Embed Size (px)
Citation preview

Cervical Aortic Arch: A Commentary
By Benjamin Felsont and Janet L. Strife
C ERVICAL AORTIC ARCH (CAA) was first described by Reid in 1914.’ Rare as it
is, CAA provides a link in the embryogenesis of the great arteries of the thorax. Its interesting variations offer a clarifying dimension to the complex confusion of anomalies of the thoracic aorta. The high location of the CAA is usually attributed to persistence of the right or left third arch instead of the fourth arch, thereby rerouting the aorta via the neck. However, failure of the normal caudal migration of the fully developed fourth arch in the growing embryo from the occipital level in the thoracic cage at the seventh week of gestation has also been invoked as a cause of cervical ectopy of the aortic arch.* D’Cruz et al considered CAA to be the result of a confluence of the third and fourth arches as a result of anomalous growth of the pharyngeal pouch tissue, along with failure of the normal fourth arch to descend into the thorax with the heart.3
A good reason to separate CAA from the other forms of anomalous aortic arch is that its unusual connections confirm some of the views that have been expressed as being responsible for the mal- development of aortic arch (Felson, Letter from the Editor, p 69). For example, the separate
ABBREVIATIONS
CAA, cervical aortic arch PA, posteroanterior RSA, right subclavian artery LSA, left subclavian artery
From the Departments of Radiology and Pediatrics, Uni- versity of Cincinnati, College of Medicine, and the Depart-
ment of Radiology. Children’s Hospital Medical Center, Cincinnati.
tDr Felson died Ott 22. 1988. Benjamin Felson: Professor Emeritus of Radiology. Uni-
versity of Cincinnati College of Medicine, Janet L. Strife: Associate Professor of Pediatric Radiology, Children’s Hos- pital Medical Center.
Address reprint requests to Janet L. Strife, MD. Depart- ment of Radiology, Children’s Hospital Medical Center, Cincinnati, OH 45229-2899.
0 1989 by W.B. Saunders Company. 0037-198X/89/2401-0007$5.00/0
origins of the internal and external carotid arteries without an intervening common carotid or subclavian artery afford strong evidence to support the third aortic arch theory. The origin of the vertebral artery directly from the cervical aorta rather than from the subclavian artery lends further validity to this theory. Obviously the missing common carotid and subclavian artery segments must have been incorporated in the anomalous third arch, so that they have already been “used up,” thus their branches arise directly from the aortic arch rather than from the normal parent artery. 2*4 McCue et al noted that the dorsal aorta segment between the third and fourth aortic arches is called the ductus caroticus and normally persists into adult life.’
To our knowledge, the first clinical report of cervical aortic arch was published in 1947 by Beavan and Fatti.* The patient died following ligation of a CAA that had been mistaken for an aneurysm of the right innominate artery. We have been able to find about 50 cases of CAA reported in the literature since that time, includ- ing the two by Predey (p 96) and three of our own, included in this article.
There is no clear sex preponderance. Many of the patients have been asymptomatic. Dys- phagia is the most common symptom. Wheezing, coughing, stridor, choking, apneic spells, and repeated bouts of aspiration pneumonia have been reported, generally attributable to compres- sion of the esophagus or trachea by a vascular ring. Swallowing problems are more common in patients who have a documented ductus or liga- mentum.
The CAA is generally palpable in the right or left supraclavicular area, occasionally higher. Good femoral pulsation is generally noted, but in several cases compression of the supraclavicular mass sometimes caused the femoral pulses to decrease or disappear.537-q A murmur or thrill is sometimes encountered over the cervical mass. Occasionally, a blood pressure differential is noted in the two arms. The weakened or absent radial pulse always occurs on the side contralat- era1 to the CAA. A subclavian steal syndrome has been reported.”
Cardiac anomalies may occasionally accom-
114 Seminars in Roentgenology, Vol XXIV, No 2 (April), 1989: pp 114- 120

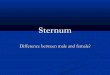
Fig 1. (A) Chest radiograph demonstrates abnormal widening of the mediistinum bikerally. The deacembng aorta appears to be right sided. (6) Lateral barium asophagram showing the large posterior indantation of the m&d portion of the esophagus. (Cj The injection was made with the catheter just above the aortic vafva. The right ascem6q aarta, the left cervical aortic arch, the transverse portion of the aortic arch. and subsequent filling of a right-aided dueem&g aorta is seen. (II) This injaction into the diverticulum demonstrates the origin of the right aubcfmdian artery. Thia dke&auhe’n was “hidden” on the previous arteriogram by the ascending aorta. 63 A line representation of the vasouiar anatomy in thie patient with left cervical aortic arch. RCC, right common carotid; LCC, left common carotid; V, vertebral. (Reprinted wfth permission from Bissat OS at al: Vascular rings: Magnetic resonance imaging, AJR 1987; 149:261-6.0 by Williams & Wilkins Co.“)

116 FELSON AND STRIFE
E
Descending aorte
Fig 1. (Cont’d).
parry CAA. Tetralogy of Fallot,‘“*” pulmonary atresia with VSD (pseudotruncus),43’0 double outlet right ventricle,” ventricular septal defect,“*” and occasionally patent ductus arteriosus may be associated. The descending aorta may have coarctation and obstruc- tion~~s~13*i4
CASE MATERIAL
Case 1: (Previously Reported)” This 3r,&year-old white boy had had dysphagia associated
with frequent upper respiratory infections since birth. A pulsating mass was palpable in the left side of the neck.
PA chest radiographs (Fig IA) showed widening of both the right and left upper mediastinum. The entire trachea was shifted to the right but not indented. The aorta descended along the right side of the spine and appeared to be very wide. The superior border of the mediastinum was obscured as it extended above the clavicles. On the left side this conformed to the palpable pulsating cervical mass. Barium eaophagram (Fig 1 B) showed a large extrinsic mass indenting and displac- ing the posterior border of the middle third of the esophagus. Aortography performed from the right femoral artery (Fig 1C) showed a curious course of the thoracic aorta. The left-sided abdominal aorta deviated to the right at the diaphragm, so that the lower descending thoracic aorta was entirely right-sided. Midway up the thorax the aorta abruptly crossed to the left of the spine and extended upward into a CAA in the left supraclavicular fossa. The aorta then turned downward and to the right to become the ascending aorta within the cardiac silhouette.
Contrast injection performed with the catheter tip in the upper descending aorta showed the midline crossing toward the left CAA. A diverticulum arose from the upper end of the descending thoracic aorta and gave origin to a normal- calibered RSA (Fig 1D). The first vessel arising from the aortic arch was a large common carotid artery. The next vessel was either a left common or internal carotid artery. The next was an external carotid or vertebral artery. The last vessel was the LSA. Figure 1E is a diagrammatic representa- tion of these findings.
At operation the angiographic findings were confirmed. A ductus arteriosus extended to the right pulmonary artery. This was ligated and released surgically. The postoperative esophagram still showed the posterior defect from the retro- esophageal segment of the aorta. The child improved clini- cally and is doing well after 9 years.
Case 2 This adolescent had a pulsating mass discovered in the left
supraclavicufar fossa. The plain film (Fig 2A) shows the aortic arch in normal position but somewhat dilated. The descending aorta, also dilated, is left-sided. The trachea and esophagus are slightly deviated to the right but not indented. The lateral view (Fig 2B) shows no tracheal or esophageal displacement or indentation whatsoever.
Contrast injection in the distal thoracic aorta (Fig 2C) shows a diverticulum at the top of the descending aorta, giving origin to a normal LSA. Catheter arteriography of the ascending aorta (Fig 2D) shows a normal ascending aorta, normal innominate artery, REA, and both carotid arteries. Beyond this is the diverticulum that extends well above the left clavicle and accounts for the pulsating mass.
Comment: This is an extremely uncommon variant. There are, in effect, two aortic arches on the left: a normal one and the diverticulum. The pulsating left neck mass was the diverticulum, and was not truly a cervical arch. A similar case was previously reported from this institution. That patient had a linear posterior esophageal defect and an absent right radial pulse, indicating an anomalous right subclavian artery.”
Case 3 This young adult had a pulsating right supraclavicular
mass. Injections into the ascending and descending aorta via a left femoral catheter reveal a somewhat dilated left descending aorta (Figs 3A and 3B). An anomalous right subclavian artery arisea from a diverticufum of the aortic arch (Fig 3C). There may be a small aneurysm or band in the right subclavian or one of its branches. We have no record that a blood pressure study was obtained from the right arm. The right and left carotid arteries took theii origin more or less in normal fashion from the aortic arch as did the left subctavian artery.
PATHOLOGIC AND RADIOLOGIC ANATOMY
In view of their similarity, the pathologic anatomy and radiographic depiction of CAA are combined in this description. A review of the reported cases of CAA, the cases reported by Predey et al (p 96), and our own material in-

12. (A)Thaaorticbmobappaarsln nomnllposRlM.atthough~twidrwd. Ms~Tbalstad~~ tatlononthatrschaor m. (ClDhaddumof~00rta~0rlglntoalaft~atary. o a normal aswndlng aorta a normal innominata artery, RSA, and both carotid arteries.
sno lOI

118 FELSON AN0 STRIFE
Fig 3. W Injection into ascending aorta with origin of the left carotid artery. (B) Descending aorta visualized with filling of diverticulum and right subclavian artery (arrow) that appears tor- tuous. (C) Injection in the high descending aorta

CERVICAL AORTIC ARCH: A COMMENTARY 119
eludes 45 cases.6*8*12 These cases all involve an anomalous CAA, not merely a dilated artery in the neck. A fairly consistent complex of findings is encountered. These include:
1. Cervical position of the apex of the aortic arch on the right or left, usually in the supracla- vicular region but sometimes quite high in the neck.
2. Separate origin of the carotid arteries con- tralateral to the side of the CAA,* with absence of a contralateral innominate artery.
3. The contralateral subclavian artery usually has an anomalous origin from the aortic isthmus or the upper end of the descending thoracic aorta, often via an aortic diverticulum (Figs 1 D and 3C).
4. The ipsilateral carotid and subclavian arteries show a less consistent pattern than their contralateral counterparts. Separate external and internal carotid arteries are commonly seen, and occasionally a separate ipsilateral vertebral artery arises directly from the arch.
5. The distal aortic arch generally crosses the midline to reach the descending aorta, which usually lies on the contralateral side (Fig 1C). In doing so, it usually indents the middle third of the esophagus from behind (Fig 1 B). The CAA itself often indents or displaces the upper esophagus and trachea ipsilaterally in the frontal view (Figs 1A and 2A). It may also cause a large posterior esophageal defect on the lateral view. Whenever such a defect is demonstrated, an aortic divertic- ulum is responsible. This posterior defect some- times disappears after release of the ductus or anomalous subclavian artery when a vascular ring is present, but the defect itself probably results from traction exerted on the diverticulum pulling it behind the esophagus by the ductus or anomalous subclavian artery.
6. In those cases in which a ligament or ductus was documented, it arose from the upper descending aorta and extended to the ipsilateral pulmonary artery (documented at surgery). Most of the cases with an open or closed ductus had clinical signs consistent with a vascular ring.
7. The ductus or ligamentum arteriosus is often, if not always, on the contralateral side.
*The terms contralateral and ipsilateral refer to the side on which the CAA is found. Thus with right CAA, contralateral indicates the left side.
8. An aortic diverticulum is quite common with CAA. This persistent segment of aortic arch has been discussed elsewhere. It is always on the contralateral side of the complete CAA. It almost invariably is the site of origin of the subclavian artery. Some patients have a stenotic or atretic origin of this contralateral anomalous subclavian artery.16 This results in reduction or absence of the contralateral pulse and accounts for the blood pressure differential sometimes noted in the two arms. As stated, a subclavian steal syndrome may be present.
9. The position of the descending thoracic aorta in relationship to the spine varies consider- ably in CAA. Table 1 illustrates the relationship of the descending aorta to the side of the CAA in the 45 cases we reviewed. The lower two thirds of the esophagus may be deviated to the left of the midline by the right descending aorta. From Table 1 it is apparent that there were a total 25 cases of right CAA and 20 cases on the left. A left descending aorta was present in 33 cases (73%) as compared to a right descending aorta in 12 (27%). The descending aorta was contralat- era1 to the CAA in 29 of the 45 cases (64%) and ipsilateral in 16 (35%). In over half the cases in which the upper end of the descending aorta was described, an aortic diverticulum giving origin to an anomalous subclavian artery that supplied the contralateral arm was found.
10. Associated congenital heart disease was encountered occasionally. Curiously, two cases’,” had stenosis of the left pulmonary artery at its origin along with right ventricular hyper- trophy, and both had a left CAA.
DIFFERENTIAL DIAGNOSIS
There is little problem in the differential diag- nosis of CAA if one is aware of the entity. Aneurysm of the aorta or one of its branches, particularly the innominate or carotid artery, certainly can produce a pulsating vessel in the neck. The same applies to buckling of the great vessels.
Tabie 1. Relatiin of CAA to Deeoending Aorta
Type SdsOfCAA !3ida d D-ding Aate C&E-S
I R L 21
II R R 4
Ill L R 8
IV L L 129
‘All had an innominate kxechiiephalic) artery.
Abbreviations: CAA, cervical acwtic arch: R, right; L, left.

120
However, an aortic arch may extend into the neck under certain circumstances, yet not qualify as a conventional CAA. For example, pseudo- coarctation of the aorta is often associated with elongation, and the pulsating aortic arch may extend into the neck. The same applies to right aortic arch itself, a common anomaly that mirror images left aortic arch with anomalous right subclavian artery. This form of right aortic arch occasionally extends above the clavicle. The same applies to the right-sided arch of double aortic arch and to various types of aortic divertic- ulum, as in Cases 2 and 3. Furthermore, a high surgical or intrathoracic looping of the aortic arch may occur as in the two cases of Predey and others in the literature.
Absence of an aortic knob at its usual site, descending aorta on the wrong side, posterior indentation of the trachea, and a large posterior defect on the mid-third of the back of the esopha- gus will establish the diagnosis even without
FELSON AND STRIFE
recourse to angiography, particularly if the aor- tic diverticulum is visible.
Angiography will establish the diagnosis beyond doubt, demonstrating the abnormal sequence of the brachiocephalic vessels, the ret- roesophageal course of the aortic arch, and the contralateral descending aorta. The diagnostic features of CAA have been described with multi- ple imaging modalities, including two-dimen- sional echocardiography,” computerized tomog- raphy,” and magnetic resonance.15 Imaging the CAA is helpful if surgery is contemplated.
CAA, then, is a congenital anomaly consisting of cephalic displacement of an aortic arch, and unilateral, probably as the result of persistence of the third embryonic aortic arch with abnormal regression of the ipsilateral fourth arch. The condition is rare. The pathoradiologic findings are fairly consistent, and provide another link in the understanding of this fascinating group of anomalies of the thoracic aorta.
REFERENCES
1. Reid DC: Three examples of a right aortic arch. J Anat Physiol 1914;48:174-81
2. Beavan TED, Fatti L: Ligature of aortic arch in the neck. Br JSurg 1947;34:414-6
3. D’Cruz IA, Cantez T, Namin EP, et al: Right sided aorta. Br Heart J 1966;28:722-39
4. Cornali M, Reginato E, Azzolina G: Cervical aortic arch and a new type of double aortic arch: Report of a case. Br Heart J 1976;38:993-6
5. McCue CM, Mauck HP, Tingelstad JB, et al: Cervical aortic arch. Am J Dis Child 1973;125:738-42
6. Bourdon JL, Hoeffel JC, Worms AM, et al: The cervical aortic arch: A case with diffuse arterial dysplasia and neurocutaneous angiomatosis. Pediatr Radio1 1981;10:143- 50
7. Lipchick EO, Young LW: Unusual symptomatic aortic arch anomalies. Radiology 1967;80:85-90
8. Mullins CE, Gillette PC, McNamara DG: The complex of cervical aortic arch. Pediatrics 1973;s 1:210-5
9. Morgan MG, Glasser SP, Swain J, et al: Right cervical aortic arch and aortic stenosis: A case report. J La State Med
Sot 1976;128:281-3 10. Moncada R, Shannon M, Miller R, et al: The cervical
aorticarch. AJR 1975;125:591-601
11. Takao R, Imamura H, Koga Y, et al: Right-sided cervical aortic arch associated with tetralogy of Fallot and peculiar tortuosity of the descending aorta. Cardiovasc
Radio1 1979;2:51-4. 12. Haughton VM, Fellows KE, Rosenbaum AE: The
cervical aortic arches. Radiology 1975;114:675-81 13. Hellenbrand WE, Kelley MJ, Tamer NS, et al: Cervi-
cal aortic arch with retroesophageai aortic obstruction: Report of a case with successful surgical intervention. Ann Thorac Surg 1918;26:86-92
14. Tiraboschi R, Crupi G, Locatelli G, et al: Cervical aortic arch with aortic obstruction: Report of two cases. Thorax 1980;35:26-30
15. Bisset GS III, Strife JL, Kirks DR, et al: Vascular rings: MR Imaging. AJR 1987;149:251-6
16. Felson B, Cohen S, Courter SR, et al: Anomalous right subclavian artery. Radiology 1950;54:340-9
17. Mahoney EB, Manning JA: Congenital abnormalities of the aortic arch. Surgery 1964;55:1-14
18. D’Cruz IA, Stanley A, Vitullo D, et al: Noninvasive diagnosis of right cervical aortic arch. Chest 1983;83:820-2
19. Schiebler ML, Feuerstein IM, Paushter DM, et al: Computed tomography appearance of a right cervical aortic arch. Chest 1986;90:439-440


![Universal Airlinesuvairlines.com/admin/resources/RPVM.pdfN09 45.0 EIN 36.8 Descend to 5000' ROUTING 01.9 E124 18.0 Descend to 4000 Mcr [DJ5ØJj Descend to 4000 ROUTING STAR 17 [17]](https://img.pdfslide.us/doc/110x75/6094f01510b17f1bd676a982/universal-n09-450-ein-368-descend-to-5000-routing-019-e124-180-descend-to-4000.jpg)