-
8/11/2019 Cerebral Palsy an Overview of the Disease and Its
Management
1/5
J.L. Pons et al. (Eds.): Converging Clinical & Engi.
Research on NR, BIOSYSROB 1, pp. 11171121.
DOI: 10.1007/978-3-642-34546-3_183 Springer-Verlag Berlin
Heidelberg 2013
Cerebral Palsy: An Overview of the Disease andIts Management
Ignacio Martnez Caballero1,4, Sergio Lerma Lara2,4,
and Maria Antonia Linares Lpez3,4
1Medical Coordinator of the Neuro-Orthopedic Unit,
Pediatric Orthopedic [email protected] in Charge
of the Motion Analysis Laboratory of the Neuro-Orthopedic Unit.
Pediatric [email protected]
3Chief of the Pediatric Rehabilitation Department
4
Hospital Infantil Nio Jess. Madrid. Spain
Abstract. How a neurologic disease affects to the muscles, bones
is introduced.
Classifications systems and treatments according functional
levels and ages are
already established. How to improve treatment outcomes is an
important task.
1 Introduction
Cerebral palsy is a static encephalopathy presented in a patient
with a growing
skeleton. Due to that, the orthopaedic symptoms are getting
worse until the
skeletal maturity.
Associated cognitive, sensorial and neurological problems are
common. [1] [2] [3].
The incidence of the disease, 2-3/1.000 new born babies, makes
necessary a
great effort of management. [3]
2 Pathogenesis
The upper motor neuron lesion creates spasticity, lack of
selective motor control
and the predominance of some agonists over their antagonists
produces joint
deformities.
Symptoms with excess of features, such us Hypertonia, Clonus or
Co-
contraction and others with deficit of them, like weakness or
poor balance, will
cause muscle, and joint problems. [1]The initially flexible
joint deformities will become rigid, because the muscle
shortening related to its lower growth speed compared to bone.
The growth
-
8/11/2019 Cerebral Palsy an Overview of the Disease and Its
Management
2/5
1118 I.M. Caballero, S.L. Lara, and M.A.L. Lpez
Fig. 1 Pathogenesis of musculo-skeletal problems according to
Bache
hormone increase the bone length and the lack of muscle stimulus
for growing,
like stretching, justify the lower muscle fiber length.
Weight bearing introduces Biomechanics in the skeletal
deformity
pathogenesis. Bone will grow guided partially by torque forces,
and together with
the ground reaction vectors axis deviations may appear. The
muscle will work
with inefficient lever arms around the joints because the bone
has bad transverse,
sagittal or frontal axis. This will lead to the bone lever arm
dysfunction that needsto be corrected. [2]
3 Classifications Systems
Topographic criteria are commonly used. Tetraplegic, triplegic,
diplegic, or
hemiplegic refers to the number or extremities affected, four,
three, two or one
respectively.
The motor control with will give us the movement disorders of
spasticity,
dystonia, mixed problems or less frequently ataxia and
athetosis, being the first thecommonest. Dystonia or extrapyramidal
diseases are the worse scenarios.
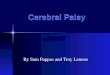
The functional classification based on functional walking
abilities, GMFCS
(Gross Motor Function System) with 5 levels, offers the
possibility of setting goal
treatments.
For GMCS Levels IV and V the spine and hips are clinically
followed from an
early age, because the greater incidence of scoliosis and hip
subluxation. These
will finally affect the body posture on a wheelchair. Functional
weight bearing can
be a goal in some of these patients. For Levels III and II, the
ability of walking
makes the gait disorders a priority of treatment.
-
8/11/2019 Cerebral Palsy an Overview of the Disease and Its
Management
3/5
Cerebral Palsy: An Overview of the Disease and Its Management
1119
6-12 Years 12-16 Years
Fig. 2 GMFCS functional Levels according to Palisano. [2]
[3]
4 Treatment
All the treatments are complementary. Physiotherapy, orthotics,
Botulinum Toxin
have the goal of improving the diminished joint range of motion
and used at the
beginning. The spasticity can be handle first globally with oral
drugs, with
Intrathecal Baclofen or Dorsal Rhizotomy, and ideally would
cause a positive
effect preventing orthopedic deformities. However the patients
still need
orthopedic surgery after the general spasticity treatment.
The frequency of type of treatment is different according the
age of the patient.
[1].
Fig. 3Frequency of type of treatment related to age. (From Bache
and Graham).
A good treatment guide, according GMFCS levels and ages has
been
established in recent literature. [3]
Level I
Level II
Level III
Level IV
Level V
-
8/11/2019 Cerebral Palsy an Overview of the Disease and Its
Management
4/5
1120 I.M. Caballero, S.L. Lara, and M.A.L. Lpez
Fig. 3Treatment according ages and Functional GMFCS Level. Each
color is a different
type of treatment. The hexagon represent the time for orthopedic
surgery. In levels V, IV,
III appears sooner because the possible need of profilactic hip
subluxation surgery. (From
the Updated European consensus in Botulinum Toxin Therapy
2009).
Despite the lack of studies, according the medicine based on
evidence criteria,
some therapies such us Bobath, Vjta o Therasuit, still claim to
have a role in the
general management. Better design studies will clarify this
point.
A realistic goal, the patient selection, and an adequate
surgical plan are basic
conditions for reaching a successful treatment. For better
treatment decisions therole of motion analysis laboratories has
been extensively debated. [2]
Fig. 4 The evaluation process for orthopedic surgery includes
clinical and functional
evaluation, radiology and motion laboratory studies. FMS and FAQ
are functional scales.
(From Young and Graham)
LermaLara,S.PT,MSc.
NEURO-ORTOPEDIA INFANTIL
-
8/11/2019 Cerebral Palsy an Overview of the Disease and Its
Management
5/5
Cerebral Palsy: An Overview of the Disease and Its Management
1121
Observational gait studies are not enough for quantifying and
detect deeply the
disorders that occur while we walk.
This tool has showed the ability of changing surgical planning
and even
reducing costs related. [6]
For pre-treatment evaluation, some scales like the FMS
(Functional Mobility
Scale) or the FAQ (Functional Ambulatory Questionnaire) offer a
reference. [2][4] [5]
The long recovery period needs a close follow up, checking
physiotherapy, the
orthotic devices and even taking care of psychological aspects.
The Single Event
Multilevel Surgery achieves the best of the lower limb alignment
in the sagittal,
transversal and frontal planes, but this is not always enough
for cerebral palsy
patients. The trunk position, and muscle strength remains
challenging in some of
them.
5 Conclusions
A road map of treatment is already set for cerebral palsy
patients following
Functional Levels and ages. However improving outcomes is a
necessary task for
all of us.
References
[1]
Bache, C., Selber, P., Graham, H.K.: Themanagement of
spasticdiplegia. CurrentOrthopaedics 17, 88104 (2003)
[2] Gage, S., Koop, N.: The Identification and Treatment of Gait
Problems in Cerebral
Palsy, 3rd edn. Mc Keith University Press (2009)
[3] Heinen, F., et al.: The updated European consensus 2009 on
the use of Botulinum
Toxin for children with cerebral palsy. Eur. J. Paediatric
Neurol. 14(1), 4566 (2010)
[4] Young, J.L., et al.: Management of the Knee in Spastic
diplegia: What is the dose?
Orthop. Clin. North Am. 41, 561577 (2010)
[5] Freeman, M.: Physical Therapy in Cerebral Palsy. Springer
(2005)
[6] Wren, T.: The effect of preoperative gait analysis on costs
and amount of surgery. J.
Pediatr. Orthop. 29(6), 558563 (2009)