Embed Size (px)
Citation preview
CEREBROVASCULAR DISEASE ANDLATE LIFE DEPRESSION: AN AGEOLD ASSOCIATION REVISITED
RAHUL RAO*
Guy's Hospital, St Thomas' Street, London SE1 9RT, UK
ABSTRACT
Objectives. To examine the relationship between depression and cerebrovascular disease in three distinct settings:depression in established cerebrovascular disease, cerebrovascular disease in established depression and depression invascular dementia.
Methods. Medline, EMBASE, PsychLit and PsychInfo databases were scanned to locate relevant articles. Datawere also extracted from other articles, cited by those articles generated from the above databases.
Results. Using operational criteria, the prevalence of depression is higher than controls only within the ®rst yearafter stroke, but most studies have not employed control groups. The prevalence of depression in vascular dementiacompared with Alzheimer's disease is higher in the majority of studies, but matching for sociodemographic factorsand severity of cognitive impairment has been inconsistent. An association between frontal/subcortical cerebro-vascular lesions and depression in later life has been observed, but there may be methodological ¯aws underlying thisobservation in some computerized tomography studies.
Conclusion. There is some evidence that cerebrovascular disease has an aetiopathological role in late lifedepression. The increased likelihood of damage to frontal/subcortical brain circuitry following stroke, transientischaemia and hypertension may explain the high prevalence of depression in older people with vascular risk factors.
More valid de®nitions of lesion location and the use of appropriately matched control groups would seek to clarifythis issue. The extrapolation to care settings from the high prevalence of depression accompanying cerebrovasculardisease and the prolongation of disability in depressed people with stroke, suggests closer liaison between old agepsychiatrists, neurologists and physicians caring for the elderly. Copyright # 2000 John Wiley & Sons, Ltd.
KEY WORDSÐageing; depression; stroke; prevalence; frontal lobe; brain imaging; vascular dementia
During the mid 19th century, Durand-Fardel(1843) reported irritability and depression to becommon acute sequelae of strokes. There has sincebeen a steadily increasing volume of researchexamining the relationship between depressionand cerebrovascular disease. These studies fallinto three distinct categories: depression in estab-lished cerebrovascular disease, cerebrovasculardisease in established depressive disorder anddepression in vascular dementia. This reviewcritically evaluates each of these associations inturn, intentionally excluding other disorders suchas emotionalism and apathy which, althoughclinically important consequences of stroke,
would require more extensive discussion in theirown right. Both apathy (Marin et al., 1995; Levyet al., 1998) and emotionalism (Andersen, 1997;Calvert et al., 1998) have been the subject of recentreviews.
The following review was based on a search ofMedline, EMBASE, PsychInfo and PsychLitdatabases from 1980 to December 1998. Morerecent articles were sought from monthly issues ofIndex Medicus. The following words were used toextract articles of interest: depression; cerebro-vascular disorders; stroke; vascular dementia;brain imaging; frontal lobe; rating scale. Articleswere then selected if they, in part of whole,examined the relationship between cerebrovasculardisease and depression. Further articles of interestwere then selected on the basis of the aboveselection criterion.
Copyright # 2000 John Wiley & Sons, Ltd. Received 2 August 1999Accepted 29 August 1999
INTERNATIONAL JOURNAL OF GERIATRIC PSYCHIATRY
Int. J. Geriat. Psychiatry 15, 419±433 (2000)
*Correspondence to: Dr R. Rao, Senior Lecturer in Old AgePsychiatry, Job Ward, Thomas Guy House, Guy's Hospital,St Thomas' Street, London SE1 9RT, UK. Tel: �44-171-232-0148. Fax: �44-171-394-1097. e-mail: [email protected]

DEPRESSION ACCOMPANYINGCEREBROVASCULAR DISEASE
In the context of mood disorders associatedwith cerebrovascular disease, depression followingstroke (commonly referred to as `post-strokedepression') has commanded the largest volumeof research over the past three decades. Depressionis more likely to occur after a stroke than in othermedical disorders with similar levels of disability(Folstein et al., 1977) and compared with age- andsex-matched community residents (House et al.,1991; Dam et al., 1989; Andersen et al., 1994).
A number of studies have found high sensitivitiesand speci®cities when validating established depres-sion rating scales against diagnostic instruments fordepression in stroke populations. These scalesinclude the Hamilton Rating Scale for Depression(HRSD) (Ng et al., 1995), General Health Ques-tionnaire (Robinson and Price, 1982), GeriatricDepression Scale (Johnson et al., 1995), Zung Self-rating Scale for Depression (Agrell and Dehlin,1989) and the Centre for Epidemiological StudiesÐDepression Scale (Shinar et al., 1986). The HRSDhas been used most frequently in screening for post-stroke depression. However, rating scales fordepression used in stroke may be sensitive, butoften lack speci®city when compared with diag-nostic instruments (Schramke et al., 1998).
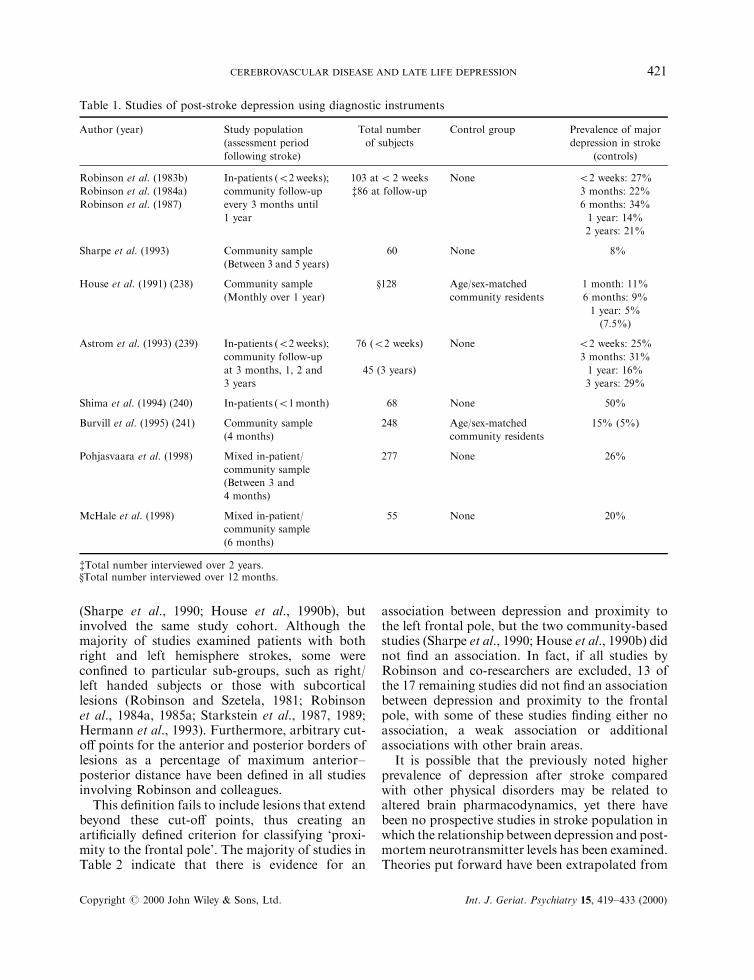
The prevalence of post-stroke depression indi�erent populations has been subject of a numberof studies, but few have used standardized diag-nostic instruments at speci®c time periods afterstroke. Table 1 outlines the characteristics ofstudies that have used such instruments. A studyexcluded from this table assessed 103 stroke clinicattenders over an 18 month period using DSM IIIcriteria for major depression, but its sample washeterogeneous, with a wide variation in the timeinterval since the last stroke (more than 10 years in18% of the group).
However, 45% of those people who had su�eredtheir last stroke between 6 months and 2 yearspreviously were given a diagnosis of DSM IIImajor depression (Robinson and Price, 1982). Onlytwo of the studies shown in Table 1 used strokeregisters (House et al., 1991; Burvill et al., 1995),and only one of these studies patients followingtheir ®rst stroke (House et al., 1991). Most studiesdo not, however, include a control group, which isproblematic when interpreting the prevalence ofpost-stroke depression. However, this cannotdetract from the observation that the prevalence
of post-stroke depression during the ®rst monthranges from 11 to 50%, declining only after 2 yearsfollowing stroke. It is striking that communitysamples show comparatively lower prevalence ratesfor depression.
It is possible that patients with less severe strokes(and probably less neurological and functionalde®cit) not requiring hospital admission have lesssevere depressive symptomatology. The applicationof these studies to clinical practice suggests thatpatients should be screened for major depressionfor at least 2 years after their stroke. Clearly, thereis large variation between studies in the prevalenceof post-stroke depression, depending on methodo-logical di�erences such as restriction to certainstroke sub-types, diagnostic criteria, and demo-graphy of the study population (e.g. in-patientsversus community residents). However, in spite ofthe high prevalence of post-stroke depression in themajority of studies, a diagnosis of depressionfollowing stroke may be missed during routineclinical practice.
Risk factors for post-stroke depression
Several factors in¯uence both the course andseverity of post-stroke depression, including age(Robinson et al., 1984a; Morris et al., 1992), timesince stroke (Robinson et al., 1987; House et al.,1991), severity of intellectual impairment (Houseet al., 1990a; Andersen et al., 1995, 1996), socialsupport (Shima et al., 1994; Morris et al., 1991;Astrom et al., 1992), and past history of depression(Andersen et al., 1995; Schwartz et al., 1993). Thetwo most widely studied risk factors in relation topost-stroke depression have been physical disabilityand location of stroke lesion. The relationshipbetween physical disability and depression is com-plex, as there appears to be a reciprocal relationshipbetween the two factors. There is comparativelygreater evidence for depression being a risk factorfor prolonged neurological disability rather thanvice versa (Ebrahim et al., 1987; Colantonio et al.,1992; Diamond et al., 1995). Other studies have notfound a signi®cant relationship between depressionand physical disability (Robinson and Price, 1982;Lammi et al., 1989).
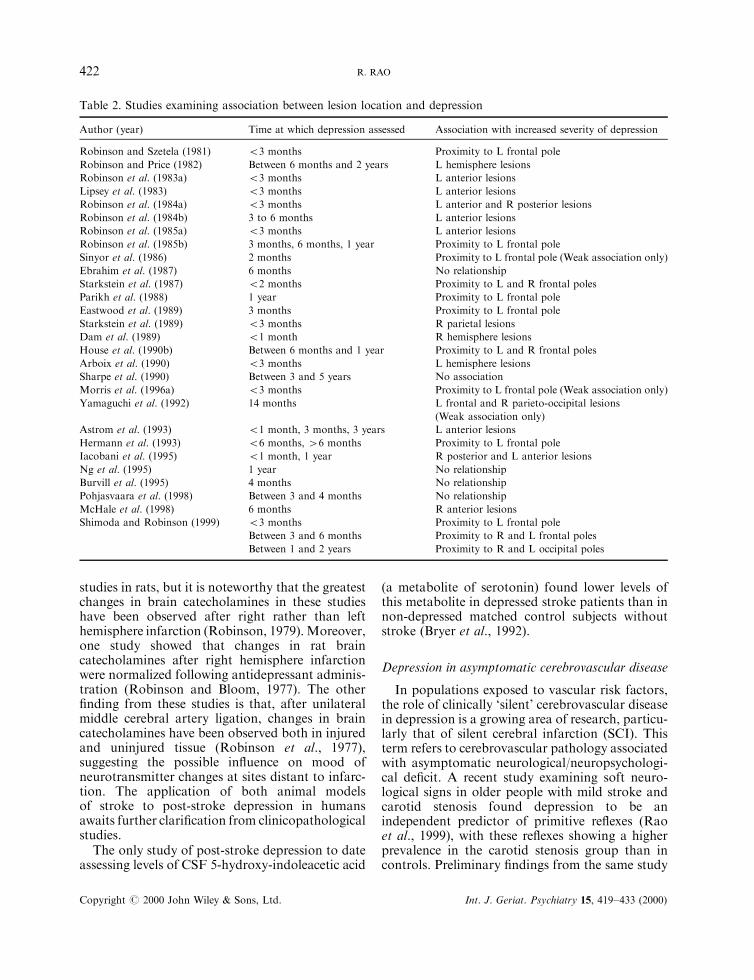
Interest in the relationship between location ofstroke lesion and depression began during the1980s, largely owing to a large number of studies byRobinson and colleagues. These and other relevantstudies are outlined in Table 2. Only two studiesinvolved community residents on a stroke register
Copyright # 2000 John Wiley & Sons, Ltd. Int. J. Geriat. Psychiatry 15, 419±433 (2000)
420 R. RAO
(Sharpe et al., 1990; House et al., 1990b), butinvolved the same study cohort. Although themajority of studies examined patients with bothright and left hemisphere strokes, some werecon®ned to particular sub-groups, such as right/left handed subjects or those with subcorticallesions (Robinson and Szetela, 1981; Robinsonet al., 1984a, 1985a; Starkstein et al., 1987, 1989;Hermann et al., 1993). Furthermore, arbitrary cut-o� points for the anterior and posterior borders oflesions as a percentage of maximum anterior±posterior distance have been de®ned in all studiesinvolving Robinson and colleagues.
This de®nition fails to include lesions that extendbeyond these cut-o� points, thus creating anarti®cially de®ned criterion for classifying `proxi-mity to the frontal pole'. The majority of studies inTable 2 indicate that there is evidence for an
association between depression and proximity tothe left frontal pole, but the two community-basedstudies (Sharpe et al., 1990; House et al., 1990b) didnot ®nd an association. In fact, if all studies byRobinson and co-researchers are excluded, 13 ofthe 17 remaining studies did not ®nd an associationbetween depression and proximity to the frontalpole, with some of these studies ®nding either noassociation, a weak association or additionalassociations with other brain areas.
It is possible that the previously noted higherprevalence of depression after stroke comparedwith other physical disorders may be related toaltered brain pharmacodynamics, yet there havebeen no prospective studies in stroke population inwhich the relationship between depression and post-mortem neurotransmitter levels has been examined.Theories put forward have been extrapolated from
Table 1. Studies of post-stroke depression using diagnostic instruments
Author (year) Study population
(assessment period
following stroke)
Total number
of subjects
Control group Prevalence of major
depression in stroke
(controls)
Robinson et al. (1983b)
Robinson et al. (1984a)
Robinson et al. (1987)
In-patients (52 weeks);
community follow-up
every 3 months until
1 year
103 at5 2 weeks
{86 at follow-up
None 52 weeks: 27%
3 months: 22%
6 months: 34%
1 year: 14%
2 years: 21%
Sharpe et al. (1993) Community sample
(Between 3 and 5 years)
60 None 8%
House et al. (1991) (238) Community sample
(Monthly over 1 year)
}128 Age/sex-matched
community residents
1 month: 11%
6 months: 9%
1 year: 5%
(7.5%)
Astrom et al. (1993) (239) In-patients (52 weeks);
community follow-up
at 3 months, 1, 2 and
3 years
76 (52 weeks)
45 (3 years)
None 52 weeks: 25%
3 months: 31%
1 year: 16%
3 years: 29%
Shima et al. (1994) (240) In-patients (51month) 68 None 50%
Burvill et al. (1995) (241) Community sample
(4 months)
248 Age/sex-matched
community residents
15% (5%)
Pohjasvaara et al. (1998) Mixed in-patient/
community sample
(Between 3 and
4 months)
277 None 26%
McHale et al. (1998) Mixed in-patient/
community sample
(6 months)
55 None 20%
{Total number interviewed over 2 years.}Total number interviewed over 12 months.
Copyright # 2000 John Wiley & Sons, Ltd. Int. J. Geriat. Psychiatry 15, 419±433 (2000)
CEREBROVASCULAR DISEASE AND LATE LIFE DEPRESSION 421
studies in rats, but it is noteworthy that the greatestchanges in brain catecholamines in these studieshave been observed after right rather than lefthemisphere infarction (Robinson, 1979).Moreover,one study showed that changes in rat braincatecholamines after right hemisphere infarctionwere normalized following antidepressant adminis-tration (Robinson and Bloom, 1977). The other®nding from these studies is that, after unilateralmiddle cerebral artery ligation, changes in braincatecholamines have been observed both in injuredand uninjured tissue (Robinson et al., 1977),suggesting the possible in¯uence on mood ofneurotransmitter changes at sites distant to infarc-tion. The application of both animal modelsof stroke to post-stroke depression in humansawaits further clari®cation from clinicopathologicalstudies.
The only study of post-stroke depression to dateassessing levels of CSF 5-hydroxy-indoleacetic acid
(a metabolite of serotonin) found lower levels ofthis metabolite in depressed stroke patients than innon-depressed matched control subjects withoutstroke (Bryer et al., 1992).
Depression in asymptomatic cerebrovascular disease
In populations exposed to vascular risk factors,the role of clinically `silent' cerebrovascular diseasein depression is a growing area of research, particu-larly that of silent cerebral infarction (SCI). Thisterm refers to cerebrovascular pathology associatedwith asymptomatic neurological/neuropsychologi-cal de®cit. A recent study examining soft neuro-logical signs in older people with mild stroke andcarotid stenosis found depression to be anindependent predictor of primitive re¯exes (Raoet al., 1999), with these re¯exes showing a higherprevalence in the carotid stenosis group than incontrols. Preliminary ®ndings from the same study
Table 2. Studies examining association between lesion location and depression
Author (year) Time at which depression assessed Association with increased severity of depression
Robinson and Szetela (1981) 53 months Proximity to L frontal pole
Robinson and Price (1982) Between 6 months and 2 years L hemisphere lesions
Robinson et al. (1983a) 53 months L anterior lesions
Lipsey et al. (1983) 53 months L anterior lesions
Robinson et al. (1984a) 53 months L anterior and R posterior lesions
Robinson et al. (1984b) 3 to 6 months L anterior lesions
Robinson et al. (1985a) 53 months L anterior lesions
Robinson et al. (1985b) 3 months, 6 months, 1 year Proximity to L frontal pole
Sinyor et al. (1986) 2 months Proximity to L frontal pole (Weak association only)
Ebrahim et al. (1987) 6 months No relationship
Starkstein et al. (1987) 52 months Proximity to L and R frontal poles
Parikh et al. (1988) 1 year Proximity to L frontal pole
Eastwood et al. (1989) 3 months Proximity to L frontal pole
Starkstein et al. (1989) 53 months R parietal lesions
Dam et al. (1989) 51 month R hemisphere lesions
House et al. (1990b) Between 6 months and 1 year Proximity to L and R frontal poles
Arboix et al. (1990) 53 months L hemisphere lesions
Sharpe et al. (1990) Between 3 and 5 years No association
Morris et al. (1996a) 53 months Proximity to L frontal pole (Weak association only)
Yamaguchi et al. (1992) 14 months L frontal and R parieto-occipital lesions
(Weak association only)
Astrom et al. (1993) 51 month, 3 months, 3 years L anterior lesions
Hermann et al. (1993) 56 months, 46 months Proximity to L frontal pole
Iacobani et al. (1995) 51 month, 1 year R posterior and L anterior lesions
Ng et al. (1995) 1 year No relationship
Burvill et al. (1995) 4 months No relationship
Pohjasvaara et al. (1998) Between 3 and 4 months No relationship
McHale et al. (1998) 6 months R anterior lesions
Shimoda and Robinson (1999) 53 months
Between 3 and 6 months
Between 1 and 2 years
Proximity to L frontal pole
Proximity to R and L frontal poles
Proximity to R and L occipital poles
Copyright # 2000 John Wiley & Sons, Ltd. Int. J. Geriat. Psychiatry 15, 419±433 (2000)
422 R. RAO
also suggest that depression is more likely to bepresent in people with carotid stenosis than inhealthy controls (Rao, 1998a). The observationsthat stress (Everson et al., 1997a) is a correlate andhopelessness (Everson et al., 1997b) an independentpredictor of carotid atherosclerosis, providesimportant pointers to a possible causal ratherthan an e�ectual relationship between mood andcerebrovascular disease.
Chronic changes in cerebral vasculature second-ary to hypertension may also result in frontal/subcortical brain dysfunction (Rao and Howard,1998). It is possible that this may be responsible forthe association between raised blood pressure anddepression observed in other studies (Rabkin et al.,1983; Fujikawa et al., 1994a; Krishnan et al.,1994a).
Although diabetes mellitus has shown a higherprevalence of depression with longer exposure tothis vascular risk factor (Holroyd and Duryee,1997), it is equally likely to be present in depressionwith and without SCI (Krishnan et al., 1994a).Little is known about the role of other vascular riskfactors such as atrial ®brillation in the pathogenesisof depression accompanying SCI.
CEREBROVASCULAR DISEASEACCOMPANYING DEPRESSION
The contribution of cerebrovascular disease hasalso been explored in studies of patients with anestablished diagnosis of depressive disorder, whereSCI may be present. In a study of patients meetingDSM III-R criteria for depression, SCI wasobserved in over 65% of participants (Fujikawaet al., 1993). In one of the largest magneticresonance imaging (MRI) studies, 244 patients(average age 34), with a wide variety of psychiatricdisorders were compared with 154 control subjects(Brown et al., 1992). The only group in whom asigni®cant di�erence was observed in the preva-lence of white matter hyperintensities (WMHI) inrelation to the control group was patients withmajor depression. However, age was noted to bethe largest contributing factor in that this di�erencewas not observed in a sub-group younger than 45.
Interest in the contribution of cerebrovasculardisease to late life depression developed as struc-tural brain imaging became more widely used, withthe relatively higher prevalence of cerebrovasculardisease noted in depression compared with non-depressed controls (Jacoby and Levy, 1980). As
most of these studies involved the use of MRI,white matter hyperintensities (WMHI) becameincreasingly relevant as correlates of depression(Zubenko et al., 1990; Sultzer et al., 1995).
One aspect of this became the subject of anumber of studies during the 1980s: namely, thecontribution of cerebrovascular disease to resistantdepression in patients referred for electroconvulsivetherapy (ECT) (Co�ey et al., 1987). In a study ofbrain imaging carried out in patients referred forECT, Co�ey et al. (1988) found that subcorticalwhite matter lesions seen onMRI were signi®cantlyassociated with lacunar infarcts of the basal gangliaand thalamus. In two other MRI studies, the samegroup found that over 50% of depressed patientsreferred for ECT had white matter lesions rated asmoderate or severe (Co�ey et al., 1989) and thatsubcortical white matter hyperintensities weremore common compared with an age/sex-matchedcontrol group (Co�ey et al., 1990). Subcorticalwhite matter disease in depression continues tocommand great interest, particularly in relation topathology in frontal/subcortical brain circuitry. Astudy comparing 67 elderly subjects with majordepression and 44 matched controls found thatdepressed patients were two and a half times aslikely to show subcortical white matter disease thancontrols (Zubenko et al., 1990).
Treatment resistant depression has also been thefocus of more recent studies. Following anobservation that treatment resistance may beassociated with subcortical cerebrovascular disease(Simpson et al., 1997a), Simpson et al. (1997b)studied 58 treatment resistant older people withDSM III-R depression. Lesions of the basalganglia, diabetes, lower mean arterial pressure,and hyperintensity of the pontine reticular for-mation correctly predicted 96% of patients withpoor outcome. A study of 39 elderly people withsevere depression by Hickie et al. (1995) also foundsubcortical hyperintensities on MRI to be associ-ated with a poorer response to treatment.
However, both these studies de®ned treatmentresistance according to global clinical impressionrather than clearly de®ned treatment regimens,prompting a further study of treatment resistancein 75 elderly people with DSM III-R majordepression. In this study, Simpson et al. (1998)found that neuropsychological impairment sugges-tive of frontal/subcortical dysfunction was morecommon in the treatment resistant group than incontrols. Resistance to antidepressant mono-therapy over 12 weeks was associated with a higher
Copyright # 2000 John Wiley & Sons, Ltd. Int. J. Geriat. Psychiatry 15, 419±433 (2000)
CEREBROVASCULAR DISEASE AND LATE LIFE DEPRESSION 423
prevalence of deep white matter and basal ganglialesions as well as frontal, extrapyramidal andpyramidal neurological signs. Severe deep WMHIare also known to in¯uence long-term survival. In atwo year longitudinal study of 60 older people withDSM III-R depression and no history of stroke, thepresence of severe WMHI predicted persistence ofdepression and relapse, with the median survivaltime in people with severe lesions being less thanhalf of that of those without such lesions (O'Brienet al., 1998).
Other studies have replicated the associationbetween WMHI and late life depression, assessingthese in elderly depressed patients matched with acontrol group. Greenwald et al. (1996) found moresevere subcortical hyperintensities in depressedpatients; Iadaka et al. (1996) found that depressedpatients showed more extensive periventricularhyperintensities in the frontal region/greaterseverity of hyperintensities in the putamen andglobus pallidus. As ischaemic cerebrovascularpathology is known to be closely linked withwhite matter pathology, the claim that depressionin later life is associated with WMHI even aftercontrolling for vascular risk factors (O'Brien et al.,1996a) may be ¯awed in that such lesions may berelated to SCI (Rao, 1996). There is, however, somelimited evidence for an association betweenWMHIand depression even after controlling for vascularrisk factors (O'Brien et al., 1996b).
Another approach to the study of cerebro-vascular disease in depression is the comparisonof cerebrovascular pathology seen on structuralimaging between early- and late-onset depression.A similar ®nding of an increased prevalence ofWMHI (Iadaka et al., 1996) and subcorticalperiventricular hyperintensities (Figiel et al., 1991;Salloway et al., 1996) in late-onset cases hasemerged.
Functional imaging represents a breakthroughin the assessment of cerebrovascular circulationand studies employing this tool have enabled therelationship between mood and regional blood¯ow to be examined. The most widely usedmethod of studying regional cerebral blood ¯ow(rCBF) is by means of single photon emissioncomputerized tomography (SPECT) using radio-labelled HMPAO. There has been some consist-ency in the association between regional blood¯ow abnormalities and depression (Mathew et al.,1980). The vast majority of studies using controlgroups have found that depression is stronglyassociated with decreased rCBF in either the
frontal or prefrontal cortex. This has beenobserved both bilaterally (Schlegel et al., 1989;Austin et al., 1992; Mayberg et al., 1994; Ito et al.,1996) or con®ned to the left hemisphere (Benchet al., 1993; Sackeim et al., 1993). One study foundleft frontal hyperperfusion (Uytdenhoef et al.,1983), but this ®nding has not been consistentlyreplicated.
DEPRESSION IN VASCULAR DEMENTIA
Depression accompanying vascular dementia wasthe subject of a number of studies during the mid1980s to mid 1990s, but has not drawn a great dealof interest since that time. These studies aredescribed in Table 3. The majority of studies todate have found a signi®cantly higher prevalenceof depression in vascular dementia than inAlzheimer's disease.
As seen from the table, the prevalence of majordepression as de®ned by DSM III, DSM III-R orResearch Diagnostic Criteria (RDC) ranges from6% to 45%. However, in only two of these studieswere groups equivalent in age, sex ratio andseverity of cognitive impairment (Sultzer et al.,1992; Cohen et al., 1993). The relationship betweenbrain imaging abnormalities and depression invascular dementia has been examined in a recentstudy by Barber et al. (1999), in which an associa-tion between frontal deep white matter (but notperiventricular) lesions and depression was noted.The same study also found that basal gangliahyperintensities were more frequent in vasculardementia than in Alzheimer's disease or controls. Itis possible that both of these pathologies areimplicated in the pathogenesis of mood disorderin vascular dementia.
The other important factor in¯uencing theinterpretation of these studies is the in¯uence ofcognitive impairment on mood. The term `pseudo-dementia' as applied to depression mimickingchronic organic brain disease came into popularuse in the 1970s (Wells, 1979), and refers to thein¯uence of mood disorder on cognitive state.Conversely, cognitive impairment is known toin¯uence mood state, and the term `depression ofdementia' has been applied to depressed mood (notresponsive to somatic treatment for depression) inthe setting of intellectual decline, whose severity isassociated with the severity of cognitive de®cit.This latter phenomenon has been noted in post-stroke depression (Andersen et al., 1996), but
Copyright # 2000 John Wiley & Sons, Ltd. Int. J. Geriat. Psychiatry 15, 419±433 (2000)
424 R. RAO
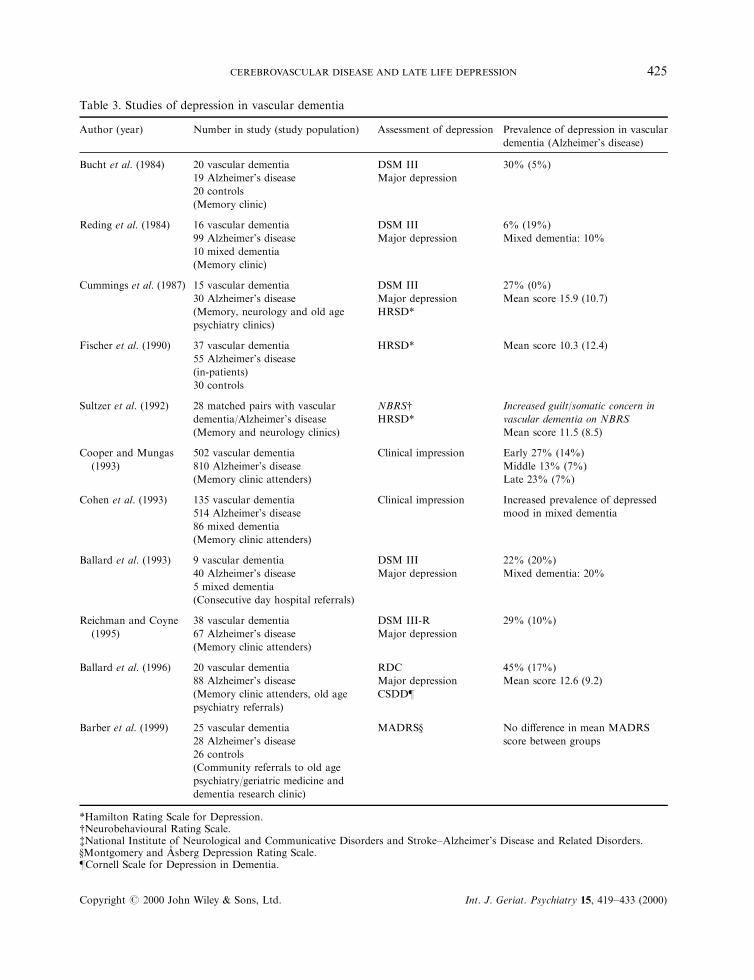
Table 3. Studies of depression in vascular dementia
Author (year) Number in study (study population) Assessment of depression Prevalence of depression in vascular
dementia (Alzheimer's disease)
Bucht et al. (1984) 20 vascular dementia
19 Alzheimer's disease
20 controls
(Memory clinic)
DSM III
Major depression
30% (5%)
Reding et al. (1984) 16 vascular dementia
99 Alzheimer's disease
10 mixed dementia
(Memory clinic)
DSM III
Major depression
6% (19%)
Mixed dementia: 10%
Cummings et al. (1987) 15 vascular dementia
30 Alzheimer's disease
(Memory, neurology and old age
psychiatry clinics)
DSM III
Major depression
HRSD*
27% (0%)
Mean score 15.9 (10.7)
Fischer et al. (1990) 37 vascular dementia
55 Alzheimer's disease
(in-patients)
30 controls
HRSD* Mean score 10.3 (12.4)
Sultzer et al. (1992) 28 matched pairs with vascular
dementia/Alzheimer's disease
(Memory and neurology clinics)
NBRS{HRSD*
Increased guilt/somatic concern in
vascular dementia on NBRS
Mean score 11.5 (8.5)
Cooper and Mungas
(1993)
502 vascular dementia
810 Alzheimer's disease
(Memory clinic attenders)
Clinical impression Early 27% (14%)
Middle 13% (7%)
Late 23% (7%)
Cohen et al. (1993) 135 vascular dementia
514 Alzheimer's disease
86 mixed dementia
(Memory clinic attenders)
Clinical impression Increased prevalence of depressed
mood in mixed dementia
Ballard et al. (1993) 9 vascular dementia
40 Alzheimer's disease
5 mixed dementia
(Consecutive day hospital referrals)
DSM III
Major depression
22% (20%)
Mixed dementia: 20%
Reichman and Coyne
(1995)
38 vascular dementia
67 Alzheimer's disease
(Memory clinic attenders)
DSM III-R
Major depression
29% (10%)
Ballard et al. (1996) 20 vascular dementia
88 Alzheimer's disease
(Memory clinic attenders, old age
psychiatry referrals)
RDC
Major depression
CSDD}
45% (17%)
Mean score 12.6 (9.2)
Barber et al. (1999) 25 vascular dementia
28 Alzheimer's disease
26 controls
(Community referrals to old age
psychiatry/geriatric medicine and
dementia research clinic)
MADRS} No di�erence in mean MADRS
score between groups
*Hamilton Rating Scale for Depression.{Neurobehavioural Rating Scale.{National Institute of Neurological and Communicative Disorders and Stroke±Alzheimer's Disease and Related Disorders.}Montgomery and AÊ sberg Depression Rating Scale.}Cornell Scale for Depression in Dementia.
Copyright # 2000 John Wiley & Sons, Ltd. Int. J. Geriat. Psychiatry 15, 419±433 (2000)
CEREBROVASCULAR DISEASE AND LATE LIFE DEPRESSION 425

studies examining the relationship between intel-lectual function and mood listed in Table 3 foundno signi®cant association between score on themini mental state examination and major depres-sion or depression rating scale scores.
Although one study found depression afterstroke to be associated with lower mini mentalstate examination scores for up to one year(Downhill and Robinson, 1994), a communitystudy of stroke patients found a negative associa-tion between severity of cognitive impairment anddepressive symptoms on the Beck Depression Scaleand Present State Examination, revealing noassociation with major depression (House et al.,1990a).
In the context of cerebrovascular disease, therelationship between cognitive impairment anddepression is complex for several reasons. It islikely that (as discussed above) cognitive impair-ment and depression co-exist in the same personwith cerebrovascular disease. However, there isalso a longitudinal relationship known to existbetween the two factors. This is exempli®ed by theconcept of `pre-stroke depression', in which silentcerebrovascular pathology manifests as depressionprior to the onset of cognitive dysfunction inboth lacunar and cortical stroke (Colantonio et al.,1993).
FRONTAL/SUBCORTICAL DYSFUNCTION:A FINAL COMMON PATHWAY INDEPRESSION ACCOMPANYINGCEREBROVASCULAR DISEASE?
There is some suggestion from the evidence abovethat damage to anterior brain regions, theirprojections to subcortical structures and sub-cortical structures themselves, is associated with ahigher prevalence and severity of depression thanpathology in other brain areas. The suggestion ofcerebrovascular disease as a putative underlyingmechanism, however, may ignore the contributionof non-vascular processes.
This is borne out by studies in younger peoplewith depressive disorder. Baxter et al. (1989) foundthat younger depressed patients showed bilateralprefrontal glucose hypometabolism and thatdepression severity correlated with a decrease inmetabolic rate. Likewise, depression in schizo-phrenia is known to share a similar picture ofprefrontal hypometabolism (Cohen et al., 1989).Frontal lobe dysfunction is also a feature of
depression accompanying other neurological dis-orders. Depression has been associated with pre-frontal hypometabolism in both Parkinson'sdisease (Ring et al., 1994) and Huntington's chorea(Mayberg, 1993). Additionally, frontal hypo-perfusion has been noted in depression associatedwith epilepsy (Schmitz et al., 1997) and Alzheimer'sdisease (Hirono et al., 1998).
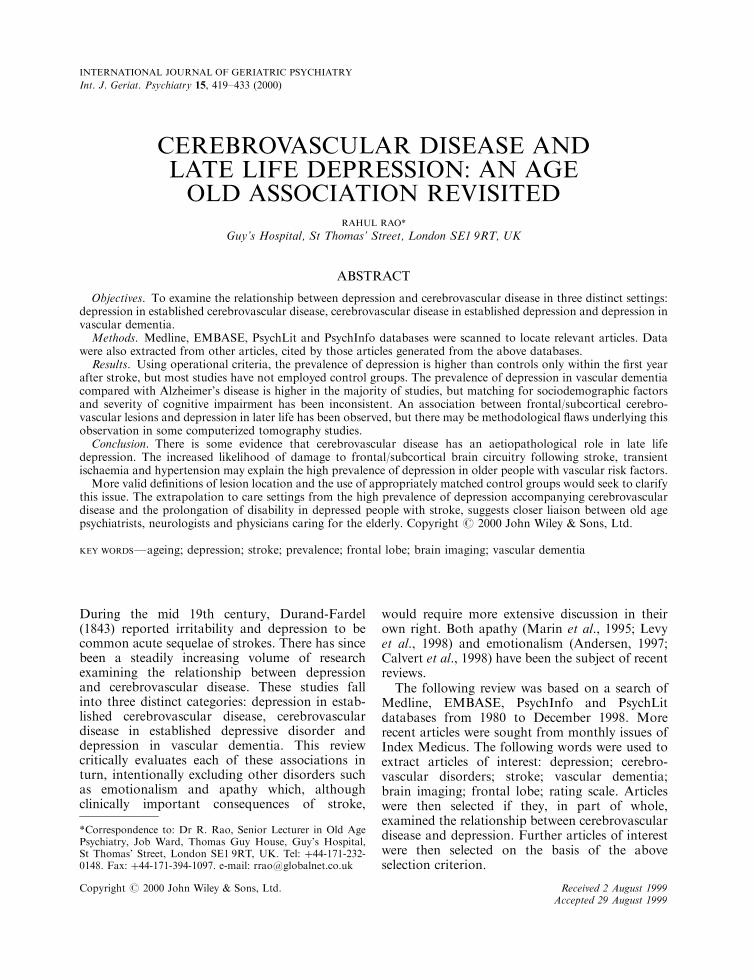
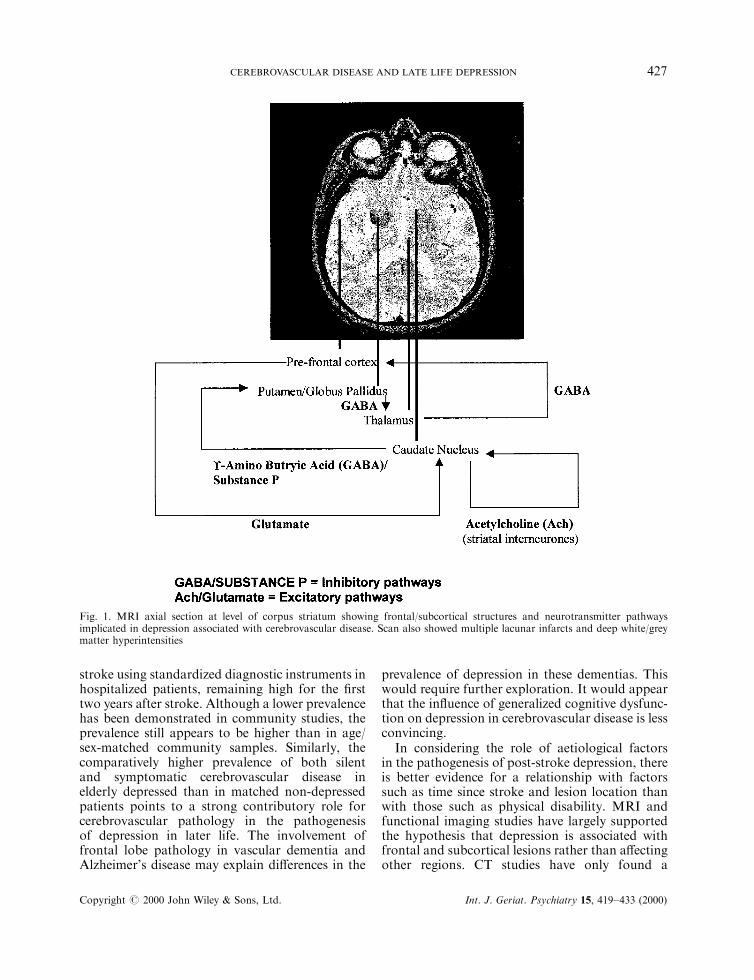
The neuroanatomical circuit most commonlyimplicated in depression is a loop comprising thedorsolateral prefrontal cortex, caudate nucleus,globus pallidus and thalamus (Fig. 1). Damage toone or more of these pathways may result indisruption to a number of neurochemical path-ways. Depression is thought to result from overallexcessive inhibitory input to the prefrontal cortex(Alexopoulos et al., 1997a). This is a rathersimplistic model, as other frontal/subcortical path-ways arising from orbitomedial and anteriorcingulate cortices have also been implicated indepression associated with cerebrovascular disease(Alexopoulos et al., 1997b). These, together withthe prefrontal dorsolateral cortex, have additionalconnections with the limbic system, subthalamicnuclei and substantia nigra. In addition to theneurochemical pathways already de®ned, this mayalso in¯uence noradrenergic, serotonergic anddopaminergic function (Cummings, 1993).
The key issue is whether, given that frontal/subcortical dysfunction has a consistent associationwith depression and that such dysfunction alsoexists in younger people/other neurological dis-orders without vascular risk factors, depressionassociated with cerebrovascular disease is a noso-logically distinct entity. Hickie and Scott (1998)have suggested that so-called `vascular depression'is characterized by observable psychomotorchange, subcortical neuropsychological signs, late-onset, reduced familial rates of depression, treat-ment-resistance, vascular risk factors and subcor-tical MRI changes. There is also evidence for theinvolvement of genetically determined vascular riskfactors such as Apolipoprotein E-4 (Krishnan et al.,1994b), but two more recent studies have notreplicated this ®nding when examining the associ-ation between ApoE-4 and late-onset depression(Forsell et al., 1997; Schmand et al., 1998).
CONCLUSIONS
Studies of post-stroke depression have shown aprevalence of up to 50% within the ®rst month of
Copyright # 2000 John Wiley & Sons, Ltd. Int. J. Geriat. Psychiatry 15, 419±433 (2000)
426 R. RAO
stroke using standardized diagnostic instruments inhospitalized patients, remaining high for the ®rsttwo years after stroke. Although a lower prevalencehas been demonstrated in community studies, theprevalence still appears to be higher than in age/sex-matched community samples. Similarly, thecomparatively higher prevalence of both silentand symptomatic cerebrovascular disease inelderly depressed than in matched non-depressedpatients points to a strong contributory role forcerebrovascular pathology in the pathogenesisof depression in later life. The involvement offrontal lobe pathology in vascular dementia andAlzheimer's disease may explain di�erences in the
prevalence of depression in these dementias. Thiswould require further exploration. It would appearthat the in¯uence of generalized cognitive dysfunc-tion on depression in cerebrovascular disease is lessconvincing.
In considering the role of aetiological factorsin the pathogenesis of post-stroke depression, thereis better evidence for a relationship with factorssuch as time since stroke and lesion location thanwith those such as physical disability. MRI andfunctional imaging studies have largely supportedthe hypothesis that depression is associated withfrontal and subcortical lesions rather than a�ectingother regions. CT studies have only found a
Fig. 1. MRI axial section at level of corpus striatum showing frontal/subcortical structures and neurotransmitter pathwaysimplicated in depression associated with cerebrovascular disease. Scan also showed multiple lacunar infarcts and deep white/greymatter hyperintensities
Copyright # 2000 John Wiley & Sons, Ltd. Int. J. Geriat. Psychiatry 15, 419±433 (2000)
CEREBROVASCULAR DISEASE AND LATE LIFE DEPRESSION 427
consistent association with depression less thanthree months after stroke, mostly in hospitalizedpatients. It is likely that some of the di�erencesbetween studies exploring the relationship betweenproximity to the frontal pole and severity ofdepression are attributable to the fact that di�erentstudies represent the same cohort. This is clearlyshown by studies that have (Robinson and col-leagues) and have not (House, Sharpe and col-leagues) found a strong association. There are twopossible explanations for these ®ndings. Firstly, onegroup involved hospital in-patients and the otherassessed people on a community stroke register.Secondly, di�erent methods were employed inde®ning the location of lesions.
It is clear that a standardized quanti®cation ofparameters such as `distance from the frontal pole'is urgently needed before a more de®nitive state-ment can be made from structural brain imaging.
Taken as a whole, the available evidence suggeststhat depression accompanying cerebrovasculardisease is more likely to be associated withfrontal/subcortical dysfunction than with damageto other regional brain areas. Thus, clinical ®ndingsof psychomotor slowing, frontal-type cognitivede®cit, brain imaging evidence of subcorticalinfarction/white matter lesions and treatmentresistancemay not be surprising. The comparativelyhigh prevalence of depression associated withcerebrovascular disease may be explained by thefact that lacunar infarction accounts for up to 40%of anterior circulation ischaemic stroke (Lodderet al., 1994).
These are selectively subcortical in their distri-bution, sparing the cortex and subcortical arcuate`U' ®bres supplying the deeper gyri, and frequentlyinvolve the lenticulostriate end-arteries from thecarotid circulation (Ghika et al., 1990). Hyperten-sion is known to be associated with a similaroutcome in the absence of demonstrable infarction,by ischaemic demyelination of subcortical projec-tions from the frontal cortex (Cummings, 1994).Both processes may be clinically silent, as shown bya recent study that found a similar prevalence ofdepression in patients with carotid stenosis andthose with stroke (Rao, 1998b).
There is still considerable scope for examiningrisk factors, clinical and brain imaging features,treatment and outcome of depression associatedwith cerebrovascular disease in unbiased samples(such as the use of a community stroke register).Studies would also need to distinguish ®rst-everfrom recurrent stroke, as well as examining
di�erences between stroke sub-types. To be morevalid, imaging and mood assessment should ideallytake place within close temporal proximity.
The development of combined imaging tech-niques such as di�usion- and perfusion-weightedMRI (Philips, 1999) would allow both anatomicaland physiological correlates of depression to beassessed. Clinicopathological studies such as theuse of postmortem radio-ligand binding would giveclues regarding brain pharmacodynamics afterstroke, particularly in the case of the treatment ofpost-stroke depression. Lastly, the role of otherpathological mechanisms such as hypertension andtransient ischaemia requires exploration.
Depression accompanying stroke represents asizeable public health problem, particularly giventhat the presence of depression is also associatedwith higher mortality (Morris et al., 1993a, 1993b),even after controlling for sociodemographic andother vascular risk factors such as hypertension(Everson et al., 1998). Improved detection ofdepression, and referral from the settings ofprimary care, health care of the elderly andneurology is critical. Psychiatrists should have acentral role in this process, so that appropriatepharmacological and psychological treatment canbe implemented for a neurological disorder thataccounts for 3±4% of the National Health Servicebudget and is still conceived by physicians as an`understandable' (and therefore undertreated)cause of depression (Feibel and Springer, 1982).
ACKNOWLEDGEMENTS
I would like to thank Dr Robert Howard for hisadvice on earlier drafts of the manuscript andProfessor Alistair Macdonald for his supportduring its preparation.
REFERENCES
Agrell B, Dehlin O. 1989. Comparison of six depressionrating scales in geriatric stroke patients. Stroke 20:1190±1194.
Alexopoulos GS, Meyers BS, Young RC, Campbell S,Silbersweig D, Charlson M. 1997a. `Vascular depres-sion' hypothesis. Arch. Gen. Psych. 54: 915±922.
Alexopoulos GS, Meyers BS, Young RC, Kakuma T,Silbersweig D, Charlson M. 1997b. Clinically de®nedvascular depression. Am. J. Psychiat. 154: 562±565.
Copyright # 2000 John Wiley & Sons, Ltd. Int. J. Geriat. Psychiatry 15, 419±433 (2000)
428 R. RAO
Andersen G. 1997. Post-stroke depression and patho-logical crying: clinical aspects and new pharmaco-logical approaches. Aphasiology 11: 651±664.
Andersen G, Vestergaard K, Riis J, Lauritzen L. 1994.Incidence of post-stroke depression during the ®rstyear in a large unselected stroke population deter-mined using a valid standardized rating scale. ActaPsychiat. Scand. 90: 190±195.
Andersen G, Vestergaard K, Ingemann-Nielsen M,Lauritzen L. 1995. Risk factors for post-strokedepression. Acta Psychiat. Scand. 92: 193±198.
Andersen G, Vestergaard K, Riis JO, Ingemann-NielsenM. 1996. Dementia of depression or depression ofdementia in stroke? Acta Psychiat. Scand. 94: 272±278.
Arboix A, Marti-Vilaltia JL, Garcia JH. 1990. A�ectivedisorders in subcortical ischemic cerebrovascularpathology. Prospective clinical study of 43 patients.Stroke 21: 842±847.
Astrom M, Asplund K, Astrom T. 1992. Psychosocialfunction and life satisfaction after stroke. Stroke 23:527±531.
Astrom M, Adolfsson R, Asplund K. 1993. Majordepression in stroke patients. A 3-year longitudinalstudy. Stroke 24: 976±982.
Austin MP, Dougall N, Ross M, Murray C, O'CarrollRE, Mo�oot A, Ebmeier KP, Goodwin GM. 1992.Single photon emission tomography with 99mTc-exametazime in major depression and the pattern ofbrain activity underlying the psychotic/neurotic con-tinuum. J. A�ect. Disord. 26: 31±43.
Ballard C, Bannister C, Solis M, Oyebode F, Wilcock G.1996. The prevalence, associations and symptoms ofdepression amongst dementia su�erers. J. A�ect.Disord. 36: 135±144.
Ballard CG, Cassidy G, Bannister C, Mohan RN.1993. Prevalence, symptom pro®le, and aetiology ofdepression in dementia su�erers. J. A�ect. Disord. 29:1±6.
Barber R, Scheltens P, Gholkar A, Ballard C,McKeith I,Ince P, Perry R, O'Brien J. 1999. White matter lesionson magnetic resonance imaging in dementia with Lewybodies, Alzheimer's disease, vascular dementia, andnorming aging. J. Neurol. Neurosurg. Psychiat. 67:66±72.
Baxter LR Jr, Schwartz JM, Phelps ME, Mazziotta JC,Guze BH, Selin CE, Gerner RH, Sumida RM. 1989.Reduction of prefrontal cortex glucose metabolismcommon to three types of depression. Arch. Gen.Psychiat. 46: 243±250.
Bench CJ, Friston KJ, Brown RG, Frackowiak RS,Dolan RJ. 1993. Regional cerebral blood ¯ow indepression measured by positron emission tomogra-phy: the relationship with clinical dimensions. Psychol.Med. 23: 579±590.
Brown FW, Lewine RJ, Hudgins PA, Risch SC. 1992.White matter hyperintensity signals in psychiatric andnonpsychiatric subjects. Am. J. Psychiat. 149:620±625.
Bryer JB, Starkstein SE, Votypka V, Parikh RM, PriceTR, Robinson RG. 1992. Reduction of CSF mono-amine metabolites in poststroke depression: a pre-liminary report. J. Neuropsychiat. Clin. Neurosci. 4:440±442.
Bucht G, Adolfsson R, Winblad B. 1984. Dementia ofthe Alzheimer type and multi-infarct dementia: aclinical description and diagnostic problems. J. Am.Geriatr. Soc. 32: 491±498.
Burvill PW, Johnson GA, Jamrozik KD, Anderson CS,Stewart-Wynne EG, Chakera TM. 1995. Prevalence ofdepression after stroke: the Perth Community StrokeStudy. Br. J. Psychiat. 166: 320±327.
Calvert T, Knapp P, House A. 1998. Psychologicalassociations with emotionalism after stroke. J. Neurol.Neurosurg. Psychiat. 65: 928±929.
Co�ey CE, Hinkle PE, Weiner RD, Nemero� CB,Krishnan KR, Varia I, Sullivan DC. 1987. Electro-convulsive therapy of depression in patients with whitematter hyperintensity. Biol. Psychiat. 22: 629±636.
Co�ey CE, Figiel GS, Djang WT, Saunders WB, WeinerRD. 1989. White matter hyperintensity on magneticresonance imaging: clinical and neuroanatomiccorrelates in the depressed elderly. J. Neuropsychiat.Clin. Neurosci. 1: 135±144.
Co�ey CE, Figiel GS, Djang WT, Weiner RD. 1990.Subcortical hyperintensity on magnetic resonanceimaging: a comparison of normal and depressedelderly subjects. Am. J. Psychiat. 147: 187±189.
Cohen RM, Semple WE, Gross M, Nordahl TE, KingAC, Pickar D, Post RM. 1989. Evidence for commonalterations in cerebral glucose metabolism in majora�ective disorders and schizophrenia. Neuropsycho-pharmacology 2: 241±254.
Cohen D, Eisdorfer C, Gorelick P, Paveza G, LuchinsDJ, Freels S, Ashford JW, Semla T, Levy P,Hirschman R. 1993. Psychopathology associatedwith Alzheimer's disease and related disorders.J. Gerontol. 48: 255±260.
Colantonio A, Kasi SV, Ostfeld AM. 1992. Depressiveand other psychosocial factors as predictors of strokein the elderly. Am. J. Epidemiol. 136: 884±894.
Colantonio A, Kasi SV, Ostfeld AM, Berkman LF. 1993.Psychosocial predictors of stroke outcomes in anelderly population. J. Gerontol. 48: 261±268.
Cooper JK, Mungas D. 1993. Risk factor and beha-vioural di�erences between vascular dementia andAlzheimer's dementias: the pathway to end-stagedisease. J. Geriatr. Psychiat. Neurol. 1: 29±33.
Cummings JL. 1993. Frontal±subcortical circuits andhuman behaviour. Arch. Neurol. 50: 873±880.
Cummings JL. 1994. Vascular subcortical dementias:clinical aspects. Dementia 5: 177±180.
Cummings JL, Miller B, Hill MA, Neshkes R. 1987.Neuropsychiatric aspects of multi-infarct dementiaand dementia of the Alzheimer type. Arch. Neurol. 44:389±393.
Copyright # 2000 John Wiley & Sons, Ltd. Int. J. Geriat. Psychiatry 15, 419±433 (2000)
CEREBROVASCULAR DISEASE AND LATE LIFE DEPRESSION 429

Dam H, Pedersen HE, Ahlgren P. 1989. Depressionamong patients with stroke. Acta Psychiat. Scand. 80:118±124.
Diamond PT, Holroyd S, Macciocchi SN, Felsenthal G.1995. Prevalence of depression and outcome on thegeriatric rehabilitation unit. Am. J. Phys. Med. Rehab.74: 214±217.
Downhill JE Jr, Robinson RG. 1994. Longitudinalassessment of depression and cognitive impairmentfollowing stroke. J. Nerv. Ment. Dis. 182: 425±431.
Durand-Fardel M. 1843. Traite du Ramollisement duCerveau. Balliere: Paris.
Eastwood MR, Rifat SL, Nobbs H, Ruderman J. 1989.Mood disorder following cerebrovascular accident.Brit. J. Psychiat. 154: 195±200.
Ebrahim S, Barer D, Nouri F. 1987. A�ective illness afterstroke. Brit. J. Psychiat. 151: 52±56.
Everson SA, Kaplan GA, Goldberg DE, Salonen R,Salonen JT. 1997a. Hopelessness and 4-year progres-sion of carotid atherosclerosis. The Kuopio IschemicHeart Disease Risk Factor Study. Arterioscl. Thromb.Vasc. Biol. 17: 1490±1495.
Everson SA, Lynch JW, Chesney MA, Kaplan GA,Goldberg DE, Shade SB, Cohen RD, Salonen R,Salonen JT. 1997b. Interaction of workplace demandsand cardiovascular reactivity in progression of carotidatherosclerosis: population based study. Brit. Med. J.314: 553±558.
Everson SA, Roberts RE, Goldberg DE, Kaplan GA.1998. Depressive symptoms and increased risk ofstroke mortality over a 29-year period. Arch. Int. Med.158: 1133±1138.
Feibel JH, Springer CJ. 1982. Depression and failure toresume social activities after stroke. Arch. Phys. Med.Rehab. 63: 276±277.
Figiel GS, Krishnan KR, Doraiswamy PM, Rao VP,Nemero� CB, Boyko OB. 1991. Subcortical hyper-intensities on brain magnetic resonance imaging: acomparison between late age onset and early onsetelderly depressed subjects. Neurobiol. Ageing 12:245±247.
Fischer P, Simanyi M, Danielczyk W. 1990. Depressionin dementia of the Alzheimer type and in multi-infarctdementia. Am. J. Psychiat. 147: 1484±1487.
Folstein MF, Maiberger R, McHugh PR. 1977. Mooddisorder as a speci®c complication of stroke. J. Neurol.Neurosurg. Psychiat. 40: 1018±1020.
Forsell Y, Corder EH, Basun H, Lannfelt L, Viitanen M,Winblad B. 1977. Depression and dementia in relationto apolipoprotein E polymorphism in a populationsample age 75 � . Biol. Psychiat. 42: 898±903.
Fujikawa T, Yamawaki S, Touhouda Y. 1993. Incidenceof silent cerebral infarction in patients with majordepression. Stroke 24: 1631±1634.
Fujikawa T, Yamawaki S, Touhouda Y. 1994a. Back-ground factors and clinical symptoms of majordepression with silent cerebral infarction. Stroke 25:798±801.
Fujikawa T, Yamawaki S, Touhouda Y. 1994b. Clinicalstudy of correlation between presenile or seniledepressive state with silent cerebral infarction. Clinicalsymptoms and background factors. Jap. J. Psychosom.Med. 34: 362±367.
Ghika JA, Bogousslavsky J, Regli F. 1990. Deepperforators of the carotid system: template of thevascular territories. Arch. Neurol. 47: 1097±1100.
Greenwald BS, Kramer-Ginsberg E, Krishnan KR,Ashtari M, Aupperle PM, Patel M. 1996. MRI signalhyperintensities in geriatric depression. Am. J. Psy-chiat. 153: 1212±1215.
Hermann M, Bartels C, Wallesch CW. 1993. Depressionin acute and chronic aphasia: symptoms, pathoanato-mical±clinical correlations and functional implica-tions. J. Neurol. Neurosurg. Psychiat. 56: 672±678.
Hickie I, Scott E. 1998. Late-onset depressive disorders:a preventable variant of cerebrovascular disease?Psychol. Med. 28: 1007±1013.
Hickie I, Scott E, Mitchell P, Wilhelm K, Austin MP,Bennett B. 1995. Subcortical hyperintensities onmagnetic resonance imaging: clinical correlates andprognostic signi®cance in patients with severe depres-sion. Biol. Psychiat. 37: 151±160.
Hirono N, Mori E, Ishii K, Ikejiri Y, Imamura T,Shimomura T, Hashimoto M, Yamashita M, SasakiM. 1998. Frontal lobe hypometabolism and depres-sion in Alzheimer's disease. Neurology 50: 380±383.
Holroyd S, Duryee JJ. 1997. Di�erences in geriatricpsychiatry outpatients with early- vs late-onset depres-sion. Int. J. Geriatr. Psychiat. 12: 1100±1106.
House A, Dennis M, Warlow C, Hawton K, MolyneuxA. 1990a. Mood disorders after stroke and theirrelation to lesion location. A CT scan study. Brain113: 1113±1129.
House A, Dennis M, Warlow C, Hawton K, MolyneuxA. 1990b. The relationship between intellectualimpairment and mood disorder in the ®rst year afterstroke. Psychol. Med. 20: 805±814.
House A, Dennis M,Mogridge L,Warlow C, Hawton K,Jones L. 1991. Mood disorders in the year after ®rststroke. Brit. J. Psychiat. 158: 83±92.
Iacoboni M, Padovani A, Di Piero V, Lenzi GL. 1995.Poststroke depression: relationships with morpho-logical damage and cognition over time. It. J. Neurol.Sci. 16: 209±216.
Iadaka T, Nakajima T, Kawamoto K, Fukuda H, SuzukiY, Machara T, Shiraishi H. 1996. Signal hyperinten-sities on brain magnetic resonance imaging in elderlydepressed patients. Eur. Neurol. 36: 293±299.
Ito H, Kawashima R, Awata S, Ono S, Sato K, Goto R,Koyama M, Sato M, Fukuda H. 1996. Hypoperfusionin the limbic system and prefrontal cortex in depres-sion: SPECT with anatomic standardization tech-nique. J. Nucl. Med. 37: 410±414.
Jacoby RJ, Levy R. 1980. Computed tomography in theelderly. 3. A�ective disorder. Brit. J. Psychiat. 136:270±275.
Copyright # 2000 John Wiley & Sons, Ltd. Int. J. Geriat. Psychiatry 15, 419±433 (2000)
430 R. RAO

Johnson G, Burvill PW, Anderson CS, Jamrozik K,Stewart-Wynne EG, Chakera TM. 1995. Screeninginstruments for depression and anxiety followingstroke: experience in the Perth community strokestudy. Acta Psychiat. Scand. 91: 252±257.
Krishnan KR, Tupler LA, McDonald WM, Fujikawa T,Yamawaki S. 1994a. Background factors and clinicalsymptoms of major depression with silent cerebralinfarction. Stroke 25: 2507.
Krishnan KRR, Fitchie JC, Tupler LA,McDonaldWM,Knight D, Nancro� CB, Marcovinch S. 1994b. Apo-lipoprotein E-e 4. Neurology 44: 2420±2421.
Lammi UK, Kivela SL, Nissinen A, Punsar S, KarvonenM. 1989. Mental disability among elderly men inFinland: prevalence, predictors and correlates. ActaPsychiat. Scand. 80: 459±468.
Levy ML, Cummings JL, Fairbanks LA. 1998. Apathy isnot depression. J. Neuropsychiat. Clin. Neurosci. 10:314±319.
Lipsey JR, Robinson RG, Pearlson GD, Rao K, PriceTR. 1983. Mood change following bilateral hemi-sphere brain injury. Brit. J. Psychiat. 143: 266±273.
Lodder J, Bamford J, Kappelle J, Boiten J. 1994. Whatcauses false clinical prediction of small deep infarcts?Stroke 25: 86±91.
MacHale SM, O'Rourke SJ, Wardlaw JM, Dennis MS.1998. Depression and its relation to lesion locationafter stroke J. Neurol. Neurosurg. Psychiat. 64:371±374.
Marin RS, Fogel BS, Hawkins J, Du�y J, Krupp B.1995. Apathy: a treatable syndrome. J. Neuropsychiat.Clin. Neurosci. 7: 23±30.
Mathew RJ, Meyer JS, Semchuk KM, Francis D, MortelK, Claghorn JL. 1980. Regional cerebral blood ¯ow indepression: a preliminary report. J. Clin. Psychiat. 41:71±72.
Mayberg HS. 1993. Neuroimaging studies of depressionin neurologic disease. In Depression in NeurologicDisease, Starkstein SE, Robinson RG (eds); JohnsHopkins University Press: Baltimore.
Mayberg HS, Lewis PJ, Regenold W, Wagner HN Jr.1994. Paralimbic hypoperfusion in unipolar depres-sion. J. Nucl. Med. 35: 929±934.
Morris PL, Robinson RG, Raphael B, Bishop D. 1991.The relationship between the perception of socialsupport and post-stroke depression in hospitalizedpatients. Psychiatry 54: 306±316.
Morris PL, Robinson RG, Raphael B, Samuels J,Molloy P. 1992. The relationship between risk factorsfor a�ective disorder and poststroke depression inhospitalised stroke patients. Austr. NZ J. Psychiat. 26:208±217.
Morris PL, Robinson RG, Andrzejewski P, Samuels J,Price TR. 1993a. Association of depression with10-year poststroke mortality. Am. J. Psychiat. 150:124±129.
Morris PL, Robinson RG, Samuels J. 1993b. Depres-sion, introversion and mortality following stroke.Austr. NZ J. Psychiat. 27: 443±449.
Morris PL, Robinson RG, de Carvalho ML, Albert P,Wells JC, Samuels JF, Eden-Fetzer D, Price TR.1996a. Lesion characteristics and depressed mood inthe stroke data bank study. J. Neuropsychiat. Clin.Neurosci. 8: 153±159.
Morris PL, Robinson RG, Raphael B, Hopwood MJ.1996b. Lesion location and poststroke depression.J. Neuropsychiat. Clin. Neurosci. 8: 399±403.
Ng KC, Chan KL, Straughan PT. 1995. A study of post-stroke depression in a rehabilitative center. ActaPsychiat. Scand. 92: 75±79.
O'Brien J, Desmond P, Ames D, Schweitzer I, HarriganS, Tress B. 1996a. A magnetic resonance imaging studyof white matter lesions in depression and Alzheimer'sdisease. Brit. J. Psychiat. 168: 477±485.
O'Brien J, Ames D, Schweitzer I. 1996b. White matterchanges in depression and Alzheimer's disease: areview of magnetic resonance imaging studies. Int. J.Geriatr. Psychiat. 11: 681±694.
O'Brien J, Ames D, Chiu E, I, Desmond P, Tress B.1998. Severe deep white matter lesions and outcome inelderly patients with major depressive disorder: followup study. Brit. Med. J 317: 982±984.
Parikh RM, Lipsey JR, Robinson RG, Price TR. 1988. Atwo year longitudinal study of poststroke mooddisorders: prognostic factors related to one and twoyear outcome. Int. J. Psychiatr. Med. 18: 45±56.
Philips P. 1999. Improved stroke imaging techniques.J.A.M.A. 281: 2073±2074.
Pohjasvaara T, Leppavuori A, Siira I, Vataja R, KasteM, Erkinjuntti T. 1998. Frequency and clinicaldeterminants of poststroke depression. Stroke 29:2311±2317.
Rabkin JG, Charles E, Kass F. 1983. Hypertension andDSM-III depression in psychiatric outpatients. Am. J.Psychiat. 140: 1072±1074.
Rao R. 1996. Pathogenesis of white matter lesions inAlzheimer's disease and depression. Brit. J. Psychiat.169: 114.
Rao R. 1998a. Depression after transient ischemicattack: a clinically distinct subtype of vasculardepression? Arch. Gen. Psychiat. 55: 753±754.
Rao R. 1998b. A Study of Mood and Cognition inVascular Disease. MD Thesis. University of London,London.
Rao R, Howard R. 1998. Vascular dementia: dead oralive? Int. J. Geriatr. Psychiat. 13: 277±284.
Rao R, Jackson S, Howard R. 1999. Primitive re¯exes incerebrovascular disease: a community study of olderpeople with stroke and carotid stenosis. Int. J. Geriatr.Psychiat. 14: 964±972.
Reding MJ, Haycox J, Wigforss K, Brush D, Blass JP.1984. Follow up of patients referred to a dementiaservice. J. Am. Geriatr. Soc. 32: 265±268.
Copyright # 2000 John Wiley & Sons, Ltd. Int. J. Geriat. Psychiatry 15, 419±433 (2000)
CEREBROVASCULAR DISEASE AND LATE LIFE DEPRESSION 431
Reichman WE, Coyne AC. 1995. Depressive symptomsin Alzheimer's disease and multi-infarct dementia.J. Geriatr. Psychiat. Neurol. 8: 96±99.
Ring HA, Bench CJ, Trimble MR, Brooks DJ,Frakowiak RSJ, Dolan RJ. 1994. Depression inParkinson's disease: a positron emission study. Brit.J. Psychiat. 165: 333±339.
Robinson RG. 1979. Di�erential behavioral and bio-chemical e�ects of right and left hemispheric cerebralinfarction in the rat. Science 205: 707±710.
Robinson RG, Bloom FE. 1977. Pharmacologicaltreatment following experimental cerebral infarction:implications for understanding psychological symp-toms of human stroke. Biol. Psychiat. 12: 669±680.
Robinson RG, Price TR. 1982. Post-stroke depressivedisorders: a follow-up study of 103 patients. Stroke 13:635±641.
Robinson RG, Szetela B. 1981. Mood change followingleft hemispheric brain injury. Ann. Neurol. 9: 447±453.
Robinson RG, Bloom FE, Battenberg EL. 1977. A¯uorescent histochemical study of changes in nor-adrenergic neurons following experimental cerebralinfarction in the rat. Brain Res. 132: 259±272.
Robinson RG, Kubos KL, Starr LB, Rao K, Price TR.1983a. Mood changes in stroke patients: relationshipto lesion location. Compr. Psychiat. 24: 555±566.
Robinson RG, Starr LB, Kubos KL, Price TR. 1983b. Atwo-year longitudinal study of post-stroke mooddisorders: ®ndings during the initial evaluation. Stroke14: 736±741.
Robinson RG, Kubos KL, Starr LB, Rao K, Price TR.1984a. Mood disorders in stroke patients. Importanceof location of lesion. Brain 107: 81±93.
Robinson RG, Starr LB, Lipsey JR, Rao K, Price TR.1984b. A two-year longitudinal study of post-strokemood disorders: dynamic changes in associatedvariables over the ®rst six months of follow-up. Stroke15: 510±517.
Robinson RG, Lipsey JR, Bolla-Wilson K, Bolduc PL,Pearlson GD, Rao K, Price TR. 1985a. Mooddisorders in left-handed stroke patients. Am. J.Psychiat. 142: 1424±1429.
Robinson RG, Starr LB, Lipsey JR, Rao K, Price TR.1985b. A two-year longitudinal study of post-stroke mood disorders. In-hospital prognostic factorsassociated with six-month outcome. J. Nerv. Ment.Dis. 173: 221±226.
Robinson RG, Bolduc PL, Price TR. 1987. Two-yearlongitudinal study of poststroke mood disorders:diagnosis and outcome at one and two years. Stroke18: 579±584.
Sackeim HA, Prohovnik I, Moeller JR, Mayeux R,Stern Y, Devanand DP. 1993. Regional cerebral blood¯ow in mood disorders. II. Comparison of majordepression and Alzheimer's disease. J. Nucl. Med. 34:1090±1101.
Salloway S, Malloy P, Kohn R, Gillard E, Du�y J, RoggJ, Tung G, Richardson E, Thomas C, Westlake R.
1996. MRI and neuropsychological di�erences inearly- and late-life-onset geriatric depression. Neuro-logy 46: 1567±1574.
Schlegel S, Aldenho� JB, Eissner D, Lindner P, NickelO. 1989. Regional cerebral blood ¯ow in depression:associations with psychopathology. J. A�ect. Disord.17: 211±218.
Schmand B, Hooijer C, Jonker C, Lindeboom J, HavekesLM. 1998. Apolipoprotein E phenotype is not relatedto late-life depression in a population-based sample.Soc. Psychiat. Psychiat. Epidemiol. 33: 21±26.
Schmitz EB, Moriarty J, Costa DC, Ring HA, Ell PJ,Trimble MR. 1997. Psychiatric pro®les and patterns ofcerebral blood ¯ow in focal epilepsy: interactionsbetween depression/obsessionality, and perfusionrelated to the laterality of the epilepsy. J. Neurol.Neurosurg. Psychiat. 62: 458±463.
Schramke CJ, Stowe RM, Ratcli� G, Goldstein G,Condray R. 1998. Poststroke depression and anxiety:di�erent assessment methods result in variations inincidence and severity estimates. J. Clin. Exp. Neu-ropsychol. 20: 723±737.
Schwartz JA, Speed NM, Brunberg JA, Brewer TL,Brown M, Greden JF. 1993. Depression in strokerehabilitation. Biol. Psychiat. 33: 694±699.
Sharpe M, Hawton K, House A, Molyneux A, Sander-cock P, Bamford J, Warlow C. 1990. Mood disordersin long-term survivors of stroke: associations withbrain lesion location and volume. Psychol. Med. 20:815±828.
Shima S, Kitagawa Y, Kitamura T, Fujinawa A,Watanabe Y. 1994. Poststroke depression. Gen.Hosp. Psychiat. 16: 286±289.
Shimoda K, Robinson RG. 1999. Poststroke depressionand anxiety: Di�erent assessment methods result invariations in incidence and severity estimates. Biol.Psychiat. 45: 187±192.
Shinar D, Gross CR, Price TR, Banko M, Bolduc PL,Robinson RG. 1986. Screening for depression instroke patients: the reliability and validity of theCenter for Epidemiologic Studies Depression Scale.Stroke 17: 241±245.
Simpson S, Talbot PR, Snowden JS, Neary D. 1997a.Subcortical vascular disease in elderly patients withtreatment resistant depression. J. Neurol. Neurosurg.Psychiat. 62: 196±197.
Simpson SW, Jackson A, Baldwin RC, Burns A. 1997b.Subcortical hyperintensitites in late-life depression:acute response to treatment and neuropsychologicalimpairment. Int. Psychogeriat. 9: 257±275.
Simpson S, Baldwin RC, Jackson A, Burns AS. 1998. Issubcortical disease associated with a poor response toantidepressants? Neurological, neuropsychologicaland neuroradiological ®ndings in late-life depression.Psychol. Med. 28: 1015±1026.
Sinyor D, Jacques P, Kaloupek DG, Becker R,Goldenberg M, Coopersmith H. 1986. Poststrokedepression and lesion location. Brain 109: 537±546.
Copyright # 2000 John Wiley & Sons, Ltd. Int. J. Geriat. Psychiatry 15, 419±433 (2000)
432 R. RAO
Starkstein SE, Robinson RG, Price TR. 1987. Com-parison of cortical and subcortical lesions in theproduction of poststroke mood disorders. Brain 110:1045±1059.
Starkstein SE, Robinson RG, Honig MA, Parikh RM.1989. Mood changes after right-hemisphere lesions.Brit. J. Psychiat. 155: 79±85.
Sultzer DL, Levin HS, Mahler ME, High WM,Cummings JL. 1992. A comparison of psychiatricsymptoms in vascular dementia and Alzheimer'sdisease. Am. J. Psychiat. 150: 1806±1812.
Sultzer DL, Mahler ME, Cummings JL, Van Gorp WG,Hinkin CH, Brown C. 1995. Cortical abnormalitiesassociated with subcortical lesions in vasculardementia. Clinical and positron emission tomographic®ndings. Arch. Neurol. 52: 773±780.
Uytdenhoef P, Portelange P, Jacquy J, Charles G,Linkowski P, Mendlewicz J. 1983. Regional cerebralblood ¯ow and lateralized hemispheric dysfunction indepression. Brit. J. Psychiat. 143: 128±132.
Wells CE. 1979. Pseudodementia. Am. J. Psychiat. 136:895±900.
Yamaguchi S, Kobayashi S, Koide H, Tsunematsu T.1992. Longitudinal study of regional cerebral blood¯ow changes in depression after stroke. Stroke 23:1716±1722.
Zubenko GS, Sullivan P, Nelson JP, Belle SH, Hu�FJ, Wolf GL. 1990. Brain imaging abnormalitiesin mental disorders of late life. Arch. Neurol. 47:1107±1111.
Copyright # 2000 John Wiley & Sons, Ltd. Int. J. Geriat. Psychiatry 15, 419±433 (2000)
CEREBROVASCULAR DISEASE AND LATE LIFE DEPRESSION 433