Embed Size (px)
Citation preview
277
Hypertensive disorders of pregnancy are one of the most seri-ous complications in pregnancy because they cause serious maternal and perinatal morbidity and mortality. Although numerous hypertensive patients have relatively good out-come, difficulty in differentiating among various hyperten-sive conditions, inability to predict which patients are at highest risk, and variability in the progression of preeclamp-sia make these disorders the greatest challenge of clinical medicine in obstetrics.
CLASSIFICATIONVarious systems have been used to classify hypertensive dis-orders of pregnancy. Some terms, such as pregnancy-induced hypertension, have misleading connotations about the under-lying mechanism. Misleading terms refl ect the lack of clear understanding about the etiology and lack of a gold standard diagnostic test. The current classification was developed by the National Institutes of Health working group on hyper-tension in pregnancy. 49 This classification proposes that hypertensive disorders of pregnancy be divided into four categories: preeclampsia-eclampsia, gestational hyperten-sion, chronic hypertension, and preeclampsia superimposed on chronic hypertension.
Preeclampsia-EclampsiaPreeclampsia is new-onset hypertension with proteinuria with or without edema. Edema alone with hypertension is unreliable for diagnosis of preeclampsia because signifi cant edema occurs in normal pregnancy, and it is difficult to dis-tinguish physiologic change from pathologic edema. Edema that occurs in nondependent sites, rapidly increasing edema (as evidenced by rapid weight gain of at least 2.25 kg or 5 lb per week), or persisting facial edema after the patient has been upright for several hours should be suspected as patho-logic edema. Hypertension is defined as blood pressure
greater than 140/90 mm Hg or mean arterial pressure greater than 105 mm Hg. Proteinuria is defined as protein excretion of 30 mg/dL in a random specimen (equal to 1� on urine strips) or 300 mg in a 24-hour urine specimen. Eclampsia is the development of convulsions or coma or both in the clinical set-ting of preeclampsia.
Gestational HypertensionGestational hypertension is hypertension occurring after the 20th week of pregnancy or during the first 24 hours postpartum without evidence of proteinuria or other signs of preeclampsia and in the absence of evidence of preexist-ing hypertension.
Chronic HypertensionChronic hypertension is hypertension diagnosed before preg-nancy or before the 20th week of pregnancy. Hypertension is defined as blood pressure greater than 140/90 mm Hg. This definition may overlook isolated systolic or diastolic hyper-tension. Some investigators have suggested use of mean arte-rial pressure greater than 105 mm Hg as the alternative diag-nostic criterion. Mean arterial pressure is calculated as diastolic pressure plus one-third pulse pressure (pulse pres-sure is systolic pressure minus diastolic pressure). Hyperten-sion diagnosed any time during pregnancy but persisting beyond the 42nd postpartum day is also classified as chronic hypertension.
Superimposed PreeclampsiaSuperimposed preeclampsia is either aggravation of hyper-tension or onset or increase in degree of proteinuria in a patient with a chronic hypertensive disorder. Aggravation of hypertension is an increase in systolic pressure by 30 mm Hg or diastolic pressure by 15 mm Hg.
CHAPTER
Hypertensive Disorders of Pregnancy
Dinesh M. Shah
15

278 SECTION III PREGNANCY DISORDERS AND THEIR IMPACT ON THE FETUS
Comment on ClassificationIncreases of 30 mm Hg in systolic blood pressure and of 15 mm Hg in diastolic blood pressure have been shown to be unreliable criteria for diagnosis of preeclampsia. Most patients with an increase of this magnitude do not have a hypertensive disorder. 94 One of the difficulties of diagnosing hypertension before the 20th week of gestation is that a patient’s blood pressure is generally lower in the first half of pregnancy compared with the nonpregnant state. The lower-ing of blood pressure is a result of the vasorelaxant effect of gestation, which masks hypertension in some patients before the 20th week of pregnancy. Patients with chronic hyperten-sion have been shown to have a greater decline in their blood pressure than normal patients. 77 Diagnosis of chronic hyper-tension as persisting after the 42nd postpartum day is useful only for classifying patients retrospectively (e.g., for grouping patients in a study), but is not useful for clinicians in manag-ing the index pregnancy.
PREECLAMPSIA-ECLAMPSIA PathophysiologyUteroplacental ischemia is a fundamental abnormality recog-nized in preeclampsia-eclampsia. 53 The diagnosis of uteropla-cental ischemia is based on histopathologic examination of the placenta, revealing ischemic lesions 4 ; study of the uterine vascular bed, revealing vascular lesions known as acute ath-erosis 101 ; restriction of fetal growth secondary to reduced uteroplacental blood fl ow 38 ; and radionuclide studies of utero-placental perfusion, showing reduced clearance of radionu-clide. 44 Understanding the pathogenic mechanism requires understanding uterine vascular modeling in implantation and development of the placenta and understanding the mecha-nisms of regulation of blood fl ow in the maternal uteroplacen-tal vasculature.
UTERINE VASCULAR MODELINGTerminal uterine vessels are known as spiral arteries. In the process of gestational development, under the infl uence of sex steroids, these vessels grow in length and to some degree in diameter. 26 Trophoblastic invasion of these vessels occurs in the process of implantation and development of the pla-centa. Trophoblastic invasion results in complete replace-ment of endothelium by a layer of trophoblastic cells. The medial coat of the vessel, which consists of smooth muscle cells and connective tissue, is completely replaced by the invading trophoblasts. 57 At the end of this remodeling, the spiral artery is made of a thin adventitial layer internally lined by trophoblasts; it is considerably dilated in diameter and is known as the uteroplacental vessel. 11
It has been suggested that trophoblastic invasion occurs in two phases. The first phase extends from the time of implanta-tion until the 10th to 12th week of gestation 57 ; invasive growth progresses to two-thirds depth in the decidua. The second phase extends from the 12th week to the 16th to 18th week of gestation. The vessels are remodeled up to the terminal resistance portion of the vessel into the myometrial layer; this results in a marked decrease in the resistance to the
blood fl ow into the uteroplacental vessels and into the intervil-lous space. As placentation progresses, trophoblastic invasion incorporates greater numbers of vessels, until an average of 100 decidual arteries are tapped for intervillous circulation. 11
In patients who eventually develop preeclampsia, the invasion depth in the second-phase trophoblastic invasion might be deficient. 56 The insufficient depth allows greater numbers of decidual spiral arteries to retain the resistance portion of the vessel, which prevents adequate dilation of these vessels. More important, the contractile portion of these vessels remains intact, which has profound implica-tions for the effect of vasomotor regulators of circulation.
VASOMOTOR REGULATION OF UTEROPLACENTAL CIRCULATION
Regulation of Uterine Blood FlowIt is now well recognized that many organs have mechanisms for regional regulation of blood fl ow. The uterus is similar to the kidney in its embryologic origin, anatomic vascular arrange-ment, and mechanisms for regulation of blood fl ow. Similar to the kidney, uteroplacental circulation produces various vasodi-lators and vasoconstrictors, including eicosanoids, 92 endothe-lin, 33 nitric oxide, 42 renin, 45 , 73 , 89 and angiotensinogen. 46 , 73
Various aberrations occur in these vasomotor regulators in preeclampsia. Prostaglandin production has been shown to be decreased in preeclampsia; however, such deficiency accounts for only a small degree of change in blood pressure (3 to 5 mm Hg). 21 Thromboxane is considered a counter-regulatory vasoconstrictor eicosanoid to prostacyclin, and its production has been shown to be increased. 20 Viewing these two facts together, the balance of eicosanoids could be dis-turbed in preeclampsia. 21 , 97 Some investigators have sug-gested that endothelin levels may be increased in preeclamp-sia. 91 Others have shown that it is not. 72
In experimental gravid animal models, pharmacologic interventions to decrease nitric oxide production are associ-ated with development of systemic hypertension. 103 Nitric oxide production by measurements of urinary metabolite has been shown not to be deficient in human preeclampsia, however. 16
Role of the Renin-Angiotensin SystemThe renin-angiotensin system might be involved in the patho-genesis of preeclampsia. 87 The role of angiotensin II in regulat-ing uterine blood fl ow directly or through alterations of eicosanoids has been suggested in experimental settings. Uter-ine venous angiotensin II levels are higher in hypertensive human pregnancy. 59 More important, systemic vasculature becomes more responsive to angiotensin II in preeclampsia. 23
In view of evidence for uteroplacental ischemia and evi-dence for local renin and angiotensinogen production in the uterus, it is reasonable to assume that uterine vasculature is also modified to become more sensitive to angiotensin II in human preeclampsia. This vascular maladaptation, i.e., in-creased responsiveness to angiotensin II and development of hypertension, was first described by Goldblatt similar patho-physiology has been shown in renin gene overexpression models with development of hypertension. 47 This research on renin gene overexpression models with hypertension

Chapter 15 Hypertensive Disorders of Pregnancy 279
emphasizes the role of renin in the evolution of vascular maladaptation.
The change in the vasculature in renin-mediated hyper-tension is primarily driven by functional changes in the vas-culature. Such functional changes in vasculature in renin-mediated hypertension are biochemically mediated by alterations in the cyclooxygenase pathway of arachidonic acid metabolism and increased thromboxane production, 100
protein kinase C-mediated mechanism and its effect on cal-cium handling by the vascular smooth muscle, 50 alterations in the Na � -K � pump and cotransport, 51 and change in endo-thelin expression and release. 7 Initial change in vasculature in renin-mediated vasoconstriction seems to be mediated through increased sympathoadrenal activity. Many of these alterations have been described in human preeclampsia, 20 , 21 including increased sympathoadrenal activity. 70
Takimoto and colleagues 90 reported the development of preeclampsia-eclampsia syndrome by crossbreeding trans-genic mice, with the introduction of human renin ( Ren ) and human angiotensinogen ( AGT ) genes into the mouse genome. Specifically, when male mice carrying human Ren were mated with female mice carrying human AGT, preeclampsia syn-drome developed, and renin overexpression was shown on the fetal side of the placenta. One important aspect of the mouse model of preeclampsia is that fetal renin from the placenta seemed to transfer to the maternal circulation much more readily than is reported in humans. 36
In human preeclampsia, renin gene expression is increased in the decidua vera on the maternal side. 75 Increased renin production from the uterus has been shown to occur in response to decreased blood fl ow to the uterus in experimen-tal settings. 102 Collectively, these data suggest a role of increased renin production in the uteroplacental interphase in the pathogenic mechanism of preeclampsia.
Increased heterodimerization of angiotensin AT 1 and bra-dykinin B 2 receptors has been described in preeclampsia. 1a
These investigators have suggested the concept that AT 1 -B 2
heterodimerization mediates at least part of the increased responsiveness to angiotensin II in preeclampsia by using the B 2 intracellular domain for the signal transduction. 1a Suscep-tibility of AT 1 homodimers to inactivation by peroxide treat-ment suggests that oxidative stress of normal pregnancy may confer some of the angiotensin II refractoriness. 1a The mech-anism by which the AT 1 -B 2 heterodimerization is induced is not yet defined.
Patients with preeclampsia develop autoantibodies against the second loop of the AT 1 receptor (AT 1 -AA), 96 which might be another mechanism involved in AT 1 receptor and adreno-receptor signaling. How an antibody against the AT 1 receptor could cause signal transduction to occur through the � 1 ad-renoreceptor remains unexplained. These antibodies enhance the tissue factor expression in vitro with increased immunore-activity for tissue factor in preeclamptic placentas. 10 These data on AT 1 -AA correlate with the findings of anti-ssDNA and anti-dsDNA autoantibodies in preeclampsia, 104 suggesting an abnor-mal or unrestrained B cell activation in preeclampsia or perhaps aberrantly increased antigen presentation, or both.
Angiotensinogen mutation with increased angiotensin II production and susceptibility to development of preeclamp-sia has been shown in some populations, but not in others. 98
Because other biochemical aberrations that mediate vascular maladaptation are renin mediated, renin from uteroplacental interphase might have a role in initiating the pathogenesis of preeclampsia ( Fig. 15-1 ).
In addition to development of systemic hypertension, alterations in regional organ circulation occur in sites that are normally renin-angiotensin dependent. This reduction in local blood fl ow could explain the spectrum of clinical mani-festations of preeclampsia.
Vasomotor Implications of Vascular ModelingThe intactness of the resistance portion of the uteroplacental vessels with preserved ability for vasoconstriction should have profound implications for uteroplacental ischemia. These vessels should also become increasingly responsive to angio-tensin II that is produced locally. The local renin-angiotensin system could initiate vasoconstriction-mediated ischemia and cellular injury in the uteroplacental vascular bed.
PATHOPHYSIOLOGIC BASIS OF CLINICAL MANIFESTATIONSThe renin-angiotensin system is involved in physiologic regu-lation of blood fl ow in various organs, including the heart and systemic vasculature and the uterus, kidney, liver, and brain ( Table 15-1 ). These are also the sites for major clinical mani-festations of preeclampsia-eclampsia, which emphasizes the role of the renin-angiotensin system in the pathogenesis of this disorder. Clinical manifestations are described here according to the systemic or regional circulations involved. The primary mechanism at all sites is increased responsive-ness to angiotensin II, leading to increased vascular resistance initially and vasoconstriction later with attendant hypoxemia and cell damage. When vasoconstriction and hypoxemia occur, endothelial dysfunction sets in, and free radical forma-tion and lipid peroxidation may accelerate the process fur-ther. 68 Endothelial dysfunction can occur earlier in individu-als susceptible to such endothelial damage (e.g., thrombophilic conditions). 34 Other studies suggest that such individuals might not be at an increased risk. 52
Angiotensinogen
Angiotensinogenmutation
Renin
↑ Renin
↑ Angiotensin II
Sympathoadrenalactivity
Eicosanoidimbalance
Endothelinrelease
EndotheliumCyclooxygenasepathway
Arachidonic acid
Figure 15–1. Renin-angiotensin system in pathogenesis of preeclampsia.

280 SECTION III PREGNANCY DISORDERS AND THEIR IMPACT ON THE FETUS
Cardiovascular ManifestationsIncreased sympathoadrenal activity may mediate increases in cardiac output. Increase in cardiac work demanded by increased cardiac output is generally well tolerated by young patients, but it may occasionally precipitate left ventricular failure. Decreased renal perfusion, high hydrostatic pressure owing to the cardiovascular changes, and decrease in oncotic pressure owing to proteinuria compounded by fl uid over-load may result in development of pulmonary edema.
Systemic vasculature is most frequently and fairly consis-tently involved with vasoconstriction, the primary manifesta-tion being development of hypertension. Usually, systolic and diastolic blood pressures are elevated, and hypertension is pro-portional to renal manifestations, especially proteinuria, at least in uncomplicated cases. Hypertension to some degree depends on increased sympathoadrenal activity, which explains the fl uc-tuations in blood pressure and accelerations related to anxiety.
High cardiac output in the face of markedly increased peripheral vascular resistance may result in traumatic intra-vascular hemolysis. This condition can cause a decreased haptoglobin level, increased free hemoglobin level, increased bilirubin levels, burr cells and schistocytes in the peripheral blood, and an increased free serum iron level.
Uterine VasculatureInitially, high cardiac output and increased vascular resis-tance without change in vessel diameter may result in increased uteroplacental perfusion. Later, with a marked increase in local vasoconstriction, regional blood fl ow would decrease.
Uteroplacental ischemia and placental infarcts are well-recognized pathologic findings of preeclampsia-eclampsia syndrome. 53 Decreased uteroplacental blood fl ow explains increased frequency of somatic growth deficiency in this condition 38 (see also Chapter 14 ). Severe reductions in uteroplacental blood fl ow can cause fetal hypoxemia, which is clinically manifested as fetal distress, hypoxemic multiorgan failure, or death. Uteroplacental interface hypoxemia can also result in cellular injury to the decidua and injury to the vascular wall itself, with resultant small hemorrhages.
Two processes—hypoxemic cell injury and hemorrhage—sometimes cause small disruptions of placental attachment, which cause further disruption of the vascular wall as a result of the mechanics of physical separation. Disruption of the vascular wall causes bleeding in the uteroplacental inter-face; this may explain development of abruptio placentae.
TABLE 15–1 Findings and Clinical Manifestations of Preeclampsia
Vasculature or System Findings Clinical Manifestations
Cardiovascular Increased cardiac output and systemic vasoconstriction
Increased hydrostatic pressure High cardiac output and hypertension
Systemic hypertension
Generalized edema Intravascular hemolysis
Uteroplacental Uteroplacental insuffi ciency
Decidual ischemia Decidual thrombosis
Fetal somatic growth defi ciency; fetal hypoxemia and distress
Abruptio placentae; placental infarcts Thrombocytopenia
Renal Decreased renal blood fl ow and glomerular fi ltration rate; endothelial damage
High AII responsiveness of tubular vasculature All of the above
Proteinuria; elevated creatinine and decreased creatinine clearance; oliguria
Elevated uric acid Renal tubular necrosis and renal
failure
Cerebrovascular Cerebral motor ischemia
High cerebral perfusion pressure with regional ischemia
Cerebral edema Regional ischemia
Generalized grand mal seizures (eclampsia)
Cerebral hemorrhage
Coma Central blindness; loss of speech
Hepatic Ischemia; hepatic cellular injury Mitochondrial injury
Elevated liver enzymes Intracellular fatty deposit
Hematologic Intravascular hemolysis
Decidual thrombosis, release of FDP
Schistocyte burr cells; elevated free hemoglobin and iron; decreased haptoglobin levels
Thrombocytopenia; antiplatelet antibodies
AII, angiotensin II; FDP, fi brin degradation products.

Chapter 15 Hypertensive Disorders of Pregnancy 281
Uteroplacental interface vessels normally have fibrin deposi-tion, a process that can be aggravated by vasoconstriction, and further decreases in the blood fl ow in these vessels. These reductions in blood fl ow explain the decidual throm-bosis and initiation of thrombocytopenia with local platelet consumption. 64 Dissemination of small fibrin degradation products from these vessels and release of tissue thrombo-plastin from decidual and trophoblast cell injury can cause disseminated intravascular coagulopathy. 60
Renal VasculatureDecreased renal blood fl ow and high renal perfusion pres-sure and associated hypoxemia can cause glomerular injury, which causes proteinuria. Glomerular injury may be associ-ated with fibrin deposits in the basal layer and swelling of endothelial cells, resulting in glomerular endotheliosis seen in renal histology. 19 A severe decrease in renal blood fl ow can cause oliguria, and severe vasoconstriction and hypoxemia with cellular injury might explain renal tubular necrosis seen occasionally in preeclampsia.
Excess circulating placental soluble fms-like tyrosine kinase 1 (sFlt-1), an antagonist of vascular endothelial growth factor (VEGF) and placental growth factor, has been shown in preeclampsia. By reducing the circulating levels of VEGF and placental growth factor, sFlt-1 may contribute to the endothe-lial dysfunction and impaired renal vasorelaxation. 32 , 43 This sFlt-1 is a splice variant of VEGF receptor-1 (VEGFR-1); it is produced by the placenta and has been known to enter the maternal circulation. Administration of sFlt-1 to pregnant rats induced hypertension, proteinuria, and glomerular endothelio-sis. 43 Recent experimental evidence showing attenuation of hypertension and decrease in renal injury by infusion of recom-binant VEGF 121 in a rat model further validates the role of sFLT-1 in the pathogenesis of preeclampsia. 37a Similarly, soluble endoglin, a novel placenta-derived soluble transforming growth factor-� coreceptor, seems to contribute to the pathophysiology by dysregulating signaling in the vasculature. 93
Decreased renal tubular blood fl ow (this vasculature is sensitive to angiotensin II) results in proximal tubular ex-change of urate in favor of plasma, which explains frequent association of elevated serum uric acid as a manifestation of preeclampsia. Elevated uric acid more accurately refl ects an-giotensin II responsiveness, 18 explaining the ability of elevated uric acid to predict fetal death better than systemic hyperten-sion does. 66 Decreased glomerular filtration rate, combined with proteinuria-induced decrease in oncotic pressure and high hydrostatic pressure secondary to increased cardiac out-put, increased vascular resistance, and sodium and obligatory water retention (aldosterone effect), causes increased depen-dent and even generalized edema of preeclampsia.
Rare cases of diabetes insipidus of renal origin occur. Mea-surements of arginine vasopressin levels are generally normal, and placental aminopeptidase is responsible for rapid degra-dation of arginine vasopressin, resulting in functional deficit.
Hepatic Vascular ChangesAngiotensin II responsiveness of hepatic vasculature is well recognized; it has been used for selective chemotherapy for tumors by angiotensin II infusion-induced vasoconstriction of normal vasculature to protect normal liver tissue. In later phases of disease, hepatic vasoconstriction-mediated hypox-
emia and cellular injury are expected to result in release of he-patic enzymes into the circulation, with elevation of liver en-zymes in blood. 31 Hepatic vasculature in the subcapsular region seems particularly susceptible to injury, resulting in small hem-orrhages. In combination with disseminated intravascular co-agulopathy, these hemorrhages can become larger and cause major subcapsular hematomas of the liver. Tissue injury with edema of liver parenchyma and capsule and with stretching of the capsule could explain the hepatic origin of epigastric pain.
HELLP syndrome 99 is a combination of intravascular hemolysis, elevated liver enzymes, and thrombocytopenia or low platelets. Acute fatty liver of pregnancy (AFLP) 30 , 45 is a condition with a predominantly hepatic manifestation; it is frequently associated with thrombocytopenia and frequently occurs without cardiovascular manifestations of preeclamp-sia. Cellular hypoxemic injury explains mitochondrial dam-age, disruption of fatty acid metabolism, and deposition of microvesicular fat in hepatic cells. Susceptible women (women with a carrier state of deficiency of enzymes of fatty acid metabolism and short-chain and long-chain fatty acid dehydrogenase) might develop AFLP. 28 In most cases, AFLP occurs independent of preeclampsia. There seems to be some overlap in the pathophysiology of AFLP and preeclampsia with AFLP; hepatic manifestations predominate in individu-als with such susceptibility. Mitochondrial enzyme defects may occur as gene defects or be acquired through cell injury mediated by free radicals.
Central Nervous SystemHigh cardiac output and increased vascular resistance may be associated with greater regional circulation in the brain at higher perfusion pressure. 2 Some regions of the brain, espe-cially in advanced stages of the disease, might have locally decreased perfusion.
Vasoconstriction and hypoxemia in the microvasculature of the brain result in cellular injury. The injury causes extra-cellular release of intracellular sodium, which provides the means for generating aberrant electric impulses. The motor cortex seems to be particularly susceptible to such cellular injury, with resultant convulsions and eclampsia. 61 Vasocon-striction of different regions of the brain produces different manifestations: Vasoconstriction in the frontal cortex causes frontal headache, constriction in the occipital cortex causes visual disturbances and central blindness, and constriction in the Broca area causes loss of speech. Blindness may also develop as a result of retinal detachment. Most patients who develop blindness recover completely without medical inter-vention. In cases of cerebral edema, coma and loss of recent memory of specific convulsive episodes occur.
Cerebrovascular accidents occur as a result of cerebral vasospasm, hypoxemia-induced vascular damage, and systolic hypertension that causes mechanical rupture or disruption of the vessel wall. Current data in developed countries suggest that almost 70% of hypertension-related maternal mortality is due to cerebrovascular accidents. 63 Data on stroke and severe preeclampsia and eclampsia suggest a paradigm shift to focus on reduction in systolic blood pressure. 41
Hyperrefl exia has been recognized as a sign of neurologic irritability in epilepsy and is seen before eclamptic seizures, but many women have normally active deep tendon refl exes without neurologic irritability.

282 SECTION III PREGNANCY DISORDERS AND THEIR IMPACT ON THE FETUS
Clinical Considerations PREDISPOSING FACTORSSeveral factors are associated with, or suggested to be associ-ated with, an increased risk of preeclampsia-eclampsia, as follows:
Parity : Eclampsia and preeclampsia are recognized to occur more frequently in the first pregnancy. 6
Age : Relationship to age is described as a J-shaped curve with slightly increased incidence in young primigravidae and a more pronounced increased incidence in older primi-gravidae. 6
Race : Incidence of hypertension is not increased in African Americans, in contrast to a commonly held belief, although a higher incidence of proteinuria is observed. 80
Family : In a study of women with eclampsia, their daughters had an incidence of preeclampsia of 26%, their sisters had an incidence of 37%, and their daughters-in-law had an incidence of 8%.
Genetics : Genetic predisposition has been suspected on the basis of increased familial incidence, suggesting a reces-sive trait possibly of maternal origin.
Diet : Most studies suggest that protein, carbohydrate, or total calorie intake does not infl uence the incidence of pre-eclampsia.
Social status : Several reports suggest that populations with lower socioeconomic status have a higher incidence of preeclampsia and severe preeclampsia.
Twin pregnancies : Twinning is associated with a higher inci-dence of preeclampsia compared with singleton gestation. Severe preeclampsia occurs more frequently in monozy-gotic twinning, especially in multiparous women.
Diabetes : The incidence of preeclampsia is generally thought to be increased in diabetic pregnancies. 12
Hydatidiform mole : The higher incidence and early onset of preeclampsia are well recognized in molar gestation 54 ; these features are also observed in triploidy gestations, which usually have partial mole. 84
Hydrops fetalis : The incidence of preeclampsia seems to be increased only in nonimmune hydrops fetalis. 71
Polyhydramnios : Increased incidence of preeclampsia observed in association with polyhydramnios is related to causes of polyhydramnios, including multiple gestation, diabetes, and hydrops fetalis. 71
Climate and season : Despite considerable interest and analy-sis, climatic and seasonal factors do not seem to contrib-ute to the incidence of preeclampsia.
Cigarette smoking : The incidence of preeclampsia is lower in smokers compared with nonsmokers. 85 If preeclampsia does occur, however, fetal risks are greater in smokers compared with nonsmokers.
Although susceptibility to preeclampsia might be increased by maternal thrombophilic mutations, most of the data have been inconclusive and contradictory. A more recent case-control study suggests, however, that prevalence of factor V and factor II mutations is increased in patients with preeclampsia without a previous thromboembolic disorder. 3 Researchers have suggested that the thrombophilic mechanism might inter-act with other pathogenic factors to determine clinical features of the disease. 3
DIFFERENTIAL DIAGNOSISOne of the most fundamental issues faced by clinicians is dif-ferentiation of a preexisting hypertensive disorder from the development of preeclampsia. Preeclampsia is a progressive disorder of increasing severity, which demands intervention in the form of delivery to halt the progression of the condi-tion. This contrasts with preexisting hypertensive disorders, which exhibit stable manifestations, allowing clinicians to prolong gestation.
This difference in clinical course of action has profound implications for prevention of interventional prematurity. Because preeclampsia is progressive, observation of the patient may reveal progression of the disorder. This approach is fraught, however, with the risk of the patient’s developing serious complications of preeclampsia. Such an approach is valid when the severity of suspected preeclampsia is judged to be mild or moderate, and gestational age is preterm enough to justify postponement of delivery. This philosophy should maximize perinatal outcome within the bounds of maternal safety. 76
Preexisting essential hypertension should be suspected in the absence of proteinuria and other laboratory findings, especially if there is a family history of hypertension, and in the presence of maternal obesity. Corroborative informa-tion on mild elevations in blood pressure before pregnancy may be obtained by careful inquiry into all previous health care encounters by the patient, including visits for contra-ceptive advice.
Preexisting chronic hypertension secondary to renal dis-ease can be readily diagnosed in patients with type I diabetes mellitus or known systemic lupus erythematosus. In other patients, preexisting renal disease should be suspected when proteinuria is in marked disproportion to the degree of hyper-tension, especially in multiparous patients 44 and whenever a patient presents with clinical manifestations of preeclampsia at preterm gestation. This suspicion is supported by renal biopsy data showing that 43% of multiparous women present-ing with preeclampsia had evidence of preexisting renal parenchymal or vascular disease. 19 It is supported further by follow-up data on patients presenting with preeclampsia before 34 weeks’ gestation, of whom almost 70% had labora-tory or renal biopsy evidence of preexisting renal disease. 29
Because most patients with chronic hypertension have essential hypertension, new-onset proteinuria in patients with essential hypertension makes it easier to diagnose superimposed preeclampsia. This diagnosis requires, how-ever, that an estimation of proteinuria be obtained earlier in pregnancy by quantitative laboratory analysis (e.g., from a 24-hour urine collection). In the presence of preexisting proteinuria in chronic hypertensive disorders of renal cause, a physiologic increase in proteinuria early in the third tri-mester is difficult to distinguish from pathologic proteinuria caused by superimposed preeclampsia. Under these circum-stances, development of other laboratory abnormalities (e.g., thrombocytopenia) may assist the diagnosis. Generally, proteinuria in the severe range—5 g in 24 hours or greater—should be regarded as superimposed preeclampsia in patients with preexisting proteinuria.
Convulsions or coma not related to a hypertensive disorder can develop from neurologic causes; hypertension, proteinuria,
Chapter 15 Hypertensive Disorders of Pregnancy 283
or edema provides corroborating background. In a few patients, the disease process may progress so rapidly that con-vulsions might occur without proteinuria or before protein-uria develops.
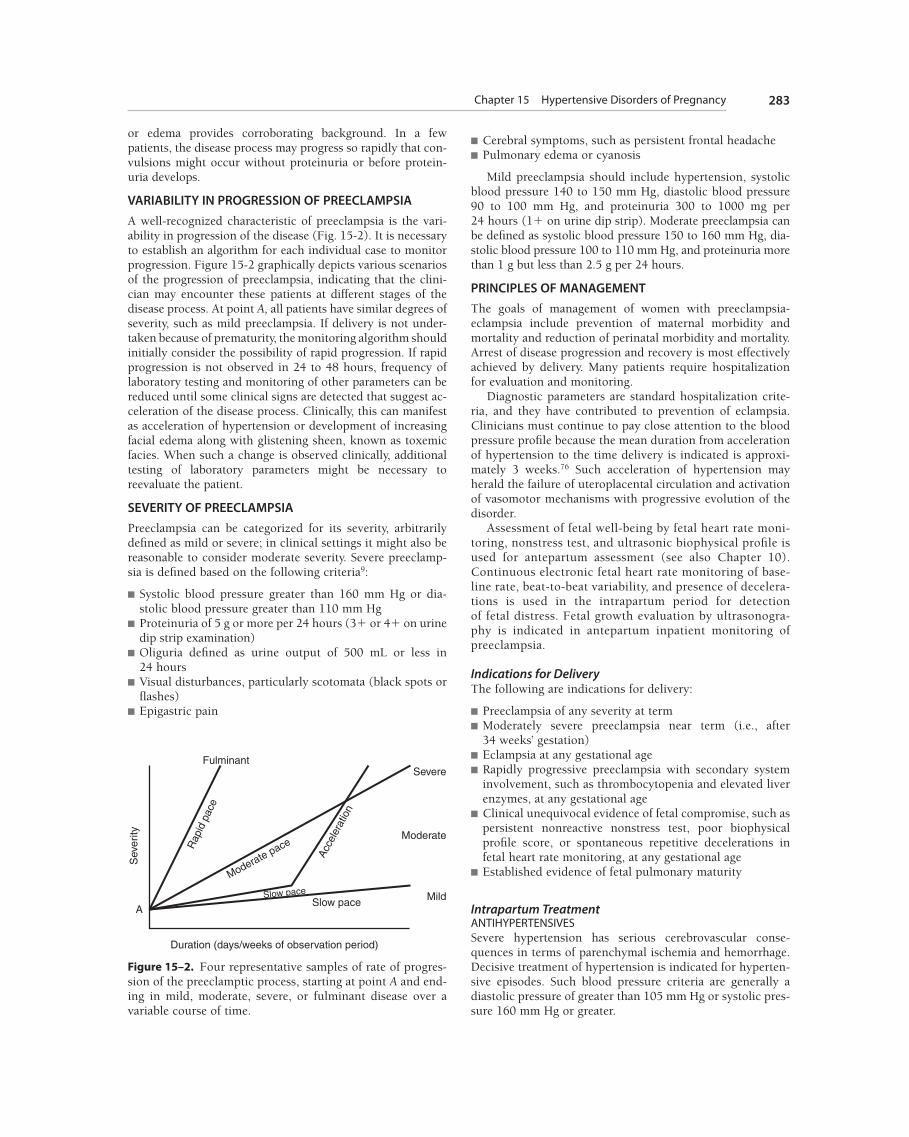
VARIABILITY IN PROGRESSION OF PREECLAMPSIAA well-recognized characteristic of preeclampsia is the vari-ability in progression of the disease ( Fig. 15-2 ). It is necessary to establish an algorithm for each individual case to monitor progression. Figure 15-2 graphically depicts various scenarios of the progression of preeclampsia, indicating that the clini-cian may encounter these patients at different stages of the disease process. At point A, all patients have similar degrees of severity, such as mild preeclampsia. If delivery is not under-taken because of prematurity, the monitoring algorithm should initially consider the possibility of rapid progression. If rapid progression is not observed in 24 to 48 hours, frequency of laboratory testing and monitoring of other parameters can be reduced until some clinical signs are detected that suggest ac-celeration of the disease process. Clinically, this can manifest as acceleration of hypertension or development of increasing facial edema along with glistening sheen, known as toxemic facies. When such a change is observed clinically, additional testing of laboratory parameters might be necessary to reevaluate the patient.
SEVERITY OF PREECLAMPSIAPreeclampsia can be categorized for its severity, arbitrarily defined as mild or severe; in clinical settings it might also be reasonable to consider moderate severity. Severe preeclamp-sia is defined based on the following criteria 9 :
■ Systolic blood pressure greater than 160 mm Hg or dia-stolic blood pressure greater than 110 mm Hg
■ Proteinuria of 5 g or more per 24 hours (3� or 4� on urine dip strip examination)
■ Oliguria defined as urine output of 500 mL or less in 24 hours
■ Visual disturbances, particularly scotomata (black spots or fl ashes)
■ Epigastric pain
■ Cerebral symptoms, such as persistent frontal headache■ Pulmonary edema or cyanosis
Mild preeclampsia should include hypertension, systolic blood pressure 140 to 150 mm Hg, diastolic blood pressure 90 to 100 mm Hg, and proteinuria 300 to 1000 mg per 24 hours (1� on urine dip strip). Moderate preeclampsia can be defined as systolic blood pressure 150 to 160 mm Hg, dia-stolic blood pressure 100 to 110 mm Hg, and proteinuria more than 1 g but less than 2.5 g per 24 hours.
PRINCIPLES OF MANAGEMENTThe goals of management of women with preeclampsia-eclampsia include prevention of maternal morbidity and mortality and reduction of perinatal morbidity and mortality. Arrest of disease progression and recovery is most effectively achieved by delivery. Many patients require hospitalization for evaluation and monitoring.
Diagnostic parameters are standard hospitalization crite-ria, and they have contributed to prevention of eclampsia. Clinicians must continue to pay close attention to the blood pressure profile because the mean duration from acceleration of hypertension to the time delivery is indicated is approxi-mately 3 weeks. 76 Such acceleration of hypertension may herald the failure of uteroplacental circulation and activation of vasomotor mechanisms with progressive evolution of the disorder.
Assessment of fetal well-being by fetal heart rate moni-toring, nonstress test, and ultrasonic biophysical profile is used for antepartum assessment (see also Chapter 10 ). Continuous electronic fetal heart rate monitoring of base-line rate, beat-to-beat variability, and presence of decelera-tions is used in the intrapartum period for detection of fetal distress. Fetal growth evaluation by ultrasonogra-phy is indicated in antepartum inpatient monitoring of preeclampsia.
Indications for DeliveryThe following are indications for delivery:
■ Preeclampsia of any severity at term■ Moderately severe preeclampsia near term (i.e., after
34 weeks’ gestation)■ Eclampsia at any gestational age■ Rapidly progressive preeclampsia with secondary system
involvement, such as thrombocytopenia and elevated liver enzymes, at any gestational age
■ Clinical unequivocal evidence of fetal compromise, such as persistent nonreactive nonstress test, poor biophysical profile score, or spontaneous repetitive decelerations in fetal heart rate monitoring, at any gestational age
■ Established evidence of fetal pulmonary maturity
Intrapartum Treatment ANTIHYPERTENSIVESSevere hypertension has serious cerebrovascular conse-quences in terms of parenchymal ischemia and hemorrhage. Decisive treatment of hypertension is indicated for hyperten-sive episodes. Such blood pressure criteria are generally a diastolic pressure of greater than 105 mm Hg or systolic pres-sure 160 mm Hg or greater.
FulminantSevere
Moderate
Mild
Duration (days/weeks of observation period)
Sev
erity
Slow paceA
Rap
id p
ace
Moderate pace
Acc
eler
atio
n
Slow pace
Figure 15–2. Four representative samples of rate of progres-sion of the preeclamptic process, starting at point A and end-ing in mild, moderate, severe, or fulminant disease over a variable course of time.

284 SECTION III PREGNANCY DISORDERS AND THEIR IMPACT ON THE FETUS
Sublingual nifedipine and an intravenous bolus of hydralazine are the primary antihypertensives used. The results of meta-analysis of randomized, controlled trials are not robust enough to guide clinical practice, but they do not support use of hydralazine as first-line treatment of severe hypertension in pregnancy; labetalol and nifedipine show most promise, but clinical trials are needed. 39 There is no evidence of inadvertent precipitation of angina and myocar-dial infarction with use of sublingual nifedipine in this gener-ally healthy young population. Caution is indicated, how-ever, with use of nifedipine for older mothers (40 years old and older) when there is a family history of coronary artery disease at a young age and especially in women who are heavy smokers. Labetalol and clonidine have also been used for the same purpose ( Table 15-2 ).
CORTICOSTEROIDSEvidence supports use of glucocorticoids safely in patients with preeclampsia for accelerating fetal pulmonary maturation. 67
Method of DeliveryCesarean section is best reserved for specific obstetric clinical indications. Availability of cervical ripening agents contain-ing prostaglandins makes the success of vaginal delivery more feasible. Vaginal delivery after induction of labor is the mainstay method for patients with preeclampsia and most cases of eclampsia because induction of labor in patients with preeclampsia may be easier than predicted by cervical findings. 105
Seizure Prophylaxis and Treatment of EclampsiaMagnesium sulfate infusion for prevention of seizures is rou-tinely recommended by most authorities in the United States. This recommendation is made partly because the signs and symptoms of preeclampsia are unreliable predictors of eclampsia, 83 and partly because magnesium sulfate infusion is remarkably safe prophylaxis. 61 Several other agents have been
used for seizure prophylaxis, including phenytoin. An inter-national randomized trial now supports use of magnesium sulfate, however, as the agent of choice over phenytoin for such prophylaxis. 14
Magnesium sulfate is well recognized as the treatment for preventing further seizures in patients presenting with eclampsia. 61 Magnesium sulfate can be used safely even in patients taking nifedipine (a calcium channel blocker) because there is no evidence of adverse consequences, and there is no sound theoretical basis for avoiding such a com-bination.
The most commonly used regimen of magnesium sulfate is intravenous infusion 106 given as a 2- to 4-g bolus over 5 to 30 minutes followed by continuous infusion starting at 1 g/h and increasing to 2 g/h to maintain therapeutic levels of 4 to 6 mEq/L. Intramuscular injection of magne-sium sulfate has fallen out of favor because of pain associ-ated with the injections and lack of precision in maintain-ing therapeutic levels. Close supervision of the patient’s deep tendon refl exes and urine output measurements is important.
Serum magnesium concentrations in the neonate are very similar to the concentrations in the mother. 61 Stone and Pritchard 86 reported that Apgar scores do not correlate with magnesium levels. Clinical observations by neonatologists suggest higher frequency of neonatal hypotonia and decreased intestinal motility in infants exposed to magnesium sulfate (see also Chapter 49 , Part 2 ).
PREVENTION OF PREECLAMPSIAUntil all aspects of the pathogenic mechanisms are well defined, prevention of preeclampsia remains an unrealized goal. Studies of aspirin and calcium supplementation have not supported their use in either low-risk or high-risk popula-tions. 37 , 79 Selective use of aspirin in conditions where suppres-sion of platelet activation may be benefi cial includes antiphos-pholipid antibody syndrome.
TABLE 15–2 Pharmacotherapy for Maternal Hypertensive Emergencies
Drug Initial Dose Repeat Doses Comments and Precautions
Hydralazine (bolus) 5 mg IV bolus; response time 10-15 min
5-10 mg every 20-30 min If no response with total dose of 20 mg, consider alternatives
Hydralazine (infusion) 40 mg in 500 mL D5/LR; begin at 15-25 mL/h
Begin at 1 mL/min, titrate against blood pressure
Nifedipine 10 mg sublingual, response time 10 min with maximum eff ect at 30 min
10 mg in 30 min If no response after 20 mg, consider alternatives; avoid in elderly patients or inpatients with family history of coronary disease, especially if smokers
Clonidine 0.1 mg PO 0.1 mg in 30 min, then 0.1 mg every h
Patient must be placed on equiv-alent maintenance dose tid
Labetalol 20 mg IV bolus, response time 5-10 min
20 mg dose or begin in-fusion of 1-2 mg/min
Check cardiac functional suppression
D5/LR, 5% dextrose in lactated Ringer’s solution.

Chapter 15 Hypertensive Disorders of Pregnancy 285
OUTCOME IN PREECLAMPSIA-ECLAMPSIA
Perinatal OutcomePerinatal mortality is increased in women with preeclampsia-eclampsia. 48 , 78 , 83 The fetal death rate has decreased more recently, 17 but perinatal morbidity secondary to clinically indicated interventional prematurity continues to be a major problem. 76 Major causes of perinatal morbidity and mortality are uteroplacental insufficiency, abruptio placen-tae, 48 and interventional prematurity. 76 Fetal death rate cor-relates with clinical parameters that refl ect the disease pro-cess. The fetal death rate has been shown to increase with increases in hypertension and degree of proteinuria 22 and with high uric acid levels. 66
Perinatal morbidity is primarily a result of the need for delivery. Although prematurity remains the most important threat to the infants of hypertensive mothers, analysis sug-gests that these infants might have better outcomes than preterm infants delivered spontaneously. 74 A study of neuro-developmental outcome suggests that maternal hypertension seems to protect against cerebral palsy in preterm infants without increasing the risk of cognitive impairment indepen-dent of use of magnesium sulfate. 24 More recent improve-ments in perinatal mortality seem to be due to reduction in fetal, but predominantly in neonatal, death rates.
Maternal Mortality and MorbidityMaternal mortality is still a major risk from hypertensive disorders. 35 Marked improvements in maternal morbidity and mortality have occurred. These improvements are attrib-utable to improvements in medical care (e.g., blood transfu-sion, prevention of aspiration), improvements in methods of stabilization (e.g., reduced use of sedation) of eclamptic and severe preeclamptic patients, and expedited delivery af-ter stabilization. Maternal mortality rates close to zero have been achieved. 83 In areas of the world where good medical care is readily available, cerebrovascular accidents remain the most common reason for maternal mortality, accounting for 60% to 70% of all deaths caused by hypertensive disor-ders. 63 Future decrease in maternal mortality and morbidity rates in hypertensive disorders in developed parts of the world will come from assertive and decisive treatment of severe hypertension.
Remote PrognosisLong-term follow-up studies of eclampsia by Chesley and coworkers 5 revealed that in women with hypertension in the first pregnancy, 33% had a hypertensive disorder in any subse-quent pregnancy, and 5% had a recurrence of eclampsia. Mul-tiparous women with eclampsia had recurrence of hypertension in 50% of subsequent pregnancies. 5 Sibai and associates 81 reported a 45% recurrence of preeclampsia in women with severe preeclampsia, and they showed that risk of such recur-rence is higher in women who develop preeclampsia in the late second or early third trimester. 82 Renal biopsy data from the University of Chicago suggest that approximately 22% of primi-gravidae with preeclampsia have an underlying renal disorder. 19 Collectively, these data suggest that 22% to 45% of primigravid women who develop preeclampsia, severe preeclampsia, or eclampsia have essential hypertension or renal parenchymal disease, or both, as the primary cause.
It has been suggested that there is an increased risk for developing hypertension later in life in women who develop preeclampsia in their first pregnancy. This misconception is due to erroneously including chronic hypertensive disorders in the preeclamptic patients being studied. Long-term follow-up studies of preeclampsia-eclampsia in the first pregnancy by Chesley and coworkers 5 suggest there was no increase in the rate of hypertension. Multiparous women do exhibit excess rates of hypertension and cardiovascular mortality, however, which is best explained by underlying hypertensive disorders.
OTHER HYPERTENSIVE DISORDERS Gestational HypertensionGestational hypertension typically occurs in the third trimes-ter. Recurrence of nonproteinuric hypertension of this type in 15% to 25% of patients with hypertensive disorders suggests an underlying hypertensive disorder, especially if there is a family history of essential hypertension. Under such circum-stances, and in the absence of signs and symptoms of pre-eclampsia, antihypertensive treatment should be consid-ered. 55 Such antihypertensive therapy may reduce the need for hospitalization, and makes outpatient monitoring and management easier. Patients managed as outpatients benefit from ambulatory blood pressure monitoring.
Antihypertensive treatment is similar to that for patients with chronic hypertension. Acceleration of hypertension or need for progressively increasing antihypertensive therapy may indicate development of superimposed preeclampsia or misdiagnosis of the condition as transient hypertension. Careful evaluation of signs and symptoms of preeclampsia before beginning antihypertensive therapy can minimize such difficulties. Patients with severe hypertension without evidence of preeclampsia might have severe hypertension because of cocaine abuse. 95 All patients with severe hyperten-sion manifesting in an episodic manner should have a toxi-cology urine screen test for accurate diagnosis and appropri-ate treatment of hypertension and substance abuse.
Chronic HypertensionChronic hypertension in pregnancy is hypertension (i.e., blood pressure greater than 140/90 mm Hg) diagnosed before the 20th week of gestation or hypertension before pregnancy. Overt hypertension is easily diagnosed, but latent hypertension does not become apparent until later in pregnancy. Latent hypertension is frequently misdiag-nosed as transient hypertension.
CLASSIFICATIONHypertension in pregnancy is classified as primary, second-ary, or chronic ( Box 15-1 ). Primary (essential or idiopathic) hypertension is the most common type observed; secondary hypertension is secondary to a known cause. Causes of sec-ondary hypertension include renal parenchymal disease and renal vascular disease, adrenal diseases, coarctation of the aorta, and thyrotoxicosis. Renal parenchymal disease is the second most common cause of chronic hypertension; other causes are rare.

286 SECTION III PREGNANCY DISORDERS AND THEIR IMPACT ON THE FETUS
EVALUATION OF PREGNANT HYPERTENSIVE PATIENTSEvaluation of a pregnant hypertensive patient includes a complete physical examination, including a funduscopic examination for severe hypertension. 13 Heart size must be evaluated if long-standing or significant hypertension is a factor. Auscultation over the renal arteries should be per-formed to rule out a bruit consistent with renovascular hypertension; however, a bruit is rarely first detected by obstetricians. Simultaneous palpation of the femoral and radial arteries should be performed to rule out coarctation of the aorta; this is rarely first detected by obstetricians.
SCREENING LABORATORY DATAA complete urinalysis for protein and for microscopic sediment should be performed to diagnose renal disease. A 24-hour uri-nalysis for protein and determination of creatinine clearance should be performed to assess renal function. Serum electrolyte levels to rule out primary hyperaldosteronism should be checked only if the diagnosis is not obviously essential hyper-tension or renal disease.
If blood pressure elevation is episodic and reaches systolic pressures of 180 mm Hg and diastolic pressures greater than 110 mm H g, urinary catecholamines should be measured to rule out pheochromocytoma. These patients should also have a toxicology screen. 95
Ultrasonography of the kidneys may be considered when clinically relevant (e.g., chronic pyelonephritis) to assess renal size and pelvic dilation if the patient did not have a diagnostic study before pregnancy. Electrocardiography and an echocar-diogram can be considered depending on the severity of the hypertension.
PRECONCEPTION COUNSELING If possible, counseling should be provided before concep-tion to a woman who has chronic hypertension. This pre-conception counseling is important for establishing ade-quate control of hypertension and making changes in the antihypertensive regimen. It is important to establish base-line data and to teach self-monitoring of blood pressure. If the patient is taking diuretic medication, she should be advised that she should discontinue use of this medication before conception. An appropriate diet that curtails heavy salt use is recommended. Patients taking angiotensin-converting enzyme inhibitors should be advised to discon-tinue them because of serious risks of fetal defects and pregnancy loss.
MANAGEMENT DURING PREGNANCY Bed rest is suggested to increase uterine blood fl ow and promote nutrition to the fetus. 88 Uterine size and compres-sion of the inferior vena cava and aorta are factors that alter blood pressure recordings in the supine position in the third trimester. The currently recommended position for outpatient blood pressure measurement, as advocated by the American Heart Association, is the sitting position. The brachial artery blood pressure is highest when sitting, lower when lying on the back, and lowest when lying on the side.
Home Blood Pressure Monitoring All patients with chronic hypertension benefit from self-monitoring of blood pressure. Self-monitoring reduces use of antihypertensives and need for hospitalization. 62 Self-monitored blood pressure readings tend to be lower, and they also refl ect patients’ blood pressure readings in their environment more accurately. It is advisable to take blood pressure measurements at least three times a day. If the patient works outside the home, blood pressures should be taken during the work week and weekend. This practice identifies the effects of the environment on blood pressure.
Newer digital blood pressure monitors are easy to use and moderately inexpensive. For these reasons, the sphygmoma-nometer and stethoscope for self-monitoring can be abandoned. It is important to check calibration of the patient’s machine in the office.
Other Considerations Therapeutic abortion is generally not necessary or recom-mended, but the decision regarding whether to continue the pregnancy should be determined on an individual basis. It is essential to establish the estimated date of confi nement. History, early pelvic examination, and early ultrasonography aid in this process. Ultrasonography is needed (at 3- to 6-week intervals from 24 to 28, 28 to 32, and 32 to 36 weeks) during pregnancy to detect intrauterine growth restriction, which is most likely to develop after the 30th week of gestation.
BOX 15–1 Classifi cation of Hypertension in Pregnancy
PRIMARY HYPERTENSION Essential or idiopathic hypertension—the most common
type observed
SECONDARY HYPERTENSION Hypertension secondary to a known cause
Renal Disease Parenchymal disease (glomerulonephritis, chronic pyelo-
nephritis, interstitial nephritis, polycystic kidney) Renal vascular disease
Adrenal Disease Cushing syndrome (cortical) Hyperaldosteronism (cortical) Pheochromocytoma (medullary)
Other Coarctation of aorta Thyrotoxicosis
CHRONIC HYPERTENSION Hypertensive disease with superimposed preeclampsia A patient should be considered at risk of chronic hyperten-
sive disease of pregnancy in the presence of one or more of the following
■ Diastolic blood pressure in a nonpregnant state or before the 20th week of gestation consistently �80 mm Hg
■ History of hypertension ■ History of secondary causes of hypertension (e.g., renal
disease) ■ Family history of hypertension ■ Hypertension in a previous pregnancy ■ Hypertension with oral contraceptives

Chapter 15 Hypertensive Disorders of Pregnancy 287
PharmacotherapyThere is a general consensus that severe hypertension should be treated to reduce maternal risks of cerebral vascular com-plications. Meta analysis of several small trials suggests that treatment of mild and moderate hypertension reduces the occurrence of severe hypertension and repeat hospitaliza-tions later in pregnancy. 1
There is no current proof that pharmacotherapy ( Table 15-3 ) alters fetal salvage or prevents preeclampsia, but it does control major accelerations of maternal blood pressure during preg-nancy. This control might reduce the risk of complications of severe hypertension, especially cerebrovascular accidents. Anti-hypertensive medication should be started when home diastolic blood pressure consistently exceeds 84 mm Hg or office blood pressure readings consistently exceed 90 mm Hg.
Pharmacologic agents inhibiting renin-angiotensin system (angiotensin converting enzyme (ACE) inhibitors and angio-tensin II type I receptor inhibitors) are classifi ed by the FDA as class D with the black box warning about their association with fetal growth restriction, fatal neonatal renal failure, and fetal anomalies with exposure during the second trimester. ACE in-hibitors have recently been shown to be associated with major congenital malformations after exposure during the fi rst trimes-ter and are contraindicated anytime during pregnancy. 8a ACE inhibitors are important for diabetic patients with nephropathy and should be prescribed after delivery along with effective contraception. 68a
The current drug of choice is methyldopa (Aldomet). 65
Since the mid-1980s, beta blockers such as propranolol or atenolol have been used. 69 These agents increase the risk of intrauterine growth restriction, however, and might increase fetal morbidity. Alternative drugs include calcium channel blockers, 8 clonidine, and labetalol. 27 , 77 An analysis of clinical trials of beta blockers indicates that the effect of these agents on perinatal outcome is uncertain; the worrying trend toward an increase in infants who are small for gestational age is partly dependent on one small outlying trial. 40 All drugs may cross the placenta; however, except for angiotensin convert-ing enzyme inhibitors, these drugs have not been shown to cause birth defects. 25 , 58
One should avoid using two antihypertensives of the same class whenever a patient needs more than one agent to con-trol hypertension. This situation is most likely to occur for agents acting on the adrenergic system (e.g., combining methyldopa with labetalol should be avoided). It is better to
use a vasodilator, such as nifedipine, as a second agent. Until better evidence is available, the choice of an antihypertensive should depend on the experience and familiarity with a par-ticular drug, and on what is known about adverse maternal and fetal side effects, with the exception of diazoxide and ketanserin, both of which are probably not good choices. 15
Labetalol and long-acting nifedipine are becoming the most commonly used antihypertensive agents in pregnant women. It is hoped that current trials in progress or in process of being launched will provide further clinical evidence-based guidelines.
ComplicationsChronic hypertension is associated with a fourfold to eight-fold increase in the incidence of abruptio placentae. Planned delivery at or near term may be advisable. The patient should be observed for preeclampsia as indicated by an increase in blood pressure and development of proteinuria. The patient should be hospitalized if preeclampsia is suspected.
ANTEPARTUM FETAL EVALUATIONAntepartum fetal evaluation includes serial ultrasound exami-nations to diagnose intrauterine growth restriction. Beginning at 32 weeks of gestation, nonstress tests should be performed twice a week, and fetal movement activity counts should show at least four movements per hour or three movements in 30 minutes, indicating fetal health.
LABOR AND DELIVERYIf a decision is made to proceed to delivery, and the cervix is not favorable for induction of labor, prostaglandin may be administered vaginally. Continuous electronic fetal monitor-ing should be performed during labor. Regional analgesia with epidural administration is ideal, as is also the case for patients with preeclampsia. It is recommended that a pedia-trician be available for evaluation of the newborn.
SUMMARYWomen who have chronic hypertension usually do well dur-ing pregnancy, although 5% to 10% have major catastrophic events. Patients with chronic hypertension may take oral contraceptives postpartum; a barrier form of contraception is an alternative. For women who have completed their childbearing, a permanent form of contraception may be desirable.
TABLE 15–3 Common Antihypertensive Agents for Chronic Hypertension in Pregnancy
Agent Mechanism of Action Dose
Methyldopa Centrally acting alpha agonist 250 mg bid to 500 mg qid
Clonidine Centrally acting alpha agonist 0.1-0.6 mg tid, rarely exceeding 0.4 mg tid
Nifedipine XL Calcium channel blocker 30 mg XL qd to 60 mg XL bid; maximum dose 120 mg/day
Amlodipine besylate (Norvasc) Calcium channel blocker 5-10 mg/day
Labetalol Beta blocker Starting dose 100 mg bid; usual dose 200-400 mg bid; maximum dose 1600-2400 mg
XL, long-acting.

288 SECTION III PREGNANCY DISORDERS AND THEIR IMPACT ON THE FETUS
Superimposed Preeclampsia-EclampsiaSuperimposed preeclampsia-eclampsia is a condition that supervenes on a preexisting hypertensive disorder of any cause. Clinically, this is the most severe form of disease; it is associated with the most severe degree of hypertension and proteinuria. A diagnosis of superimposed preeclampsia gen-erally indicates a need for expedited delivery. Establishment of baseline data on renal and other functions during the pre-natal course is helpful for comparison. Usually, liver function abnormality indicates superimposed preeclampsia; however, association of methyldopa with elevation of liver enzymes without development of superimposed preeclampsia is known to occur. When such a diagnosis is under consider-ation, hospitalization is essential for evaluation, close super-vision, monitoring, and delivery.
15. Duley L, Henderson-Smart DJ : Drugs for treatment of high blood pressure during pregnancy , Cochrane Database Syst Rev ( 4 ): CD001449 , 2002 .
16. Egerman RS et al : Neuropeptide Y and nitrite levels in pre-eclamptic and normotensive gravid women , Am J Obstet Gynecol 181 : 921 , 1999 .
17. Ferranzzani S et al : Proteinuria and outcome of 444 pregnan-cies complicated by hypertension , Am J Obstet Gynecol 162 : 366 , 1990 .
18. Ferris TF, Gorden P : Effect of angiotensin and norepinephrine upon urate clearance in man , Am J Med 44 : 359 , 1968 .
19. Fisher KA et al : Hypertension in pregnancy: clinical-pathological correlations and remote prognosis , Medicine 60 : 267 , 1981 .
20. Fitzgerald DJ et al : Thromboxane A 2 synthesis in pregnancy-induced hypertension , Lancet 335 : 751 , 1990 .
21. Fitzgerald DJ, FitzGerald GA : Eicosanoids in the pathogenesis of preeclampsia . In Laragh JH, Brenner BM, editor: Hyperten-sion: pathophysiology, diagnosis and management ( vol 2 ). New York , Raven Press , 1990 , p 1789 .
22. Friedman EA, Neff RK : Pregnancy outcome as related to hyper-tension, edema and proteinuria . In Lindheimer MD et al, edi-tors: Hypertension in pregnancy . New York , Wiley , 1976 , p 13 .
23. Gant NF et al : A study of angiotensin II pressor response throughout primigravid pregnancy , J Clin Invest 51 : 2682 , 1973 .
24. Gray PH et al : Maternal hypertension and neurodevelopmental outcome in very preterm infants , Arch Dis Child 79 : F88 , 1998 .
25. Hanssens M et al : Fetal and neonatal effects of treatment with angiotensin-converting enzyme inhibitors in pregnancy , Obstet Gynecol 78 : 128 , 1991 .
26. Harris JWS, Ramsey EM : The morphology of human uteropla-cental vasculature , Contrib Embryol 38 : 43 , 1966 .
27. Horvath JS et al : Clonidine hydrochloride: a safe and effective antihypertensive agent in pregnancy , Obstet Gynecol 66 : 634 , 1985 .
28. Ibdah JA et al : A fetal fatty-acid oxidation disorder as a cause of liver disease in pregnant women , N Engl J Med 340 : 1723 , 1999 .
29. Ihle BU et al : Early onset pre-eclampsia: recognition of under-lying renal disease , BMJ 294 : 79 , 1987 .
30. Kaplan MM : Acute fatty liver of pregnancy , N Engl J Med 313 : 367 , 1985 .
31. Killam AP et al : Pregnancy-induced hypertension complicated by acute liver disease and disseminated intravascular coagula-tion: fi ve case reports , Am J Obstet Gynecol 123 : 823 , 1975 .
32. Koga K et al : Elevated serum soluble vascular endothelial growth factor receptor 1 (sVEGFR-1) levels in women with preeclampsia , J Clin Endocrinol Metabol 88 : 2348 , 2003 .
33. Kubota T et al : Synthesis and release of endothelin-1 by human decidual cells , J Clin Endocrinol Metab 75 : 1230 , 1992 .
34. Kupferminic MJ : Increased frequency of genetic thrombophilia in women with complications of pregnancy , N Engl J Med 340 : 9 , 1999 .
35. Lawson HW et al : Maternal mortality related to preeclampsia and eclampsia in the United States 1979-1986 , MMWR Morbid Mortal Wkly Rep CDC Surveill Summ 40 : 1 , 1991 .
36. Lentz T et al : Prorenin secretion from human placenta per-fused in vitro , Am J Physiol 260 : E876 , 1991 .
37. Levine RJ et al : Trial of calcium to prevent preeclampsia , N Engl J Med 337 : 69 , 1997 .
37a. Li Z, Zhang Y, Ying Ma J et al : Recombinant vascular endothe-lial growth factor 121 attenuates hypertension and improves
REFERENCES
1. Abalos E, Duley L, Steyn DW, Henderson-Smart DJ : Antihyper-tensive drug therapy for mild to moderate hypertension during pregnancy , Cochrane Database Syst Rev 24 ;( 1 ): CD002252 , 2007 .
1a. Abdalla S et al : Increased AT 1 receptor heterodimers in pre-eclampsia mediate enhanced angiotensin II responsiveness , Nat Med 7 : 1003 , 2001 .
2. Belfort MA et al : Preeclampsia may cause both overperfusion and underperfusion of the brain: a cerebral perfusion based model , Acta Obstet Gynecol Scand 78 : 586 , 1999 .
3. Benedetto C et al : Factor V Leiden and factor II G20210A in preeclampsia and HELLP syndrome , Acta Obstet Gynecol Scand 81 : 1095 , 2002 .
4. Brosens I, Renaer M : On the pathogenesis of placental infarcts in pre-eclampsia , J Obstet Gynaecol Br 79 : 794 , 1972 .
5. Chesley LC et al : The remote prognosis of eclamptic women , Am J Obstet Gynecol 124 : 446 , 1976 .
6. Christianson RE : Studies on blood pressure during pregnancy , Am J Obstet Gynecol 125 : 509 , 1976 .
7. Chua BH et al : Regulation of endothelin-1 mRNA by angioten-sin II in rat heart endothelial cells , Biochem Biophys Acta 117 : 201 , 1993 .
8. Constantine G et al : Nifedipine as a second line antihyperten-sive drug in pregnancy , Br J Obstet Gynaecol 94 : 1136 , 1987 .
8a. Cooper WO, Hernandez-Diaz S, Arbogast PG et al : Major con-genital malformations after fi rst-trimester exposure to ACE in-hibitors , N Engl J Med 354 ( 23 ): 2443 , 2006
9. Cunningham FG, Lindheimer MD : Hypertension in pregnancy , N Engl J Med 326 : 927 , 1992 .
10. Dechend R et al : AT1 receptor agonistic antibodies from pre-eclamptic patients cause vascular cells to express tissue factor , Circulation 101 : 2382 , 2000 .
11. DeWolf FD et al : Ultrastructure of the spiral arteries in the human placental bed at the end of normal pregnancy , Am J Ob-stet Gynecol 117 : 833 , 1973 .
12. Diamond MP et al : Complication of insulin-dependent diabetic pregnancies by preeclampsia and/or chronic hypertension: analysis of outcome , Am J Perinatol 2 : 263 , 1985 .
13. Dimmitt SB et al : Usefulness of ophthalmoscopy in mild to moderate hypertension , Lancet 20 : 1103 , 1989 .
14. Duley L et al : Which anticonvulsant for women with eclamp-sia? Evidence from the collaborative eclampsia trial , Lancet 345 : 1455 , 1995 .

Chapter 15 Hypertensive Disorders of Pregnancy 289
kidney damage in a rat model of preeclampsia , Hypertension 50 ( 4 ): 686 , 2007 .
38. Lin CC , et al : Fetal outcome in hypertensive disorders of pregnancy , Am J Obstet Gynecol 142 : 255 , 1982 .
39. Magee LA et al : Hydralazine for treatment of severe hyperten-sion in pregnancy: meta-analysis , BMJ 327 : 955 , 2003 .
40. Magee LA, Duley L : Oral beta-blockers for mild to moderate hypertension during pregnancy , Cochrane Database Syst Rev ( 3 ): CD002863 , 2003 .
40a. Magee LA, Miremadi S, Li J et al : Therapy with both magne-sium sulfate and nifedipine does not increase the risk of seri-ous magnesium-related maternal side effects in women with preeclampsia , Am J Obstet Gynecol 193 ( 1 ): 153 , 2005 .
41. Martin JN Jr et al : Stroke and severe preeclampsia and eclampsia: a paradigm shift focusing on systolic blood pres-sure , Obstet Gynecol 205 : 246 , 2005 .
42. Matsumoto M et al : Endothelium-derived relaxation of the pregnant and nonpregnant canine uterine artery , J Reprod Med 37 : 529 , 1992 .
43. Maynard SE et al : Excess placental soluble fms-like tyrosine kinase 1 (sFlt1) may contribute to endothelial dysfunction, hypertension, and proteinuria in preeclampsia , J Clin Invest 111 : 649 , 2003 .
44. McClure Browne JC et al : The maternal placental blood fl ow in normotensive and hypertensive women , J Obstet Gynaecol 60 : 141 , 1953 .
45. Moise KJ, Shah DM : Acute fatty liver of pregnancy: etiology of fetal distress and fetal wastage , Obstet Gynecol 69 : 482 , 1987 .
46. Morgan T et al : Human spiral artery renin-angiotensin system , Hypertension 32 : 683 , 1998 .
47. Mullins JJ et al : Fulminant hypertension in transgenic rats harbouring the mouse Ren-2 gene , Nature 344 : 541 , 1990 .
48. Naeye RL, Friedman EA : Causes of perinatal death associated with gestational hypertension and proteinuria , Am J Obstet Gy-necol 133 : 8 , 1979 .
49. National High Blood Pressure Education Program Working Group : Report on high blood pressure during pregnancy , Am J Obstet Gynecol 163 : 1689 , 1990 .
50. O’Donnell ME : Endothelial cell sodium-potassium-chloride co-transport: evidence of regulation by Ca 2 � and protein kinase C , J Biol Chem 266 : 11559 , 1991 .
51. Orlov SN et al : Na � -K � pump and Na � -K � co-transport in cul-tured vascular smooth muscle cells from spontaneously hypertensive and normotensive rats: baseline activity and regula-tion , J Hypertens 10 : 733 , 1992 .
52. O’Shaughnessy KM et al : Factor V Leiden and thermolabile methylenetetrahydrofolate reductase gene variants in an East Anglian preeclampsia cohort , Hypertension 33 : 1338 , 1999 .
53. Page EW : On the pathogenesis of pre-eclampsia and eclampsia , J Obstet Gynaecol Br Commonw 79 : 883 , 1972 .
54. Page EW : The relation between hydatid moles, relative is-chaemia of the gravid uterus and the placental origin of eclampsia , Am J Obstet Gynecol 37 : 291 , 1939 .
55. Pickles CJ et al : The fetal outcome in a randomized double-blind controlled trial of labetalol versus placebo in pregnancy-induced hypertension , Br J Obstet Gynaecol 96 : 38 , 1989 .
56. Pijnenborg R et al : Placental bed spiral arteries in the hyper-tensive disorders of pregnancy , Br J Obstet Gynaecol 98 : 648 , 1991 .
57. Pijnenborg R et al : Trophoblastic invasion of human decidua from 8 to 18 weeks of pregnancy , Placenta 1 : 3 , 1980 .
58. Piper JM et al : Pregnancy outcome following exposure to angiotensin-converting enzyme inhibitors , Obstet Gynecol 80 : 429 , 1992 .
59. Pipkin FB et al : The uteroplacental renin-angiotensin system in normal and hypertensive pregnancy , Contrib Nephrol 25 : 49 , 1981 .
60. Pritchard JA et al : Coagulation changes in eclampsia: their fre-quency and pathogenesis , Am J Obstet Gynecol 124 : 855 , 1976 .
61. Pritchard JA, Pritchard SA : Standardized treatment of 154 con-secutive cases of eclampsia , Am J Obstet Gynecol 123 : 543 , 1975 .
62. Rayburn WF : Self blood pressure monitoring during preg-nancy , Am J Obstet Gynecol 148 : 159 , 1984 .
63. Redman CWG : The treatment of hypertension in pregnancy , Kidney Int 18 : 267 , 1980 .
64. Redman CWG et al : Early platelet consumption in preeclamp-sia , BMJ 1 : 467 , 1978 .
65. Redman CWG et al : Fetal outcome in trial of antihypertensive treatment in pregnancy , Lancet 2 : 753 , 1976 .
66. Redman CWG et al : Plasma-urate measurements in predicting fetal death in hypertensive pregnancy , Lancet 1 : 1370 , 1976 .
67. Ricke PS et al : Use of corticosteroids in pregnancy-induced hypertension , Obstet Gynecol 48 : 163 , 1976 .
68. Roberts JM et al : Clinical and biochemical evidence of endo-thelial cell dysfunction in pregnancy syndrome preeclampsia , Am J Hypertens 4 : 700 , 1991 .
68a. Robles NR, Romero B, Fernandez-Carbonero E et al : Angiotensin-converting enzyme inhibitors versus angiotensin receptor blockers for diabetic nephropathy: a retrospective comparison , J Renin Angiotensin Aldosterone Syst 10 ( 4 ): 195 , 2009 .
69. Rubin PC et al : Placebo-controlled trial of atenolol in treatment of pregnancy-associated hypertension , Lancet 1 : 431 , 1983 .
70. Schobel HP et al : Preeclampsia: a state of sympathetic overactivity , N Engl J Med 335 : 1480 , 1996 .
71. Scott JS : Pregnancy toxaemia associated with hydrops fetalis, hydatidiform mole and hydramnios , J Obstet Gynaecol 65 : 689 , 1958 .
72. Shah DM et al : Circulating endothelin-1 is not increased in severe preeclampsia , J Matern Fetal Med 1 : 177 , 1992 .
73. Shah DM et al : Definitive molecular evidence of RAS in human uterine decidual cells , Hypertension 36 : 159 , 2000 .
74. Shah DM et al : Neonatal outcome of premature infants of mothers with preeclampsia , J Perinatol 15 : 264 , 1995 .
75. Shah DM et al : Reproductive tissue renin gene expression in preeclampsia , Hypertens Pregnancy 19 : 341 , 2000 .
76. Shah DM, Reed G : Parameters associated with adverse perina-tal outcome in hypertensive pregnancies , J Hum Hypertens 10 : 511 , 1996 .
77. Sibai BM et al : A comparison of no medication versus methyl-dopa or labetalol in chronic hypertension during pregnancy , Am J Obstet Gynecol 162 : 960 , 1990 .
78. Sibai BM et al : Pregnancy outcome in 303 cases with severe preeclampsia , Obstet Gynecol 64 : 319 , 1984 .
79. Sibai BM et al : Prevention of preeclampsia with low-dose aspi-rin in healthy, nulliparous pregnant women , N Engl J Med 329 : 1213 , 1993 .
80. Sibai BM et al : Risk factors for preeclampsia in healthy nullipa-rous women: a prospective multicenter study , Am J Obstet Gynecol 172 : 642 , 1995 .
81. Sibai BM et al : Severe preeclampsia-eclampsia in young primi-gravid women: subsequent pregnancy outcome and remote prognosis , Am J Obstet Gynecol 155 : 1011 , 1986 .

290 SECTION III PREGNANCY DISORDERS AND THEIR IMPACT ON THE FETUS
82. Sibai BM et al : Severe preeclampsia in the second trimester: recurrence risk and long-term prognosis , Am J Obstet Gynecol 165 : 1408 , 1991 .
83. Sibai BM et al : The incidence of nonpreventable eclampsia , Am J Obstet Gynecol 154 : 581 , 1986 .
84. Sorem KA, Shah DM : Advanced triploid pregnancy and preclampsia , South Med J 88 : 1144 , 1995 .
85. Spinillo A et al : Cigarette smoking in pregnancy and risk of pre-eclampsia , J Hum Hypertens 8 : 771 , 1994 .
86. Stone SR, Pritchard JA : Effect of maternally administered mag-nesium sulfate on the neonate , Obstet Gynecol 35 : 574 , 1970 .
87. Symonds EM : Aetiology of preeclampsia: a review , J R Soc Med 73 : 871 , 1980 .
88. Symonds EM : Bed rest in pregnancy , Br J Obstet Gynaecol 89 : 593 , 1982 .
89. Symonds EM : Renin and reproduction , Am J Obstet Gynecol 158 : 754 , 1988 .
90. Takimoto E et al : Hypertension induced in pregnant mice by placental renin and maternal angiotensinogen , Science 274 : 995 , 1996 .
91. Taylor RN et al : Women with preeclampsia have higher plasma endothelin levels than women with normal pregnancies , J Clin Endocrinol Metab 71 : 1675 , 1990 .
92. Terragno NA et al : Prostaglandins and the regulation of uterine blood fl ow in pregnancy , Nature 249 : 57 , 1974 .
93. Venkatesha S, et al : Soluble endoglin contributes to the patho-genesis of preeclampsia , Nat Med 12 : 642 , 2006 .
94. Villar MA, Sibai BM : Clinical significance of elevated mean arterial blood pressure in second trimester and threshold increase in systolic or diastolic blood pressure during third trimester , Am J Obstet Gynecol 160 : 419 , 1989 .
95. Volpe JJ : Effect of cocaine use on the fetus , N Engl J Med 327 : 399 , 1992 .
96. Wallukat G et al : Patients with preeclampsia develop agonistic autoantibodies against the angiotensin AT 1 receptor , J Clin Invest 103 : 945 , 1999 .
97. Walsh SW : Preeclampsia: An imbalance in placental prostacy-clin and thromboxane production , Am J Obstet Gynecol 152 : 335 , 1985 .
98. Ward K et al : A molecular variant of angiotensinogen associated with preeclampsia , Nat Genet 4 : 59 , 1993 .
99. Weinstein L : Syndrome of haemolysis, elevated liver enzymes, and low platelet count: a severe consequence of hypertension in pregnancy , Am J Obstet Gynecol 142 : 159 , 1982 .
100. Wilcox CS et al : Thromboxane mediates renal hemodynamic response in infused angiotensin II , Kidney Int 40 : 1090 , 1991 .
101. Wolf FD et al : The ultrastructure of acute atherosis in hyper-tensive pregnancy , Am J Obstet Gynecol 123 : 164 , 1975 .
102. Woods LL : Role of renin-angiotensin system in hypertension during reduced uteroplacental perfusion pressure , Am J Physiol 257 : 204 , 1989 .
103. Yallampalli C, Garfield RE : Inhibition of nitric oxide synthe-sis in rats during pregnancy produces signs similar to those of preeclampsia , Am J Obstet Gynecol 169 : 1327 , 1993 .
104. Yamamoto T et al : Anti-ssDNA and -dsDNA antibodies in preeclampsia , Asia Oceania J Obstet Gynaecol 20 : 93 , 1994 .
105. Zuspan FP : Factors affecting delivery in preeclampsia: condi-tion of the cervix and uterine activity , Am J Obstet Gynecol 100 : 672 , 1968 .
106. Zuspan FP : Problems encountered in the treatment of pregnancy-induced hypertension: a point of view , Am J Obstet Gynecol 131 : 591 , 1978 .





























