-
ObjectivesIncidence and
SignificanceSelectionManagementIntrapartumDelivery
-
Definitionlongitudinal liebreech or lower extremity
presentingcephalic pole in the uterine fundus
Typesfrank- flexed hips, extended kneescomplete- flexed hips,
flexed kneesfootling- extended hip(s)
-
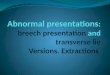
Types of BreechCompleteFootlingFrank
-
Incidence3 to 4% of all pregnanciesincreases with decreasing
gestational age 7 to 10% at 32 weeks 25 to 35% at < 28 weeks
-
Etiology of Breech Presentation
idiopathicprematurity (head to trunk size)uterine or pelvic
structural abnormalityuterine fibroidfetal anomaly or
abnormalitypolyhydramniosmultiple gestation
-
Diagnosis maternal perception of movementLeopolds maneuversFH
auscultated above umbilicusvaginal examultrasoundX-ray
-
Recommendations for Breech Deliveryrecommend trial of labour at
36 weeks or when estimated weight is 2500 to 4000 gramsoffer trial
of labour at 31 to 35 weeks gestation or when estimated weight is
1500 to 2500 gramsoffer caesasean section at 30 weeks gestation or
when estimated weight is < 1500 grams*no recommendation for when
estimated weight is > 4000 grams* * acknowledged lack of
evidence for recommendation
-
Selection Criteria for Trial of Labourfrank or complete
breechfetal head not hyperextendedestimated fetal weight 2500 to
4000g
-
Ultrasound Assessmentconfirm lie and type of breechassess head
positionobtain estimate of fetal weightassess for IUGR and
congenital anomaliesassess amniotic fluid volumeconfirm placental
localization
-
Contraindications to Trial of Labourfetal or maternal
contraindication to labourfootling breechhyperextension of the
fetal headabsence of informed consentabsence of experienced
maternity health care giver
-
Management in Labourplanned delivery in hospitaladmission in
early labour or with ROMappropriate fetal surveillanceepidural and
ARM for usual indicationsimmediate vaginal exam at ROM to rule out
cord prolapsegood progress in labour ( 0.5 cm/h after 3
cm)induction and augmentation permissible
-
Management at Deliveryexperienced newborn resuscitator
presentempty maternal bladdermaternity attendant with experience in
breech delivery forceps if available, may be helpful
-
Entering the PelvisObstetrics - Normal and Problem Pregnancies,
2nd EditionEdited by SG Gabbe, JR Niebyl, JL Simpson. (1991)
-
Descent of the BreechObstetrics - Normal and Problem
Pregnancies, 2nd EditionEdited by SG Gabbe, JR Niebyl, JL Simpson.
(1991)
-
Spontaneous ExpulsionObstetrics - Normal and Problem
Pregnancies, 2nd EditionEdited by SG Gabbe, JR Niebyl, JL Simpson.
(1991)spontaneous expulsion to the umbilicusthe sacrum should be
gently guided anteriorlysingleton breech extraction is
contraindicatedC/S is indicated for failure of descent or
expulsion
-
Hurry up & Wait!
DONT PULL!traction deflexes the fetal headmay cause nuchal
armObstetrics - Normal and Problem Pregnancies, 2nd EditionEdited
by SG Gabbe, JR Niebyl, JL Simpson. (1991)
-
Deliver Legs by lateral rotation of thighs and flexion of knees
- keep sacrum anteriorObstetrics - Normal and Problem Pregnancies,
2nd EditionEdited by SG Gabbe, JR Niebyl, JL Simpson. (1991)
-
Delivery of Armsgood maternal pushingdeliver when winging of
scapulae seenrotate arm to anteriorsweep humerus across the chest
and deliverrotate other arm anterior and repeat to
deliverObstetrics - Normal and Problem Pregnancies, 2nd
EditionEdited by SG Gabbe, JR Niebyl, JL Simpson. (1991)
-
Avoid Over-extensionObstetrics - Normal and Problem
Pregnancies,2nd EditionEdited by SG Gabbe, JR Niebyl, JL Simpson.
(1991)
-
Delivery of the head Mauriceau - Smellie - Veit manoeuvre to
deliver the head in flexion The body should be supported in a
horizontal position
-
Delivery of the headObstetrics - Normal and Problem Pregnancies,
2nd EditionEdited by SG Gabbe, JR Niebyl, JL Simpson. (1991)
-
Delivery of the headForcepsassistant elevating babedirect
applicationObstetrics - Normal and Problem Pregnancies, 2nd
EditionEdited by SG Gabbe, JR Niebyl, JL Simpson. (1991)
-
Prevention of Breech
consider external cephalic version at 36 weeks gestation for
eligible candidatessuccess rate 30 - 70% depending on
experienceresults in lower cesarean section rate
-
Conclusions
proper selection of patientsthorough explanation and informed
consentgood progress in labour ( 0.5 cm/h after 3 cm)induction and
augmentation permissibleexperienced attendantsstandard fetal
monitoringassisted delivery - DONT PULL - stay cool!