Embed Size (px)
DESCRIPTION
mengenai amputasi
Citation preview

CHAPTER 56
Amputations
56.1 The general method for amputations
You will need to amputate a patient’s leg about five timesmore often than his arm. Once you have cut off a limb thereis no going back, so try to retain as much function as youcan. The patient is unlikely to get an arm prosthesis, andit would be of little use even if he could get one. So aiminstead for the longest possible stump of an arm. Every cen-timetre is useful, so is an elbow which he can use as a hook,and so is any kind of a wrist.
A patient’s leg must have a prosthesis which will bear hisweight. There are a limited number of these, and the stumpsfor hem are standardized. So always do one of the standard legamputations. There are three technological grades of prosthe-sis; of these the third is not necessarily the worst. A patientmight have: (1) A sophisticated modern prosthesis costing $300 or more. (2) A simpler modern prosthesis costing $ 30,such as one of those developed by Huckstep for polio (26.2),which any bicycle mechanic can mend. Or, (3) the patientmight have a traditional prosthesis, such as a pylon, a pegleg, or elephant boot. Don’t despise these; when well madethey last longer than any of the others, and are better than amodern prosthesis for working in the fields.
A leg prosthesis can: (1) Have a cup to bear weight on thesides of the stump, in which case the scar should be at theend. (2) Bear weight on the end of the stump, in which casethe scar should be posterior. (3) Have a modern total contactsocke in which the position of the scar is unimportant. Limbfitting centres vary in their scope and preferences, so visityour local one and find out what they like. A good pros-thetist can fit any well constructed stump with a prosthesis.
IN THE ARM CONSERVE EVERY CENTIMETRE, IN THE LEGDO A STANDARD AMPUTATION
In the abdomen poor surgical craftsmenship is hidden,but on an amputation stump it is there for everyone to see.In a perfect stump: (1) The scar is not exposed to pressure.(2) The skin slides easily over the bone. (3) The skin is not in-folded. (4) There is no redundant soft tissue. (5) There is noprotruding spur of bone. (6) The stump is painless. And, (7)the wound has healed by first intention. Most amputationstumps should be conical.
Fish mouth flaps As a general rule, cut the fish mouthflaps shown in Fig. 56-4. The alternative is a guillotine am-putation, as described in Section 56.2. Fish mouth flaps mustbe long enough to cover the soft tissues of the stump, but notbe so long that their blood supply is inadequate and theynecrose. If the flaps are equal, the scar will come at the endof a stump. If they are unequal the scar can come at thefront or the back. Try to place the scar where it is not goingto be pressed on. In the hand and the foot, place it dor-sally. Higher up the arm the scar can be anywhere. In theleg, its site depends on the kind of prosthesis the patient isto have—end bearing, side bearing, or total contact. In thelower arm and leg transverse scars are better than antero-posterior ones because they do not get drawn up betweenthe two bones.
Immediate suture or delayed primary closure? Delayedprimary closure is always wise: (1) If the patient’s limb isalready infected, or might easily become so. (2) In all battlecasualties. (3) If there is much soft tissue injury. (4) If theblood supply of the stump is uncertain. If you decide on
SOME TRADITIONAL APPLIANCES
A B C
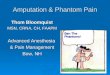
Fig. 56.1: SOME LOCALLY MADE APPLIANCES. A, a traditionalsplint for a child’s forearm as used by the Pokot in Uganda. B, a Pokotsplint for fractures of the shaft of the humerus—exactly what Section 71.17would approve of! C, this Zimbabwian patient used his ingenuity in over-coming the disability of an amputation, and although the result is not bau-tiful and required constant attention, he was able to get around. Kindlycontributed by Kevin Rankin and Peter Cox.
1

56 Amputations
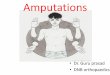
WHERE TO AMPUTATE?
ADULT
CHILD
Save every centimetre in the armDo classical amputations in the leg
disarticulation
amputation
save everycentimetre
disarticulateif you can
DISARTICULATIONIS SPECIALLYDESIRABLEIN CHILDREN
vary these tosave allpossible length
upper arm
supracondylar
disarticulation
proximal forearm
distal forearm
wristcarpus
for the fingerssee Chapter 75
CLASSICALSITES ONLY
25 cm
aboveknee
12−18 cm
belowknee
a common mistakeis to amputate here
Syme’s
transmetatarsal
similar amputationsas in fingers
Fig. 56.2: AMPUTATION SITES. In the arm save every centimetre. Inthe leg amputate at the classical sites only.
delayed primary closure, cut the flaps long, to allow themto retract. Leave the patient’s muscle and fascia unsutured,bandage the skin flaps over dry gauze swabs, don’t put inany stitches, and bring him back to the theatre 3 to 5 dayslater. If his wound is not infected, close it. If it is infected,leave the flaps open for a week or longer, and close it laterby secondary suture.
Postoperative care. Much depends on what happens toa patient after he leaves the theatre. His leg stump must beprepared for the prosthesis, and he need, to be taught howto use it. Firm bandaging will hasten to conversion of hisstump from a bulky cylinder to a narrow cone, and exerciseswill strengthen its remaining muscles. So, give the stumpsomething to do. After a lower leg amputation he can learnto kick a large rubber ball about.
How do amputations differ in children? Most of thesame principles apply in a child. Disarticulate a joint if youcan, especially at his knee, because this will preserve its epi-physis. Removing a limb by amputating through the shaftof a bone produces an effect which varies with the site. Itcan either cause excessive bony overgrowth with the needfor a revision amputations later, or a short stump.
• SAW, amputation, with hinged back, 230 mm, (a) saw,
AMPUTATION EQUIPMENT
AMPUTATION SAW
GIGLI SAW
AMPUTATION KNIFE
TENOTOMY KNIFE
Fig. 56.3: EQUIPMENT FOR AMPUTATION. If necessary, you can useany saw or a domestic knife.
one only. (b) Spare blades for the above, three only. Theback of the saw stiffens it during the early part of the cut,but can be hinged back later to let the saw pass through.
• SAW, Gigli, (a) pair of handles, one pair only, (b), Sawblades, 30 cm, four only A Gigli bone saw is a piece of wirewith sharp teeth on it which you pull to–and–fro betweentwo handles. Use it to cut bone in awkward places.
• KNIFE, amputation, Liston 180 mm, one only If youdon’t have an amputation knife, sharpen a long kitchenknife and use that.
Here is the sequence of steps for all amputations. theyare not repeated in the instructions for the specific sites de-scribed later. Follow the steps in the order in which we givethem here.
GENERAL METHOD FOR AMPUTATIONS
INDICATIONS (1) An arm which is so severely injured thatthere is no chance of recovery of any part of the hand, fin-gers or thumb. (2) A leg which is so severely injured that youcannot restore the continuity of its vessels or nerves, espe-cially when there is gross contamination or severe muscle orskin loss. Loss of bone alone without nerve or vascular in-jury does not usually justify amputation. (3) Gas gangrene.(4) Established gangrene due to vascular injury. (5) Con-tinued infection with severe bone or nerve injury. (6) Sec-ondary haemorrhage if all other measures fail. (7) Multiplein injuries in a gravely ill shocked patient. Amputation maybe the simplest and fastest way of removing large amountsof damaged muscle, and so saving his life. (8) Occasionallyalso for epitheliomas, bone tumours, or snake bites.
CAUTION! If you amputate for a malignancy, biospy it first.ANAESTHESIA Relaxation is unecessary Ketamine is ad-
equate (8.1). Subarachnoid (spinal) anaesthesia (A 7.4) isparticularly useful for below knee amputations. Nobody likeshearing their bones being sawn through, so if a patient isconscious premeditate him heavily.
TOURNIQUET Use a tourniquet (3.8), except when youare amputating for ischaemia. Bleeding is a useful sign that
2

56.1 The general method for amputations
a muscle is alive. If it is dead you may need to amputatehigher up. A tourniquet may also make ischaemia worse.Release it before you suture the muscles, so that you cantie the bleeding vessels before you cover them.
When you use a tourniquet, exsanguinate the patient’slimb with an Esmarch bandage first (3.3), except whenyou are amputating for sepsis or malignancy which it mayspread.
CAUTION! Don’t rely on digital pressure over the mainvessels to control bleeding.
CUTTING FISH MOUTH FLAPS FOR AN AMPUTATION
Decide where you are going to saw the bone (the point ofsection) and plan the flaps in relation to that point. Placethe angle of the fish mouth at the site of bone section. Markthem out carefully with methylene blue or scratch marks.
If the flaps are equal, make the length of each of themequal to 3/4 of the diameter of the limb as in A, Fig. 56-4.
If the flaps are unequal, make the longer flap equal tothe diameter of the limb, and the shorter one equal to halfits diameter, as in B. Cut through the skin down to the deepfascia, and reflect this up with the skin as part of the flap.The shin of the stump will need to slide over the deep fascia,so keep them together. If you are amputating for ischaemia,minimize trauma to the flaps. Handle them with stay suturesrather than with forceps.
CAUTION! (1) Start by making fish mouth flaps long. Youcan always trim them if they are too long later, but you can-not lengthen them if they are too short. (2) Cut them roundnot pointed. (3) Their combined length should be equal oneand a half times the diameter of the limb at the site of bonesection. (4) If you are amputating a severely lacerated limb,try to preserve all viable skin.
CONTROLLING BLEEDING DURING AN AMPUTATION
Early in the operation, find the major arteries and veins.Tie them separately with double transfixion ligatures (3.2)preferably linen. Then cut them between these ligatures.Later, after you have removed the limb, release the tourni-quet slowly and tie the remaining smaller vessels. If the cutends of the muscles bleed furiously, apply packs for five min-utes.
If the amputation is very high you may have to expose themain artery higher up at one of the classical sites describedin Sections 3.4 to 3.7.
CAUTION! (1) If you don’t use a tourniquet, find and tie themajor vessels before you cut them. (2) Don’t clamp them,cut them and then try to tie them. If a clamp slips there willbe massive bleeding. (3) Careful haemostatsis of the stumpis essential. If a clot forms, it is easily infected.
CUTTING MUSCLES DURING AN AMPUTATION
Muscles always contract, after you have cut them. So cutthem transversely about 5 cm distal the site of bone section.Leave them a little longer if you are using delayed primaryclosure, because they will have more time to shrink.
Use a long sharp amputation knife or carving knife to cutthe muscles straight down to the bone. Don’t use a scalpelwhich makes many small cuts, and leaves shreds of injuredmuscle.
THE GEOMETRYOF FISH MOUTHFLAPS
A
B
C
D
F
E
EQUAL FLAPS
UNEQUAL FLAPS
X
site of bone section
1/2 x
stump
is this endthe patient
3/4 x
X
X
with deep fasciaskin reflectedof section,to the siteflap reflected
leg or armto be
removed
5 cm
muscle cut5 cm distalto the site ofbone section
cut musclescontracting
don’t strip theperiosteumhere
periosteum cutall around the bonebefore it is sawn
the musclesremoved withperiosteum
muscles sewnover bone
equal flaps makethe scar at the endof the stump
unequal flaps makethe scar at the sideof the stump
Fig. 56.4: FISH MOUTH FLAPS. Together, the flaps should be one and ahalf times the diameter of the limb. Either make them as two equal flaps,each 3/4 of the diameter of the limb, or, make one flap equal to the wholediameter and the other flap equal to half of it. Kindly contributed by PeterBewes.
CUTTING NERVES DURING AN AMPUTATION
Don’t tie nerves. A painful neuroma will result, especially inthe fingers. Instead, gently pull each nerve into the wound,cut it cleanly with a knife, then let it retract above the ampu-tation site.
3

56 Amputations
towel withone or twoslots in it
HOW TO COVER THESTUMP WHILE YOU SAW
Fig. 56.5: HOW TO COVER THE STUMP WHILE YOU SAW. Thetowel with two slots in it is for forearm and lower leg. The central flapgoes between the bones. From an unknown source.
SAWING BONES DURING AN AMPUTATION
Clear the muscle from the site of section, and incise the pe-riosteum all round it. Reflect this distally for one or two cen-timetres with the muscles, so as to leave bare bone for thesaw.
Use a saw with well set teeth. Start by steadying it withyour thumb. Draw it towards you across the bone a fewtimes. When it has made a good slot in the bone, start saw-ing hard. Ask an assistant to hold the patient’s limb to steadyit, and pull gently to prevent the saw locking in the bone andsplitting it. Finally, remove any spikes with bone forceps, andbevel any protruding edges with a coarse rasp.
CAUTION! (1) Don’t reflect the periosteum proximally, be-cause the bone under it will die, and a ring sequestrum willform. (2) Don’t damage the surrounding muscle with thesaw. Cut the muscle first, or retract it well out of the way witha towel wrapped round the limb, as in Fig. 56-5, then saw.(3) Bone dust from the saw acts as a foreign body, so washit away with saline.
DEALING WITH FAT DURING AN AMPUTATION
If a patient’s limb is very fat, cautiously remove as much sub-cutaneous fat as is necessary. Don’t remove too much, es-pecially near the edges of the flap, or it may necrose. Learnto design flaps so that they come together accurately withoutdog ears’ If they form, leave them, they will soon disappear.
CLOSING THE WOUND AFTER AN AMPUTATION
SUTURES As indicated above, delayed primary suture willbe safer. Suture the skin and deep fascia separately.
Close the flaps without tension, without leaving gaping ar-eas between the sutures, and without tying them too tight.
DRAINS If you use delayed primary suture, no drains arenecessary. If you close a stump by immediate suture, inserta drain under the muscle flap (if there is one) over the endof the bone. If possible, use a suction drain. If you don’thave one, insert a 2 cm corrugated rubber drain. Bring bothits ends out loosely through the two ends of the incision asshown in F, Fig. 56-4.
CLOSING THE STUMP
Fig. 56.6: CLOSING AN AMPUTATION STUMP. Close the deep fascia,then the skin.
If no blood is oozing from the drains, remove them at 48hours, if blood continues to flow, leave them for a further 24hours.
DRESSINGS Dress the stump firmly, but not too tightly. Aplaster covering will make it more comfortable. Change thedressings at 48 hours.
POSTOPERATIVE CARE FOR AN AMPUTATION
As soon as the skin has healed, bandage the stump. Forthe leg, sew two 15 cm crepe bandages end-to-end. For thearm, use one 10 cm bandage. Roll the bandage tightly, thenwind it round the stump. Apply more tension to the end of thestump, than to its base, or it will become bulbous. Reapplythe bandage several times a day until the prosthesis is fitted.Don’t use adhesive strapping, or you may tear the skin of thestump.
THE FURTHER MANAGEMENT FOR AN AMPUTATION
Read on for: guillotine amputations (56.2), amputating forgangrene (56.3), amputating through the upper arm andelbow (56.4), the lower arm and wrist (56.5), above theknee (56.6), through the knee (56.7), below the knee (56.8),Syme’s amputation (56.9), and amputating through the footand toes (56.10).
DIFFICULTIES WITH AMPUTATIONS
If a patient’s LIMB IS TRAPPED in a falling building, youmay have to amputate it on the spot. Give him ketamineor intravenous morphine (8.6), or infiltrate his tissues with alocal anaesthetic. Control bleeding by pressing on the pres-sure point, or with a tourniquet and then tie the vessels. Cutthrough his trapped limb with an amputation knife and a saw,as far distally as you can, and apply a firm pressure dressingto the stump. Transfer him to hospital for a formal amputa-tion at the next most suitable site higher up his limb, eitherimmediately, or later.
If a patient is SEVERELY SHOCKED, you can do a quickprovisional amputation distal to the site of election. Later,when his wound has healed, you can do a definitive am-putation with immediate primary closure. He will no longerbe shocked, his skin will be normal, and there will be lessdanger of infection.
If you amputate in an emergency for shock, or sepsis, or toremove a grossly crushed limb, don’t do the final amputationuntil the stump is healing well.
4

56.3 Amputating for ischaemic gangrene
If his STUMP BLEEDS SOME HOURS AFTER THE OP-ERATION (reactionary haemorrhage), take him back tothe theatre, explore his wound, tie the vessels, leave hiswound open and sew it up secondarily. To prevent this hap-pening: (1) tie the major vessels carefully, (2) release thetourniquet slowly, (3) control the vessels thoroughly, and (4),apply a pressure dressing.
If his STUMP BLEEDS SOME DAYS LATER (secondaryhaemorrhage), it is likely to be serious. Explore the wound.In desperation, open it, pack it with dry gauze, and removethe gauze 48 hours later.
If his STUMP BECOMES INFECTED, this may havebeen your fault. Did you: (1) Close the wound by imme-diate primary suture, when delayed primary suture wouldhave been wiser? (2) Fail to control bleeding, before closingthe flaps, so that the blood clot beneath them has becomeinfected? (3) Strip up the periosteum from the stump so thata ring sequestrum has formed and become infected?
If a PERSISTENT SINUS develops in the stump, ex-plore it; you may find a piece of necrotic tendon, or an areaof osteomyelitis. Another possibility is a stitch sinus. If theoffending stitch might be securing a vessel, don’t remove ituntil you have tied the vessel higher up. Explore the stump,remove all dead and dying tissue, and pack it ready for sec-ondary closure.
If the FLAPS BREAK DOWN, you probably cut them tooshort and closed them too tight. Wait until the granulationtissue is fit for grafting and then graft it. The final qualityof the skin over the stump will be worse than it would havebeen if the flaps had survived, and it may break down later.Alternatively, you may have to amputate higher up.
If a PATCH OF GANGRENE forms in a flap, be careful,it may hide a larger area of necrosis underneath. You maybe able to trim it away, or you may have to amputate againhigher up, especially if a patient’s limb is ischaemic. If it isnot ischaemic, you may be able to excise the gangrenousarea, allow granulations to develop, and apply a split skingraft.
If he has GAS GANGRENE, amputate high up, throughhis shoulder if need be, and leave the wound open.
If a PROSTHESIS CANNOT BE FITTED, you probablydesigned the stump wrong. The reasons include: (1) boneadherent to the scar, (2) a spicule of bone sticking outthrough the skin, (3) a flexion contracture in a below kneeor above knee amputation, (4) too short a stump.
CUT FLAPS LONG REFLECT THE DEEP FASCIA WITH THESKIN DELAYED PRIMARY CLOSURE IS SAFER
56.2 Guillotine amputations
If you amputate a severely infected limb, the infection maybe spread to the stump, especially if you are amputating forgas gangrene. It will be less likely to do so if you: (1) Cutstraight down to the bone all round the limb, and then sawthe bone through at the same level, (2) leave the surface un-sutured, and (3) revise the amputation later if necessary. Aguillotine amputation is quick, and the flaps are less likelyto necrose if the blood supply is poor. Some surgeons neveruse them.
GUILLOTINE AMPUTATIONS Apply a tourniquet. Cut theflaps as far distally as you can, so that you can refashionthem later. Cut the patient’s skin down to his deep fascia allround his limb 2 cm distal to the site of bone section. Let itretract. Then cut the muscle all round his limb down to thesame site.
Tie and cut all the large vessels you meet. Cut all majornerves at least 2 cm proximal to the end of the stump. Dressthe patient’s stump with vaseline gauze and plenty of drygauze. Bandage it, and let it granulate. When it has healed,or there is no further risk of infection, either: (1) revise theamputation higher up, or (2) graft it, or (3) refer him.
56.3 Amputating for ischaemic gangrene
Deciding where to amputate can be difficult. The lower youamputate, the greater the chance that the patient will walkagain afterwards. But there is also more chance that thetissue through which you amputate will not be viable, sothat his stump will become infected or gangrenous. Feel hispulses carefully, if you cannot feel his popliteal pulse, do anabove knee amputation.
If his muscles do not look healthy when you cut them,abandon the operation at that site, and amputate higher up.Healthy muscle is a nice bright red, and has a good capillaryooze. Ischaemic muscle is a dusky bluish red, and bleedslittle or not at all. The tissues of a diabetic are at particularrisk, including those of his other limb. So handle the flapswith your fingers, not with forceps. Protect his other limbduring the operation so as to make sure that pressure soresdo not form. Control his diabetes as in A 17.7.
When you amputate for ischaemia, always close thewound by delayed primary closure (54.4).
56.4 Amputating through the upper arm andelbow
Save as much of the length of the patient’s arm as you can,because he will probably have no prosthesis. If possible,disarticulate his elbow. If you amputate higher up, a con-venient place is 18 to 20 cm below his acromion. If you canleave him with a reasonable length of humerus, he can useit to hold things by gripping them against his chest. If youhave to amputate very high up, even a very short stump
A GUILLOTINE AMPUTATION
Fig. 56.7: A GUILLOTINE AMPUTATION. A guillotine amputation isquick, and the flaps are less likely to necrose if the blood supply is poor.
5

56 Amputations
will preserve the outline of his shoulder. If he is to havea prosthesis, don’t amputate through the lower 4 cm of hishumerus, because it will be difficult to fit.
Remember that his brachial artery lies quite superficially,and is overlapped medially by his biceps.
AMPUTATING THROUGH THE UPPER ARM
For the general method see Section 56.1. Prepare the op-eration site, and abduct the patient’s arm to about 80◦ on anarm board. Place a block under his arm just proximal to theamputation site. Apply a tourniquet as high as you can.
THE MID UPPER ARM AS AN AMPUTATION SITE
Start proximally at the site of bone section, and mark outequal anterior and posterior skin flaps. Make the length ofeach flap 3/4 of the diameter of his arm at the site of section.
Find, doubly ligate, and cut his brachial artery and veinjust above the site of section. Find, gently pull and cut themajor nerves so that their ends retract well above the stump.
Cut the anterior muscles 1.5 cm distal to the site of sec-tion. Cut the triceps 4 cm distal to the site of section. Cutthe periosteum all round the patient’s humerus and saw itthrough. Rasp the end of his humerus smooth. Bevel histriceps to make a thin flap, reflect it anteriorly over the endof his humerus, and sew it to the anterior muscle and fascia.Release the tourniquet, control bleeding, drain and close thestump as usual (56.1).
THE SUPRACONDYLAR REGION AS AN AMPUTATIONSITE
Starting proximally at the site of bone section, mark outequal anterior and posterior skin flaps, each as long as 3/4
SUPRACONDYLARAMPUTATION OFTHE UPPER ARM
biceps
musculocutanous nerve
brachial artery
median nerve
ulnar nerve
triceps
brachialis
brachioradialis
radialnerve
radialis longusextensor carpi
LATERAL SIDE
MEDIAL SIDE
Fig. 56.8: AMPUTATING THROUGH THE UPPER ARM. If you canleave a patient with a reasonable length of humerus, he can use it to holdthings by gripping them against his chest. After Robb and Smith with the kindpermissin of Graham Stack.
of the diameter of the patient’s arm at the site of section, asin Fig. 56-8. Find, clamp, tie, and cut his brachial artery andvein just proximal to the site of section. Cut his median, ul-nar, and radial nerves at a higher level so their ends retractwell above the stump.
Cut the muscles in the anterior compartment of his arm1.5 cm distal to the site of section. Free the insertion ofhis triceps tendon from his olecranon. Preserve his tricepsfascia and muscle as a long flap.
If he has any hope of an elbow prosthesis, reflect thisflap proximally and cut the periosteum all round his humerusat least 4 cm above his elbow joint to allow room for theelbow mechanisms of the prosthesis.
If he has no hope of an elbow prosthesis, leave asmuch bone as you can. Saw across his humerus at the levelyou choose, and rasp its end smooth. Trim his triceps ten-don to make a long flap, carry it across the end of the bone,and sew it to the fascia over the anterior muscles.
Release the tourniquet, control bleeding, drain and closethe stump as usual (56.1).
DISARTICULATING THE ELBOW
Make equal anterior and posterior skin flaps. Start at thelevel of the patient’s epicondyles and curve the posterior flap2.5 cm distal to the tip of his olecranon. Bring the anteriorflap just distal to the insertion of his biceps tendon. If neces-sary make any suitable flap.
Reflect the flaps to the level of his epicondyles. Start onthe medial side. Find and divide the lacertus fibrosus. Freethe origin of his flexor muscles from his medial epicondyleand reflect it distally to expose the neurovascular bundle onthe medial side of his biceps tendon. Tie and cut his brachialartery just above the joint. Gently pull his median nerve andcut it proximally. Find his ulnar nerve in its groove behind hismedial epicondyle and cut it proximally in the same way.
Free his biceps tendon from his radius, and his brachialistendon from the coronoid process of his ulna. Find his radialnerve in the groove between brachialis and brachioradialis,pull it, and cut it proximally.
On the lateral side of his elbow, cut his extensor muscles6.5 cm distal to the joint, and reflect their origin proximally.
Cut the patient’s triceps tendon near the tip of his olecra-non. Cut the capsule on the front of the joint, complete thedisarticulation, and remove his forearm.
Leave the articular surface of his humerus intact. Reflecthis triceps tendon anteriorly and sew it to the tendons of hisbrachialis and biceps.
Make a thin flap from his extensor muscles, reflect it me-dially and sew it to the remains of his flexor muscles on hismedial epicondyle. Suture the muscle mass to cover thebony prominences and exposed tendons at the end of hishumerus. Put sutures through the periosteum when neces-sary. Close the flaps without tension.
Release the tourniquet, control bleeding, drain and closethe stump as usual (56.1).
56.5 Amputating through the lower arm andwrist
Losing a hand is a tragedy. Minimize it by trying to pre-serve as much of the length of a patient’s forearm as youcan. An elbow with even a short length of forearm is better
6

56.5 Amputating through the lower arm and wrist
than none. If possible, amputate through his metacarpus orwrist, rather than higher up. Ischaemia is an exception. Thecirculation in the distal forearm; like that of the distal lowerleg, is not good. So if his arm is ischaemic, an amputationhigher up his forearm may be better than one lower down.
If you have to amputate through his wrist, a plastic sur-geon may later be able to make an ’alligator mouth’ out ofhis two forearm bones, so that he has something to grip with(Krukenberg’s operation). Anteroposterior flaps are betterthan lateral ones, because the scar cannot retract betweenthe bones.
AMPUTATING THROUGH THE FOREARM
For the general method see Section 56.1.
AMPUTATING THROUGH THE PROXIMAL FOREARM
Abduct the patient’s arm on an arm board or side table, andplace it supine. If you cut the flaps with his arm prone, theywill later be twisted.
If there is enough good skin, make equal anterior and pos-terior flaps. If skin is scarce, make the best flaps you can.
Reflect the skin flaps with the deep fascia to the site ofsection. Tie, and cut his radial and ulnar arteries just abovethis site. Find his median, ulnar, and radial nerves, pullthem gently, and cut them proximally. Cut his muscles trans-versely distal to the site of section, so that they retract aboveit. Trim away all excess muscle. Saw his radius and ulna andsmooth their cut edges.
Release the tourniquet, control bleeding, drain and closethe stump as usual.
Start elbow and shoulder movements as soon as possible.
AMPUTATING THROUGH THE DISTAL FOREARM
Start at the site of section and cut equal anterior and pos-terior flaps, as in Fig. 56-9. Make them as long as aboutone half the diameter of the forearm at the amputation site.Reflect the flaps proximally to the site of bone section.
Clamp, tie, and cut his radial and ulnar arteries just proxi-mal to the site of section. Find his radial, ulnar, and mediannerves, pull them gently and cut them high up so that theyretract above the end of the stump. Saw both bones.
Release the tourniquet, control bleeding, drain and closehis stump as usual (56.1).
DISARTICULATING THE WRIST
Make a long palmar and a short dorsal flap. Start the incision1.5 cm distal to the patient’s radial styloid, extend it distallytowards the base of his first metacarpal. Carry it distallyacross his palm, and then proximally to end 1.5 cm distalto his ulnar styloid. Make a short dorsal flap by joining thetwo ends of the palmar incision over the dorsum of his hand.Bring the dorsal flap distally level with the base of his middlemetacarpal. If skin is scarce, vary the design of the flaps.
Reflect the flaps proximally with the underlying fascia tohis wrist joint. Tie and cut his radial and ulnar arteries justproximal to the joint. Gently draw his median, ulnar, andradial nerves distally into the wound, and cut them short.Cut all tendons just above his wrist and let them to retract
into his forearm. Cut round the capsule of his wrist joint andremove his hand.
Saw or nibble off his radial and ulnar styloids. Rasp theraw ends of the bones smooth and round.
CAUTION! Don’t injure his radioulnar joint or its triangularligament. If you injure them, he will be unable to rotate hisforearm, and the joint will be painful.
Release the tourniquet, control bleeding, drain and closetha stump as usual (56.1).
AMPUTATING THROUGH THE CARPUS
Make a short dorsal flap and a palmar one twice as long.Reflect the flaps proximally to the site of bone section, andexpose the soft tissues under them.
Pull the flexor and extensor tendons, of his wrist distally,cut them, and allow them to retract into his forearm. Findthe four tendons which flex and extend his wrist (flexor andextensor carpi radial is and ulnaris), free their insertions, andreflect them proximally to the site of bone section.
Find his median and ulnar nerves and the fine filamentsof his radial nerve. Pull them distally and cut them well prox-
AMPUTATINGTHROUGH THEFOREARM
A
B
C
drain both sides
equal anterior and posterior flaps
retract the flaps
saw both bones
Fig. 56.9: AMPUTATING THROUGH THE FOREARM. Preserve asmuch length as you can. An elbow with even a short length of forearm isbetter than none. After Robb and Smith with the kind permissin of Graham Stack.
7

56 Amputations
DISARTICULATINGTHE WRIST
roundedpreserve this
rounded
preservethis
Fig. 56.10: DISARTICULATING THE WRIST. Try to preserve the pa-tient’s distal radio–ulnar joint and his triangular joint. After Champbell,with kind permission.
imal to the site of section. Tie and cut his radial and ulnararteries proximal to the site of section.
Cut the remaining soft tissues down to bone. Saw acrosshis carpal bones, and rasp all rough edges smooth. Anchorthe tendons of his wrist flexors and extensors to his remain-ing carpal bones in line with their normal insertions.
Release the tourniquet, control bleeding, drain and closethe stump as usual (56.1).
AMPUTATING THROUGH THE METACARPUS
Do this as for amputation through the carpus, but preservewhat you can of the patient’s metacarpals, and especiallyhis thumb.
56.6 Amputation above the knee
Many above knee amputations for severe injuries couldhave been avoided, if only a below knee amputation hadbeen done early enough, and not delayed. Provided thestump avoids the condyles of a patient’s femur, the longer itis the better.
Be sure to exercise the stump immediately after the am-putation, so as to strengthen: (1) the patient’s remainingadductor muscles, and prevent the prosthesis moving out-wards when he walks, and (2) his extensors, because theywill have to extend both his hip and the prosthesis which isto form his knee. He will also have to learn to balance withhis hip instead of his foot muscles.
Study the anatomy of his leg carefully, so that you canfind his subsartorial canal fast, and tie his femoral artery.The canal and its vessels are described in Section 3.6.
AMPUTATING ABOVE THE KNEE
Prepare his thigh. Raise his leg so that you can prepare hisupper thigh and groin. Put a drape behind it and anotherone in front.
AMPUTATING ABOVETHE KNEE
A
B
A CROSS SECTION LOOKINGUP AT THE RIGHT LEG
pneumatictourniquet
site ofbone section
25 cm
rectus femoris
sartorius
femoral artery
femoral vein
great saphenous vein
adductor longus
gracilis
adductor magus
semimembranosussemitendinosus
bicepsfemoris
sciaticnerve
profundafemorisartery
linea aspera
intermediusvastus
lateralisvastus
Fig. 56.11: AMPUTATING ABOVE THE KNEE. Provided the stumpavoids the condyles of a patient’s femur, the longer it is the better.
Plan to leave 25 cm of his femur from the tip of his greatertrochanter. If possible, make equal anterior and posteriorflaps. If necessary, adapt them rather than amputatinghigher up. Start the anterior flap on the medial side of histhigh just proximal to the site of bone section. Curve it dis-tally over the front of his thigh, to end on the lateral sideopposite your starting point as in B, Fig. 56-11. Cut the pos-terior flap in a similar way. The combined length of the twoflaps should be one and a half times the diameter of his thighat the site of bone section.
Reflect the flaps to the site of section. Deepen the medialend of the anterior flap so as to expose his femoral arteryunderneath sartorius. Tie and divide his femoral artery andvein (3.6). Use two transfixion sutures for the artery. Beginthe incision in his quadriceps along the line of the anteriorflap, and bevel it proximally to the site of section, so as tomake a muscle flap not more than 1.5 cm thick.
CAUTION! If you are operating for arterial disease and themuscles do not seem viable (56.3), be prepared to amputate
8

56.7 Disarticulating the knee
higher up.Ask your assistant to raise the patient’s leg while you cut
across and bevel his posterior muscles distal to the site ofsection, in the same way as his anterior ones, so they retractto it. Trim away any excessively bulky muscle masses.
Find, clamp, and tie his profunda femoris artery on theposterior aspect of his femur adjacent to the linea aspera.
Find his sciatic nerve under his hamstring muscles, sepa-rate it from its bed without tension, pull it down, tie and cut itabout 5 cm proximal to the end of his femur. Tie the arterythat accompanies the sciatic nerve, but not the nerve itself.
CAUTION! The collateral vessels which accompany hissciatic nerve can bleed profusely.
Cut the periosteum all round his femur and saw it acrossimmediately distal to this cut. Rasp away the prominence ofthe linea aspera and smooth the end of the bone.
Slowly release the tourniquet, and tie bleeding vessels asthey appear.
Sew the anterior muscle flap over the end of the bone.Sew its fascia to the posterior fascia of his thigh. Trim awayany excess muscle or fascia. Insert drains deep to this flap.
Cover the stump with a crepe bandage and then apply aplaster cap. This will relieve pain, and its weight will help toprevent a flexion contracture developing.
CAUTION! Don’t let a flexion contracture develop.
PROSTHESES FOR AN ABOVE KNEE AMPUTATION
If the patient is a long time waiting for his prothesis, padhis stump well, make a cast round it and fit it into a sawnoff thinned down crutch. Keep it in place with more plasterbandages. This will enable him to walk until his permanentprothesis is ready.
If you have to amputate both a patient’s legs above hisknees, consider the possibility of getting him short ’stumpy’protheses for both his legs. He may prefer them to a wheelchair, and they will be easier to balance with than prosthe-ses of the standard length. He will however walk closer tothe ground, and need two short sticks. ’Stumpy’ prosthesesare much easier to make, because they don’t have jointedknees, and need only be sockets with simple boots on. Keepthem in place with cords over his shoulder.
IF THERE IS A DANGER OF SEPSIS, USE DELAYEDPRIMARY CLOSURE
56.7 Disarticulating the knee
Disarticulating the knee: (1) Is one of the easier amputa-tions. (2) Preserves the distal femoral epiphysis of a child,and so allows his stump to grow. (3) Cuts little muscle andno bone, so it is quick, there is little bleeding, and infectionis unlikely. (4) Allows the normal weight bearing end of thebone to bear weight in the prosthesis. Although long flapsare necessary to bring the scar posteriorly, there are suchexcellent anastomoses round the knee that they seldom be-come gangrenous, so it is a good amputation for ischaemicpatients. If you have a choice, disarticulating the knee isbetter than amputating above it. Good prostheses are nowavailable for disarticulated knees.
DISARTICULATINGTHE KNEE A
B
D
E
D
C
10 cm
5 cm
Raising theanterior flap
patellar tendon
The tibialnerve is beingcut proximally
The cruciateligaments and theposterior jointcapsule havebeen cut
anteriorcruciate
tibialnerve
the wound is drained
note the drain onboth sides
patellar tendon
the patellar tendon hasbeen sewn to theanterior cruciate ligaments
Fig. 56.12: DISARTICULATING THE KNEE. A, the flaps marked out.B, the flaps being raised. C, cutting the cruciate ligaments and the poste-rior joint capsule. D, cutting the tibial nerve. E, the patellar tendon sewnto the anterior cruciate ligaments. F, the stump with drains in place. AfterChampbell, with kind permission.
DISARTICULATING THE KNEE
For the general method see Section 56.1.ANAESTHESIA If possible, anaesthetize the patient, and
then turn him onto his face, as in ’Primary Anaesthesia’ Sec-tion 16.12.
METHOD Apply a tourniquet. Cut a long, broad anteriorflap, and a shorter posterior one, as in A, Fig. 56-12. Markthese out with his knee flexed.
Start the anterior incision on the posteromedial side of hisknee just proximal to the joint line. Extend it 10 cm below histibial plateau, and then curve it proximally to end at a pointjust proximal to the joint line on the posterolateral side of hisknee.
Start the posterior incision at the origin of the anterior one.Extend it 5 cm distal to the popliteal flexor crease. Thencurve it proximally to meet the anterior incision.
CAUTION! The anterior flap must have an adequate bloodsupply. If it might not, cut two equal medial and lateral flapsbeginning just above the insertion of the patellar tendon.
9

56 Amputations
Dissect the deep structures on the medial side of the pa-tient’s knee. Expose the tendons of his medial hamstringsand cut them as far distally as you can.
Find, tie and cut the main trunk of his popliteal artery justdistal to its superior genicular branches. These arise high inthe popliteal fossa. Tie his popliteal vein. Reflect the poste-rior flap, cut the fascia, and dissect downwards in the midlinebetween his medial hamstrings on one side and his lateralones on the other.
Cut the deep fascia along the border of the anterior skinflap. Cut his patellar tendon as close to its insertion intohis tibia as you can. Reflect his skin, his fascia, his patellartendon, and the synovial membranes as a single flap (B).
On the lateral aspect of his knee, expose and divide hisbiceps tendon and his iliotibial tract.
Find his common peroneal nerve below his biceps tendon,as it goes towards the head of his fibula. Cut it proximally soit retracts above the level of the amputation.
Reflect the short posterior flap and cut his collateral andcruciate ligaments near their attachments to his femur (C).Find his tibial nerve, draw it gently into the wound, and cut itproximally (D).
Dissect the posterior joint capsule from his tibia. Strip theheads of his gastrocnemius from his femur, and remove hisleg.
CAUTION! (1) The popliteal vessels lie very close to theposterior surface of the knee joint. If you have already tiedthem high up, they should not be in danger. (2) There isno need to disturb the articular cartilage of his femur, or toremove his patella.
Draw his patellar tendon posteriorly through the inter-condylar notch of his femur, and sew it to the ends of hishamstring tendons with several interrupted sutures (E).
Stitch his sartorius and his iliotibial tract to the fascial partof his extensor mechanism. Remove the medial and lateraltubercles of the lower end of his femur. Remove the tourni-quet, control bleeding, drain and close the stump as usual.
Prepare to fit a permanent prosthesis in 6 to 8 weeks.
56.8 Amputating below the knee
This is the most common amputation. If a patient has a goodprothesis, he can do almost anything with it. The methoddescribed below, that of Perssen, as modified by Anderssen,uses two short equal medial and lateral flaps, and is espe-cially suitable for leprosy and ischaemia. You can use it.for all purposes, except when a guillotine incision would bewiser (56.2).
The best length of stump for a modern prosthesis is 12 to18 cm below the patient’s tibial tuberosity. If he is to have thetraditional type of peg leg he needs a shorter 10 cm stump.A stump of only 5 cm too easily slips out of a prothesis, sothat he will be better with an amputation higher up. Don’tamputate below the muscle area of his calf, because the tis-sue here has a poor blood supply.
AMPUTATING BELOW THE KNEE
For the general method, see Section 56.1.ANAESTHESIA It is a great help to be able to turn the
patient onto his face, so a low subarachnoid anaesthetic (A7.6) is suitable. If you cannot anaesthetize him lying on hisface, bend his knee over the end of the table.
AMPUTATING BELOW THE KNEE
A
B
8 − 14 cm
2 cm 2 cm
A B C
sawn obliquely
oblique notch
Fig. 56.13: AMPUTATING BELOW THE KNEE using two equal me-dial and lateral flaps. This is the most common amputation. If a patienthas a good prothesis, he can do almost anything with it. After Perssen andAnderssen.
PREPARATION Wash, shave, and paint the operationsite. Apply a tourniquet. As soon as he is anaesthetized,raise his leg steeply for a few minutes to drain the bloodfrom it. Then bow up the tourniquet. Wrap his foot securelyin a sterile towel.
Mark out the flaps.Line ’A’ is the site of bone section 8 to 14 cm distal to his
tibial tubercle, 12 cm is optimal. This is about the length ofyour index finger, with the base of your second metacarpalon his tibial tubercle.
Line ’B’ is 2 cm distal to ’A’, and marks the point wherethe flaps divide anteriorly.
Line ’C’ marks the distal extent of the flaps.If you are not certain of the geometry of the flaps, cut them
too long rather than too short.Cut through the patient’s skin, his subcutaneous tissue,
and his deep fascia. Cut through the periosteum on the an-terior surface of his tibia.
Raise two medial and lateral semicircular flaps to includethe skin, subcutaneous tissue, deep fascia and the perios-teum on the front of his tibia. Reflect them proximally for2 cm only.
Divide the underlying muscle at this level, and tie the ma-jor vessels as you meet them.
Cut an oblique notch in the front of the tibia, then sawthrough it at line ’A: The notch will be easier to make, if yousaw it before you saw through the tibia.
Saw through the fibula obliquely 1 to 3 cm higher up.Raise his leg, remove the tourniquet, find and tie the re-
maining vessels. Suture the fascia with interrupted monofil-ament sutures.
10

56.9 Syme’s amputation
Don’t try to suture the muscles. They are still attached tothe deep fascia, and should fall neatly into place under thesutured layer of deep fascia.
CAUTION! If there are any of the indications for delayedprimary suture, as listed Section 56.1, this would probablybe wiser. Otherwise, closehis skin with interrupted monofil-ament sutures. Leave any dog ears.
If you have done a neat job, there should be no deadspaces in which a haematoma can collect. If you are notconfident that you have eliminated any dead spaces, inserta drain.
Cover the stump, including the patient’s knee, with gener-ous gauze pads, and apply a firm pressure dressing. Moulda thin plaster shell round the stump, including the distal partof his thigh, with his knee fully extended, or apply a backslab.This is an effective way of preventing a flexion contracture.
Day 3. Keep the stump elevated. Start quadriceps exer-cises.
Day 14. Remove the plaster shell and the sutures. Bindthe stump with a tight bandage. Start’ active knee exercisesagainst resistance.
Day 28. Fit him with his first prosthesis.CAUTION! Watch for and prevent a flexion contracture,
because it will prevent a prosthesis being fitted. If you aretoo late to prevent it, the best treatment may be to cut thestump even shorter, to allow the contacture to become evenmore severe, and then to fit a peg leg.
56.9 Syme’s amputation
This is a disarticulation of a patient’s ankle, adapted so thatthe stump can bear his weight. All the bones of his foot areremoved, and his malleoli are sawn off, so that the end ofhis tibia is flat. A large full thickness heel flap is removedsubperiosteally from his calcaneus, and brought forward tomake a solid covering for the end of his tibia. He can walkabout his house on it without a prosthesis or crutches, eventhough his leg is about 5 cm short. He can also wear a sim-ple and durable elephant boot. His distal tibial epiphysis ispreserved, so it is good amputation if he is a child.
This is an excellent amputation if it is well done, but itis also the most difficult of the amputations described here.If you are not skilled, amputating below his knee would bewiser. However, if a Syme’s amputation fails, a below kneeamputation is always possible.
A patient’s posterior tibial vessels run into his foot justbehind his medial malleolus. If you cut them too high, theycannot supply his heel flap. So: (1) Shell out his calcaneusfrom under the periosteum when you dissect the flap. If youcan preserve the periosteum a useful piece of new bone willform in it. (2) Cut the vessels as far distally as you can. (3) Besure to keep the heel flap correctly aligned postoperatively,so that the patient can walk on it.
SYME’S AMPUTATION
INDICATIONS Lesions confined to the forefoot only, whenthe operator is fairly skilled.
CONTRAINDICATIONS (1) Arterial disease, unless this isstrictly confined to the distal part of the foot. One and prefer-ably both ankle pulses should be present. (2) The need foran elegant prosthesis. A woman is likely to prefer a belowknee amputation. (3) Infection. Syme’s amputation has a
SYMESAMPUTATION
working in herekeeping closeto bone
Achilles tendoncutting the
plantarflexed
furtherplantarflexed
still furtherplantar flexed
sawing across thelower end of the tibia
2
3
456
78
9
1011
12
13 14
A B C D
GF
H
I
E
Fig. 56.14: SYME’S AMPUTATION. Fig. 56-14 SYME’S AMPUTA-TION. A shows the incision and B, the completed stump immediately aftersuture. C, shows how the stump can be held in place with strapping post-operatively. Ultimately, the stump should look like D. E, the patient’s anklejoint has been exposed and its ligaments cut. F, his foot has been furtherplantar flexed and its Achilles tendon is about to be cut. G, extreme flexionallows his calcaneus to be dissected out of its surrounding tissues subpe-riosteally. H, the lower end of the tibia is being sawn through. I, showsa cross section of his ankle joint with the tibialis anterior tendon (1), thegreat saphenous vein (2), the tibialis posterior tendon (3), the flexor digito-rum longus tendon (4), the tibial nerve (5), the posterior tibial artery andvein (6), the plantaris tendon (7), the Achilles tendon and its overlyingbursa (8), the small saphenous vein (9), the flexor hallucis longus tendon(10), the peroneus longus and brevis tendons (11), the extensor digitorumtendon (12), and the tendon ofextensor hallucis tongus (13). After Campbellwith kind permission.
special posterior flap and is not suitable for delayed primaryclosure. (4) A very inexperienced operator. (5) This is not a
11

56 Amputations
good amputation for leprosy.METHOD For the general method, see Section 56.1. Ap-
ply a tourniquet to the patient’s thigh (3.8), and let his anklehang over the end of the table. Stand at the end of it facinghis foot.
Mark out the flaps with methylene blue. Hold his ankle at90◦. Start the incision at the distal tip of his lateral malleolus.Bring it over the front of his ankle, level with the distal end ofhis tibia to a point one finger’s breadth inferior to the tip of hismedial malleolus. Then, bring the incision under the sole ofhis foot to the tip of his medial malleobus. Cut all structuresdown to the bone.
Forcibly plantar flex his foot and cut all anterior structuresdown to the bone. Put a knife into his ankle joint between hismedial malleolus and his talus and cut his deltoid ligament.Do the same on the lateral side and cut his calcaneofibularligaments.
Put a bone hook posteriorly in his talus to plantar flex hisfoot even more.
Using a new, sharp scalpel blade, dissect the tissuesaway from the medial and lateral sides of his talus and cal-caneus, keeping as close to the bone as you can, f possiblewithin the periosteum. Then cut his calcaneus out of hisheel. Work at it from all sides keeping very close to thebones. When you get tired of one approach, start from an-other. This is the most difficult and the most critical part ofthe operation.
Pull his talus and calcaneus forward with a bone hook.Dissect posteriorly, and cut the posterior capsule of his ankleand his Achilles tendon. Then dissect subperiosteally roundthe ball of his heel, so as to free his calcaneus and reach thefirst incision on his sole. As you do so, steadily dislocate hisfoot downwards more and more, until you reach the distalend of the plantar skin flap and finally free it from his ankle.
CAUTION! (1) Keep within the periosteum very close tothe bone: as you dissect his calcaneus out of his heel flap,or you will cut his posterior tibial and peroneal arteries whichare very close to the back of the joint capsule. If necessary,remove his calcaneus piece by piece. (2) Don’t trim awayany muscle or fat in the heel pad, because he needs it towalk on. (3) Keep close to the bone, and don’t button holethe heel flap.
Remove his whole foot except for the heel flap.Dissect the heel flap from his malleoli, and reflect it pos-
teriorly. Saw off his malleoli and the articular cartilage of histibia in a single cut. Make sure that the ends of his tibia andfibula are accurately horizontal, so that he can bear weightsquarely on the stump.
CAUTION! (1) The cut surfaces of his bones must parallelto the ground when he stands. (2) If you are amputating in achild, don’t destroy his distal tibial epiphysis.
Round and smooth all the sharp corners of his tibia andfibula. Cut his medial and lateral plantar nerves proximally.
Pull on any tendons you can see, cut them and let themretract proximally into his leg.
Tie and cut his posterior tibial artery and vein just proximalto the cut distal edge of the heel flap. Tie his anterior tibialartery in the anterior flap.
Using a step incision cut his Achilles tendon about 10 cmproximal to the heel flap. This will prevent the heel stumpdisplacing. If you don’t do this, his Achilles tendon is apt topull up the back of the stump. Cut it high up, or you mayinjure his posterior tibial vessels.
Release the tourniquet, and control bleeding. Bring hisheel flap forward to cover the ends of the bones.
CAUTION! (1) Don’t remove the dog ears, however big.They carry an important share of the flap’s blood supply andwill disappear later. (2) Prevent the heel pad from tilting outof alignment with the patient’s tibia-this is a real disaster!Apply two long U–shaped strips of strapping as in C, Fig. 56-14. Put the first piece on starting below his knee posteriorly,bring it round the flap, and then anteriorly, so as to flex theflap over the stump. Apply the second strip from one side tothe other. Keep these strips in place for at least three weeks,and replace them as necessary.
POSTOPERATIVE CARE FOR A SYME’S AMPUTATION
Check the strapping daily, to make sure that the patient’sheel pad is centred over his tibia. Adjust it if necessary.
At 2 weeks reapply the strapping, and put on a wellmoulded cast round the stump. He should not bear weightyet.
At 6 weeks take the mould for the prosthesis. By now thestump has usually stuck firmly enough to the tibia to bearweight inside a cast, so apply a new one and let him bearweight on it.
At 10 to 12 weeks he is ready for his definitive prosthesis,either an elephant boot, or a more sophisticated one.
56.10 Amputating through the foot and toes
This is one of the less useful amputations, its main use is incrush injuries of a patient’s toes. Its advantage is that if hefills the front of his shoe with cotton wool, he can walk rea-sonably well without a prosthesis. Try to preserve as muchof his metatarsals as you can. If you cannot preserve them,do a Syme’s amputation, or amputate below his knee. If nec-essary, you can amputate as far back as their bases. Don’t tryto amputate through his tarsus, because the stump will tilt.If you can preserve his dorsiflexors, he will have a reason-able stump, if you lose them, his foot may go into plantarflexion.
Amputating through the metatarsals is sometimes indi-cated in leprosy with very distal ulcers under the heads ofthe metatarsals. It is a poor amputation for arterial gan-grene, which usually needs an amputation below the knee,or even above it.
Amputate toes in the same way as the fingers (75.24). Pre-serve a patient’s big toe, if you can, because it has consider-able functional value, particularly in the ’take off’ of nor-mal walking. Its most important part is the head of the firstmetatarsal, so preserve this if you can, even if it does meancobbling up the remains of an injured foot. The distal pha-lanx of the big toe matters much less.
Amputating a patient’s second toe soon causes severe hal-lux valgus, but amputating his third, fourth and fifth willcause him little disability.
AMPUTATING THROUGH THE FOOT AND TOES
METATARSAL AMPUTATION
INDICATIONS (1) Crush injuries of the patient’s toes. (2)Occasionally, in leprosy when there are large and persistentulcers due to osteitis. (3) Gross infections presenting latewith osteitis.
12

56.10 Amputating through the foot and toes
METATARSALAMPUTATION
B
E
C
A No!
don’t do this amputation if apatient’s toes are gangrenous
longerplantarflap
to do thisamputation, one and preferably bothpulses must bepresent
D
Fig. 56.15: METATARSAL AMPUTATION. This is one of the less usefulamputations, its main use is in crush injuries of a patient’s toes. After Roband Smith with kind permission.
CONTRAINDICATIONS The risk of failure is considerableif his toes are gangrenous, particularly if he is diabetic.
METHODS For the general method see Section 56.1.Make a long plantar and a short dorsal flap, as in Fig. 56-15. This will bring the suture line dorsally.
Start the dorsal incision at the site of bone section onthe anteromedial aspect of the patient’s foot. Curve it dis-tally a little to reach the midpoint of the lateral side of hisfoot. Take the plantar incision distally beyond his metatarsalheads 1 cm proximal to the crease of his toes. The foot isthicker medially, so make the flap slightly longer on the me-dial than on the lateral side.
Cut the plantar flap to include his subcutaneous fat and athin bevelled layer of his plantar muscles. Reflect the plantar flap proximally to the site of bone section and then uselarge bone cutters to divide his metatarsals. Find the nervesand cut them well proximally. Pull the tendons and cut themso that they retract into the stump of his foot.
Release the tourniquet, control bleeding, drain and closethe stump as usual (56.1).
TOE AMPUTATIONS
Amputating the big toe
Amputating the third toe Amputating the last four toes
DC
B
No! Don’t amputate the second toeA
Fig. 56.16: TOE AMPUTATIONS. A, avoid amputating the second toe ifyou can. B, amputating the big toe. C, the incision for amputating the 3rdtoe. D, amputating the stumps of the last four toes. Partly from TechniquesElementaires pour Medecins Isolé, with kind permission.
AMPUTATING AT THE BASE OF A PROXIMALPHALANX
The big toe Make a long posteromedial flap. Start the in-cision at the base of the patient’s big toe in the midline dor-sally. Curve it distally over the medial side of his toe for a dis-tance slightly greater than its dorsoplantar diameter. Thenbring it proximally across the plantar surface. Section hisflexor and extensor tendons and suture them together overthe end of the bone to maintain the position of the sesamoidsunder the head of his first metatarsal.
Alternatively, some surgeons make a ’V’ or a ’Y’ on themedial side of the foot.
Second toe. Avoid amputating this.
The remaining toes. Make a short dorsal racquet incision,proceed as in the corresponding amputation in the hand.
PLAN FLAPS LONG, YOU CAN ALWAYS SHORTEN THEMLATER
13
![Lower Extremity Amputation and Leg Blood Flow€¦ · leg amputation [1-3]. In general, exercise therapists commonly recommend resistance training for subjects with amputation below](https://img.pdfslide.us/doc/110x75/6013975e90eb0d4e6520c0db/lower-extremity-amputation-and-leg-blood-flow-leg-amputation-1-3-in-general.jpg)