Embed Size (px)
Citation preview

CHALLENGES IN IDENTIFYING SLEEP STAGES FROM PATIENTS TREATED WITH SEDATIVE-HYPNOTIC DRUGS AND ANTIDEPRESSANTS
Acda RN, Fernandez A, Raman S, Williams V, Fafowora O
Integrated Sleep Disorders Center, McGuire Veterans Medical Center, Richmond, VA
INTRODUCTION:In February 2016, results of a study released by the U.S.Centers for Disease Control and Prevention (CDC) indicatedthat more than a third of American adults are not gettingenough sleep on a regular basis. As of 2010, about 4% ofadult Americans take prescription sleep aids, while close to13% of Americans over the age of 12 reported use of anti-depressants in 2014.
IMPLICATIONSPerforming diagnostics and application of therapeutic PAPtreatments during live acquisitions often involve qualitativeand appreciable decision making processes from aregistered technologist or technician. Historically, it hasbeen understood that staging polysomnograms havetendencies to be subjective in nature as shown in recentAASM Sleep ISR with varying degrees of difficulty.Contributing factors such as pharmacological effects inrelation to a person’s sleep architecture,electroencephalography (EEG), electrooculography (EOG)and electromyogram (EMG) are common challenges thattechnologists encounter in delivering quality staging forphysicians and care to patients.
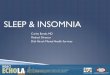
Shown in Figure 1.0 is a perfect example of stagingdisagreements where only 9.07% of the total population ofSleep ISR takers agreed with the Gold Standard. Much worseyet is the percentage that are in Full Agreement with theassessment of this particular epoch at 5.27%..
Antidepressants include tricyclic agents (TCAs), monoamine oxidaseinhibitors (MAOIs), serotonin antagonist reuptake inhibitors (SARIs),and selective serotonin reuptake inhibitors (SSRIs). Some physicianshave been prescribing antidepressants due to the strong bi-directional correlation between depression and insomnia.
EFFECTS ON SLEEP QUALITYVariable effects on sleep quality have been observed on differentkinds of antidepressants. Some are sedating while others arestimulating.
EFFECTS ON SLEEP ARCHITECTURE- Suppresses Stage R sleep except for SARIs- Increases latency to the onset of Stage R sleep (See Fig 3.0)- SSRIs appear to increase stage N1 sleep- REM rebound (exaggerated) effects have been observed when
they are abruptly stopped
POTENTIAL PITFALLS- An observed effect of antidepressants is excessive EOG activity
(commonly referred as Prozac Eyes). Technologists usuallymistaken epochs such as shown in Figure 2.0 as Stage R.
- Figure 2.1 shows the same subject’s real Stage R. Please notethe differences in EEG and EMG amplitude against Fig 2.0.
REFERENCES1. Liu Y, Wheaton AG, Chapman DP, Cunningham TJ, Lu H, Croft JB. Prevalence of healthy sleep duration among adults — United States, 2014. MMWR Morb Mortal Wkly Rep. 2016;65(6):137–141.2. Chong Y, Fryar CD, Gu Q. Prescription sleep aid use among adults: United States, 2005–2010. NCHS data brief, no 127. Hyattsville, MD: National Center for Health Statistics. 2013.3. Pratt LA, Brody DJ, Gu Q. Antidepressant use among persons aged 12 and over: United States, 2011–2014. NCHS data brief, no 283. Hyattsville, MD: National Center for Health Statistics. 20174. Kilduff TS, Mendelson WB. Mechanisms of action and pharmacologic effects. In: Principles and Practices of Sleep Medicine, 6th ed, Kryger MH, Roth T, Dement WC (Eds), Elsevier Saunders, St Louis, MO 2016. p.424.5. Buysse DJ, Tyagi S. Clinical pharmacology of other drugs used as hypnotics. In: Principles and Practices of Sleep Medicine, 6th ed, Kryger MH, Roth T, Dement WC (Eds), Elsevier Saunders, St Louis, MO 2016. p.432.6. Chawala, J, MD. "Insomnia Medication." Medscape. Updated: Aug 01, 2016.7. Pagel, J.F, and Parnes, B.L., 2001, Medication for the Treatment of Sleep Disorders: An Overview, Primary care Companion p118-125.
Benzodiazepines, barbiturates and nonbenzodiazepine receptoragonists are sedative-hypnotics medications prescribed to slowdown the body's functions. Over the years, barbiturates has largelybeen replaced by benzodiazepines and nonbenzodiazepine drugsdue to the lower risk of addiction and overdose.
EFFECTS ON SLEEP QUALITYReduced time to sleep onset and potentially reduce wakefulnessand increase the total sleep time.
EFFECTS ON SLEEP ARCHITECTURE- Reduces the amount of stage N1 sleep.- Potentially increases spindle activity during N2- Modestly reduces rapid eye movement (REM) sleep when used
at higher than indicated doses.
POTENTIAL PITFALLS- Patients with advanced Parkinson’s Disease are usually
prescribed with sedative-hypnotics to help reduce wakefulness.Due to slowing of the alpha rhythm and increase of activity inslower frequencies, techs need to practice vigilance in scoringNREM and Wake transitions as PD patients often suffer fromthe worst cases of disrupted sleep.
- Traditionally, the success of PAP therapy depends on a patient’sresponse resulting in Stage R. Increasing PAP pressures in thehopes of “forcing” REM should be discouraged as it may lead toadditional discomfort and PAP-induced events (Fig 3.0).
- Figure 3.0 shows Central Apneas being observed due tocontinuous increase in PAP pressure despite the absence ofrespiratory events.
ANTIDEPRESSANTS
CONCLUSIONRecognizing the possible pharmacological effects on apatient’s sleep architecture is very important in aidingtechnologists and other sleep professionals in stagingpolysomnograms based on usual interpretation methodsthat are applied to the majority of acquisitions. Being ableto appropriately score and stage acquisitions of varyingdegrees of difficulty helps in minimizing misdiagnosis,delays in diagnosis and treatments, as well as results inbetter overall patient engagement and outcomes.
SEDATIVE-HYPNOTICS Below are lists of the most commonly prescribed antidepressantsand sedative-hypnotics. Please note that this is not acomprehensive list of drugs that may be available in the markettoday.

Impact of montelukast and fluticasone on quality of life in mild pediatric sleep apneaAndrew E Bluher, MD1, Craig C Brawley, MD2, Tina D Cunningham, PhD3, Cristina M Baldassari, MD4
1 Department of Otolaryngology – Head and Neck Surgery, Eastern Virginia Medical School, Norfolk, Virginia, USA2 Department of Otolaryngology – Head and Neck Surgery, Northwestern University Feinberg School of Medicine, Chicago, Illinois, USA 3 Healthcare Delivery Science Program, Eastern Virginia Medical School, Norfolk, Virginia, USA4 Department of Pediatric Otolaryngology, Children’s Hospital of The King’s Daughters, Norfolk, Virginia, USA
Research has shown improvement in apnea-
hypopnea index in children with mild obstructive sleep
apnea treated with anti-inflammatory medications.
Data on quality of life outcomes in children receiving
these medications is lacking. We aim to assess
quality of life in children with mild obstructive sleep
apnea treated with montelukast and fluticasone.
Children between 3 and 16 years old with mild sleep
apnea (apnea-hypopnea index > 1 and ≤5)
presenting to a tertiary care hospital were recruited
prospectively and treated with 4 months oxf
montelukast and fluticasone. Subjects’ caregivers
completed the OSA-18, a validated quality of life
survey, at baseline and 4 months. Children with
ongoing obstruction at follow-up underwent
adenotonsillectomy.
A power analysis was conducted prior to undertaking
this study. A group size of 16 was deemed sufficient
to detect a 20-point difference in OSA-18 QOL scores
with 80% power and a .05 significance level.
Descriptive statistics were reported. Means and
standard deviations were used for continuous
outcomes and frequencies and counts were used for
categorical outcomes. Paired t-test was used to
compare continuous outcomes between baseline and
follow-up, and two-sample t-test was utilized to detect
differences between groups. To investigate factors
that were associated with failure of medical therapy,
logistic regression models were fitted. Odds ratios
and 95% confidence intervals were reported. The
analysis was performed using SAS software version
9.3 (SAS Institute, Cary, North Carolina).
Thirty-one patients were included. Mean (SD) age was
6.8 (3.9) years. Most subjects (54.8%) were black and
48% were obese. Mean (SD) apnea-hypopnea index of
the subjects was 2.8 (1.0). The mean (SD) baseline
OSA-18 score was 60.2 (18.5), indicating a moderate
impact of sleep disturbance on quality of life. Following
treatment, there was significant improvement (p<0.005)
in mean OSA-18 score. Four children discontinued
montelukast due to behavioral side effects. Seven
children (22%) underwent adenotonsillectomy after failing
medical therapy. Demographic factors such as obesity
[OR 0.63 (0.11, 3.49)] and apnea hypopnea index [OR
1.38 (0.59, 3.66)] failed to predict which children would
respond to anti-inflammatory medications.
Children with mild OSA treated with montelukast and
fluticasone experience significant improvements in QOL.
Baseline disease-specific QOL scores may be useful in
predicting which children will respond to medical therapy.
Further research is needed to determine the optimal duration
of anti-inflammatory medications and to compare outcomes for
medical and surgical therapy for non-severe pediatric OSA.
Introduction
Procedures
Results Conclusion
1. Aldea Perona A, García-Sáiz M, Sanz Álvarez E. Psychiatric Disorders and
Montelukast in Children: A Disproportionality Analysis of the VigiBase(®). Drug Saf.
2016;39(1):69-78.
2. Baldassari CM, Mitchell RB, Schubert C, Rudnick EF. Pediatric obstructive sleep
apnea and quality of life: a meta-analysis. Otolaryngol Head Neck Surg.
2008;138(3):265-273.
3. Calapai G, Casciaro M, Miroddi M, Calapai F, Navarra M, Gangemi S. Montelukast-
induced adverse drug reactions: a review of case reports in the literature.
Pharmacology. 2014;94(1-2):60-70.
4. Chan CC, Au CT, Lam HS, Lee DL, Wing YK, Li AM. Intranasal corticosteroids for
mild childhood obstructive sleep apnea--a randomized, placebo-controlled study.
Sleep Med. 2015;16(3):358-363.
5. Chervin RD, Ellenberg SS, Hou X, et al. Prognosis for Spontaneous Resolution of
OSA in Children. Chest. 2015;148(5):1204-1213.
6. Franco RA, Rosenfeld RM, Rao M. First place--resident clinical science award 1999.
Quality of life for children with obstructive sleep apnea. Otolaryngol Head Neck
Surg. 2000;123(1 Pt 1):9-16.
7. Goldbart AD, Greenberg-Dotan S, Tal A. Montelukast for children with obstructive
sleep apnea: a double-blind, placebo-controlled study. Pediatrics. 2012;130(3):e575-
580.
8. Kheirandish-Gozal L, Bandla HP, Gozal D. Montelukast for Children with Obstructive
Sleep Apnea: Results of a Double-Blind, Randomized, Placebo-Controlled Trial. Ann
Am Thorac Soc. 2016;13(10):1736-1741.
9. Kheirandish-Gozal L, Bhattacharjee R, Bandla HPR, Gozal D. Antiinflammatory
therapy outcomes for mild OSA in children. Chest. 2014;146(1):88-95.
10. Landau YE, Bar-Yishay O, Greenberg-Dotan S, Goldbart AD, Tarasiuk A, Tal A.
Impaired behavioral and neurocognitive function in preschool children with
obstructive sleep apnea. Pediatr Pulmonol. 2012;47(2):180-188.
11. Marcus CL, Moore RH, Rosen CL, et al. A randomized trial of adenotonsillectomy for
childhood sleep apnea. N Engl J Med. 2013;368(25):2366-2376.
12. Volsky PG, Woughter MA, Beydoun HA, Derkay CS, Baldassari CM.
Adenotonsillectomy vs observation for management of mild obstructive sleep apnea
in children. Otolaryngol Head Neck Surg. 2014;150(1):126-132.
ReferencesCategory Results
Age, mean SD, yrs 6.8 3.9
BMI percentile, mean SD 71.2 29.7
Obese 15 (48.4%)
Obstructive AHI 2.8 1.0
Central AHI 1.1 0.9
Arousal Index 9.5 2.8
Oxygen Nadir (%) 90.6 2.7
Race
Black 17 (54.8%)
White 13 (41.9%)
Multiracial 1 (3.2%)
Asthma 8 (25.8%)
Second hand smoke 7 (24.8%)
Allergic rhinitis 5 (16.1%)
Table 1. Subject Demographic Data (n = 31).
0
2
4
6
8
10
12
14
16
Within normallimits (18-40)
Mild QOLimpairment
(40-59)
ModerateQOL
impairment(60-79)
Severe QOLimpairment
(80-126)
Num
ber
of P
atients
Total OSA-18 QOL Scores
Baseline Follow-up
Variables Baseline OSA-18
Scores
mean (SD)
Follow up OSA-
18 Scores
mean (SD)
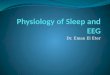
OSA-18 Total 60.2 (18.5) 40.4 (16.1)
Sleep Disturbances 15.3 (5.5) 9.8 (4.7)
Physical Symptoms 12.0 (4.8) 7.3 (3.8)
Emotional
Symptoms
10.1 (5.4) 7.2 (5.1)
Daytime Function 11.0 (4.6) 7.9 (4.5)
Caregiver Concerns 11.7 (5.6) 7.4 (3.9)
Table 2. OSA-18 QOL Scores for children with Mild OSA
treated with Anti-Inflammatory Therapy
Figure 2. Mean Total OSA-18 QOL Scores Before and
After Medical Therapy for Children with Mild OSA.
Patient CharacteristicsThirty-five patients were enrolled in the study with 4
patients failing to return for follow-up. Thus, thirty-one
patients were included in the analysis. Subjects’ AHI
ranged from 1.1 to 4.3, with a mean of 2.8 (SD 1.0).
Mean nadir oxygen saturation was 90.6% with a range
from 84% to 95%.

Patients with obstructive sleep apnea (OSA)
treated with continuous positive airway pressure
(CPAP) have variable compliance. Level of
support provided by the healthcare team can
influence adherence. Compliance is particularly
difficult in the Veteran population. This is a
retrospective chart review of patients seen in the
Hampton Veterans Affairs Medical Center (VAMC)
CPAP Clinic with attention to time since last CPAP
Clinic visit and the relationship to CPAP
compliance. A high degree of variability in
compliance is seen at inter-visit intervals of up to
15 months; following 18 months, data is limited,
but compliance appears remarkably poor.
• To determine whether there is a particular time
frame since last follow-up visit that is
associated with lack of adherence to CPAP.
• To determine whether a change in the protocol
for ongoing monitoring of CPAP therapy at the
our institution is needed.
• To provide the most appropriate support to our
patient population to enable the best possible
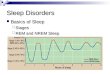
healthcare outcomes.Figure 1. High
degree of
variation in
compliance is
seen at time
intervals up to
15 months. Low
numbers of
patients were
seen at intervals
of greater than
18 months;
these patients
had markedly
low compliance.
This study assesses our manner of processing referrals
to CPAP Clinic, specifically addressing time since last
visit, in order to improve system efficiency.
Based on our preliminary data, the majority of patients
who had not been seen in over 18 months demonstrated
very low compliance. However, the number of patients in
this category was low, thus limiting the generalizability of
this association.
Next steps:
• Evaluate more patient encounters to determine
whether additional data support an association
between > 18 months since last visit and unacceptably
low compliance with CPAP
• Multivariate analysis to determine whether additional
variables, such as data from sleep studies, may
interact with the time interval since last visit to better
predict CPAP compliance.
CPAP compliance can be challenging in patients,
including Veterans, with OSA1, although benefits
have been demonstrated2-4. The Hampton VAMC
CPAP clinic sees patients with OSA on CPAP at
least annually to assess treatment and reorder
supplies. CPAP therapy orders are often provided
by the Sleep Medicine physician based on chart
review and discussion with CPAP clinic techs. VA
and Centers for Medicare and Medicaid Services
(CMS) require patients who are noncompliant with
CPAP use to be reevaluated by polysomnography
prior to renewal of CPAP therapy5. Thus,
determination of the most appropriate next step
(routine CPAP Clinic follow-up, repeat sleep
testing, or Sleep physician visit) is a challenge.
We hypothesized that comparing CPAP
compliance with the time since most recent CPAP
Clinic appointment will yield a cutoff point after
which the rate of CPAP compliance is
unacceptably low, requiring clinical re-evaluation
by the provider.
CPAP Compliance and Time Since Last CPAP Clinic VisitMolly M. Herring, DO, and Sean Hesselbacher, MD, FAASM | Eastern Virginia Medical School | Hampton Veterans Affairs Medical Center
Conflicts of Interest: None
Abstract
Background
Methods
Results Conclusions
• Retrospective chart review
• Adult patients with
OSA treated with
CPAP
• All follow up visits
seen in Hampton
VAMC CPAP Clinic
over a 3-month period
in 2018
• Data collected:
• Demographics
• CPAP settings and
compliance
• Time since last CPAP
Clinic visit.
• Data analysis
• Correlation and linear
regression models
• Association between
time since last CPAP
Clinic visit and CPAP
compliance.
1. El-Solh, AA; Ayyar, L; Akinnusi, M; Relia, S; and Akinnusi, O. Positive Airway
Pressure Adherence in Veterans with Posttraumatic Stress Disorder. SLEEP
2010; 33(11):1495-1500.
2. Tamanna, S; Parker, J; Lyons, J; and Ullah, MI. The Effect of Continuous
Positive Air Pressure (CPAP) on Nightmares in Patients with Posttraumatic
Stress Disorder (PTSD) and Obstructive Sleep Apnea (OSA). Journal of
Clinical Sleep Medicine 2014; 10(6):631-636.
3. El-Solh, AA; Vermont, L; Homish, G; and Kufel, T. The effect of continuous
positive airway pressure on post-traumatic stress disorder symptoms in
veterans with post-traumatic stress disorder and obstructive sleep apnea: a
prospective study. Sleep Medicine 2017; 33:145-150.
4. Ullah, MI; Campbell, DG; Bhagat, R: Lyons, J; and Tamanna, S. Improving
PTSD Symptoms and Preventing Progression of Subclinical PTSD to an Overt
Disorder by Treating Comorbid OSA With CPAP. Journal of Clinical Sleep
Medicine 2017; 13(10):1191-1198.
5. “Positive Airway Pressure (PAP) Devices: Complying with Documentation &
Coverage Requirements.” Medicare Learning Network. ICN 905064, October
2016. Accessed online <https://www.cms.gov/Outreach-and-
Education/Medicare-Learning-Network-
MLN/MLNProducts/downloads/PAP_DocCvg_Factsheet_ICN905064.pdf> 9
August 2018.
6. Bouloukaki, I; Giannadaki, K; Mermigkis, C; Tzanakis, N; Mauroudi, E;
Moniaki, V; Michelakis, S; Siafakas, N; and Schiza, S. Intensive versus
standard follow-up to improve continuous positive airway pressure
compliance. European Respiratory Journal 2014; 44:1262-1274.
References
ObjectivesTable 1. Demographic and overall CPAP usage data.
Mean or Number
Standard Deviation or Percentage
Age (years) 53.2 11.3Male gender 104/115 90.4%
Time since last CPAP Clinic visit (months) 8.1 5.6AHI, treated(events/hour) 2.5 3.9Days with CPAP use ≥4 h (%) 55.9 35.9Days with any CPAP use (%) 68.7 31.8
Figure 2.
Similarly, there
is a high degree
of variability in
compliance with
any daily CPAP
use above an
inter-visit period
of 18 months.

Association of attention deficit hyperactivity disorder and obstructive sleep apnea in adults.Sean E. Hesselbacher1, 2, Akshar A. Ayer, Salim R. Surani3, Zoya S. Surani, Alishah A. Suleman, Joseph Varon, Shyamsunder Subramanian4
Hampton VA Medical Center, Hampton, VA1; Eastern Virginia Medical School, Norfolk, VA2; Texas A&M University, Corpus Christi, TX3; University Hospitals Case Medical Center, Cleveland, OH4
Results
Conclusions
References
1. Kessler RC, Adler L, Barkley R, et al. The prevalence and correlates
of adult ADHD in the United States: results from the National
Comorbidity Survey Replication. Am J Psychiatry. 2006: 163: 716-
723.
2. Kessler RC, Adler L, et al. The World Health Organization adult
ADHD self-report scale (ASRS): a short screening scale for use in
the general population. Psychol Med. 2005; 25: 245-256.
3. Kessler RC, Adler L, Gruber MJ, et al. Validity of the World Health
Organization Adult ADHD Self-Report Scale (ASRS) Screener in a
representative sample of health plan members. Int J Methods
Psychiatr Res. 2007; 16: 52-65.
• The association between obstructive sleep apnea (OSA)
and attention deficit hyperactivity disorder (ADHD) is well-
established in children.
• There is a paucity of literature regarding this association in
adults.
• ADHD is common in adults with estimated prevalence of
4.4%1.
• The Adult ADHD Self-Report Scale (ASRS) is a validated
18-question screen for adult ADHD2.
• Part A is 6 questions; positive screen if 4/6 questions are
answered abnormally
• Sensitivity 68.7%
• Specificity 99.5%
•These data do not suggest a relationship between the presence of OSA and the
presence of ADHD symptoms.
•ADHD+ screen was associated with higher ESS scores, most notably in patients with
any severity of OSA.
•Proportion of ADHD+ screen was substantially higher than the reported prevalence
of ADHD (4.4%)2,3. A positive screen would be expected in ~7.3% of the general
population; therefore, it appears this study population may have a higher prevalence
of ADHD than the general population.
•A similar study of a broader population may yield different results.
Abstract
Objectives: The association between obstructive sleep apnea (OSA) and
attention deficit hyperactivity disorder (ADHD) is well-established in children.
However, there is a paucity of literature regarding this association in adults.
The aim of this study was to determine if ADHD is more common in adult
patients with OSA.
Materials and Methods: All patients referred to a sleep center for sleep
evaluation were administered an adult ADHD screening questionnaire (Adult
ADHD Self-Report Scale (ASRS-v1.1)) and diagnostic polysomnogram. The
ADHD screen is considered positive if 4 of 6 questions in part A of the
screening questionnaire were answered abnormally.
Results: The study population consisted of 194 participants, predominantly
male (62%), Caucasian (54%), and Hispanic (44%). OSA (AHI ≥5
events/hour) was identified in 160 (83%) of participants, with 116 (60%)
having moderate to severe OSA (AHI ≥15 events/hour). The ADHD screen
was positive in 37 (19%) of participants. There was no significant association
between the presence of OSA of any severity and results on the ADHD
screen. Likewise, the presence of a positive ADHD screen was not
associated with any significant difference in AHI.
Conclusions: These data do not suggest a relationship between the
presence of OSA and the presence of ADHD symptoms. This may be
affected by the population studied, which had a high prevalence of OSA. It
should be noted that the proportion of subjects with a positive ADHD screen
was substantially higher than the reported prevalence of ADHD; therefore, a
similar study of a broader population may yield different results.
Conflicts of Interest Disclosure: I do not have any relationships with
any entities producing, marketing, re-selling, or distributing health
care goods or services consumed by, or used on, patients.
Background
Objectives
Methods
• Consecutive patients referred to Baylor College of Medicine/Methodist Hospital Sleep
Center for sleep evaluation were administered the ASRS screen for adult ADHD and
diagnostic polysomnogram (PSG).
• ASRS results were compared with demographic and PSG data for significant
associations. P>0.05 considered significant.
Demographic characteristics of the participants.
Association of ADHD symptoms with sleepiness.
• The primary aim of this study was to determine if ADHD is more common
in adult patients with OSA.
• Secondary objectives were to determine associations between OSA and
ADHD in subgroups of adults
• Gender
• Ethnicity
• Age
• Sleepiness
*P<0.05; **P<0.01; ***P<0.001
ADHD+ OSA(5)+ P-value OSA(15)+ P-value
All (n=194) 37 160 n.s. 116 n.s.
Male (n=120) 17 105 n.s. 80 n.s.
Female (n=74) 20 55 n.s. 36 n.s.
Caucasian (n=105) 19 86 n.s. 61 n.s.
Hispanic (n=85) 16 72 n.s. 53 n.s.
Obese (n=151) 33 131 n.s. 100 n.s.
Non-obese (n=41) 4 27 n.s. 14 n.s.
Age <50 (n=66) 19 50 n.s 39 n.s.
Age 50-64 (n=69) 12 63 n.s. 46 n.s.
Age ≥65 (n=59) 6 47 n.s. 31 n.s.
Total participants: 194
Age (years): 55.6 ±13.9
Gender: 62% male; 38% female.
Ethnicity: 54% Caucasian, 44% Hispanic, 2% other
OSA (AHI ≥5): 160 (82.5%)
Moderate to severe OSA (AHI ≥15): 116 (59.8%)
ADHD screen positive (≥4 abnormal responses): 37 (19.1%)
Association* between OSA and ADHD
Effects of social media by bedtime use.
n.s. = not significant
*Contigency analysis; Fisher’s exact test