Embed Size (px)
Citation preview
Oceania Care Company Limited - Maureen Plowman Rest Home
CURRENT STATUS: 07-Oct-13
The following summary has been accepted by the Ministry of Health as being an accurate reflection of the Certification audit conducted against the Health and Disability Services Standards – NZS8134.1:2008; NZS8134.2:2008 & NZS8134.3:2008 on the audit date(s) specified.
GENERAL OVERVIEW
Maureen Plowman Home is a 55 bed residential care facility located in Browns Bay Auckland. At this audit there are 54 residents receiving care. This includes 37 residents requiring rest home level care and 17 residents requiring dementia level care. The dementia unit is fully occupied. There have been no changes to management since the last audit. There have been no changes to the facility or grounds since the last audit with the exception of general maintenance.
At this audit there are eight areas identified as requiring improvement. These include: evidencing open disclosure; document control processes; and monitoring implementation of the quality and risk programme. Ensuring residents needs/outcome and goals and care plans are sufficiently detailed and individualised; ensuring assessments are sufficiently documented when residents in the dementia unit are suspected of having an infection; the staff medication competency assessment process; and ensuring all components of medication management practices meet required standards are areas requiring improvement.
AUDIT SUMMARY AS AT 07-OCT-13
Standards have been assessed and summarised below:
Key
Indicator Description Definition
Includes commendable elements above the required levels of performance
All standards applicable to this service fully attained with some standards exceeded
No short fallsStandards applicable to this service fully attained
Some minor shortfalls but no major deficiencies and required levels of performance seem achievable without extensive extra activity
Some standards applicable to this service partially attained and of low risk
Indicator Description Definition
A number of shortfalls that require specific action to address
Some standards applicable to this service partially attained and of medium or high risk and/or unattained and of low risk
Major shortfalls, significant action is needed to achieve the required levels of performance
Some standards applicable to this service unattained and of moderate or high risk
Consumer Rights Day of Audit
07-Oct-13
Assessment
Includes 13 standards that support an outcome where consumers receive safe services of an appropriate standard that comply with consumer rights legislation. Services are provided in a manner that is respectful of consumer rights, facilities, informed choice, minimises harm and acknowledges cultural and individual values and beliefs.
Some standards applicable to this service partially attained and of medium or high risk and/or unattained and of low risk
Organisational Management Day of Audit
07-Oct-13
Assessment
Includes 9 standards that support an outcome where consumers receive services that comply with legislation and are managed in a safe, efficient and effective manner.
Some standards applicable to this service partially attained and of low risk
Continuum of Service Delivery Day of Audit
07-Oct-13
Assessment
Includes 13 standards that support an outcome where consumers participate in and receive timely assessment, followed by services that are planned, coordinated, and delivered in a timely and appropriate manner, consistent with current legislation.
Some standards applicable to this service partially attained and of medium or high risk and/or unattained and of low risk
Safe and Appropriate Environment Day of Audit
07-Oct-13
Assessment
Includes 8 standards that support an outcome where services are provided in a clean, safe environment that is appropriate to the age/needs of the consumer, ensure physical privacy is maintained, has adequate space and amenities to facilitate independence, is in a setting appropriate to the consumer group and meets the needs of people with disabilities.
Standards applicable to this service fully attained
Restraint Minimisation and Safe Practice Day of Audit
07-Oct-13
Assessment
Includes 3 standards that support outcomes where consumers receive and experience services in the least restrictive and safe manner through restraint minimisation.
Standards applicable to this service fully attained
Infection Prevention and Control Day of Audit
07-Oct-13
Assessment
Includes 6 standards that support an outcome which minimises the risk of infection to consumers, service providers and visitors. Infection control policies and procedures are practical, safe and appropriate for the type of service provided and reflect current accepted good practice and legislative requirements. The organisation provides relevant education on infection control to all service providers and consumers. Surveillance for infection is carried out as specified in the infection control programme.
Standards applicable to this service fully attained
AUDIT RESULTS AS AT 07-OCT-13
Consumer Rights
There is a documented complaints process which is implemented to ensure all complaints are followed up and information is used as an opportunity to improve service delivery as appropriate.
The residents and family members interviewed express satisfaction with the manner in which the service respects their rights and report that they are treated with respect and dignity and are free from discrimination. As observed at the onsite audit, residents receive services that uphold their rights. Staff demonstrate understanding of their obligations regarding residents' rights and how to incorporate that knowledge into their day-to-day practices and interactions with residents and family/whānau.
The service meets the individual resident's culture, beliefs and values. Staff are provided with training on the treaty of Waitangi and provision of culturally appropriate care.
The service acknowledges that all residents have a right to full and frank information as identified in the open disclosure policy. Evidence that open disclosure is occurring following reportable events is not always evident in resident records reviewed and this is an area requiring improvement. An interpreter service is accessed through the district health board as required.
Written consent is gained as appropriate. Staff interviewed acknowledge the resident's right to make choices based on information presented to them and the right to withdraw consent and/or refuse treatment. Advance directives, advance care plans and end of life care planning are made available and acted upon where valid.
Organisational Management
The day to day operation of the facility is undertaken by a management team who are appropriately experienced and/or qualified.
The organisation's purpose, values, and mission are developed nationally and incorporated into the Maureen Plowman Home business plan. Organisation risks and hazards are documented, mitigation strategies identified and are monitored. Policies and procedures are developed corporately. An area for improvement is identified in relation to policy and procedure documentation control processes.
Documented quality and risk management systems are implemented to assist residents, visitors and staff safety. Quality is reviewed and measured via the internal audit schedule, complaints/compliments management, and resident satisfaction surveys. All quality and risk activities are monitored by the facility manager and corrective actions are put in place as appropriate. Incidents/accidents are being reported and managed. The reported rates are analysed and benchmarked as quality indicators with other Oceania Group residential care facilities on a monthly basis. Not all complaints are being included in the quality indicator data and the registers in individual resident files which summarise reported incidents/events are not current/complete. These are areas requiring improvement.
The service implements safe staffing levels and skill mix to ensure contractual requirements and residents' care needs are met. Human resources management processes are implemented and comply with the organisation's policies, reflect current good practice and meets legislative requirements. Staff members are required to complete the organisation's orientation programme. Knowledge and skills are maintained through on-going education which is frequent and appropriate to staff roles. Staff performance appraisals are being completed in a timely manner.
The service have a resident information system that complies with legislative requirements. There is no information of a private and personal nature publicly displayed.
Continuum of Service Delivery
Resident's entry into services is facilitated in a competent, equitable, timely, and respectful manner, when their need for services has been identified. Admission agreements are in place for all residents and sighted. The service is coordinated in a manner that promotes continuity in service delivery and promotes a team approach where appropriate. The clinical leader (CL) notifies the general practitioner (GP) in a timely manner in the event that a resident manifests medical problems that require immediate attention. Each resident's person centred care plan (PCCP) is reviewed every six months through a Multi-Disciplinary Meeting. Assessments of individual resident individual, cultural and spiritual needs are not adequately documented. The PCCP's are not sufficiently detailed on occasions. These are areas requiring improvement. Despite this, the residents and family members interviewed verify the residents individual needs are being met. Evaluations detailing the residents response to changes in treatment/care is occurring with one exception noted. While interventions are provided; ongoing evaluation is not adequately documented when a resident is suspected of having an infection in the dementia unit and requires improvement. Activity plans are evaluated in a timely manner. The Dementia Unit has different activities appropriate to needs of the residents. The facility utilises a Resident Transfer Form which is
included in the Yellow Envelope when the resident needs to admitted in public hospital, or when transferred to another facility. The resident's PCCP is also attached with the Resident Transfer Form. Not all components of medication management practices meet professional and legislative requirements and requires improvement. While processes are implemented to assess staff competency for medication administration the assessment process does not include controlled drugs and requires improvement.
Safe and Appropriate Environment
Maureen Plowman Home has clearly documented emergency response processes which are understood and implemented by the service as required. The service has an approved fire evacuation plan and six monthly fire evacuation drills are conducted. There is at least one staff member (normally more) on duty with a current first aid certificate at all times.
The building has a current building warrant of fitness and ongoing checks to maintain the building warrant of fitness are being undertaken. All clinical equipment has a current performance monitoring label and electrical safety testing of appliances/equipment is occurring.
The facilities are fit for purpose (including the provision of a secure dementia unit) and provides appropriate furnishings and equipment. All resident bedrooms are single occupancy. There are sufficient toilets and showers present.
The dining, lounge and activities areas in the rest home and the dementia unit meet residents' relaxation, activity and dining needs. Calls bells are located in all residents' rooms and bathroom areas.
The facility is predominantly heated centrally and ventilation occurs via opening the doors and windows. A number of resident rooms and the lounge in the dementia unit also have heaters present. There are appropriate outdoor areas (including courtyards) that have seating and are sheltered for residents' use. There is a secure courtyard for use by residents in the secure dementia unit.
Restraint Minimisation and Safe Practice
Maureen Plowman Home maintains a process for determining approval of all types of restraint used, restraint processes, duration of restraint, and on-going education on restraint use and this processes is made known to service providers and others. Restraint policies and procedures are sighted and implemented. Restraint is included in the PCCP which includes risk management plan, the duration of which the restraint will be used and the type of restraint to be used. Evaluations are documented and sighted.
Infection Prevention and Control
The facility has a clearly defined infection prevention and control programme that is reviewed annually. Infection control is part of health and safety meeting every month. Surveillance for infection is carried out in accordance with agreed objectives, priorities, and methods that have been specified in the infection control programme. The surveillance result is communicated to the staff during staff meetings as well as to management through the IntraNet. They have an intensive infection control programme which is appropriate for the size of the facility.
Maureen Plowman HomeOceania Care Company Ltd
Certification audit - Audit ReportAudit Date: 07-Oct-13
Audit ReportTo: HealthCERT, Ministry of Health
Provider Name Oceania Care Company Ltd
Premise Name Street Address Suburb City
Maureen Plowman Home 2 Valley Rd Browns Bay AUCKLAND
Proposed changes of current services (e.g. reconfiguration):
Type of Audit Certification audit and (if applicable)
Date(s) of Audit Start Date: 07-Oct-13 End Date: 08-Oct-13
Designated Auditing Agency
Health Audit (NZ) Limited
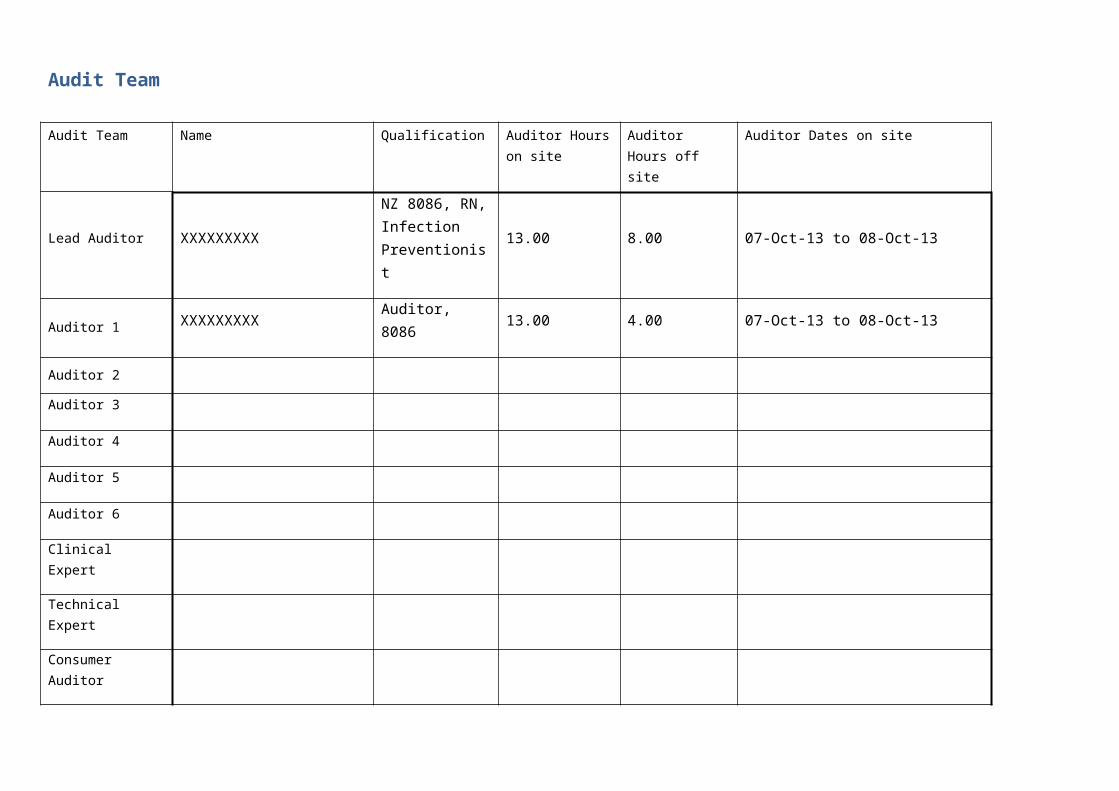
Audit Team
Audit Team Name Qualification Auditor Hours on site
Auditor Hours off site
Auditor Dates on site
Lead Auditor XXXXXXXXXNZ 8086, RN, Infection Preventionist
13.00 8.00 07-Oct-13 to 08-Oct-13
Auditor 1 XXXXXXXXX Auditor, 8086 13.00 4.00 07-Oct-13 to 08-Oct-13
Auditor 2
Auditor 3
Auditor 4
Auditor 5
Auditor 6
Clinical Expert
Technical Expert
Consumer Auditor
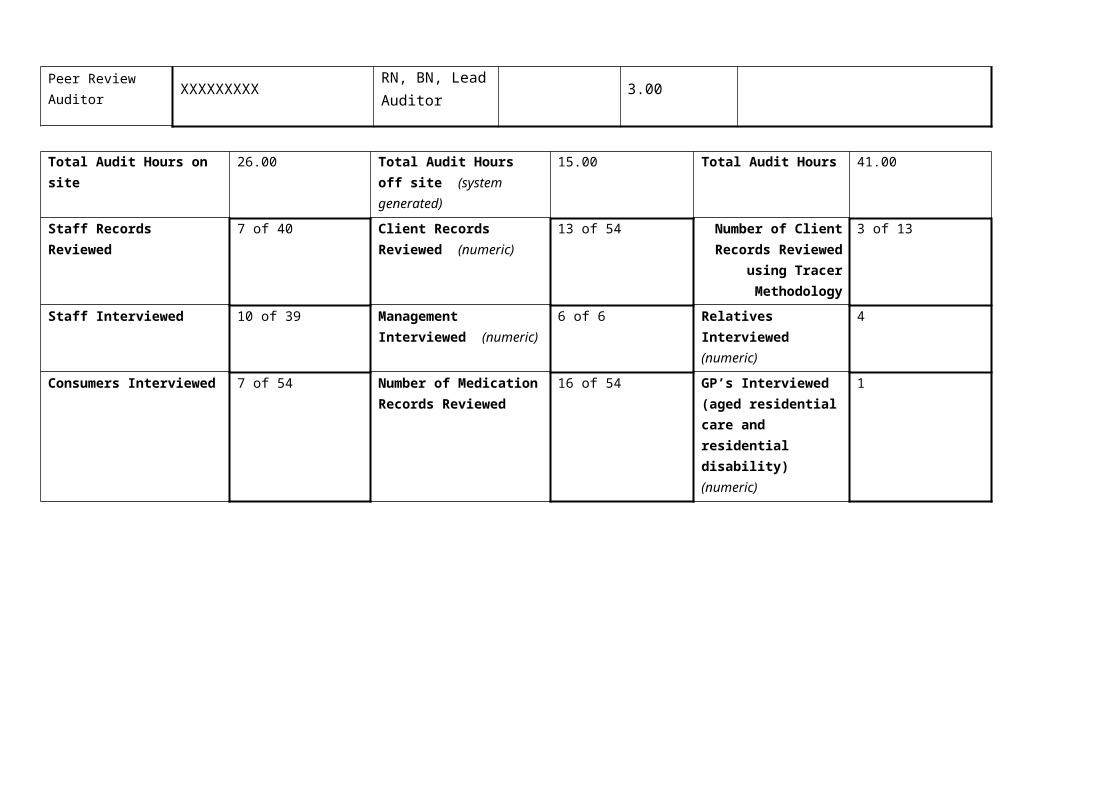
Peer Review Auditor XXXXXXXXX
RN, BN, Lead Auditor
3.00
Total Audit Hours on site 26.00 Total Audit Hours off site (system generated)
15.00 Total Audit Hours 41.00
Staff Records Reviewed 7 of 40 Client Records Reviewed (numeric)
13 of 54 Number of Client Records Reviewed
using Tracer Methodology
3 of 13
Staff Interviewed 10 of 39 Management Interviewed (numeric)
6 of 6 Relatives Interviewed (numeric)
4
Consumers Interviewed 7 of 54 Number of Medication Records Reviewed
16 of 54 GP’s Interviewed (aged residential care and residential disability) (numeric)
1
Declaration
I, (full name of agent or employee of the company) XXXXXXXXX (occupation) Director of (place) Auckland hereby submit this audit report pursuant to section 36 of the Health and Disability Services (Safety) Act 2001 on behalf ofHealth Audit (NZ) Limited, an auditing agency designated under section 32 of the Act.
I confirm that Health Audit (NZ) Limitedhas in place effective arrangements to avoid or manage any conflicts of interest that may arise.
Dated this 17 day of October 2013
Please check the box below to indicate that you are a DAA delegated authority, and agree to the terms in the Declaration section of this document.
This also indicates that you have finished editing the document and have updated the Summary of Attainment and CAR sections using the instructions at the bottom of this page.
Click here to indicate that you have provided all the information that is relevant to the audit:
The audit summary has been developed in consultation with the provider:
Electronic Sign Off from a DAA delegated authority (click here):
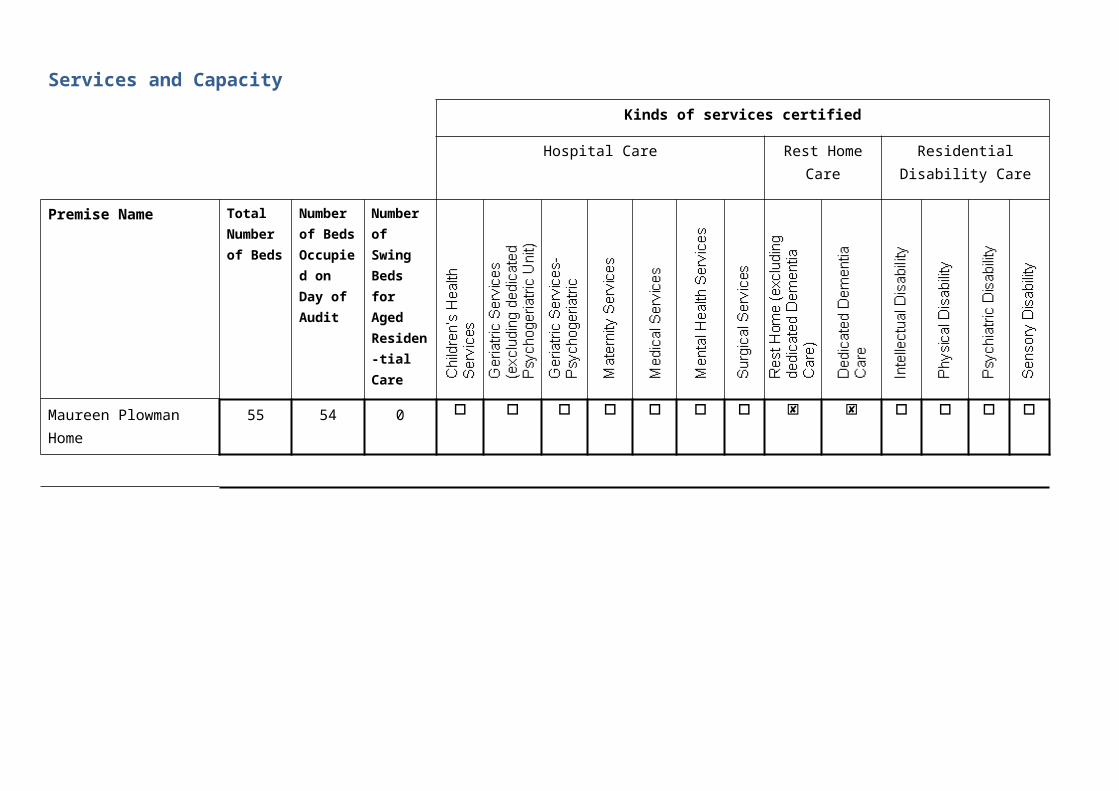
Services and Capacity
Kinds of services certified
Hospital Care Rest Home Care
Residential Disability Care
Premise Name Total Number of Beds
Number of Beds Occupied on Day of Audit
Number of Swing Beds for Aged Residen-tial Care
Maureen Plowman Home
55 54 0
Executive Summary of Audit
General OverviewMaureen Plowman Home is a 55 bed residential care facility located in Browns Bay Auckland. At this audit there are 54 residents receiving care. This includes 37 residents requiring rest home level care and 17 residents requiring dementia level care. The dementia unit is fully occupied. There have been no changes to management since the last audit. There have been no changes to the facility or grounds since the last audit with the exception of general maintenance.At this audit there are eight areas identified as requiring improvement. These include: evidencing open disclosure; document control processes; and monitoring implementation of the quality and risk programme. Ensuring residents needs/outcome and goals and care plans are sufficiently detailed and individualised; ensuring assessments are sufficiently documented when residents in the dementia unit are suspected of having an infection; the staff medication competency assessment process; and ensuring all components of medication management practices meet required standards are areas requiring improvement.
1.1 Consumer RightsThere is a documented complaints process which is implemented to ensure all complaints are followed up and information is used as an opportunity to improve service delivery as appropriate.The residents and family members interviewed express satisfaction with the manner in which the service respects their rights and report that they are treated with respect and dignity and are free from discrimination. As observed at the onsite audit, residents receive services that uphold their rights. Staff demonstrate understanding of their obligations regarding residents' rights and how to incorporate that knowledge into their day-to-day practices and interactions with residents and family/whānau. The service meets the individual resident's culture, beliefs and values. Staff are provided with training on the treaty of Waitangi and provision of culturally appropriate care.The service acknowledges that all residents have a right to full and frank information as identified in the open disclosure policy. Evidence that open disclosure is occurring following reportable events is not always evident in resident records reviewed and this is an area requiring improvement. An interpreter service is accessed through the district health board as required. Written consent is gained as appropriate. Staff interviewed acknowledge the resident's right to make choices based on information presented to them and the right to withdraw consent and/or refuse treatment. Advance directives, advance care plans and end of life care planning are made available and acted upon where valid.
1.2 Organisational ManagementThe day to day operation of the facility is undertaken by a management team who are appropriately experienced and/or qualified.The organisation's purpose, values, and mission are developed nationally and incorporated into the Maureen Plowman Home business plan. Organisation risks and hazards are documented, mitigation strategies identified and are monitored. Policies and procedures are developed corporately. An area for improvement is identified in relation to policy and procedure documentation control processes.
Documented quality and risk management systems are implemented to assist residents, visitors and staff safety. Quality is reviewed and measured via the internal audit schedule, complaints/compliments management, and resident satisfaction surveys. All quality and risk activities are monitored by the facility manager and corrective actions are put in place as appropriate. Incidents/accidents are being reported and managed. The reported rates are analysed and benchmarked as quality indicators with other Oceania Group residential care facilities on a monthly basis. Not all complaints are being included in the quality indicator data and the registers in individual resident files which summarise reported incidents/events are not current/complete. These are areas requiring improvement. The service implements safe staffing levels and skill mix to ensure contractual requirements and residents' care needs are met. Human resources management processes are implemented and comply with the organisation's policies, reflect current good practice and meets legislative requirements. Staff members are required to complete the organisation's orientation programme. Knowledge and skills are maintained through on-going education which is frequent and appropriate to staff roles. Staff performance appraisals are being completed in a timely manner.The service have a resident information system that complies with legislative requirements. There is no information of a private and personal nature publicly displayed.
1.3 Continuum of Service DeliveryResident’s entry into services is facilitated in a competent, equitable, timely, and respectful manner, when their need for services has been identified. Admission agreements are in place for all residents and sighted. The service is coordinated in a manner that promotes continuity in service delivery and promotes a team approach where appropriate. The clinical leader (CL) notifies the general practitioner (GP) in a timely manner in the event that a resident manifests medical problems that require immediate attention. Each resident’s person centred care plan (PCCP) is reviewed every six months through a Multi-Disciplinary Meeting. Assessments of individual resident individual, cultural and spiritual needs are not adequately documented. The PCCP's are not sufficiently detailed on occasions. These are areas requiring improvement. Despite this, the residents and family members interviewed verify the residents individual needs are being met. Evaluations detailing the residents response to changes in treatment/care is occurring with one exception noted. While interventions are provided; ongoing evaluation is not adequately documented when a resident is suspected of having an infection in the dementia unit and requires improvement. Activity plans are evaluated in a timely manner. The Dementia Unit has different activities appropriate to needs of the residents. The facility utilises a Resident Transfer Form which is included in the Yellow Envelope when the resident needs to admitted in public hospital, or when transferred to another facility. The resident’s PCCP is also attached with the Resident Transfer Form. Not all components of medication management practices meet professional and legislative requirements and requires improvement. While processes are implemented to assess staff competency for medication administration the assessment process does not include controlled drugs and requires improvement.
1.4 Safe and Appropriate EnvironmentMaureen Plowman Home has clearly documented emergency response processes which are understood and implemented by the service as required. The service has an approved fire evacuation plan and six monthly fire evacuation drills are conducted. There is at least one staff member (normally more) on duty with a current first aid certificate at all times.The building has a current building warrant of fitness and ongoing checks to maintain the building warrant of fitness are being undertaken. All clinical equipment has a current performance monitoring label and electrical safety testing of appliances/equipment is occurring.
The facilities are fit for purpose (including the provision of a secure dementia unit) and provides appropriate furnishings and equipment. All resident bedrooms are single occupancy. There are sufficient toilets and showers present. The dining, lounge and activities areas in the rest home and the dementia unit meet residents' relaxation, activity and dining needs. Calls bells are located in all residents' rooms and bathroom areas. The facility is predominantly heated centrally and ventilation occurs via opening the doors and windows. A number of resident rooms and the lounge in the dementia unit also have heaters present. There are appropriate outdoor areas (including courtyards) that have seating and are sheltered for residents' use. There is a secure courtyard for use by residents in the secure dementia unit.
2 Restraint Minimisation and Safe PracticeMaureen Plowman Home maintains a process for determining approval of all types of restraint used, restraint processes, duration of restraint, and on-going education on restraint use and this processes is made known to service providers and others. Restraint policies and procedures are sighted and implemented. Restraint is included in the PCCP which includes risk management plan, the duration of which the restraint will be used and the type of restraint to be used. Evaluations are documented and sighted.
3. Infection Prevention and ControlThe facility has a clearly defined infection prevention and control programme that is reviewed annually. Infection control is part of health and safety meeting every month. Surveillance for infection is carried out in accordance with agreed objectives, priorities, and methods that have been specified in the infection control programme. The surveillance result is communicated to the staff during staff meetings as well as to management through the IntraNet. They have an intensive infection control programme which is appropriate for the size of the facility.
Summary of Attainment
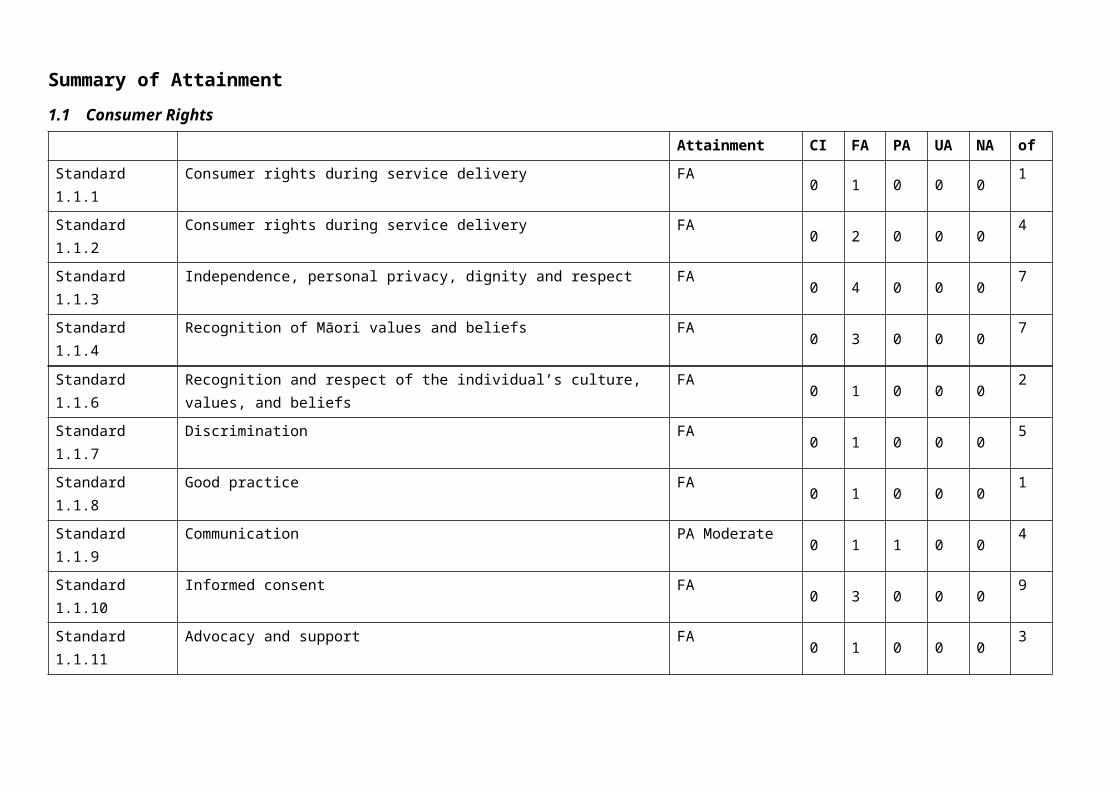
1.1 Consumer Rights
Attainment CI FA PA UA NA ofStandard 1.1.1 Consumer rights during service delivery FA 0 1 0 0 0 1
Standard 1.1.2 Consumer rights during service delivery FA 0 2 0 0 0 4
Standard 1.1.3 Independence, personal privacy, dignity and respect FA 0 4 0 0 0 7
Standard 1.1.4 Recognition of Māori values and beliefs FA 0 3 0 0 0 7
Standard 1.1.6 Recognition and respect of the individual’s culture, values, and beliefs FA 0 1 0 0 0 2
Standard 1.1.7 Discrimination FA 0 1 0 0 0 5
Standard 1.1.8 Good practice FA 0 1 0 0 0 1
Standard 1.1.9 Communication PA Moderate 0 1 1 0 0 4
Standard 1.1.10 Informed consent FA 0 3 0 0 0 9
Standard 1.1.11 Advocacy and support FA 0 1 0 0 0 3
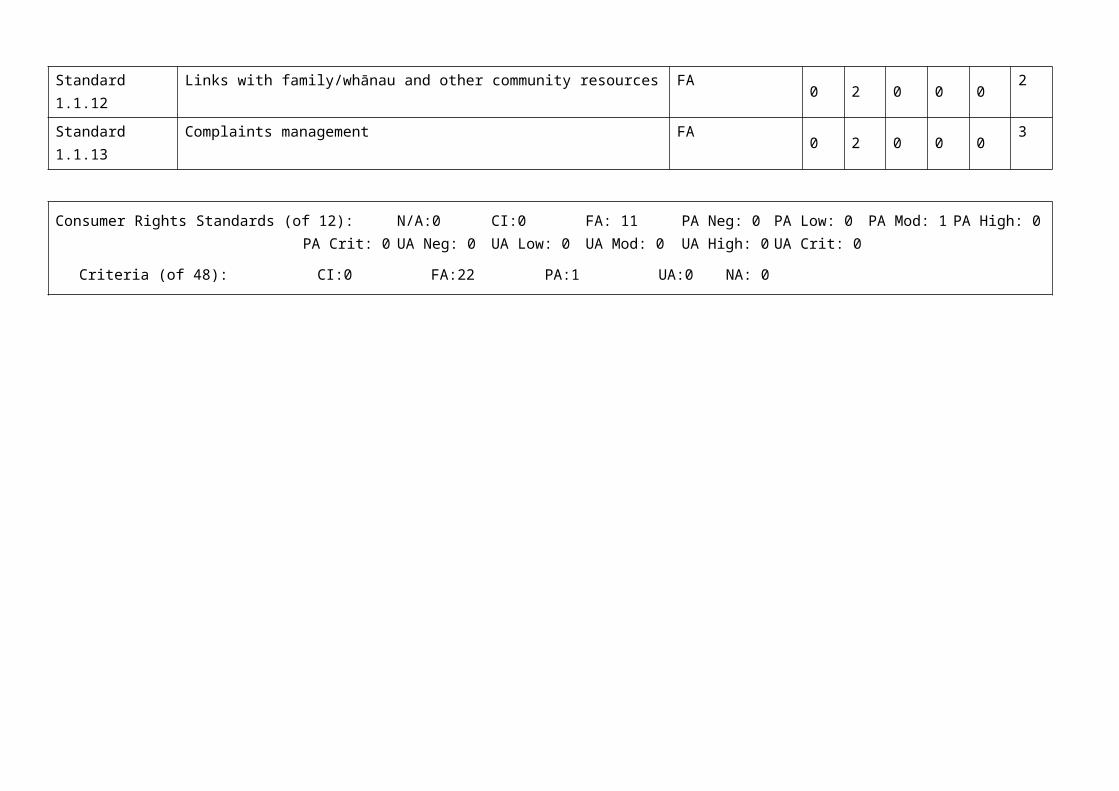
Standard 1.1.12 Links with family/whānau and other community resources FA 0 2 0 0 0 2
Standard 1.1.13 Complaints management FA 0 2 0 0 0 3
Consumer Rights Standards (of 12): N/A:0 CI:0 FA: 11 PA Neg: 0 PA Low: 0 PA Mod: 1 PA High: 0 PA Crit: 0UA Neg: 0 UA Low: 0 UA Mod: 0 UA High: 0 UA Crit: 0
Criteria (of 48): CI:0 FA:22 PA:1 UA:0 NA: 0
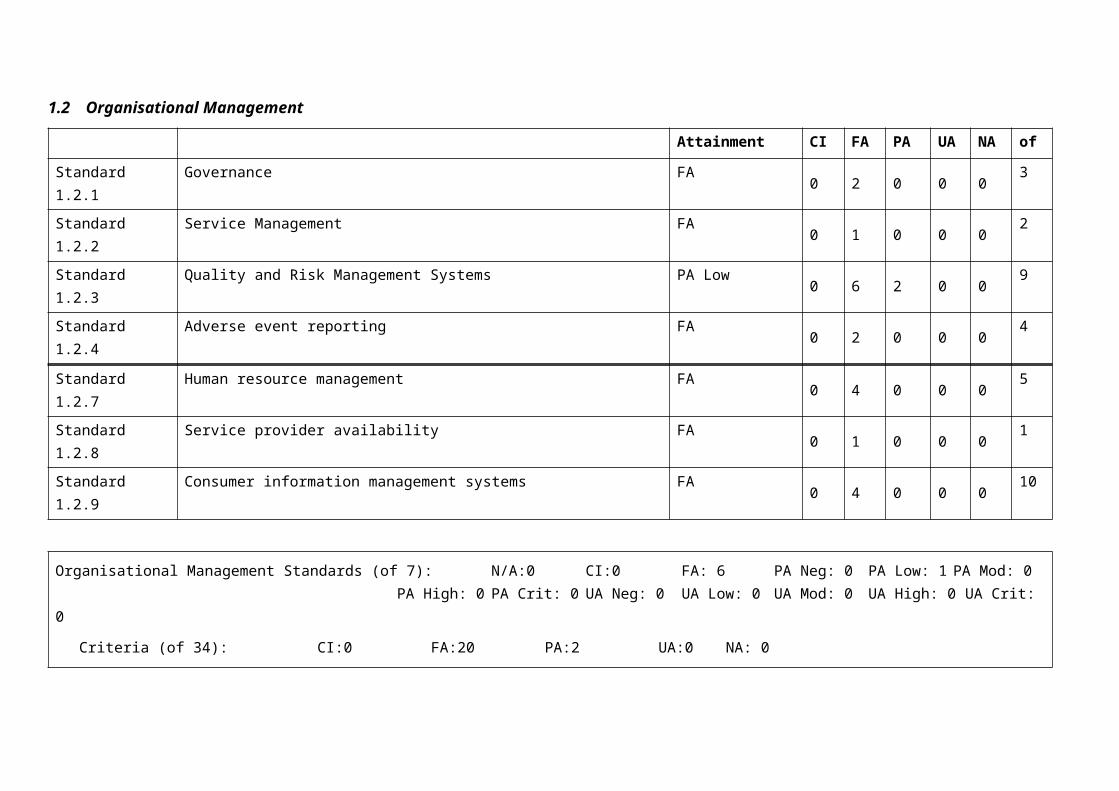
1.2 Organisational Management
Attainment CI FA PA UA NA of
Standard 1.2.1 Governance FA 0 2 0 0 0 3
Standard 1.2.2 Service Management FA 0 1 0 0 0 2
Standard 1.2.3 Quality and Risk Management Systems PA Low 0 6 2 0 0 9
Standard 1.2.4 Adverse event reporting FA 0 2 0 0 0 4
Standard 1.2.7 Human resource management FA 0 4 0 0 0 5
Standard 1.2.8 Service provider availability FA 0 1 0 0 0 1
Standard 1.2.9 Consumer information management systems FA 0 4 0 0 0 10
Organisational Management Standards (of 7): N/A:0 CI:0 FA: 6 PA Neg: 0 PA Low: 1 PA Mod: 0 PA High: 0PA Crit: 0 UA Neg: 0 UA Low: 0 UA Mod: 0 UA High: 0 UA Crit: 0
Criteria (of 34): CI:0 FA:20 PA:2 UA:0 NA: 0
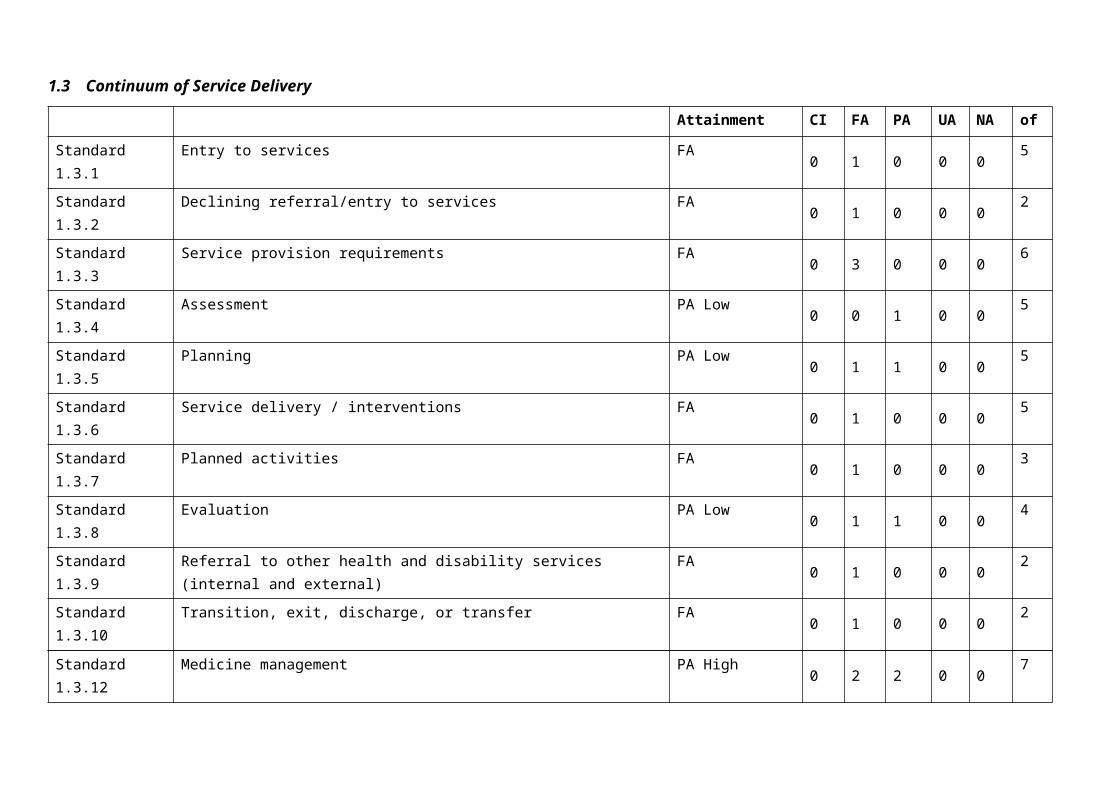
1.3 Continuum of Service Delivery
Attainment CI FA PA UA NA of
Standard 1.3.1 Entry to services FA 0 1 0 0 0 5
Standard 1.3.2 Declining referral/entry to services FA 0 1 0 0 0 2
Standard 1.3.3 Service provision requirements FA 0 3 0 0 0 6
Standard 1.3.4 Assessment PA Low 0 0 1 0 0 5
Standard 1.3.5 Planning PA Low 0 1 1 0 0 5
Standard 1.3.6 Service delivery / interventions FA 0 1 0 0 0 5
Standard 1.3.7 Planned activities FA 0 1 0 0 0 3
Standard 1.3.8 Evaluation PA Low 0 1 1 0 0 4
Standard 1.3.9 Referral to other health and disability services (internal and external) FA 0 1 0 0 0 2
Standard 1.3.10 Transition, exit, discharge, or transfer FA 0 1 0 0 0 2
Standard 1.3.12 Medicine management PA High 0 2 2 0 0 7
Standard 1.3.13 Nutrition, safe food, and fluid management FA 0 3 0 0 0 5
Continuum of Service Delivery Standards (of 12): N/A:0 CI:0 FA: 8 PA Neg: 0 PA Low: 3 PA Mod: 0 PA High: 1PA Crit: 0 UA Neg: 0 UA Low: 0 UA Mod: 0 UA High: 0 UA Crit: 0
Criteria (of 51): CI:0 FA:16 PA:5 UA:0 NA: 0
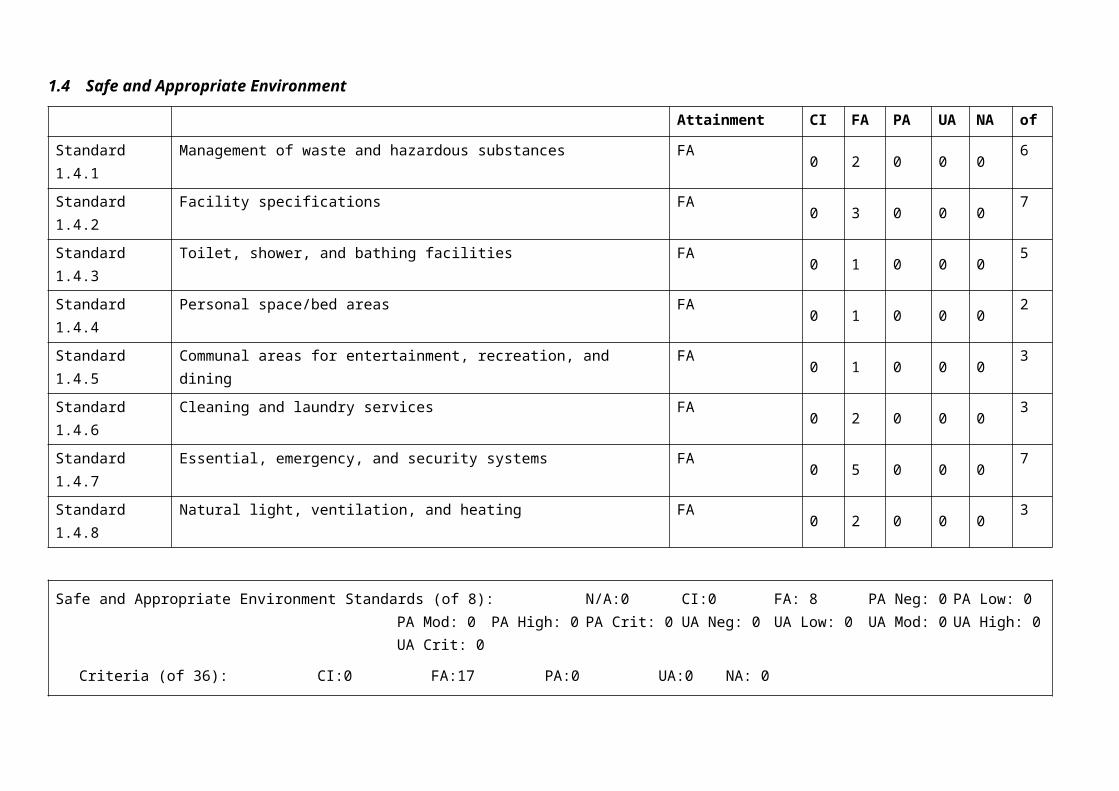
1.4 Safe and Appropriate Environment
Attainment CI FA PA UA NA of
Standard 1.4.1 Management of waste and hazardous substances FA 0 2 0 0 0 6
Standard 1.4.2 Facility specifications FA 0 3 0 0 0 7
Standard 1.4.3 Toilet, shower, and bathing facilities FA 0 1 0 0 0 5
Standard 1.4.4 Personal space/bed areas FA 0 1 0 0 0 2
Standard 1.4.5 Communal areas for entertainment, recreation, and dining FA 0 1 0 0 0 3
Standard 1.4.6 Cleaning and laundry services FA 0 2 0 0 0 3
Standard 1.4.7 Essential, emergency, and security systems FA 0 5 0 0 0 7
Standard 1.4.8 Natural light, ventilation, and heating FA 0 2 0 0 0 3
Safe and Appropriate Environment Standards (of 8): N/A:0 CI:0 FA: 8 PA Neg: 0 PA Low: 0 PA Mod: 0PA High: 0 PA Crit: 0 UA Neg: 0 UA Low: 0 UA Mod: 0 UA High: 0 UA Crit: 0
Criteria (of 36): CI:0 FA:17 PA:0 UA:0 NA: 0
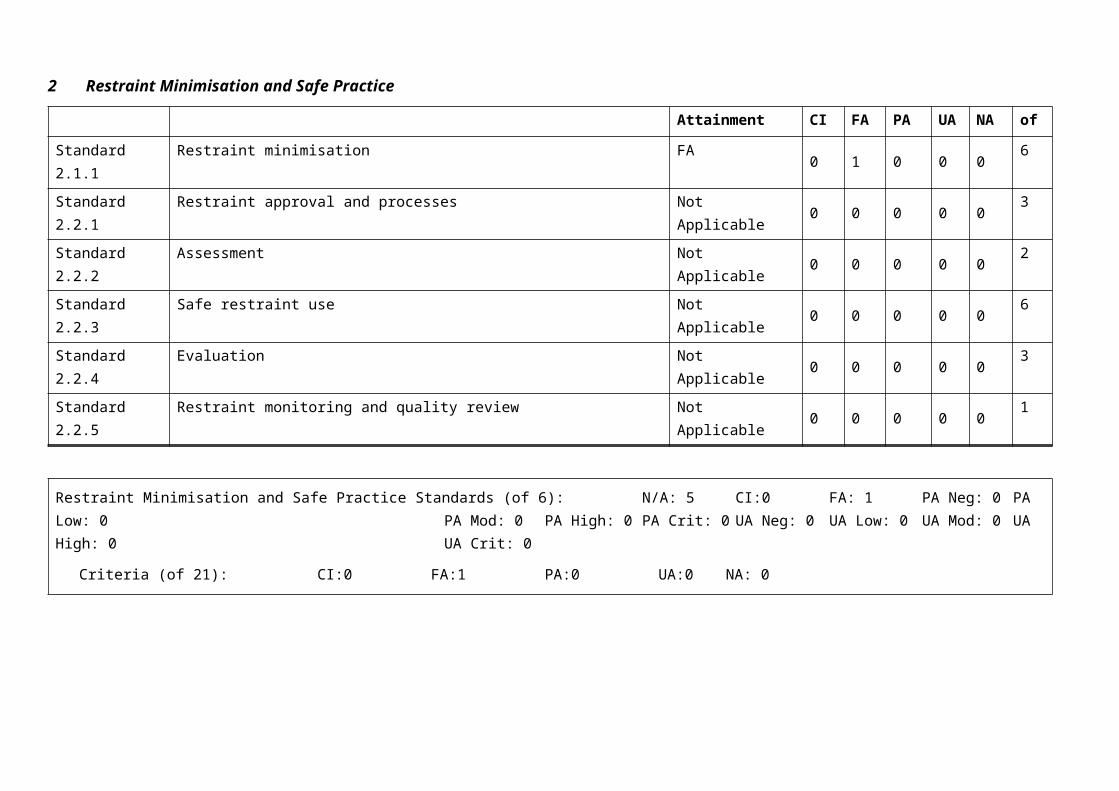
2 Restraint Minimisation and Safe Practice
Attainment CI FA PA UA NA of
Standard 2.1.1 Restraint minimisation FA 0 1 0 0 0 6
Standard 2.2.1 Restraint approval and processes Not Applicable 0 0 0 0 0 3
Standard 2.2.2 Assessment Not Applicable 0 0 0 0 0 2
Standard 2.2.3 Safe restraint use Not Applicable 0 0 0 0 0 6
Standard 2.2.4 Evaluation Not Applicable 0 0 0 0 0 3
Standard 2.2.5 Restraint monitoring and quality review Not Applicable 0 0 0 0 0 1
Restraint Minimisation and Safe Practice Standards (of 6): N/A: 5 CI:0 FA: 1 PA Neg: 0 PA Low: 0 PA Mod: 0 PA High: 0 PA Crit: 0 UA Neg: 0 UA Low: 0 UA Mod: 0 UA High: 0 UA Crit: 0
Criteria (of 21): CI:0 FA:1 PA:0 UA:0 NA: 0
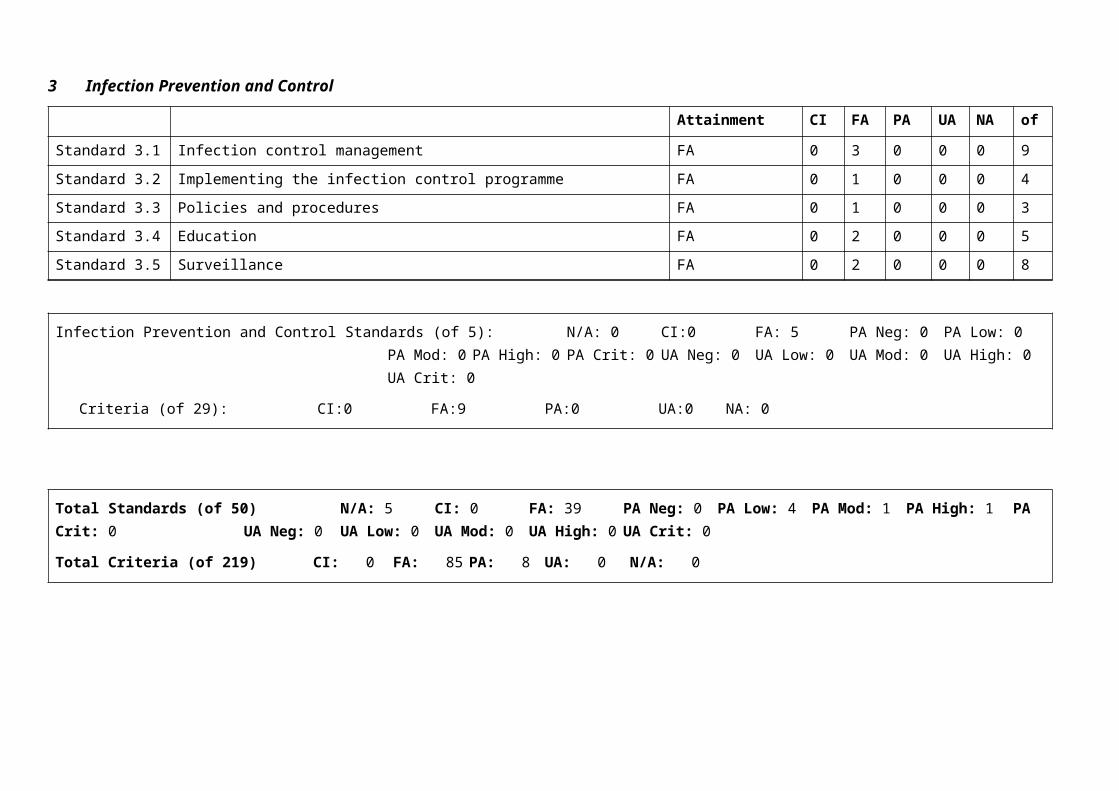
3 Infection Prevention and Control
Attainment CI FA PA UA NA of
Standard 3.1 Infection control management FA 0 3 0 0 0 9
Standard 3.2 Implementing the infection control programme FA 0 1 0 0 0 4
Standard 3.3 Policies and procedures FA 0 1 0 0 0 3
Standard 3.4 Education FA 0 2 0 0 0 5
Standard 3.5 Surveillance FA 0 2 0 0 0 8
Infection Prevention and Control Standards (of 5): N/A: 0 CI:0 FA: 5 PA Neg: 0 PA Low: 0 PA Mod: 0 PA High: 0PA Crit: 0 UA Neg: 0 UA Low: 0 UA Mod: 0 UA High: 0 UA Crit: 0
Criteria (of 29): CI:0 FA:9 PA:0 UA:0 NA: 0
Total Standards (of 50) N/A: 5 CI: 0 FA: 39 PA Neg: 0 PA Low: 4 PA Mod: 1 PA High: 1 PA Crit: 0 UA Neg: 0 UA Low: 0 UA Mod: 0 UA High: 0 UA Crit: 0
Total Criteria (of 219) CI: 0 FA: 85 PA: 8 UA: 0 N/A: 0
Corrective Action Requests (CAR) Report
Provider Name: Oceania Care Company LtdType of Audit: Certification audit
Date(s) of Audit Report: Start Date:07-Oct-13 End Date: 08-Oct-13DAA: Health Audit (NZ) LimitedLead Auditor: XXXXXXXXX
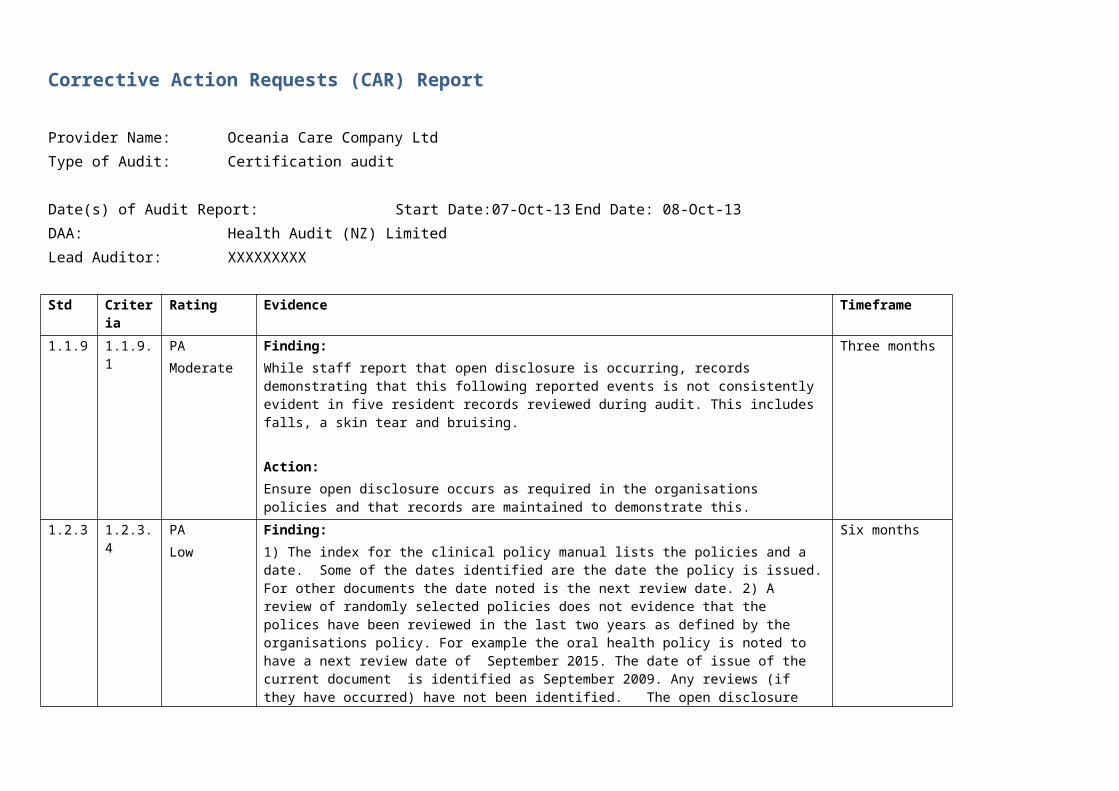
Std Criteria Rating Evidence Timeframe1.1.9 1.1.9.1 PA
ModerateFinding:While staff report that open disclosure is occurring, records demonstrating that this following reported events is not consistently evident in five resident records reviewed during audit. This includes falls, a skin tear and bruising.
Action:Ensure open disclosure occurs as required in the organisations policies and that records are maintained to demonstrate this.
Three months
1.2.3 1.2.3.4 PALow
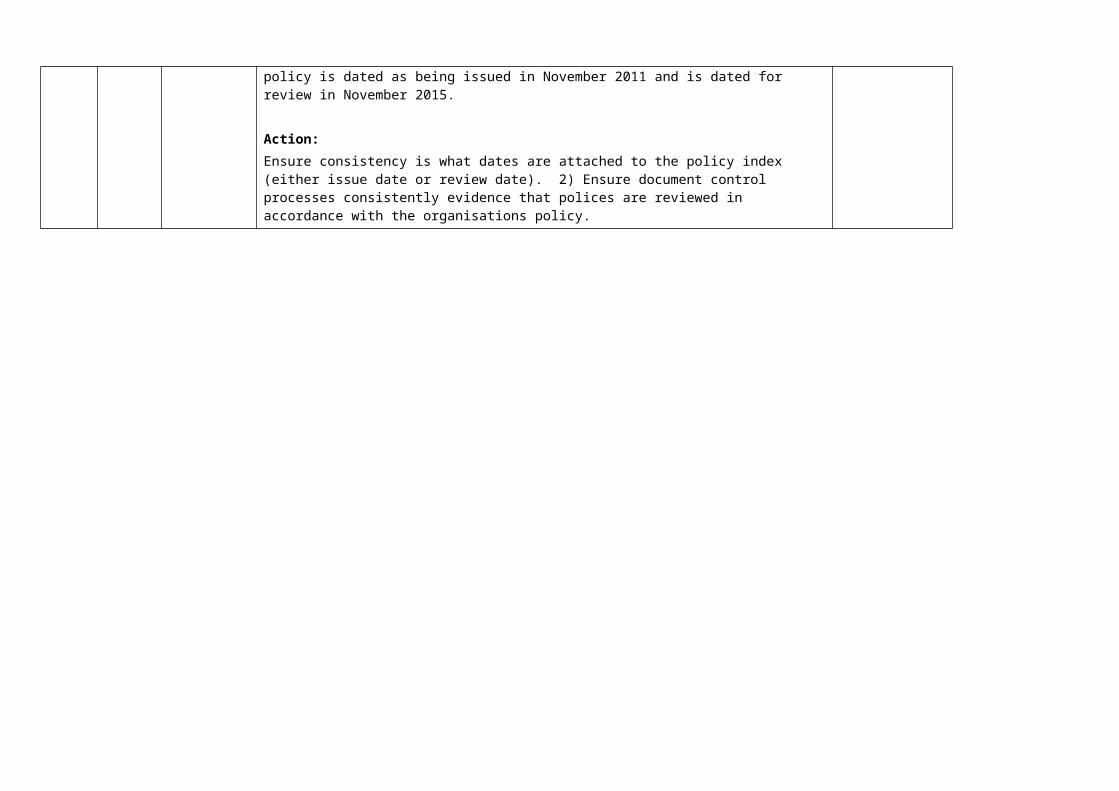
Finding:1) The index for the clinical policy manual lists the policies and a date. Some of the dates identified are the date the policy is issued. For other documents the date noted is the next review date. 2) A review of randomly selected policies does not evidence that the polices have been reviewed in the last two years as defined by the organisations policy. For example the oral health policy is noted to have a next review date of September 2015. The date of issue of the current document is identified as September 2009. Any reviews (if they have occurred) have not been identified. The open disclosure policy is dated as being issued in November 2011 and is dated for review in November 2015.
Action:Ensure consistency is what dates are attached to the policy index (either issue date or review date). 2) Ensure document control processes consistently evidence that polices are reviewed in accordance with the organisations policy.
Six months
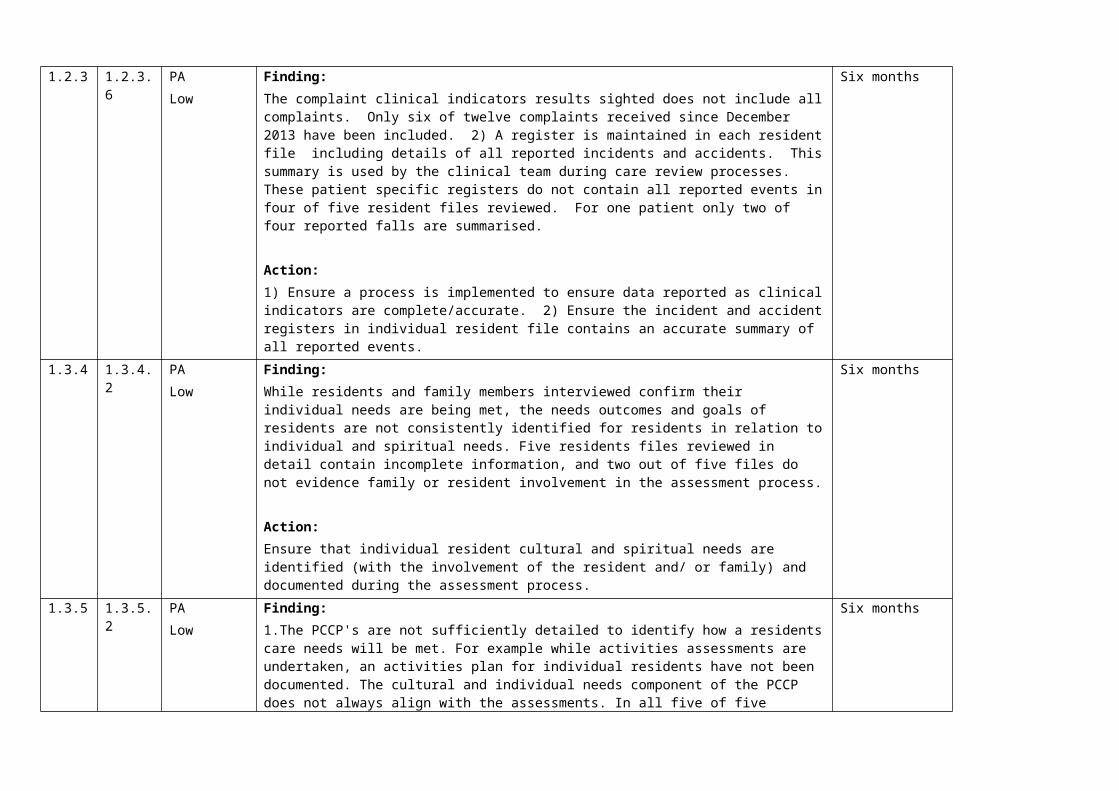
1.2.3 1.2.3.6 PALow
Finding:The complaint clinical indicators results sighted does not include all complaints. Only six of twelve complaints received since December 2013 have been included. 2) A register is maintained in each resident file including details of all reported incidents and accidents. This summary is used by the clinical team during care review processes. These patient specific registers do not contain all reported events in four of five resident files reviewed. For one patient only two of four reported falls are summarised.
Action:1) Ensure a process is implemented to ensure data reported as clinical indicators are complete/accurate. 2) Ensure the incident and accident registers in individual resident file contains an accurate summary of all reported events.
Six months
1.3.4 1.3.4.2 PALow
Finding:While residents and family members interviewed confirm their individual needs are being met, the needs outcomes and goals of residents are not consistently identified for residents in relation to individual and spiritual needs. Five residents files reviewed in detail contain incomplete information, and two out of five files do not evidence family or resident involvement in the assessment process.
Action:Ensure that individual resident cultural and spiritual needs are identified (with the involvement of the resident and/ or family) and documented during the assessment process.
Six months
1.3.5 1.3.5.2 PALow
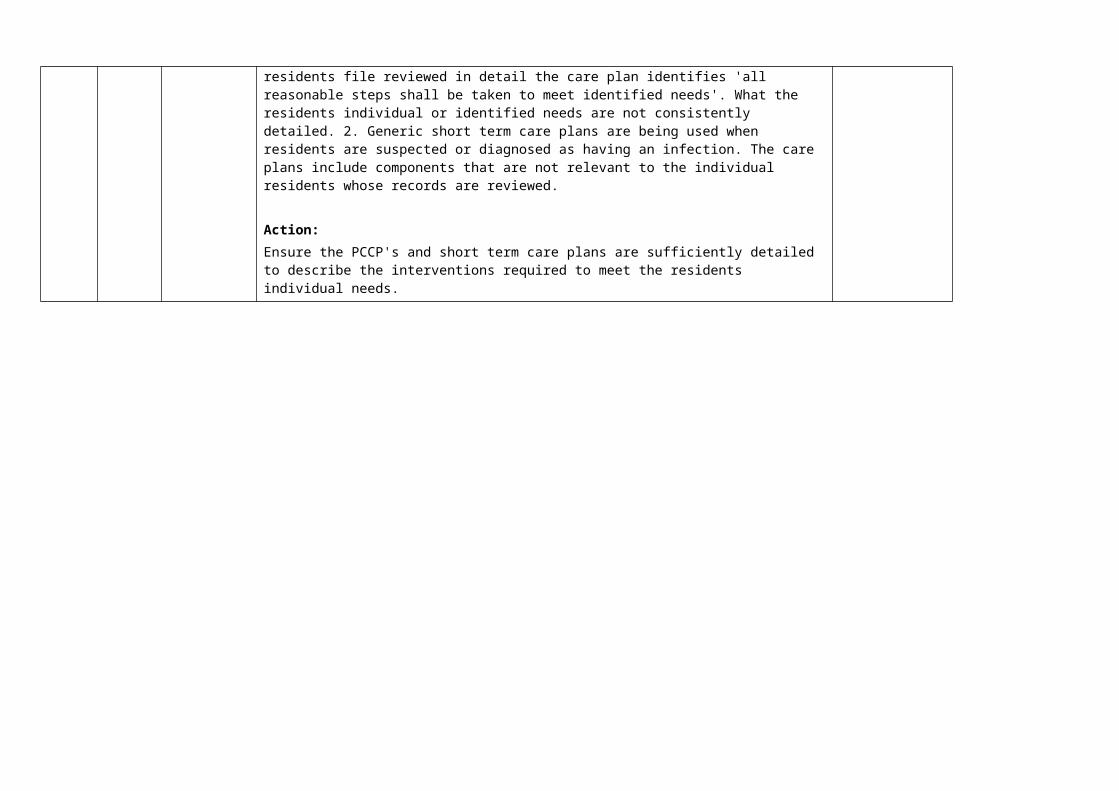
Finding:1.The PCCP's are not sufficiently detailed to identify how a residents care needs will be met. For example while activities assessments are undertaken, an activities plan for individual residents have not been documented. The cultural and individual needs component of the PCCP does not always align with the assessments. In all five of five residents file reviewed in detail the care plan identifies 'all reasonable steps shall be taken to meet identified needs'. What the residents individual or identified needs are not consistently detailed. 2. Generic short term care plans are being used when residents are suspected or diagnosed as having an infection. The care plans include components that are not relevant to the individual residents whose records are reviewed.
Action:Ensure the PCCP's and short term care plans are sufficiently detailed to describe the interventions required to meet the residents individual needs.
Six months
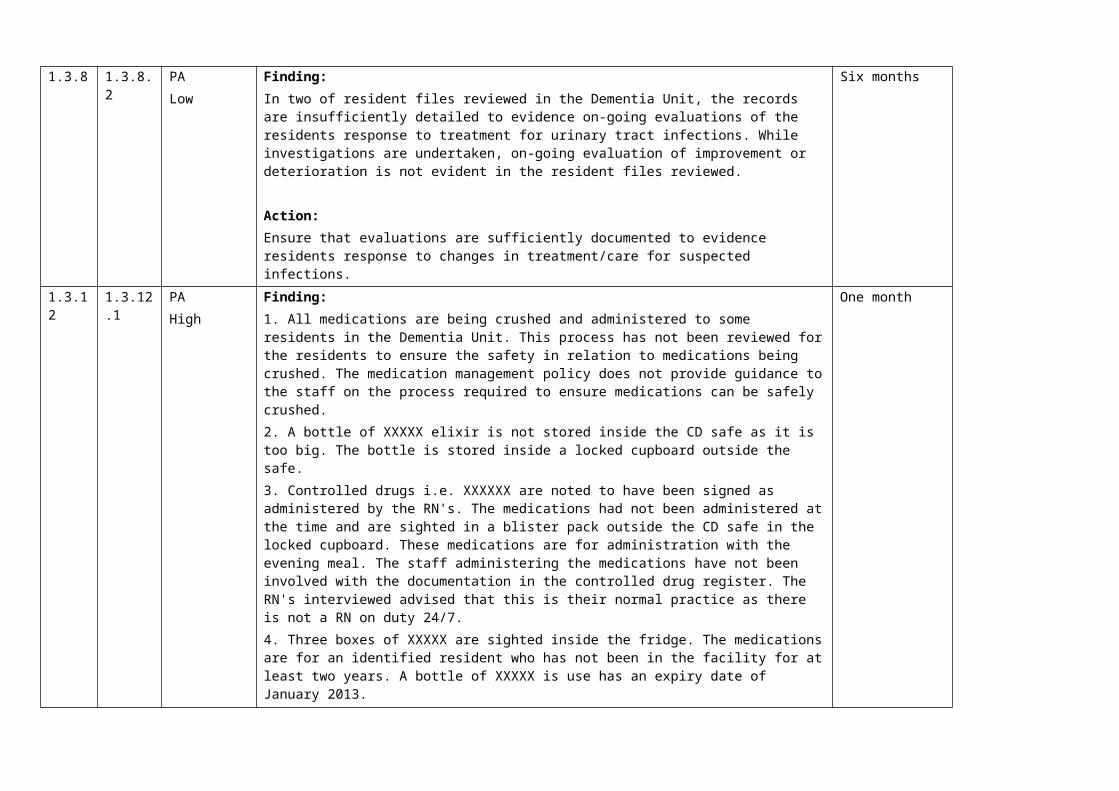
1.3.8 1.3.8.2 PALow
Finding:In two of resident files reviewed in the Dementia Unit, the records are insufficiently detailed to evidence on-going evaluations of the residents response to treatment for urinary tract infections. While investigations are undertaken, on-going evaluation of improvement or deterioration is not evident in the resident files reviewed.
Action:Ensure that evaluations are sufficiently documented to evidence residents response to changes in treatment/care for suspected infections.
Six months
1.3.12 1.3.12.1 PAHigh
Finding:1. All medications are being crushed and administered to some residents in the Dementia Unit. This process has not been reviewed for the residents to ensure the safety in relation to medications being crushed. The medication management policy does not provide guidance to the staff on the process required to ensure medications can be safely crushed.2. A bottle of XXXXX elixir is not stored inside the CD safe as it is too big. The bottle is stored inside a locked cupboard outside the safe.3. Controlled drugs i.e. XXXXXX are noted to have been signed as administered by the RN's. The medications had not been administered at the time and are sighted in a blister pack outside the CD safe in the locked cupboard. These medications are for administration with the evening meal. The staff administering the medications have not been involved with the documentation in the controlled drug register. The RN's interviewed advised that this is their normal practice as there is not a RN on duty 24/7.4. Three boxes of XXXXX are sighted inside the fridge. The medications are for an identified resident who has not been in the facility for at least two years. A bottle of XXXXX is use has an expiry date of January 2013.5. Unwanted and expired medications are being returned to the pharmacy. A register is not being maintained of what items are being returned in variance to the organisations policy.
At audit, areas for improvement are identified including administration of regular medications, administration and storage of controlled drugs as well as returning expired/unwanted medications to the pharmacy.
Action:Ensure all components of medication management practices meet professional and legislative requirements.
One month
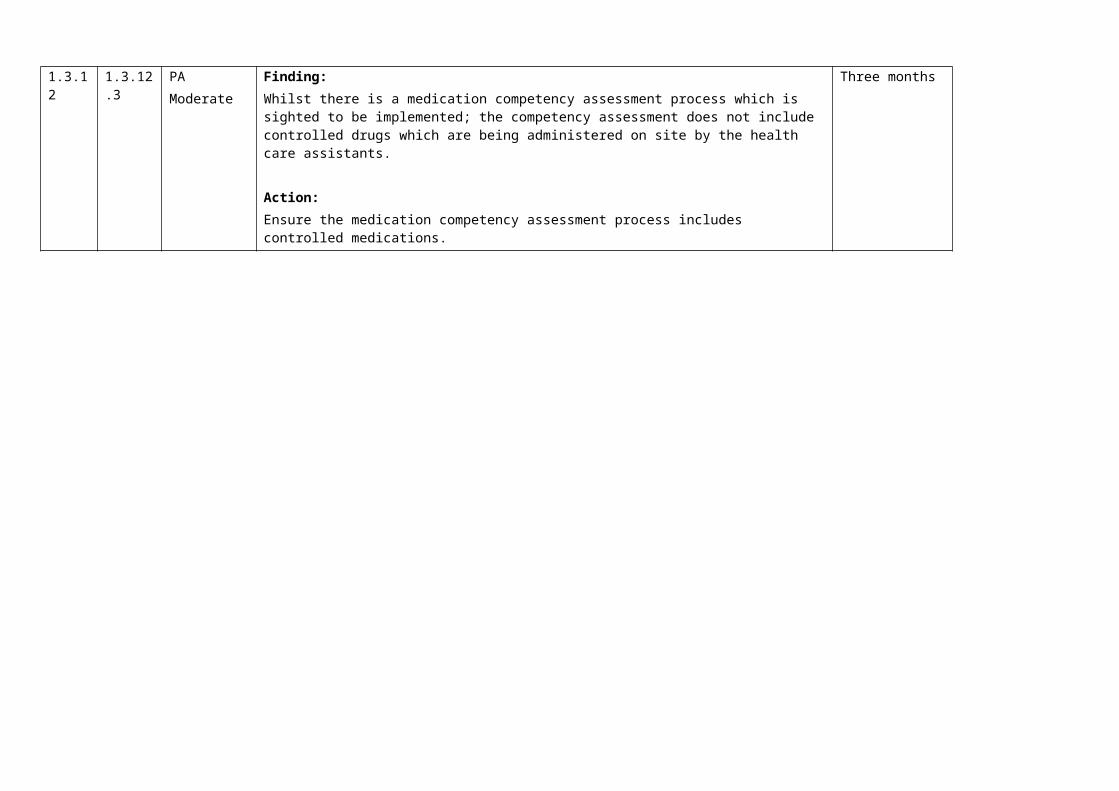
1.3.12 1.3.12.3 PAModerate
Finding:Whilst there is a medication competency assessment process which is sighted to be implemented; the competency assessment does not include controlled drugs which are being administered on site by the health care assistants.
Action:Ensure the medication competency assessment process includes controlled medications.
Three months

Continuous Improvement (CI) Report
Provider Name: Oceania Care Company LtdType of Audit: Certification audit
Date(s) of Audit Report: Start Date:07-Oct-13 End Date: 08-Oct-13DAA: Health Audit (NZ) LimitedLead Auditor: XXXXXXXXX
1. HEALTH AND DISABILITY SERVICES (CORE) STANDARDS
OUTCOME 1.1 CONSUMER RIGHTSConsumers receive safe services of an appropriate standard that comply with consumer rights legislation. Services are provided in a manner that is respectful of consumer rights, facilitates informed choice, minimises harm, and acknowledges cultural and individual values and beliefs.
STANDARD 1.1.1 Consumer Rights During Service DeliveryConsumers receive services in accordance with consumer rights legislation.
ARC D1.1c; D3.1a ARHSS D1.1c; D3.1a
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThe staff (one registered nurse (RN), the clinical leader and four healthcare assistants (HCAs) interviewed demonstrate knowledge and understanding of consumer rights, obligations and how to incorporate them as part of their everyday practice. As observed at the onsite audit staff are seen to be addressing residents with respect, knocking on doors and asking to enter rooms prior to entering, and providing the residents with choices. Education on consumer rights is last conducted in part of the two yearly in-service education programme and last conducted in on 7 August 2013 (attended by 22 staff) and records sighted.
The Aged Related Residential Care (ARRC) service agreement requirements are met.
Criterion 1.1.1.1 Service providers demonstrate knowledge and understanding of consumer rights and obligations, and incorporate them as part of their everyday practice.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.1.2 Consumer Rights During Service DeliveryConsumers are informed of their rights.
ARC D6.1; D6.2; D16.1b.iii ARHSS D6.1; D6.2; D16.1b.iii
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThe Code of Health and Disability Services Consumers' Rights (the Code) is displayed in English at the main entrance to the facility and is in both pamphlet and poster form. Those of the seven residents (seven rest home) and four family interviewed (one rest home and three in the dementia care unit) who can recollect the admission processes report they are provided with information on the Code and advocacy services on admission, the information is in the admission pack and information brochure and the admitting staff provide verbal information on the Code. The residents and family members who are unable to fully recall the admission processes advise they were provided with much information during the admission process and felt fully informed. One family member commented the code of rights is clearly displayed on entering the facility. All seven residents and four family interviewed report they are treated with respect and dignity and their privacy is maintained. The GP interviewed by the second auditor expressed no concerns regarding breaches of the residents' rights during service delivery and spoke highly of the care staff. The ARRC requirements are met.
Criterion 1.1.2.3 Opportunities are provided for explanations, discussion, and clarification about the Code with the consumer, family/whānau of choice where appropriate and/or their legal representative during contact with the service.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.1.2.4 Information about the Nationwide Health and Disability Advocacy Service is clearly displayed and easily accessible and should be brought to the attention of consumers.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.1.3 Independence, Personal Privacy, Dignity, And RespectConsumers are treated with respect and receive services in a manner that has regard for their dignity, privacy, and independence.
ARC D3.1b; D3.1d; D3.1f; D3.1i; D3.1j; D4.1a; D14.4; E4.1a ARHSS D3.1b; D3.1d; D3.1f; D3.1i; D3.1j; D4.1b; D14.4
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAAbuse and Neglect Prevention Policy and Guidelines’ (updated June 2012) sighted. The policy provides definition on types of abuse and neglect. Staff training is provided. Procedures for reporting are documented. The policy is cross referenced to the ‘Advocacy Policy’, ‘Complaints Policy’ and ‘Unwanted Events Policy’. ‘Sexuality and Intimacy Policy’ (updated June 2012) sighted. The policy includes acknowledging sexuality and responding appropriately to sexual behaviour. The 'Spirituality and Counselling Policy’ (updated June 2012) is also sighted. Residents spiritual beliefs and preferences are identified. Church services are provided. The Oceania Philosophy of Care is also sighted.
‘Gifts Policy’ is sighted (updated December 2011) details what is and what is not acceptable to accept as a gift or token of appreciation from a resident or family member
While cultural assessments are occurring (and sighted in the five resident files where this was reviewed in detail), two of the five resident assessments do not detail that the resident or family contributed to the assessment. The staff member conducting the assessments advises residents and families are involved however this was inadvertently not noted on the assessment form. Some generic phrases are also being used. This is raised as an area for improvement in 1.3.4.2. While all staff interviewed are aware of the residents individual needs and can articulate these, they are not always sufficiently detailed in the person centred care plan (PCCP) sighted during audit. This is raised as an area requiring improvement in 1.3.5.2. There is currently one resident who does not communicate in English. The staff caring for this resident are able to identify key words used to communicate with the resident and also use body language/sign language.
All seven residents and four family/whānau interviewed express high levels of satisfaction with the way they are treated by all staff and report that the residents' dignity, privacy and independence is always respected. The RN, clinical leader, cleaner, laundry employee and four HCAs interviewed demonstrate knowledge of providing services in a manner that respects the residents' dignity, privacy and dignity.
All residents have single rooms which affords privacy. During interview with seven of seven rest home residents and four of four family/whanau members (three family members of residents in the dementia unit and one resident in the rest home) they confirm that all their rights are respected by staff and that the service is responsive to their identified needs, culture values and beliefs. The four family members advise they visit often and have never had any concerns with how their family member or other residents are spoken with and/or treated by staff.
Information on the Nationwide Health and Disability Advocacy Services is provided in the admission information, with brochures displayed and available at the entrance to the facility.
Education on advocacy is last conducted on 7 August 2013 (attended by 22 staff) and abuse and neglect on 10 June 2013 ( attended by 21 staff) as part of the in-service programme.
The ARRC requirements are met.
Criterion 1.1.3.1 The service respects the physical, visual, auditory, and personal privacy of the consumer and their belongings at all times.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.1.3.2 Consumers receive services that are responsive to the needs, values, and beliefs of the cultural, religious, social, and/or ethnic group with which each consumer identifies.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.1.3.6 Services are provided in a manner that maximises each consumer's independence and reflects the wishes of the consumer.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.1.3.7 Consumers are kept safe and are not subjected to, or at risk of, abuse and/or neglect.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.1.4 Recognition Of Māori Values And BeliefsConsumers who identify as Māori have their health and disability needs met in a manner that respects and acknowledges their individual and cultural, values and beliefs.
ARC A3.1; A3.2; D20.1i ARHSS A3.1; A3.2; D20.1i
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThe ‘Maori Health Plan’ (updated January 2012) sighted. The policy identifies the Oceania commitment to the principles of the Treaty of Waitangi and is cross referenced to TIKANGA Recommended Best Practice Policy - Auckland District Health Board. The policy is sighted at audit. The facility manager advises there are currently no residents who have identified their ethnicity as Maori and there are no barriers for Maori residents accessing services as long as the prospective resident has a current needs assessment and beds are available. The facility manager advises Maori residents have been receiving care until recently but required transfer to another facility when the resident required hospital level care. Staff are provided with training on the Treaty of Waitangi and providing culturally appropriate care. This training last occurred on 3 April 2013 (10 staff attended) and 21 August 2013 (17 staff attended) and records sighted. The four HCAs interviewed and the RN verify that whanau involvement is encouraged (with the residents agreement).
The ARRC requirements are met.
Criterion 1.1.4.2 Māori consumers have access to appropriate services, and barriers to access within the control of the organisation are identified and eliminated.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.1.4.3 The organisation plans to ensure Māori receive services commensurate with their needs.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.1.4.5 The importance of whānau and their involvement with Māori consumers is recognised and supported by service providers.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.1.6 Recognition And Respect Of The Individual's Culture, Values, And BeliefsConsumers receive culturally safe services which recognise and respect their ethnic, cultural, spiritual values, and beliefs.
ARC D3.1g; D4.1c ARHSS D3.1g; D4.1d
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FA‘Culturally Competent Services Policy’ is sighted (updated June 2012). The policy makes reference to the work of Mason Durie and the four cornerstones of health. The person centred planning process incorporates Te Whare Tapa Wha. Working relationships are developed and maintained with local Iwi. The policy states that Maori residents have equal access to services. The policy provides guidelines for working with all cultures and is cross referenced to the Interpreter Policy, the ‘New Zealand Guide to Ethnic Groups’ and the Maori Health Plan. An introduction to the ‘Cultural Appropriate Services Policy’ is included in orientation.
‘Interpreter Policy’ (updated November 2012) is sighted. The policy ensures timely and appropriate access to interpretation services where English is not used for day to day communication by residents of families. The facility manager and the clinical leader are able to identify the process for accessing interpreters (where these are required) via the DHB.

There is currently one resident who is not communicating in English (although is reported to have been able to do so in the past). Staff caring for the resident are able to identify how communicate with this resident and the processes observed during audit.
While cultural assessments are occurring including identification of any spiritual needs the resident may have and these assessments are sighted in the thirteen resident files reviewed during audit. A detailed review of five resident assessments do not evidence that the resident or family contributed to the assessment for two residents. The staff member conducting the assessments advises residents and families are involved however this was inadvertently not noted on the assessment form. Some generic phrases are also being used. This is raised as an area for improvement in 1.3.4.2. While all staff interviewed are aware of the residents individual cultural and spiritual needs and can articulate these, they are not always sufficiently detailed in the person centred care plan (PCCP) sighted during audit. As an example one residents assessment notes the resident has a Church of England faith but is not currently practising. The PCCP notes the resident needs to be reminded of when the Church services are on as attending is important to the resident. Another resident assessment notes the resident is of an identified faith and is practicing. The PCCP does not include this information. Another resident has moved to Maureen Plowman Home to be near a spouse who is in the dementia unit. This is not included in the rest home residents PCCP when reviewed during audit. This is raised as an area requiring improvement in 1.3.5.2. Despite this all seven rest home residents interviewed and all four family members (three family of residents in the dementia unit and one in the rest home) verify staff provide care that meets their individual spiritual and cultural needs. The four HCAs interviewed and the activities coordinator is able to identify the individual needs of residents and this aligns with the information provided by the residents and family members during interview.
The ARRC requirements are met.
Criterion 1.1.6.2 The consumer and when appropriate and requested by the consumer the family/whānau of choice or other representatives, are consulted on their individual values and beliefs.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.1.7 Discrimination
Consumers are free from any discrimination, coercion, harassment, sexual, financial, or other exploitation.
ARHSS D16.5e
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThe facility manager reports that harassment or neglect of any nature towards residents will not be tolerated. Staff are advised during the orientation programme of the conduct and behaviour that is expected from them and any variances will be investigated and followed up promptly.In-service education on elder abuse and neglect is last conducted in June 2013 which is attended by 21 staff. The four of four HCAs interviewed demonstrate knowledge on the signs of abuse, neglect and discrimination. The seven staff records reviewed have position descriptions, confidentiality agreements and a code of conduct which details the expectations of the organisations. The RN interviewed is aware of her responsibilities and professional boundaries as identified by the New Zealand Nursing Council. The facility manager advises there have been are no instances of abuse or neglect reported since her employment (16 months prior to audit).
As observed on the day of audit professional boundaries are maintained for the well-being of the residents that still encourages a friendly and home like environment. All seven residents and all four family/whānau have no concerns with discrimination/abuse or neglect and speak highly of how they are treated by all staff.
The ARRC requirements are met.
Criterion 1.1.7.3 Service providers maintain professional boundaries and refrain from acts or behaviours which could benefit the provider at the expense or well-being of the consumer.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.1.8 Good Practice
Consumers receive services of an appropriate standard.
ARC A1.7b; A2.2; D1.3; D17.2; D17.7c ARHSS A2.2; D1.3; D17.2; D17.10c
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAEvidence-based practice is observed, promoting and encouraging good practice (evidenced in interviews with the RN, clinical manager, facility manager and four HCAs). Examples include updating policies and procedures and this process is facilitated and overseen by Oceania nationally.
The service has regular visits by the GP (weekly), links with the local mental health services, and the DHB specialist nurses. One resident with challenging behaviours is being seen regularly by gerontology mental health services who are actively involved with developing and updating the residents plan of care.There is regular in-service education and staff access external education that is focused on aged care and best practice. All seven residents and three family/whānau interviewed satisfaction with the care delivered with the exception one resident does not like some of the meal choices. Three of the residents advised the facility manager and clinical leader are available at any time to meet with them and will help the communicate their needs/requests to the GP if necessary.Quality improvement projects are being undertaken. Currently a falls prevention project is occurring and calendar in the staff tea room identify any time a resident has a fall, the time of day and whether an injury occurred or not. Staff are encouraged to ensure residents are wearing appropriate footwear, clutter is removed and the environment made safe. The number of days being falls is being calculated and falls safety promoted.
ARRC requirements are met.
Criterion 1.1.8.1 The service provides an environment that encourages good practice, which should include evidence-based practice.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.1.9 Communication
Service providers communicate effectively with consumers and provide an environment conducive to effective communication.
ARC A13.1; A13.2; A14.1; D11.3; D12.1; D12.3a; D12.4; D12.5; D16.1b.ii; D16.4b; D16.5e.iii; D20.3 ARHSS A13.1; A13.2; A14.1; D11.3; D12.1; D12.3a; D12.4; D12.5; D16.1bii; D16.4b; D16.53i.i.3.iii; D20.3
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: PA ModerateThe 'Open Disclosure Policy’ sighted (updated November 2011). The policy provides a definition of open disclosure and key principles. While staff report that open disclosure is occurring, records demonstrating this following reported events is not consistently evident in five resident records reviewed during audit. Open disclosure is not documented as occurring for six of seven resident falls, a resident with a skin tear and bruising. This is identified as an area requiring improvement. Open disclosure is occurring with family on other components of care.
The clinical leader and facility manager advise interpreters are obtained from the DHB if required to ensure effective communication with residents. Currently there is one resident who is no longer communicating in English. The resident’s family members assist staff with communication as and when required.
Criterion 1.1.9.1 Consumers have a right to full and frank information and open disclosure from service providers.
Audit Evidence Attainment: PA Risk level for PA/UA: ModerateThe 'Open Disclosure Policy’ sighted (updated November 2011). The policy provides a definition of open disclosure and key principles. While staff report that open disclosure is occurring, records demonstrating that this following reported events is not consistently evident in five resident records reviewed during audit. This includes disclosure related to six out of seven resident falls, a skin tear and bruising. This is identified as an area requiring improvement. The family communication records sighted in the resident files reviewed during audit verify that family members are informed of changes in the residents health status, recommendations from the GP and changes in medication. The seven rest home residents interviewed verify they are advised of proposed changes in medication and are active participants in decision making about their health and wellbeing.
Finding StatementWhile staff report that open disclosure is occurring, records demonstrating that this following reported events is not consistently evident in five resident records reviewed during audit. This includes falls, a skin tear and bruising.
Corrective Action Required:Ensure open disclosure occurs as required in the organisations policies and that records are maintained to demonstrate this.
Timeframe:Three months
Criterion 1.1.9.4 Wherever necessary and reasonably practicable, interpreter services are provided.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.1.10 Informed ConsentConsumers and where appropriate their family/whānau of choice are provided with the information they need to make informed choices and give informed consent.
ARC D3.1d; D11.3; D12.2; D13.1 ARHSS D3.1d; D11.3; D12.2; D13.1
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThe “Informed Consent Policy” (updated November 2011) is sighted. The policy includes definitions. All residents sign an ‘Informed Consent form’. This includes consent to medical treatment, permission to photograph and the collection and storage of information. Completed consent forms are sighted in all 13 resident files reviewed by the two auditors during audit. A second consent form for 'transportation' is also present in the resident files.‘End of Life Decisions Policy’ (updated February 2013) is sighted. Discussions are commenced on entry to Maureen Plowman as to the residents requests related to resuscitation/advanced directives and general care/treatment. The involvement of family is encouraged. Advanced directives are defined. Where an advanced directives has been made, these are required to be reviewed every six months. Where a resident has an advanced directive and is for resuscitation this is clearly noted with a heart symbol on the spine of the residents file.Thirteen resident files reviewed during audit demonstrate that advanced directive are discussed with competent residents at admission and subsequently six monthly. Where the resident has made an advanced directive the GP has verified the residents competency. The remaining residents have an 'end of life' document present which obtains the next of kin feedback on what they understand to be the resident wishes for end of life care. The GP also verifies the resident is not competent in decision making. The facility manager identify this document is considered by the GP when making end of life treatment decisions. One resident is sighted to have an advanced directive and an 'end of life' information document present in the residents file. The clinical leader advises only one document should be present. The resident is not competent in decision making as verified by the GP in the consultation the week prior to audit. The current document is retained in the residents file and the other document removed for archiving during audit.Where a resident has an enduring power of attorney or welfare guardian appointed, a copy of documents verifying this is present in all but one applicable file sampled. The RN interviewed is able to demonstrate that she has been communicating regularly with this resident’s family (the resident is receiving dementia level care), seeking a copy of the legal documents. If these documents are not forthcoming will escalate this to the facility manager for follow-up.
The seven rest home level residents interviewed and the four family members interviewed verify they were provided with full information prior to completing the written consent processes. One of one rest home resident interviewed confirms making an advanced directive for active treatment and resuscitation which was agreed with the GP. The family member interviewed confirms the resident has made this decision autonomously and family are aware of the residents requests.
Criterion 1.1.10.2 Service providers demonstrate their ability to provide the information that consumers need to have, to be actively involved in their recovery, care, treatment, and support as well as for decision-making.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.1.10.4 The service is able to demonstrate that written consent is obtained where required.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.1.10.7 Advance directives that are made available to service providers are acted on where valid.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.1.11 Advocacy And SupportService providers recognise and facilitate the right of consumers to advocacy/support persons of their choice.
ARC D4.1d; D4.1e ARHSS D4.1e; D4.1f
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FA ‘Advocacy Policy and Procedure’ (update June 2012) is sighted. The policy provides definitions of advocacy and states that information on advocacy is made available. A procedure for accessing independent advocacy services is provided. The policy is cross referenced to the ‘Complaints Policy’, ‘Resident Rights Policy’ and the ‘Code of Resident Rights and Responsibilities Policy’. Information on independency advocacy services is included in the information provided to new residents and family in the entry to service process. There are also pamphlets present in the main reception area. The facility manager, four of four HCAs and the RN are all aware of the residents right to independent advocacy and confirm this will be facilitated where requested/required.Those of the seven residents (seven rest home) and four family/whanau interviewed (one rest home and three in the dementia care unit) who can recollect the admission processes with clarity report they are provided with information on advocacy services at admission. The residents and family/whanau members who are unable to fully recall the admission processes cannot recall if they were provided with this information during the admission process 'as a lot of information was given', however they are unconcerned and feel fully informed. The service actively encourages residents to participate fully in determining how their health and welfare is managed, as confirmed at interview with the RN and clinical leader. Family/whānau are encouraged to involve themselves as advocates (evidenced in interviews with four family/whānau). The ARRC contract requirements are met.
Criterion 1.1.11.1 Consumers are informed of their rights to an independent advocate, how to access them, and their right to have a support person/s of their choice present.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.1.12 Links With Family/Whānau And Other Community ResourcesConsumers are able to maintain links with their family/whānau and their community.
ARC D3.1h; D3.1e ARHSS D3.1h; D3.1e; D16.5f
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FA A number of residents are observed independently and/or being accompanied by visitors going out into the community. Family/whānau are encouraged to visit. All seven residents and four family/whānau interviewed confirm they can have visitors of their choice and visiting hours are flexible to meet individual resident and family/whanau needs. Residents are supported and encouraged to access community services independently, with visitors or as part of the planned activities programme (refer to 1.3.7).
The ARRC requirements are met.
Criterion 1.1.12.1 Consumers have access to visitors of their choice.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.1.12.2 Consumers are supported to access services within the community when appropriate.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.1.13 Complaints ManagementThe right of the consumer to make a complaint is understood, respected, and upheld.
ARC D6.2; D13.3h; E4.1biii.3 ARHSS D6.2; D13.3g
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FA‘Complaints Policy’ (updated July 2012) is sighted. The policy states it complies with the Code of Health and Disability Consumers’ Rights Act 1996.The policy includes the management of both verbal and written complaints. All complaints are required to be documented and maintained in a complaints register. Time frames are identified as is the right to receive independent advocacy services. A complaints flow chart is documented. It is noted that the complaints policy does not directly include actions to be taken in the event the complainant is not satisfied with the result of the investigation, however the right to seek independent advocacy services is clearly documented on all complaint information given to residents.A complaints register is being maintained and includes details of twelve complaints received between December 2012 and the date of audit. A review of four complaints selected at random in relation to missing dentures, episodes of challenging behaviours, phone calls and a staff member demonstrates the complaints are acknowledged, investigated and responded to within the time frames required to meet the Code. The RN, clinical leader, facility manager, cleaner and laundry employee are aware of their responsibilities in relation to the reporting and management of complaints and can articulate the organisations policy and processes. All seven rest home residents advise they have no complaints. Two resident advise concerns raised with management in the past were quickly addressed by staff and management. The facility manager advises there have been no complaints to the H&DC, Ministry of Health, and District Health Board since the last audit.The number of complaints is included in the organisations 'quality indicator' data which is reported monthly as a component of the quality monitoring processes. It is observed at audit that the quality indicator data identifies there have been six complaints in the above period (rather than the 12 as noted in the complaints register). Ensuring all complaints are included in the indicator data/quality monitoring processes is an area requiring improvement and is raised in 1.2.3.6.
Criterion 1.1.13.1 The service has an easily accessed, responsive, and fair complaints process, which is documented and complies with Right 10 of the Code.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.1.13.3 An up-to-date complaints register is maintained that includes all complaints, dates, and actions taken.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
OUTCOME 1.2 ORGANISATIONAL MANAGEMENTConsumers receive services that comply with legislation and are managed in a safe, efficient, and effective manner.
STANDARD 1.2.1 GovernanceThe governing body of the organisation ensures services are planned, coordinated, and appropriate to the needs of consumers.
ARC A2.1; A18.1; A27.1; A30.1; D5.1; D5.2; D5.3; D17.3d; D17.4b; D17.5; E1.1; E2.1 ARHSS A2.1; A18.1; A27.1; A30.1; D5.1; D5.2; D5.3; D17.5
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThe Oceania Group develops a template for business planning. The facility manager (FM) at Maureen Plowman Home (MPH) has utilised the template to developed a facility specific business plan. This includes information on bed numbers and occupancy, identified key performance indicators and keys for success. The plan notes the provision of rest home and dementia level care. The business plan includes a maintenance plan and action plans for patient/resident care needs, increased service delivery, human resource issues, quality and risk activities, infection prevention and control as well as other components. There is a strengths, weakness, opportunities and threat (SWOT) analysis for MPH with reference to competitors in the marketplace.The purpose, values and mission statement is developed centrally within input from the facility manager. This is via 'cluster meetings and conferences'. The values are 'deliver, excellence, passion and respect'. Monitoring of how the service meets these values is a component of staff performance appraisals and connect values awards. All 55 Oceania sites participate in acknowledging staff who demonstrate meeting the organisations values. Residents, family and staff can make nominations. MPH have won the overarching northern area (ten sites) award the last four times in (six weekly award periods). A number of staff have also won individual awards. The values vision statement and mission statement is displayed in the main corridor entrance area of the facility.The facility manager has worked at MPH for 18 months. Prior to this worked for Oceania Group as a clinical leader for three and a half years. The FM job description is dated June 2012 and details key accountabilities, key responsibilities, competencies and key performance indicators. The FM is a RN with a current APC (sighted). The FM curriculum vitae (CV) identifies the FM has a diploma in business studies and will graduate imminently. The FM has a post graduate certificate in long term chronic condition management (completed in 2010 via University of Auckland). The FMs CV demonstrates the FM has working in a variety of settings including cardiothoracic ICU, medical services, family and community health and aged care. The FM has attended more than eight hours of education related to the management of a residential care facility as required to meet the ARRC contract in the last year. Topics include health and safety, quality and risk, health and safety, restraint minimisation, the Oceania Management annual conference (last held 19 June 2013) and Oceania Group cluster meetings at least four time per annum.
ARRC contract requirements are met.
Criterion 1.2.1.1 The purpose, values, scope, direction, and goals of the organisation are clearly identified and regularly reviewed.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.2.1.3 The organisation is managed by a suitably qualified and/or experienced person with authority, accountability, and responsibility for the provision of services.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.2.2 Service ManagementThe organisation ensures the day-to-day operation of the service is managed in an efficient and effective manner which ensures the provision of timely, appropriate, and safe services to consumers.
ARC D3.1; D19.1a; E3.3a ARHSS D3.1; D4.1a; D19.1a
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThe clinical leader (CL) is in charge when the FM is on leave or away. The CL has worked at Oceania MPH since August 2011. The CL is the restraint coordinator and the infection prevention and control nurse. The CL has a documented position description which details her roles, responsibilities, competencies and key performance indicators. The position description details the CL undertakes delegated responsibilities as directed by the FM. The CLs CV details she has worked in aged care facilities in New Zealand and overseas as a senior registered nurse. This is her first appointment in a clinical leader role. The CL maintains a current APC which is sighted.
The CL is participating in relevant ongoing education including (but not limited to) chemical handling, dementia care, diabetes, infection prevention and control, grief and loss, respect privacy and dignity. The CL performance appraisal was last undertaken in November 2012.
The ARRC requirements are met.
Criterion 1.2.2.1 During a temporary absence a suitably qualified and/or experienced person performs the manager's role.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.2.3 Quality And Risk Management SystemsThe organisation has an established, documented, and maintained quality and risk management system that reflects continuous quality improvement principles.
ARC A4.1; D1.1; D1.2; D5.4; D10.1; D17.7a; D17.7b; D17.7e; D19.1b; D19.2; D19.3a.i-v; D19.4; D19.5 ARHSS A4.1; D1.1; D1.2; D5.4; D10.1; D16.6; D17.10a; D17.10b; D17.10e; D19.1b; D19.2; D19.3a-iv; D19.4; D19.5
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: PA Low‘Quality Improvement Policy’ (updated June 2012) is sighted. The policy makes reference to ISO 8402-1986 and sates continuous improvement is maintained.The quality and risk programme includes:-business planning process (refer to 1.2.1)- policy procedure development/review- compliments and complaints- quality improvement projects- incident/accident reporting- internal audits- monitoring indicators - monitoring the use of restraint and enablers- surveillance for residents who develop infections- staff training/education- resident and family/whanau feedback and resident meetings
- resident satisfaction surveys - hazard identification and management- risk review and management. Quality and risk information is discussed at a variety of forums including the quality improvement staff meetings and health and safety meetings and verified in minutes of these meetings as sighted. The minutes of the last three meetings sighted reflect discussions on supplier performance, staff education, resident care, resident satisfaction, incidents/accidents, compliments, complaints, residents with infections, results of internal audits and quality improvement projects.
Nine staff interviewed (four HCAs, one cleaner, one laundry employee, one activities staff , one RN and the clinical leader), are able to detail their responsibilities in relation to the reporting of complaints and incidents /accidents. The clinical staff are able to identify their responsibilities for reporting of residents who are suspected of having an infection. The staff confirm being provided with appropriate feedback on incidents/accidents, complaints/compliments, and infection rates including via the monthly staff meeting. Staff when asked identified a number of quality improvement activities have occurred since the last audit. This include: implementing a falls prevention programme, the RNs having 'pink pages' to document in the progress notes and improving oral hygiene cares for residents in the dementia unit.
The policies and procedures provide the framework for the review and document control processes for policies and procedures. All companywide clinical documents are to be reviewed by Oceania Group on a two yearly basis and the final version is accessible in a PDF file via the intranet and in two hardcopy manuals on site. The FM is responsible for ensuring the paper based versions are current. Staff are required to review and sign they have reviewed new documents. The clinical manual index on the intranet contains the document name and dates. Some of the dates noted are the issue date and others are the review date. Not all policies identify when reviews have occurred. These are areas requiring improvement.
Internal audits are occurring and the frequency is noted in an internal audit schedule. A review of five audits selected at random from the calendar which included laundry service, cleaning services, skin and pressure area risk assessment, current annual practising certificates (APC), drivers licence and first aid certificates and incident and accident reporting demonstrates a high level of compliance with the organisations policies. Where areas for improvement are identified a corrective action plan is documented and implemented. Corrective action plans are also sighted to be developed in response to incidents/ accidents and complaints.
Quality improvement projects are being undertaken. The desired outcome and steps to achieve this are documented and displayed for staff on the wall in the staff room. Current quality improvement projects are occurring in relation to documentation in resident files, improving residents oral health and establishing a dementia support group for the family of residents with dementia.
Oceania Group have a number of indicators which are reported on each month and graphed. The data enables individual Oceania facilities to benchmark results with other Oceania facilities. It is observed at audit that data submitted in relation to complaints is not complete with only six of twelve reported complaints being included. This is an area requiring improvement.
Incidents/ accidents are being reported (refer to 1.3.4). A register is present in resident files for the recording of all reported events that involve individual residents. These records are reviewed by the clinical team during care reviews. These registers are not being consistently updated and not all reported events are included. This is also an area requiring improvement.
‘Clinical Risk Management Policy’ (updated June 2012) sighted. The policy states that systems to identify and manage clinical risk are in place. A ‘Clinical Risk Management Plan’ is documented which includes identified organisation risks including clinical, environmental, health and safety equipment, security, staffing, staff training, communication and emergency events. The risk register is reviewed by the clinical quality team (comprises the general manager clinical quality and six clinical quality managers). The risk register is dated as being last reviewed in August 2012 by the Oceania group manager clinical and quality. The FM advises risk is reviewed from a facility level monthly and components related to financial risk, occupancy, staff turnover, operational issues is monitored as a component of the FM monthly report. The last three month FM reports sighted. The complaints process and indicators are also reported to be used to monitor clinical risk.
There are hazard registers. These are reviewed and updated each month as a component of the health and safety meeting. The H&S committee comprises the FM, a RN and at least four other staff. This committee reviews all staff incident and accidents, health and safety indicators, new processes and equipment, staff training, and policy and procedure which have been reviewed. Minutes of the health and safety meetings dated 2 October 2013, 4 September 2013 and 1 August 2013 sighted.
There are resident meetings. These occur three monthly. Minutes of the last two meetings dated 26 July 2013 (21 residents attended) and 15 April 2013 (25 residents attended) includes discussions on changes in staffing, food and beverages, use of hand gel/hand hygiene, doctors’ visits, ensuring adequate hydration, weekend activities and that a new facility vehicle/van has been purchased.
‘Satisfaction Survey Policy’ is sighted (updated July 2012). A patient satisfaction survey is last undertaken in February and July 2013. Surveys are given to residents by the activities coordinator. Six resident responses selected at random demonstrate an individual correction action plan is documented where the resident expressed any concerns or made a request. The resident satisfaction survey included seeking feedback on food, laundry services, care planning, cultural needs, patient’s awareness of incident and accident and complaints reporting processes, care and environmental cleanliness.
The ARRC requirements are met.
Criterion 1.2.3.1 The organisation has a quality and risk management system which is understood and implemented by service providers.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.2.3.3 The service develops and implements policies and procedures that are aligned with current good practice and service delivery, meet the requirements of legislation, and are reviewed at regular intervals as defined by policy.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.2.3.4 There is a document control system to manage the policies and procedures. This system shall ensure documents are approved, up to date, available to service providers and managed to preclude the use of obsolete documents.
Audit Evidence Attainment: PA Risk level for PA/UA: LowThe 'document control procedure for new or reviewed documents’ (issued July 2012) is sighted. The ‘Document Control Policy’ (updated July 2012) is also sighted. The policy includes approval, distribution, format, change control, amendments, maintenance and storage, withdrawal of documents. All companywide clinical documents are reviewed on a two yearly basis and the final version is accessible in a PDF file via the intranet. Policies are reviewed in a scheduled basis by the clinical quality team (group manager and six regional clinical quality managers. The CGM have all been FM so are aware of the policy requirements ''bigger picture'. The final versions are advised to the facility managers via email. Specific policies may be distributes to managers. There may be a link to the intranet or the policy may be attached. Staff training is required when new documents are developed. Obsolete copies are removed by the FM (but stored electronically), an amendment log is maintained and sighted. Staff are required to review and sign they have reviewed the new policy. Examples of the signing sheets sighted in three policy folders selected at random (health and safety, emergency procedures and infection prevention and control) reviewed during audit. The FM advises there are no site specific policies at MPH. There is a hardcopy folder containing policies and procedures in the staff tea room and one in the nurses’ station.It is observed at audit that the electronic index for the clinical policy manual on the Oceania intranet lists the clinical policies and a date. Some of the dates identified are the date the policy is issued. For other documents the date noted is the next review date. A review of randomly selected policies does not evidence that the polices have been reviewed in the last two years as defined by the organisations policy. For example the oral health policy is noted to have a next review date of September 2015. The date of
issue of the current document is identified as September 2009. Any reviews (if they have occurred) have not been identified in variance to document control processes evident on other randomly reviewed policies. The open disclosure policy is dated as being issued in November 2011 and is dated for review in November 2015.
Finding Statement1) The index for the clinical policy manual lists the policies and a date. Some of the dates identified are the date the policy is issued. For other documents the date noted is the next review date. 2) A review of randomly selected policies does not evidence that the polices have been reviewed in the last two years as defined by the organisations policy. For example the oral health policy is noted to have a next review date of September 2015. The date of issue of the current document is identified as September 2009. Any reviews (if they have occurred) have not been identified. The open disclosure policy is dated as being issued in November 2011 and is dated for review in November 2015.
Corrective Action Required:Ensure consistency is what dates are attached to the policy index (either issue date or review date). 2) Ensure document control processes consistently evidence that polices are reviewed in accordance with the organisations policy.
Timeframe:Six months
Criterion 1.2.3.5 Key components of service delivery shall be explicitly linked to the quality management system.This shall include, but is not limited to:
(a) Event reporting;
(b) Complaints management;
(c) Infection control;
(d) Health and safety;
(e) Restraint minimisation.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.2.3.6 Quality improvement data are collected, analysed, and evaluated and the results communicated to service providers and, where appropriate, consumers.
Audit Evidence Attainment: PA Risk level for PA/UA: LowA range of quality indicators are evaluated each month and are reported as total reported events for the month. The indicators includes episodes of absconding, choking, infections, medication errors, use of restraint, weight loss and wounds. A review of the complaint clinical indicators results sighted does not include all complaints. Only six of twelve reported complaints received since December 2013 have been included. This is an area requiring improvement. A review of the quality indicators for falls and wounds shows all reported events have been included in the quality indicator data for the five residents whose records reviewed at audit.
A register is maintained in each resident file including details of all reported incidents and accidents. This summary is used by the clinical team during care review processes. These patient specific registers do not contain all reported events in four of five resident files reviewed. For one patient only two of four reported falls are summarised. Ensuring the resident registers are current and accurate is also an area requiring improvement.
Finding StatementThe complaint clinical indicators results sighted does not include all complaints. Only six of twelve complaints received since December 2013 have been included. 2) A register is maintained in each resident file including details of all reported incidents and accidents. This summary is used by the clinical team during care review processes. These patient specific registers do not contain all reported events in four of five resident files reviewed. For one patient only two of four reported falls are summarised.
Corrective Action Required:1) Ensure a process is implemented to ensure data reported as clinical indicators are complete/accurate. 2) Ensure the incident and accident registers in individual resident file contains an accurate summary of all reported events.
Timeframe:Six months
Criterion 1.2.3.7 A process to measure achievement against the quality and risk management plan is implemented.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.2.3.8 A corrective action plan addressing areas requiring improvement in order to meet the specified Standard or requirements is developed and implemented.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.2.3.9 Actual and potential risks are identified, documented and where appropriate communicated to consumers, their family/whānau of choice, visitors, and those commonly associated with providing services. This shall include:
(a) Identified risks are monitored, analysed, evaluated, and reviewed at a frequency determined by the severity of the risk and the probability of change in the status of that risk;
(b) A process that addresses/treats the risks associated with service provision is developed and implemented.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.2.4 Adverse Event ReportingAll adverse, unplanned, or untoward events are systematically recorded by the service and reported to affected consumers and where appropriate their family/whānau of choice in an open manner.
ARC D19.3a.vi.; D19.3b; D19.3c ARHSS D19.3a.vi.; D19.3b; D19.3c
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThe ‘Incident/Accident and Sentinel Event Policy’ (updated March 2012) is sighted. The policy provides definitions, guidelines, legislation and management. Template incident reporting forms are documented. Staff interviewed including four HCAs, one RN, a cleaner, a laundry employee, the activities coordinator are able to identify the type of events which are to be reported via the incident/event reporting system. The staff advise they are provided with feedback on reported events as a component of the monthly quality/staff meeting. The staff involved with resident care advise they are also informed of relevant reported events (e.g. falls, wounds and infections) during shift handovers.
The Facility Manager is responsible for ensuring corrective, preventive and follow up actions are completed. Incidents are entered onto the Oceania Group clinical indicator programme to enable benchmarking with other facilities. A range of quality indicators are evaluated each month and are reported as total reported events for the facility per month. The indicators includes episodes of absconding, choking, infections, medication errors, use of restraint, weight loss and wounds. A review of the clinical indicators for falls and wounds shows all reported events (the last three months data reviewed) have been included in the clinical indicator data for the five residents whose records reviewed at audit.
A register is maintained in each resident file including details of all reported incidents and accidents. This summary is used by the clinical team during care review processes. These patient specific registers do not contain all reported events in four of five resident files reviewed. For one patient only two of four reported falls are summarised. Ensuring the resident registers are current and accurate is raised as an area requiring improvement in 1.2.3.6. For all reported events, short term care plans have been developed where required and post fall assessments have been completed.
Sentinel event management is documented. Examples of sentinel events are defined. The FM advises there have been no sentinel events since her employment. The FM is able to identify the type of events which must be reported to external organisations including (but not limited to): the police, Ministry of Health, DHB, Medical Officer of Health and the reporting of serious harm events. The adverse event process requires escalation to the senior management team for essential notifications.
Criterion 1.2.4.2 The service provider understands their statutory and/or regulatory obligations in relation to essential notification reporting and the correct authority is notified where required.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.2.4.3 The service provider documents adverse, unplanned, or untoward events including service shortfalls in order to identify opportunities to improve service delivery, and to identify and manage risk.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.2.7 Human Resource ManagementHuman resource management processes are conducted in accordance with good employment practice and meet the requirements of legislation.
ARC D17.6; D17.7; D17.8; E4.5d; E4.5e; E4.5f; E4.5g; E4.5h ARHSS D17.7, D17.9, D17.10, D17.11
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FARecords are available to evidence that monitoring is occurring of the expiry of relevant staff and contractors annual practising certificates (APCs). Current APCs sighted for the FM, CL, and two RNs, three GPs, one dietitian, and seven pharmacists. A copy of the physiotherapists APC is obtained during audit. A copy of the Pharmacies 'licence to operate' is also present along with a copy of the contract for the provision of GP services. The drivers licence for the three staff who drive the facility vehicle are also on file.
The ‘Orientation Recruitment and Selection Policy’ is sighted. The policy makes reference to the Employment Relations Act 2000, individual employment agreements, position descriptions, recruitment via a recruitment agency, applicant’s legal entitlement to work in New Zealand and the clarification of skills and experience in relation to the role, pre-employment health screening, interview processes, reference checking, police checking and drug screening. A review of seven staff personal files evidences changes in recruitment related documentations and some processes has occurred over time. Robust recruitment processes are occurring. For all four staff employed since 2010 records demonstrating the application process, interview, reference checks, police checks and
completion of the occupational health questionnaire are present. The remaining three files were staff employed between six and seventeen years ago. Police checks are present in all seven staff files reviewed.
Staff are required to complete an orientation programme. Four caregivers, the cleaner and the laundry employee interviewed verify they are buddied with another staff member for orientation. For the HCAs this includes three days supernumery. All six staff advised the orientation suitably prepared them for their roles and includes an introduction to the facility, key policies/procedures, emergency procedures, hand hygiene, infection prevention and control, safe handling of chemicals and residents care needs (where applicable). Records demonstrating staff have completed the organisations orientation programme is present in five of seven staff files reviewed. One staff member is currently still orientating and the remaining staff member was employed over five years ago.
‘Career Pathways Programme Policy’ (July 2012) is sighted. This describes the Competency an Professional Development Framework. The mandatory requirements of each role is defined.
‘Oceania Performance Management Policy’ is sighted (due for review June 2013). Formal appraisals are requires at three months and thereafter annually. Performance appraisals have been undertaken in accordance with this policy (or earlier during orientation) in all staff files reviewed.
There is a comprehensive staff education programme in place. Education is planned over a two year period and includes the requirements to meet both the ARRC contract and the requirements of these standards. Records of attendance are maintained in various formats. Mandatory training is recorded on signing sheets and on an electronic data base. Non mandatory training is recorded on signing sheets. Certificates of attendance (where these are issued) are placed in individual staff files.
Examples of completed training includes (but is not limited to):- delirium: 13 February 2013 (15 staff attended)- infection prevention and control: 13 February 2013 (five staff attended)-quality improvement: 13 February 2013 (five staff attended)- Maori Health plan: 3 April 2013 and August 2013 (a total of 27 staff attended)-abuse and neglect: 10 June 2013 (21 staff attended)- the aging process: 14 August 2013 (15 staff attended)- continence management: 28 August 2013 (19 staff attended)- falls management : 11 September 2013 (22 staff attended)-fire evacuation: 25 September 2013 (29 staff attended). Two other in-services held in May 2013.-chemical handling: 15 November 2013 (16 staff attended)
Twelve staff are currently working to complete an industry approved qualification in dementia care. Records are retained identifying the names of staff
ARRC contract requirements are met.
Criterion 1.2.7.2 Professional qualifications are validated, including evidence of registration and scope of practice for service providers.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.2.7.3 The appointment of appropriate service providers to safely meet the needs of consumers.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.2.7.4 New service providers receive an orientation/induction programme that covers the essential components of the service provided.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.2.7.5 A system to identify, plan, facilitate, and record ongoing education for service providers to provide safe and effective services to consumers.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.2.8 Service Provider AvailabilityConsumers receive timely, appropriate, and safe service from suitably qualified/skilled and/or experienced service providers.
ARC D17.1; D17.3a; D17.3 b; D17.3c; D17.3e; D17.3f; D17.3g; D17.4a; D17.4c; D17.4d; E4.5 a; E4.5 b; E4.5c ARHSS D17.1; D17.3; D17.4; D17.6; D17.8
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThe 'Interim RN shortage Policy’ sighted (updated January 2012). The policy makes reference to the ARRC contract, Hospital Act and the Health Practitioners Competence Assurance Act. A rostering methodology guideline is also sighted dated April 2013 (draft) which reference employer obligations and principals of rostering.Interview with the facility manager advises an electronic programme is used to identify staffing needs. Interview with four HCA and one RN identifies shifts are busy (in particular the morning shift) and help is obtained if the resident needs are high. During audit one resident is sighted being cared for one on one by a HCA as part of a process to manage challenging behaviours. This resident initially had 24 hour individual care which is being adjusted over time.
A review of the roster for the week commencing 7 October 2013 demonstrates:
- the clinical leader works full time hours. -there is a RN on duty five days a week. The RN is present during the morning shifts the CL is not on site and several days when the CL is on site.- the facility manager (who is also a RN) and an office administrator both work full time hours weekdays- an activities coordinator works weekdays (9.am to 4.30 pm). An activities assistant has been recently employed three afternoons a week between 1pm and 4 pm) to work in the dementia unit.- a maintenance man is on site three days a week - the laundry is staff seven days a week (8.am to 3 pm weekdays and 9.am to 1pm on weekends)- a cleaner is on site seven days a week (9.am to 3 pm weekdays and 9.am to 1pm on weekends)- there is a cook and three kitchen assistants working in the kitchen each day between 6.30am and 8 pm
The HCA work the following shifts in the Rest home.A team leader works daily 6.45 am to 3.15 pmtwo HCA work 7 am to 3pm (one CA is specialising a resident 1:1)one HCA works 7 am to 1.30 pmone HCA works 3 pm to 11.15 pmone HCA works 3 pm to 11.00 pmtwo HCA works 11 pm to 7.00 am
The care staff work the following shifts in the Dementia Unit.A team leader works daily 6.45 and to 3.15 pmone HCA works 7 am to 3pm one HCA works 7 am to 12.30 pmone HCA works 3 pm to 11.15 pmone HCA works 3 pm to 10.00 pmone HCA works 11 pm to 7.00 am
There is a designated RN on call from 4.30 pm to 8.am the following day.
The staff working in the dementia unit have either completed an industry approved qualification in dementia care or have been employed less than one year and are currently working to complete this qualification.
There is at least one staff member (normally more) on duty at all times who have a current first aid certificate.
ARRC contract requirements are met.
Criterion 1.2.8.1 There is a clearly documented and implemented process which determines service provider levels and skill mixes in order to provide safe service delivery.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.2.9 Consumer Information Management SystemsConsumer information is uniquely identifiable, accurately recorded, current, confidential, and accessible when required.
ARC A15.1; D7.1; D8.1; D22; E5.1 ARHSS A15.1; D7.1; D8.1; D22
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThe information entered into the eight residents' records reviewed is accurate and up to date. The is no private resident information displayed. All resident records are stored in locked rooms. The progress note entries sighted in the residents’ files reviewed are legible and record the date, time, signature and designation of the staff member. The resident files reviewed evidence integration. Each resident has one folder that contains all their clinical information. A record is maintained of the records that are archived on site. The administration officer reports that records are destroyed after 10 years post resident death/discharge by a contracted documentation destruction service.
The ARRC requirements are met.
Criterion 1.2.9.1 Information is entered into the consumer information management system in an accurate and timely manner, appropriate to the service type and setting.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.2.9.7 Information of a private or personal nature is maintained in a secure manner that is not publicly accessible or observable.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.2.9.9 All records are legible and the name and designation of the service provider is identifiable.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:

Criterion 1.2.9.10 All records pertaining to individual consumer service delivery are integrated.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
OUTCOME 1.3 CONTINUUM OF SERVICE DELIVERYConsumers participate in and receive timely assessment, followed by services that are planned, coordinated, and delivered in a timely and appropriate manner, consistent with current legislation.
STANDARD 1.3.1 Entry To ServicesConsumers' entry into services is facilitated in a competent, equitable, timely, and respectful manner, when their need for services has been identified.
ARC A13.2d; D11.1; D11.2; D13.3; D13.4; D14.1; D14.2; E3.1; E4.1b ARHSS A13.2d; D11.1; D11.2; D13.3; D13.4; D14.1; D14.2
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAResident’s entry into services is facilitated in a competent, equitable, timely, and respectful manner, when their need for services has been identified. Admission Agreements are in place for all residents and sighted which is kept in the Facility Manager's office. On admission, the resident is orientated to the facility and is provided with company pamphlet and book. A resident admission checklist is sighted in order to orient the resident to the facility. The resident comes with a NASC assessment on admission. Informed Consents and Advance Directives are also sighted as part of the admission process. ARRC requirements are met.
Criterion 1.3.1.4 Entry criteria, assessment, and entry screening processes are documented and clearly communicated to consumers, their family/whānau of choice where appropriate, local communities, and referral agencies.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.3.2 Declining Referral/Entry To ServicesWhere referral/entry to the service is declined, the immediate risk to the consumer and/or their family/whānau is managed by the organisation, where appropriate.
ARHSS D4.2
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAWhere referral/entry to the service is declined, the immediate risk to the resident and/or their family/whanau is managed by the organisation, where appropriate. The Clinical Leader (CL) completes a pre-admission Enquiry Form and is kept in the Enquiry Book. She mentions that when they have no occupancy, she informs the family/resident why the entry to the facility is declined and then refers them to other Oceania facilities. The CL declines residents who are hospital level care.
Criterion 1.3.2.2 When entry to the service has been declined, the consumers and where appropriate their family/whānau of choice are informed of the reason for this and of other options or alternative services.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.3.3 Service Provision RequirementsConsumers receive timely, competent, and appropriate services in order to meet their assessed needs and desired outcome/goals.
ARC D3.1c; D9.1; D9.2; D16.3a; D16.3e; D16.3l; D16.5b; D16.5ci; D16.5c.ii; D16.5e ARHSS D3.1c; D9.1; D9.2; D16.3a; D16.3d; D16.5b; D16.5d; D16.5e; D16.5i
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAResident’s receive timely, competent, and appropriate services in order to meet the assessed needs and desired outcome/goals. All the RN’s have a current Annual Practising Certificates as sighted. The Initial Person Centred Care Plan (IPCCP) is in place upon admission as sighted. The clinical leader (CL) and registered nurse (RN) create the Person Centred Care Plan (PCCP) after three weeks and evaluate the PCCP for each resident in a timely manner. The service is coordinated in a manner that promotes continuity in service delivery and promotes a team approach where appropriate. The CL and RN's notify the GP when a new resident is admitted to the facility and the GP admits the new resident within 24-48 hours as per policy. The CL and RN's also notify the GP in a timely manner in the event that a resident manifests medical problems that require immediate attention. The GP advises during interview that his orders are implemented in a timely manner.The RN’s and Health care assistants (HCA's) utilise a hand-over sheet to inform the next shift for any concern about the residents. The contents of the hand-over are comprehensive and appropriate. HCA's write daily in the progress notes while the RN's write separately in the pink progress notes. A communication book is sighted which includes doctor's visits and other resident's issues.Recreation assessment is completed on admission and reviewed in a timely manner but the activities which the resident prefers or intends to participate are not incorporated in the recreation section of the PCCP. A multi-disciplinary review form is sighted which includes recreation evaluation but noted insufficient information about the resident's activities. In two of resident files reviewed in the Dementia Unit, the records are insufficiently detailed to evidence on-going evaluations of the residents response to treatment for urinary tract infections. While investigations are undertaken, on-going evaluation of improvement or deterioration is not evident in the resident files reviewed.
Tracer Methodology 1: (Rest Home Unit) XXXXXX This information has been deleted as it is specific to the health care of a resident. Tracer Methodology 2: (Dementia Unit)XXXXXX This information has been deleted as it is specific to the health care of a resident.Tracer Methodology 3: (Dementia Unit)XXXXXX This information has been deleted as it is specific to the health care of a resident.
The additional files sampled demonstrates that individual resident values and beliefs are not adequately documented and resident or family involvement in completing all assessments cannot be verified for all residents whose record is sampled. (Raised as an area requiring improvement in 1.3.4.2). While activity
assessments are undertaken, individual resident activity plans have not been developed in any of the sampled files. This is an area requiring improvement and is raised in 1.3.5.2.
ARC requirements D3.1c and D16.5cii are not met.
Criterion 1.3.3.1 Each stage of service provision (assessment, planning, provision, evaluation, review, and exit) is undertaken by suitably qualified and/or experienced service providers who are competent to perform the function.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.3.3.3 Each stage of service provision (assessment, planning, provision, evaluation, review, and exit) is provided within time frames that safely meet the needs of the consumer.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.3.3.4 The service is coordinated in a manner that promotes continuity in service delivery and promotes a team approach where appropriate.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.3.4 AssessmentConsumers' needs, support requirements, and preferences are gathered and recorded in a timely manner.
ARC D16.2; E4.2 ARHSS D16.2; D16.3d; D16.5g.ii
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: PA Low
Industry recognised assessment tools are used for assessment to identify individual resident needs.While residents and family members interviewed confirm their individual needs are being met, the needs outcomes and goals of residents are not consistently identified for residents in relation to individual and spiritual needs. Five residents files reviewed in detail contain incomplete information on these topics, and two out of five files do not evidence family or resident involvement in the assessment process. This is an area requiring improvement.ARC requirement D16.2 is not met.
Criterion 1.3.4.2 The needs, outcomes, and/or goals of consumers are identified via the assessment process and are documented to serve as the basis for service delivery planning.
Audit Evidence Attainment: PA Risk level for PA/UA: Low
Resident’s needs, support requirements, and preferences are gathered and recorded in a timely manner. Recognised tools such as Waterlow Pressure, Tinetti assessment for gait/balance/falls, dietary, continence, cultural, recreation, mobility, bowel, MMSE, Abbey Pain, Geriatric, Mini-nutrition and oral are used for the basis of creating the
resident’s IPCCP and PCCP. The CL and RN's create the PCCP for each resident within three weeks and evaluates these PCCP every six months through a multi-disciplinary review. The NASC assessment for each resident is taken into consideration and is used as a basis for care planning.The needs, outcomes, and/or goals of the residents are identified via the assessment process and are documented to serve as the basis for service delivery planning. The CL and RN's create the IPCCP upon admission and is replaced by the PCCP within three weeks as per policy and is sighted. It defines the goals and the interventions for each domain and is evaluated in a timely manner. Not all PCCP's are sufficiently detailed to include individual needs/values/beliefs. This is an area for improvement. For example, while residents and family members are interviewed confirm their individual needs are met, the needs, outcomes and goals of residents are not consistently identified for residents in relation to individual and spiritual needs. Five residents files reviewed in detail contain incomplete information, and two out of five files do not evidence family or resident involvement in the assessment process.
Short term care plans are created and sighted for residents with infections (although not all are individualised - Refer to CAR 1.3.5.2). A wound care plan and management is in place and sighted for the resident with bilateral leg ulcers. Recreation assessment is completed upon admission and evaluated every six months by the Activities Coordinator. The desired goal is clearly stated in the recreation section of the PCCP.
Finding StatementWhile residents and family members interviewed confirm their individual needs are being met, the needs outcomes and goals of residents are not consistently identified for residents in relation to individual and spiritual needs. Five residents files reviewed in detail contain incomplete information, and two out of five files do not evidence family or resident involvement in the assessment process.
Corrective Action Required:Ensure that individual resident cultural and spiritual needs are identified (with the involvement of the resident and/ or family) and documented during the assessment process.
Timeframe:Six months
STANDARD 1.3.5 PlanningConsumers' service delivery plans are consumer focused, integrated, and promote continuity of service delivery.
ARC D16.3b; D16.3f; D16.3g; D16.3h; D16.3i; D16.3j; D16.3k; E4.3 ARHSS D16.3b; D16.3d; D16.3e; D16.3f; D16.3g
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: PA Low
Service delivery plans are resident focused, integrated, and promote continuity of service delivery. PCCP’s are created and evaluated six monthly manner. Appropriate interventions are in place to meet the desired outcomes. The PCCP's are not sufficiently detailed in relation to residents individual cultural and spiritual needs. Whilst activity assessments are being undertaken; individual resident activity plans are not developed. Generic short term care plans are used when patients in the dementia unit are suspected or diagnosed as having an infection. The interventions are not always relevant to individual resident's needs as evidenced in the two files sampled. These are areas requiring improvement.
All documentations are integrated in each resident folder with allocated sections for the GP, RN and HCA progress notes, allied services, assessment tools and references. The eight of eight PCCP's reviewed reflect goals and appropriate interventions to achieve the desired outcomes. Any required changes to resident’s care is written in the progress notes or in the short term care plan. Generic short term care plans are used in the dementia unit and do not reflect the resident needs in two of two occasions. Evaluation of a residents progress when an infection is considered is not consistently documented in the dementia unit and this is an area for improvement in 1.3.8.2. ARC requirements D16.3g, D16.3h, D16.3.3i, D16.3j. are not met.
Criterion 1.3.5.2 Service delivery plans describe the required support and/or intervention to achieve the desired outcomes identified by the ongoing assessment process.
Audit Evidence Attainment: PA Risk level for PA/UA: Low
Service delivery plans describe the required support and/or intervention to achieve the desired outcomes identified by the on-going assessment process. However, the PCCP's are not sufficiently detailed to identify how a residents individual cultural and spiritual care needs will be met. In all five of five residents file reviewed in detail the care plan identifies 'all reasonable steps shall be taken to meet identified needs'. What the resident’s individual or identified needs are is not clearly detailed. Despite this all seven residents and all four members confirm staff are aware of the residents individual needs and these are being met in a timely manner.
While activities assessments are undertaken, an activities plan for individual residents has not been documented for all residents whose records reviewed at audit..
Generic short term care plans are being used when residents are suspected or diagnosed as having an infection. The care plans include components that are not relevant to the individual residents whose records are reviewed. PCCP’s are created and evaluated in a timely manner. Appropriate interventions are in place to meet the desired outcomes.
The GP interviewed reports excellent communication with the CL and RN's to ensure continuity of care for the residents. There is no individual activity plan sighted.
Finding Statement1.The PCCP's are not sufficiently detailed to identify how a residents care needs will be met. For example while activities assessments are undertaken, an activities plan for individual residents have not been documented. The cultural and individual needs component of the PCCP does not always align with the assessments. In all five of five residents file reviewed in detail the care plan identifies 'all reasonable steps shall be taken to meet identified needs'. What the residents individual or identified needs are not consistently detailed. 2. Generic short term care plans are being used when residents are suspected or diagnosed as having an infection. The care plans include components that are not relevant to the individual residents whose records are reviewed.
Corrective Action Required:Ensure the PCCP's and short term care plans are sufficiently detailed to describe the interventions required to meet the residents individual needs.
Timeframe:Six months
Criterion 1.3.5.3 Service delivery plans demonstrate service integration.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.3.6 Service Delivery/InterventionsConsumers receive adequate and appropriate services in order to meet their assessed needs and desired outcomes.
ARC D16.1a; D16.1b.i; D16.5a; D18.3; D18.4; E4.4 ARHSS D16.1a; D16.1b.i; D16.5a; D16.5c; D16.5f; D16.5g.i; D16.6; D18.3; D18.4
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FA
Resident’s receive adequate and appropriate services in order to meet their assessed needs and desired outcomes. Appropriate interventions are sighted in the resident’s PCCP. New residents are welcome and orientated to the facility. They utilise a resident orientation checklist as sighted. The eight of eight resident’s PCCP clearly defines the appropriate interventions in order to meet the desired goal (with the exceptions as noted in 1.3.5.). Interventions sighted includes (but is not limited to): pain management, assisting residents with changing care needs in relation to activities of daily living, diagnosis and treatment of infections, and provision of wound care.
Appropriate interventions are monitored by all RN’s and HCA's on duty. Any modification or addition to the planned interventions are updated accordingly by the CL and RN's. All eight resident and all four family members confirm their care needs are met.
ARRC requirements are met.
Criterion 1.3.6.1 The provision of services and/or interventions are consistent with, and contribute to, meeting the consumers' assessed needs, and desired outcomes.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.3.7 Planned ActivitiesWhere specified as part of the service delivery plan for a consumer, activity requirements are appropriate to their needs, age, culture, and the setting of the service.
ARC D16.5c.iii; D16.5d ARHSS D16.5g.iii; D16.5g.iv; D16.5h
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FA
Activity requirements are appropriate to the resident’s needs, age, culture, and the setting of the service. The activities coordinator and activities assistant create a weekly plan of activities and posts these plans in the bulletin boards. Each resident has a recreation assessment which is reviewed every six months by the activities coordinator. Activity programme attendance sheet's per resident are maintained and sighted. The resident’s in the dementia unit have activities that are more appropriate for them. Those who are able to participate in the rest home unit activities are also welcome to join. The activities coordinator and activities assistant use both group and one-on-one approach in facilitating activities for the residents. There are some residents who refuse to participate in group activities whom the activities assistant spends time or some HCA's the residents prefer. The programme includes activities that are physical, intellectual, sensory, social and fun. Activities in progress during audit are sighted to have good resident participation. Seven of seven residents interviewed and the four family members confirm the activities programme offers choice and the residents can participate in activities they enjoy. One rest home resident has a spouse in the dementia unit. The resident from the dementia unit spends most of the day with the Resthome level resident in the Resthome resident’s room. The rest home resident and a family member interviewed confirm this arrangement suits both residents very well and was one of the considerations when seeking a long term care facility. Both the Resthome level care resident, the family member, the facility manager and staff advise there are no concerns about the security and safety of the resident with dementia who does not wander and stays with the spouse.
While individual resident activity assessments are being done, individual resident care plans have not been developed. This is raised as an area for improvement in 1.3.5.2.
ARRC requirements are met.
Criterion 1.3.7.1 Activities are planned and provided/facilitated to develop and maintain strengths (skills, resources, and interests) that are meaningful to the consumer.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.3.8 EvaluationConsumers' service delivery plans are evaluated in a comprehensive and timely manner.
ARC D16.3c; D16.3d; D16.4a ARHSS D16.3c; D16.4a
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: PA Low
Resident’s PCCP's are evaluated in a comprehensive and timely manner. Eight of eight resident's PCCP are reviewed every six months through a multi-disciplinary review and evidence is sighted. Recreation assessments are reviewed by the activities coordinator in a timely manner. Liaison with other services is recorded by the CL and RN's in the communication book.
Where progress is different to expectations changes in care are provided. Examples sighted at audit wound care, increased protein diet, pain management, staff worked to provide distractions and interactions to deescalate challenging behaviour and when infections were suspected, urinalysis undertaken and oral intake increased.
In two of two resident files reviewed in the dementia unit where the resident had an infection, the records are insufficiently detailed to evidence on-going evaluations of the resident’s response to treatment for urinary tract infections. While investigations are undertaken, on-going evaluation of improvement or deterioration is not evident in the resident files reviewed.
Short term care plans are created by the CL and RN's in order to resolve problems like urinary tract infection (UTI), wounds and other medical events. The RN's contact the GP further medical intervention or advise as well as the company dietician for residents with weight loss. The CL refers the residents to appropriate external services i.e. Care Team-Mental Health Services. In the two short term care plans in the Dementia Unit, the interventions noted are not individualised and not all interventions noted are relevant to the resident audited. (Refer to 1.3.5.2).ARC requirements D16.3c, D16.3d, D16.4a are not met.
Criterion 1.3.8.2 Evaluations are documented, consumer-focused, indicate the degree of achievement or response to the support and/or intervention, and progress towards meeting the desired outcome.
Audit Evidence Attainment: PA Risk level for PA/UA: LowIn the majority of resident files reviewed evaluations are documented, resident-focused, indicate the degree of achievement or response to the support and/or intervention, and progress towards meeting the desired outcome. The exception noted at audit is documented response to treatment of two residents with urinary tract infections in the Dementia Unit. Eight of eight resident's PCCP are reviewed every six months through a Multi-Disciplinary Review and evidence is sighted. Recreation assessments are reviewed by the Activities Coordinator in a timely manner. Liaison with other services is recorded by the CL and RN's in the communication book.
Finding StatementIn two of resident files reviewed in the Dementia Unit, the records are insufficiently detailed to evidence on-going evaluations of the residents response to treatment for urinary tract infections. While investigations are undertaken, on-going evaluation of improvement or deterioration is not evident in the resident files reviewed.
Corrective Action Required:Ensure that evaluations are sufficiently documented to evidence residents response to changes in treatment/care for suspected infections.
Timeframe:Six months
Criterion 1.3.8.3 Where progress is different from expected, the service responds by initiating changes to the service delivery plan.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.3.9 Referral To Other Health And Disability Services (Internal And External)Consumer support for access or referral to other health and/or disability service providers is appropriately facilitated, or provided to meet consumer choice/needs.
ARC D16.4c; D16.4d; D20.1; D20.4 ARHSS D16.4c; D16.4d; D20.1; D20.4
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAResident’s support for access or referral to other health and/or disability service providers is appropriately facilitated, or provided to the president’s choice/needs. The CL and RN's refers the resident accordingly as per medical condition, either to the GP or to the public hospital. The CL refers residents to Mental Health Services for Older People who responds accordingly in a timely manner. She sends information’s to them including medical history and a copy of the medication sheet and provides a copy for the GP as well. The GP refers the residents to the appropriate specialists for further investigation and management. The CL also refers the resident to their company dietician when there is weight loss or swallowing problems. Referral form is sighted and is kept in the resident’s folder.ARRC requirements are met.
Criterion 1.3.9.1 Consumers are given the choice and advised of their options to access other health and disability services where indicated or requested. A record of this process is maintained.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.3.10 Transition, Exit, Discharge, Or TransferConsumers experience a planned and coordinated transition, exit, discharge, or transfer from services.
ARC D21 ARHSS D21
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAResident’s experience a planned and coordinated transition, exit, discharge, or transfer from services. The facility utilises a resident transfer form which is included in the yellow envelope when the resident needs to admitted in public hospital, or when transferred to another facility. The resident’s PCCP is also attached with the resident transfer form as identified by staff during interview.ARRC requirement is met.
Criterion 1.3.10.2 Service providers identify, document, and minimise risks associated with each consumer's transition, exit, discharge, or transfer, including expressed concerns of the consumer and, if appropriate, family/whānau of choice or other representatives.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.3.12 Medicine ManagementConsumers receive medicines in a safe and timely manner that complies with current legislative requirements and safe practice guidelines.
ARC D1.1g; D15.3c; D16.5e.i.2; D18.2; D19.2d ARHSS D1.1g; D15.3g; D16.5i..i.2; D18.2; D19.2d
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: PA HighThe medicine management system is implemented by the service that facilitates safe prescribing, dispensing, review and reconciliation. All staff giving medications are competent as sighted in their files. The staff competency programme does not include controlled drugs and this is an area requiring
improvement. All applicable staff and contractors Annual Practising Certificates are current as sighted. At audit, areas for improvement are also raised in ensuring a safe process for crushing medications, storage of controlled drugs, ensuring medication is kept within expiry dates and only for current residents and documentation related to returning unwanted medications back to pharmacy. Ensuring that staff are competent for controlled drugs administration is also an area for improvement raised in 1.3.12.3.The policy and procedure for self-administration of medicines is sighted. The are no residents currently self-administering medications. The CL is able to explain the procedure during the interview process on how a resident can self-administer medications e.g. the RN will assess the resident for competency and will be signed off by the GP. The RN will check the resident and will sign in the medication folder. The GP reviews the resident medications every three months. The medicines will be kept inside a locked cupboard in the resident's room. The medicine management information is recorded to a level of detail and communicated to the resident's to comply with legislation and guidelines. The signing sheets are colour coded i.e. red for controlled drugs. At audit, areas for improvement are identified including administration of regular medications, administration and storage of controlled drugs as well as returning expired/unwanted medications to the pharmacy. ARC requirements D1.1g, D15.3c, D19.2d are not met.
Criterion 1.3.12.1 A medicines management system is implemented to manage the safe and appropriate prescribing, dispensing, administration, review, storage, disposal, and medicine reconciliation in order to comply with legislation, protocols, and guidelines.
Audit Evidence Attainment: PA Risk level for PA/UA: HighThe medicine management system is implemented by the service that facilitates safe prescribing, dispensing, administration, review, storage, and reconciliation. The treatment room can be opened by RN's using sets of keys. The facility uses the robotics system for their medications. Sharps bins are sighted in the treatment rooms. The controlled drug cupboard is locked inside a locked cupboard in the treatment room. Controlled drug register sighted. The GP signs the drug chart on admission and will be sent to the pharmacy who will generate a medication sheet which is also signed by the GP. The 16 of 16 medication charts sighted are reviewed by the GP in a timely manner (at least every three months). The GP signs and dates all discontinued medications. Medication reconciliation system is in place on admission and medication reconciliation form is sighted. Controlled drugs are entered to the controlled drugs register by the RN's upon receiving the medicines from the pharmacy. A weekly stock take is implemented and recordings are sighted. Three medication rounds are witnessed.All medication charts have photos, special instructions and allergies. Medication return (unwanted and expired medications) are collected every week by the pharmacy staff. A register is not being maintained as required to meet the organisation’s policies and is an area requiring improvement. The GP sends a fax to the facility for antibiotics or changes in the medication. The CL reports that they do not receive telephone orders from the GP. Fridge monitoring is being done every week by the RN. Medication reconciliation processes are in place.During audit is in noted a number of practices do not comply with current accepted practices. These include.1. All medications are being crushed and administered to some residents in the Dementia Unit. This process has not been reviewed for the residents to ensure the safety in relation to medications being crushed. The medication management policy does not provide guidance to the staff on the process required to ensure medications can be safely crushed.2. A bottle of XXXX elixir is not stored inside the CD safe as it is too big. The bottle is stored inside a locked cupboard outside the safe. 3. Controlled drugs are noted to have been signed as administered by the RN's. The medications had not been administered at the time and are sighted in a blister pack outside the CD safe in the locked cupboard. These medications are for administration with the evening meal. The staff administering the medications have not been involved with the documentation in the controlled drug register. The RN's interviewed advised that this is their normal practice as there is no RN on duty 24/7.
4. Three boxes of XXXX are sighted inside the fridge. The identified resident has not been in the facility for at least two years. A bottle of XXXXX is use has an expiry date of January 2013. 5. Unwanted and expired medications are being returned to the pharmacy. A register is not being maintained of what items are being returned in variance to the organisations policy.
Finding Statement1. All medications are being crushed and administered to some residents in the Dementia Unit. This process has not been reviewed for the residents to ensure the safety in relation to medications being crushed. The medication management policy does not provide guidance to the staff on the process required to ensure medications can be safely crushed.2. A bottle of XXXXX elixir is not stored inside the CD safe as it is too big. The bottle is stored inside a locked cupboard outside the safe. 3. Controlled drugs i.e. XXXXX are noted to have been signed as administered by the RN's. The medications had not been administered at the time and are sighted in a blister pack outside the CD safe in the locked cupboard. These medications are for administration with the evening meal. The staff administering the medications have not been involved with the documentation in the controlled drug register. The RN's interviewed advised that this is their normal practice as there is not a RN on duty 24/7. 4. Three boxes of XXXXX are sighted inside the fridge. The medications are for an identified resident who has not been in the facility for at least two years. A bottle of XXXXX is use has an expiry date of January 2013. 5. Unwanted and expired medications are being returned to the pharmacy. A register is not being maintained of what items are being returned in variance to the organisations policy. At audit, areas for improvement are identified including administration of regular medications, administration and storage of controlled drugs as well as returning expired/unwanted medications to the pharmacy.
Corrective Action Required:Ensure all components of medication management practices meet professional and legislative requirements.
Timeframe:One month
Criterion 1.3.12.3 Service providers responsible for medicine management are competent to perform the function for each stage they manage.
Audit Evidence Attainment: PA Risk level for PA/UA: ModerateService providers responsible for medicine management are assessed annually for competency in medication administration. The competency process is verified at audit with competency assessments for oral medications completed and present in staff files. The medication competency register is also sighted. The competency does not include controlled drugs and caregivers are administering controlled drugs. This is an area requiring improvement.
Finding StatementWhilst there is a medication competency assessment process which is sighted to be implemented; the competency assessment does not include controlled drugs which are being administered on site by the health care assistants.Corrective Action Required:Ensure the medication competency assessment process includes controlled medications.
Timeframe:Three months
Criterion 1.3.12.5 The facilitation of safe self-administration of medicines by consumers where appropriate.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.3.12.6 Medicine management information is recorded to a level of detail, and communicated to consumers at a frequency and detail to comply with legislation and guidelines.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.3.13 Nutrition, Safe Food, And Fluid ManagementA consumer's individual food, fluids and nutritional needs are met where this service is a component of service delivery.
ARC D1.1a; D15.2b; D19.2c; E3.3f ARHSS D1.1a; D15.2b; D15.2f; D19.2c
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAFood, fluid and nutritional needs of residents are provided in line with recognised nutritional guidelines. The RN completes the Dietary Assessment on admission and the cook signs this form with another copy kept in the kitchen file. The original Dietary Assessment form is kept in the resident's file. The cook updates the list of residents in the kitchen bulletin board as necessary. List of residents on special diets are sighted in the kitchen bulletin board. In the event that a resident loses weight, the RN commences a short term care plan, food & fluid monitoring charts, liaises with the cook to commence on high protein drink and refers the resident to the GP for possible food supplement. Weights are done monthly and evaluated by the RN's while residents who lose weight are weighed weekly. The CL refers the resident to the dietician when residents continue losing weight despite their management. Fluid restrictions and consistencies are noted in their care plans. Residents who have additional or modified nutritional requirements or special diets have their needs met. The RN and the cook coordinate if diet modification happens. The dietician provides guidelines to the RN and cook. Staff are aware of the resident's diet. Any change in the resident's diet is coordinated by the CL to the cook in a timely manner.Seven of eight residents and three of four family members interviewed confirm being provided with food choices and that the meals provided meets the resident’s needs. One resident advises there is too much mince or meat in gravy on the menu and wants some more substantial types of meat. This resident confirms if there are food items on the menu that are not liked; staff readily provide an alternative meal choice. All residents and family members confirm there is sufficient quantity of food provided.All aspects of food procurement, production, preparation, storage, transportation, delivery and disposal comply with current legislation and guidelines. Kitchen and other staff wear disposable hats when preparing and serving meals. Fridge and freezer temperatures are monitored and recorded daily. Recording sheets are sighted. Food production temperature is sighted. All cooked foods in the fridge are dated as well as all canned goods. Foods in the fridge are also labelled and dated properly. The menu is reviewed by the Dietician as sighted. The cook verbalises that there are enough equipment’s that she needs in preparing the meals. All kitchen equipment’s that need fixing is checked by the maintenance person and disposes equipment’s as needed There are enough supply of food in the store room in the event of an emergency. The kitchen is free from mouse droppings and no food is touching the floor. The kitchen staff utilise a communication book to inform other kitchen staff on what has been prepared and any kitchen-related concerns. The cook and all kitchen staff hold current Food Safety Certificates as sighted. The foods are labelled and dated properly as sighted inside the fridge. Food Production Temperature Sheet, Food Service Sheet are sighted. Fridge and Freezer Temperature Monitoring is done once per day. A kitchen cleaning schedule is sighted. An Emergency Menu Plan is in place as well as the Emergency Stocks are sighted. The cook reports that they can provide sufficient food for residents and staff for at least a month in the event of an emergency.ARC requirement are met.
Criterion 1.3.13.1 Food, fluid, and nutritional needs of consumers are provided in line with recognised nutritional guidelines appropriate to the consumer group.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.3.13.2 Consumers who have additional or modified nutritional requirements or special diets have these needs met.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.3.13.5 All aspects of food procurement, production, preparation, storage, transportation, delivery, and disposal comply with current legislation, and guidelines.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
OUTCOME 1.4 SAFE AND APPROPRIATE ENVIRONMENTServices are provided in a clean, safe environment that is appropriate to the age/needs of the consumer, ensures physical privacy is maintained, has adequate space and amenities to facilitate independence, is in a setting appropriate to the consumer group and meets the needs of people with disabilities.These requirements are superseded, when a consumer is in seclusion as provided for by of NZS 8134.2.3.
STANDARD 1.4.1 Management Of Waste And Hazardous SubstancesConsumers, visitors, and service providers are protected from harm as a result of exposure to waste, infectious or hazardous substances, generated during service delivery.
ARC D19.3c.v; ARHSS D19.3c.v
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThe 'Accidental Exposure of Blood/Body Fluids policy, 'Soiled linen Policy' and 'Health care Waste Policy' sighted. These provide guidance for staff on expected practices and managing untoward events.
The Emergency Response flip charts are located strategically throughout the facility and includes management of hazardous materials (HAZMAT) incident management and chemical spillage.
Supplies of appropriate personal protection sighted at audit included aprons, gloves, masks and eye protection. Supplies for use in an emergency/pandemic event are located in a designated cupboard. Seven staff interviewed including four HCAs, a cleaner, the laundry employee and the RN and the facility manager confirm there are adequate supplies of PPE always readily available.
Waste and hazardous substances sighted being disposed of in accordance with the organisations policy. Sharps containers are available for the disposal of sharps. Waste and hazardous substances are clearly labelled. Chemicals are stored in containers with manufacturer original labels.
The ARRC requirements are met.
Criterion 1.4.1.1 Service providers follow a documented process for the safe and appropriate storage and disposal of waste, infectious or hazardous substances that complies with current legislation and territorial authority requirements.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement Corrective Action Required:
Timeframe:
Criterion 1.4.1.6 Protective equipment and clothing appropriate to the risks involved when handling waste or hazardous substances is provided and used by service providers.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.4.2 Facility SpecificationsConsumers are provided with an appropriate, accessible physical environment and facilities that are fit for their purpose.
ARC D4.1b; D15.1; D15.2a; D15.2e; D15.3; D20.2; D20.3; D20.4; E3.2; E3.3e; E3.4a; E3.4c; E3.4d ARHSS D4.1c; D15.1; D15.2a; D15.2e; D15.2g; D15.3a; D15.3b; D15.3c; D15.3e; D15.3f; D15.3g; D15.3h; D15.3i; D20.2; D20.3; D20.4
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThe building has a current building warrant of fitness (WOF) with an expiry date of 2 July 2014. Ongoing checks to maintain the building WOF are being maintained and records of this are sighted.Electrical test and tagging (ETT) is being undertaken and all equipment sighted in use in the rest home and dementia unit have current test and tag labels. A number of extension cords located in the maintenance man’s office had expired ETT labels. These items were tested and tagged during audit. Calibration of clinical equipment is occurring and sitting scales, tympanic thermometer, the hoist and sphygmomanometer all have current performance monitoring labels present (expiry May 2014). Monitoring is occurring of the hot water temperature in resident care areas monthly. Where the temperature is noted to be above 45 degrees Celsius remedial activities have been undertaken and the water retested to be within required limits.The environment promotes the safe mobilisation of residents. There are handrails present in the hallways. Grab rails are present in all bathroom areas reviewed at random during audit. The floor surfaces are flat with no unexpected ledges or gradients. The corridors are uncluttered. Mobility scooters have a designated storage area. Residents sighted mobilising in the corridors independently including residents using walking frames. The maintenance man demonstrated the process of reporting maintenance issues and all reported tasks are noted to have been completed in a timely manner.
There are external courtyards which are accessible by residents including within the secure dementia unit. All seven rest home residents interviewed and all four family members interviewed (one in the rest home and three in the dementia unit) confirm the facility is maintained and there is sufficient space to mobilise around.The facility vehicle is new and has a wheelchair hoist, a current warrant of fitness and registration.
The ARRC requirements are met.
Criterion 1.4.2.1 All buildings, plant, and equipment comply with legislation.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.4.2.4 The physical environment minimises risk of harm, promotes safe mobility, aids independence and is appropriate to the needs of the consumer/group.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.4.2.6 Consumers are provided with safe and accessible external areas that meet their needs.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.4.3 Toilet, Shower, And Bathing FacilitiesConsumers are provided with adequate toilet/shower/bathing facilities. Consumers are assured privacy when attending to personal hygiene requirements or receiving assistance with personal hygiene requirements.
ARC E3.3d ARHSS D15.3c
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThere are sufficient showers and toilets on site for use by residents as verified during a visual walk-a-bout the facility. In each wing there are all resident use showers and separate toilets including those near the lounge areas. Ablution areas have privacy mechanism and signage present which notes if the room is engaged and vacant. Three HCAs and the facility manager interviewed confirm there are enough toilets and showers available for residents' use.
The ARRC requirements are met.
Criterion 1.4.3.1 There are adequate numbers of accessible toilets/showers/bathing facilities conveniently located and in close proximity to each service area to meet the needs of consumers. This excludes any toilets/showers/bathing facilities designated for service providers or visitor use.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.4.4 Personal Space/Bed AreasConsumers are provided with adequate personal space/bed areas appropriate to the consumer group and setting.
ARC E3.3b; E3.3c ARHSS D15.2e; D16.6b.ii
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAAll 55 patient bedrooms are single occupancy. There is sufficient space in the rooms for residents to mobilise including while using mobility devices. This is verified during a visual review of the facility and during interview with staff and all four family members interviewed (one rest home level care and three dementia level care) and all seven rest home residents interviewed.
The ARRC requirements are met.
Criterion 1.4.4.1 Adequate space is provided to allow the consumer and service provider to move safely around their personal space/bed area. Consumers who use mobility aids shall be able to safely maneuvers with the assistance of their aid within their personal space/bed area.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.4.5 Communal Areas For Entertainment, Recreation, And DiningConsumers are provided with safe, adequate, age appropriate, and accessible areas to meet their relaxation, activity, and dining needs.
ARC E3.4b ARHSS D15.3d
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAAll 55 bedrooms are single occupancy. There is a larger designated activity room in the rest home, a large library /lunge area and a dining area. There is also a smaller lounge and two beverage bays with tea &coffee making facilities. There is a lounge and separate dining area in the dementia unit.
All four family members interviewed (one rest home level care and three dementia level care) and all seven rest home residents interviewed confirm there is adequate communal and recreation areas available for the residents.
The ARRC requirements are met.
Criterion 1.4.5.1 Adequate access is provided where appropriate to lounge, playroom, visitor, and dining facilities to meet the needs of consumers.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.4.6 Cleaning And Laundry ServicesConsumers are provided with safe and hygienic cleaning and laundry services appropriate to the setting in which the service is being provided.
ARC D15.2c; D15.2d; D19.2e ARHSS D15.2c; D15.2d; D19.2e
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAMonitoring the effectiveness of the cleaning and laundry services is undertaken via the audit programme and resident satisfaction survey. Internal audits of cleaning was undertaken in April 2013 and October 2013 and of the laundry services in March and September 2013. The results show a high level of compliance with the organisations policies. The results are discussed with staff involved and at staff meetings as verified in minutes sighted and staff interviews.
Resident’s personal laundry and a small amount of delicate facility laundry is washed on site. Residents interviewed report the cleaned laundry is normally returned within 24 hours. The majority of facility linen is laundered and dried off site. Soiled linen is collected on a daily basis weekdays.All chemicals sighted at audit are stored securely. Cleaning chemicals are mixed via wall mounted auto mixing units. The cleaning trolleys are locked in a designated room when not in use. All four family members interviewed (three dementia level care and one rest home level care) and all seven rest home residents interviewed confirm the facility is kept clean and tidy and their personal laundry is returned in a timely manner.
The ARRC requirements are met.
Criterion 1.4.6.2 The methods, frequency, and materials used for cleaning and laundry processes are monitored for effectiveness.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.4.6.3 Service providers have access to designated areas for the safe and hygienic storage of cleaning/laundry equipment and chemicals.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.4.7 Essential, Emergency, And Security SystemsConsumers receive an appropriate and timely response during emergency and security situations.
ARC D15.3e; D19.6 ARHSS D15.3i; D19.6
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FATraining on management of fire, tsunami and other emergency procedures is included in the orientation programme. The facility is located in close proximity to Browns Bay Beach. Records verifying completion of the orientation programme are present in five of seven staff files reviewed. One staff member is still completing the orientation programme. The 'Disaster and Emergency Management Plan' is dated as being updated in April 2013. There are emergency response flip charts throughout the facility which provides guidance for staff on the management of emergency events including (but not limited to):- fire evacuation- threat to personal safety- unauthorised person/unwelcome visitor- utility failure- robbery or hold up- gale force winds or flooding- earthquake or volcanic activity-emergency care (accident or collapse)- missing resident- shock- eye injury- severe bleeding-choking-epileptic fitsThere are at least 18 staff with a current first aid certificate or resuscitation (level two) certificate. Certificates evidencing training are present in applicable staff files reviewed during audit. A list of staff with a current first aid certificate is displayed in the staff room and staff office areas. There is always at least one staff member (normally two) on duty at all times with a current first aid/resuscitation certificate as verified on the roster sighted. Maureen Plowman Home has a fire evacuation plan which has been approved by the New Zealand Fire Service in a letter dated 15 November 2006. The most recent fire evacuation drill occurred on 1 August 2013 and the evacuation time was 6 minutes. Training on fire safety procedures was last provided to staff on 25 September 2013 and 29 staff attended. Call bells are present in all bedrooms and bathrooms areas. All seven family rest home residents interviewed advise call bells are answered in a timely manner.
There are adequate supplies of equipment and utilities for use in emergency. This is includes a BBQ and spare bottle of gas. There are supplies of portable medical gas (oxygen), pandemic equipment, and equipment for use in an emergency (torches, PPE, disposable crockery and cutlery, lighters/matches, batteries and a radio. Supplies of dried food stuffs and 740 litres of drinking water is available. The quantity and expiry date of each item is noted to be checked regularly. Spare blankets/duvets are sighted in the linen cupboard. The front doors automatically lock automatically at 5 pm at night. Visitors can enter after this time if they know the keypad access number. Otherwise there is a phone at the front door that visitors can use to contact staff who come and let visitors in if necessary. The afternoon caregiver interviewed advised staff are required to check all doors and windows are locked each night and that all residents are accounted for. A contracted security company patrols and checks the outside of the building three times over the evening and night.
The ARRC requirements are met.
Criterion 1.4.7.1 Service providers receive appropriate information, training, and equipment to respond to identified emergency and security situations. This shall include fire safety and emergency procedures.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.4.7.3 Where required by legislation there is an approved evacuation plan.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.4.7.4 Alternative energy and utility sources are available in the event of the main supplies failing.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.4.7.5 An appropriate 'call system' is available to summon assistance when required.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.4.7.6 The organisation identifies and implements appropriate security arrangements relevant to the consumer group and the setting.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 1.4.8 Natural Light, Ventilation, And HeatingConsumers are provided with adequate natural light, safe ventilation, and an environment that is maintained at a safe and comfortable temperature.
ARC D15.2f ARHSS D15.2g
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAAll residents' bedrooms have a large window. There are no unpleasant odours present. The maintenance man advised the heating automatically turns on if the temperature is below the set parameters and thermostat sighted to be activated episodically during audit. The temperature is currently set at 22 degrees C at audit. Heating is provided centrally and is within the ceiling compartment. Several resident rooms and the lounge in the dementia unit have additional wall or ceiling mounted heating. All four family members interviewed (three dementia level care and one rest home level care) and all seven rest home residents interviewed verify the facility is appropriately warm and ventilated.
There is no smoking onsite. The ARRC requirements are met.
Criterion 1.4.8.1 Areas used by consumers and service providers are ventilated and heated appropriately.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 1.4.8.2 All consumer-designated rooms (personal/living areas) have at least one external window of normal proportions to provide natural light.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
2. HEALTH AND DISABILITY SERVICES (RESTRAINT MINIMISATION AND SAFE PRACTICE) STANDARDS
OUTCOME 2.1 RESTRAINT MINIMISATION
STANDARD 2.1.1 Restraint minimisationServices demonstrate that the use of restraint is actively minimised.
ARC E4.4a ARHSS D16.6
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAService provider demonstrates that the use of restraint is actively minimised. The CL and care staff advise there is currently no residents with personal restraint in use and no restraints are sighted in use during audit. A restraint register is sighted. Assessment and consent forms are available and in use for the most recent resident who had restraints used. One resident had a lap belt in use in August 2013 for two days due to inappropriate behaviour. The resident progressed to having one on one care during all shifts. Documentation on the use of the lap belt is sighted in the residents' progress notes, and a challenging behaviour monitoring form is completed and sighted. Risk minimisation is documented in the residents’ PCCP. The use of restraint i.e. lap belt is communicated to the family as well as with the care team (Mental Health Services). The resident is also provided with explanation on why the need for restraint. The DHB care team provided is involved in this residents care and reviewed the resident’s medication through their psychiatrist. The resident is now settled and has one-on-care now in the mornings only. The resident is free to mobilise in the mornings with this supervision. The resident is deemed to not require individualised supervision in the afternoons and during the night.
There is no residents using enablers. Restraint policy is sighted and includes an enabler being voluntary with the intention to promote or maintain independence and safety. Staff interviewed are able to discuss what is an enabler and the rationale of using it.All staff have a current restraint competency as sighted.ARRC requirement is met.
Criterion 2.1.1.4 The use of enablers shall be voluntary and the least restrictive option to meet the needs of the consumer with the intention of promoting or maintaining consumer independence and safety.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
3. HEALTH AND DISABILITY SERVICES (INFECTION PREVENTION AND CONTROL) STANDARDS
STANDARD 3.1 Infection control managementThere is a managed environment, which minimises the risk of infection to consumers, service providers, and visitors. This shall be appropriate to the size and scope of the service.
ARC D5.4e ARHSS D5.4e
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThe responsibility for infection control is clearly defined and there are clear lines of accountability for infection control matters in the facility. The CL is the infection control co-ordinator. The facility has a clearly defined infection prevention and control program that is reviewed annually. Infection control is part of health and safety meeting every month. When a resident is suspected having urinary tract infection (UTI), the RN performs an assessment, obtains mid-stream urine sample, performs dipstick and sends the urine sample to the laboratory for sensitivity. The RN reports the laboratory result to the GP who then prescribes the appropriate antibiotic as per sensitivity. The RN creates a short term care plan. The RN completes an Incident Report and gives this Incident
Report to the CL who will then enters the data to the IntraNet for benchmarking and pre-populates an Infection Control demographics. Evidences that infections are reported during staff meetings are sighted.Sanitary hand gels are available throughout the facility and there are adequate hand washing facilities for staff, visitors and residents. Staff interviewed are able to explain when not to come to work.ARC requirement is met.
Criterion 3.1.1 The responsibility for infection control is clearly defined and there are clear lines of accountability for infection control matters in the organisation leading to the governing body and/or senior management.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 3.1.3 The organisation has a clearly defined and documented infection control programme that is reviewed at least annually.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 3.1.9 Service providers and/or consumers and visitors suffering from, or exposed to and susceptible to, infectious diseases should be prevented from exposing others while infectious.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 3.2 Implementing the infection control programmeThere are adequate human, physical, and information resources to implement the infection control programme and meet the needs of the organisation.
ARC D5.4e ARHSS D5.4e
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThere are adequate human, physical, and information resources to implement the infection control programme and meet the needs of the organisation. Hand washing signs are sighted around the facility to remind staff the importance of having proper hand washing. The organisation maintains regular in-service training on infection control including standard precautions, use of personal protective equipment, laundry care and hand washing/hand hygiene.The ARRC requirement is met.
Criterion 3.2.1 The infection control team/personnel and/or committee shall comprise, or have access to, persons with the range of skills, expertise, and resources necessary to achieve the requirements of this Standard.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 3.3 Policies and proceduresDocumented policies and procedures for the prevention and control of infection reflect current accepted good practice and relevant legislative requirements and are readily available and are implemented in the organisation. These policies and procedures are practical, safe, and appropriate/suitable for the type of service provided.
ARC D5.4e, D19.2a ARHSS D5.4e, D19.2a
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FADocumented policies and procedures for the prevention and control of infection reflect current accepted good practice and relevant legislative requirements and are readily available and are implemented in the organisation. These policies and procedures are practical, safe, and appropriate/suitable for the type of service provided. Policies and procedures sighted. The service evidences implementation of the policies and procedures. Five staff interviewed are able to identify where the policies and located and that they are informed when updates are made.ARRC requirements are met.
Criterion 3.3.1 There are written policies and procedures for the prevention and control of infection which comply with relevant legislation and current accepted good practice.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 3.4 EducationThe organisation provides relevant education on infection control to all service providers, support staff, and consumers.
ARC D5.4e ARHSS D5.4e
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FAThe organisation provides relevant education on infection control to all service providers, support staff, and residents. The infection control education is provided by either the CL or the facility manager who are both suitably qualified and maintains a knowledge of current practice. All staff complete an annual quiz as part of the annual update. All staff have hand washing competencies as sighted. Infection control training record is sighted. Staff are able to discuss the importance of proper hand washing and how to break the chain of infection. Residents interviewed are also aware of the importance of hand washing and mentioned when hand washing is required.ARRC requirements are met.
Criterion 3.4.1 Infection control education is provided by a suitably qualified person who maintains their knowledge of current practice.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 3.4.5 Consumer education occurs in a manner that recognises and meets the communication method, style, and preference of the consumer. Where applicable a record of this education should be kept.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
STANDARD 3.5 SurveillanceSurveillance for infection is carried out in accordance with agreed objectives, priorities, and methods that have been specified in the infection control programme.
Evaluation methods used: D SI STI MI CI MaI V CQ SQ STQ Ma L
How is achievement of this standard met or not met? Attainment: FASurveillance for resident infections is carried out in accordance with agreed objectives, priorities, and methods that have been specified in the infection control programme. The infection control committee consisting of the CL, one caregiver, one kitchen employee, one cleaning staff member and one laundry employee. This is appropriate for the service setting. Infection control processes are in place and are documented. A monthly infection register is maintained and antibiotic use is monitored. The organisation has an internal benchmarking system through the IntraNet. Infections are investigated. The surveillance result is reported to the staff during the staff meeting. Minutes of the staff meetings are sighted.All staff interviewed confirm they are kept updated on infection data and prevention strategies.
Criterion 3.5.1 The organisation, through its infection control committee/infection control expert, determines the type of surveillance required and the frequency with which it is undertaken. This shall be appropriate to the size and complexity of the organisation.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe:
Criterion 3.5.7 Results of surveillance, conclusions, and specific recommendations to assist in achieving infection reduction and prevention outcomes are acted upon, evaluated, and reported to relevant personnel and management in a timely manner.
Audit Evidence Attainment: FA Risk level for PA/UA:
Finding Statement
Corrective Action Required:
Timeframe: