Embed Size (px)
Citation preview

C H A P T E Rz z z z z z z z z z z z z z z z z z z z z z z z z z z27
Management Techniquesfor Spinal InjuriesManagement Techniquesfor Spinal Injuries
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Ronald W. Lindsey, M.D.Spiros G. Pneumaticos, M.D.Zbigniew Gugala, M.D.
Many treatment techniques have been used for managinginjuries involving the spine. Initially, most were nonopera-tive, but over the past century, numerous surgical tech-niques have also been described. Various types of spinalinstrumentation systems have been devised, and the surgi-cal indications for spinal injuries have been better definedto facilitate the success of operative management. However,many types of spinal injuries can still be satisfactorilytreated by nonoperative methods without many of theinherent risks of surgery; others can be treated by eitheroperative or nonoperative methods. Therefore, it is imper-ative that the clinician understand the role of nonoperativetreatment and remain facile with techniques such as spinaltraction, reduction by manipulation, and orthotic immobi-lization.
Traditionally, the term conservative care has been synon-ymous with nonoperative treatment. Recent advances inour understanding of the different types of spinal injuriesand their risk for complications have allowed the termconservative care to be used for either nonoperative oroperative treatment. Optimal management must considerearly patient mobilization, maintenance of acceptable spi-nal alignment and stability, the presence of associatedinjuries, and the risk and severity of potential complica-tions associated with each type of treatment. Being familiarwith both surgical and nonsurgical treatment approachesallows the clinician to individualize treatment based on thenature of the injury and the demands of the specificpatient.
The objectives of nonoperative management of spinalinjuries are similar to those of operative treatment andinclude the following:
1. Avoiding progression of neurologic deficit and, whendeficit is present, enhancing its resolution
2. Reducing unacceptable spinal deformity or malalign-ment to an acceptable functional range
3. Maintaining spinal alignment within a functional rangethroughout the course of treatment
4. Healing the spine in a functional alignment sufficient topermit return of physiologic loads through the spine
Nonoperative management should consist of immobili-zation that is well tolerated, permit timely mobilization,and allow for healing within a reasonable period. There-fore, the ultimate success of nonoperative treatment re-quires proper patient selection, as well as complete un-derstanding and strict adherence to the principles ofnonoperative management.
Detailed descriptions of modern spine biomechanicsand pathomechanics, as well as the classification systemsused to determine spine stability, are included in thesubsequent chapters dealing with each specific injurytype. In this chapter, factors determining optimal treat-ment for spine injuries are presented. Regardless of thetreatment method used, the objectives of preserving neuro-logic function, minimizing post-traumatic deformity, andachieving a stable functional spine remain the standardof care.
CERVICAL TRACTIONz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Cervical traction is frequently indicated for the treatmentof cervical spine injury to achieve the following objectives:(1) reduce cervical spine deformity, (2) indirectly de-compress traumatized neural elements, and (3) providecervical spine stability. Familiarity with the use of cervicaltraction is essential in the treatment of cervical spinetrauma because of its ease of application and lowmorbidity when applied properly.
The modes by which cervical traction can be appliedinclude a head halter, tongs, or a halo ring. Head haltertraction consists of straps that attach to the head at thechin and the occiput, and only small amounts of weight(5 to 10 lb) can be applied safely. In addition to reducedtraction weight, limitations of head halter traction
746
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 1/31 P 746 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 1/31 P 746 BLACK T

include poor attachment to the head and the ability tocontrol only axial compression through distraction. Exces-sive weight over an extended period can cause pressureulcerations at the chin or occiput. Currently, halter tractionis rarely indicated for spine trauma.
Tongs Traction
When applying traction with tongs, in contrast to headhalters, fixation into the skull is achieved through the useof special pins with a pointed tip that abruptly flares out.This design allows for pin insertion through the outercortex of the skull without penetration of the inner cortex.The flared nature of the pin design distributes pin pressureover its entire width on insertion while engaging the outertable.
Several types of tongs presently exist and include theGardner-Wells or Trippi-Wells models. Tongs, similar tohead halters, essentially control motion in a single planethrough the application of longitudinal traction. Gardner-Wells tongs (Fig. 27–1) have achieved the widest accep-tance because of their ability to withstand high loads andtheir ease of application. Gardner-Wells tongs can beapplied quickly by a single physician. Trippi-Wells tongsconsist of the same pins as Gardner-Wells tongs, but theyare used in a multipin fashion. Because of the ability oftongs to resist motion in only one plane, they are associatedwith a high incidence of loosening. Tongs are typicallyindicated when longitudinal traction is to be temporarilyapplied or the patient is to remain bedridden.
APPLICATION OF TONGS
In preparation for the application of tongs, the patient ispositioned supine with the head resting on the table topand no pillow support. The physician stands at the top(head) of the table above the patient for easy access toeither side of the head. Pins should be placed just belowthe greatest diameter (equator) of the skull in a mannerthat avoids the temporalis muscle and superficial temporalartery and vein (Fig. 27–2). The standard site for pininsertion is approximately 1 cm posterior to the externalauditory meatus and 1 cm superior to the pinna of the ear.
Asymmetric pin placement, either slightly posterior toaffect flexion or slightly anterior to affect extension, caneither facilitate or inhibit fracture reduction.
The use of Gardner-Wells tongs does not require shav-ing of the pin site. The skin and hair are prepared with aniodine solution, and the pin can be inserted directly intothe skin without an incision. Before pin placement, localanesthetic is injected into the skin with care taken toinfiltrate the periosteum down to the galea. The pins,which must be sterile and handled accordingly, are posi-tioned orthogonally on either side of the skull beforetightening. Tightening the pins by alternating from side toside will maintain pin symmetry. Gardner-Wells tongs arespring-loaded and thereby prevent perforation of the innertable of the skull. The force of pin insertion is gauged bythe spring-loaded force indicator contained in one of thepins, and optimal insertion torque is typically 6 to 8 in-lb.After the tongs are in place, the pins should be cleanedonce a day with hydrogen peroxide at the skin–pininterface. After the first 24 hours of tongs application, thespring-loaded pins must be retightened; additional tighten-ing should not be done to avoid the risk of perforating theinner table.
Halo Ring Traction
Cervical traction can be applied more efficiently through ahalo ring. The multipin attachment of the halo to the skullreduces the distribution of the pin load, thereby allowingfor higher traction loads to be applied for an extendedperiod. Experimentally, the measured pull-out strength fora halo ring is almost twice that of Gardner-Wells tongs(440 versus 233 lb).72 Furthermore, the circumferentialpin fixation to the skull better resists multiplane spinemotion and allows for traction in flexion, extension, orsimultaneous bivector traction techniques.110 Finally, amajor advantage of halo ring traction is that it can berapidly converted to a halo vest orthosis once spinalreduction has been achieved.
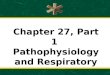
FIGURE 27–2. Pins for traction tongs are placed below the cranial brim orthe widest diameter of the skull (equator), anterior and superior to theearlobe. Care must be taken to position the pins posterior to thetemporalis muscle. Precalibrated indicator pins are set to protrude at 8 lbof pressure.
FIGURE 27–1. Gardner-Wells tongs have angulated pins designed to bettercounteract traction forces. The tongs can be made from magneticresonance imaging–compatible materials (carbon fiber, titanium), whichobviates the need for removal of the tongs and facilitates head andcervical spine imaging.
747CHAPTER 27 • Management Techniques for Spinal Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 2/31 P 747 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 2/31 P 747 BLACK T

The design of the halo ring has dramatically improvedsince its advent as a device for stabilization of facialfractures.19 Currently available halo rings are made of lightand radiolucent materials (titanium, carbon composites)that permit computed tomography (CT) and magneticresonance imaging (MRI). More recently, open-ring andcrown-type halo designs that encircle only a part of thehead have also been developed. These devices are openposteriorly to avoid the need to pass the head through aring and thus ease application and improve safety. Withsome crown designs, the posterior ends of the incompletering must be angled inferiorly to ensure posterior pinplacement below the equator of the skull. Halo rings areavailable in a variety of sizes to fit virtually any patient,including young children. A properly fitted halo ringprovides 1 to 2 cm of clearance around every aspect of thepatient’s skull. The appropriate ring size can usually bedetermined by measuring the circumference of the skull1 cm above the ears and eyebrows and then referring to themanufacturer’s chart for preferred ring sizes.
HALO RING APPLICATION
A halo ring is routinely applied under local anesthesia;occasionally, light pharmacologic sedation may be neces-sary. The patient is positioned supine, and to permitapplication of a full-ring halo, the patient’s occiput iselevated with a folded towel or the head is gently posi-tioned beyond the edge of the bed. Open-back halo ringscan be applied without these maneuvers and are thereforepreferred. Before application of a halo ring, all patientsshould be in a hard collar, including those undergoingconversion of traction tongs to halo immobilization. Thehalo ring is temporary positioned equidistant from thepatient’s head, 1 cm above the eyebrows and 1 cm abovethe tip of the ears. It is extremely important that the ring bepositioned just below the greatest circumference of thepatient’s skull to prevent the halo ring from becomingdisplaced upward and out of position. The halo ring isprovisionally stabilized with three blunt positioning pins,and locations for the sharp head pins are then determined(Fig. 27–3). The optimal location for the anterior pins is1 cm superior and two thirds lateral to the orbital rim, justbelow the greatest circumference of the skull (Fig. 27–4A).Along the medial aspect of the safe zone lie the supraorbitaland supratrochlear nerves and the underlying frontal sinus.Placement of pins in the temporalis region behind thehairline confers a cosmetic advantage but is, however,
anatomically and biomechanically inferior.18, 47 Insertionsites for the posterior pins are less critical because neuro-muscular structures are lacking and the skull is thicker andmore uniform in that area. The posterior sites should beinferior to the widest portion of the skull, yet superiorenough to prevent impingement of the ring or crown onthe upper helix of the ear (see Fig. 27–4B).
While the halo is held in position, the skin is shavedand prepared with an iodine solution. Local anesthetic,typically a 1% lidocaine solution, is injected with theneedle passed through the holes for the sharp pins untilthe periosteum is elevated. Small stab incisions are madeand the pins inserted in a diagonal fashion to maintainequal distance between the halo ring and skull. Pinsshould be inserted perpendicular to the skull becauseangulated pin insertion has been reported to be biome-chanically inferior.122 The pins are tightened with a torquescrewdriver, and during this maneuver the patient is askedto close the eyes and relax the forehead to prevent eyebrowtenting or tethering. When all sharp pins are in place, theblunt pins are removed and the sharp pins tightened in adiagonal fashion up to a torque of 6 to 8 in-lb.17 Pin torqueshould never exceed 10 in-lb because of the risk ofpenetration of the outer cortex.17 Breakaway wrenches canbe used to prevent the pins from being tightened past themaximal torque; however, torque limits are more reliablymeasured with a calibrated torque screwdriver. Locknutsare then placed on each pin and gently tightened to secure
Spring-loadedpins (front)
A B
Blank pins(back)
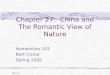
FIGURE 27–3. The halo ring is heldin a temporary position equidistantfrom the patient’s head, 1 cm abovethe eyebrows and 1 cm above thetip of the ears, with the use ofblunt positioning pins (A). With thehalo ring held in place, sharp halopins are then placed just below theskull equator. Spring-loaded pins areplaced in front and a blank pin on theback (B). The pins are inserted andtightened in a diagonal fashion.
SO
A B
ST
FIGURE 27–4. The safe zone for the anterior pins is located 1 cm superiorand two thirds lateral to the orbital rim, just below the greatestcircumference of the skull. On the medial aspect of the safe zone are thesupraorbital (SO) and supratrochlear (ST) nerves (A). The zone for theposterior pins is inferior to the widest portion of the skull, yet superiorenough to prevent ring or crown impingement on the upper helix of theear (B).
748 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 3/31 P 748 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 3/31 P 748 BLACK T

the pin to the ring. Once the halo application is complete, atraction bow can be mounted. The traction weight protocolfor halo rings can be much more aggressive than that fortongs, and weights can exceed 100 lb when indicated.
Cervical Traction Weight
After tongs or a halo ring has been applied, cervical tractioncan begin at approximately 10 to 15 lb, with immediateevaluation by lateral radiographs to avoid overdistraction(Fig. 27–5). Traction weight can be increased by 5- to 10-lbincrements, depending on the size and weight of thepatient. Serial lateral radiographs should be obtainedapproximately 10 to 15 minutes after each application ofweight to allow for soft tissue creep. Fluoroscopy can beused instead of plain radiographs to facilitate this process.The patient must be completely relaxed, and analgesics ormuscle relaxants can often assist in minimizing musclespasm or tension. At higher weights (greater than 40 lb), 30to 60 minutes should elapse before further load increase.The head of the bed should be slightly elevated to providebody weight resistance to traction.
The maximal amount of weight that can safely beapplied for closed traction reduction of the cervical spineremains controversial. It has been suggested that a slow,gradual increase in traction weight will effect spinal reduc-tion at a lower total traction load.90 Some physicianssupport a more rapid incremental increase in weight andhave applied weights up to 150 lb without any adverseeffects.70 Typically, the maximal weight tolerated will be
limited by the skeletal fixation used, and for cranial tongs,the limit is up to 100 lb.
The objective of using cervical traction is to achieve themaximal effect of the weight being applied. The maximaltraction weight should be considered to be a function ofthe patient’s size, body weight, or body habitus (or anycombination of these attributes) rather than an absolutenumber (100-lb cervical traction may be well tolerated bya burly 300-lb male weightlifter, but not appropriate for a115-lb female). The greater the associated ligamentousdisruption, the less total weight that is appropriate. Themaximal weight should also correspond to the level of thecervical injury; specifically, upper cervical injuries requireless weight than do injuries at the cervicothoracic junction.When these parameters are respected and sufficient timeis permitted between incremental increases in tractionweight, the maximal weight can usually be limited to 70 lbor less for lower cervical injury in an average-sized adult.Regardless of whether spinal reduction has been achieved,it is imperative that the maximal traction weight bedecreased to 10 to 15 lb once the monitored reductionprocess has been terminated.
Most cervical spine injuries can be reduced with onlylongitudinal traction, but small changes in the vector oftraction (i.e., slightly more flexion or more extension) canbe helpful in some cases. Spinal manipulation can behazardous and is therefore controversial.82 Lee and associ-ates compared cervical traction and manipulation underanesthesia and determined that traction alone was prefera-ble.70 Cotler and co-workers suggested that gentle manip-ulation in combination with traction could be of benefit in
FIGURE 27–5. A, Admission lateral radiograph showed no abnormal distraction. B, After cervical traction was initiated at 20 lb, it resulted in markedoverdistraction. Traction should always be initiated at 10 lb.
749CHAPTER 27 • Management Techniques for Spinal Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 4/31 P 749 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 4/31 P 749 BLACK T

awake patients.30 Manual manipulation as a means ofachieving cervical spine reduction should never be per-formed in a patient under general anesthesia or in anunconscious patient. Light sedation in an otherwise alertpatient allows the physician to detect neurologic alter-ations. In general, the authors do not support manualmanipulation and prefer that patients who do not respondto traction be treated surgically.
SPINAL BRACINGz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
The Halo-Vest Orthosis
The advent of the halo ring inspired the development of thehalo vest apparatus by Perry and Nickel in 1959.96, 100 Theoriginal halo consisted of a complete ring attached to abody cast and was used to immobilize a patient withpoliomyelitis. Since then, the halo vest orthosis has under-gone dramatic changes in design and currently providesthe most effective stabilization available for a cervicalorthosis (Fig. 27–6).
The stabilizing property of any halo vest orthosis ismost dependent on adequate fitting of the vest to thepatient’s torso. The appropriate size of vest is determinedafter measurement of the patient’s chest circumference andtorso length. The most common body jackets that areattached to the halo ring are adjustable double-shell plasticvests. Occasionally, a plaster body cast can be used forpatients who are noncompliant or extremely difficult to fit.The vest is attached to the halo ring with four upright bars.The posterior and anterior shells of the vest can be applied
before or after halo ring fixation. Care is taken to applymanual traction before the upright bars are completelytightened. The cast or vest must be well fitted to the torsoand shoulders to prevent vertical toggle of the apparatus.Although the halo vest is the most stable orthosis forcervical spine immobilization, it does not completelyrestrict motion across the spine.
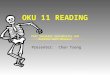
Despite adequate fit, the halo vest has been shown topermit up to 31% of normal cervical spine motion,depending on the patient’s position, activity, and degree ofspinal instability6, 65 (Fig. 27–7). The most restrictedmotion was typically below C2, and the least restricted wasabove C2.76
Despite the effectiveness of halo skeletal fixation inachieving cervical spine immobilization, complications arecommon and include pin loosening, pin site infection,pressure sores, headache, loss of reduction, dural punc-ture, and dysphagia (Table 27–1). Most of these compli-cations usually result from either improper halo ringapplication or an ill-fitted vest. In a series of 126 patientstreated with halo immobilization, Kostuik reported hisexperience with halo vest complications.66 A single case ofskull perforation occurred in a patient with severeosteoporosis. Decubitus ulcers, pressure sores, and respi-ratory compromise were especially prevalent in quadriple-gic patients immobilized with a halo cast/vest.
FIGURE 27–6. Halo vest orthosis.
C7-T1
20%
C6-C7
26%
C5-C6
Motion segment
28%
C4-C5
38%
C3-C4
32%
C2-C3
42%
100
Per
cent
of m
otio
n al
low
ed in
halo
-ves
t ort
hosi
s
50
25
75
FIGURE 27–7. Halo vest immobilization does not restrict all cervical spinemovement. The proportion of normal cervical spine motion allowed in ahalo vest at each level averages 31% and ranges from 42% in the uppercervical spine to 20% in the lower cervical spine. (From Koch, R.A.;Nickel, V.L. Spine 3:103–107, 1978.)
TABLE 27–1z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Complications of Halo Ring Immobilization
Complication % of Patients
Pin loosening 36Pin site infection 20Severe pin discomfort 18Pressure sores 11Nerve injury 2Dysphagia 2Bleeding at pin sites 2Dural puncture 1
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z zFrom Garfin, S.R., et al. J Bone Joint Surg Am 68:320–325, 1986.
750 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 5/31 P 750 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 5/31 P 750 BLACK T

Acute pin infection and subsequent loosening remainthe most common problems associated with halo vests andcan occur in up to 60% of patients. Pin sites should becleaned with hydrogen peroxide twice daily, and antibioticointments or sterile dressings are not usually necessary.Focal erythema about the pin typically suggests pin loosen-ing, local infection, or both. A loose pin can be gentlyretightened once; however, multiple attempts at retighten-ing will risk penetration of the internal cortex and shouldbe avoided. In the face of recurrent loosening, a new pinshould be placed in an adjacent location and the loose pinremoved. Pin site infection can usually be treated with oraland topical antibiotics and retention of the pin. Whenpin site drainage or abscess formation persists, the pinshould be removed only after a new pin is inserted at adifferent site.
Loss of cervical reduction is a major concern with anyhalo vest and occurs in about 10% of patients. Poorly fittedvests and patient noncompliance with the orthosis are themajor causes of loss of reduction if the original indicationfor a halo vest is appropriate. Regardless of the reason, aninability to maintain reduction with the halo vest necessi-tates either longitudinal traction or operative stabilization.
Spinal Orthoses
Spinal orthoses are external devices that can restrictmotion of the spine by acting indirectly to reinforce theintervening soft tissue. Because of a lack of standardregulations, spinal orthotic appliances are currently avail-able in a wide diversity of designs and materials. Thereported claims touting the stabilizing properties of manyspinal braces parallel the paucity of scientific data soundlydocumenting their clinical efficacy. Additionally, the effec-tiveness of cervical bracing for the specific injury isdifficult to determine because it is entirely dependent onthe willingness of the patient to comply with orthotic use.
Despite the heterogeneity of designs, the theoreticalfunctions of all spinal braces are analogous and includerestriction of spinal movement, maintenance of spinalalignment, reduction of pain, and support of the trunkmusculature. In conjunction with these mechanical func-tions, spinal braces also function psychologically as kines-thetic reminders for the patient to modify activity. Spinalbraces achieve their stabilizing effects indirectly, with theireffectiveness being a function of the rigidity of the spine-enveloping tissues, the distance between the spine and thebrace (i.e., thickness of the intervening tissue), the lengthand rigidity of the orthosis, the degree of mobility of thespinal segment to be stabilized, and the presence ofpotential anatomic fixation points. Although spinal bracesare generally applied to stabilize a specific spinal motionsegment, their immobilization properties affect the entirespinal region (i.e., cervical, thoracic, and lumbar). Thematerials used for bracing (rubber, foam, plastics) shouldbe lightweight and elastic and allow for ventilation, im-proved hygiene, and comfort.
CERVICAL BRACES
Cervical spine bracing is particularly challenging becauseof the wide range of normal spinal motion in extent,
direction, and variation of movements. As a result of theinability of the vital structures in the neck to withstandprolonged compression, cervical braces use the craniumand thorax as fixation points. The effectiveness of anycervical brace is a function of (1) orthotic design andstabilizing properties, (2) specific injury biomechanics,and (3) the patient’s compliance. Cervical orthoses (COs)can be used as definitive therapy for some spinal injuriesor as a temporary immobilizer for postinjury transport orduring the early hospital diagnostic process. These bracescan generally be divided into two basic types: COs andhigh and low cervicothoracic orthoses (CTOs) (Fig. 27–8).
COs include both soft and rigid cervical collars. Theformer are basically foam cylinders that encircle the neck(Fig. 27–9A). The mechanical function of soft collars isminimal, and they permit up to 80% of normal cervicalmotion.59, 60, 64 Soft collars act principally as propriocep-tive ‘‘reminders’’ for the patient to voluntarily restrict neck
FIGURE 27–8. Basic classification of cervical and cervicothoracic braces:cervical orthoses (A), high CTOs (B), and low CTOs (C). (Redrawn fromSypert, G.W. External spinal orthotics. Neurosurgery 20:642–649, 1987.)
751CHAPTER 27 • Management Techniques for Spinal Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 6/31 P 751 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 6/31 P 751 BLACK T

motion and provide some psychologic comfort. Patientcompliance with soft collars is usually high because of thecomfort and minimally restrictive nature of the brace. Softcollars are indicated for mild cervical sprains or to providepostoperative comfort after stable internal fixation.
High-thoracic CTOs have molded occipital-mandibularsupports that extend to the upper part of the thorax,typically not lower than the level of the sternal notch
anteriorly and the T3 spinous process posteriorly22 (seeFig. 27–8B). Rigid collars encompass a very heterogeneousgroup of cervical brace designs and include the Philadel-phia collar, the Miami J brace, the NecLoc collar, theNewport/Aspen collar, the Stifneck collar, the Malibubrace, and the Nebraska collar, among others. High-thoracic CTOs stabilize the cervical spine by maintainingsome tension between the occiput/mandible and the upperpart of the thorax. They are significantly more effectivethan soft collars. Biomechanical differences, however, existeven among the various high-thoracic CTO designs. Thecomparative effectiveness of the various COs and CTOs inrestriction of total cervical motion is presented in Table27–2. The immobilizing properties of selected COs andCTOs for specific cervical motion segments are depicted inTables 27–3 and 27–4.
The Philadelphia collar (see Fig. 27–9B), the mostpopular high-thoracic CTO, is a very comfortable orthosisfor patients.60, 86 It can restrict 71% of normal cervicalflexion and extension, 34% of lateral bending, and about54% of normal rotation.42, 59, 60 Despite its popularity, thePhiladelphia collar is less effective than the Miami J,NecLoc, or Stifneck in restricting cervical motion. Inaddition, its higher skin contact pressure on the occiputmay result in scalp ulcerations, especially in supinepatients.101 The Philadelphia collar is optimally indicatedfor the management of cervical sprains, as a temporaryimmobilizer during the spine trauma diagnostic process,or to provide postoperative support for an internallystabilized spine.
Among the high-thoracic CTOs, the Miami J collar isthe most effective brace in stabilizing all planes of thecervical spine.52 The Miami J collar generally limits 73% offlexion-extension, 51% of lateral bending, and 65% ofrotation.86 This collar causes less occipital and mandibularskin pressure and is therefore considered an excellentlong-term cervical immobilizer for a severely unstable
TABLE 27–2z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Comparison of Total Cervical Motion Restricted by Various Cervical Orthoses
Orthosis
Motion Restricted (%)
Combined Flexion-Extension Flexion Extension Lateral Bending Axial Rotation
COSoft collar59, 64 26 23 20 8 7
High-thoracic CTOPhiladelphia59, 64, 109* 70 74 59 34 56Miami J109* 73 85 75 51 65NecLoc64* 80 86 78 60 73Newport/Aspen55* 62 59 64 31 38Stifneck52* 70 73 63 50 57Malibu81 — 86 82 55 74Nebraska2 87 74 60 75 91
Low-thoracic CTOSOMI59 72 93 42 34 66Yale59 86 — — 61 76Four poster59 79 89 82 54 73Minerva113 79 78 78 51 88LMCO2 83 68 66 50 60
Halo vest59 96 — — 99 96
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z*Askins, V.; et al. Spine 22:1193–1198, 1997.Abbreviations: CO, cervical orthosis; CTO, cervicothoracic orthosis; LMCO, Lehrman-Minerva CO; SOMI, sternal-occipital-mandibular immobilizer.
FIGURE 27–9. Cervical braces: the soft collar (A) is made of firm foamheld around the neck with Velcro closure; the Philadelphia collar (B),which is made of flexible polymer molded to the mandible and occiput,supports and extends down to the upper part of the thorax; and theSOMI (sternal-occipital-mandibular immobilizer) (C) is an extendedcervicothoracic orthosis that consists of a rigid metal frame that rests onthe thorax and padded metal strips that pass over the shoulders.
752 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 7/31 P 752 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 7/31 P 752 BLACK T

cervical injury.101 Another high-thoracic CTO, the NecLoccollar, is commonly used in the prehospital setting forpatient extrication and transport. Its excellent biomechan-ical properties are further enhanced by its ease of applica-tion. The NecLoc collar restricts up to 80% of flexion-extension, 60% of lateral bending, and 73% of axialrotation.64, 109
The Newport/Aspen collar provides better spine immo-bilization than the Philadelphia collar but to a lesser extentthan the Miami J or the NecLoc55, 81; it limits only 62% ofcervical flexion-extension, 31% of lateral bending, and38% of rotation.52, 55, 86 The major advantage of theNewport/Aspen collar is its comfort and low risk of skinulceration. Plaisier and colleagues studied the risk of skinulceration with various CTOs by measuring their effect on
local capillary closing pressure.101 Only the Newport/Aspen CTO had contact pressures below capillary closingpressure.
Among high-thoracic CTOs, the Stifneck collar isunique in that it is a one-piece orthosis. The effectivenessof cervical stabilization by the Stifneck is comparable tothat of the Philadelphia collar, and its ease of applicationfavors use in the prehospital setting. The Malibu rigidhigh-thoracic CTO has a design similar to that of anextended Philadelphia collar; however, it is more effectivein limiting cervical spine motion. In a study by Lunsfordand co-workers, the Malibu brace outperformed the MiamiJ and Newport/Aspen collars by limiting total cervicalmotion.81 The Nebraska collar, which is a variation of theMinerva orthosis, has a high support for the occiput along
TABLE 27–3z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Comparison of Flexion Restricted by Various Cervical Orthoses at Each Motion Segment
Orthosis
Normal Flexion Restricted (%)
Occ–C1 C1–C2 C2–C3 C3–C4 C4–C5 C5–C6 C6–C7 C7–T1
COSoft collar59 −86* 33 37 24 18 13 22 14
High-thoracic CTOPhiladelphia59 −29 49 78 68 55 46 50 38Miami J† 27 70 51 62 56 57 62 —NecLoc64† 40 72 71 73 69 58 67 —Newport/Aspen55† −20 54 27 38 65 15 33 —Stifneck52† −2 54 38 57 47 49 43 —
Low-thoracic CTOSOMI59 −300 65 87 84 81 75 77 65Yale59 −100 38 74 83 80 83 80 64Four poster59 −210 43 76 78 82 74 70 69Minerva113 −24 60 62 68 78 67 65 —
Halo vest59 −39 77 68 65 80 86 76 —
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z*Negative values demonstrate a ″snaking″ effect.†Askins, V.; et al. Spine 22:1193–1198, 1997.Abbreviations: CO, cervical orthosis; CTO, cervicothoracic orthosis; SOMI, sternal-occipital-mandibular immobilizer.
TABLE 27–4z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Comparison of Extension Restricted by Various Cervical Orthoses at Each Motion Segment
Orthosis
Normal Extension Restricted (%)
Occ–C1 C1–C2 C2–C3 C3–C4 C4–C5 C5–C6 C6–C7 C7–T1
COSoft collar59 24 67 18 26 30 26 9 3
High-thoracic CTOPhiladelphia59 62 25 63 56 41 44 30 51Miami J* 72 58 64 54 55 55 51 —NecLoc64* 84 51 79 72 65 58 46 —Newport/Aspen55* 57 51 65 56 53 58 37 —Stifneck52* 63 52 39 49 56 55 28 —
Low-thoracic CTOSOMI59 50 11 8 20 39 43 32 23Yale59 59 42 66 64 58 61 53 63Four poster59 49 47 58 60 65 72 63 64Minerva113 48 49 21 44 41 65 48 —
Halo vest59 80 57 85 100 97 84 76 —
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z*Askins, V.; et al. Spine 22:1193–1198, 1997.Abbreviations: CO, cervical orthosis; CTO, cervicothoracic orthosis; SOMI, sternal-occipital-mandibular immobilizer.
753CHAPTER 27 • Management Techniques for Spinal Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 8/31 P 753 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 8/31 P 753 BLACK T

with a strap placed around the forehead and a shortbreastplate.2 The Nebraska collar was found to be evenmore effective than some low-thoracic CTOs (i.e., SOMI[sternal-occipital-mandibular immobilizer]) in restrictingall planes of cervical motion.2
Low-thoracic CTOs, similar to high-thoracic CTOs,attach to the cranium at the occiput and mandible, butthey extend to the lower part of the thorax below thesternal notch and T3 spinous process22 (see Fig. 27–8C).Commonly used low-thoracic CTOs include the SOMI, theYale brace, the four-poster brace, and the Minerva-typeorthoses. All these braces provide better fixation to thehead and trunk than high-thoracic CTOs and are thereforethe most effective of all cervical braces. The majordifference between high- and low-thoracic CTOs is theability of the latter to provide better control of spinalrotation and sagittal motion in the mid and lower cervicalspine.
The SOMI (see Fig. 27–9C), the most popular low-thoracic CTO, consists of rigid metal frames with paddedshoulder straps, a strap placed around the trunk, andvariable sizes of the chest component. The SOMI brace ismost effective in stabilizing the C1–C5 region, especially inflexion-extension, and is therefore recommended forupper cervical fractures that are unstable in the sagittalplane (i.e., type II hangman’s fracture). SOMI braces arereported to be comfortable and well tolerated by patients,especially in the upright position.
The Yale brace is a modified form of the Philadelphiacollar that has a molded plastic shell extending over thefront and back of the thorax. The Yale brace restricts 87%of flexion-extension, 61% of lateral bending, and 75% ofaxial rotation.60 This brace is more effective than the SOMIin limiting flexion-extension at C2–C3 and C3–T1, butless effective at C1–C2.58 Similar to other CTOs, the Yalebrace does not provide sufficient control of motion at theocciput–C1 level. Patient comfort and compliance are highwith the Yale brace, and the lack of bulky posteriorcomponents (similar to the SOMI) can further enhancepatient comfort while lying prone. Most four-poster braces
are less accepted by patients because of their bulkyposterior components.
Minerva-type braces have extended occipital supportand are equipped with a forehead strap for better immobi-lization of the head.113 These braces provide adequatecervical spine immobilization from C1 to C7. Whencompared with other CTOs, Minerva-type braces offerbetter control of flexion-extension at C1–C2 and can limitup to 88% of normal axial rotation.113 In one analysis oftotal residual cervical motion, the Minerva orthosis hadstabilizing characteristics comparable to those of a halo vestorthosis.14
Studies to date have demonstrated that all cervical spineorthoses possess inherent deficiencies. Although bothhigh- and low-thoracic CTOs can significantly restrictupper cervical spine motion, ‘‘paradoxical’’ motion or‘‘snaking’’ can usually occur in sagittal flexion at theocciput–C1 level. ‘‘Snaking,’’ which can also occur withhalo vest stabilization,60 is least pronounced with Minerva-type orthoses.14 Comparative studies of the biomechanicalproperties of cervical braces reveal significant variability inall planes of cervical motion measured. Moreover, mostclinical studies of cervical bracing typically use healthyvolunteers, and it is clear that ultimate orthotic perfor-mance may differ significantly in an unstable cervical spine.The altered spinal biomechanics after injury in combina-tion with associated soft tissue spasms may adversely affectthe effectiveness of the orthosis in clinical settings. Finally,although general indications have been established forspecific cervical brace applications60 (Table 27–5), noclinical consensus has been reached on the suitability ofeach CO for a specific spine injury. Therefore, it isimperative that the physician individualize selection of aparticular cervical brace on the basis of injury type andpatient profile.
The duration that a cervical brace is applied is alsocontroversial and depends on the function that it is serving.Brace use can be limited to protecting the patient duringtransport or throughout the emergency evaluation process.For confirmed unstable spinal injuries, these orthoses can
TABLE 27–5z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Recommended Orthosis for Selected Cervical Injuries
Injury Motion Segment Affected Plane of Instability Recommended Orthosis
Ring C1 (Jefferson’s fracture)Stable Occ–C1 All Yale braceUnstable Occ–C2 All Halo vest
Odontoid fracture (types II and III) C1–C2 All Halo vestAtlantoaxial instability C1–C2 Flexion SOMIHangman’s fracture
Stable C2–C3 Flexion SOMIUnstable C2–C3 All Halo vest
Midcervical flexion injuries C3–C5 Flexion Yale brace, SOMILow-cervical flexion injuries C5–T1 Flexion Yale brace, SOMI,
Four-poster braceMidcervical extension injuries C3–C5 Extension HaloLow-cervical extension injuries C5–T1 Extension Yale brace,
Four-poster brace
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z zAbbreviation: SOMI, sternal-occipital-mandibular immobilizer.
754 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 9/31 P 754 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 9/31 P 754 BLACK T

be used in combination with restricted activity untildefinitive treatment can be implemented. In patients withstable fractures or minor soft tissue injuries, COs can beused for several weeks or months until the patient’ssymptoms and risk have resolved.
THORACIC AND LUMBAR BRACES
The thoracic spine is unique among spinal regions in termsof its inherent rigidity and location between highly mobileadjacent cervical and lumbar segments. The midspinelocation of the thoracic segments makes this region partic-ularly amenable to bracing. Furthermore, the rib cage,sternum, and shoulder girdle act as additional stabilizers.However, achieving significant restriction of movement inan unstable thoracic spine can be difficult because of thecontinuous breathing movements. In addition, rotation,the principal motion of the thoracic spine, is much moredifficult to control than flexion and extension. Therefore,thoracic spinal bracing is indicated only for acute spinaltrauma or postoperative support, and it is rarely effectivefor degenerative disorders.
The lumbar spine, particular its lower segments, isdifficult to brace because of the limited caudal fixationpoints and its physiologic hypermobility. Typically, ade-quate stabilization requires that the brace extend as muchas four or five vertebral levels proximal and distal to theunstable segment.13 Even when the brace includes ahip spica component, hip flexion is not adequatelycontrolled, and this mobility results in inadequate lumbarprotection.8
The goal of thoracolumbar bracing is to support thespine by limiting overall trunk motion, decreasing muscu-lar activity, increasing intra-abdominal pressure, reducingspinal loads, and limiting spinal motion. Current availableorthoses include lumbosacral corsets, Jewett braces, andfull-contact custom-molded orthoses. Selection of theappropriate orthotic is dependent on the type of injury, theextent of spinal stability, associated injuries, body habitus,and the patient’s age.7, 119
Lumbosacral corsets and elastic bands are generallyused to diminish pain, decrease lumbar spine mobility, andsupport the paraspinal muscles. Although these bracesreduce overall upper trunk motion, they have little effecton intersegmental spinal motion or loads. Neither soft norrigid corsets have any stabilizing effect on sagittal, axial, ortransverse intervertebral translation.8 Corsets decrease lowback pain primarily because they act as a ‘‘reminder’’ to thepatient to avoid excessive forward or lateral bending.Paradoxically, however, increased motion can occur atL5–S1 as a result of long lumbosacral corsets. Corsetsshould therefore be restricted to patients with stable injurypatterns or elderly patients with osteoporosis.7 Among thepotential adverse effects of lumbosacral corsets are disusemuscle atrophy, osteopenia/osteoporosis, psychologic de-pendency, and concentration of forces at the lumbosacraljunction.
One of the oldest and probably the most reliablethoracolumbosacral orthosis (TLSO) is the Jewett hyperex-tension brace (Fig. 27–10). This brace applies three-pointfixation anteriorly at the sternum and pubis and posteriorlyat the thoracolumbar junction to maintain the thoracolum-
bar spine in extension. The brace allows for hyperexten-sion, prevents flexion, and is lightweight and easily adjust-able. The Jewett brace is generally recommended forpatients with injuries at the T6–L3 region that are unstablein flexion.7 Nagel and associates demonstrated that theJewett brace reduces intersegmental motion and flexion atthe thoracolumbar junction whereas lateral bending andaxial rotation are not affected because of its lack of pelvicsupport.93 In a finite-element model simulating thora-columbar injuries, the Jewett hyperextension brace re-stored stiffness to normal values in one- and two-columnlumbar fractures, but it was ineffective for three-columninjuries.99
In a cadaver study, Nagel and colleagues compared theeffectiveness of the Taylor-Knight brace, the Jewett brace,and a body cast in immobilizing the L1–L2 segment afterprogressive ligament injury in the posterior, middle, andanterior columns.93 The Taylor-Knight brace effectivelyreduced flexion and lateral bending, but it provided littleresistance to axial rotation. The Jewett brace reducedflexion 40%, but it also had minimal effect on lateralbending or rotation. Only the body cast markedly reducedintersegmental spinal motion in all planes.
The full-contact TLSO is currently the most effectiveorthosis for nonoperative management of patients withthoracolumbar fractures.99 The advantages of a custom-molded full-contact TLSO (Fig. 27–11) include distribu-tion of force over a large surface area, improved fixation ofthe pelvis and thorax, better control of lateral bending andaxial rotation, consistent patient and nursing acceptance,and improved, nonobscured radiographs.7 Theoretically,the TLSO allows for correction of deformity by patientpositioning during the molding process. In patients withcompromised sensation, a total-contact orthosis is alwayspreferable to a cast because it can be removed for skinmonitoring and readily adjusted to relieve areas subjectedto excessive pressure.
Reid and co-workers reviewed patients with thora-columbar burst fractures who were treated with a custom-
FIGURE 27–10. The Jewett brace is a three-point fixation system (arrows)that maintains extension of the thoracolumbar area. The brace has a lightadjustable aluminum frame that allows free extension but preventsflexion.
755CHAPTER 27 • Management Techniques for Spinal Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 10/31 P 755 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 10/31 P 755 BLACK T

molded TLSO and permitted early ambulation.102 Allpatients healed without loss of spinal alignment or progres-sion of neurologic deficit. Studies by Cantor and colleaguesand Mumford and co-workers also reported favorableresults without complications for patients with thora-columbar burst fractures treated with custom-moldedTLSOs.25, 92 Studies suggest that custom-molded TLSOsare indicated for patients with instabilities in more thanone plane, impaired skin sensation, or multiple osteopo-rotic compression fractures. A total-contact TLSO maybe indicated for very obese or noncompliant patients.7
Custom-molded TLSOs had a greater immobilizing effectthan lumbosacral corsets and chair-back braces; however,overall restriction of trunk rotation was limited in all thesebraces.68
Biomechanically, lumbar braces were found to be mosteffective at the center and to have increased spinal motionat the ends of the brace.40 The Baycast jacket limitedintersegmental spinal motion to 50% to 60% of normal;extension of the Baycast jacket with a leg spica (Fig.27–12) additionally reduced spinal motion at the L4–L5and L5–S1 regions to 12% and 8% of the normal range.40
Treatment protocols for application of a thoracolumbarbrace vary greatly among physicians. It is preferable thatbraces be worn at all times, during sleep and all dailyactivities. Standard total-contact TLSO or other braces donot effectively immobilize segments below L4 and aboveT8, so a spica TLSO with 15° to 30° of hip flexion isrecommended for injuries below L4 and a custom-moldedcervical extension for injuries above T8.
SPECIFIC BEDS FORSPINE-INJURED PATIENTSz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Bed selection in the management of patients with spineinjuries is critical for optimal reduction and prevention
of secondary complications. Standard hospital beds aresuitable for most cervical, thoracic, and lumbar injuries inthe acute setting but should be modified with an ‘‘eggcrate’’ mattress to prevent decubitus ulcers. These beds arepreferable for multitrauma patients so that traction can beapplied to both the cervical spine and extremities. Patientscan be logrolled if the other injuries allow.
Prolonged immobilization can be the principal cause ofmorbidity in bedridden patients; therefore, early mobili-zation of spine-disabled patients on special rotating bedswas developed for that purpose. The bed is usuallymaintained in perpetual motion with each patient rotatedmore than 200 times a day. Bed mobility is generally onlyinterrupted for treatment, feeding, diagnostic tests, andpersonal hygiene.
Two types of beds with turning frames are currentlypopular. In the Stryker bed, the patient is turned along thelongitudinal axis to allow dorsal skin care and personalhygiene. Traction can be applied in the longitudinal axis,but it is very difficult to achieve traction forces in any otherplane. The suitability of this frame for cervical spineimmobilization has been criticized.87, 114 The Rotorestframe is a table that continuously turns the patient equallyfrom side to side in an affixed posture, with a maximalexcursion of 124° every 4.5 minutes (Fig. 27–13). Skeletalalignment is achieved by a series of adjustable supportpacks that create surface compartments. Centrally placedcervical, thoracic, and pelvic hatches permit wound care,personal hygiene, lumbar puncture, chest auscultation,and bowel and bladder hygiene without altering thepatient’s position. The Rotorest frame allows for tractionforces in multiple planes, both to the axial skeleton and tothe extremities.
McGuire and colleagues compared the Stryker frameand the Rotorest in unstable cervical and lumbar seg-
FIGURE 27–11. A custom-molded thoracolumbosacral orthosis must befabricated by a skilled orthotist. After fitting, the skin should be checkedfor excessive pressure, and if present, the brace should be modified.Molding for the orthosis should be delayed if the patient has abdominaldistention or excessive weight gain from fluid retention. (Redrawn fromSypert, G.W. External spinal orthotics. Neurosurgery 20:642–649, 1987.)
FIGURE 27–12. Custom-molded thoracolumbosacral orthosis extendedwith a lumbosacral spica. (Redrawn from Sypert, G.W. External spinalorthotics. Neurosurgery 20:642–649, 1987.)
756 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 11/31 P 756 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 11/31 P 756 BLACK T

ments and demonstrated that the Rotorest bed wasmore effective.87 The Stryker frame permitted significantdisplacement of both unstable lumbar and cervical seg-ments during transition from the supine to the proneposition.
NONOPERATIVE MANAGEMENTOF SPECIFIC SPINAL INJURIESz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Occipitocervical Injuries
Occipitocervical injuries (Fig. 27–14) are usually lethal,but when the rare patient is encountered, it is imperativethat the physician have a high index of suspicion toproperly ensure the patient’s survival. Occipitocervicalmalalignment can be determined by using the Powers ratioto assess the lateral radiograph (Fig. 27–15). Initially, alloccipitocervical subluxations or dislocations should be me-ticulously immobilized on a backboard with sandbags andtape to secure the position of the head. Type I (anterior)and III (posterior) injuries (Fig. 27–16) can be treated withminimal traction (5 lb), but the pins should be placed in amanner that allows slight extension or flexion, respectively,to achieve reduction.121 In type II (axial distraction)injuries, occiput alignment is generally acceptable, andtraction involving any degree of distraction is strictlycontraindicated. This injury is extremely unstable, andposterior occipital-cervical fusion with at least 3 months ofhalo vest immobilization is more appropriate definitivetreatment. Lateral flexion-extension stress radiographs areessential to document stability before halo removal.
Occipital condyle fractures occur quite frequently andcan usually be managed nonoperatively (Fig. 27–17).Type I (impacted occipital condyle fracture) and type II(occipital condyle fracture in conjunction with a basilarskull fracture) fractures typically require only in situimmobilization with a cervical collar for 8 weeks.5 Themore unstable type III injury (occipital condyle fractureplus an avulsion fracture caused by pull of the alar
A
B
C
� 1
O
BCOA
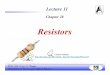
FIGURE 27–15. The Powers ratio is a value of the distance between thebasion (B) and the posterior arch of the atlas (C) divided by the distancebetween the opision (O) and the anterior arch of the atlas (A). Normally,the Powers ratio is 1 or less. A Powers ratio greater than 1 suggestsanterior occipitocervical subluxation or dislocation. (Redrawn fromEismont, F.J.; Frazier, D.D. In: Levine A.M.; et al., eds. Spine Trauma.Philadelphia, W.B. Saunders, 1998, p. 198.)
FIGURE 27–13. A rotating bed used for multiple-trauma and spine-injured patients permits access to all areas of the body. Pulmonary andskin problems are reduced by the rotating motion.
FIGURE 27–14. Fixed occipitocervical subluxation in a 12-year-old boywithout a neurologic deficit.
757CHAPTER 27 • Management Techniques for Spinal Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 12/31 P 757 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 12/31 P 757 BLACK T

ligament) requires halo vest immobilization for 12 weeks.Surgery is warranted for occipital condyle fractures onlyafter an attempt at conservative treatment is unsuccessfulbecause of occipitocervical pain.5
Fractures of the Atlas
Fractures of the atlas can generally be treated nonopera-tively if the fracture is stable and in acceptable alignment.Atlas fractures frequently occur in conjunction with othercervical spine injuries, and these other injuries will oftendetermine the optimal method of treatment. Most isolatedatlas fractures are stable because of an intact transverseligament (Fig. 27–18), are not associated with neurologicdeficit, and can usually be treated nonoperatively. Posteriorarch fractures are generally stable and nondisplaced andrequire only a high-thoracic CTO for 2 to 3 months. Whenthe transverse ligament is disrupted, a Jefferson or lateralmass fracture can result in greater than 7 mm of lateraldisplacement (Fig. 27–19). These fractures will benefitfrom cervical traction to achieve reduction and eventualhalo vest stabilization (Fig. 27–20).
Axial traction should be applied through a halo ring (asopposed to tongs) to facilitate eventual vest application.Weight should begin at about 10 lb and typically beincreased gradually up to as much as 40 lb before fullreduction of the ring can be appreciated on an open-mouthview. Patients must be maintained in traction for at least 4weeks for sufficient healing to permit placement in a halovest. Traction is removed while the patient remains supine,and an open-mouth radiograph is taken after 1 hour. Iflateral mass symmetry is maintained, a halo vest is applied.If malalignment recurs, traction is reapplied and healingreevaluated at 2-week intervals. Traction may be necessaryfor up to 6 to 8 weeks before halo vest support can be
FIGURE 27–16. Classification of occipitocervical subluxation and dislo-cation proposed by Traynelis and colleagues. (From Traynelis, V.C.; et al.J Neurosurg 65:863–870, 1986.)
Type I
Type II
Type III
FIGURE 27–17. Anderson-Montesano classification of occipital condylefractures. (From Anderson, P.A.; Montesano, P.X. Spine 13:731–736,1988.)
FIGURE 27–18. A Jefferson fracture of the atlas with a preservedtransverse ligament.
758 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 13/31 P 758 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 13/31 P 758 BLACK T

applied for an additional 6 weeks. When reduction cannotbe achieved or maintained or the patient is unable totolerate prolonged traction or a halo vest orthosis, surgicalreduction and fusion are warranted.
Transverse ligament disruptions without fractures of theatlas are extremely unstable. Additionally, these injuries areinherently at great risk for neurologic compromise and arebest managed operatively.
Odontoid Fractures
Type I odontoid fractures (apical ligament and bonyavulsion) (Fig. 27–21) are essentially stable and requirelimited if any external support.4 Type III fractures (exten-sion extending below the waist of the odontoid into thebody of C2) usually heal uneventfully. Reduction isachieved by axial halo traction, and to ensure that densalignment is maintained, these injuries are optimally im-mobilized in a halo vest because other COs are associatedwith up to a 15% incidence of nonunion.28 Type IIodontoid injuries (fracture through the waist of the odon-toid) have an extremely high incidence of nonunion andusually warrant operative management. Nonoperativetreatment is reasonable if the injury is recognized early, thedisplacement is minimal and can be reduced, reduction ismaintained, and the patient is not elderly.15, 28
Nonoperative treatment is initiated with halo ringtraction. Traction is usually effective with relatively lightweight (10 to 20 lb), and application of bivector tractioncan assist in correcting translation (if >5 mm) and angula-
FIGURE 27–19. A Jefferson fracture of the atlas with a disrupted transverseligament results in laterally displaced masses of C1 more than 7 mm intotal (a + b).
FIGURE 27–20. Open-mouth view of a significantly displaced C1 fracture taken at the time of injury (A). Traction (30 lb) reduces the deformity (B) andmust be maintained for at least 6 weeks before halo vest application. Late follow-up shows maintenance of reduction (C).
759CHAPTER 27 • Management Techniques for Spinal Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 14/31 P 759 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 14/31 P 759 BLACK T

tion (if >10°). When lateral radiography has confirmed thereduction, a halo vest can be applied. After the patient isupright, serial follow-up radiographs are essential until thefracture has healed. Loss of reduction warrants adjustmentof the halo by neck flexion-extension or sagittal-planetranslation. When malalignment or instability persists,treatment should be operative.
Traumatic Spondylolisthesis of the Axis(Hangman’s Fractures)
Bipedicular or pars interarticularis fractures (hangman’sfractures) of the second cervical vertebra have varyingdegrees of angular or translational stability that determinethe appropriate treatment (Fig. 27–22). Type I fracturesresult from hyperextension and axial loading and haveminimal (less than 3 mm) displacement and angulation(less than 11°) (Fig. 27–23).73 Reduction is not required,and after stable lateral flexion-extension radiographs, ahigh- or low-thoracic CTO for 2 to 3 months is sufficientimmobilization. A similar treatment protocol is appropri-ate for type IA fractures (less than 3-mm translation, butwithout angulation). It is critical that the physicianaccurately distinguish between a stable type I injury andthe more unstable type II injury.
Type II hangman’s fractures (vertical pars fractureadjacent to the body with significant translation andflexion angulation) are extremely unstable. The patient’ssupine hyperextended neck position may spontaneouslyreduce the fracture, and slight flexion stress views may bewarranted to confirm the injury pattern. Reduction isachieved by halo ring application and, with the headslightly extended, gentle cervical traction under fluoro-scopic control. Angulation may correct easily with exten-
sion, whereas residual translation often requires elevationof the torso by placing a rolled towel at the cervico-thoracic junction, which permits the upper cervical spineto translate posteriorly. Postreduction immobilization con-sists of a halo vest if the reduction can be maintainedwithin 3 to 6 mm of normal alignment. If greater than 6 to8 mm of translation persists, the patient is preferablymaintained in halo traction for 4 to 6 weeks and thensecondarily placed in a halo vest. Type II injuries willtypically heal at the pars and anteriorly with some degreeof C2–C3 ankylosis.
Type IIA hangman’s fractures (oblique midpars fractureswith severe angulation and no translation) are also ex-tremely unstable injuries that can be reduced with simpleextension, but distraction is absolutely contraindicatedbecause of complete disruption of the anterior longitudinalligament and annulus and the risk of pronounced axialdisplacement (Fig. 27–24). Once the neck is extended intoa reduced position, a halo vest should be applied underfluoroscopic control and worn for 2 to 3 months.
Type III fractures are uncommon and consist of C2 parsfractures associated with unilateral or bilateral C2–C3 facetdislocation. Nonoperative management (i.e., traction, ma-nipulation) is contraindicated in these injuries because ofloss of continuity between the C2 body and the posteriorelements/facets.
Lower Cervical Spine Injuries
Ligamentous injuries of the lower cervical spine can rangefrom simple sprains without malalignment, to subluxationwith partial loss of cervical spine ligamentous stability, tofrank dislocation with total ligamentous disruption. Lowercervical spine instability has been described by White andco-workers (Table 27–6) and is based on the extent ofsegmental angular or translation displacement129, 130 (Fig.27–25). Dislocations may spontaneously reduce withsupine positioning, and the degree of instability is oftennot easily appreciated on a static radiograph. Likewise,dislocations may become fixed or locked in a malalignedposition and require cervical traction or open manipula-
Type I
Type II
Type III
FIGURE 27–21. Anderson and D’Alonzo classification of odontoidfractures.
D
�
FIGURE 27–22. The severity of traumatic spondylolisthesis of the axis(hangman’s fractures) is characterized by angulation (α) and translation(D). (Redrawn from Levine, A.M. In: Levine A.M.; et al., eds. SpineTrauma. Philadelphia, W.B. Saunders, 1998, p. 280.)
760 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 15/31 P 760 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 15/31 P 760 BLACK T

tion for reduction. After reduction and depending on theextent of disruption of the posterior ligamentous complex,cervical immobilization in a cervical orthosis for 6 to 8weeks is sufficient. If reduction cannot be maintainedor pain persists after adequate immobilization, operativestabilization is indicated.
Cervical compression fractures involve less than 50%loss of anterior vertebral body height and maintenance ofposterior ligamentous integrity. Usually, a CO for symp-tomatic relief is sufficient treatment for this stable frac-ture. When compression of the anterior vertebrae exceeds50% of the vertebral body height, flexion-distraction oc-curs in conjunction with posterior ligamentous disruption.Flexion–axial compression loading injuries associated withdisc disruption plus an anterior vertebral body fracture aremore challenging because CO or halo vest immobilizationalone is plagued by a high incidence of persistent fracturedisplacement and loss of alignment.29 Moreover, when theinjury pattern also includes disruption of the facet capsule
Type I Type II Type IIIType IIA
FIGURE 27–23. Levine and Edwardsclassification of traumatic spondy-lolisthesis of the axis (hangman’sfracture).
FIGURE 27–24. Type IIA hangman’s fracture before traction (A) and after cervical traction has been applied (B). Traction is contraindicated fortype IIA hangman’s fractures because it leads to significant overdistraction.
TABLE 27–6z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Checklist for the Diagnosis of Clinical Instabilityof the Lower Cervical Spine
Element Points*
Anterior elements destroyed or unable to function 2Posterior elements destroyed or unable to function 2Radiographic criteria 4
Sagittal displacement >3.5 mm 2Relative sagittal angulation >11° 2
Positive stretch test 2Spinal cord injury 2Nerve root injury 1Abnormal disc narrowing 1Dangerous loading anticipated 1
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z*A total of 5 or more points represents instability.Source: White, A.A.; et al. Spine 1:15–27, 1976.
761CHAPTER 27 • Management Techniques for Spinal Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 16/31 P 761 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 16/31 P 761 BLACK T

and posterior ligamentous structures, a significant risk forlate instability exists.27, 126
Although unilateral or bilateral facet subluxations, dis-locations, or fractures (or combinations of these injuries)are variations of the same injury patterns, determination ofoptimal treatment requires that distinctions be made be-tween these specific injuries. As unilateral or bilateral facetinjuries progress from subluxation to perched facets andfinally to frank dislocation, the extent of cervical spinemalalignment reflects the degree of facet capsule or poste-rior ligament disruption, or both (Fig. 27–26). Facetsubluxations or unilateral dislocations may achieve somedegree of segmental stability after reduction and nonoper-ative treatment. However, a facet fracture suggests persis-
tent rotational and flexion instability and is most appropri-ately managed surgically.
Reduction of Unilateral or BilateralFacet Injuries
Unilateral and bilateral facet injuries should be reduced byclosed means with skeletal traction in patients who areoriented and able to be assessed neurologically. Afterreduction, unilateral facet dislocations can often be treatedin closed fashion with a halo vest, whereas bilateral facetdislocations are best managed with operative stabiliza-tion. Gardner-Wells tongs should be applied if operativestabilization is anticipated, whereas a halo ring is used forunilateral facet dislocations that are to be maintained in ahalo vest. The patient is placed supine on a bed withapproximately 20° of head elevation to offset the skeletaltraction to be applied. If sedation is used, only mild dosesof analgesics or muscle relaxants (or both) are warranted.Throughout the maneuver, the patient has to remainresponsive and neurologically stable.
Initially, a weight of 10 to 15 lb is applied throughtraction in line with the spine. Serial static radiographs ordynamic fluoroscopy should assess spinal alignment afterthe initial weight is applied and after each subsequentaddition of 5 to 10 lb. Static radiographs are best obtained15 to 20 minutes after each weight increase to allow for softtissue distraction. If the facets unlock, the neck should beslightly extended and the traction weight decreased toapproximately 10 lb to permit the facets to spontaneouslyreduce (Fig. 27–27). Changing the direction of the tractionvector can facilitate the reduction of unlocked facets andassist in maintaining the reduction (Fig. 27–28). Whenspinal reduction has been achieved, halo vest applicationor surgical stabilization should be performed before per-mitting upright mobilization.
Occasionally, resistant unilateral facet dislocations willbenefit from the head and neck being slightly turned away
FIGURE 27–25. Angular displacement 11° greater than thatat the adjacent vertebral segments suggests instability fromposterior ligamentous disruption, just as translation greaterthan 3.5 mm does. (From White, A.A.; Panjabi, M.M.Clinical Biomechanics of the Spine. Philadelphia, J.B.Lippincott, 1978, pp. 236–251.)
FIGURE 27–26. Normal position (A) of the cervical vertebrae in the lateralprojection. A subluxated position (B) is recognized by fanning of thespinous process, increased angulation of the vertebrae, and excessiveseparation of the facets. Perched facets (C) are recognized by the tip of theinferior facet resting on the tip of the superior facet. Dislocated facets (D)are determined by the displacement of the inferior facet anterior to thesuperior facet.
762 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 17/31 P 762 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 17/31 P 762 BLACK T

from the side of dislocation to facilitate disengagement ofthe facet. Bilateral facet dislocations are extremely unstableand will generally reduce with low traction weight andslight flexion, followed by neck extension without rota-tional manipulation. If the patient’s neurologic status be-comes altered during any of these maneuvers, all tractionand manipulation should be terminated and the spinesecured in a neutral position. Open surgical reduction isabsolutely indicated in these patients, as well as those whosimply fail attempts at closed treatment. Reduced unilateralor bilateral facet dislocations can still fail because ofpersistent instability and pain despite halo vest immobili-zation and therefore warrant surgical stabilization.
Eismont and coauthors reported the risk of neurologicdeficit from an associated disc herniation after closedreduction of cervical spine facet dislocations.37 Althoughother authors have reported similar findings,82, 106 theactual incidence of this catastrophe remains relativelylow. Rizzolo and colleagues recommended that imme-diate closed cervical skeletal traction reduction be per-formed without a previous MRI scan only in alert, orientedpatients who are neurologically intact.105 MRI is abso-lutely indicated for patients with neurologic deficit beforetraction and for patients who require open surgical re-duction.
Sears and Fazl reviewed 70 patients with facet injuriestreated in a halo vest and found that stability and anatomicreduction could be maintained with a halo in only 44% and21% of patients, respectively.111 These results corroboratedan earlier study by Koch and Nickel, who demonstratedthat maintaining facet reduction requires constant distrac-tion and that halo vest patients typically experience axialcompression during standing and walking.65 Rorabeck andcolleagues reviewed a group of patients with facet frac-tures, 14 of whom were treated operatively without pain orany need for secondary surgery.108 These patients werecompared with a separate injury group that was treatednonoperatively; in this second group, seven patients hadpain and five patients required secondary surgical proce-dures. Therefore, although unilateral facet fractures canrespond to nonoperative management, a successful out-come is not guaranteed.
Fracture separation of the lateral articular mass, unlikefacet injuries, results from hyperextension or axial load-ing and lateral bending instead of flexion-rotation. Thisparticular injury is often missed on plain radiography,which depicts segmental translation and rotation withoutflexion or facet displacement. When the patient is supine,the displaced lateral mass can reduce spontaneously evenbefore the application of traction. Nonoperative treatment
FIGURE 27–27. Initial position of a unilateral facetdislocation in both the sagittal and the axial planes (A).Traction permits some distraction but not reduction(B). Flexion of the neck increases distraction, but thefacet is still dislocated (C). Lateral tilt away from theside of dislocation unlocks the dislocation (D), andafter extending and putting the neck in a neutralposition, the reduction is completed (E).
763CHAPTER 27 • Management Techniques for Spinal Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 18/31 P 763 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 18/31 P 763 BLACK T

consists of a halo vest and is indicated only if the injury isnondisplaced. Unfortunately, even a nondisplaced fractureseparation may displace secondarily, so surgical stabiliza-tion is preferable for this injury.
Vertebral Body Fractures
Compression fractures of the lower cervical spine arecaused by flexion-induced axial compression forces thatresult in loss of anterior body height and some degree ofdistraction posteriorly. When flexion is combined withsignificant rotation or translation, subluxation of the in-jured vertebra can occur. When the force of injury ispredominantly axial, burst fractures are produced alongwith disruption of the anterior and middle columns and arefrequently associated with neurologic injury (Fig. 27–29).Treatment of both these injury patterns should initiallyconsist of halo traction beginning at 15 to 20 lb andincreasing in 5-lb increments until normal alignment hasbeen restored. Pronounced instability frequently persists inpatients with significant posterior ligamentous disruptionor a large anterior teardrop fracture. Nonoperative treat-ment consisting of a halo vest should be restricted toneurologically intact patients with pure flexion injuries andminimal residual deformity (less than 20° of anterior bodycompression). Patients with unstable injuries who are notcandidates for surgery or a halo vest because of polytraumarequire extended bedrest with halo traction until earlyhealing has been achieved.
Most lower cervical spine injuries will heal with suffi-cient stability if they can be anatomically reduced and thereduction is maintained throughout treatment. Exceptionsinclude torsionally unstable fractures (i.e., lateral mass or
facet fractures) and injuries associated with significant softtissue disruption. Soft tissue or ligamentous injuries areextremely difficult to accurately diagnose with static radio-graphs, and dynamic or stress radiographs are oftennecessary. Dynamic radiographs are also recommended atthe completion of brace treatment. Although nonoperativetreatment is quite effective, the medical and economicimpact of such treatment has been challenged.31 Operativetreatment results in less time in bed, earlier physicaltherapy, and an overall decrease in total cost to society.Therefore, the clinician must carefully determine the inju-ries that are likely to respond favorably to nonoperativetreatment without any risk of late instability, pain, orneurologic deficit.
Teardrop fractures are unique flexion/compression inju-ries in the mid to lower cervical spine (C3–C7) and areextremely dangerous because of the high incidence ofassociated instability and neurologic deficit. Even whenseemingly well aligned, these injuries can progress rapidlyto significant deformity as a result of their extensiveligamentous disruption.
Extension teardrop fractures can be stable (no posteriorligamentous disruption), and thus are suitable for cervicalbrace immobilization for 3 months, with lateral flexion-
Neutral
A
B
Neutral A
A B
FIGURE 27–28. Reduction of a facet dislocation by traction. Facets treatedwith traction in the neutral position will unlock and remain perched.Changing the direction of the traction vector above neutral (to point A)permits reduction of the unlocked facets. Changing the traction vectorbelow neutral (to point B) allows maintenance of reduction at lowertraction weights.
FIGURE 27–29. Burst fracture of the C6 vertebra with partial displacementof the body into the canal (arrow).
764 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 19/31 P 764 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 19/31 P 764 BLACK T

extension radiographs obtained to document stability.Radiographically, unstable teardrop fractures have greaterthan 3 mm of retrolisthesis or more than 11° of angula-tion or give rise to neurologic deficits (or any combina-tion of these findings); such fractures should be placedin tongs traction to restore alignment before surgicalstabilization.
Thoracic Spine Injuries
The thoracic spine is inherently stable because of therigidity created by the structural configuration of the spine,sternum, and rib cage. Injuries in this region usuallyrequire a significant component of axial load or flexion (orboth), and more severe injuries also involve a componentof torsion130 (Table 27–7).
Associated injuries occur in approximately 75% ofthoracic spine injuries and can include rib fractures,pulmonary contusions, pneumothorax, cardiac contu-sions, and vascular injuries. Profound neurologic deficitoccurs more frequently in the thoracic spine than in thecervical or thoracolumbar regions. In a series of 376thoracic spine fractures, 235 (63%) resulted in completeneurologic injuries.89 This high incidence of completeneurologic injury is due to the small size of the neuralcanal, the tenuous arterial blood supply to the thoraciccord, and the high energy required to inflict injury.
Thoracic spine fractures can usually be managednonoperatively when the patient is neurologically intact.Even patients with axial load or burst fractures aregenerally neurologically intact, unless the fracture has acomponent of significant flexion or angulation, rotation, ortranslation.
An injured thoracic spine is more inherently stable thanits cervical or lumbar counterparts; however, orthoticsupport is still essential in allowing earlier mobility andmaintaining spinal alignment (Fig. 27–30). The standard
FIGURE 27–30. Fractures of the high thoracic region (T1–T6) aredifficult to control. In this typical fracture of T3, no immobilization wasused, and at 4 weeks the fracture had collapsed with a kyphoticdeformity of 38°.
TABLE 27–7z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Checklist for the Diagnosis of Clinical Instabilityof the Thoracic and Thoracolumbar Spine
Element Points*
Anterior elements destroyed or unable to function 2Posterior elements destroyed or unable to function 2Radiographic criteria 4
Sagittal displacement >2.5 mm 2Relative sagittal angulation >5° 2
Spinal cord or cauda equina damage 2Disruption of costovertebral articulations 1Dangerous loading anticipated 2
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z*A total of 5 or more points represents instability.Source: White, A.A.; Panjabi, M.M. Clinical Biomechanics of the Spine.
Philadelphia, J.B. Lippincott, 1978, pp. 236–251.
765CHAPTER 27 • Management Techniques for Spinal Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/24/02 33 P 20/31 P 765 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/24/02 33 P 20/31 P 765 BLACK T

orthotic device, the TLSO, can include a cervical extension(CTLSO) for a high thoracic injury. Despite appropriatebracing, certain thoracic spine fractures may be compli-cated by late collapse and deformity. Therefore, thesepatients must be carefully monitored and occasionallymaintained on an initial regimen of strict bedrest beforebrace application. Surgical intervention is warranted ifthe fracture is extremely unstable or bracing is poorlytolerated. Fractures secondary to gunshot injury are usu-ally amenable to bracing even in the presence of a completeneurologic deficit.
Thoracolumbar Spine Fractures
Nonoperative measures have traditionally been the stan-dard treatment of most thoracolumbar spine fractures andare most appropriate for stable thoracolumbar fractures.Before the advent of modern surgical techniques, the onlytreatment available for thoracolumbar fractures was pos-tural reduction with hyperextension and immobiliza-tion.9, 10, 44, 97 Fracture reduction was achieved by gravity,pillows, and manual manipulation in injuries with orwithout neurologic deficit. Although the risk of early orlate neurologic loss was low, the recommended length ofbedrest could approach 12 weeks. Union occurred in up to98% of these patients,9 and the initial indications fornonoperative treatment have even included irreduciblefracture-dislocations, locked facets, and gunshot wounds.
Frankel and coauthors reported on a series of 205thoracolumbar spine fractures treated with postural reduc-tion, bedrest, and orthotic support.44 Partial neurologicdeficit improved in 72% of patients, whereas neurologicdeterioration was noted in only 2% and late instabilityoccurred in only two patients. These authors reservedsurgery for patients with significant or progressive neuro-logic deficit. Currently, nonoperative treatment should bereserved for patients who are neurologically stable or intactand retain spine stability131 (Table 27–8). Post-traumatic
kyphosis of up to 30° has been deemed acceptable inpatients with stable burst fractures and no neurologicdeficit.67
Weinstein and co-workers reported on the long-termoutcome of 42 patients with unstable thoracolumbar burstfractures managed nonoperatively.127 Neurologically intactpatients did not have any worsening of their neurologicdeficit. Spinal kyphosis was 26° in flexion and 17° inextension, and although some back pain was present in90% of patients, only three required late operations.Interestingly, canal patency improved by 22% at follow-upas a result of resorption of bone fragments and canalremodeling. No correlation was found between the initialradiographic severity of the injury and residual deformityor symptoms at follow-up. These authors recommendednonoperative treatment of thoracolumbar fractures in pa-tients with a nonpathologic single-level burst fracture andno neurologic deficit.
Denis reviewed 52 burst fractures without neurologicdeficit that were treated nonoperatively and comparedthese patients with 13 who were stabilized with Harring-ton rods.34 The large sagittal diameter of the spinal canal atthe thoracolumbar junction appeared to also favor nonop-erative treatment of selected burst fractures. However, 25%of the nonoperative patients were unable to return to workfull-time, and late neurologic deterioration developed in18%. Finn and Stauffer determined that the extent ofthoracolumbar spinal canal encroachment did not directlycorrelate with the degree of neurologic deficit.41
Nonoperative treatment of thoracolumbar fractures typ-ically begins with a period of recumbency ranging from3 to 8 weeks. During this time, acceptable alignment of thespine should be achieved and maintained. Afterward, thepatient is maintained in a TLSO for 3 to 4 months andpermitted to ambulate as tolerated. Nonoperative treat-ment is preferred for stable burst fractures in patientswithout neurologic deficit or significant canal compromise(<50%) and with an initial kyphosis of less than 30°. Allnonoperative patients required serial clinical and radio-graphic assessment to detect potential deformity or pro-gression of neurologic deficit.
Factors associated with a successful outcome in thenonoperative treatment of burst fractures of the thora-columbar spine have been identified by several authorsand include the degree of initial kyphosis, the extent ofanterior and posterior body height collapse, the number ofcolumns injured, and the degree of initial canal compro-mise.20, 25, 49, 67, 104 James and associates suggested that anintact posterior column was the best predictor of success intreating a stable burst fracture nonoperatively.56 Reconsti-tution of canal size over time with conservative treatmentwas found to be age dependent, with greater canal recon-stitution occurring in younger patients. Other predictorshave been reported to be residual motion at the fracture siteand the extent of the initial kyphosis.25, 67, 92, 131
Fredrickson and colleagues recommended that nonop-erative treatment be reserved for patients without sig-nificant neurologic involvement (single nerve root orless), significant posterior ligamentous disruption, andtranslation injuries and with less than 25° of initialkyphosis.45 Immobilization in a standard hospital bedand special turning frames (i.e., Rotorest bed) were re-
TABLE 27–8z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Checklist for the Diagnosis of Clinical Instabilityof the Lumbosacral Spine
Element Points*
Anterior elements destroyed or unable to function 2Posterior elements destroyed or unable to function 2Radiographic criteria 4
Flexion-extension radiographsSagittal translation >4.5 mm or 15% 2Sagittal rotation
>15° at L1–L2, L2–L3, L3–L4 2>20° at L4–L5 2>25° at L5–S1 2
Resting radiographsSagittal displacement >4.5 mm or 15% 2Relative sagittal angulation >22° 2
Cauda equina damage 3Dangerous loading anticipated 1
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z*A total of 5 or more points represents instability.Source: White, A.A.; Panjabi, M.M. Clinical Biomechanics of the Spine.
Philadelphia, J.B. Lippincott, 1978, pp. 236–251.
766 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 21/31 P 766 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 21/31 P 766 BLACK T

served for polytraumatized patients restricted to prolongedbedrest.
Nonoperative patients are initially treated with a periodof bedrest that can range from several days to 8 weeks,depending on the degree of fracture instability. Beforeambulation, the patient is fitted for a molded body cast orcustom TLSO. Injuries treated in this manner must be ableto withstand normal weight bearing, but more strenuousactivities (excessive bending, exercising, or lifting) are pro-hibited. Serial radiographs are taken throughout the treat-ment course to ensure that the kyphosis is less than 30°and canal compromise is less than 50%. Clinically, painshould progressively decrease and the patient should re-main intact neurologically; otherwise, surgery is indicated.
SURGICAL MANAGEMENTOF CERVICAL ANDTHORACOLUMBAR INJURIESz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Goals of Surgical Management
Most spine fractures can be treated nonoperatively. Only asmall select group of unstable spine injuries with orwithout neurologic involvement warrant surgical treat-ment. Objectives of surgery include (1) restoration ofspinal alignment, (2) restoration and maintenance of spinalstability, and (3) decompression of compromised neuralelements.
The first goal of surgery is to reduce significant spinedeformity to functionally acceptable alignment. The abilityof any spinal instrumentation system to achieve this goal isbased on its ability to effectively oppose the deformingforces and counteract the existing instability. Selection ofappropriate instrumentation should therefore be deter-mined by the mechanism of the fracture and its subse-quent deforming forces. For example, the use of dis-traction instrumentation for a flexion-distraction type offracture will further destabilize the spine. By contrast, theapplication of extension and compression type of instru-mentation posteriorly would correct this deformity. Incases with associated facet dislocations, care must be takenwhen performing the reduction maneuver to avoidextruding disc material into the spinal canal.74
The second goal of surgery is to restore and maintainspinal stability in an unstable spine. The appropriateselection of instrumentation is again crucial in preventingrecurrence of the deformity. Modern fixation devices forboth anterior and posterior surgical procedures permitbetter stabilization while compromising a minimal numberof motion segments. Advocates of anterior surgical stabili-zation contend that posterior fixation provides insufficientsupport for either axial or compressive loads on a compro-mised anterior spinal column.35 The disadvantage of ante-rior surgery is the increased risk of morbidity because ofthe proximity of great vessels, chest and abdominal viscera,and the spinal cord. Furthermore, deformity reduction andstabilization seem to be less reliable with anterior tech-niques than with posterior procedures despite the recentimprovements in anterior instrumentation.3, 46, 62
Posterior fixation, particularly with the evolution ofpedicle screws, has achieved excellent correction of defor-mity through indirect reduction techniques. Aebi andcolleagues used limited segmental fixation in one clini-cal series and reported correction of kyphosis from 15.8°to 3.5°.1 Lindsey and co-workers demonstrated similarshort-term results with these techniques, although theinitial kyphotic deformity had recurred by the 2-yearfollow-up.78, 79
A principal goal of surgical management is adequatedecompression of the neural elements to allow for maximalrestoration of neurologic function. Decompression can beperformed anteriorly, posteriorly, posterolaterally, trans-pedicularly, indirectly, or any combination of these ap-proaches. Usually, the type of injury and timing of surgicalintervention will determine the most appropriate type ofdecompression (i.e., posterior versus anterior).
Indirect decompression secondary to posterior restora-tion of spinal alignment has been shown to be veryeffective in patients undergoing surgery within 48 to 72hours.50 By applying distraction and correcting angulationwith posterior instrumentation, indirect reduction isachieved through ligamentotaxis. The posterior longitudi-nal ligament becomes taut and can reduce retropulsedbony fragments away from the spinal canal (Fig. 27–31).
The literature suggests that the results of anterior directversus posterior indirect spinal canal decompression aresimilar in patients with incomplete neurologic defi-cits.26, 54, 71, 92 Gertzbein and colleagues reviewed theoutcomes of patients with thoracolumbar fractures andincomplete neurologic deficits treated by anterior (direct)versus posterior (indirect) decompression.48 In patientstreated posteriorly versus anteriorly, neurologic status im-proved in 83% and 88%, respectively. Neurologic improve-ment in both groups was significantly better than the 60%to 70% recovery rate with nonoperative treatment cited inthe literature. In a separate multicenter study49 of 1019patients with thoracolumbar spine fractures who weremonitored for 2 years, the neurologic outcome of anteriorand posterior surgery was similar.
Currently, the posterior indirect reduction technique isthe standard method of treatment of most thoracolumbarspine fractures. Absolute indications for anterior decom-pression include a neurologically incomplete patient withgreater than 50% canal compromise and one or more ofthe following: (1) more than 72 hours postinjury, (2) failedattempt at posterior reduction, and (3) significant loss ofanterior and middle column (vertebral body) supportdespite posterior reduction.
Timing of Surgery
The optimal timing of surgery after spinal injury remainscontroversial. Some clinicians contend that surgery isurgent and should be performed as soon as possible,whereas others support a delay in surgery to allow forresolution of post-traumatic swelling. The only absoluteindication for immediate or emergency surgery is pro-gressive neurologic deterioration in patients with spinalfracture-dislocations and incomplete or no neurologicdeficit.16
767CHAPTER 27 • Management Techniques for Spinal Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 22/31 P 767 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 22/31 P 767 BLACK T

Acute spinal deformity in a traumatized patient alwayswarrants immediate spinal realignment to restore spinalcanal diameter, effect some degree of neural decompres-sion,16 and theoretically maximize the potential for neuro-logic recovery. Currently, no clear scientific evidence hasdemonstrated that immediate surgical intervention willimprove neurologic recovery in patients with acute spinalcord injury. One retrospective study suggests that surgerywithin 72 hours of injury might improve neurologicrecovery and decrease hospitalization time in those withcervical spinal cord injuries.91 In a prospective study,however, Vaccaro and associates found no significantneurologic benefit associated with post-traumatic surgicaldecompression performed less than 72 hours after injuryversus waiting more than 5 days.124 Furthermore, compar-ison of the two groups demonstrated no significant differ-ence in the length of postoperative intensive care stay or thelength of inpatient rehabilitation.
Early stabilization and mobilization of patients withlong bone fractures have proved advantageous in avoiding
complications such as adult respiratory distress syndromeand deep venous thrombosis.51, 57 Such treatment appearsto also be advantageous for spinal injury patients.21, 39
Surgical intervention should be performed expediently toavoid these complications, as well as to allow for earlymobilization, proper skin care, and upright patient posi-tioning. In the absence of neurologic deficit, it is reasonableto delay surgery to facilitate surgical planning and decreasespinal cord and nerve root edema. Furthermore, hematomaorganization occurs at about 48 hours after injury anddecreases intraoperative blood loss.44 An excessive delay insurgery, however, may have adverse effects on the surgeon’sability to reduce the fracture and achieve canal clearance.Other reports have shown that optimal canal clearance isrealized when spine surgery is performed within 4 daysand no later than 7 to 10 days after injury.36, 49, 131
Management of a polytrauma patient with an associatedspinal injury presents a particularly difficult problem,depending on the severity of the other injuries, the degreeof spinal instability, and the patient’s neurologic status.
FIGURE 27–31. L1 burst fracture reduced intraoperatively with ligamentotaxis and stabilized with posterior segmental instrumentation.
768 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 23/31 P 768 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 23/31 P 768 BLACK T

Surgical planning in these patients can be facilitated withthe use of a simple algorithm (Fig. 27–32). The effects ofearly versus late stabilization of spinal fractures in poly-trauma patients have been the focus in several recentclinical studies.24, 88, 112 These studies consistently demon-strated that surgery performed within 72 hours in patientswith an Injury Severity Score greater than 18 significantlydecreased overall patient morbidity and hospital stay(Table 27–9). No significant difference in the rate ofperioperative complications was associated with early sur-gery in polytrauma patients, but blood loss was noted to besignificantly higher in those requiring early anterior spinalapproaches.
In most institutions, stabilization of spinal fractures isperformed in a semiurgent fashion once medical optimiza-tion of the patient has been accomplished, preferablywithin 3 days of the injury. Within this time frame, the
surgical approach/technique should be predicated only onthe nature of the injury. When a prolonged delay isanticipated, every effort should be made to maintain spinalalignment within an acceptable range. Late surgical inter-vention may require more extensive surgery (i.e., bothanterior and posterior approaches or more extensive de-compression) to achieve adequate spinal alignment, de-compression, and stability.
Anesthesia
Induction of anesthesia can be very challenging in patientswith spinal trauma, particularly those with unstable cervi-cal spine fractures and incomplete neurologic deficit.Maintaining alignment of the cervical spine during intuba-tion is vital in preventing neurologic deterioration. Awakefiberscopic intubation is the safest method to achieveairway control, especially in a medically stable patient whodoes not require urgent intubation. Fiberscopic intubationcan be performed through either the nasotracheal ororotracheal route. Nasotracheal intubation is preferred inpatients with associated maxillofacial fractures, but it isabsolutely contraindicated in those with basilar skullfractures.
Multiple reports have shown the beneficial effects ofhypotensive anesthesia in the intraoperative reduction ofestimated blood loss.43, 69, 83, 116 Similar findings werereported by Ullrich and co-workers in a retrospectivestudy comparing normotensive anesthesia with hypoten-sive anesthesia in patients stabilized with Harrington rodinstrumentation for thoracolumbar fractures.123 Blood losswas significantly reduced with hypotensive anesthesia, andno neurologic deterioration was noted intraoperativelywith either the Stagnara wake-up test or somatosensoryevoked potentials (SEPs). Theoretically, low oxygen ten-
Thoracoabdominalsurgery
Thoracolumbar fxORIF
Consider ORIFThoracolumbar fx
Long-bone fxORIFLong-bone fx
ORIF
C-spine fxORIFA
Closed reduction
Incomplete
No neurodeficit
Supine position OK Supine position unsafe
Neurodeficit
Multiple traumawith c-spine injury
Complete
Multiple trauma withthoracolumbar injury
Thoracoabdominalsurgery
B
FIGURE 27–32. Algorithm for the surgical management of polytrauma patients with cervical (A) and thoracolumbar fractures (B).Abbreviation: ORIF, Open reduction internal fixation.
TABLE 27–9z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Effect of Surgical Timing for Patients with Spine Fracturesand an ISS Greater Than 18
Timing of Stabilization
Early (<48 hr) Late (>48 hr)
Patients (n) 16 46GCS 14 13AISS—head 1 3AISS—chest 2 2Ventilator days 1.0 11.0ICU days 3.9 14.0Hospital days 11.0 26.0Average cost $26,250 $54,130
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z zAbbreviations: AISS, Abbreviated Injury Severity Score; GCS, Glasgow
Coma Scale; ICU, intensive care unit; ISS, Injury Severity Score.
769CHAPTER 27 • Management Techniques for Spinal Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 24/31 P 769 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 24/31 P 769 BLACK T

sion can potentially inflict further ischemic injury to thealready traumatized cord, and it is recommended thatmean arterial pressure be kept between 80 and 90 mm Hgduring hypotensive anesthesia.77, 118
Selection of the anesthetic agent is also of criticalimportance and may influence the surgical procedure. Ithas been well documented that some inhalation agentshave an effect on evoked potentials. Sloan maintains thatthe most effective anesthetic regimen used in conjunc-tion with SEPs is low-dose inhalation agents in combina-tion with intravenous infusion of sedatives, preferablypropofol with an analgesic.115 This regimen not onlyallows for reliable recording of SEPs but is also readilyreversible and thus facilitates the use of a wake-up test. Inpatients with spinal cord injury, succinylcholine, a depo-larizing agent, should not be used because it can lead tothe rapid release of potassium and thereby increase the riskfor ventricular arrhythmias and cardiac arrest.
Operative Positioning
The surgical positioning of patients with spinal trauma isa delicate endeavor. Care must be taken to avoid anyneurologic deterioration, yet positioning should not com-promise the exposure for the planned surgical approach.Care must be taken to avoid pressure around the eyes andprevent injury to the globe or retinal artery thrombosis.Padding of all bony prominences and protection of super-ficial neural structures are important. Proper positioning ofthe upper extremities when the patient is prone is crucial toavoid brachial plexus injury. For that purpose, the shouldershould not be overextended and not abducted beyond 90°.Similarly, the ulnar nerve must be protected with the armeither secured at the patient’s side or flexed 90° on apadded arm board. Compression stockings on the lowerextremities are useful in preventing venous congestion.Finally, after positioning, it is important to check for thepresence of distal pulses, especially when the patient is inthe prone position.
CERVICAL SPINE—ANTERIOR APPROACH
The patient can be placed on a regular bed or Strykerframe in the supine position. During positioning, care istaken to maintain spinal alignment. The occiput is paddedwith a circular foam pillow with a center cutout or placedin a Mayfield horseshoe cushion. In that position, axialtraction may be applied in the form of head halter tractionor skull tongs traction (Gardner-Wells tongs). The elbowsare carefully padded to protect the ulnar nerve, and thearms are tucked at the patient’s side. The shoulders may beretracted distally, and longitudinal tape strips can beapplied to allow better intraoperative radiographic evalu-ation of the cervical spine. Care must be taken to avoidexcessive constriction of the arms with the tape and tapingdirectly over the nipples. A roll is placed longitudinallybetween the scapulae to allow for shoulder retraction andextension of the cervical spine for better exposure of theoperative field. Extreme cervical extension should becarefully avoided to prevent increased spinal cord com-pression under anesthesia.
The head is turned away from the incision site. A left- orright-sided approach can be carried out, depending on thesurgeon’s preference. Advocates of the left-sided approachclaim that it is preferable because of the recurrent laryngealnerve’s more consistent course on the left side; proponentsof the right-sided approach maintain that it is moreconvenient for a right-handed surgeon.
For anterior cervical spine surgery we prefer the use ofa regular operating table with the occiput placed on awell-padded circular foam pillow with a center cutout.Gardner-Wells tongs are used to maintain alignment andapply traction intraoperatively. Exposure of the fracturesite is carried out through a left-sided surgical approach.
CERVICAL SPINE—POSTERIOR APPROACH
After general anesthesia has been induced, the patient isturned in the prone position on a regular operative tablewith longitudinal chest rolls to allow decompression of theabdominal and chest cavities. Turning of the patient canalso be facilitated with the Stryker frame. The principalsurgeon must maintain control of the head and neck of thepatient during all turns. The head can be placed in aMayfield horseshoe head cushion. Positioning must avoidcircumferential pressure around the eye, which couldresult in retinal artery thrombosis or globe injuries. TheMayfield headrest attaches to the outer layer of the skulland rigidly fixes the head and the neck in the proneposition without any pressure on the face or the eyes. Thisframe can be adjusted to exert longitudinal traction andflexion or extension as needed through the universal jointsand finally fix the entire head and neck rigidly beforesurgery.
Alternatively, the Mayfield skull clamp can be used tosecurely fix the head and neck in the desired position.Furthermore, in situations in which a halo vest is inplace, the halo ring can be secured to the three-pinMayfield skull clamp (Fig. 27–33), as described by Rheaand coauthors.103
FIGURE 27–33. In cases in which a halo ring has previously been applied,the three-pin Mayfield skull clamp can be used to secure the halo ring.
770 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 25/31 P 770 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 25/31 P 770 BLACK T

The operating table should be placed in a slight reverseTrendelenburg position to prevent sliding of the patientand provide the surgeon with comfortable access to theoperative field. The presence of distal pulses must bedocumented. The arms are tucked along the side of thepatient, and care is taken to protect the ulnar nerves at theelbows. The shoulders are retracted distally and secured inthat position with longitudinal tape to facilitate radio-graphic access.
For posterior cervical spine surgery, it is our preferenceto position the patient prone on chest rolls on a regularoperating table, using a Mayfield skull clamp to secure thepatient’s head and neck.
THORACOLUMBAR SPINE
Operative positioning for the posterior approach to thethoracolumbar spine can be accomplished with the use ofa regular or radiolucent operating table and well-paddedchest rolls. The rolls are positioned transversely at the levelof the sternum and the iliac crests. Most thoracolumbarspine fractures have some degree of kyphosis, and theposition of the rolls will allow the thoracolumbar junctionto sag, thereby both decompressing the abdomen andallowing for postural reduction (Fig. 27–34). The armsshould not be overly extended nor abducted past 90° toprevent brachial plexus injuries. The elbows are padded toprotect the ulnar nerves, and the arms are rested onwell-padded arm boards. The knees are flexed with caretaken to avoid pressure on the patellas and feet, and thepresence of distal pulses must be documented. Alterna-tively, the Stryker frame can be used for the posteriorapproach and will facilitate rotational positioning of thepatient. We prefer the use of a four-poster frame on aregular operating table for patient positioning in theposterior approach to the thoracolumbar spine. This framewill allow postural reduction of the spine and will alsofacilitate access for intraoperative radiographs.
Anterior thoracolumbar spinal surgery is recommendedfor patients who require direct decompression of the duralsac. This technique is accomplished by making a leftanterolateral incision with the patient in the right decubi-tus position on a regular operating table, although in someinstances a right-sided approach may be used. The patientis positioned so that the fracture is located at the flexionbreak of the table. It is critical that the patient be in thetrue lateral position, especially if instrumentation is to beused. Hip supports are used to maintain the relativeposition of the patient on the operating table. The arm onthe side of the operative approach is placed on a Mayostand, and the other is allowed to rest on an arm board.
Padding is applied, particularly over the bony promi-nences. The hips and knees are slightly flexed with apillow placed between the knees to prevent pressureinjury. An axillary roll is placed under the axilla on thedown side, approximately 6 inches from its apex toprevent injury to the brachial plexus. When a thoracotomyis planned, intubation should be done with a double-lumen tube so that the lung on the side of the approachcan be selectively deflated.
Intraoperative Monitoring
Prevention of neurologic deterioration is one of the majorobjectives of spinal surgery after trauma. Intraoperativemonitoring, though not beneficial in patients with com-plete spinal cord injuries, may be helpful in a neuro-logically intact or incomplete patient.125 Spinal monitor-ing techniques, traditionally used in spinal deformitysurgery, are also becoming popular for treatment of spinefractures.11, 12 The most commonly used intraoperativespinal monitoring measures are SEPs and the Stagnarawake-up test.
STAGNARA WAKE-UP TEST
The concept of waking the patient during the surgery todetermine the integrity of the spinal cord was introducedin 1973 by Vauzelle and colleagues.125 The wake-up test,named after one of its originators, is a simple, cost-effective, and very reliable test for assessing gross motorfunction when administered appropriately. The patient,after having been informed preoperatively about thedetails of the test, is awakened intraoperatively and askedto perform specific voluntary movements to demonstrategross motor function. If the patient demonstrates sym-metric motor function on command, the test is negative,the patient is reanesthetized, and the surgical procedureresumes. If the test is positive, a motor deficit has beendetected, immediate corrective measures (i.e., removal ofspinal instrumentation, more extensive decompression)must be undertaken, and the examination is then repeated.The results are usually very reliable, provided that thepatient is adequately awakened and able to cooperate. TheStagnara wake-up test has two major weaknesses: it is atest of gross motor function that provides no informationregarding specific nerve root integrity, and it does notevaluate sensory function. Medical considerations includehypertension, which could potentially precipitate a car-diac insult in patients with preexisting cardiovasculardisease, and the greater risk of air embolism from in-creased intrathoracic pressure—hence the recommenda-tion to flood the operative field with irrigation fluid beforethe test. Thus far, however, no reports have evaluated theefficacy of the wake-up test for spinal trauma surgery.
SOMATOSENSORY EVOKED POTENTIALS
SEPs are widely used for spinal monitoring during sur-gery.38, 94, 95, 120 They are elicited by stimulating a mixedperipheral nerve, preferably the tibial or peroneal nerve inthe lower extremities and the median and ulnar nerves in
FIGURE 27–34. Kyphotic deformity occurs in most thoracolumbar spinefractures. Sagging the spine between two rolls both decompresses theabdomen and permits postural reduction.
771CHAPTER 27 • Management Techniques for Spinal Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 26/31 P 771 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 26/31 P 771 BLACK T

the upper extremities, to record responses from levelscaudal and cephalad to the level of the surgery. The data arerecorded and the amplitude and latency are compared withbaseline values. Monitoring of the tibial and peronealnerves predominantly reflects the function of the L5 and S1roots, respectively. Robinson and colleagues demonstratedthe efficacy of femoral SEPs for monitoring the midlumbarroots during surgical treatment of thoracolumbar fractures,particularly those involving the T12–L4 levels.107 Interest-ingly, SEPs are used to monitor the motor function of thespinal cord. Such monitoring is based on the close proxim-ity of the sensory tracts to the motor tracts and theassumption that trauma to the motor tracts will affect thesensory responses. This reasoning is generally valid whenthe mechanism of injury is trauma, but it is not always thecase when a vascular insult has occurred.61 A decrease inamplitude of greater than 50% or prolongation of latencyby 10% in comparison to baseline values (or both) issignificant.32, 98 Muscle relaxation, core temperature, andmean arterial pressure of 60 mm Hg and higher seem tohave no significant effect on SEPs. In contrast, anestheticagents have a dose-related effect.115
SEPs are typically elicited by stimulating a peripheralmixed nerve and recording a response at sites caudal andcephalad to the level of the surgery. Delays in conductionor depression of the spinal response may indicate corddamage or a physiologic block of function. On the otherhand, absence of conduction is associated with severe andusually irreversible cord damage.33, 53, 75 The mean SEPwas shown to have the strongest individual relationship tothe outcome of improvement in the Motor Index Score at6 months.75 In contrast to this study, Katz and associatesreviewed 57 patients who were studied with SEPs anddermatomal evoked potentials and monitored for morethan 1 year.63 The study examined the ability of these teststo predict motor recovery after acute spinal cord injury.Evoked potentials added little or no useful prognosticinformation to the initial physical examination in patientswith either complete or incomplete spinal cord injury. Thebeneficial role of SEP monitoring in spine injury surgery islimited and yet to be determined.
Postoperative Care
Patients whose spine injuries are treated surgically alsorequire special postoperative management. In the immedi-ate postsurgical period, vital functions are meticulouslymonitored. Observation of upper airway function is es-pecially important after anterior cervical spine surgery.Airway obstruction can be due to local edema, woundhematoma, postoperative dryness, or gland hypersecretion.The patient’s neurologic function should clearly be moni-tored in the immediate postoperative period, and monitor-ing should include both motor and sensory examinations.Progressive deterioration of the patient’s neurologic statusis suggestive of an epidural hematoma and is an indicationfor immediate decompressive surgery.
The postoperative use of orthotic devices, despite inter-nal spine fixation, further restricts excessive spine mo-tion, allows for soft tissue healing, and decreases postoper-ative pain. Spinal bracing also has a psychologic effect in
assisting the patient’s postoperative pain tolerance. Further-more, postoperative bracing results in a lower incidence ofhardware failure, surgical loss of correction, and pseudar-throsis. Indications for postoperative bracing depend onthe severity of injury, the degree of spinal instability, thepresence of neurologic deficit, the type and quality ofinternal fixation, bone quality, and the patient’s individualprofile. The specific characteristics and indications forspinal braces have been presented earlier in this chapter.
Rigid internal fixation of the cervical spine usuallyobviates the need for a halo vest. A halo vest is stillrecommended when instability persists after internal fixa-tion or when the risk of loosening after operative reductionis high. Cervical braces, such as high- or low-thoracicCTOs, usually provide sufficient additional postsurgicalexternal stabilization. The duration of bracing can varyfrom 2 to 6 weeks and has to be individualized to thespecific patient.
A total-contact thoracolumbar orthosis (TLO) is recom-mended for the postoperative management of thoracolum-bar injury. The TLO should be applied during theimmediate postoperative period. A TLSO is used forfractures extending between T8 and L4. A hip spica TLSOcan be used for injuries to the lumbosacral junction,whereas a sternal pad can be fitted for injuries above T8 tocounteract kyphotic forces.
After uneventful spine surgery, patients are routinelydischarged from the hospital on the second or thirdpostoperative day. Return to sedentary occupational activ-ity can be expected within 2 weeks, and full functionalrecovery can range from 6 weeks to 3 months, dependingon the specific injury. Postoperative follow-up visits areusually scheduled at 7 to 10 days, 6 weeks, and 3 months.At the completion of spine healing, dynamic stress radio-graphic should be taken to document recovery of the spineinjury.
Postoperative management of a neurologically impairedspinal injury patient requires special attention. Bedriddenpatients must be frequently turned to avoid skin break-down over pressure areas. Custom-molded braces areprovided as soon as possible to facilitate early mobilization.Occasionally, orthoses are fitted on the upper and lowerextremities to prevent contractures and maintain jointflexibility. Physical therapy is a crucial component of theoverall care and must be instituted as soon as possible.Depending on the level of spinal injury, patients mustbecome proficient with transfers, self-catheterization, andmaintenance of a bowel routine. Emotional and psycho-logic support should be readily available to both the patientand family. Unfortunately, these injuries usually involveyoung adults and are an enormous individual tragedy; theyalso incur considerable socioeconomic cost and require ashort- and long-term multidisciplinary approach.
Complications
Complications of surgical treatment of spinal trauma havebeen reported frequently. Most complications are the resultof failure to understand the patient’s altered spinal mechan-ics, poor surgical technique, or poor choice of instrumen-tation. Failure to achieve and maintain adequate reduction
772 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 27/31 P 772 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 27/31 P 772 BLACK T

can be related to the severity of the fracture, the quality ofthe patient’s bone, and technical difficulties with thesurgery.
McAfee and co-workers reviewed the complications of40 patients with thoracolumbar fractures treated withHarrington distraction rods.85 Twenty-six of the 30 patientswho were monitored for more than 2 years requiredadditional spine surgery. Deep wound infection occurred in15% of patients and wound dehiscence in 7%; five patientsexperienced neurologic deterioration. In approximately30% of patients, dislodgement or disengagement of theinstrumentation occurred along with loss of fixation. Lossof fixation was more likely in translational injuries becauseHarrington distraction instrumentation relies on intactligamentous structures for stability. The use of a claw-typeconfiguration of hooks placed segmentally cephalad andcaudal to the lamina appears to decrease this complication.
The development of pedicle screws for spinal segmentalinstrumentation has provided more rigid and reliableposterior fixation; however, complications have accompa-nied the use of pedicle screws. Lonstein and coauthorsreported their experience with 4790 pedicle screws in-serted in 915 operative procedures.80 Penetration of thecortex of the pedicle occurred in 2.2%, and penetration ofthe anterior cortex of the vertebral body, the most commontype of perforation, occurred in 2.8%. Late-onset discom-fort or pain caused by pseudarthrosis or the instrumenta-tion and requiring removal of the instrumentation occurredwith 23% of the screws. Nerve root irritation was caused by0.2% of the screws, and 0.5% of the screws had broken.
Failure of instrumentation can be attributed to im-proper implant selection or implant construct for a specificspinal injury. The choice of an implant and its mode ofapplication is always determined by the biomechanicalstability of the segment to be instrumented. Poor bonequality or poor fixation technique can result in hardwaredislodgement and cause the construct to fail. Finally, allhardware will eventually fail in the presence of pseudar-throsis, regardless of the design, strength, or the manner inwhich the instrumentation is applied.
Postoperative wound infections are also a commoncomplication after spine surgery. The risk of infectionranges between 1% and 6% and is highly dependent onexpedient surgery, meticulous surgical technique, andthe use of perioperative prophylactic antibiotics. The mostfrequent offending organism, Staphylococcus aureus, is re-sponsible for about 50% of cases. Aggressive treatmentis the mainstay of management of postoperative spinalwound infection. Irrigation and debridement of the woundmust be performed as soon as possible, cultures obtained,and empirical antibiotic administration started until cul-ture results are available. The implants, along with via-ble bone graft, must be retained if they are well toleratedand provide stability to the spine. Repeat debridement isperformed as needed. Wounds can be closed over drains orcan be packed open. Some recommend the use of inflow-outflow systems for deep infections. Most reports concurthat a satisfactory outcome can be achieved after this formof treatment.84, 117, 128, 132
The most devastating complication in spinal traumasurgery is neurologic deterioration. Most situations ofneurologic decompensation result from inadequate decom-
pression of neural structures. When an incomplete deficitpersists, repeat imaging (i.e., myelography, CT, and othertechniques) is indicated to determine whether the patientwould benefit from additional surgery. Postoperative neu-rologic deterioration may be caused by several factors,including direct neural injury from manipulation, instru-mentation, or correction of a deformity during the surgery.Rapid postoperative deterioration when the patient isinitially improved may be the result of an expandingepidural hematoma. The treating physician must be alertfor this potentially catastrophic complication and evacuatethe hematoma emergently to minimize residual long-termneurologic deficit.
Finally, leakage of cerebrospinal fluid may complicatespinal trauma surgery. The leakage can be a result of aniatrogenic laceration or may be caused by the initial injury.When cerebrospinal fluid leakage is recognized intraop-eratively, an attempt should be made to repair the injury.Leakage of cerebrospinal fluid because of a dural tear at theinjury level is a special concern in spinal trauma. Cammisaand colleagues reviewed 30 patients with a laminarfracture in association with a burst fracture of the thoracicor the lumbar spine.23 Eleven of the 30, all withpreoperative neurologic deficits, had evidence of a durallaceration at surgery; 4 of the 11 had neural elementsentrapped in the laminar fracture site. Therefore, a highindex of suspicion is warranted in any patient with aneurologic deficit and a burst fracture in association witha laminar fracture. If leakage of cerebrospinal fluid isrecognized postoperatively, treatment may include reoper-ation and repair of the leak in the lumbar spine orantibiotics, recumbency, and lumbar subarachnoid drainsfor both the cervical and lumbar spine.
REFERENCES
1. Aebi, M.; Etter, C.; Kehl, T.; et al. Stabilization of the lower thoracicspine with the internal spinal skeletal fixation system. Indications,techniques, and first results of treatment. Spine 12:544–551, 1987.
2. Alberts, L.R.; Mahoney, C.R.; Neff, J.R. Comparison of the Nebraskacollar, a new prototype cervical immobilization collar, with threestandard models. J Orthop Trauma 12:425–430, 1998.
3. An, H.S.; Lim, T.H.; You, J.W.; et al. Biomechanical evaluation ofanterior thoracolumbar spinal instrumentation. Spine 15:1979–1983, 1995.
4. Anderson, L.D.; D’Alonzo, R.T. Fractures of the odontoid process ofthe axis. J Bone Joint Surg Am 56:1663–1674, 1974.
5. Anderson, P.A.; Montesano, P.X. Morphology and treatment ofoccipital condyle fractures. Spine 13:731–736, 1988.
6. Anderson, P.A.; Budorick, T.E.; Easton, K.B.; et al. Failure of halovest to prevent in vivo motion in patients with injured cervicalspines. Spine 16(Suppl):501–505, 1991.
7. Anderson, P.A. Nonsurgical treatment of patients with thoracolum-bar fractures. Instr Course Lect 44:57–65, 1995.
8. Axelsson, P.; Johnsson, R.; Stromqvist, B. Lumbar orthosis withunilateral hip immobilization. Spine 18:876–879, 1993.
9. Bedbrook, G.M.; Hon, O.B.E. Treatment of thoracolumbar disloca-tion and fractures with paraplegia. Clin Orthop 112:27–43, 1975.
10. Bedbrook, G.M. Spinal injuries with tetraplegia and paraplegia.J Bone Joint Surg Br 61:267–284, 1979.
11. Ben-David, B.; Taylor, P.D.; Haller, G.S. Posterior spinal fusioncomplicated by posterior column injury: A case report of a falsenegative wake-up test. Spine 12:540–543, 1987.
12. Ben-David, B. Spinal cord monitoring. Orthop Clin North Am19:427–448, 1988.
13. Benzel, E.C. Spinal orthosis. In: Benzel, E.C., ed. Biomechanics ofSpinal Stabilization. New York, McGraw-Hill, 1995, pp. 247–258.
773CHAPTER 27 • Management Techniques for Spinal Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 28/31 P 773 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 28/31 P 773 BLACK T

14. Benzel, E.C.; Hadden, T.A.; Saulsbery, C.M. A comparison of theMinerva and halo jackets for stabilization of the cervical spine.J Neurosurg 70:411–414, 1989.
15. Blockey, N.J.; Purser, D.W. Fractures of the odontoid process of theaxis. J Bone Joint Surg Br 38:794–817, 1956.
16. Bohlman, H.H. Surgical management of cervical spine fractures anddislocations. Instr Course Lect 34:163–187, 1985.
17. Botte, M.J.; Byrne, T.P.; Garfin, S.R. Application of the halo devicefor immobilization of the cervical spine utilizing an increasedtorque pressure. J Bone Joint Surg Am 69:750–752, 1987.
18. Botte, M.J.; Garfin, S.R.; Byrne, T.P.; et al. The halo skeletal fixator:Principles of application and maintenance. Clin Orthop 239:12–18,1989.
19. Botte, M.J.; Byrne, T.P; Abrams, R.A.; Garfin, S.R. Halo skeletalfixation: Techniques of application and prevention of complica-tions. J Am Acad Orthop Surg 4:44–53, 1996.
20. Bravo, P.; Labarta, C.; Alcaraz, M.; et al. Outcome after vertebralfractures with neurological lesion treated either surgically orconservatively in Spain. Paraplegia 31:358–366, 1993.
21. Brazinski, M.; Yoo, J.U. Review of pulmonary complicationsassociated with early versus late stabilization of thoracic and lumbarfractures. Paper presented at the 12th Annual Meeting of theOrthopaedic Trauma Association, Boston, 1996.
22. Brown, C.W.; Chow, G.H. Orthoses for spinal trauma andpostoperative care. In: Goldberg, B.; Hsu, J.D., eds. AAOS Atlas ofOrthoses and Assistive Devices, 3rd ed. St. Louis, Mosby–YearBook, 1997.
23. Cammisa, F.P., Jr.; Eismont, F.J.; Green, B.A. Dural lacerationoccurring with burst fractures and associated laminar fractures.J Bone Joint Surg Am 71:1044–1052, 1989.
24. Campagnolo, D.I.; Esquieres, R.E.; Kopacz, K.J. Effect of stabiliza-tion on length of stay and medical complications following spinalcord injury. J Spinal Cord Med 20:331–334, 1997.
25. Cantor, J.B.; Lebwohl, N.H.; Garvey, T.; et al. Nonoperativemanagement of stable thoracolumbar burst fractures with earlyambulation and bracing. Spine 18:971–976, 1993.
26. Chapman, J.R.; Anderson, P.A. Thoracolumbar spine fractures withneurologic deficit. Orthop Clin North Am 25:595–612, 1994.
27. Cheshire, D.J.E. The stability of the cervical spine following theconservative treatment of fractures and fracture-dislocations. Para-plegia 7:193–203, 1969.
28. Clark, C.R.; White, A.A. Fractures of the dens. J Bone Joint Surg Am67:1340–1348, 1985.
29. Cooper, P.R.; Maravilla, K.R.; Sklar, F.H.; et al. Halo immobilizationof cervical spine fractures. J Neurosurg 50:603–610, 1979.
30. Cotler, H.B.; Miller, L.S.; DeLucia, F.A.; et al. Closed reduction ofcervical spine dislocations. Clin Orthop 214:185–199, 1987.
31. Cotler, H.B.; Cotler, J.M.; Alden, M.E.; et al. The medical andeconomic impact of closed cervical spine dislocations. Spine15:448–452, 1990.
32. Dawson, E.G.; Sherman, J.E.; Kanim, L.E.; Nuwer, M.R. Spinal cordmonitoring. Results of the Scoliosis Research Society and theEuropean Spinal Deformity Society survey. Spine 16(Suppl):361–364, 1991.
33. Delamarter, R.B.; Bohlman, H.H.; Dodge, L.D.; Biro, C. Experi-mental lumbar spinal stenosis. Analysis of the cortical evokedpotentials, microvasculature, and histopathology. J Bone Joint SurgAm 72:110–120, 1990.
34. Denis, F. Spinal instability as defined by the three-column spineconcept in acute spinal trauma. Clin Orthop 189:65–76, 1984.
35. Dunn, H.K. Anterior spine stabilization and decompression forthoracolumbar injuries. Orthop Clin North Am 17:113–119, 1986.
36. Edwards, C.C.; Levine, A.M. Early rodsleeve stabilization of theinjured thoracic and lumbar spine. Orthop Clin North Am 17:121–145, 1986.
37. Eismont, F.J.; Arena, M.J.; Green, B.A. Extrusion of an intervertebraldisc associated with traumatic subluxation or dislocation of cervicalfacets. J Bone Joint Surg Am 73:1555–1560, 1991.
38. Engler, G.L.; Spielholz, N.J.; Bernhard, W.N.; et al. Somatosensoryevoked potentials during Harrington instrumentation for scoliosis.J Bone Joint Surg Am 60:528–532, 1978.
39. Fellrath, R.F.; Hanley, E.N. Multitrauma and thoracolumbar frac-tures. Semin Spine Surg 7:103–108, 1995.
40. Fidler, M.W.; Plasmans, C.M. The effect of four types of support onthe segmental mobility of the lumbosacral spine. J Bone Joint SurgAm 65:943–947, 1983.
41. Finn, C.A.; Stauffer, E.S. Burst fracture of the fifth lumbar vertebra.J Bone Joint Surg Am 74:398–403, 1992.
42. Fisher, S.V.; Bowar, J.F.; Awad, E.A.; et al. Cervical orthoses effect oncervical spine motion: Roentgenographic and goniometric methodof study. Arch Phys Med Rehabil 58:109–115, 1977.
43. Fox, H.J.; Thomas, C.H.; Thompson, A.G. Spinal instrumentationfor Duchenne’s muscular dystrophy: Experience of hypotensiveanaesthesia to minimize blood loss. J Pediatr Orthop 17:750–753,1997.
44. Frankel, H,L,; Hancock, D.O.; Hyslop, G.; et al. The value ofpostural reduction in the initial management of closed injuries ofthe spine with paraplegia and tetraplegia. Paraplegia 7:179–192,1969.
45. Fredrickson, B.E.; Yuan, H.; Miller, H.M. Burst fractures of the fifthlumbar vertebra. J Bone Joint Surg Am 64:1088–1094, 1982.
46. Gardner, V.O.; Thalgott, J.S.; White, J.I.; et al. The contouredanterior spinal plate system (CASP). Indications, techniques, andresults. Spine 19:550–555, 1994.
47. Garfin, S.R.; Botte, M.J.; Centeno, R.S.; et al. Osteology of the skullas it affects halo pin placement. Spine 10:696–698, 1985.
48. Gertzbein, S.D.; Court-Brown, C.M.; Marks, P. The neurologicaloutcome following surgery for spinal fractures. Spine 13:641–644,1988.
49. Gertzbein, S.D. Scoliosis Research Society multicenter spinefracture study. Spine 17:528–540, 1992.
50. Gertzbein, S.D.; Crowe, P.J.; Fazl, M.; et al. Canal clearance in burstfractures using the AO internal fixator. Spine 17:558–560, 1992.
51. Goto, G.; Crosby, G. Anesthesia and the spinal cord. Anesth ClinNorth Am 10:493–519, 1992.
52. Graziano, A.F.; Scheidel, E.A.; Cline, J.R.; Baer, L.J. A radiographiccomparison of prehospital cervical immobilization methods. AnnEmerg Med 16:1127–1131, 1987.
53. Grundy, B.L.; Friedman, W. Electrophysiological evaluation of thepatient with acute spinal cord injury. Crit Care Clin 3:519–548,1997.
54. Hu, S.S.; Capen, D.A.; Rimoldi, R.L.; et al. The effect of surgicaldecompression on neurologic outcome after lumbar fracture. ClinOrthop 288:166–173, 1993.
55. Hughes, S.J. How effective is the Newport/Aspen collar? Aprospective radiographic evaluation in healthy adult volunteers.J Trauma 45:374–378, 1998.
56. James, K.S.; Wenger, K.H.; Schlegel, J.D.; et al. Biomechanicalevaluation of the stability of thoracolumbar burst fractures. Spine19:1731–1740, 1994.
57. Johnson, K.D.; Cadambi, A.; Seibert, G.B. Incidence of adultrespiratory distress syndrome in patients with multiple musculo-skeletal injuries: Effect of early operative stabilization of fractures.J Trauma 25:375–377, 1985.
58. Johnson, R.M.; Hart, D.L.; Owen, J.R.; et al. The Yale cervicalorthosis: An evaluation of its effectiveness in restricting cervi-cal motion in normal subjects and a comparison with other cervicalorthoses. Phys Ther 58:865–871, 1978.
59. Johnson, R.M.; Hart, D.L.; Simmons, B.F.; et al. Cervical orthoses:A study comparing their effectiveness in restricting cervical motionin normal subjects. J Bone Joint Surg Am 59:332–339, 1977.
60. Johnson, R.M.; Owen, J.R.; Hart, D.L.; et al. Cervical orthoses: Aguide for their selection and use. Clin Orthop 154:34–45, 1981.
61. Kai, Y.; Owen, J.H.; Lenke, L.G., et al. Use of sciatic neurogenicmotor evoked potentials versus spinal potentials to predictearly-onset neurologic deficits when intervention is still possibleduring overdistraction. Spine 18:1134–1139, 1993.
62. Kaneda, K.; Abumi, K.; Fujiya, M. Burst fractures with neurologicdeficit of the thoracolumbar-lumbar spine. Results of anteriordecompression and stabilization with anterior instrumentation.Spine 9:788–795, 1984.
63. Katz, R.T.; Toleikis, R.J.; Knuth, A.E. Somatosensory-evoked anddermatomal-evoked potentials are not clinically useful in theprognostication of acute spinal cord injury. Spine 16:730–735,1991.
64. Kaufman, W.A.; Lunsford, T.R.; Lunsford, B.R.; Lance, L.L. Com-parison of three prefabricated cervical collars. Orthot Prosthet39:21–29, 1986.
65. Koch, R.A.; Nickel, V.L. The halo vest: An evaluation of motion andforces across the neck. Spine 3:103–107, 1978.
66. Kostuik, J.P. Indications for use of the halo immobilizations. ClinOrthop 154:46–56, 1981.
774 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 29/31 P 774 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 29/31 P 774 BLACK T

67. Krompinger, W.J.; Fredrickson, B.E.; Mino, D.E.; et al. Conservativetreatment of fractures of the thoracic and lumbar spine. OrthopClin North Am 17:161–170, 1986.
68. Lantz, S.A.; Schultz, A.B. Lumbar spine orthosis wearing. Spine11:834–842, 1986.
69. Lawhon, S.M.; Kahn, A.; Crawford, A.H.; Brinker, M.S. Controlledhypotensive anesthesia during spinal surgery. A retrospective study.Spine 9:450–453, 1984.
70. Lee, A.S.; MacLean, J.C.B.; Newton, D.A. Rapid traction forreduction of cervical spine dislocations. J Bone Joint Surg Br76:352–356, 1994.
71. Lemons, V.R.; Wagner, F.C.; Montesano, P.X. Management ofthoracolumbar fractures with accompanying neurological injury.Neurosurgery 30:667–671, 1992.
72. Lerman, J.A.; Haynes, R.J.; Koeneman, E.J.; et al. A biomechanicalcomparison of Gardner-Wells tongs and halo device used forcervical spine traction. Spine 19:2403–2406, 1994.
73. Levine, A.M.; Edwards, C.C. The management of traumaticspondylolisthesis of the axis. J Bone Joint Surg Am 67:217–226,1985.
74. Levine, A.; Bosse, M.; Edwards, C.C. Bilateral facet dislocations inthe thoracolumbar spine. Spine 13:630–640, 1988.
75. Li, C.; Houlden, D.A.; Rowed, D.W. Somatosensory evokedpotentials and neurological grades as predictors of outcomes inacute spinal cord injury. J Neurosurg 72:600–609, 1990.
76. Lind, B.; Sihlbom, H.; Nordwall, A. Forces and motions acrossthe neck in patients treated with halo-vest. Spine 13:162–167,1988.
77. Lindop, M.J. Complications and morbidity of controlled hypoten-sion. Br J Anaesth 47:799–803, 1975.
78. Lindsey, R.W.; Dick, W. The Fixateur Interne in the reduction andstabilization of thoracolumbar spine fractures in patients withneurologic deficit. Spine 16(Suppl):140–145, 1991.
79. Lindsey, R.W.; Dick, W.; Nuchuck, S.; et al. Residual intersegmentalspinal mobility following limited pedicle fixation of thoracolumbarspine fractures with the Fixateur Interne. Spine 18:474–478, 1993.
80. Lonstein, J.E.; Denis, F.; Perra, J.H.; et al. Complications associatedwith pedicle screws. J Bone Joint Surg Am 81:1519–1528, 1999.
81. Lunsford, T.R.; Davidson, M.; Lunsford, B.R. The effectiveness offour contemporary cervical orthoses in restricting cervical motion.J Orthot Prosthet 6:93–99, 1994.
82. Mahale, Y.J.; Silver, J.R.; Henderson, N.J. Neurological complica-tions of the reduction of cervical spine dislocations. J Bone JointSurg Br 75:403–409, 1993.
83. Malcolm-Smith, N.A.; McMaster, M.J. The use of induced hypoten-sion to control bleeding during posterior fusion for scoliosis. J BoneJoint Surg Am 65:225–228, 1983.
84. Massie, J.B.; Heller, J.G.; Abitbol, J.J.; et al. Postoperative posteriorspinal wound infections. Clin Orthop 284:99–108, 1992.
85. McAfee, P.C.; Bohlman, H.H.; Yuan, H.A. Anterior decompressionof traumatic thoracolumbar fractures with incomplete neurologicaldeficit using a retroperitoneal approach. J Bone Joint Surg Am67:89–104, 1985.
86. McGuire, R.A.; Degnan, G.; Amundson, G.M. Evaluation of currentextrication orthoses in immobilization of the unstable cervicalspine. Spine 15:1064–1067, 1990.
87. McGuire, R.A.; Green, B.A.; Eismont, F.J.; et al. Comparison ofstability provided to the unstable spine by the kinetic therapy tableand the Stryker frame. Neurosurgery 22:842–845, 1988.
88. McLain, R.F.; Benson, D.R. Urgent surgical stabilization of spinalfractures in polytrauma patients. Spine 24:1646–1654, 1999.
89. Meyer, P.R. Fractures of the thoracic spine. In: Meyer, P.R., ed.Surgery of Spine Trauma. New York, Churchill Livingstone, 1989,pp. 525–624, 717–820.
90. Miller, L.S.; Cotler, H.B.; De Lucia, F.A.; et al. Biomechanicalanalysis of cervical distraction. Spine 12:831–837, 1987.
91. Mirza, S.K.; Krengel, W.F.; Chapman, J.R.; et al. Early versusdelayed surgery for acute cervical spinal cord injury. Clin Orthop359:104–114, 1999.
92. Mumford, J.; Weinstein, J.N.; Spratt, K.F.; et al. Thoracolumbarburst fractures: The clinical efficacy and outcome of nonoperativemanagement. Spine 18:955–970, 1993.
93. Nagel, D.A.; Koogle, T.A.; Piziali, R.L.; et al. Stability of the upperlumbar spine following progressive disruptions and the applicationof individual internal and external fixation devices. J Bone JointSurg Am 63:62–70, 1981.
94. Nash, C.L.; Lorig, R.A.; Schatzinger, L.A.; et al. Spinal cordmonitoring during operative treatment of the spine. Clin Orthop126:100–105, 1977.
95. Nash, C.L.; Brown, R.H. Spinal cord monitoring. J Bone Joint SurgAm 71:627–630, 1989.
96. Nickel, V.L.; Perry, J.; Garret, A.; Heppenstall, M. The halo. J BoneJoint Surg Am 50:1400–1409, 1968.
97. Nicoll, E.A. Fractures of the dorso-lumbar spine. J Bone Joint SurgBr 31:376–393, 1949.
98. Nuwer, M.R.; Dawson, E.G.; Carlson, L.G.; et al. Somatosensoryevoked potential spinal cord monitoring reduces neurologic deficitsafter scoliosis surgery: Results of a large multicenter survey.Electroencephalogr Clin Neurophysiol 96:6–11, 1995.
99. Patwardhan, A.G.; Li, S.P.; Gavin, T.; et al. Orthotic stabilization ofthoracolumbar injuries: A biomechanical analysis of the Jewetthyperextension orthosis. Spine 15:654–661, 1990.
100. Perry, J.; Nickel, V.L. Total cervical-spine fusion for neck paralysis.J Bone Joint Surg Am 41:37–60, 1959.
101. Plaisier, B.; Gabram, S.G.; Schwartz, R.J.; Jacobs, L.M. Prospec-tive evaluation of craniofacial pressure in four different cervicalorthoses. J Trauma 37:714–720, 1994.
102. Reid, D.C.; Hu, R.; Davis, L.A.; et al. The nonoperative treatment ofburst fractures of the thoracolumbar junction. J Trauma 28:1188–1194, 1988.
103. Rhea, A.H.; Tranmer, B.I.; Gross, C.E. Intraoperative cervical spinestabilization using the halo ring and the Mayfield three-pin skullclamp. J Neurosurg 64:157–158, 1986.
104. Rimoldi, R.; Zigler, J.; Capen, D.; Hu, S. The effect of surgi-cal intervention on rehabilitation time in patients with thoraco-lumbar and lumbar spinal cord injuries. Spine 17:1443–1449,1992.
105. Rizzolo, S.J.; Vaccaro, A.R.; Cotler, J.M. Cervical spine trauma.Spine 19:2288–2298, 1994.
106. Robertson, P.A.; Ryan, M.D. Neurological deterioration afterreduction of cervical subluxation: Mechanical compression by disctissue. J Bone Joint Surg Br 74:224–227, 1992.
107. Robinson, L.R.; Slimp, J.C.; Anderson, P.A.; Stolov, W.C. Theefficacy of femoral nerve intraoperative somatosensory evokedpotentials during surgical treatment of thoracolumbar fractures.Spine 18:1793–1797, 1993.
108. Rorabeck, C.H.; Rock, M.G.; Hawkins, R.J.; et al. Unilateral facetdislocation of the cervical spine. An analysis of the results oftreatment in 26 patients. Spine 12:23–27, 1987.
109. Rosen, P.B.; McSwain, N.E.; Arata, M.; et al. Comparison oftwo new immobilization collars. Ann Emerg Med 21:1189–1195,1992.
110. Rushton, S.A.; Vaccaro, A.R.; Levine, M.J.; et al. Bivector traction forunstable cervical spine fractures: A description of its applicationand preliminary results. J Spinal Disord 10:436–440, 1997.
111. Sears, W.; Fazl, M. Prediction of stability of cervical spine fracturemanaged in the halo vest and indications for surgical intervention.J Neurosurg 72:426–432, 1990.
112. Schiegel, J.; Bayley, J.; Yuan, H.; et al. Timing of surgicaldecompression and fixation of acute spinal fractures. J OrthopTrauma 10:323–330, 1996.
113. Sharpe, K.P.; Rao, S.; Ziogas, A. Evaluation of the effectiveness of theMinerva cervicothoracic orthosis. Spine 20:1475–1479, 1995.
114. Slabaugh, P.B.; Nickel, V.L. Complications with use of the Strykerframe. J Bone Joint Surg Am 60:2222–2223, 1978.
115. Sloan, T.B. Anesthesia during spinal surgery with electrophysiolog-ical monitoring. Semin Spine Surg 9:302–308, 1997.
116. Sollevi, A. Hypotensive anesthesia and blood loss. Acta Anaesthe-siol Scand Suppl 89:39–43, 1988.
117. Stambough, J.L.; Beringer, D. Postoperative wound infectionscomplicating adult spine surgery. J Spinal Disord 5:277–285, 1992.
118. Strunin, L. Organ perfusion during controlled hypotension. BrJ Anaesth 47:793–798, 1975.
119. Sypert, G.W. External spinal orthotics. Neurosurgery 20:642–649,1987.
120. Tamaki, T.; Nogushi, T.; Takano, H.; et al. Spinal cord monitoringas a clinical utilization of the spinal evoked potential. Clin Orthop184:58–64, 1984.
121. Traynelis, V.C.; Marano, G.D.; Dunker, R.O.; et al. Traumaticatlantooccipital dislocation. J Neurosurg 65:863–870, 1986.
122. Triggs, K.J.; Ballock, R.T.; Lee, T.Q.; et al. The effect of angledinsertion on halo pin fixation. Spine 14:781–783, 1989.
775CHAPTER 27 • Management Techniques for Spinal Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 30/31 P 775 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 30/31 P 775 BLACK T

123. Ullrich, P.F.; Keene, J.S.; Hogan, K.J.; et al. Results of hypotensiveanesthesia in operative treatment of thoracolumbar fractures.J Spinal Disord 3:329–333, 1990.
124. Vaccaro, A.R.; Daugherty, R.J.; Sheehan, T.P.; et al. Neurologicoutcome of early versus late surgery for cervical spinal cord injury.Spine 22:2609–2613, 1997.
125. Vauzelle, C.; Stagnara, P.; Jouvinroux, P. Functional monitoring ofspinal cord activity during spinal surgery. Clin Orthop 93:173–178,1973.
126. Waters, R.L.; Adkins, R.H.; Nelson, R.; Garland, D. Cervical spinalcord trauma: Evaluation and nonoperative treatment with halo-vestimmobilization. Contemp Orthop 14:35–45, 1987.
127. Weinstein, J.N.; Collalto, P.; Lehmann, T.R. Thoracolumbar ‘‘burst’’fractures treated conservatively: A long-term follow-up. Spine13:33–38, 1988.
128. Weinstein, M.A.; McCabe, J.P.; Cammisa, F.P. Postoperative spinalwound infection: A review of 22,391 consecutive index procedures.J Spinal Disord 12:422–426, 2000.
129. White, A.A.; Southwick, W.O.; Panjabi, M.M. Clinical instability ofthe lower cervical spine. Spine 1:85–96, 1976.
130. White, A.A.; Panjabi, M.M. Clinical Biomechanics of the Spine.Philadephia, J.B. Lippincott, 1978, pp. 236–251.
131. Willen, J.; Lindahl, S.; Irstam, L.; Nordwall, A. Unstable thora-columbar fractures: A study by CT and conventional roentgenol-ogy of the reduction effect of Harrington instrumentation. Spine9:215–219, 1984.
132. Wimmer, C.; Gluch, H. Management of postoperative woundinfection in posterior spinal fusion with instrumentation. J SpinalDisord 9:505–508, 1996.
776 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 31/31 P 776 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h27 10/9/02 26 P 31/31 P 776 BLACK T