Embed Size (px)
Citation preview

Neurosurgical
Cervical spine disease and anaesthesiaian calder
AbstractThe cervical spine is obliged to support and manoeuvre the heavy
weight of the head (about 6 kg) throughout life. it is not surprising
that arthritic and traumatic processes are common in this spinal region.
stenosis of the spinal or root canal is the most frequent reason for
surgery. instability is a vague term, with many grades of severity and
clinical import. excluding instability in unconscious patients is a common
icu problem. The cause of neurological deterioration during anaesthesia
is uncertain. airway management will remain under suspicion, but pro-
longed minor deformity of the cord and relative hypotension are prob-
ably to blame. Difficulty with direct laryngoscopy is frequent, particularly
with upper cervical spine lesions. it is difficult to identify reduced cranio-
cervical junction movement by clinical examination. airway obstruction
due to swelling of the tissues of the neck is an important complication
of anterior cervical surgery. eye damage, particularly corneal abrasion,
must be avoided by obsessive care of the eyes.
Keywords cervical spine; intubation; spinal cord injury; tracheal
Surgery for disease of the cervical spine
Surgery for disease of the cervical spine is performed mostly for the relief of stenosis, and to ensure stability. Discs and osteo-phytes can be approached anteriorly (anterior lesions above C2 may require a mandibular split) with the patient placed supine. However, lesions at multiple levels may require laminectomy or laminoplasty (with or without pedicle-screw fixation to prevent instability), which requires the use of the prone position, with the head held in pin fixation. The sitting position is occasionally required for grossly obese patients, or for those with a marked flexion deformity.
Neurological deterioration during cervical spine surgeryThis is clearly the major concern for all involved. Accepted risk factors are:1
• myelopathy present before operation• instrumentation (screws/rods)• high cervical level• multiple-level surgery.
The risk imposed by anaesthesia is very difficult to estimate. Nevertheless, being anaesthetized imposes a risk. There are a considerable number of reports of thoracic cord or cauda equina
Ian Calder, FRCA, is Consultant Anaesthetist at the National Hospital for
Neurology and Neurosurgery, Queen Square, London.
aNaesTHesia aND iNTeNsiVe care MeDiciNe 9:6 22
injury during non-spinal surgery in patients with spinal stenosis.2 It seems likely that these injuries result from impaired cord per-fusion due to prolonged minor malposition and hypotension. It should be remembered that there are several reports of cord dam-age in normal spines following prolonged deformation.3 Spinal stenosis increases the risk (instability might be regarded as ‘just’ another cause of stenosis). There is almost certainly a tendency to blame airway management in cases of cord damage in the cer-vical region, which had they occurred at a thoracic level would have been ascribed to malposition and/or hypotension.4,5 It is very difficult to find a convincing report of cord damage due to airway management.2 However, that does not mean that airway management does not cause cord injury, or that we can relax our attempts to reduce risk. High-risk cases comprise: patients with pre-existing myelopathy; patients known to have severe spinal canal stenosis (Figure 1); and patients with marked or potentially marked instability (Figure 2).
Anaesthetic management of high-risk cases
The hazards to the spinal cord imposed by anaesthesia can be summarized as either a ‘quick crunch’ during airway manage-ment or positioning, or a ‘slow squeeze’ due to a combination of minor malposition and relative hypotension during lengthy surgery (Figure 3).
The objective must be to place the patient in a position, which is the best compromise between surgical access and comfort. This may be best achieved by awake intubation and positioning, and with currently available drugs and techniques (remifentanil sedation and flexible fibre-optic intubation) this is generally easy to achieve. However, awake intubation and positioning is not a panacea, since severe complications, including airway-related death can occur,6 and there is no evidence that a better neuro-logical outcome results.7 A patient’s best interests are unlikely to be served by practitioners adopting an unfamiliar technique. Practitioners must also consider what their response will be, if having positioned a patient, there appears to be a neurological
Figure 1 spinal
stenosis due to
osteophytes at
c3/4.
7 © 2008 elsevier ltd. all rights reserved.

Neurosurgical
deterioration. Cases have been reported where surgery eventu-ally went ahead after repeated cancellations.
An alternative approach is to use cord monitoring (sensory evoked potentials or motor evoked potentials) as a guide to cord perfusion. However, it is often impossible to obtain potentials in patients with preoperative myelopathy, and cord injury can occur undetected by potential monitoring. Nevertheless, because evoked potentials are sensitive to hypotension, they are seen by most as a valuable guide to adequacy of perfusion. Whether evoked potentials are available or not, it is wise to maintain a good per-fusion pressure, although what constitutes ‘good’ is debatable. This often entails inotrope infusion. Drugs such as metaraminol or phenylephrine, which can be given peripherally, are useful.
Emergency airway management
There is currently no evidence that competently performed direct laryngoscopy is neurologically dangerous. Manual in- line stabilization (MILS) is currently routinely applied during direct laryngoscopy, although there is no evidence that it makes any difference to outcome.7 Many studies have compared cervical spine angulation during direct (Macintosh) laryngoscopy with other techniques, such as fibre-optic endoscopy, laryngeal mask airway (LMA), intubating laryngeal mask airway (ILMA), light wand, Bonfils, Glidescope, and Bullard. These studies have shown that angulation of the spine is greater with Macintosh laryngo-scopy than with the alternatives, but intubation is achieved more quickly with the Macintosh. Two points can be made about these studies. First, they have all ignored the advice of Nolan and Wilson that only the amount of glottic exposure required to insert a gum-elastic bougie should be sought during laryngoscopy.8 If this option had been included in the protocols of the studies, significant differences in angulation may not have been found. Second, studies of movement in cadaver models of cervical in-stability have found that basic life-support manoeuvres, such as jaw thrust, produced greater reductions in the space available for the cord than direct laryngoscopy.9 If this is the case in vivo it can be argued that the method chosen for intubation is of lesser significance than care with basic life support.
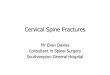
Figure 2 Fracture of the axis vertebra.
aNaesTHesia aND iNTeNsiVe care MeDiciNe 9:6 2
The airway must always take precedence, and in emergen-cies practitioners should adopt the technique that best suits their competencies. Anaesthetists who are competent only in direct laryngoscopy should not undertake elective cervical spine anaes-thesia because difficult laryngoscopy is common. There are sev-eral very useful items of equipment available to aid intubation, but the flexible fibre-optic laryngoscope remains the most gener-ally useful device.
Difficult airway management in cervical surgery
Causes of difficulty: cervical diseases such as Klippel–Feil syndrome, rheumatoid arthritis and ankylosing spondylitis are well-known causes of difficulty. Any modality of airway man-agement may be difficult, but it is mainly problems with direct laryngoscopy that concern anaesthetists because most cervical spine surgery requires tracheal intubation. In general, the very difficult cases are obvious.
Cord injury during anaesthesia: quick crunch or slow squeeze
The spectrum of belief about the causation of cord damage during
anaesthesia can be represented as ranging from the consequences
of catastrophic cord compression during airway management to
the eventual effect of relatively slight pressure applied for a long
time, such as during prolonged deep sleep, aggravated by relative
hypotension. The top illustration is reproduced with permission,
from Hirsch NP, smith gB, Hirsch Po. alfred Kirstein. Pioneer of
direct laryngoscopy. Anaesthesia 1986; 41: 42–5.
Figure 3
28 © 2008 elsevier ltd. all rights reserved.

Neurosurgical
Difficult laryngoscopy is much more frequent when the occipito-atlanto-axial complex is involved. This is partly because of the effect of impaired cranio-cervical junction extension and partly because there is an association with temporo-mandibular joint dysfunction.10 The detection of impaired cranio-cervical movement by clinical examination is problematic. This may be due to compensatory increases in movement at cervical joints below the cranio-cervical junction, so that the total range of cranio-cervical movement is not particularly abnormal.11 Mouth-opening ability appears to be the best clinical indicator of difficulty. This is partly because of the association of temporo-mandibular joint disease and partly because of the inhibitory effect of cervical spine immobility on mouth-opening.10,12 Poor protrusion and/or an interdental distance of less than 3 cm sug-gest that cranio-cervical extension may be impaired.
Examination of radiological investigations is always worth while. Reduced cranio-cervical mobility can be inferred from a poor separation of the posterior elements of the occiput, atlas and axis vertebrae, or evidence of involvement of the cranio- cervical junction by a disease process.10
Postoperative airway obstruction: airway obstruction is not uncommon after anterior cervical surgery. A haematoma may be present, but in many cases obstruction is due to tissue swelling. It usually presents within 6 hours but can occur later. Airway obstruction is particularly likely after combined anterior–posterior cervical surgery, especially if the anterior surgery occurs before the posterior procedure. Such patients should not be extubated until it is clear that the airway is unobstructed.There are some important diagnostic points:• stridor is unusual – the obstruction is due to swollen tissue in
the supra- and peri-glottic regions• patients say they ‘can’t breathe’ and want to sit up• oximetry may return almost normal values until very late• the presence of a drain in the neck does not prevent swelling.The priority is to open the wound, which may relieve tissue tension enough to restore an airway. Re-intubation may be diffi-cult due to gross swelling of the soft tissues in the pharynx. These patients may have to be managed in a semi-sitting posture. Awake fibre-optic intubation is sometimes a good option, but swelling may render it impossible. Direct laryngoscopy after sevoflurane and oxygen induction is the traditional approach, but in the author’s experience induction with maintenance of spontaneous respiration has not been successful. Positive pressure has been required to achieve airway patency, and propofol and muscle relaxation have been helpful. The gum-elastic bougie is a vital aid and LMA/fibre-scope/tracheal tube/Aintree catheter/ILMA techniques have all proved useful. The use of suxamethonium in myelopathic patients is hazardous because of abnormal potassium shifts.
‘Clearing’ the cervical spine in suspected injury
One-quarter to half of patients with a traumatic cervical spine injury have an associated head injury. Therefore, a common dilemma is the need to confirm or exclude a cervical injury in an unconscious patient.13 Table 1 summarizes current practice in the UK.
Neurological deterioration following a traumatic cervical spine injury is a worrying and not well-understood phenomenon.
aNaesTHesia aND iNTeNsiVe care MeDiciNe 9:6 2
Approximately 5% of patients admitted with traumatic cer-vical injury will deteriorate neurologically. Most deteriorate early (24 hours), some are delayed (1–7 days), and occasion-ally patients undergo late deterioration (weeks; subacute post- traumatic ascending myelopathy).
Airway obstruction due to bilateral recurrent laryngeal nerve palsy is rare, but unilateral nerve damage is seen from time to time and causes a ‘lowing’ cough and a weak voice.
Eye damage during cervical anaesthesia
There are three causes of oculopathy: corneal abrasion; isch-aemic optic neuropathy (ION); and central retinal artery throm-bosis (CRAT). ION and CRAT result in permanent visual loss in most cases.
Corneal abrasion: most ‘abrasions’ are hypoxic injuries follow-ing corneal drying due to failure to tape the eye shut. Such abra-sions can take many months to heal. Ocular contamination by skin-prep fluids is a hazard in prone patients.
Ischaemic optic neuropathy: although this condition can occur in supine patients (1:64000), it is much more common (1:11000) after prone surgery. Visual loss may be unilateral and is pain-less. Major blood loss, hypotension and prolonged surgery are associated with ION, but it can occur after short, bloodless surgery without hypotension. Reduced nerve perfusion due to increased orbital and intra-ocular pressure in the prone position is believed to be the cause.14 Diabetes, hypertension and smok-ing are believed to be risk factors. Ophthalmoscopic appearances may be normal if the lesion is posterior, but the disc is swollen and there may be flame-shaped haemorrhages when the anterior portion of the optic nerve is affected.
Central retinal artery thrombosis is the ophthalmological find-ing when external pressure damages the eye but can also be due to emboli from carotid disease. Absent eye movements, proptosis and orbital swelling have been seen in nearly all reported cases. It is currently unclear as to whether CRAT can occur in prone patients without embolism or external pressure. The ophthalmo-scopic appearances are of retinal oedema (‘cloudy swelling’) and
Criteria for stability following cervical trauma
Conscious patient Unconscious patient
alert, no distracting injuries Plain radiographs are
inadequate
No midline pain The combination of plain
radiographs and cT scans is
adequate to diagnose bony
and ligamentous instability
Normal movement Mri scans are not required
for the exclusion of instability
No neurology –
Table 1
29 © 2008 elsevier ltd. all rights reserved.

Neurosurgical
a cherry-red spot at the fovea. The flow in the retinal vessels may be interrupted and emboli visible.
It is essential to prevent external ocular pressure. In prone patients the use of a pin fixation system is the most satisfactory method. The horseshoe headrest should not be used for prone patients. ◆
REFERENCES
1 May DM, Jones sJ, crockard Ha. somatosensory evoked potential
monitoring in cervical surgery: identification of pre- and
intraoperative risk factors associated with neurological deterioration.
J Neurosurg 1996; 85: 566–73.
2 Mccleod aDM, calder i. spinal cord injury and direct laryngoscopy –
the legend lives on. Br J Anaesth 2000; 84: 705–9.
3 Dickerman rD, Mittler Ma, Warshaw c, epstein Ja. spinal cord injury
in a 14-year-old male secondary to spinal hyperflexion with exercise.
Spinal Cord 2006; 44: 192–5.
4 edge cJ, Hyman N, addy V, et al. Posterior spinal ligament
rupture associated with laryngeal mask insertion in a patient with
undisclosed unstable cervical spine. Br J Anaesth 2002; 89: 514–17.
5 Hirose H, akhrass r. Tetraplegia after coronary artery bypass, a rare
complication. Ann Thorac Cardiovasc Surg 2005; 4: 270–2.
aNaesTHesia aND iNTeNsiVe care MeDiciNe 9:6 23
6 Peterson gN, Down KB, caplan ra, et al. Management of the difficult
airway: a closed claims analysis. Anesthesiology 2005; 103: 33–9.
7 crosby eT. airway management in adults after cervical spine trauma.
Anesthesiology 2006; 104: 1293–318.
8 Nolan JP, Wilson Me. orotracheal intubation in patients with
potential cervical spine injuries. an indication for the gum elastic
bougie. Anaesthesia 1993; 48: 630–3.
9 Donaldson iii WF, Heil BV, Donaldson VP, et al. The effect of airway
maneuvers on the unstable c1-c2 segment. a cadaver study. Spine
1997; 22: 1215–18.
10 calder i, calder J, crockard Ha. Difficult direct laryngsocopy and
cervical spine disease. Anaesthesia 1995; 50: 756–63.
11 urakami Y, Takennaka i, Nakamura M, et al. The reliability of
the Bellhouse test for evaluating extension capacity of the
occipitoatlantoaxial complex. Anesth Analg 2002; 95: 1437–41.
12 calder i, Picard J, chapman M, et al. Mouth opening – a new angle.
Anesthesiology 2003; 99: 799–801.
13 Morris cg, Mccoy W, lavery gg. spinal immobilization for
unconscious patients with multiple injuries. Br Med J 2004;
329: 495–9.
14 Hunt K, Bajekal r, calder i, et al. changes in intraocular pressure
in anesthetized prone patients. J Neurosurg Anesthesiol 2004;
16: 287–90.
0 © 2008 elsevier ltd. all rights reserved.