Embed Size (px)
Citation preview

GYNECOLOGIC CANCER INTERGROUP (GCIG)
Cervix Cancer Committee
Friday, June 3, 2016, 10:30 am – 12:30 pmLaSalle I Room, DoubleTree Hotel, Chicago
Chair: Satoru Sagae Co-Chair: Brad Monk
Harmonization Liaisons: Hiltz/Keller (Ops), Reuss (Stats)

PUBLISHED/IN PREPARATION:
Advances and Concepts in Cervical Cancer Trials: A Road Map for the Future.Sagae S, Monk BJ, Pujade-Lauraine E, Gaffney DK, Narayan K, Ryu SY, McCormack M, Plante M, Casado A, Reuss A, Chávez-Blanco A, Kitchener H, Nam BH, Jhingran A, Temkin S, Mileshkin L, Berns E, Scholl S, Doll C, Abu-Rustum NR, Lecuru F, Small W Jr; Gynecologic Cancer InterGroup Cervix Cancer brainstorming day.
Int J Gynecol Cancer. 2016 Jan;26(1):199-207.
CLOSED TRIALS: ( 3 minutes)RTOG (GOG) TIME-C IMRT study in endometrial or cervical cancer

CURRENT ACTIVE RANDOMIZED TRIALS WITH GCIG PARTICIPATION: 40 min.( 3-5 minutes each)
Surgery plus Radiation +/- CT1. KGOG 0801 (GOG, RTOG) Post-Op RT vs CCRT (intermed.risk post op)
Ryu 185->200->220/480
Chemoradiation2. KGOG-THAI TACO (CCRN) (RTOG, GICOM, VietNam, + )
Ryu 168->200->210/5003. ANZGOG OUTBACK (CCRN) (GOG, RTOG, + )
Mileshkin 558 ->656->750/780->9004. MRC-NCRI INTERLACE (CCRN) (GICOM, MaNGO, + )
McCormack 60-> 89->129 /770

Minimal Invasive Surgery
5. (NCIC) CCTG SHAPE (CCRN) (DGOG, + )
Plante 81 -> 113->178/700
6. G-GOC ConCerv
Ramirez 77/100
7. G-GOC LACC
Ramirez 380 -> 405->443/740
8. GOG 0278 Conservative surgery (cone/nodes or hyst/(nodes) in early stage
cervical cancer. (evaluation of physical function and QOL) Monk 110 /220
Immunotherapy
9. GOG high risk maintenance (ADXS-HPV) immunotherapy Monk move to phase III
Vulvar Cancer
10. GOG 0279 Phase II Trial Evaluating Cisplatin and Gemcitabine Concurrent with IMRT in Treatment of Locally Adv. SCC of the Vulva Monk 50/52 almost closed
11. DGOG GROINSS-V II (EORTC-GCG, GOG) van der Zee
1653pts enclosed 80% SN negative SN positive n=370 ( <2mm+ n=180) 0.025% recurrence

NEW/PROPOSED/DEVELOPING CONCEPTS(seeking groups):
1. RTOG Hypofractionation Jhingran/Small/Gaffney
2. (NCIC) CCTG Neo-adj. CT & fertility sparing surgery (stage IBI) Plante
3. NOGGO Sentinel lymph node biopsy Survey status Keller/Sehouli
4. GINECO SENTICOL-III A prospective obs. trial on sentinel lymph node mapping in patients with early stages cervical cancer Lecuru,Plante,Abu-Rustum
5. EORTC-GCG CURE-C Curative Radiotherapy to the primary tumor vs. best supportive care in initially metastatic cervical cancinoma Ottevanger
6. ANZGOG EXCISE – EXcisional treatment Comparison for In Situ Endocervical adenocarcinoma
Brand/Mileshkin
7. Management and Care of Women With Invasive Cervical Cancer:American Society of Clinical Oncology Resource-Stratified Clinical Practice Guideline
JGO – Journal of Global Oncology Chuang/Berek

Hypofraction Trial For Cervical Cancer
45 Gy/25 fractions37.5 Gy/15
fractionsVS.
Brachytherapy schedule – up to the site
Endpoints: RFS and Patient reported Outcomes

Stage IB1 (2-4 cm) Cervical cancer treated with Neoadjuvant chemotherapy followed by
fertility Sparing Surgery (CoNteSSa)
Marie Plante (CCTG)
Jeffrey Goh & Vivek Arora (ANZGOG)


Radical hysterectomy

Outcome measures
• Primary end point• Successful fertility preservation defined as intact uterine corpus with no adjuvant XRT
• Secondary end points• Response rates to chemotherapy
• Toxicity
• Recurrence rate
• 3 and 5 year disease free survival
• Proportion requiring trimodality treatment
• QoL indices
• Ovarian function indices
• Obstetrical outcome
10

Statistics and design
Single arm phase-2 type of study (75 patients)
Two statistical issues
- Fertility preservation (realistically 50-60%)
- assuming a 30% suboptimal response to NACT
- assuming a 10-20% high-risk features in the trachelectomy specimen requiring rad hyst or RT
- Recurrence rate: Safety monitoring guidelines
- DSMC requirements
- Based on literature: relapse rates for standard Tx
- Based on accrual11

Feasibility
- This study is doable within the GCIG
- Already an established large international and successful collaboration with numerous groups through SHAPE
- Great interest for this study concept
- We need strong support
- Accrual and funding from all interested groups
12

International survey about the sentinel lymph
node biopsy in cervical cancer
Survey within the GCIG
On behalf of the working group
Jalid Sehouli, Filiberto Vercellino, Marie Plante, Nadeem Abu-
Rustum, Fabrice Lecuru, Stefano Greggi

Group or Country Number of filled in
Questionnaires
AGO-AUST / Austria 6
AGO, NOGGO / Germany 32
BGOG / Belgium 14
DGOG / Netherland 1
GEICO / Spain 26
G-GOC, GOG / US 4
GINECO / France 12
Japan 6
KGOG / Korea 2
MITO, MaNGO / Italy 4
NCIC CTG / Canada 12
Great Britain 2
Switzerland 2
ANZGOG / Australia 1
NSGO / Norway, Denmark, Sweden, Finland 11
ISGO / Israel 5
GICOM /Mexico 2
Groups without country specification 24
Sum 166

Q35 Would you support international study
concepts about the role of SLNB in the
management of CC?
• 120 of 124 said yes
• 3 of 124 said no
• 1 of 124 is not sure

Cervix cancer committee
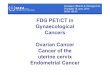
SENTICOL III: International prospective validation
trial of sentinel node biopsy in cervical cancer
A Gynecologic Cancer interGroup (GCIG) trial, lead by the GINECO
F Lecuru, N Abu-Rustum, P Mathevet, M Plante.

Objectives
Main objective:
« co-primary » disease free survival and health related quality of life non-inferiority of SLN biopsy vs lymphadenectomy for DFS
superiority of SLN biopsy for QoL
The hypothesis is that SLN biopsy alone provides similar survival and better quality of life.
Secondary objectives:- Longitudinal and other dimensions of health related Quality of life.
- Surgical morbidity and mortality.
- Evaluation of mapping with Indocyanine green (ICG).
- Outcome of patients with ITC and micrometastases.
- Positive and negative predictive values of SLN biopsy.
- Outcome of pN1 patients according to the size of metastasis and treatment.
- Overall survival.
- Recurrence free survival.

Schema
SCC/Adk
Stage≤IIa
<40mm
No pregnancy
SLN biopsySLN biopsy
Cormier algorithm
No dissection if neg
SLN biopsy
+ PLN Dissection
Qualit
y o
f lif
e
Dis
ease f
ree s
urv
ival
pN0
pN0
Randomized study
Surgical quality assurance

Inclusion criteria:
- Squamous or adenocarcinoma of the cervix (proven by biopsy or cone biopsy)
- Stage Ia1 with lymphovascular emboli to IIa1 (clinical stage)
- Maximum diameter ≤40mm on MRI
- No suspicious node on pelvic and abdominal MRI (small axis ≥ 8-10mm and
morphologic criteria)
- Informed consent given
Exclusion criteria:
- Age <18 years
- Pregnancy
- Previous pelvic of abdominal cancer
- Previous chemo and/or radiation therapy for the cervical cancer
- Allergy to blue dye, isotope or Indocyanine green

Statistics
1-DFS With a 3 years-disease free survival of 85% to demonstrate a non-inferiority of SLN biopsy vs SLN
biopsy + lymphadenectomy with a non-inferiority margin of 5% (80 vs 85%, HR = 1.373). With a unilateral alpha error of 5%, and a power of 80%, 900 patients in 3 years, with 5 years of follow-up should be included to observe the required 263 events. An interim analysis is planned when at least 110 events will be observed to reject H0 or H1 using O Brien Fleming and alpha spending function.
2-HRQoL We target 3 HRQoL dimensions global health, pain and physical functioning of EORTC QLQC 30.
To demonstrate a superiority of at least one of the 3 targeted dimensions without significant deterioration in at least one with a minimal important difference in mean score of at least 5 points (SD: 20), and a bilateral alpha type one error of 0.015 (Bonferroni adjustment) it would be required to have 815 patients with available HRQoL scores to reach 85% statistical power.
900 patients have to be randomized
An international collaboration is requested

CUrative Radiotherapy to the primarytumor vs. bEst supportive care in
patients with initially metastatic Cervicalcarcinoma (CURE-C trial)
Igor Sirák, M.D., Ph.D
Department of Oncology and Radiotherapy
University Hospital
Hradec Králové
Czech Republic
EORTC ROG-GCG-QLG
Fernanda G. Herrera, M.D.
Lausanne University Hospital
Department of Oncology – Radiotherapy Service
University of Lausanne
Switzerland
Study coordinator Joint study coordinator

Inclusion criteria
• Histologically confirmed cancer of the uterine cervix
• Stage IVB metastatic disease
• No clinical evidence of brain metastases
• Presence of untreated primary cervical carcinoma
• No need for urgent upfront radiotherapy for life threating symptoms
• No previous RT treatment in the pelvis or para-aortic area
• No prior history of Crohn’s disease, ulcerative colitis; or other chronic bowel disease
• Performance status 0-2
• Life expectancy ≥ 6 months
• Adequate hematological formulae

Phase II randomized trial
R A N D O MI Z A T I O N
RTPLATINUM-BASEDCHT 4x (+/- BEV)
BSC: including palliative RT up to 40Gy BED2 in case of symptomatic progression, 2nd line CHT, etc.
S T A N D A R D A R M
E X P E R I M E N T A L A R M

Endpoints
Time to progression
Quality of life (A Translational part of the research)
Overall Survival
Treatment toxicity
Evaluation of treatment feasibility in a multi-institutional setting
Response to initial chemotherapy by RECIST criteria: CR, PR vs. SD
Performance status
Bevacizumab yes/no
Primary:
Secondary:
Stratification factors

Statistics
Due to the variability of the BSC, a comparative phase II design is proposed
As proposed by Korn et al (JCO 2001), a phase II comparative screening design can be implemented as a superiority phase III trial design with an increased type I error and optimistic treatment effect
For this trial, using a one sided log-rank test at a level of significance of 10% (alpha), to test for a HR=0.63 (increase from 50% to 65% event-free survival at 12 months) at 80% power would need about:
• 80 events ~100 patients in 1:1 randomization.
The event-free curves between the two arms will be compared with a non-parametric test stratified for the stratification factors
With the above assumptions, a hazard ratio of minimum would need to be observed 0.75 to reach significance

EXCISE – EXcisional treatment Comparison
for In Situ Endocervical adenocarcinoma
Excisional treatment in women with cervical adenocarcinoma-in-
situ (AIS): a prospective randomised controlled non-inferiority trial
to compare AIS recurrence after loop electrosurgical excision
procedure (LEEP) to cold knife cone biopsy (CKC).
P A Cohen, A Munro, J Codde, M
Bulsara, C D H Wrede, McNally O M,
Sykes P, Eva L, Rao A, Symcock B,
Brand A
3 June 2016

Loop electrosurgical excision
procedure (LEEP)
Against LEEP
• Incomplete excision
• Thermal artefact
• Greater risk of a positive
endocervical margin
In favour of LEEP
• Avoid general anaesthesia
• Outpatient setting
• Lower morbidity, and reduced
rates of obstetric complications

EXCISE
• Aim: to determine if the treatment of cervical AIS by LEEP is non-inferior to CKC
with regard to 5-year recurrence rate in women managed conservatively
• Hypothesis: LEEP will not be inferior to CKC with regard to AIS persistence and
recurrence in conservatively managed women
• Primary objective: to compare the 5-year recurrence rate of cervical AIS following
LEEP to that after CKC, in conservatively managed women.

Procedures
• Randomization:
Randomization will be 1:1 (CKC: LEEP). Sequence generation will be by
computer with no blocking or stratification.
• Blinding:
Study investigators and participants will not be blinded to the
intervention. Those conducting data analysis will be blinded to the
intervention.

Sample Size• Estimated using a 2 group test of non-inferiority of proportions
• Primary end point is the AIS recurrence rate at 5 years and the
comparison will be between CKC and LEEP, based on a 1-sided
test for non-inferiority
• Assumes an 8% rate of AIS recurrence at 5 years after CKC, and a
5% non-inferiority margin (upper 95% confidence rate of AIS
recurrence of 13% is still within the non-inferiority margin).
• Sample size needed is 730 (365 per group). Assuming a 10%
drop-out rate, a total sample size of 810 participants (405 per
group) would need to be randomised. (One-sided Type I error is
set at 5% with 80% power. )

www.asco.org/rs-cervical-cancer-treatment-guideline ©American Society of Clinical Oncology 2016. All rights reserved.
Management and Care of Women with Invasive Cervical Cancer: American Society of Clinical Oncology Resource-Stratified Clinical Practice Guideline
Chuang L, Temin S, Camacho R, Duennas-Gonzalez A, Feldman S, Gluten M, Gupta V, Horton S, Jacob G, Kidd E, Lishimpi K, Nakisige C, Nam J, Ngan H, Small W, Thomas G, Berek J Journal of Global Oncology May 25, 2016.

Treatment CapacityTreatment Setting
Basic Limited Enhanced Maximal
Surgery Simple (extrafascial) hysterectomy or more
extensive hysterectomy can be performed*
*Where medical facilities exist to take care
of women who are at high risk for
postoperative complications
Modified radical and radical
hysterectomy
Capable of performing most major
surgeries, including radical
hysterectomy, radical trachelectomy,*
pelvic and para-aortic LN sampling,
and pelvic exenteration*
Following are not available: PET scan,
interventional radiology, sentinel node
biopsy/IORT, and bevacizumab
*Can be performed in some enhanced
levels
Radical hysterectomy, radical
trachelectomy, pelvic and para-
aortic LN sampling, sentinel
node biopsy, and pelvic
exenteration; radiation therapy,
chemotherapy, interventional
radiology, palliative care
service, and bevacizumab are all
available
Chemo-therapy Availability of chemotherapy drugs is
unpredictable
Chemotherapy may be
available
Chemotherapy available; bevacizumab
not available
Chemotherapy available;
bevacizumab is available
Radiation therapy No radiation therapy available Limited external RT with no
brachytherapy available; in
some areas where there are
only brachytherapy and no
external RT, this will be
considered as basic level
RT including external beam and
brachytherapy available; interventional
radiology not available
RT including external beam and
brachytherapy available;
interventional radiology
available
www.asco.org/guidelines/rs-cervical-cancer-treatment-guideline©American Society of Clinical Oncology 2016. All rights reserved.

Recommendations for Stage IB and IIA Disease
Type of
Disease
Setting
Basic Limited Enhanced Maximal
IB1, Non-
FSExtrafascial
hysterectomy
Radical hysterectomy plus PLND or radical hysterectomy (see Note)
with adjuvant RT or RT with concurrent low-dose chemotherapy
(concurrent chemoRT), if needed
Radical hysterectomy plus
PLND
Radical hysterectomy plus PLND;
may offer SLN
NACT if available, then
extrafascial
hysterectomy
ChemoRT or RT followed by extrafascial or radical hysterectomy
(see Note) ± PLND ± PANB*
If no RT is available but chemotherapy is available, NACT may be used
to shrink the tumor to make it removable by surgery (extrafascial or
modified radical hysterectomy [see Note] ± PLND ± PANB*)
Pelvic RT plus
brachytherapy plus
concurrent low-dose
platinum-based
chemotherapy
Pelvic RT plus brachytherapy plus
concurrent low-dose platinum-
based chemotherapy
Note Wherever radical hysterectomy with concurrent chemoRT listed as a
surgical option above, extrafascial hysterectomy is recommended if
there is residual disease after RT or chemoRT with a boost of 64-68
Gy or initial tumor > 6 cm.
Radical hysterectomy may be used following RT or chemoRT to a
dose of 50 Gy
www.asco.org/guidelines/rs-cervical-cancer-treatment-guideline©American Society of Clinical Oncology 2016. All rights reserved.