Embed Size (px)
Citation preview

Ž .Journal of Neuroimmunology 93 1999 8–14
Cerebrospinal fluid abnormalities in a phase III trial of Avonex w
ž / 1IFNb-1a for relapsing multiple sclerosis
Richard A. Rudick a,), Diane L. Cookfair b, Nancy A. Simonian c, Richard M. Ransohoff a,John R. Richert d, Lawrence D. Jacobs b, Robert M. Herndon e, Andres M. Salazar f,
Jill S. Fischer a, Carl V. Granger b, Donald E. Goodkin g, Jack H. Simon h,David M. Bartoszak f, Dennis N. Bourdette i, Jonathan Braiman f,
Carol M. Brownscheidle b, Michael E. Coats f, Stanley L. Cohan d, David S. Dougherty f,Revere P. Kinkel a, Michele K. Mass d, Frederick E. Munchsauer b, Kathy O’Reilly b,
Roger L. Priore b, Patrick M. Pullicino b, Barbara J. Scherokman j, Karl Wende b,Bianca Weinstock-Guttman a, Ruth H. Whitham i, The Multiple Sclerosis Collaborative
Research Group 2
a Mellen Center For Multiple Sclerosis Treatment and Research, Department of Neurology, Area U-100, The CleÕeland Clinic Foundation,CleÕeland, OH 44106, USA
b UniÕersity of Buffalo, Buffalo, NY, USAc Biogen, Cambridge, MA, USA
d Georgetown UniÕersity Medical Center, Washington, DC, USAe Good Samaritan Hospital and Medical Center, Portland, OR, USA
f Walter Reed Army Medical Center, Washington, DC, USAg UniÕersity of California, San Francisco, CA, USA
h UniÕersity of Colorado Health Sciences Center, DenÕer, CO, USAi Oregon Health Sciences UniÕersity, Portland, OR, USA
j Kaiser Permanente Medical Center, Springfield, VA, USA
Received 1 April 1998; revised 7 July 1998; accepted 7 July 1998
Abstract
Background and objectiÕe: This report provides results of CSF analyses done in a subset of relapsing remitting MS patientsparticipating in a placebo-controlled, double-blind, phase III clinical trial of IFNb-Studies supported by the National Multiple Sclerosis
Ž . Ž w .Society grants RG2019, RG2827 ,a Avonex , Biogen . The clinical trial demonstrated that IFNb-1a treatment resulted in significantlyreduced disability progression, annual relapse rate, and new brain lesions visualized by cranial magnetic resonance imaging. The
Ž .objectives of the current study were to determine: a whether CSF abnormalities in MS patients correlated with disease or MRIŽ . Ž .characteristics, and b effects of IFNb-1a therapy on these CSF abnormalities. Methods: CSF was analyzed from 262 87% of the 301
study subjects at entry into the clinical trial, and a second CSF sample was analyzed from 137 of these 262 subjects after 2 years ofŽ .therapy. CSF cell counts, oligoclonal bands OCB , IgG index, and free kappa light chains were measured using standard assays. Baseline
CSF results were compared with demographic, disease, and MRI parameters. Differences in on-study relapse rate, gadoliniumenhancement, and EDSS change according to baseline CSF status was used to determine the predictive value of CSF for subsequent
Ž .clinical and MRI disease activity. Change in CSF parameters after 104 weeks were used to determine the effects of treatment. Results: 1At study baseline, 37% of the subjects had abnormal CSF WBC counts, 61% had abnormal levels of CSF free kappa light chains, 84%
Ž .had abnormal IgG index values, and 90% were positive for OCB. 2 Baseline IgG index, kappa light chains, and OCB showed weaklypositive, statistically significant correlations with Gd-enhanced lesion volume and T2 lesion volume. WBC showed a statistically
) Corresponding author. Tel.: q1-216-444-8603; Fax: q1-216-445-7013; E-mail: [email protected] Ž . Ž .Studies supported by the National Multiple Sclerosis Society grants RG2019, RG2827 ; the NINDS NS26321 ; and Biogen Inc.2 MSCRG, Buffalo, Cleveland, Washington, Portland, USA
0165-5728r99r$ - see front matter q 1999 Elsevier Science B.V. All rights reserved.Ž .PII: S0165-5728 98 00174-X

( )R.A. Rudick et al.rJournal of Neuroimmunology 93 1999 8–14 9
Ž .significant correlation with Gd-enhancing lesion volume but was uncorrelated with T2 lesion volume. 3 There was an associatedŽ .between baseline CSF WBC counts and on-study clinical and MRI disease activity in placebo recipients. 4 IFNb-1a treatment resulted
in significantly reduced CSF WBC counts, but there was no treatment-related change in CSF IgG index, kappa light chains, or OCB,which remained relatively stable over time in both patient groups. Conclusions: The current study documents significant reductions inCSF WBC counts in patients treated with IFNb-1a for 104 weeks. This finding is considered relevant to the therapeutic response, sinceCSF WBC counts were found to be positively correlated with subsequent clinical and MRI disease activity in placebo-treated relapsingMS patients. q 1999 Elsevier Science B.V. All rights reserved.
Keywords: Multiple sclerosis; Interferon; Interferon beta; Controlled clinical trials; Cerebrospinal fluid; CSF free kappa light chains; Oligoclonal bands;CSF IgG index
1. Introduction
Two forms of recombinant interferon beta, IFNb-1aŽ w . Ž wAvonex , Biogen and IFNb-1b Betaseron , Berlex
.Laboratories , have been approved by US and Europeanregulatory agencies for relapsing remitting MS, based on
Žmulticenter placebo-controlled clinical trials The IFNB.Study Group, 1993; Jacobs et al., 1995 . Beneficial effects
of IFNb treatment include reduced relapse frequency, lessprogression of neurologic disability, fewer gadolinium en-hancing MRI brain lesions, and less accumulation of MRIT2 lesion volume. The precise mechanisms of action ofIFNb in MS patients are presently unknown, however.IFNb is likely to inhibit pathologic events at an early stageof new lesion formation, in view of its inhibition of newgadolinium enhancing lesions. IFNb-1b was reported toincrease soluble VCAM levels and this effect was found tocorrelate with the effect of IFNb-1b on the number of
Ž .gadolinium enhancing lesions Calabresi et al., 1997 . Thissuggested the possibility that the effect of IFNb therapy ongadolinium enhancing lesions may be associated with re-duced leukocyte trafficking into the CNS. We found in-creased CSF levels of the anti-inflammatory cytokine IL-10in relapsing remitting MS patients treated with IFNb-1a,and this effect was significantly correlated with a favorable
Ž .clinical response to therapy Rudick et al., 1998 . Thisfinding further suggested that IFNb-1a exerts therapeuticeffects by inhibiting inflammation within the CNS.
Cerebrospinal fluid inflammatory changes have beencommonly observed in patients with MS. A lymphocyticpleocytosis has been found in about 60% of patients in the
Ž .relapsing remitting phase of MS Link and Muller, 1971 .¨
Ž .Intrathecal immunoglobulin Ig synthesis has been ob-served by electrophoretic techniques as oligoclonal bandsŽ .OCB and by immunoassays as increased concentrationsof IgG or free kappa light chains. CSF abnormalities have
Žbeen used to aid in the diagnosis of MS Rudick et al.,.1989; Andersson et al., 1994 , and also as a marker for
Žresponse to therapy Tourtellotte et al., 1980; Hommes et.al., 1984 .
This report provides results of CSF analyses done in asubset of the MS patients participating in the placebo-con-trolled phase III clinical trial of IFNb-1a. The CSF studieswere conducted in parallel with the NIH and Biogen-sponsored clinical trial. The objectives of the study, set out
Ž .in advance of the trial, were to determine: a whether CSFabnormalities commonly reported in MS patients corre-
Ž .lated with disease or MRI characteristics, and b theeffects of IFNb-1a therapy on these CSF abnormalities.
2. Methods
2.1. Study design
Details of the clinical trial methodology have beenŽ .published Jacobs et al., 1995 . Briefly, 301 subjects with
relapsing MS were enrolled at 4 clinical sites in the US.Subjects had definite relapsing remitting MS, baselineEDSS of 1.0–3.5 inclusive, at least 2 relapses in themedical record in the prior 3 years, no relapses for at least2 months prior to study entry, and were between 18 and 55years of age. The study was a double-blind, placebo-con-trolled, randomized clinical trial. The sample size calcula-tion was not based on anticipated changes in CSF parame-
Table 1Characteristics of all study subjects with baseline CSF data
Ž .Parameter Number Mean SD Median Range % Abnormal
Ž . Ž .Disease duration years 262 6.3 5.78 4.83 1–31 NAŽ .EDSS at study baseline 262 2.4 0.84 2.5 1.0–3.5 NAŽ .Relapse rate pre-study 262 1.2 0.57 1.0 0.67–3.7 NA
3 aŽ . Ž .Gadolinium lesion volume mm 259 231 457 18.0 0 to 2858 53.8%3Ž . Ž .MRI T2 lesion volume mm 228 13,730 13,221 10,658 0 to 66,900 NA
3 bŽ . Ž .WBC cellsrmm 249 7.6 13.6 4.0 0–150 37.3%bŽ . Ž .Free kappa chains ugrml 262 0.70 0.66 0.47 0.05–4.59 60.7%bŽ .IgG index 254 1.25 0.84 1.04 0.40–10.1 83.9%bOligoclonal bands 262 NA NA NA 89.7%
a Percent enhancing.b Normal: -0.34 ugrml for free kappa chains; -0.67 for IgG index, -6rmm3 for CSF cell count, and absent for OCB.

( )R.A. Rudick et al.rJournal of Neuroimmunology 93 1999 8–1410
Table 2Baseline CSF results by treatment arma for the 2-year patient subset
wPlacebo recipients Avonex recipients
CSF WBC Count Ns68 Ns66Ž . Ž . Ž .Mean SD 6.35 10.4 6.71 7.66
Median 4.0 4.0Range 0–73 0–35
3Ž .% Abnormal G6rmm 27.9% 45.5%
Free Kappa Chains Ns72 Ns65Ž . Ž . Ž .Mean SD 0.70 0.64 0.74 0.52
Median 0.49 0.61Range 0.05–3.24 0.05–1.86
Ž .% Abnormal G0.34 ugrml 66.7% 72.3%
IgG Index Ns65 Ns62Ž . Ž . Ž .Mean SD 1.23 0.60 1.42 0.73
Median 1.03 1.26Range 0.51–3.2 0.45–3.86
Ž .% Abnormal G0.67 83.1% 90.3%
Oligoclonal Bands Ns72 Ns65% With Oligoclonal Bands 86.1% 97.0%
a There were no statistically significant CSF differences between placeborecipients and IFNb-1a recipients at baseline.
ters, which were considered exploratory measures in theoriginal study plan. Study visits were scheduled at baselineand every 6 months.
Ž w .Interferon beta-1a Avonex , a natural sequence, gly-cosylated, recombinant Chinese hamster ovary product,was administered intramuscularly at a dose of 6.0 million
Ž .international units 30 mcg weekly for up to 104 weeksŽ .Jacobs and Munschauer, 1992 . Under the direction of thetreating neurologist, patients received appropriate standardmedical care for MS symptoms, and disease relapses weretreated with either IV methylprednisolone followed by abrief oral steroid taper or with intramuscular ACTH.
Ž .CSF was obtained by lumbar puncture LP from 262Ž .87% of the 301 subjects at entry into the clinical trial.Data from these 262 subjects was used to compare CSFcharacteristics with demographic, disease, and MRI param-
Ž .eters at study baseline. 137 52% of these 262 subjectsunderwent a second LP after 2 years of therapy. Data from
these 137 subjects was used to evaluate change in CSF inplacebo and IFNb-1a treated subjects.
CSF and serum IgG and albumin were determined bystandard methods at clinical labs at each of the clinical
Žsites and used to calculate an IgG index Link and Tib-.bling, 1977 . Blood and CSF OCB, and CSF cell counts
were detected using standard methods by clinical labs ateach site. Free kappa light chains were quantified at the
ŽCleveland site with an ELISA assay Stanescu et al.,.1991 .
2.2. Statistical methods
Univariate baseline correlations between CSF variablesand MRI data were determined using Spearman rank corre-lation coefficients. Categorical analyses were performedusing the chi-square or Fisher’s exact test as appropriate.Differences in mean values at baseline and within personpercent change over 2 years were compared using a t-testor Mann–Whitney rank sum test as appropriate.
3. Results
The age and gender distribution for the 262 individualswho underwent baseline LPs did not differ from that
Žreported for the 301 patients enrolled in the trial Jacobs et. Ž .al., 1995 . The mean age SD of the 262 study subjectsŽ .was 36.7 7.23 and 67% were female. Table 1 lists disease
characteristics and CSF findings for these subjects. Dura-tion of disease, baseline EDSS, pre-study relapse rate,gadolinium enhancing lesion volume, and T2 lesion vol-ume were not significantly different in this group com-
Ž .pared with the total study population Jacobs et al., 1996 .The number and type of CSF abnormalities observed weretypical for relapsing MS patients. Thirty-seven percent of
Žthe subjects had elevated CSF WBC counts G 63.WBCrmm , 61% had abnormal levels of CSF free kappaŽ .light chains G0.34 ugrml , 84% had high IgG index
Ž .values G0.67 , and 90% of the subjects were positive foroligoclonal bands.
Table 2 shows baseline CSF results for Placebo andAvonex w recipients who were treated on protocol for 2
Table 3Spearman rank r values for baseline MRI and CSF characteristics
Baseline variables WBC, Ns246 Free Kappa Chains, Ns262 IgG Index, Ns254 OCB, Ns262bGd lesion volume 0.184)) 0.188)) 0.188)) P)N )
cT2 lesion volume 0.097 0.164)) 0.219))) P)N))
WBC count 0.367))) 0.335))) P)N)
aFree kappa chains 0.367))) 0.670))) P)N)))
IgG Index 0.335))) 0.670))) P)N)))
aNs236 for correlations between CSF parameters.b P)N: Mean for OCB positive patients is greater than that for OCB negative patients.cNs214.) pF0.05.)) pF0.001.))) pF0.0001.

( )R.A. Rudick et al.rJournal of Neuroimmunology 93 1999 8–14 11
Table 4Baseline CSF WBC predicts subsequent disease activity in placebo recipients
a b cNormal Abnormal p-value
RelapsesNumber in year 1
Ž . Ž . Ž .Mean SD 0.60 0.81 1.06 1.01 0.02Ž . Ž . Ž .No. of % relapse free 17r30 56.7% 27r84 32.1% 0.03
Number in year 2Ž . Ž . Ž .Mean SD 1.42 1.19 1.89 1.79 0.17Ž . Ž . Ž .No. of % relapse free 9r24 37.5 13r57 22.8 0.19
Gadolinium enhancementŽ . Ž . Ž .No. of % enhanced at year 1 6r28 21.4% 48r109 51.5% 0.01Ž . Ž . Ž .No. of % enhanced at year 2 6r24 25% 28r52 53.9% 0.03
dChange in EDSS in 2 yearsŽ . Ž . Ž .Mean SD 0.33 1.60 0.90 1.38 0.04
a Normal -2 WBCrmm3.bAbnormal G2 WBCrmm3.c Mann–Whitney p-value.d Unsustained Change in EDSS among placebo patients. Time to onset of sustained change in EDSS was compared in all placebo recipients with baseline
Ž .CSF data 77 placebo recipients with baseline WBC -6 and 55 placebo recipients with baseline WBC G6 . Placebo recipients with CSF WBC -6Ž .trended toward longer time to sustained progression ps0.09 .
years and had a second LP. There were no significantdifferences between the larger group of patients who hadan initial lumbar puncture, and the smaller cohort ofsubjects who had repeat LPs. Similarly, there were nosignificant baseline CSF differences between the placeborecipients and the Avonex w recipients who had both base-line and year 2 lumbar punctures.
Table 3 shows correlations between baseline diseasecharacteristics and CSF parameters, and between individ-ual CSF parameters. Baseline WBC count showed a statis-tically significant, moderately strong correlation with kappalight chains, IgG index, and OCB. There was a muchstronger correlation between kappa light chains, IgG index,and OCB. This suggested that kappa light chains, IgG
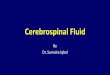
Ž .Fig. 1. Proportion of patients with a change in CSF status normal vs. abnormal between baseline and week 104 of therapy. Subjects generally retained thesame status during the treatment. For kappa light chains and IgG index, subjects who changed status were more likely to become normal, and there was nodifference in the two treatment arms. For CSF WBC status, subjects in the Avonex w group were more than twice as likely to become normal and were less
Ž .than half as likely to become abnormal than were subjects in the placebo arm Fisher Exact Test, ps0.028 . Note that this analysis only involved patientswith a change in CSF status between baseline and week 104.

( )R.A. Rudick et al.rJournal of Neuroimmunology 93 1999 8–1412
index, and OCB were measuring a separate biologicaldimension from WBC.
CSF WBC, kappa light chains, and IgG index were notsignificantly correlated with baseline disease duration,
Ž .EDSS, or pre-study relapse rate data not shown . Simi-larly, there were no differences in these disease parametersin subjects with and without OCB. Baseline IgG index,kappa light chains, WBC, and the presence of OCB showedweakly positive, statistically significant correlations withGd-enhanced lesion volume and T2 lesion volume. Ofinterest, WBC showed a statistically significant correlationwith Gd-enhancing lesion volume, but was completelyuncorrelated with T2 lesion volume. CSF abnormalities,however, showed some association with age and gender atbaseline. There was a weak inverse correlation between
Ž .age and the IgG index rsy0.141, p-0.03 , kappaŽ . Žlight chains rsy0.148, p-0.02 and WBC rs
.y0.128, p-0.05 ; younger patients had more abnormali-ties than older patients. There was no association betweenOCB status and age. Slightly more females were positive
Žfor OCBs at baseline than males 91.8% vs. 83.6%, p-.0.06 , and females had significantly higher IgG index
Ž Ž . Ž . Ž .values than males mean SD 1.32 0.92 vs. 1.03 0.54 ;.Mann–Whitney p-0.001 . There was no significant asso-
ciation between gender and either kappa light chains orWBC status.
There was a significant relationship between baselineCSF WBC and subsequent disease activity in the placebo
Ž .recipients Table 4 . Subjects with abnormal WBC atbaseline had a higher relapse rate during the subsequentyear, and were significantly less likely to remain relapse-free. Subjects with abnormal WBC at baseline had a 3-foldincrease in the mean EDSS change over 2 years, and weresignificantly more likely to have Gd-enhancing lesionsafter one and 2 years. However, baseline kappa lightchains, IgG index, and OCB status were not associatedwith on-study relapse rate, change in EDSS, or MRIfindings. These data indicate that baseline WBC status, butnot kappa light chains, IgG, or OCB status, was positivelycorrelated with subsequent disease activity.
We evaluated the frequency with which the CSF param-eters changed from normal to abnormal, or from abnormal
Ž .to normal during between week 0 and week 104 Fig. 1 .Kappa light chains retained the same status in 80% of thecases, IgG index in 90% of the cases, and OCB in 88% ofthe cases, indicating that these measures were quite stableover the 2-year time course. CSF WBC count was lessstable. CSF cell count remained the same in about 66% ofthe subjects, but changed in the other one-third. Fig. 1shows change according to the on-study treatment groupfor WBC and kappa light chains, and IgG index. Treat-ment group did not influence the direction of change for
Žkappa light chains or IgG index or for OCB, data not.shown . Subjects were equally likely to change in the same
direction in either treatment group. The direction of changefor WBC, however, depended on treatment group. Patients
in the IFNb-1a group were more than twice as likely tobecome normal, while patients in the placebo group weremore than twice as likely to become abnormal, and thiswas a significant difference between treatment armsŽ .Fisher’s exact test ps0.028 .
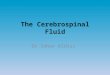
Fig. 2 shows percent change in CSF parameters during104 weeks on study according to treatment group. Therewas a significant difference in WBC change over 2 yearsbetween treatment arms. IFNb-1a recipients were morelikely to show decreased WBC than placebo recipientsŽ .Mann–Whitney ps0.04 . There were no significanttreatment arm effects on kappa light chains or IgG index.
Ž .The mean SD change in CSF WBC between baseline andw Ž .2 years for Avonex recipients was y1.75 13.8 and for
Ž . Ž .placebo recipients 0.095 7.97 Mann–Whitney ps0.03 .Excluding a single outlier in the Avonex w group with anincrease in CSF WBC of 82, the mean change was y3.34.
Ž .The mean SD change in CSF kappa light chains in thew Ž .Avonex recipients was y0.127 0.482 and for the
Ž . Žplacebo recipients y0.075 0.525 Mann–Whitney ps.0.308 .
An additional analysis was completed to determinewhether the treatment arm effect on WBC could be ex-plained by differential corticosteroid use in the two treat-ment arms. Subjects in both treatment arms were dividedaccording to whether they received corticosteroid treat-
Ž .Fig. 2. Box plots showing mean and interquartile range boxes forŽ .change from baseline for CSF WBC count panel A and CSF kappa light
Ž .chains panel B . There was a significant reduction in CSF WBC countsw Žin Avonex recipients compared with placebo recipients Mann–Whit-.ney p-0.04 .

( )R.A. Rudick et al.rJournal of Neuroimmunology 93 1999 8–14 13
ment within 2 months of their week 104 LP, as CSFchanges from a course of corticosteroids have been re-
Žported to persist for longer than 2 months Tourtellotte et. wal., 1980 . Eleven percent of Avonex recipients and 12%
of placebo recipients received steroids within 2 months oftheir second lumbar puncture. There was no significantdifference in the mean WBC change within either treat-ment arm between subjects treated with corticosteroids andsubjects not treated with corticosteroids. Despite smallernumbers, Avonex w recipients not treated with steroidstrended toward a reduction in CSF WBC compared with
Ž .placebo recipients not treated with steroids ps0.074 .Thus, corticosteroid administration did not appear to ex-plain reduced CSF WBC observed in the Avonex w recipi-ents.
4. Discussion
Our original purpose in studying CSF in the Avonex w
clinical trial was to better understand biological effects ofIFNb-1a in MS patients. Additionally, we were interestedin the relationship between CSF abnormalities in MSpatients and disease factors. The design of the studyfacilitated these goals, since patients were randomized toIFNb-1a or placebo, and all patients had yearly MRI scansand clinical assessment at least every 6 months. Of note,the study was powered to show an effect on the primaryclinical trial outcome, time to onset of sustained change inEDSS; CSF parameters and their analyses were consideredexploratory.
Cerebrospinal fluid data in this report are relativelyunique. CSF samples were collected for a well-definedcohort of MS patients entering a large multi-center clinicaltrial. The diagnosis of MS was carefully confirmed to meeteligibility requirements for the clinical trial; subjects haddocumented relapses in the prior 2 years; and all patientswere relapse-free and corticosteroid-free for 2 monthsbefore entering the trial. The baseline level EDSS wasbetween 1.0 and 3.5 inclusive, and the average diseaseduration was approximately 6 years. Thus, the CSF sam-ples were derived from a homogeneous group of patientsin the early stages of active relapsing remitting MS. Fur-thermore, in addition to the CSF samples collected at thetime of enrollment, CSF samples were also collected at theend of 2 years for consecutively enrolled patients whocompleted 2 years of therapy and consented to a secondLP.
CSF abnormalities in these patients at study entry wereconsistent with findings reported in various prior seriesŽHershey and Trotter, 1980; Rudick et al., 1989; Olsson,
.1994; Andersson et al., 1994; Pirttila and Nurmikko, 1995 .3 ŽCSF WBC averaged 7.6 cellsrmm 37% of the cases G6
3. Žcellsrmm , kappa light chains 0.7 ugrml 60.7% of the. Žcases G0.34 ugrml , and IgG index 1.25 84% of the
.cases G0.67 . Ninety percent of the subjects had oligo-
clonal bands. The magnitude of CSF abnormality was notfound to correlate with disease duration or severity atstudy entry, but there were significant albeit weak correla-tions with gadolinium enhancement and T2 lesion volumedetermined from baseline MRI scans. An unanticipatedfinding was higher levels of IgG index in female compared
Ž .with male patients 1.32"0.92 vs. 1.03"0.54, p-0.06 ,and higher frequency of OCB in female compared with
Ž .male MS patients 92% vs. 84%, p-0.001 .Kappa light chains, IgG index, and OCB behaved in a
similar fashion. They were strongly correlated to oneanother, were abnormal at baseline in the vast majority ofcases, were stable during the treatment phase, and thesemeasures did not change with IFNb-1a treatment. On theother hand, CSF WBC counts behaved differently from theother three assays. CSF WBC counts were only weaklycorrelated with kappa light chains, IgG index, or OCB,were abnormal in only a minority of patients at baseline,and CSF WBC counts were responsive to IFNb-1a ther-apy.
We found that kappa light chains, IgG index, and OCBwere quite stable over time in both the IFNb-1a andplacebo recipients. Approximately 80% of patients in bothtreatment arms had no change in kappa light chain statusŽ .i.e., normal, abnormal between baseline and week 104.An even higher percentage of patients in each treatmentarm showed no change in IgG index and OCB betweenbaseline and week 104. In those subjects who did change,CSF was more likely to become normal in both theIFNb-1a group and the placebo group.
About one-third of patients in each treatment armŽ .changed WBC status i.e., normal, abnormal between
week 0 and week 104. However, the pattern of changediffered significantly in the two treatment arms. Of thepatients who changed over the course of the trial, themajority of IFNb-1a recipients changed from abnormal tonormal, while the majority of placebo recipients changedfrom normal to abnormal. We also observed a percentchange in WBC counts between baseline and week 104 inthe IFNb-1a treated patients compared to placebo treatedpatients, and this change could not be accounted for bycorticosteroid use in the months prior to the second LP.The therapeutic effect on CSF WBC counts is consideredto be clinically relevant, as the baseline WBC count wasfound to be positively related to subsequent onstudy dis-ease activity in placebo recipients. Compared with placeborecipients with a normal CSF cell count, placebo recipientswith a CSF pleocytosis were found to have significantlymore relapses in the subsequent year, to have a signifi-cantly lower probability of being relapse-free, a signifi-cantly higher likelihood of having gadolinium enhance-ment at 1 and 2 years, and had a 3-fold increase in EDSSworsening after 2 years. In contrast, CSF kappa lightchains, IgG index, and OCB, which failed to change withIFNb-1a therapy, did not predict onstudy disease activityin the placebo recipients.

( )R.A. Rudick et al.rJournal of Neuroimmunology 93 1999 8–1414
Our data is consistent with a number of interferoneffects that have been previously reported. Reduced traf-ficking of peripheral blood mononuclear cells into theCNS has been postulated to result from an inhibitory effect
Ž .of IFN on adhesion molecules Calabresi et al., 1997 andŽmatrix metalloproteinases Leppert et al., 1997; Stuve et
.al., 1997 . Increased levels of CSF IL-10 following 2 yearsof IFNb-1a therapy in subjects in this same clinical trialŽ .Rudick et al., 1998 was found to correlate with a favor-able clinical response to therapy. Increased expression ofIL-10 within the CNS may in turn mediate an anti-in-flammatory effect via effects of IL-10 on chemokine ex-
Ž .pression Cassatella et al., 1998 or proinflammatory cy-Ž .tokines Tripp et al., 1993 . The lack of effect of treatment
on the IgG parameters, on the other hand, is not particu-larly surprising, as IFN has been reported to increase in
Ž .vivo expression of IL-4 Rudick et al., 1998 in IFNb-1atreated MS patients, and to stimulate immunoglobulin
Žsecretion in vitro Garrone et al., 1994; Liorente et al.,.1995; Marcelletti and Katz, 1996 . IFNb-1a would be
expected to shift the immune system in the direction of aTh2 response.
The current study documents significant reductions inCSF WBC counts in patients treated with IFNb-1a for 104weeks. Since CSF WBC counts were found to be posi-tively correlated with subsequent clinical and MRI diseaseactivity in placebo recipients, this finding may explain inpart the observed therapeutic response to IFNb-1a treat-ment in MS patients.
References
Andersson, M., Alvarez-Cermeno, J., Bernardi, G., Cogato, I., Fredman,P., Frederiksen, J., Fredrikson, S., Gallo, P., Grimaldi, L.M., Gron-ning, M. et al., 1994. Cerebrospinal fluid in the diagnosis of multiple
w x w xsclerosis: a consensus report Review 50 refs . J. Neurol. Neurosurg.Psychiatry 57, 897–902.
Calabresi, P.A., Tranquill, L.R., Dambrosia, J.M., Stone, L., Maloni, H.,Bash, C.N., Frank, J.A., McFarland, H.F., 1997. Increases in solubleVCAM-1 correlate with a decrease in MRI lesions in multiple sclero-sis treated with interferon b-1b. Ann. Neurol. 41, 669–674.
Cassatella, M.A., Meda, L., Bonora, S., Ceska, M., Constantin, G., 1998.Ž .Interleukin 10 IL-10 inhibits the release of proinflammatory cy-
tokines from human polymorphonuclear leukocytes. Evidence for anautocrine role of tumor necrosis factor and IL-1 beta in mediating theproduction of IL-8 triggered by lipopolysaccharide. J. Exp. Med. 178,2207–2211.
Garrone, P., Galibert, L., Rousset, F., Fu, S.M., Banchereau, J., 1994.Regulatory effects of prostaglandin E2 on the growth and differentia-tion of human B lymphocytes activated through their CD40 antigen. J.Immunol. 152, 4284–4290.
Hershey, L.A., Trotter, J.L., 1980. The use and abuse of the cerebrospinalfluid IgG profile in the adult: a practical evaluation. Ann. Neurol. 8,426–434.
Hommes, O.R., Lamers, K.J.B., Van Geel, W., 1984. Intrathecal IgGsynthesis and IgG index after intensive and chronic immunosuppres-sive treatment of multiple sclerosis. Ann. New York Acad. Sci. 436,410–417.
Jacobs, L., Cookfair, D.L., Rudick, R.A. et al., 1995. A phase III trial ofintramuscular recombinant beta interferon as treatment for exacerbat-ing-remitting multiple sclerosis: design and conduct of study andbaseline characteristics of patients. Multiple Sclerosis 1, 118–135.
Jacobs, L.D., Cookfair, D.L., Rudick, R.A., Herndon, R.M., Richert, J.R.,Salazar, A.M., Fischer, J.S., Goodkin, D.E., Granger, C.V., Simon,J.H., Alam, J.J., Bartoszak, D.M., Bourdette, D.N., Braiman, J.,Brownscheidle, C.M., Coats, M.E., Cohan, S.L., Dougherty, D.S.,Kinkel, R.P., Mass, M.K., Munschauer, F.E. 3rd, Priore, R.L., Pulli-cino, P.M., Scherokman, B.J., Whitham, R.H. et al., 1996. Intramus-cular interferon beta-1a for disease progression in relapsing multiplesclerosis. Ann. Neurol. 39, 285–294.
Jacobs, L., Munschauer, F., 1992. Treatment of multiple sclerosis withŽ .interferons. In: Rudick, R.A., Goodkin, D.E. Eds. , Treatment of
Multiple Sclerosis: Trial Design, Results and Future Perspectives.Springer-Verlag, London, pp. 233–250.
Leppert, D., Waubant, E., Burk, M.R., Oksenbert, J.R., Hauser, S.L.,1997. Interferon beta-1b inhibits gelatinase secretion and in vitromigration of human T cells: a possible mechanism for treatmentefficacy in multiple sclerosis. Ann. Neurol. 40, 846–852.
Link, H., Muller, R., 1971. Immunoglobulins in multiple sclerosis and¨infections of the nervous system. Arch. Neurol. 25, 326–344.
Link, H., Tibbling, G., 1977. Principles of albumin and IgG analyses inneurological disorders: III. Evaluation of IgG synthesis within thecentral nervous system in multiple sclerosis. Scand. J. Clin. Lab.Invest. 37, 397–401.
Liorente, L., Zou, W., Levy, Y., Richaud-Patin, Y., Wijdenes, J., Alco-cer-Varela, J., Morel-Fourrier, B., Brouet, J.C., Alarcon-Segovia, D.,Gelanaud, P., 1995. Role of interleukin 10 in the B lymphocytehyperactivity and autoantibody production of human systemic lupuserythematosus. J. Exp. Med. 181, 839–844.
Marcelletti, J.F., Katz, D.H., 1996. IL-10 stimulates murine antigen-drivenantibody responses in vitro by regulating helper cell subset participa-tion. Cell. Immunol. 167, 86–98.
w x wOlsson, T., 1994. Multiple sclerosis: cerebrospinal fluid Review 25x Ž .refs . Ann. Neurol. 36 Suppl. , S100–2.
Pirttila, T., Nurmikko, T., 1995. CSF oligoclonal bands, MRI, and thediagnosis of multiple sclerosis. Acta Neurol. Scand. 92, 468–471.
Rudick, R.A., French, C.A., Breton, D., Williams, G.W., 1989. Relativediagnostic value of cerebrospinal fluid kappa chains in MS: compari-son with other immunoglobulin tests. Neurology 39, 964–968.
Rudick, R.A., Ransohoff, R.M., Lee, J.-C., Peppler, R., Yu, M., Mathisen,P.M., Tuohy, V., 1998. In vivo effects of interferon beta-1a onimmunosuppressive cytokines in multiple sclerosis. Neurology 50,1294–1300.
Stanescu, G.L., Swick, A.R., Tuohy, V.K., Rudick, R.A., 1991. Sensitivecompetitive-binding ELISAs for quantifying free kappa and lambdalight chains in cerebrospinal fluid. J. Clin. Lab. Anal. 5, 206–211.
Stuve, O., Dooley, N.P., Uhm, J.H., Antel, J.P., Francis, G.S., Williams,G., Yong, W.V., 1997. Interferon-1b decreases the migration of Tlymphocytes in vitro: effects on matrix metalloproteinase-9. Ann.Neurol. 40, 853–863.
The IFNB Study Group, 1993. Interferon beta-1b is effective inrelapsing-remitting multiple sclerosis: I. Clinical results of a multicen-ter, randomized, double-blind, placebo-controlled trial. Neurology 43,655–661.
Tourtellotte, W.W., Baumhefner, R.W., Potvin, A.R., Ma, B.I., Potvin,J.H., Mendez, M., Syndulko, K., Mendez, M., 1980. Multiple sclero-sis de novo CNS IgG synthesis: effect of ACTH and corticosteroids.Neurology 30, 1155–1162.
Tripp, C.S., Wolf, S.F., Unanue, E.R., 1993. Interleukin 12 and tumornecrosis factor alpha are costimulators of interferon gamma produc-tion by natural killer cells in severe combined immunodeficiencymice with listeriosis, and interleukin 10 is a physiologic antagonist.Proc. Natl. Acad. Sci. 90, 3725–3729.