in older children. The fewstudies that have investigated thisquestion indicated that parental re-ports of child weight tend to overesti-mate the lightest children and under-estimate the heaviest children, or aregression toward the overall mea-sured mean.63,76,80,82
From these reporting biases relatedto measured child size, one should ex-pect the prevalences of child over-weight and obesity based on parentalreports to systematically underesti-mate corresponding prevalences basedon measured BMI. Nevertheless, thestudies that have found both preva-lences of obesity are about equallyrepresented by those that found pa-rental reports to yield higher preva-lences of obesity compared with esti-mates based on measured BMI81,82
and those that found parental reportsto yield lower prevalences of obesi-ty.79,80 In a study that included parentsof Japanese children in the first andfourth grades, the differences betweenprevalences of obesity based on pa-rental reports and measured BMIwere small but in both directionswhen reported separately accordingto gender.77
From the available literature one mustconclude that prevalences of childobesity based on parental reports donot differ systematically or dramati-cally from corresponding prevalencesbased on direct measurements. In allof these studies differences betweenprevalences of childhood obesity de-termined by measurements and par-ent reports were small, usually within�5% (in the absolute prevalence).
After reviewing the available literatureonparental reportsof height andweight,
a few summary recommendationsemerge relative to appropriatenessfor studies and practices related tochild overweight and obesity. First, ofcourse, is that BMI derived from di-rectly measured height and weight isalways preferable to similar dataobtained from parental reports. Cer-tainly, in clinical settings where deci-sions concerning diagnosis or treat-ment are made, BMI assessmentsshould be made by using directly mea-sured height and weight. The probabil-ity of misclassification of individualsrelative to overweight or obesity sta-tus is simply too great to use parentalreports of child height and weight.
As when choosing to use BMI data cal-culated from self-reports of height andweight for any purpose, BMI estimatesfrom parental reports always shouldbe used with less certainty than corre-sponding data obtained from directmeasurements. One dimension of theuncertainty is that the direction of thebiases using parental reports com-pared with BMI estimates from directmeasurements are poorly understood,so one cannot reasonably concludethat the true mean BMI or prevalenceof obesity is more or less than that ob-tained from parental reports.
Accordingly, important decisions re-garding obesity trends and programsfor groups should not be based only oncomparisons of prevalences of childoverweight and obesity based on BMIderived from parental reports withthose from national or regional sur-veys that used directmeasurements ofheight andweight for estimates of BMI.While acknowledging the uncertaintyof BMI based on parental reports, itdoes not seem unreasonable to com-pare prevalences of overweight orobesity when similar approaches forobtaining the parental reports havebeen used for the estimateswhen suchdata are all that are available.
A strong recommendation is that thosewho use parental reports routinely intheir surveys develop research to vali-date this approach and to documentits reliability and validity. The availableliterature is simply too sparse to allowany reasonable conclusions to bedrawn regarding specific factors thatmay be related to unreliability or bi-ases in parental reports (eg, child age,gender of the parent, prevalence ofobesity, socioeconomic status, BMI ofparents, etc).
SKINFOLD THICKNESS
A skinfold thickness is the double layerof skin and subcutaneous fat (pannic-ulus adiposus) lifted as a fold andmea-sured with standardized calipers andmethodology at specific sites on thebody.83 The rationale for measuringskinfolds as an indicator of overweightand obesity is that subcutaneous fat ispart of and highly correlated with totalbody fat. Skinfolds have a long historyof use as an indicator of nutritionalstatus and body fatness, and their va-lidity andmeasurement properties arewell established.84,85
Skinfold-thickness measurements gen-erally are more highly correlated withtotal body fatness than is BMI,28,51,86
although the association varies bythe degree of body fatness. Skinfold-thickness cutoffs can correctly identifythe fattest children about as well asBMI.46,87,88 Nevertheless, for the presentdiscussion, skinfolds are of interest iftheir addition improves the accurateidentification of children as over-weight or obese beyond that providedby BMI alone. There are few data ad-dressing this specific question, al-though Mei et al46 found that triceps orsubscapular skinfold measurementsgreater than a series of cutoffs failedto improve the identification of the fat-test children (by dual-energy radio-graph absorptiometry) beyond thatachieved by using a 95th-percentile
S16 HIMES by guest on December 10, 2020www.aappublications.org/newsDownloaded from

cutoff for BMI. So, children with a BMIat the tail of the population distribu-tion (ie, �95th percentile) have littlemisclassification as the fattest be-cause there is little “hidden” muscu-larity or fatness.
There are several practical reasonsthatmake skinfolds challenging to use.Measurement reliabilities for skinfoldmeasurements are usually much lowerthan for height and weight,27 even inwell-trained hands. Attaining the maxi-mummeasurement reliabilities for skin-fold measurements requires substan-tial experience and regular practice,probably more than most personnelhave in clinical and community set-tings. Finally, there are no publishedreference percentiles available forskinfold thickness for US children, sono optimum percentile cutoffs havebeen defined.
In sum, skinfold-thickness measure-ments remain important in many re-search applications, but they cannotbe recommended as a routine part ofscreening, management, or surveil-lance of child and adolescent over-weight and obesity.
WAIST CIRCUMFERENCE
The measurement of waist circumfer-ence is an attempt to capture infor-mation regarding the distribution ofbody fat, in this case the visceral adi-pose tissue that has been linked to in-creased health risks and metabolicdisorders in children and adults.89,90 Inmultiple regression models, waist cir-cumference (as a continuous mea-sure) does better than BMI in predict-ing insulin resistance, blood pressure,serum cholesterol levels, and triglyc-eride levels,91–93 especially in adoles-cents. Also, the ratio of waist circum-ference to height has been shown to beassociated with cardiovascular riskfactors.94
Nevertheless, when it comes to accu-rately identifying the fattest children,
thresholds of waist circumference dono better than those of BMI or tricepsskinfold thickness.87 There is no infor-mation regarding any additional bene-fit of using waist circumference toidentify the fattest children once BMIcriteria have been applied.
Waist circumference is easier to mea-sure reliably than skinfolds, and inter-observer measurement reliabilities areusually intermediate between thosefor height and weight and those forskinfold thicknesses.27 Age-based per-centiles of waist circumference areavailable for US children,95 but no opti-mum cutoffs for identifying the fattestchildren have been developed.
Themain utility of waist circumferenceper se is as a measure of fat distribu-tion rather than total body fatness.Consequently, although some of thefindings regarding identifying adoles-cents at risk for concurrent or futuremorbidity are important, there is littleto indicate that including waist cir-cumference adds appreciably in theidentification of the fattest individualsbeyond what is available with BMI. Ac-cordingly, waist circumference is notrecommended to be routinely includedin screening and surveillance for childand adolescent overweight and obesity.
PERCENTAGE BODY FAT FROMBIOELECTRICAL IMPEDANCE
Bioelectrical impedance analysis (BIA)measures the opposition of body tis-sues to a small (�1-mA) alternatingcurrent that is imperceptible to thesubject. Because bioelectrical imped-ance differs between lean tissue (be-cause of its water content) and fat tis-sue, BIA combined with body heightmay be used to estimate body water,fat-free mass, and body fat.96 Totalbody fat may then be divided by bodyweight and multiplied by 100 to yieldthe percentage of body weight that isfat. BIA has gained popularity because
it is noninvasive, portable, and reliablymeasured.97 Measurement reliabilitiesfor BIA are generally high and can ap-proach those for height and weight.98
The best studies of the validity of BIA inestimating total body fat use empiricalequations that relate themeasured re-sistance and reactance and child an-thropometry to an independent crite-rion measure of total body fat. It turnsout that the BIA prediction equationsare closely tied to the referent popula-tion, so different equations can yielddifferent body-fat estimates for chil-dren in other samples with the sameBMI.99 Consequently, although mea-sured with good reliability, biases re-sulting from prediction equations thatjust do not fit right in the populationstudied are a concern with BIA.
With the introduction of simple foot-to-foot BIA assessments that just requirethat the child step on scales with elec-trode foot plates, BIA has become in-creasingly popular because the childis not required to lay quietly supine forthe procedure. Nevertheless, somemodels of the foot-to-foot BIA appara-tus only provide the summary mea-sure of percentage body fat, and thedetails of the resistance, reactance,equations, or the referent populationare not available. Accordingly, one isleft to only hope that the equations areappropriate in a particular population.In a study of overweight and obese ad-olescents, foot-to-foot estimates un-derestimated total percent body fat by2% to 3% body fat.100
Another practical concern for usingBIA to estimate overweight and obesityis that there are no percentile refer-ence data for percent body fat in USchildren and no criterion thresholdsestablished to identify those at great-est health risk. Means and SDs for per-cent body fat for US adolescents olderthan 12 years derived from BIA havebeen published.101
SUPPLEMENT ARTICLE
PEDIATRICS Volume 124, Supplement 1, September 2009 S17 by guest on December 10, 2020www.aappublications.org/newsDownloaded from

With BIA, then, one is left with a techni-cally excellent method but with practi-cal constraints (need for appropriateequations and reference data) thatlimit its usefulness in most settingswhere identification and managementof overweight and obesity are con-ducted. Consequently, BIA is not rec-ommended for routine use in additionto assessment using BMI. More de-tailed descriptions of BIA and othermeasures of body composition havebeen elaborated elsewhere.97,102
SUMMARY AND CONCLUSIONS
BMI is an important indicator of over-weight and obesity in childhood andadolescence. Whenmeasurements aretaken carefully and compared with
appropriate growth charts and recom-mended cutoffs, BMI provides an ex-cellent indicator of overweight andobesity sufficient for most clinical,screening, and surveillance purposes.
Accurate measurements of height andweight require that adequate attentionbe given to data collection and man-agement. Choosing appropriate equip-ment and measurement protocols andproviding regular training and stan-dardization of data collectors are crit-ical aspects that apply to all settings inwhich BMI will be measured and used.
Proxy measures for directly measuredBMI, such as self-reports or parentalreports of height andweight, aremuchless preferred and should only be usedwith caution and cognizance of the
limitations, biases, and uncertaintiesattending these measures.
There is little evidence that other mea-sures of body fat such as skinfolds,waist circumference, or bioelectricalimpedance are sufficiently practicableor provide appreciable added informa-tion to be used in the identification ofchildren and adolescents who areoverweight or obese. Consequently, formost clinical, school, or communitysettings these measures are not rec-ommended for routine practice. Thesealternative measures of fatness re-main important for research and per-haps in some specialized screeningsituations that include a specific focuson risk factors for cardiovascular ordiabetic disease.
REFERENCES
1. Freedman DS, Sherry B. The validity of BMI as an index of body fatness and risk among children.Pediatrics. 2009;124(3 suppl):S23–S34
2. Himes JH, Dietz WH. Guidelines for overweight in adolescent preventive services: recommenda-tions from an expert committee. The Expert Committee on Clinical Guidelines for Overweight inAdolescent Preventive Services. Am J Clin Nutr. 1994;59(2):307–316
3. Barlow SE, Dietz WH. Obesity evaluation and treatment: Expert Committee recommendations. TheMaternal and Child Health Bureau, Health Resources and Services Administration, and theDepartment of Health and Human Services. Pediatrics. 1998;102(3). Available at: www.pediatrics.org/cgi/content/full/102/3/e29
4. Krebs NF, Himes JH, Jacobson D, Nicklas TA, Guilday P, Styne D. Assessment of child and adoles-cent overweight and obesity. Pediatrics. 2007;120(suppl 4):S193–S228
5. Nunnally JC. Psychometric Theory. 2nd ed. New York, NY: McGraw-Hill Publishing Company; 1978
6. Zeller RA, Carmines EG.Measurement in the Social Sciences: The Link Between Theory and Data.Cambridge, United Kingdom: Cambridge University Press; 1980
7. Rao DH, Sastry JG. Day-to-day variation in body weights of children. Ann Hum Biol. 1976;3(1):75–76
8. Lampl M, Birch L, Picciano MF, JohnsonML, Frongillo EA Jr. Child factor in measurement depend-ability. Am J Hum Biol. 2001;13(4):548–557
9. Wasse M. Part of a letter from the Reverand Mr. Wasse, Rector of Aynho in Northamptonshire, toDr. Mead, concerning the difference in the height of a human body between morning and night.Philos Trans (1683–1775). 1724;33:87–88
10. Roberts N, Hogg D, Whitehouse GH, Dangerfield P. Quantitative analysis of diurnal variation involume and water content of lumbar intervertebral discs. Clin Anat. 1998;11(1):1–8
11. Strickland AL, Shearin RB. Diurnal height variation in children. J Pediatr. 1972;80(6):1023–1025
12. Voss LD, Bailey BJ. Diurnal variation in stature: is stretching the answer? Arch Dis Child. 1997;77(4):319–322
13. Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, et al. CDC growth charts: United States. Adv Data.2000;(314):1–27
14. Khosla T, Billewicz WZ. Measurement of change in body-weight. Br J Nutr. 1964;18(PubMed did notprovide):227–239
15. Marshall EL. A review of American research on seasonal variation in stature and body weight.J Pediatr. 1937;10:819–831
16. Brown KH, Black RE, Becker S. Seasonal changes in nutritional status and the prevalence of
S18 HIMES by guest on December 10, 2020www.aappublications.org/newsDownloaded from

malnutrition in a longitudinal study of young children in rural Bangladesh. Am J Clin Nutr.1982;36(2):303–313
17. Maleta K, Virtanen SM, Espo M, Kulmala T, Ashorn P. Seasonality of growth and the relationshipbetween weight and height gain in children under three years of age in rural Malawi. ActaPaediatr. 2003;92(4):491–497
18. Bransby ER. The seasonal growth of children. Med Off. 1945;73:149–151; 157–159; 165–168
19. Cole TJ. Seasonal effects on physical growth and development. In: Ulijaszek SJ, Strickland SS,eds. Seasonality and Human Ecology: 35th Symposium Volume of the Society for the Study ofHuman Biology. Cambridge, United Kingdom: Cambridge University Press; 1993:89–106
20. Ikeda M, Watanabe T. Constant growth of primary school children throughout four seasons ofyear. Tohoku J Exp Med. 1985;145(4):413–418
21. Roche AF, Himes JH. Incremental growth charts. Am J Clin Nutr. 1980;33(9):2041–2052
22. von Hippel PT, Powell B, Downey DB, Rowland NJ. The effect of school on overweight in childhood:gain in bodymass index during the school year and during summer vacation. Am J Public Health.2007;97(4):696–702
23. Roche AF, Sun SS. Human Growth: Assessment and Interpretation. Cambridge, United Kingdom:Cambridge University Press; 2003
24. Ahmed ML, Yudkin PL, Macfarlane JA, McPherson K, Dunger DB. Are measurements of heightmade by health visitors sufficiently accurate for routine screening of growth? Arch Dis Child.1990;65(12):1345–1348
25. Cotterill AM, Majrowski WH, Hearn SJ, Jenkins S, Savage MO. Assessment of the reliability ofschool nurse height measurements in an inner-city population. (The Hackney Growth Initiative).Child Care Health Dev. 1993;19(3):159–165
26. Lipman TH, Hench KD, Benyi T, et al. A multicentre randomised controlled trial of an interventionto improve the accuracy of linear growth measurement. Arch Dis Child. 2004;89(4):342–346
27. Ulijaszek SJ, Kerr DA. Anthropometric measurement error and the assessment of nutritionalstatus. Br J Nutr. 1999;82(3):165–177
28. Himes JH, Bouchard C. Validity of anthropometry in classifying youths as obese. Int J Obes.1989;13(2):183–193
29. Barlow S; Expert Committee. Expert Committee recommendations regarding the prevention,assessment, and treatment of child and adolescent overweight and obesity: summary report.Pediatrics. 2007;120(suppl 4):S164–192
30. Must A, Dallal GE, Dietz WH. Reference data for obesity: 85th and 95th percentiles of body massindex (wt/ht2) and triceps skinfold thickness. Am J Clin Nutr. 1991;53(4):839–846
31. Bellizzi MC, Dietz WH. Workshop on childhood obesity: summary of the discussion. Am J Clin Nutr.1999;70(1 pt 2):173S–175S
32. World Health Organization. Obesity: Preventing and Managing the Global Epidemic—Report of aWHO Consultation on Obesity, Geneva, 3–5 June 1997. Geneva, Switzerland: World HealthOrganization; 1998
33. Li M, Dibley MJ, Sibbritt D, Yan H. An assessment of adolescent overweight and obesity in Xi’anCity, China. Int J Pediatr Obes. 2006;1(1):50–58
34. Laxmaiah A, Nagalla B, Vijayaraghavan K, Nair M. Factors affecting prevalence of overweightamong 12- to 17-year-old urban adolescents in Hyderabad, India. Obesity (Silver Spring). 2007;15(6):1384–1390
35. de Onis M, Garza C, Onyango AW, Martorell R. WHO child growth standards. Acta Paediatr.2006;95(suppl 450):1–101
36. de OnisM, Garza C, Victora CG, Onyango AW, Frongillo EA, Martines J. TheWHOMulticentre GrowthReference Study: planning, study design, and methodology. Food Nutr Bull. 2004;25(1):S15–26
37. de OnisM, Garza C, Onyango AW, Borghi E. Comparison of theWHO child growth standards and theCDC 2000 growth charts. J Nutr. 2007;137(1):144–148
38. Mei Z, Ogden CL, Flegal KM, Grummer-Strawn LM. Comparison of the prevalence of shortness,underweight, and overweight among US children aged 0 to 59 months by using the CDC 2000 andthe WHO 2006 growth charts. J Pediatr. 2008;153(5):622–628
39. de Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growthreference for school-aged children and adolescents. Bull World Health Organ. 2007;85(9):660–667
40. Hamill PV, Drizd TA, Johnson CL, Reed RB, Roche AF. NCHS growth curves for children birth-18years: United States. Vital Health Stat 11. 1977;(165):i–iv, 1–74
41. Himes JH. Agreement among anthropometric indicators identifying the fattest adolescents. Int JObes Relat Metab Disord. 1999;23(suppl 2):S18–S21
SUPPLEMENT ARTICLE
PEDIATRICS Volume 124, Supplement 1, September 2009 S19 by guest on December 10, 2020www.aappublications.org/newsDownloaded from

42. Krebs NF, Jacobson MS; American Academy of Pediatrics, Committee on Nutrition. Prevention ofpediatric overweight and obesity. Pediatrics. 2003;112(2):424–430
43. Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR, Flegal KM. Prevalence of overweight andobesity among US children, adolescents, and adults, 1999–2002. JAMA. 2004;291(23):2847–2850
44. Koplan J, Liverman C, Kraak V. Preventing Childhood Obesity: Health in the Balance. Washington,DC: National Academies Press; 2005
45. Freedman DS, Wang J, Maynard LM, et al. Relation of BMI to fat and fat-freemass among childrenand adolescents. Int J Obes (Lond). 2005;29(1):1–8
46. Mei Z, Grummer-Strawn LM, Wang J, et al. Do skinfold measurements provide additional infor-mation to body mass index in the assessment of body fatness among children and adolescents?Pediatrics. 2007;119(6). Available at: www.pediatrics.org/cgi/content/full/119/6/e1306
47. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweightand obesity worldwide: international survey. BMJ. 2000;320(7244):1240–1243
48. National Institutes of Health. Clinical guidelines on the identification, evaluation, and treatmentof overweight and obesity in adults: the evidence report [published correction appears in ObesRes. 1998;6(6):464]. Obes Res. 1998;6(suppl 2):51S–209S
49. Wilson EB. Probable inference, the law of succession, and statistical inference. J Am Stat Assoc.1927;22(158):202–212
50. Newcombe RG. Two-sided confidence intervals for the single proportion: comparison of sevenmethods. Stat Med. 1998;17(8):857–872
51. Freedman DS, Wang J, Ogden CL, et al. The prediction of body fatness by BMI and skinfoldthicknesses among children and adolescents. Ann Hum Biol. 2007;34(2):183–194
52. Guo SS, Roche AF, Chumlea WC, Johnson C, Kuczmarski RJ, Curtin R. Statistical effects of varyingsample sizes on the precision of percentile estimates. Am J Hum Biol. 2000;12(1):64–74
53. World Health Organization. Physical Status: The Use and Interpretation of Anthropometry—Report of a WHO Expert Committee. Geneva, Switzerland: World Health Organization; 1995. WHOtechnical report series 854
54. Styne D. Growth. In: Greenspan FS, Gardner DG, eds. Basic and Clinical Endocrinology. 6th ed. NewYork, NY: Lange Medical Books/McGraw Hill; 2001:163–200
55. Gordon CC, Chumlea WC, Roche AF. Stature, recumbent length, and weight. In: Lohman TG, RocheAF, Martorell R, eds. Anthropometric Standardization Reference Manual. Champaign, IL: HumanKinetics Books; 1988:3–8
56. Zeman J, Cassano M, Perry-Parrish C, Stegall S. Emotion regulation in children and adolescents.J Dev Behav Pediatr. 2006;27(2):155–168
57. Lohman T, Roche A, Martorell R, eds. Anthropometric Standardization Reference Manual. Cham-paign, IL: Human Kinetics Books; 1988
58. Cameron N. The Measurement of Human Growth. London, United Kingdom: Croom Helm; 1984
59. Habicht JP. Standardization of quantitative epidemiological methods in the field [in Spanish]. BolOficina Sanit Panam. 1974;76(5):375–384
60. Tate RF, Klett GW. Optimal confidence intervals for the variance of a normal distribution. J AmStat Assoc. 1959;54(287):674–682
61. Himes JH. Reliability of anthropometric methods and replicate measurements. Am J Phys An-thropol. 1989;79(1):77–80
62. Sherry B, Jefferds ME, Grummer-Strawn LM. Accuracy of adolescent self-report of height andweight in assessing overweight status: a literature review. Arch Pediatr Adolesc Med. 2007;161(12):1154–1161
63. Davis H, Gergen PJ. Mexican-American mothers’ reports of the weights and heights of children 6months through 11 years old. J Am Diet Assoc. 1994;94(5):512–516
64. Himes JH, Faricy A. Validity and reliability of self-reported stature and weight of US adolescents.Am J Hum Biol. 2001;13(2):255–260
65. Himes JH, Story M. Validity of self-reported weight and stature of American Indian youth. J Ado-lesc Health. 1992;13(2):118–120
66. Hauck FR, White L, Cao G, Woolf N, Strauss K. Inaccuracy of self-reported weights and heightsamong American Indian adolescents. Ann Epidemiol. 1995;5(5):386–392
67. Brener ND, McManus T, Galuska DA, Lowry R, Wechsler H. Reliability and validity of self-reportedheight and weight among high school students. J Adolesc Health. 2003;32(4):281–287
68. Himes JH, Hannan P, Wall M, Neumark-Sztainer D. Factors associated with errors in self-reportsof stature, weight, and body mass index in Minnesota adolescents. Ann Epidemiol. 2005;15(4):272–278
S20 HIMES by guest on December 10, 2020www.aappublications.org/newsDownloaded from

69. Tsigilis N. Can secondary school students’ self-reported measures of height and weight betrusted? An effect size approach. Eur J Public Health. 2006;16(5):532–535
70. Brooks-Gunn J, WarrenMP, Rosso J, Gargiulo J. Validity of self-report measures of girls’ pubertalstatus. Child Dev. 1987;58(3):829–841
71. Shannon B, Smiciklas-Wright H, Wang MQ. Inaccuracies in self-reported weights and heights of asample of sixth-grade children. J Am Diet Assoc. 1991;91(6):675–678
72. Jansen W, van de Looij-Jansen PM, Ferreira I, de Wilde EJ, Brug J. Differences in measured andself-reported height and weight in Dutch adolescents. Ann Nutr Metab. 2006;50(4):339–346
73. Kolbe LJ, Kann L, Collins JL. Overview of the Youth Risk Behavior Surveillance System. PublicHealth Rep. 1993;108(suppl 1):2–10
74. Neumark-Sztainer D, Wall M, Haines J, Story M, Eisenberg ME. Why does dieting predict weightgain in adolescents? Findings from project EAT-II: a 5-year longitudinal study. J Am Diet Assoc.2007;107(3):448–455
75. Neumark-Sztainer D, Story M, Hannan PJ, Perry CL, Irving LM. Weight-related concerns andbehaviors among overweight and nonoverweight adolescents: implications for preventingweight-related disorders. Arch Pediatr Adolesc Med. 2002;156(2):171–178
76. Wing RR, Epstein LH, Neff D. Accuracy of parents’ reports of height and weight. J Behav Assess.1980;2(2):105–110
77. Sekine M, Yamagami T, Hamanishi S, Kagamimori S. Accuracy of the estimated prevalence ofchildhood obesity from height and weight values reported by parents: results of the ToyamaBirth Cohort study. J Epidemiol. 2002;12(1):9–13
78. Huybrechts I, De Bacquer D, Van Trimpont I, De Backer G, De Henauw S. Validity of parentallyreported weight and height for preschool-aged children in Belgium and its impact on classifi-cation into body mass index categories. Pediatrics. 2006;118(5):2109–2118
79. Dubois L, Girad M. Accuracy of maternal reports of pre-schoolers’ weights and heights asestimates of BMI values. Int J Epidemiol. 2007;36(1):132–138
80. Scholtens S, Brunekreef B, Visscher TL, et al. Reported versus measured body weight and heightof 4-year-old children and the prevalence of overweight. Eur J Public Health. 2007;17(4):369–374
81. Garcia-Marcos L, Valverde-Molina J, Sanchez-Solis M, et al. Validity of parent-reported height andweight for defining obesity among asthmatic and nonasthmatic schoolchildren. Int Arch AllergyImmunol. 2006;139(2):139–145
82. Akerman A, Williams ME, Meunier J. Perception versus reality: an exploration of children’smeasured body mass in relation to caregivers’ estimates. J Health Psychol. 2007;12(6):871–882
83. Harrison GG, Buskirk ER, Carter JEL, et al. Skinfold thicknesses and measurement technique. In:Lohman TG, Roche AF, Martorell R, eds. Anthropometric Standardization Reference Manual.Champaign, IL: Human Kinetics Books; 1988:55–70
84. Himes J. Subcutaneous fat thickness as an indicator of nutritional status. In: Green L, JohnstonP, eds. Social and Biological Predictors of Nutritional Status, Physical Growth, and NeurologicalDevelopment. New York, NY: Academic Press; 1980:9–32
85. Norgan NG. Anthropometric assessment of body fat and fatness. In: Himes JH, ed. Anthropomet-ric Assessment of Nutritional Status. New York, NY: Wiley-Liss; 1991:197–212
86. Roche AF, Sievogel RM, Chumlea WC, Webb P. Grading body fatness from limited anthropometricdata. Am J Clin Nutr. 1981;34(12):2831–2838
87. Sarría A, Moreno LA, Garcia-Llop LA, Fleta J, Morellon MP, Bueno M. Body mass index, tricepsskinfold and waist circumference in screening for adiposity in male children and adolescents.Acta Paediatr. 2001;90(4):387–392
88. Bedogni G, Iughetti L, Ferrari M, et al. Sensitivity and specificity of body mass index and skinfoldthicknesses in detecting excess adiposity in children aged 8–12 years. Ann Hum Biol. 2003;30(2):132–139
89. Katzmarzyk PT, Srinivasan SR, Chen W, Malina RM, Bouchard C, Berenson GS. Body mass index,waist circumference, and clustering of cardiovascular disease risk factors in a biracial sampleof children and adolescents. Pediatrics. 2004;114(2). Available at: www.pediatrics.org/cgi/content/full/114/2/e198
90. Gower BA, Nagy TR, Goran MI. Visceral fat, insulin sensitivity, and lipids in prepubertal children.Diabetes. 1999;48(8):1515–1521
91. Lee S, Bacha F, Gungor N, Arslanian SA. Waist circumference is an independent predictor ofinsulin resistance in black and white youths. J Pediatr. 2006;148(2):188–194
92. Maffeis C, Pietrobelli A, Grezzani A, Provera S, Tato L. Waist circumference and cardiovascularrisk factors in prepubertal children. Obes Res. 2001;9(3):179–187
93. Savva SC, Tornaritis M, Savva ME, et al. Waist circumference and waist-to-height ratio are better
SUPPLEMENT ARTICLE
PEDIATRICS Volume 124, Supplement 1, September 2009 S21 by guest on December 10, 2020www.aappublications.org/newsDownloaded from

predictors of cardiovascular disease risk factors in children than body mass index. Int J ObesRelat Metab Disord. 2000;24(11):1453–1458
94. Kahn HS, Imperatore G, Cheng YJ. A population-based comparison of BMI percentiles and waist-to-height ratio for identifying cardiovascular risk in youth. J Pediatr. 2005;146(4):482–488
95. Fernandez JR, Redden DT, Pietrobelli A, Allison DB. Waist circumference percentiles in nationallyrepresentative samples of African-American, European-American, and Mexican-American chil-dren and adolescents. J Pediatr. 2004;145(4):439–444
96. Kyle UG, Bosaeus I, De Lorenzo AD, et al. Bioelectrical impedance analysis: part I—review ofprinciples and methods. Clin Nutr. 2004;23(5):1226–1243
97. Heyward VH, Wagner DR. Applied Body Composition Assessment. 2nd ed. Champaign, IL: HumanKinetics; 2004
98. Kettaneh A, Heude B, Lommez A, Borys JM, Ducimetiere P, CharlesMA. Reliability of bioimpedanceanalysis compared with other adiposity measurements in children: the FLVS II Study. DiabetesMetab. 2005;31(6):534–541
99. Williams J, Wake M, Campbell M. Comparing estimates of body fat in children using publishedbioelectrical impedance analysis equations. Int J Pediatr Obes. 2007;2(3):174–179
100. Lazzer S, Boirie Y, Meyer M, Vermorel M. Evaluation of two foot-to-foot bioelectrical impedanceanalysers to assess body composition in overweight and obese adolescents. Br J Nutr. 2003;90(5):987–992
101. Chumlea WC, Guo SS, Kuczmarski RJ, et al. Body composition estimates from NHANES III bioelec-trical impedance data. Int J Obes Relat Metab Disord. 2002;26(12):1596–1609
102. Heymsfield SB, Lohman TG, Wang ZM, Going SB, eds. Human Body Composition. 2nd ed. Cham-paign, IL: Human Kinetics; 2005
S22 HIMES by guest on December 10, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2008-3586D2009;124;s3Pediatrics
John H. HimesObesity in Children
Challenges of Accurately Measuring and Using BMI and Other Indicators of
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/124/Supplement_1/s3including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/124/Supplement_1/s3#BIBLThis article cites 80 articles, 17 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/obesity_new_subObesityhttp://www.aappublications.org/cgi/collection/chapters_views_newsChapters Views & Newshttp://www.aappublications.org/cgi/collection/endocrinology_subEndocrinologycollection(s): This article, along with others on similar topics, appears in the following
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlits entirety can be found online at: Information about reproducing this article in parts (figures, tables) or in
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on December 10, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2008-3586D2009;124;s3Pediatrics
John H. HimesObesity in Children
Challenges of Accurately Measuring and Using BMI and Other Indicators of
http://pediatrics.aappublications.org/content/124/Supplement_1/s3on the World Wide Web at:
The online version of this article, along with updated information and services, is located
American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2009 by thebeen published continuously since 1948. Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it has
by guest on December 10, 2020www.aappublications.org/newsDownloaded from