Embed Size (px)
Citation preview
CPCK
PacPtictuegrtsrnc
PAba
UA
0d
hallenges in Defining and Identifyingatients With Non–Small Cell Lungancer and Poor Performance Status
aren Kelly
Performance status (PS), a subjective measure of the functional status of a patient withcancer and his or her ability to perform normal activities, is influenced both by tumor-related and by comorbidity-related factors. It is a reliable independent prognostic indicatorfor survival in patients with advanced non–small cell lung cancer. Patients with a poor PS(PS2) constitute up to 30% to 40% of the population of patients with advanced non–smallcell lung cancer, yet they are underrepresented in clinical trials. These patients areheterogeneous, which makes it challenging to use their PS scores alone to guide theirtherapy. A greater understanding of PS scores and the factors that affect them can begained through PS2-specific clinical trials, which can lead to the development of better PSinstruments to aid in making therapeutic decisions.Semin Oncol 31(suppl 11):3-7 © 2004 Elsevier Inc. All rights reserved.
(SOfecowcohcipcbistcp
aisrs
erformance status (PS) is an important factor in cancercare that is used to gauge functional capacity, predict
dverse events and survival, and assess quality-of-life out-omes after treatment. Clinicians commonly use a patient’sS to help guide treatment. PS reflects the effects of the pa-ient’s cancer symptoms and those of other concurrent med-cal conditions. Patients with advanced non–small cell lungancer (NSCLC) and PS2 are commonly seen in clinical prac-ice, and they may constitute up to 30% to 40% of the pop-lation of patients with NSCLC. These patients are frequentlyxcluded from clinical trials, however, making it difficult toeneralize treatment recommendations (Table 1). This articleeviews the definitions of poor PS and its prevalence in pa-ients with advanced NSCLC, and it examines the prognosticignificance of PS and the cancer-related and comorbidity-elated factors that affect it. The limitations of PS as a prog-ostic tool and approaches to overcoming them are also dis-ussed.
erformance Status Scalespatient’s PS is usually assessed by a healthcare professional
y using one of a number of PS scoring systems. The two thatre most widely used are the Karnofsky Performance Scale1
niversity of Colorado Cancer Center, Aurora, CO.ddress reprint requests to Karen Kelly, MD, University of Colorado, 12801
East 17th Ave, Room L18-8122, Aurora, CO 80010. E-mail:
[email protected]093-7754/04/$-see front matter © 2004 Elsevier Inc. All rights reserved.oi:10.1053/j.seminoncol.2004.10.003
KPS) and the Eastern Cooperative Oncology Group (ECOG)cale (Zubrod Scale),2 which is also used by the Southwestncology Group. The KPS, which expresses PS as a value
rom 0% (dead) to 100% (healthy, with no complaints orvidence of disease), was developed during the early years ofhemotherapy, and it quickly became the standard measuref PS in clinical trials. More recently, the ECOG PS scale,hich uses a five-point scoring system (a higher score indi-
ates greater impairment) based on the effects of symptomsn normal daily function as well as the proportion of wakingours the patient is confined to a bed or chair, has come intoommon use. The two scales are not equivalent, but approx-mate conversions between them are possible (Table 2).3 In arospective longitudinal study in 536 patients with lung can-er in whom both KPS and ECOG PS scores were determinedefore, during, and after treatment, a strong correlation ex-
sted between the two scores that persisted throughout thetudy.3 However, as the investigators noted, converting be-ween the scales is not always easy and free of error. A generalonsensus on scale selection would eliminate conversionroblems.3
Even when assessed by a healthcare professional, PS scalesre somewhat subjective in nature.4 There is considerablenterobserver variation in healthcare professionals, but mosttudies report at least a moderate degree of interobservereliability.5-8 In one study, this variation was generally muchmaller with the ECOG PS than the KPS, which was attrib-
ted to the greater simplicity of the ECOG instrument.7 Sig-3

ntEsnt
assowFc(iPadvs
POPppdbA1tdmt
cyvmMME
mwm.amh
atsM2ioppg(wsdhIhhf
tiLECemn
flsPvP
tpttrpafp
sd
T
V
I
I
I
4 K. Kelly
ificant differences in assessments were seen, however, be-ween oncologists and nurses in another study in which theCOG PS scale was used.8 It has been shown that patientelf-assessment of PS is reliable and provides important prog-ostic information. However, differences also exist betweenhe patient and the physician assessments.4,7-9
Disparities between patient and physician assessments andmong those by different healthcare professionals have beenhown to affect the correlations of PS with survival. A pro-pective analysis of the ECOG PS assessments by nurses,ncologists, and the patients was performed in 206 patientsith advanced NSCLC at the Japanese Red Cross Nagoyairst Hospital between 1995 and 1998.8 There was a signifi-ant difference between the assessments by the three groupsP � .001). The assessments by the three groups were signif-cantly correlated with survival, but the oncologist-assessedS scores were best fitted to the survival data. Unlike the PSssessments by oncologists, patient self-assessments did notistinguish survival between PS1 and PS2 patients, with sur-ival curves being the same until 600 days after the diagno-is.8
rognostic Significancef Performance Status
erformance status has been shown to be an independentrognostic factor for survival in advanced NSCLC. Of 77otential prognostic factors considered in an evaluation ofata from approximately 5,000 patients with inoperableronchiogenic carcinoma of the lung treated in Veteransdministration Lung Group protocols 9 to 15 between968 and 1978, the three most important prognostic fac-ors for survival were the initial KPS score, extent of theisease, and the amount of weight loss in the previous 6onths.10 The initial KPS score was the strongest prognos-
ic factor.Three more recent studies have also shown a strong
orrelation between PS and survival. A retrospective anal-sis was performed on data on 1,960 patients with ad-anced NSCLC who were treated with cisplatin-based che-otherapy in ECOG trials between 1981 and 1994.11
ean age of the patients was 60.7 years (range, 19 to 82).ost patients were men (68%) and were patients with
able 1 Challenges in Evaluating Performance Status
ariety of scales Karnofsky, EasternCooperative OncologyGroup, World HealthOrganization
nfluenced by cancer-related factors
Anorexia, fatigue, weight loss,pain
nfluenced by other factors Comorbidities, medications,age, psychosocial issues
nfluenced by assessor Physician, healthcareprovider, patient, familymember
COG PS0/1 (86%). Overall median survival was 6.5 o
onths. A lower ECOG PS was significantly associatedith longer median survival (PS0 v PS1, 9.4 months v 5.7onths; PS0 v PS2, 9.4 months v 3.3 months; both P �
05). Other significant positive prognostic factors werebsence of metastatic disease symptoms, presence of nor-al appetite, absence of bone metastases, and absence ofepatic metastases.Similarly, an analysis of data on 2,531 patients with
dvanced NSCLC treated in Southwest Oncology Grouprials between 1974 and 1988 found that a good PS was aignificant independent predictor of greater survival.12
ost patients (82%) were between 45 and 69 years of age,3% were women, and 59% were PS0/1. Median survival
n the entire population was 5.1 months, and the 1-yearverall survival rate was 16%. Median survival in PS0/1atients was significantly longer than that in PS2 to PS4atients (6.4 months v 3.4 months; P � .01). Similarly, aood PS was associated with higher 1-year survival rate20% v 9%; P � .01). Other significant favorable factorsere female sex, age �70 years, no more than one meta-
tatic lesion, less than 4.5-kg weight loss, normal lactateehydrogenase level, normal alkaline phosphatase level,emoglobin level �11 g/dL, and treatment with cisplatin.n a subanalysis of data on 904 patients, nearly all of whomad been treated with cisplatin-based therapy, PS, age,emoglobin level, and lactate dehydrogenase level wereound to be prognostic factors.12
Another analysis was performed on data on 1,052 pa-ients with advanced NSCLC who were treated with plat-num-based regimens in trials conducted by the Europeanung Cancer Working Party between 1980 and 1991.13
stimated median survival was approximately 6.7 months.ox regression analysis found that the extent of the dis-ase, KPS, white blood cell and neutrophil counts, skinetastases, serum calcium level, age, and sex were prog-ostic factors.13
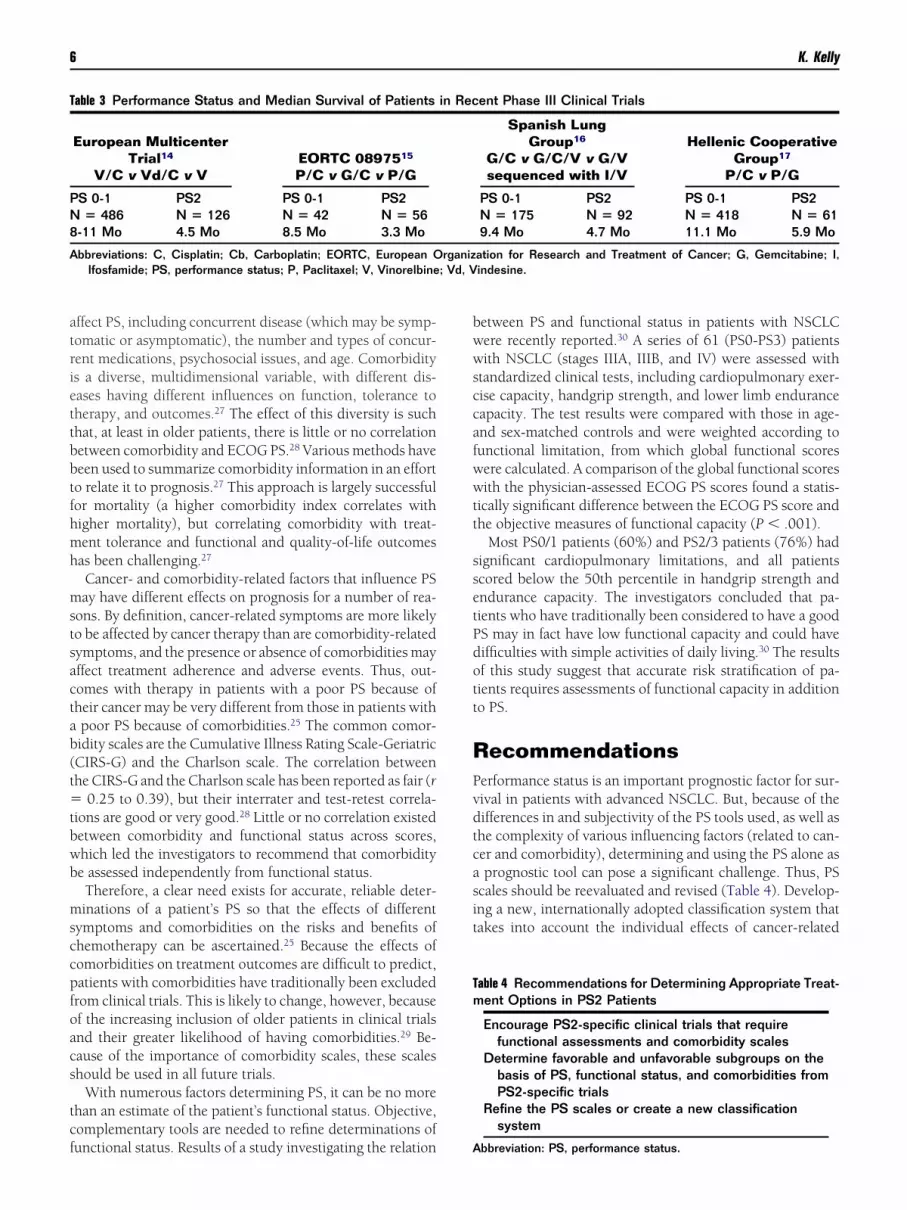
Further evidence for PS score as a strong prognosticactor in advanced NSCLC is apparent in several recentarge phase III clinical trials (Table 3).14-17 Although con-iderably underrepresented in some of the larger studies,S2 patients consistently exhibited shorter median sur-ival than their PS0/1 counterparts. In fact, in some cases,S was the sole indicator of survival.14-17
The relation between PS and symptom control is less clearhan that between PS and survival. In a meta-analysis of 290atients with advanced NSCLC treated with cisplatin-basedherapy, a better ECOG PS was a positive predictor for symp-om response (P � .05).18 However, there was also symptomesponse in 48% of the PS2 patients and in 30% of the PS3/4atients. Another study in 169 patients treated with single-gent gemcitabine or cisplatin-based combination therapyound there was a trend toward greater symptom control inatients with a KPS of 80% or higher.19
In summary, PS is the most reliable prognostic factor forurvival in patients with advanced NSCLC, but a poor PSoes not necessarily preclude symptom control and quality-
f-life benefits with therapy.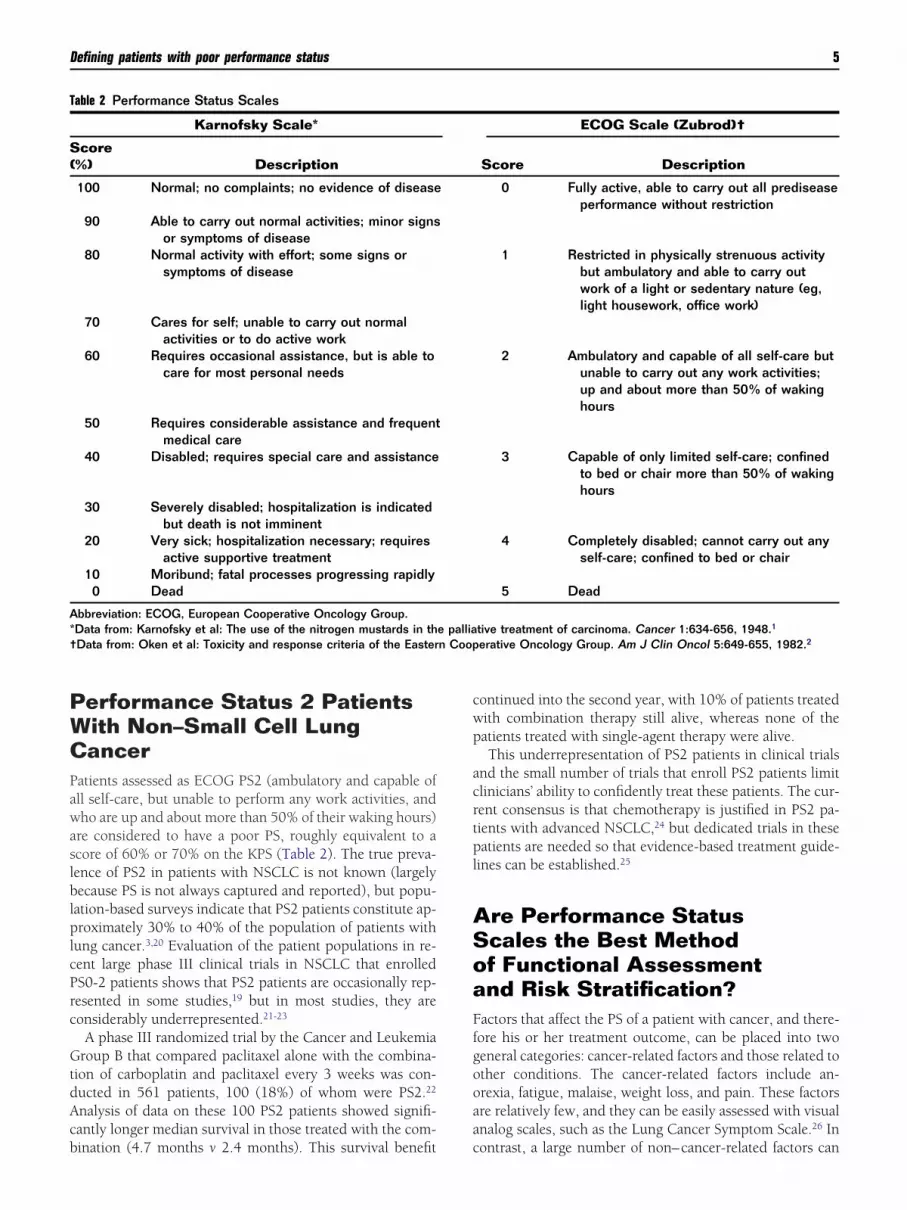
PWCPawaslblplcPrc
GtdAcb
cwp
acrtpl
ASoaFfgooaa
T
S(
A*† n Coop
Defining patients with poor performance status 5
erformance Status 2 Patientsith Non–Small Cell Lungancer
atients assessed as ECOG PS2 (ambulatory and capable ofll self-care, but unable to perform any work activities, andho are up and about more than 50% of their waking hours)
re considered to have a poor PS, roughly equivalent to acore of 60% or 70% on the KPS (Table 2). The true preva-ence of PS2 in patients with NSCLC is not known (largelyecause PS is not always captured and reported), but popu-
ation-based surveys indicate that PS2 patients constitute ap-roximately 30% to 40% of the population of patients with
ung cancer.3,20 Evaluation of the patient populations in re-ent large phase III clinical trials in NSCLC that enrolledS0-2 patients shows that PS2 patients are occasionally rep-esented in some studies,19 but in most studies, they areonsiderably underrepresented.21-23
A phase III randomized trial by the Cancer and Leukemiaroup B that compared paclitaxel alone with the combina-
ion of carboplatin and paclitaxel every 3 weeks was con-ucted in 561 patients, 100 (18%) of whom were PS2.22
nalysis of data on these 100 PS2 patients showed signifi-antly longer median survival in those treated with the com-
able 2 Performance Status Scales
Karnofsky Scale*
core%) Description
100 Normal; no complaints; no evidence of disease
90 Able to carry out normal activities; minor signsor symptoms of disease
80 Normal activity with effort; some signs orsymptoms of disease
70 Cares for self; unable to carry out normalactivities or to do active work
60 Requires occasional assistance, but is able tocare for most personal needs
50 Requires considerable assistance and frequentmedical care
40 Disabled; requires special care and assistance
30 Severely disabled; hospitalization is indicatedbut death is not imminent
20 Very sick; hospitalization necessary; requiresactive supportive treatment
10 Moribund; fatal processes progressing rapidly0 Dead
bbreviation: ECOG, European Cooperative Oncology Group.Data from: Karnofsky et al: The use of the nitrogen mustards in thData from: Oken et al: Toxicity and response criteria of the Easter
ination (4.7 months v 2.4 months). This survival benefit c
ontinued into the second year, with 10% of patients treatedith combination therapy still alive, whereas none of theatients treated with single-agent therapy were alive.This underrepresentation of PS2 patients in clinical trials
nd the small number of trials that enroll PS2 patients limitlinicians’ ability to confidently treat these patients. The cur-ent consensus is that chemotherapy is justified in PS2 pa-ients with advanced NSCLC,24 but dedicated trials in theseatients are needed so that evidence-based treatment guide-
ines can be established.25
re Performance Statuscales the Best Methodf Functional Assessmentnd Risk Stratification?
actors that affect the PS of a patient with cancer, and there-ore his or her treatment outcome, can be placed into twoeneral categories: cancer-related factors and those related tother conditions. The cancer-related factors include an-rexia, fatigue, malaise, weight loss, and pain. These factorsre relatively few, and they can be easily assessed with visualnalog scales, such as the Lung Cancer Symptom Scale.26 In
ECOG Scale (Zubrod)†
Score Description
0 Fully active, able to carry out all prediseaseperformance without restriction
1 Restricted in physically strenuous activitybut ambulatory and able to carry outwork of a light or sedentary nature (eg,light housework, office work)
2 Ambulatory and capable of all self-care butunable to carry out any work activities;up and about more than 50% of wakinghours
3 Capable of only limited self-care; confinedto bed or chair more than 50% of wakinghours
4 Completely disabled; cannot carry out anyself-care; confined to bed or chair
5 Dead
tive treatment of carcinoma. Cancer 1:634-656, 1948.1
erative Oncology Group. Am J Clin Oncol 5:649-655, 1982.2
e palliaontrast, a large number of non–cancer-related factors can
atriettbbtfhmh
mstsactab(t�tbwb
msccpfoacs
tcf
bwwsccafwwtt
ssetPdott
RPvdtcasit
T
PN8
A; Vd, V
Tm
6 K. Kelly
ffect PS, including concurrent disease (which may be symp-omatic or asymptomatic), the number and types of concur-ent medications, psychosocial issues, and age. Comorbiditys a diverse, multidimensional variable, with different dis-ases having different influences on function, tolerance toherapy, and outcomes.27 The effect of this diversity is suchhat, at least in older patients, there is little or no correlationetween comorbidity and ECOG PS.28 Various methods haveeen used to summarize comorbidity information in an efforto relate it to prognosis.27 This approach is largely successfulor mortality (a higher comorbidity index correlates withigher mortality), but correlating comorbidity with treat-ent tolerance and functional and quality-of-life outcomesas been challenging.27
Cancer- and comorbidity-related factors that influence PSay have different effects on prognosis for a number of rea-
ons. By definition, cancer-related symptoms are more likelyo be affected by cancer therapy than are comorbidity-relatedymptoms, and the presence or absence of comorbidities mayffect treatment adherence and adverse events. Thus, out-omes with therapy in patients with a poor PS because ofheir cancer may be very different from those in patients withpoor PS because of comorbidities.25 The common comor-idity scales are the Cumulative Illness Rating Scale-GeriatricCIRS-G) and the Charlson scale. The correlation betweenhe CIRS-G and the Charlson scale has been reported as fair (r
0.25 to 0.39), but their interrater and test-retest correla-ions are good or very good.28 Little or no correlation existedetween comorbidity and functional status across scores,hich led the investigators to recommend that comorbiditye assessed independently from functional status.Therefore, a clear need exists for accurate, reliable deter-inations of a patient’s PS so that the effects of different
ymptoms and comorbidities on the risks and benefits ofhemotherapy can be ascertained.25 Because the effects ofomorbidities on treatment outcomes are difficult to predict,atients with comorbidities have traditionally been excludedrom clinical trials. This is likely to change, however, becausef the increasing inclusion of older patients in clinical trialsnd their greater likelihood of having comorbidities.29 Be-ause of the importance of comorbidity scales, these scaleshould be used in all future trials.
With numerous factors determining PS, it can be no morehan an estimate of the patient’s functional status. Objective,omplementary tools are needed to refine determinations of
able 3 Performance Status and Median Survival of Patients
European MulticenterTrial14
V/C v Vd/C v VEORTC 0897515
P/C v G/C v P/G
S 0-1 PS2 PS 0-1 PS2� 486 N � 126 N � 42 N � 56
-11 Mo 4.5 Mo 8.5 Mo 3.3 Mo
bbreviations: C, Cisplatin; Cb, Carboplatin; EORTC, European OIfosfamide; PS, performance status; P, Paclitaxel; V, Vinorelbine
unctional status. Results of a study investigating the relation A
etween PS and functional status in patients with NSCLCere recently reported.30 A series of 61 (PS0-PS3) patientsith NSCLC (stages IIIA, IIIB, and IV) were assessed with
tandardized clinical tests, including cardiopulmonary exer-ise capacity, handgrip strength, and lower limb enduranceapacity. The test results were compared with those in age-nd sex-matched controls and were weighted according tounctional limitation, from which global functional scoresere calculated. A comparison of the global functional scoresith the physician-assessed ECOG PS scores found a statis-
ically significant difference between the ECOG PS score andhe objective measures of functional capacity (P � .001).
Most PS0/1 patients (60%) and PS2/3 patients (76%) hadignificant cardiopulmonary limitations, and all patientscored below the 50th percentile in handgrip strength andndurance capacity. The investigators concluded that pa-ients who have traditionally been considered to have a goodS may in fact have low functional capacity and could haveifficulties with simple activities of daily living.30 The resultsf this study suggest that accurate risk stratification of pa-ients requires assessments of functional capacity in additiono PS.
ecommendationserformance status is an important prognostic factor for sur-ival in patients with advanced NSCLC. But, because of theifferences in and subjectivity of the PS tools used, as well ashe complexity of various influencing factors (related to can-er and comorbidity), determining and using the PS alone asprognostic tool can pose a significant challenge. Thus, PS
cales should be reevaluated and revised (Table 4). Develop-ng a new, internationally adopted classification system thatakes into account the individual effects of cancer-related
ent Phase III Clinical Trials
Spanish LungGroup16
G/C v G/C/V v G/Vsequenced with I/V
Hellenic CooperativeGroup17
P/C v P/G
PS 0-1 PS2 PS 0-1 PS2N � 175 N � 92 N � 418 N � 619.4 Mo 4.7 Mo 11.1 Mo 5.9 Mo
ation for Research and Treatment of Cancer; G, Gemcitabine; I,indesine.
able 4 Recommendations for Determining Appropriate Treat-ent Options in PS2 Patients
Encourage PS2-specific clinical trials that requirefunctional assessments and comorbidity scales
Determine favorable and unfavorable subgroups on thebasis of PS, functional status, and comorbidities fromPS2-specific trials
Refine the PS scales or create a new classificationsystem
in Rec
rganiz
bbreviation: PS, performance status.

snsbtheisa
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
Defining patients with poor performance status 7
ymptoms and comorbidities on PS and that retains the prog-ostic significance of PS may lead to more appropriate patienttratification, particularly in those with a poor PS. This canegin by designing and conducting PS-specific clinical trialshat incorporate functional tools and comorbidity scales. It isoped that a greater understanding of the factors that influ-nce PS will lead to optimal treatments. This is particularlymportant in PS2 patients with advanced NSCLC, in whomubstantial symptom control can be achieved despite theirpparently poor prognosis.
eferences1. Karnofsky DA, Abelmann WH, Craver LF, et al: The use of the nitrogen
mustards in the palliative treatment of carcinoma. Cancer 1:634-656,1948
2. Oken MM, Creech RH, Tormey DC, et al: Toxicity and response criteriaof the Eastern Cooperative Oncology Group. Am J Clin Oncol 5:649-655, 1982
3. Buccheri G, Ferrigno D, Tamburini M: Karnofsky and ECOG perfor-mance status scoring in lung cancer: A prospective, longitudinal studyof 536 patients from a single institution. Eur J Cancer 32A:1135-1141,1996
4. Loprinzi CL, Laurie MA, Wieand HS, et al: Prospective evaluation ofprognostic variables from patient-completed questionnaires. NorthCentral Cancer Treatment Group. J Clin Oncol 12:601-607, 1994
5. Yates JW, Chalmer B, McKegney FP: Evaluation of patients with ad-vanced cancer using the Karnofsky performance status. Cancer 45:2220-2224, 1980
6. Schag CC, Heinrich RL, Ganz PA: Karnofsky performance status revis-ited: Reliability, validity, and guidelines. J Clin Oncol 2:187-193, 1984
7. Taylor AE, Olver IN, Sivanthan T, et al: Observer error in gradingperformance status in cancer patients. Support Care Cancer 7:332-335,1999
8. Ando M, Ando Y, Hasegawa Y, et al: Prognostic value of performancestatus assessed by patients themselves, nurses, and oncologists in ad-vanced non–small cell lung cancer. Br J Cancer 85:1634-1639, 2001
9. Blagden SP, Charman SC, Sharples LD, et al: Performance status score:Do patients and their oncologists agree? Br J Cancer 89:1022-1027,2003
0. Stanley KE: Prognostic factors for survival in patients with inoperablelung cancer. J Natl Cancer Inst 65:25-32, 1980
1. Jiroutek M, Johnson D, Blum R, et al: Prognostic factors in advancednon–small cell lung cancer (NSCLC): Analysis of Eastern CooperativeOncology Group (ECOG) trials from 1981-1992. Proc Am Soc ClinOncol 17:461, 1998 (abstr 1774)
2. Albain KS, Crowley JJ, LeBlanc M, et al: Survival determinants in ex-tensive-stage non–small-cell lung cancer: The Southwest OncologyGroup experience. J Clin Oncol 9:1618-1626, 1991
3. Paesmans M, Sculier JP, Libert P, et al: Prognostic factors for survival inadvanced non–small-cell lung cancer: Univariate and multivariate anal-yses including recursive partitioning and amalgamation algorithms in1,052 patients. The European Lung Cancer Working Party. J Clin On-col 13Z:1221-1230, 1995
4. Soria JC, Brisgand D, Le Chevalier T: Do all patients with advanced
non–small-cell lung cancer benefit from cisplatin-based combinationtherapy? Ann Oncol 12:1667-1670, 2001
5. Kosmidis P, Mylonakis N, Nicolaides C, et al: Paclitaxel plus carbopla-tin versus gemcitabine plus paclitaxel in advanced non–small-cell lungcancer: A phase III randomized trial. J Clin Oncol 20:3578-3585, 2002
6. Alberola V, Camps C, Provencio M, et al: Cisplatin plus gemcitabineversus a cisplatin-based triplet versus nonplatinum sequential doubletsin advanced non–small-cell lung cancer: A Spanish Lung Cancer Groupphase III randomized trial. J Clin Oncol 21:3207-3213, 2003
7. Smit EF, van Meerbeeck JP, Lianes P, et al: Three-arm randomizedstudy of two cisplatin-based regimens and paclitaxel plus gemcitabinein advanced non–small-cell lung cancer: A phase III trial of the Euro-pean Organization for Research and Treatment of Cancer Lung CancerGroup—EORTC 08975. J Clin Oncol 21:3909-3917, 2003
8. Hickish TF, Smith IE, O’Brien ME, et al: Clinical benefit from palliativechemotherapy in non–small-cell lung cancer extends to the elderly andthose with poor prognostic factors. Br J Cancer 78:28-33, 1998
9. Vansteenkiste J, Vandebroek J, Nackaerts K, et al: Influence of cisplatin-use, age, performance status and duration of chemotherapy on symp-tom control in advanced non–small cell lung cancer: Detailed symptomanalysis of a randomised study comparing cisplatin-vindesine to gem-citabine. Lung Cancer 40:191-199, 2003
0. Radzikowska E, Glaz P, Roszkowski K: Lung cancer in women: Age,smoking, histology, performance status, stage, initial treatment andsurvival. Population-based study of 20 561 cases. Ann Oncol 13:1087-1093, 2002
1. Scagliotti GV, De Marinis F, Rinaldi M, et al: Phase III randomized trialcomparing three platinum-based doublets in advanced non–small-celllung cancer. J Clin Oncol 20:4285-4291, 2002
2. Lilenbaum RC, Herndon J, List M, et al: Single-agent (SA) versus com-bination chemotherapy (CC) in advanced non–small cell lung cancer(NSCLC): A CALGB randomized trial of efficacy, quality of life (QOL),and cost-effectiveness. Proc Am Soc Clin Oncol 21:1a, 2002 (abstr 2)
3. Gridelli C, Perrone F, Gallo C, et al: Chemotherapy for elderly patientswith advanced non–small-cell lung cancer: The Multicenter ItalianLung Cancer in the Elderly Study (MILES) phase III randomized trial.J Natl Cancer Inst 95:362-372, 2003
4. Pfister DG, Johnson DG, Azzoli CG, et al: American Society of ClinicalOncology treatment of unresectable non–small-cell lung cancer guide-line: Update 2003. J Clin Oncol 22:330-353, 2004
5. Gridelli C, Ardizzoni A, Le Chevalier T, et al: Treatment of advancednon–small-cell lung cancer patients with ECOG performance status 2:results of an European Experts Panel. Ann Oncol 15:419-426, 2004
6. Hollen PJ, Gralla RJ, Kris MG, et al: Quality of life assessment in indi-viduals with lung cancer: Testing the Lung Cancer Symptom Scale(LCSS). Eur J Cancer 29A:S51-S58, 1993 (suppl 1)
7. Extermann M: Measurement and impact of comorbidity in older cancerpatients. Crit Rev Oncol Hematol 35:181-200, 2000
8. Extermann M, Overcash J, Lyman GH, et al: Comorbidity and func-tional status are independent in older cancer patients. J Clin Oncol16:1582-1587, 1998
9. Yancik R, Ganz PA, Varricchio CG, et al: Perspectives on comorbidityand cancer in older patients: Approaches to expand the knowledgebase. J Clin Oncol 19:1147-1151, 2001
0. Dalzell M-A, Kreisman H, Small D, et al: Is performance status relatedto functional capacity in patients with non small cell lung cancer
(NSCLC). Proc Am Soc Clin Oncol 23:669, 2004 (abstr)




























