Embed Size (px)
DESCRIPTION
cervical neoplasia
Citation preview

O
CaM
Onnpwi7nncn1esiwlcnow
ScTttmmith
FDU
Ra
RGOC5k
0©d
Reviews www.AJOG.org
NCOLOGY
ervical neoplasia in pregnancy. Part 1: screeningnd management of preinvasive disease
ark I. Hunter, MD; Bradley J. Monk, MD; Krishnansu S. Tewari, MDrimnsn
asctmtTdvptmcuP
svtcscf
mchseptpmart
NwHTtwpcicwcduatp
ne percent of the population ofchild-bearing women screened an-
ually for cervical cancer will be diag-osed with cervical intraepithelial neo-lasia (CIN).1 Among the 4 millionomen who become pregnant each year
n the United States,2 between 2% and% (ie, 80,000-320,000) will have an ab-ormal Papanicolaou test during preg-ancy.3-5 Cervical neoplasia (includingarcinoma in situ and invasive carci-oma) is estimated to complicate 1.5 to2 of every 100,000 pregnancies.6-8 Tostablish protocols for cervical cancercreening and the treatment of cervicalntraepithelial neoplasia in pregnancy,e reviewed recently published guide-
ines9-12 and prepared an algorithm spe-ific to the management of CIN in preg-ancy. The evaluation and managementf invasive cervical cancer in pregnancyill be discussed in a separate article.
creening and cervicalytology in pregnancyheoretically, patients may present for
heir first prenatal visit having begun in-ercourse within the last 3 years, or they
ay have had several consecutive nor-al Papanicolaou tests, making them el-
gible to extend the Papanicolaou test in-erval. Younger mothers and those withigher parity are known to have higher
rom the Division of Gynecologic Oncology,epartment of Obstetrics and Gynecology,niversity of California, Irvine, Irvine, CA.
eceived Feb. 3, 2008; revised March 7, 2008;ccepted April 4, 2008.
eprints: Krishnansu Tewari, MD, Division ofynecologic Oncology, Department ofbstetrics and Gynecology, University ofalifornia, Irvine, 101 The City Drive Building6, Room 260, Orange, CA [email protected].
002-9378/$34.002008 Mosby, Inc. All rights reserved.
ooi: 10.1016/j.ajog.2008.04.010
ates of human papillomavirus (HPV)nfection.13,14 It is therefore the recom-
endation of the authors that all preg-ant patients undergo Papanicolaou testcreening at the time of their initial pre-atal exam.Some clinicians may be concerned
bout the placement of a foreign object,uch as the cytobrush, into the cervicalanal. In an attempt to evaluate alterna-ives to this traditional sampling
ethod, 1 randomized trial comparedhe cytobrush with use of a Dacron swab.hey reported an improved yield of en-ocervical cells for the cytobrush (96%s 70%) without any difference in com-lications including bleeding and spon-aneous abortion15; thus, it is recom-
ended that the cytobrush, oromparable combination broom, besed during the collection of a prenatalapanicolaou test.The Papanicolaou test currently has a
ensitivity for detecting high-grade cer-ical neoplasia outside pregnancy of be-ween 70% and 80%.16 Several factorsan complicate the sampling and analy-is of cervical cytology in pregnancy, in-luding the presence of a large ectropion,requent inflammation, and the presence
Cervical cancer screening is an essential comanagement of cervical intraepithelial neopand sufficient information does not exisapproach. The American Society for Colppublished guidelines regarding the evaluatreatment of CIN in this setting. Many tevaluation of abnormal cervical cytology awoman, such as colposcopy, cervical biopsto the pregnant patient with important excepgravid condition and the risk of prematuexisting consensus guidelines in screeningassociated CIN. In the present review, cscreening are reviewed, and data from stud
Key words: cervical cancer, cervical neopl
f confusing decidual cells that are often i
JULY 2008 A
istaken for atypia.17-19 The decidualells, or Arias-Stella reaction, are large,ypervacuolated cells with variablytaining cytoplasm and a large nucleus,xplaining their association with false-ositive results. However, if care is takeno provide the cytologist with a detailedatient history, errors should be mini-ized. Overall, the Papanicolaou test
ppears to have demonstrated an accu-acy in pregnancy that is equivalent tohe nonpregnant patient.3
ormal Papanicolaou testith or without high-riskPV deoxyribonucleic acidhe follow-up of a normal Papanicolaou
est, obtained in the antepartum setting,ould not differ from the nonpregnantopulation. Consistent with the Ameri-an Cancer Society (ACS) and the Amer-can College of Obstetricians and Gyne-ologists (ACOG) guidelines, patientsho have had 3 or more normal Papani-
olaou tests and have not had a history ofysplasia, immunodeficiency, or intero diethylstilbestrol exposure and arebove the age of 30 years could poten-ially forgo the routine postpartum Pa-anicolaou test, to be repeated at 3 year
onent of prenatal care. The diagnosis andia (CIN) during pregnancy are challenging,o allow for a definitive evidence-basedopy and Cervical Pathology has recentlyof abnormal Papanicolaou tests and the
niques traditionally recommended in thethe treatment of CIN in the nonpregnant
nd electrosurgical excision, can be appliedns. The vascular cervix associated with thepregnancy loss mandates deviation fromcervical cancer in pregnancy and treating
ent guidelines regarding cervical cancerof pregnant populations are summarized.
, management, pregnancy
mplast tosctionechndy, atioreforurries
asia
ntervals.
merican Journal of Obstetrics & Gynecology 3

cettuaTtaaswsAifum
tpomstpshpatoostHtwstcsw
bPHanNStmaf
AWteiis
DiAfppcvtfbm
CIpaAarcvtpcsvspfrvrta
npemntaitti
escg
cihwgpoHrlhcctpapss
CCfefwcfigsuistscpp
damawmoletb
Reviews Oncology www.AJOG.org
4
At present, there are no randomizedontrolled trials from which to establishvidence-based guidelines on the rou-ine use of postpartum Papanicolaouests. One randomized trial evaluated these of the postpartum Papanicolaou testt 4, 6, or 8 weeks following delivery.20
he authors concluded that the longerime interval, or the 8 week interval, wasssociated with fewer false-positive testss a result of decreasing inflammation. Ithould, however, be noted that manyomen have their only cytological
creening during their perinatal visits.21
s such, the authors recommend follow-ng standard guidelines for the intervalollowing a normal Papanicolaou test,nless the follow-up may be compro-ised by poor patient compliance.Although many programs have insti-
uted reflex testing, or high-risk humanapillomavirus testing only in the presencef atypical squamous cells of undeter-ined significance (ASC-US), there are
ome sites that perform high-risk HPVesting at the time of initial cytologic sam-ling in women over 30 years of age. Thus,ome women will fall into the category ofaving normal cervical cytology with aositive high-risk HPV analysis. Clavel etl22 followed up such patients and foundhat only 4% of such women had findingsf CIN 2 or higher. This has led to the rec-mmendation, restated in the 2006 con-ensus guidelines, that women with nega-ivecervical cytologyandpositivehigh-riskPV be followed up with a repeat of both
ests at 12 months.9,11,23 Because mostomen with such findings have only tran-
ient HPV infections, it is recommendedhat pregnant women with negative cervi-al cytology and positive high-risk HPV re-ults undergo a repeat of both tests at the 6eek postpartum visit.Furthermore, many women may also
e found to have the result of a negativeapanicolaou test and negative high-riskPV. For pregnant patients 30 years old
nd older who demonstrate this double-egative finding, joint guidelines by theational Cancer Institute, the American
ociety of Colposcopy and Cervical Pa-hology (ASCCP), and the ACS recom-
end that they undergo repeat screeningt an interval no shorter than 3 years
rom the negative result.9,11,23 tAmerican Journal of Obstetrics & Gynecology JU
bsence of endocervical cellsith the expansion of the transforma-
ion zone in early pregnancy, it should beasier to sample endocervical cells dur-ng pregnancy. Papanicolaou tests lack-ng endocervical cells during pregnancyhould be repeated.24,25
iagnostic proceduresn pregnancylthough the timing and the indications
or cervical screening do not differ ap-reciably between pregnant and non-regnant patients, the management ofytologic abnormalities can be widely di-ergent. Such differences lie primarily inhe reluctance of most physicians to per-orm the necessary interventions foroth the proper diagnosis and the treat-ent of cervical neoplasia.
olposcopy during pregnancyncreasing pelvic congestion duringregnancy may make the proceduralspects of colposcopy more difficult.n increase in vaginal wall protrusionnd wall redundancy may obscure a di-ect line of visualization between theolposcope and the cervix. The use of aaginal sidewall retractor, in combina-ion with a Graves speculum, may im-rove cervical access. Alternatively, aondom with the tip removed can belipped over the speculum to retain theaginal side walls. Overall, changes as-ociated with the visual findings of theregnant cervix may significantly con-
use the interpretation of colposcopicesults. As such, only those with ad-anced training and/or extensive expe-ience should perform colposcopy onhe pregnant patient who presents withn abnormal Papanicolaou smear.The adequacy of a colposcopic exami-
ation in pregnancy can be further com-romised by the common finding of annlarged cervix. The presence of suchay prompt the need for multiple ma-
ipulations of both the speculum andhe colposcope to obtain a complete ex-mination of all 4 cervical quadrants. Asn the nonpregnant state, it is necessaryo have complete visualization of theransformation zone. Fortunately, theres a gradual eversion of the endocervix as
he pregnancy progresses.26 Economos pLY 2008
t al27 reported that most patients haveuch an eversion, as to render virtually allolposcopies adequate by 20 weeks ofestation.Given the aforementioned cervical
hanges associated with pregnancy, it ismperative that the visual impressionave a proven and reliable correlationith histology. Some authors have sug-ested that the changes associated withregnancy inherently cause an artificialverestimation of lesion severity.28
owever, 1 retrospective investigationeported on the evaluation of 612 cyto-ogic abnormalities in pregnancy.27 Fourundred forty-nine patients underwentolposcopically directed biopsy, with aorrelation of 95% to within 1 degree ofhe visual impression. Colposcopic im-ression appears be well correlated withntepartum biopsy, with only 1 of 867atients demonstrating an invasive le-ion in which the colposcopic impres-ion was preinvasive (CIN 3).27-30
ervical biopsyoncerns over excess bleeding, resulting
rom a pregnant and presumably hyper-mic cervix, prevent many physiciansrom performing biopsies, in which theyould otherwise be indicated. Such con-
erns have not been definitively con-rmed, although they have been propa-ated in the literature.19,31 Conversely,everal studies have reported the liberalse of colposcopically directed biopsies
n pregnancy.27,32-34 Although thesetudies were not designed to investigatehe use of cervical biopsy in pregnancypecifically, they do not report signifi-ant bleeding complications or adverseregnancy outcomes associated with therocedure.Although bleeding is considerably less
uring the first trimester, some authorsdvocate waiting until the second tri-ester before a biopsy is performed to
void the association of the procedureith a spontaneous, and likely unrelated,iscarriage. Others still advocate the use
f a stiff brush as a biopsy substitute for aess invasive diagnosis.35 This techniquemploys the use of a spiral brush withhickened bristles, which, when used torush a suspected cervical lesion, can
rovide a specimen that is comparable
wtbac
EAivmpOuifnoltwEu
MaATsptAhunrtiCAwfag
sHPmmAawawt
wotutctsam
AaIrgavmCcuc
pAcsaenupg
lwrtcu
SAlmm
CI
AantH
www.AJOG.org Oncology Reviews
ith that of a punch biopsy.36 Beyondhe first trimester, cervical biopsy or stiffrush procedure should be performed inny patient for whom invasive cancerannot be reliably excluded.
ndocervical curettagelthough there have been no random-
zed trials to evaluate the risk of endocer-ical curettage (ECC) in pregnancy,any authors feel that ECC is not appro-
riate when a woman is pregnant.27,37,38
ne retrospective study described these of ECC in the diagnosis of carcinoma
n situ in 33 pregnant patients.39 Theyound that 97% delivered at term, witho significant difference in either the ratef preterm delivery or the incidence of
ow birthweight, when compared withhe general population. Nonetheless,ith an absence of well-designed trials,CC in the pregnant patient isnacceptable.33
anagement of cytologicbnormalitiestypical squamous cellshe likelihood of finding an invasive le-
ion following either antepartum orostpartum biopsy is less than 1% whenhe high-risk HPV test is positive after anSC-US Papanicolaou test. However,igh-grade lesions may be diagnosed inp to 1 in 5 patients with ASC-US Papa-icolaou tests. Because there is no cur-ent evidence that either the natural his-ory or the prevalence of HPV infections altered in the pregnant state,40 the AS-CP recommendation of managingSC-US using HPV triage is acceptable,hereas colposcopy should be per-
ormed for all pregnant patients withtypical squamous cells favoring high-rade lesions.Because serial cytology has been
hown to have a lower sensitivity thanPV testing41 and because repeating aapanicolaou test in the third trimesteray be impractical, it is not recom-ended for antepartum management.SCCP 2006 guidelines recommendgainst the use of HPV triage in patientsith ASC-US younger than 20 years of
ge. The guidelines allow for pregnantomen older than 20 years with ASC-US
o be managed as the nonpregnant C
oman (ie, HPV testing by either reflexr at a return office visit), with the excep-ion that colposcopy may be deferredntil at least 6 weeks postpartum.9,11 Pa-
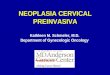
ients who are high-risk HPV negativean be followed up with a Papanicolaouest at 6 weeks postpartum. Figure 1 de-cribes specific recommendations for thessessment and follow-up of the abnor-al Papanicolaou test in pregnancy.
typical glandular cells (AGCs)nd adenocarcinoma in situ (AIS)n the pregnant patient, the Arias-Stellaeaction can often be misinterpreted as alandular atypia.42,43 The Arias-Stella re-ction was found to involve the endocer-ical canal in 9% of hysterectomy speci-ens obtained perigestationally.44
onsequently, Kim et al45 found only 1arcinoma in situ in 21 patients followedp conservatively for atypical glandularells in pregnancy. Furthermore,
FIGURE 1Algorithm for the management of tPap smear and CIN in pregnancy
Colposcopy
ASC-H
Repeat ColpEvery Trim
Cancer* CIN III CIN II C
AGC-AIS HSIL
olposcopicmpression
Biopsy CIN or (-)
Invasion
See Part 2U
Colposcopy/Postpart
GC, atypical glandular cells; AIS, adenocarcintypical squamous intraepithelial lesion of undeeoplasia; HR-HPV, high risk human papillomahelial lesion; LSIL, low grade SIL.unter. Cervical neoplasia in pregnancy. Am J Obstet Gynec
hhieng et al46 followed up 30 pregnant t
JULY 2008 A
atients and 5 postpartum patients withGCs. Of those who underwent colpos-opy and biopsy, 18% had high-gradequamous intraepithelial lesions (HSIL)nd 12% had low-grade squamous intra-pithelial lesions (LSIL). No adenocarci-oma or AIS was diagnosed. On follow-p, only 2 patients were found to haveersistent cellular atypia, 1 of which waslandular and the other squamous.According to the 2006 ASCCP guide-
ines, the evaluation of AGCs in pregnantomen should be identical to that recur-
ent for nonpregnant women, excepthat endocervical curettage, cold-knifeone biopsy, and endometrial biopsy arenacceptable.10,12
quamous intraepithelial lesionslthough pregnancy can cause physio-
ogic and visual changes in the cervix thatay be misinterpreted as dysplasia, itay be presumptive to assume that cy-
abnormal
ASC-US
Repeat Pap +/- HPV Postpartum
HR-HPV Testingsitive
opyer
I Normal
Under 20 y.o.
20+ y.o.
20+ y.o.
LSIL
Negative
anged
psy
a-in-situ; ASC-H, favor high grade; ASC-US,ined significance; CIN, cervical intraepithelial
s testing; HSIL, high grade squamous intraepi-
08.
he
Po
oscest
IN
nch
Bioum
omterm
viru
ol 20
ology consistent with an intraepithelial
merican Journal of Obstetrics & Gynecology 5

lttbottpw
lnLatiisvrowCmpd
ncupahMwpmm
tbifgctIt
pcapAdittcclap
CmaaatRawcasow
AttIHcoFcapsmci
EBovtpCacsocnonttawws
asAaiutmp
LtCswLppmpsattt
picsnL
HG
Reviews Oncology www.AJOG.org
6
esion was falsely positive. Patients withhe cervical cytology of LSIL are unlikelyo have an invasive lesion on antepartumiopsy, with none of 287 patients dem-nstrating such pathology.33 Some au-hors have even suggested that it is nei-her cost effective nor necessary toerform colposcopy on every personith LSIL cytology.33
According to the 2006 ASCCP guide-ines, colposcopy is preferred for theonadolescent pregnant woman withSIL, but deferring this procedure untilt least 6 weeks postpartum is also an op-ion. For those whose initial colposcopys performed antenatally, provided theres no cytological, histological, or colpo-copically suspected CIN 2, CIN 3, or in-asive cancer, postpartum follow-up isecommended. In other words, the rec-mmended management of pregnantomen with a histological diagnosis ofIN 1 is follow-up without any treat-ent. For such women, additional col-
oscopic and cytological examinationsuring pregnancy are unacceptable.There is little debate in regard to the
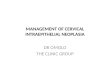
eed for patients with an HSIL Papani-olaou test to undergo colposcopy. Fig-re 2 illustrates that the majority of theseatients will have high-grade lesions onntepartum biopsy and that 1 in 100 willave an invasive lesion.30,31,49,59,69-71
urta et al47 reported on 53 patientsith biopsy proven high-grade lesions inregnancy. Most of these patients wereanaged conservatively, and approxi-
FIGURE 2Antepartum biopsy resultsfollowing low-grade and high-grade squamous intraepitheliallesions30,31,49,59,69-71
80.0
70.0
60.0
50.0LSIL (N=287)
Per
cen
t 40.0HSIL (N=500)
30.0
20.0
10.0
0.0Normal CIN I CIN II/III Invasive
Biopsy Results
unter. Cervical neoplasia in pregnancy. Am J Obstetynecol 2008.
ately 75% of them had persistence of o
American Journal of Obstetrics & Gynecology JU
heir high-grade lesion on postpartumiopsy. None of them had progression to
nvasive disease. Similarly, Vlahos et al48
ollowed up 78 biopsy-proven high-rade lesions through pregnancy, withytology and colposcopy at 8-10 week in-ervals. They reported regression to CINin 62% of patients, with no progressiono invasive disease.
The 2006 ASCCP guidelines advise allregnant women with HSIL to undergoolposcopy, preferably by clinicians whore experienced in the evaluation of col-oscopic changes induced by pregnancy.lthough the expertise of providers mayiffer based on formal training and clin-
cal interests, it is reasonable to expecthat members of the ASCCP and/orhose gynecologists and gynecologic on-ologists who have a special interest inlinical colposcopy will have accumu-ated significant experience in the evalu-tion and management of abnormal Pa-anicolaou tests in pregnancy.Biopsy of lesions suspicious for CIN 2,
IN 3, or invasive cancer is recom-ended. Patients with a histological di-
gnosis of CIN 2 or CIN 3 may undergodditional colposcopic and cytologic ex-minations at intervals no more frequenthan every 12 weeks during pregnancy.epeat biopsy during pregnancy is advis-ble only if the appearance of the lesionorsens or if cytology suggests invasive
ancer. Pregnant women with HSIL whore not diagnosed with CIN 2 or CIN 3hould undergo reevaluation with cytol-gy and colposcopy no sooner than 6eeks postpartum.Figure 1 depicts modifications to the
SCCP, ACOG, and ACS guidelines forhe treatment of LSIL and HSIL, respec-ively, in the special situation of pregnancy.n summary, all pregnant patients with anSIL Papanicolaou test should undergo
olposcopic evaluation, as would be rec-mmended for the nonpregnant patient.or the gravid cervix, however, biopsiesan be associated with an abnormally largemount of bleeding, and colposcopic im-ressions can be misleading, artificiallyuggesting a higher grade lesion. Further-
ore, a poorly timed cervical procedureould be erroneously associated with a co-ncident miscarriage, preterm labor, or
ther complication. cLY 2008
xcisional biopsy in pregnancyecause the risk of progression of CIN 2r CIN 3 to microinvasive or frankly in-asive cervical carcinoma is minimal andhe rate of spontaneous regression post-artum is relatively high, treatment ofIN during pregnancy should bevoided. In point of fact, as will be dis-ussed in the companion article on inva-ive cervical cancer in pregnancy, manyncologists follow early-stage cervicalancer in pregnancy until fetal pulmo-ary maturation has been achieved. Notnly is treatment of CIN during preg-ancy associated with significant perina-
al morbidity (including catastrophic in-raoperative hemorrhage), but there islso a high rate of incomplete excision,hich results in the persistence of CIN asell as a recurrence rate which is
ignificant.49
If the referral cytology, colposcopicppearance, and/or cervical biopsy is/areuspicious for invasive cancer, the 2006SCCP guidelines recommend that di-gnostic excision be considered. Unlessnvasive cancer is identified, treatment isnacceptable, with reevaluation with cy-
ology and colposcopy being recom-ended no sooner than 6 weeks
ostpartum.
arge loop excision of theransformation zone (LLETZ)ertainly there are cases in which inva-
ion cannot be definitively ruled outithout the use of an excision procedure.LETZ is used for such diagnostic pur-oses but may also be useful for thera-eutic purposes. The ASCCP recom-ends LLETZ in the nonpregnant
atient under the following circum-tances: biopsy-proven CIN 2, CIN 3,nd AIS; AGC-favor neoplasia or AIS cy-ology (if colposcopy and ECC are nega-ive); and normal or CIN I histology inhe setting of HSIL cytology.
Naturally physicians are reluctant toerform such an invasive procedure dur-
ng pregnancy, with the fear that even aoincidental complication could be as-ociated with the LLETZ. As such, it isecessary to examine the indications forLETZ carefully and to determine when
ervical neoplasia must be treated in
pu
hfontcptp
aLibtdtptswfwfa
ptgpmofttalwgc
fanpthtitpic
all
mfdpwespibfmc
CSumppLa5ttALwaostoioc
CBshbesiSdmltn
ip
oeptistpinb
NoItbntaps2tpceeg
iepttFsttFcvtoIppsCt
www.AJOG.org Oncology Reviews
regnancy and when it can be delayedntil the postpartum period.Several studies, over the last few decades,
ave attempted to evaluate the effects onuture child-bearing of large loop excisionf the cervix, performed outside preg-ancy. Despite a measurable shortening of
he cervical length,50 several studies con-luded that LLETZ does not appear to ap-reciably predispose patients to complica-ions in a subsequent pregnancy, includingreterm delivery.51-55
A recent metaanalysis by Kyrgiou etl,56 however, does provide evidence thatLETZ (and cold-knife conization) does
ncrease the risk of preterm birth, lowirthweight infants, and cesarean sec-ions. A recent report by Samson et al57
emonstrated a significant increase inhe risk of delivery before 37 weeks inatients who had a prior loop excision ofhe cervix. Although they also demon-trated an increased risk of low birth-eight, they did not find a significant dif-
erence in the risk of delivery before 34eeks. Other investigators have also
ound LLETZ to be significantly associ-ted with lower birthweights.58
In the same way that LLETZ outsideregnancy has demonstrated inconsis-ent effects on future gestations, investi-ators performing the procedure duringregnancy have also demonstratedixed results. Robinson et al49 reported
n a series of 20 loop excisions per-ormed for intraepithelial neoplasia be-ween 8 and 34 weeks’ gestation. Two pa-ients required blood transfusionscutely, and 3 patients had a preterm de-ivery. Of note, only patients who under-ent LLETZ between 27 and 34 weeks ofestational age were associated with suchomplications.
Conversely, Matsuhashi et al59 per-ormed 9 loop excisions at a gestationalge, ranging from 4 to 14 weeks. Heoted no significant intraoperative orostoperative complications, and all pa-ients delivered at term. One patient didave a cerclage placed at 28 weeks, al-hough she, too, delivered at term. Sim-larly, Dunn et al21 reported on 13 pa-ients undergoing loop excision inregnancy, all of whom were followed up
mmediately by the placement of a cer-
lage. The patients ranged in gestational tge from 13 to 32 weeks. All patients de-ivered at term, although 2 had a bloodoss of at least 250 milliliters.
Given the aforementioned reports, itay be suggested that LLETZ can be per-
ormed in pregnancy with a reasonableegree of maternal safety. However, thisrocedure should be performed only in aell-staffed and properly equipped op-
rating room. Furthermore, LLETZhould be reserved for patients who arereviable and in whom invasive disease
s strongly suspected or confirmed withiopsy. Alternatively, LLETZ can be per-ormed prior to a planned pregnancy ter-
ination for patients in whom such aourse is desired.
old knife cervical conizationeveral earlier studies investigated these of cold-knife conization for the treat-ent of suspected or proven severe dys-
lasia or microinvasive disease duringregnancy. Similar to the findings forLETZ, cold-knife conization has beenssociated with heavy vaginal bleeding in-15% of pregnant patients.60,61 Fur-hermore, the rate of spontaneous abor-ion was noted to be as high as 25%.gain, in parallel to the findings forLETZ, approximately 50% of patientsill have recurrent CIN following an
ntepartum conization, presumably sec-ndary to smaller-than-usual exci-ions.61,62 Because of the high complica-ion rate attributed to the performancef a cold-knife cervical conization dur-
ng pregnancy, the authors do not rec-mmend this procedure to rule out mi-roinvasive or frankly invasive disease.
oin biopsyecause pregnancy causes a relative ever-
ion of the squamocolumnar junction,igh sampling of the endocervix may note necessary. Some have advocated thexcision of a coin-shaped specimen in-tead of a cone shape in which the spec-men is wedged out in the shape of a pie.uch a shallow excision will cause lessisruption to the endocervical canal anday decrease both bleeding and preterm
abor complications.63 In contrast to aypical cone procedure on the nonpreg-ant cervix, a total of 6 hemostatic su-
ures should be placed prior to perform- t
JULY 2008 A
ng the coin procedure in the pregnantatient.This procedure should be performed
nly in the operating room, in which ad-quate exposure, blood products, androper anesthesia can be secured. Lastly,he size of the specimen should be lim-ted only to the area under question andhould in no way attempt to encompasshe entire transformation zone. The pur-ose of such an excision is to diagnose
nvasion and not to treat intraepithelialeoplasia, the management of which wille discussed in the following text.
atural historyf CIN in pregnancyt is clear from the aforementioned de-ailed investigations that the finding ofiopsy-proven CIN in pregnancy doesot warrant interruption of the gesta-
ion. In fact, CIN 1, 2, and 3 have all beenssociated with acceptably low rates ofrogression. Although Figure 3 demon-trates that it is possible for CIN 1 or CIN
to progress to CIN 3,30,31,35,67,69,71,72
his may represent a subpopulation ofatients with less than optimal immuno-ompetence, or alternatively, samplingrror during the antepartum biopsies. Inither case, the significance of such a pro-ression is of little concern.Colposcopic surveillance of CIN dur-
ng pregnancy (Figure 3) is performedxclusively for the purpose of detectingrogression to invasive disease. Persis-ent CIN 3, and therefore progression tohe same, can be managed expectantly.igure 3 demonstrates that the progres-ion from CIN 3 to invasive disease be-ween the antepartum and the postpar-um period is an unlikely event.urthermore, there is no evidence thatytologic, histologic, or colposcopic sur-eillance of a CIN 3 lesion during the an-epartum period has any effect on theverall prognosis of such a progression.n summary, all patients with biopsy-roven CIN 2 or 3 should undergo col-oscopic evaluation with directed biop-ies at the 6 week postpartum visit.olposcopic surveillance during the an-
epartum period is at the discretion of
he provider.merican Journal of Obstetrics & Gynecology 7

MWlsigpHc6stotltr
SWttipDttm
peutttoiyse
wmpomsp
R1ap22Bd3vwpF4op85tY6Dan27Cst8Pkp29MgaO12mi21Mgcn31SAP2
pT1Mht1Stni1el11PluC1miP21c1p31lc12rlp22cn2pts12aic12tMa22Ani2mO2
HG
Reviews Oncology www.AJOG.org
8
ode of deliveryith regard to intraepithelial lesions, the
ocal inflammatory reaction initiatedecondary to cervical trauma during vag-nal delivery may actually improve re-ression rates.64 Indeed, 1 study com-ared regression rates for patients withSIL delivering both vaginally and by
esarean section and found regression in7% and 13%, respectively.65 Othertudies have not demonstrated a rela-ionship between delivery mode and ratef regression.66,67 Patients with intraepi-helial disease should have a mode of de-ivery that is based only on obstetric fac-ors as well as maternal factors notelated to CIN.
ummaryith more than 3 million deliveries in
he United States and improving prena-al cervical screening programs, a signif-cant number of pregnant womenresent with cervical neoplasia each year.espite the large size of this population,
here are relatively few studies on whicho formulate evidence-based manage-
ent guidelines.As such, recommendations must be
roposed on the basis of data that arextrapolated from the nonpregnant pop-lation, with modifications sensitive to
he unique situation of pregnancy. For-unately, progression from preinvasiveo invasive disease during the time framef 1 or 2 trimesters is rare. Furthermore,
t is well established that, especially in theounger patient population, the rate ofpontaneous regression of cervical intra-
FIGURE 3Correlation betweenantepartum and postpartumhistology30,31,35,67,69,71,72
70.0
60.0
Antepartum50.0
CIN I (N=88)40.0
Per
cen
t
CIN II (N=165)30.0 CIN III (N=316)
20.0
10.0
0.30.0
Normal CIN I CIN II CIN III Invasive
Postpartum Histology
unter. Cervical neoplasia in pregnancy. Am J Obstetynecol 2008.
pithelial lesions is high.68 m
American Journal of Obstetrics & Gynecology JU
This affords the opportunity for mostomen with preinvasive disease to beanaged conservatively until the com-
letion of pregnancy. In the second partf this series, recommendations will beade regarding the treatment of inva-
ive cervical cancer discovered duringregnancy. f
EFERENCES. Insinga RP, Glass AG, Rush BB. Diagnosesnd outcomes in cervical cancer screening: Aopulation-based study. Am J Obstet Gynecol004;191:105-13.. Arias E, MacDorman MF, Strobino DM, Guyer. Annual summary of vital statistics—2002. Pe-iatrics 2003;112:1215-30.. Morimura Y, Fujimori K, Soeda S, et al. Cer-ical cytology during pregnancy—comparisonith non-pregnant women and management ofregnant women with abnormal cytology.ukushima J Med Sci 2002;48:27-37.. Douvier S, Filipuzzi L, Sagot P. [Managementf cervical intra-epithelial neoplasm duringregnancy]. Gynecol Obstet Fertil 2003;31:51-5.. Cheng X, Bian X, Lang J, et al. [Papanicolaouest in pregnancy]. Zhongguo Yi Xue Ke Xueuan Xue Bao 2000;22:174-6.. Smith LH, Dalrymple JL, Leiserowitz GS,anielsen B, Gilbert WM. Obstetrical deliveriesssociated with maternal malignancy in Califor-ia, 1992 through 1997. Am J Obstet Gynecol001;184:1504-12.; discussion 1512-3.. Smith LH, Danielsen B, Allen ME, Cress R.ancer associated with obstetric delivery: Re-ults of linkage with the California cancer regis-ry. Am J Obstet Gynecol 2003;189:1128-35.. Demeter A, Sziller I, Csapo Z, Szantho A,app Z. Outcome of pregnancies after cold-nife conization of the uterine cervix duringregnancy. Eur J Gynaecol Oncol 2002;23:07-10.. Wright TC Jr, Massad LS, Dunton CJ, Spitzer, Wilkinson EJ, Solomon D. 2006 consensusuidelines for the management of women withbnormal cervical cancer screening tests. Am Jbstet Gynecol 2007;197:346-55.0. Wright TC Jr, Massad LS, Dunton CJ, et al.006 consensus guidelines for the manage-ent of women with abnormal cervical screen-
ng tests. J Low Genit Tract Dis 2007;11:201-2.1. Wright TC Jr, Massad S, Dunton CJ, Spitzer, Wilkinson EJ, Solomon D. 2006 consensusuidelines for the management of women withervical intraepithelial neoplasia or adenocarci-oma in situ. Am J Obstet Gynecol 2007;197:40-5.2. Wright TC Jr, Massad LS, Dunton CJ,pitzer M, Wilkinson EJ, Solomon D. 2006merican Society for Colposcopy and Cervicalathology–sponsored Consensus Conference.006 consensus guidelines for the manage-
ent of women with cervical intraepithelial neo- CLY 2008
lasia or adenocarcinoma in situ. J Low Genract Dis 2007;11:223-39.3. Lorenzato F, Singer A, Mould T, Santos LC,aia A, Cariri L. Cervical cancer detection by
ybrid capture and evaluation of local risk fac-ors. Int J Gynaecol Obstet 2001;73:41-6.4. Kjellberg L, Hallmans G, Ahren AM, et al.moking, diet, pregnancy and oral contracep-
ive use as risk factors for cervical intra-epithelialeoplasia in relation to human papillomavirus
nfection. Br J Cancer 2000;82:1332-8.5. Stillson T, Knight AL, Elswick RK Jr. Theffectiveness and safety of two cervical cyto-
ogic techniques during pregnancy. J Fam Pract997;45:159-63.6. Sherman ME, Schiffman M, Herrero R, et al.erformance of a semiautomated Papanico-
aou smear screening system: results of a pop-lation-based study conducted in Guanacaste,osta Rica. Cancer 1998;84:273-80.7. Sato M, Nakamura Y, Sogawa T, et al. Im-unolocalization of glucose transporter 1 and 3
n the placenta: Application to cytodiagnosis ofapanicolaou smear. Diagn Cytopathol 2002;6:373-9.8. Pisharodi LR, Jovanoska S. Spectrum ofytologic changes in pregnancy. A review of00 abnormal cervicovaginal smears, with em-hasis on diagnostic pitfalls. Acta Cytol 1995;9:905-8.9. Michael CW, Esfahani FM. Pregnancy-re-
ated changes: A retrospective review of 278ervical smears. Diagn Cytopathol 1997;17:99-07.0. Levitt C, Shaw E, Wong S, et al. Systematiceview of the literature on postpartum care: Se-ected contraception methods, postpartum Pa-anicolaou test, and rubella immunization. Birth004;31:203-12.1. Dunn TS, Ginsburg V, Wolf D. Loop-coneerclage in pregnancy: A 5-year review. Gy-ecol Oncol 2003;90:577-80.2. Clavel C, Masure M, Bory JP, et al. Humanapillomavirus testing in primary screening forhe detection of high-grade cervical lesions: Atudy of 7932 women. Br J Cancer 2001;84:616-23.3. Wright TC Jr, Schiffman M, Solomon D, etl. Interim guidance for the use of human pap-
llomavirus DNA testing as an adjunct to cervicalytology for screening. Obstet Gynecol 2004;03:304-9.4. ACOG practice bulletin. Diagnosis andreatment of cervical carcinomas. Number 35,ay 2002. American College of Obstetricians
nd Gynecologists. Int J Gynaecol Obstet002;78:79-91.5. Davey DD, Austin RM, Birdsong G, et al.SCCP patient management guidelines: Papa-icolaou test specimen adequacy and quality
ndicators. Am J Clin Pathol 2002;118:714-8.6. Nguyen C, Montz FJ, Bristow RE. Manage-ent of stage I cervical cancer in pregnancy.bstet Gynecol Surv 2000;55:633-43.7. Economos K, Perez Veridiano N, Delke I,
ollado ML, Tancer ML. Abnormal cervical cy-
tO2pp12Rcc13ps13dvaB3Wcac33ms13iat13lcc13bdG3cO3Csu13Ean4KiC4Lf
t24sL4ov(4d14ui(s4hp24Ae24aew4SeL5Bst55Dcc15Fgcs5ples25[eiZ5Ls5
sflL5Dec5PtG5cm26Wo16sn6Ecn6S6SaA6aalJ6BcG6PvO6uJ6nO7an7so37ci
www.AJOG.org Oncology Reviews
ology in pregnancy: A 17-year experience.bstet Gynecol 1993;81:915-8.8. Broderick DMDDMAS. Histologic and col-oscopic correlates of ASCUS Pap smears inregnancy. J Low Genit Tract Dis 2002;6:116-9.9. Woodrow N, Permezel M, Butterfield L,ome R, Tan J, Quinn M. Abnormal cervicalytology in pregnancy: experience of 811ases. Aust N Z J Obstet Gynaecol 1998;38:61-5.0. Benedet JL, Selke PA, Nickerson KG. Col-oscopic evaluation of abnormal Papanicolaoumears in pregnancy. Am J Obstet Gynecol987;157:932-7.1. Paraskevaidis E, Koliopoulos G, Kalantari-ou S, et al. Management and evolution of cer-ical intraepithelial neoplasia during pregnancynd postpartum. Eur J Obstet Gynecol Reprodiol 2002;104:67-9.2. Basta A, Szczudrawa A, Pitynski K, Kolawa. [The value of colposcopy and computerised
olposcopy in diagnosis and therapeutic man-gement of CIN and early invasive cervical can-er in pregnant women]. Ginekol Pol 2002;73:07-13.3. Jain AG, Higgins RV, Boyle MJ. Manage-ent of low-grade squamous intraepithelial le-
ions during pregnancy. Am J Obstet Gynecol997;177:298-302.4. Baldauf JJ, Dreyfus M, Gao J, Ritter J, Phil-
ppe E. [Management of pregnant women withbnormal cervical smears. A series of 146 pa-ients]. J Gynecol Obstet Biol Reprod (Paris)996;25:582-7.5. Lieberman RW, Henry MR, Laskin WB, Wa-
enga J, Buckner SB, O’Connor DM. Colpos-opy in pregnancy: directed brush cytologyompared with cervical biopsy. Obstet Gynecol999;94:198-203.6. Monk BJ, Cogan M, Felix JC, et al. A stiffristled, spiral-shaped ectocervical brush: Aevice for transepithelial tissue biopsy. Obstetynecol 2002;100:1276-84.7. Palle C, Bangsboll S, Andreasson B. Cervi-al intraepithelial neoplasia in pregnancy. Actabstet Gynecol Scand 2000;79:306-10.8. Hellberg D, Axelsson O, Gad A, Nilsson S.onservative management of the abnormalmear during pregnancy. A long-term follow-p. Acta Obstet Gynecol Scand 1987;66:95-9.9. El-Bastawissi AY, Becker TM, Daling JR.ffect of cervical carcinoma in situ and its man-gement on pregnancy outcome. Obstet Gy-ecol 1999;93:207-12.0. Lu DW, Pirog EC, Zhu X, Wang HL, PintoR. Prevalence and typing of HPV DNA in atyp-
cal squamous cells in pregnant women. Actaytol 2003;47:1008-16.1. Wright TC Jr, Cox JT, Massad LS, TwiggsB, Wilkinson EJ. 2001 consensus guidelines
or the management of women with cervical cy- A
ological abnormalities. JAMA 2002;287:120-9.2. Rhatigan RM. Endocervical gland atypiaecondary to Arias-Stella change. Arch Patholab Med 1992;116:943-6.3. Kobayashi TK, Okamoto H. Cytopathologyf pregnancy-induced cell patterns in cervico-aginal smears. Am J Clin Pathol 2000;114Suppl):S6-20.4. Schneider V. Arias-Stella reaction of the en-ocervix: Frequency and location. Acta Cytol981;25:224-8.5. Kim TJ, Kim HS, Park CT, et al. Clinical eval-ation of follow-up methods and results of atyp-
cal glandular cells of undetermined significanceAGUS) detected on cervicovaginal Papmears. Gynecol Oncol 1999;73:292-8.6. Chhieng DC, Elgert P, Cangiarella JF, Co-en JM. Significance of AGUS Pap smears inregnant and postpartum women. Acta Cytol001;45:294-9.7. Murta EF, de Souza FH, de Souza MA,dad SJ. High-grade cervical squamous intra-pithelial lesion during pregnancy. Tumori002;88:246-50.8. Vlahos G, Rodolakis A, Diakomanolis E, etl. Conservative management of cervical intra-pithelial neoplasia (CIN(2-3)) in pregnantomen. Gynecol Obstet Invest 2002;54:78-81.9. Robinson WR, Webb S, Tirpack J, Degefu, O’Quinn AG. Management of cervical intra-pithelial neoplasia during pregnancy withOOP excision. Gynecol Oncol 1997;64:153-5.0. Ricciotti HA, Burke L, Kobelin M, Slomovic, Ludmir J. Ultrasound evaluation of cervicalhortening after loop excision of the transforma-ion zone (LETZ). Int J Gynaecol Obstet 1995;0:175-8.1. Cruickshank ME, Flannelly G, CampbellM, Kitchener HC. Fertility and pregnancy out-ome following large loop excision of the cervi-al transformation zone. Br J Obstet Gynaecol995;102:467-70.2. Ferenczy A, Choukroun D, Falcone T,ranco E. The effect of cervical loop electrosur-ical excision on subsequent pregnancy out-ome: North American experience. Am J Ob-tet Gynecol 1995;172:1246-50.3. Paraskevaidis E, Koliopoulos G, Lolis E, Pa-anikou E, Malamou-Mitsi V, Agnantis NJ. De-
ivery outcomes following loop electrosurgicalxcision procedure for microinvasive (FIGOtage IA1) cervical cancer. Gynecol Oncol002;86:10-3.4. Qian DY, Zeng RH, Hong DH, Cen JM.
Pregnancy and delivery outcomes after looplectrosurgical excision procedure of cervical
ntraepithelial neoplasia]. Zhonghua Fu Chan Kea Zhi 2004;39:326-8.5. Tseng CJ, Soong YK, Liang CC, Hsueh S.oop excision for cervical intraepithelial neopla-ia. J Formos Med Assoc 1992;91:1059-63.6. Kyrgiou M, Koliopoulos G, Martin-Hirsch P,
rbyn M, Prendiville W, Paraskevaidis E. Ob- 1JULY 2008 A
tetric outcomes after conservative treatmentor intraepithelial or early invasive cervicalesions: Systematic review and meta-analysis.ancet 2006;367:489-98.7. Samson SL, Bentley JR, Fahey TJ, McKayJ, Gill GH. The effect of loop electrosurgicalxcision procedure on future pregnancy out-ome. Obstet Gynecol 2005;105:325-32.8. Blomfield PI, Buxton J, Dunn J, Luesley DM.regnancy outcome after large loop excision of
he cervical transformation zone. Am J Obstetynecol 1993;169:620-5.9. Mitsuhashi A, Sekiya S. Loop electrosurgi-al excision procedure (LEEP) during first tri-ester of pregnancy. Int J Gynaecol Obstet000;71:237-9.0. Averette HE, Nasser N, Yankow SL, LittleA. Cervical conization in pregnancy. Analysis
f 180 operations. Am J Obstet Gynecol 1970;06:543-9.1. Hannigan EV, Whitehouse HH 3rd, Atkin-on WD, Becker SN. Cone biopsy during preg-ancy. Obstet Gynecol 1982;60:450-5.2. Hacker NF, Berek JS, Lagasse LD, CharlesH, Savage EW, Moore JG. Carcinoma of theervix associated with pregnancy. Obstet Gy-ecol 1982;59:735-46.3. DiSaia PCW. Clinical gynecologic oncology.t. Louis (MO): Mosby, Inc; 2002.4. Strinic T, Bukovic D, Karelovic D, Bojic L,tipic I. The effect of delivery on regression ofbnormal cervical cytologic findings. Collntropol 2002;26:577-82.5. Siristatidis C, Vitoratos N, Michailidis E, etl. The role of the mode of delivery in the alter-tion of intrapartum pathological cervical cyto-
ogic findings during the postpartum period. EurGynaecol Oncol 2002;23:358-60.6. Coppola A, Sorosky J, Casper R, Anderson, Buller RE. The clinical course of cervical car-inoma in situ diagnosed during pregnancy.ynecol Oncol 1997;67:162-5.7. Yost NP, Santoso JT, McIntire DD, Iliya FA.ostpartum regression rates of antepartum cer-ical intraepithelial neoplasia II and III lesions.bstet Gynecol 1999;93:359-62.8. Holowaty P, Miller AB, Rohan T, To T. Nat-ral history of dysplasia of the uterine cervix.Natl Cancer Inst 1999;91:252-8.9. Lurain JR, Gallup DG. Management of ab-ormal Papanicolaou smears in pregnancy.bstet Gynecol 1979;53:484-8.0. Ortiz R, Newton M. Colposcopy in the man-gement of abnormal cervical smears in preg-ancy. Am J Obstet Gynecol 1971;109:46-9.1. LaPolla JP, O’Neill C, Wetrich D. Colpo-copic management of abnormal cervical cytol-gy in pregnancy. J Reprod Med 1988;33:01-6.2. Lundvall L. Comparison between abnormalytology, colposcopy and histopathology dur-
ng pregnancy. Acta Obstet Gynecol Scand
989;68:447-52.merican Journal of Obstetrics & Gynecology 9