-
8/12/2019 Ceramic Materials in Dentistry
1/13
Australian Dental Journal 2011; 56:(1 Suppl): 8496
doi: 10.1111/j.1834-7819.2010.01299.x
Ceramic materials in dentistry: historical evolution andcurrent
practice
JR Kelly,* P Benetti*University of Connecticut Health Center,
Department of Reconstructive Sciences, Farmington, Connecticut,
USA.Sa o Paulo State University, Department of Dental Materials and
Prosthodontics, Sa o Jose dos Campos, Sa o Paulo, Brazil.
ABSTRACT
Dental ceramics are presented within a simplifying framework
allowing for facile understanding of their development,composition
and indications. Engineering assessments of clinical function are
dealt with and literature is reviewed on theclinical behaviour of
all-ceramic systems. Practical aspects are presented regarding the
choice and use of dental ceramics tomaximize aesthetics and
durability, emphasizing what we know and how we know it.
Keywords: Ceramics, particle-filled glasses, polycrystalline
ceramics, CAD CAM, all-ceramic restorations.
Abbreviation: LTD = low temperature degradation.
CERAMICS IN DENTISTRY WHERE DID THIS STUFFCOME FROM?
It is quite useful reviewing how and why ceramics cameto be used
in dentistry. This account serves threepurposes: (1) to alert
practitioners to the fact that theuse of ceramics, since the very
beginning, alwaysrepresented the adoption of high technology
versuscraft art; (2) to reinforce the concept that ceramics
andimproved ceramics were introduced in order to solvespecic
problems or to increase restorative versatility;and (3) to provide
a gentle background into the natureand science of ceramics. Astute
readers are alsoprovided with clues as to where to watch for
theemergence of new ceramic technologies.
Since a distinction was drawn between high tech-nology and craft
art it is useful to provide some basicdening characteristics of
each. Many would agree thathigh technology should include: (1)
dentistry borrow-ing materials processes shortly after their being
devel-oped by an unrelated industry; (2) incorporation of
newlearning from recent scientic literature outside of dental
medicine; and (3) the spread of outright newinventions within
dentistry. Craft art, on the otherhand, brings to mind materials
and techniques bor-rowed from those involved in jewellery making,
the artsand the manufacture of everyday goods. All audiencesthe
senior author has spoken to before have chosen
craft art as the likely source of ceramics introducedinto
dentistry at any stage of development.
In the early 1700s many European rulers were
spending enormous sums importing porcelain fromChina and Japan.
Figure 1, from Schloss Charlotten-burg in Berlin, is representative
of just small portions of one of these collections. The collection
of Augustus IIIof Saxony was perhaps the largest and is now
ondisplay at the Zwinger Museum in Dresden, his formerpalace. Such
activity led China to be characterized asbeing the bleeding bowl of
Europe. Between 1604 and1657 alone, over three million pieces of
Chineseporcelain reached Europe. 1 In 1700, East Indiamenships
unloaded 146 748 pieces in a European port injust one day as the
market for porcelain grew insatia-ble. 1
One response to this situation involved state spon-sored
research into porcelain discovery. NotableEuropean leaders
including Augustus (III) the Strong,King of Poland and Elector of
Saxony along with theMedici family of Florence, Italy were
independentlysponsoring research into the development of a
Euro-pean porcelain to match the hard, translucent andsonorous
material developed in eastern Asia nearly1100 years earlier.
Europeans strived at porcelaindiscovery without much success for
about 200 yearsand this activity is credited with being largely
respon-sible for the growth of modern analytical chemistry
84 2011 Australian Dental Association
Australian Dental JournalThe ofcial journal of the Australian
Dental Association
-
8/12/2019 Ceramic Materials in Dentistry
2/13
from its roots in alchemy. An historical timeline of porcelain
discovery appears as Fig 2.
During the late 1600s and early 1700s the rstexamples of state
sponsored research were beinginitiated in France and the Germanic
state of Saxony.One example that becomes important for
dentistry
involves the efforts of Count Walther Von Tschirnhausin
developing the mineral resources of Saxony on behalf of Augustus
III. One method Von Tschirnhaus usedinvolved subjecting minerals to
extensively high tem-peratures (easily in excess of 1436 C)2
produced in thefocal spot of a series of large burning lenses
(magni-fying glasses up to one metre in diameter), creating asolar
furnace. About this time in Berlin (Germanic stateof Prussia),
Johann Friedrich Bo ttger was reaching thelevel of journeyman
apothecary. Bo ttger had a cuteparlour trick involving melting base
metals such assilver coins to which he added a dose of the Arcanum
of
the philosophers stone.3
When poured into moulds and
cooled, the resulting product was analysed to be puregold! Bo
ttger inadvisably performed this transmuta-tion demonstration at
his employers house to impresssome important guests that resulted
in a summons byKing Frederich I (Prussian king) for a
commandperformance. Placing discretion ahead of valour ledBo ttger
to ee south to Saxony where he attempted tostudy medicine at
Wittenberg. Wanted posters hadappeared in Berlin and a price was on
the head of Bo ttger. The arrival of a contingent of a dozen
troopsfrom King Frederich seemed out of proportion, to thelocal
Wittenberg representative of Agustus III, for thecapture and return
of a supposedly common criminal.Bo ttger was placed under house
arrest for months whileAugustus was alerted and the situation
explored. Withthe presence of foreign troops confounding the
situa-tion, Bo ttger was nally spirited away by coach in thedead of
night using back roads to avoid Prussian troopsand delivered to
Augustus in Dresden. The Prussianswere additionally deceived as the
Saxons continued tobring food to the room of Bo ttger. This
base-metals-to-
gold thing was simply far too important to any stateneeding to
support armies, and Bo ttger was put as aprisoner under the wing of
Von Tschirnhaus to perfectgold production.
Serendipity and a clever intuition prevailed to saveBo ttger
from certain execution following over threeyears of unsuccessful
gold making, a project costingAugustus a small fortune.
Experimenting with hisburning lenses, Von Tschirnhaus discovered
that whileneither sand nor lime (calcium oxide) would
fuseindividually, they would do so when combined, andpresented this
at a meeting of the Academy of Sciences
of Paris in 1799.2
In fact, the resulting white product
Fig 1. Schloss Charlottenburg in Berlin is representative of
just small portions of one of the extensive porcelain collections
popular with Europeanroyalty.
Fig 2. Timeline of porcelain development from ancient China
tomodern formulations.
2011 Australian Dental Association 85
Ceramic materials in dentistry
-
8/12/2019 Ceramic Materials in Dentistry
3/13
looked suspiciously like porcelain. What had beendiscovered was
the use of a ux to create lowermelting intermediate compounds,
allowing the fusionof the high-silica sand. Since it was known that
highquality clay was a major ingredient in Chinese porce-lain,
Saxony was secretly scoured for sources of purestclay. Bo ttger,
whose expertise in chemistry was by thenextensive, realized that
porcelain had to have a glassycomponent resulting from very high
temperature reac-tions. Building on the discovery of Von
Tschirnhaus, hereasoned that lime added to clay was worth
exploring.
Research was conducted under extreme secrecybeginning in the
Albrechtsburg Castle in Meissen(modern photograph in Fig 3) and
then in the dungeonbasement of the feared Jungfernbastei (Maidens
Bas-
tion) in Dresden between 1704 and 1708, utilizing anapproach
known today as Edisonian research, where awide variety of
formulations were systematically tried.Pages from his lab notebook
memorializing the suc-cessful mixture of clay and lime (calcined
alabaster;pulverized and heated to drive-off water and
sulfurleaving fine calcium oxide powder) appear in Fig
4.Manufacturing operations were established back in
theAlbrechtsburg Castle in Meissen and by 1708 the firstpieces were
being demonstrated at the Leipzig EasterFair with production for
sale beginning in 1710. Inabout 1710 Bo ttger substituted feldspar
for lime as theflux, a move that cleanly put the Meissen
formulationwithin that of the Chinese triaxial porcelains (Fig
5)and introduced feldspathic glass which will later
Fig 4. Page from laboratory notebook of Bo ttger memorializing
the successful mixture of clay and calcined alabaster in January
1708. Earlydepiction of the feared Jungfernbastei (Maidens Bastion)
in Dresden, site of secret porcelain discovery research.
Fig 3. Albrechtburg Castle in Meissen, Germany, site of an early
porcelain discovery laboratory and the rst manufacturing site of
Europeanporcelain rivalling that from China.
86 2011 Australian Dental Association
JR Kelly and P Benetti
-
8/12/2019 Ceramic Materials in Dentistry
4/13
become the main ingredient in aesthetic porcelainformulations
for dentistry. This high temperaturereaction of the kaolin-type
clay (essentially heavilyweathered granite or feldspathic rock) and
feldsparyielded a high silica glass containing needle-like
crystalsof mullite. 2
Although Saxony tried to maintain a monopoly onporcelain making,
the secret escaped via a combinationof its role in state prestige,
industrial espionage andgreed within the Meissen porcelain works.
By 1776,porcelain making was the topic of a review paper givenat
the Academy of Sciences in Paris. In 1770 anotherapothecary, Alexis
Duchateau, tired of his stained andmalodorous dentures, sought
assistance from Parisiandentist Nicholas Dubois de Che mant.
Working withporcelain formulations and (then) high technology
kilnsof the Guehard Porcelain Factory, they succeeded by1774 in
fabricating a complete denture for Duchateau.Porcelain dentures
represented a huge step forward inpersonal hygiene, leading public
honours for de Che -mant from the likes of Edward Jenner
(smallpoxvaccine), the Academy of Sciences and the Academyof
Medicine of Paris University. Since porcelain was anew invention in
Europe and only available in collab-oration with a high technology
company from the
very beginning its use in dentistry was certainly notcraft
art.
de Che mant ed to England ahead of the FrenchRevolution where he
rened formulations in collabo-ration with Josiah Wedgewood at the
beginning of hisfamous manufacturing company. de Che mant
presum-ably worked to improve translucency moving from thecentre of
the ternary (three-part) phase diagramtowards a feldspar-rich
formulation, characteristic of todays feldspathic materials (Fig
5).
In 1808 another Parisian dentist, GiuseppangeloFonzi,
signicantly improved the versatility of ceramics
by ring individual denture teeth, each containing a
platinum pin. This invention allowed teeth to be xedto metal
frameworks enabling: (1) partial denturefabrication; (2)
repairability; and (3) increased aesthet-ics. Platinum had only
been known to Europeans sincearound 1741 and given its extremely
high melting point(1769 C) was generally only worked into small
wiresand crucibles by hammering individual red-hot nuggets.Platinum
was not used in jewellery until 1915. 4 In 1808platinum was used by
alchemists in early chemistryexperimentation, so it is likely that
Fonzi obtainedplatinum wire from a local university or an
earlyscientic supply house. It was also the only metal thatwould
not crack the denture tooth on cooling given itsclosely matched
coefcient of thermal contraction.Again, this next major improvement
in our abilityto use ceramics in dentistry clearly stands as
hightechnology.
Leucite ller crystals in porcelain metal-ceramicsystems and
strengthened pressable ceramics
Many other advances contributed to both the use of ceramics and
the discipline of xed prosthodontics,including: (1) the electric
porcelain furnace; (2)elastomeric impression materials; and (3) the
high-speed handpiece. One major advance in porcelainitself came in
1962 with the development of aformulation that could be red on
common dentalcasting alloys. This invention built on a
paperpublished in the Journal of the American CeramicsSociety
(JACS) demonstrating an oddity in the thermalexpansion of a certain
feldspar rock (with a potassiumcontent over 11%) when melted and
cooled quickly,forming a glass. 5 When reheated, this glass had
anextremely high thermal expansion due to the forma-tion of a new
crystalline component not in the originalrock, called leucite
(formed as the rock melted by aprocess known as incongruent
melting). Weinsteinet al ., again using the Edisonian research
technique(and hiring co-author Koenig of the JACS paper as
aconsultant), finally arrived at what they called com-ponent number
1 a porcelain frit that had a thermalexpansion coefficient of
nearly 20 10 ) 6 C, allowing
it to be mixed in any ratio with the normal expansionporcelain
frit (thermal expansion of 8 10 ) 6 C) todial in an expansion
contraction to match any dentalalloy. 6 So this represents an
invention built on a paperpublished in a scientic journal outside
of dentistry,and therefore again, high technology.
Most dental alloys having expansions in the range of 12 to 14 (
10) 6 C); their matching porcelains haveleucite contents around 17
to 25 mass%. Manufactur-ers have found that having the porcelain
with a slightlyhigher expansion contraction than the metal makes
formore durable restorations, presumably by leaving theporcelain in
a state of slight tangential compression.
Fig 5. Tertiary phase diagram of quartz (sand), clay and
feldspar.Dental formulations began in middle of diagram and evolved
towardsfeldspar-rich compositions to improve aesthetics. In Chinese
formu-
lations feldspar was the ux.
2011 Australian Dental Association 87
Ceramic materials in dentistry
-
8/12/2019 Ceramic Materials in Dentistry
5/13
Leucite was later used for dispersion strengthening at35 to 50
mass% in both powdered ceramics and later inthe rst pressed
ceramics. Leucite was a good choice asa strengthening ller since
its index of refraction is closeto that of the feldspathic glass,
so moderate strength-ening could be achieved without severely
increasingopacity. These compositions are also easily etched
tocreate micromechanical features for resin bonding. All-ceramic
systems based on leucite-lled feldspathicglasses remain some of the
most aesthetic and populardental ceramics, and have been
extensively studiedclinically and found to be highly reliable. 7
The use of afeldspathic glass dates back to Bo ttger in 1710.
Itbecame the major component of dental formulationswith the work of
de Che mant in England in the early1800s and a special property of
high potassiumfeldspars was taken advantage of in 1962, leading
tothe vast majority of aesthetic dental ceramics in use
today, either metal-ceramic or all-ceramic.
Non-shrinking ceramics
Except for pressing ingots, by the mid 1980s all dentalceramic
parts started as powders or mixtures of clayand power particles.
Shrinkage is inherent to themaking of parts from such starting
materials sincethe volume fraction of porosity is over 30% in
thestarting greenware and nearly 0% in the nishedproduct. Seven
different approaches were developedbeginning in the mid 1980s
through to the late 1990s todeal with or avoid shrinkage to provide
prostheses thatwere, what an engineer would call, being made to a
netshape: (1) a pressed ceramic powder polymeric binderthat
expanded and crystallized during ring to ll alost-wax mould
(Cerestore; Johnson & Johnson, NewBrunswick, NJ, USA); 8,9 (2)
casting of a special glassinto a lost-wax mould, embedding the
clear-glasscasting in an investment and heat-treating to
formcrystals within the glass (termed a glass ceramic, tradenamed
DICOR; Dentsply International, York, PA,USA); (3) lightly sintering
aluminum oxide (and latermagnesium aluminate spinel and zirconia
alumina) toform necks between touching particles and then inl-
trating this porous ceramic with glass (In-Ceram;
VitaZahnfabrik, Bad Sa ckingen, Germany); 10 (4) pressingsolid
ingots of lled-glass (leucite or lithium disilicate)into a lost-wax
mould (Empress; Ivoclar Vivadent,Schaan, Liechtenstein); 11 (5)
computer-aided machin-ing of net-shape parts from solid, full-dense
blocks(CEREC; Sirona, Bensheim, Germany); 12 (6) computer-aided
fabrication of an oversized die, pressing of alumina powder onto
the die creating an oversizedpart and sintering to nal size
(Procera; Nobel Biocare,Zu rich, Switzerland); 13 and (7)
computer-aidedmachining of oversized parts from lightly
sinteredblocks of zirconia and alumina which are then sintered
to nal size (Cercon, Lava, Vita YZ, Ivoclar e.maxzirCAD). 14
Approach number (1) provided the rst introductionof advanced
ceramics processing equipment into thedental laboratory and
approach (2) introduced glassceramics into dentistry; where
strengthening llerparticles are grown inside of the glass from
thechemistry of the glass (during a special heat treatmentcalled
ceramming) as opposed to being added asseparate powder particles.
Both of these involvedcollaborations with specialty ceramics rms,
CoorsCeramics for (1) and Corning Glass Works for (2).
Chairside CAD CAM
While all seven approaches stand clearly as being
hightechnology, numbers (5) and (7) can be viewed as
beingrevolutionary. In 1987, Mo rmann and Brandestini 12
introduced a prototype machine that would capture a3-D image of
a prepared tooth. They used 3-D designsoftware to iteratively
develop a proposed restorationand then directed the computer-aided
milling of inlaysand onlays from solid blocks of aesthetic,
lled-glass(see next section) ceramics (CEREC I, then SiemensDental
now Sirona, Bensheim, Germany). Machining of aesthetic glass-based
ceramics is relatively straight-forward and special formulations
were quickly devel-oped that were much higher quality than what
wasavailable from dental laboratory processing based oneither
strengthened and ne grained feldspathic ceram-ics (Mark II, Vita)
or the rst glass-ceramic introducedfor dental use (containing
interlocking tetrasilisicuoromica akes, DICOR-MGC, Dentsply
Interna-tional).
Green machining of oversized parts
Machining of tougher structural ceramics such asalumina and
especially transformation toughened zirco-nia (see following
section) was much more difcult,requiring heavier machinery, longer
milling times andquite often involved limited tool life. Further
advances inthe manipulation of 3-D data sets along with the fruits
of
a decade of research into ceramics processing providedthe
underpinning for an innovative solution proposed byFilser and
Gauckler at the University of Zu rich. Thisinvolved machining of an
oversized part from a ceramicblock only lightly sintered to what is
termed the initialsintering stage. 1517 With very careful control
over boththe ceramicpowder particle size distribution
andparticlepacking density, it became possible to predict
theoversized shape needed that would then shrink to thedesired net
shape. This technique has been variouslytermed green machining or
soft machining in dentalliterature. This technique allowed the
individually cus-tomized and high tolerance parts dentistry
requires to be
88 2011 Australian Dental Association
JR Kelly and P Benetti
-
8/12/2019 Ceramic Materials in Dentistry
6/13
manufactured from polycrystalline ceramics such asalumina and
zirconia.
As of today, the last major advance in dental ceramicscomes with
the introduction of transformation tough-ened zirconia. 1719 This
ceramic is arguably the mostcomplex material ever introduced for
dental use and, aswill be discussed later, its introduction has not
beenwithout a learningcurve that we are still climbing. Twoother
major changes currently underway involve: (1) theestablishment of
dedicated industrial-quality manufac-turing centres for fabrication
of prostheses; and (2) theapplication of engineering design
research into clinicaland laboratory practices to optimize
durability andaesthetics. Fruits of this second activity will be
discussedin the last section of this paper.
BACKGROUND CONCEPTS IN CERAMICS SCIENCE
There are two quite useful concepts that help demystifydental
ceramics by providing a structure within whichto organize thinking.
First, there are only three mainclasses of dental ceramics: (1)
predominantly glassymaterials; (2) particle-lled glasses; and (3)
polycrys-talline ceramics. 6,20,21 Dening characteristics will
beprovided for each of these ceramic types as they arerepresented
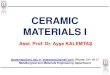
in Fig 6. Second, virtually any ceramicwithin this spectrum can be
considered as being acomposite, meaning a composition of two or
moredistinct entities. Quite a number of seemingly differentdental
ceramics can be shown to be quite similar orclosely related to each
other when reviewed within theframework these two simplifying
concepts provide.Additionally, the rationale behind the development
of ceramics of both historic and recent interest can bemore easily
understood. Two examples of the utility of these concepts include
these basic statements: (1) highlyaesthetic dental ceramics are
predominantly glassy andhigher strength substructure ceramics are
generallycrystalline; and (2) the history of development of
substructure ceramics simply involves an increase incrystalline
content to fully polycrystalline. Figures 7aand 7b provide basic
composition details and commer-cial examples of many aesthetic and
substructure dentalceramics organized by these three main divisions
usingthe composite concept (based on matrix and ller).
Predominantly glassy ceramics
Dental ceramics that best mimic the optical properties of enamel
and dentine are predominantly glassy materials.Glasses are 3-D
networks of atoms having no regularpattern to the spacing (distance
and angle) betweennearest or next nearest neighbours, thus their
structure isamorphous or without form. Glasses in dental ceram-ics
derive principally from a group of mined mineralscalled feldspar
and are based on silica (silicon oxide) andalumina (aluminum
oxide), hence feldspathic porcelains
belong to a family called aluminosilicate glasses.21
Glasses based on feldspar are resistant to
crystallization(devitrication) during ring, have long ring
ranges(resist slumping if temperatures rise above optimal) andare
extremely biocompatible. In feldspathic glasses, the3-D network of
bridges formed by silicon-oxygen-silicon bonds is broken up
occasionally by modifyingcations such as sodium and potassium that
providecharge balance to non-bridging oxygen atoms (Fig
8).Modifying cations alter important properties of theglass, e.g.
by lowering ring temperatures or increasingthermal expansion
contraction behaviour.
Particle-lled glasses
Filler particles are added to the base glass compositionin order
to improve mechanical properties and tocontrol optical effects such
as opalescence, colour andopacity. These llers are usually
crystalline but can alsobe particles of a higher melting glass.
Such composi-tions based on two or more distinct entities (phases)
areformally known as composites, a term often reservedin dentistry
to mean resin-based composites. Thinkingabout dental ceramics as
being composites is a helpfuland valid simplifying concept. Much
confusion is
cleared up in organizing ceramics by the ller particlesthey
contain (and how much), why the particles wereadded, and how they
got into the glass.
The rst llers to be used in dental ceramicscontained particles
of a crystalline mineral calledleucite. 20,21 As mentioned in the
history section above,this ller was added to create porcelains that
could besuccessfully red onto metal substructures. 22,23 Leucitehas
a very high thermal expansion contraction coef-cient (around 20 10
) 6 C) compared to feldspathicglasses (around 8 10 ) 6 C). Dental
alloys haveexpansion contraction coefcients around 12 to 14( 10 ) 6
C). Adding about 17 to 25 mass% leucite ller
Fig 6. Based on their microstructure, dental ceramics fall
within threebasic classes: (1) predominantly glass; (2)
particle-lled glass; and (3)fully polycrystalline. Each of these is
discussed in detail in the text.
2011 Australian Dental Association 89
Ceramic materials in dentistry
-
8/12/2019 Ceramic Materials in Dentistry
7/13
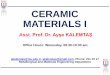
Fig 8. In feldspathic glasses, the 3-D network of bridges formed
by silicon-oxygen-silicon bonds is broken up occasionally by
modifying cations suchas sodium and potassium that provide charge
balance to non-bridging oxygen atoms.
(a)
(b)
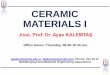
Fig 7. Composition of dental ceramics based on their being
composites consisting of a matrix and llers; (a) veneering
ceramics; (b) structural andCAD CAM ceramics.
90 2011 Australian Dental Association
JR Kelly and P Benetti
-
8/12/2019 Ceramic Materials in Dentistry
8/13
to the base dental glass create porcelains that arethermally
compatible during ring with dental alloys.Metal-ceramic systems,
rst developed in 1962, areused to fabricate 70 to 80% of xed
prostheses.
Moderate strength increases can also be achieved withappropriate
llers added and uniformly dispersedthroughout the glass, a
phenomenon termed dispersionstrengthening. The rst successful
strengthened sub-structureceramicwasmadeof feldspathicglasslled
withparticles of aluminum oxide (app. 55 mass%). 23
Leuciteisalsousedfordispersionstrengtheningatconcentrationsof
around 40 to 55 mass%, much higher than needed formetal-ceramics.
Commercial ceramics incorporating leu-cite llers for strengthening
include a group that arepressed into moulds at high temperature
(OPC, Pentron;Empress Esthetic, Ivoclar Vivadent and Finesse
All-Ceramic, Dentsply Prosthetics) and a group provided asa powder
for traditional porcelain build-up (OPC Plus,
Pentron; Fortress, Mirage Dental Systems).Beyond thermal
expansion contraction behaviour,there are two major benets to
leucite as a ller choicefor dental ceramics; the rst intended and
the secondprobably serendipitous. First, leucitewas
chosenbecauseits index of refraction is very close to that of
feldspathicglasses; an important match for maintaining
sometranslucency. Second, leucite etches at a much faster ratethan
the base glass and it is this selective etching thatcreates a
myriad of tiny features for resin cements toenter, creating a good
micromechanical bond.
Glass-ceramics (special subset of particle-lled
glasses)Crystalline ller particles can be added mechanically tothe
glass, e.g. by simply mixing together crystalline andglass powders
prior to ring. In a more recent approach,the ller particles are
grown inside the glass object(prosthesis or pellet for pressing
into a mould) after theobject has been formed. After forming, the
glass object isgiven a special heat treatment, causing the
precipitationand growth of crystallites within the glass. Since
thesellers are derived chemically from atoms of the glassitself, it
stands to reason that the composition of theremaining glass is
altered as well during this process
(termed ceraming). Such particle-lled composites arecalled
glass-ceramics. The material Dicor (Dentsply), therst commercial
glass-ceramic available for xed pros-theses, contained ller
particles of a type of crystallinemica (at app. 55 vol%). 24 More
recently, a glass-ceramiccontaining70 vol% crystalline lithium
disilicateller hasbeen commercialized for dental use (Empress 2,
nowe.maxPress and e.maxCAD, Ivoclar-Vivadent).
Polycrystalline ceramics
Polycrystalline ceramics have no glassy components; allof the
atoms are densely packed into regular arrays that
are much more difcult to drive a crack through thanatoms in the
less dense and irregular network found inglasses. Hence,
polycrystalline ceramics are generallymuch tougher and stronger
than glassy ceramics.Polycrystalline ceramics are more difcult to
processinto complex shapes (e.g. a prosthesis) than are
glassyceramics. Well-tting prostheses made from polycrys-talline
ceramics were not practical prior to the avail-ability of
computer-aided manufacturing. In general,these computer-aided
systems use a 3-D data setrepresenting either the prepared tooth or
a wax modelof the desired substructure. This 3-D data set is used
tocreate either an enlarged die upon which ceramicpowder is packed
(Procera, NobelBiocare, Zurich,Switzerland) or to machine an
oversized part for ringby machining blocks of partially red ceramic
powder(Cercon, Dentsply Prosthetics; Lava, 3M-ESPE; Y-Z,Vita
Zahnfabrik). Both of these approaches rely upon
well-characterized ceramic powders for which ringshrinkages can
be predicted accurately. 13,14
Polycrystalline ceramics tend to be relatively opaquecompared to
glassy ceramics, thus these stronger mate-rials cannot be used for
the whole wall thickness inaesthetic areas of prostheses. These
higher strengthceramics serve as substructure materials upon
whichglassy ceramics are veneered to achieve pleasing aesthet-ics.
Laboratory measures of the relative translucency of commercial
substructure ceramics areavailable, both fora single-layer of
materials and for those that areveneered. 25,26 It should be noted,
however, that whilelaboratory measures of opacity have equated
somepolycrystalline ceramics to cast alloys, all ceramic
sub-structures transmit some light and metals simply do not.
Substructure ceramics
The development of higher strength ceramics for ve-neered
all-ceramic prostheses can be represented as atransition towards
increases in the volume percentage of crystalline material with
decreasingly less glass andnally, no glass. In 1965, John McLean
reported on thestrengthening of a feldspathic glass via addition of
aluminum oxide particles, 23 the same year that General
Electric rst applied that new technology
(dispersionstrengthening of glasses) to high-tension power
lineinsulators. In the late 1980s, a method was realized
tosignicantly increase the aluminum oxide content (fromapp. 55
mass% to 70 vol%) by rst lightly ring packedalumina powder and then
inltrating the still porousalumina compact with glass. 11 During
the rst lightring, adjacent alumina particles become bonded
wherethey touch, forming a 3-D network of linked
particles.Inltration involves a low viscosity glass drawn into
theporous alumina network by capillary pressure, thusforming an
interpenetrating 3-D composite (both thealumina and glass being
continuous throughout the
2011 Australian Dental Association 91
Ceramic materials in dentistry
-
8/12/2019 Ceramic Materials in Dentistry
9/13
ceramic, neither representing an isolated ller).Although with
only 70 vol% aluminum oxide, thisceramic (In-Ceram Alumina, Vita)
has a strength andfracture toughness identical to many 100%
polycrystal-line alumina ceramics.
Two key developments allowed fully polycrystallineceramics to
become practical for xed prostheses: (1) theavailability of highly
controlled starting powders; and(2) the application of computers to
ceramics processing.Unlike glassy ceramics, polycrystalline
ceramics cannotbe simply pressed as a fully dense material into
slightlyoversized moulds (moulds that have expanded justenough to
compensate for cooling shrinkage as is donein the casting of
metals). Polycrystalline ceramics areformed from powders that can
only be packed to around70% of their theoretical density. Hence
polycrystallineceramics shrink around 30% by volume (10%
linear)when made fully dense during ring. In order for the
nal prostheses to t well, the amount of shrinkageneeds to be
accurately predicted and compensated for.Well-characterized
starting powders that can be uni-formly packed are a prerequisite
for achieving predict-able and reproducible shrinkage. Research in
ceramicsprocessing science from the late 1980s through to the1990s
led to the commercial availability of powderssuitable for dental
use. Almost simultaneously with hightechnology powder renement came
the development of computer-aided machining and the ability to
captureand manipulate 3-D data sets.
Two different approaches are now being offeredcommercially for
fabrication of prostheses from poly-crystalline ceramics, both of
which create oversizedgreenware (unred part) using 3-D data sets
and thespecic shrinkage characteristics of well-behaved start-ing
powders. In the rst approach, an oversized die ismanufactured based
on app. 20 000 measurementstaken during the mechanical scanning of
a laboratorydie. Either aluminum oxide or zirconium oxide ispressed
onto the oversized die and predictably shrunkduring ring to become
well-tting single-crown sub-structures (Procera, Nobel Biocare). 13
In the secondapproach, blocks of partially red (app. 10%
complete)zirconium oxide are machined into oversized greenware
for ring as single- and multiple-unit prosthesissubstructures
(Cercon, Dentsply Prosthetics; Lava,3M-ESPE; Y-Z, Vita; e.max
ZirCAD, Ivoclar). In thesesystems, individual blocks are bar coded
with the actualdensity of each block (for the ne-tuning of
shrinkagecalculations) and the milling machines can keep trackof
the number of blocks milled and automaticallychange milling tools
to further assure accuracy of t. 14
Transformation toughened zirconium oxide
Potentially the most interesting polycrystalline ceramicnow
available for dentistry, transformation toughened
zirconia, needs further explanation since its fracturetoughness
(and hence strength) involves an additionalmechanism not found in
other polycrystalline ceramics.While fracture toughness and
strength are outside thescope of this paper, it is sufcient here to
understandtoughness simply as meaning the difculty in driving
acrack through a material.
Unlike alumina, zirconium oxide is transformed fromone
crystalline state to another during ring. At ringtemperature,
zirconia is tetragonal and at room tem-perature monoclinic, with a
unit cell of monoclinicoccupying about 4.4% more volume than when
tetra-gonal. Unchecked, this transformation was a bit unfor-tunate
since it would lead to crumbling of the materialon cooling. In the
late 1980s, ceramic engineers learnedto stabilize the tetragonal
form at room temperature byadding small amounts (app. 38 mass%) of
calciumand later yttrium or cerium. 18 Although stabilized at
room temperature, the tetragonal form is really onlymetastable,
meaning that trapped energy still existswithin the material to
drive it back to the monoclinicstate. It turned out that the highly
localized stress aheadof a propagating crack is sufcient to trigger
grains of ceramic to transform in the vicinity of that crack tip.
Inthis case, the 4.4% volume increase becomes benecial,essentially
altering material conditions around thecrack tip, shielding it from
the outside world (moreformally stated, transformation decreases
the localstress intensity).
Although most dental zirconia is a bit opaque andcopings need to
be veneered for high aesthetics, theseprostheses can be quite
lifelike. Zirconia is not asopaque as In-Ceram alumina and can be
internallycoloured as can lithium disilicate. Figure 9 is a
clinicalcase involving both central incisors where zirconia
waschosen over crowns done in three other systems by thesame
technician (In-Ceram alumina, Vita; e.maxCAD,Ivoclar; Captek,
Precious Chemicals Company, Alta-monte Springs, FL, USA).
With fracture toughness twice or more that of alumina ceramics,
transformation toughened zirconiarepresents an exciting potential
substructure material.Possible problems with these zirconia
ceramics may
involve long-term instability in the presence of water,porcelain
compatibility issues, and some limitations incase selection due to
their opacity. However, as of writing this, three-year clinical
data involving manyposterior single-unit and three-unit prostheses
(plus 1ve-unit) have revealed no major problems (discussedmore
fully below).
Zirconia substructures issues
Two issues are of concern with zirconia, one quite realand one
potential. Of real concern are reports of signicant percentages of
single-unit and multi-unit
92 2011 Australian Dental Association
JR Kelly and P Benetti
-
8/12/2019 Ceramic Materials in Dentistry
10/13
prostheses having porcelain chipping and cracking (e.g.25 to
50%). 17 Of potential concern is the propensity
forpartially-stabilized zirconia to auto-catalytically trans-form
at surface grain boundaries due to an interactionwith water. This
may create major structural issues inthe future.
Many authorities have offered numerous explana-tions for
porcelain chipping that simply do notwithstand critical thinking or
analysis, including: (1)non-anatomic substructure design; (2)
unsupportedporcelain; (3) weaker porcelain; (4) thermal expan-sion
contraction mismatches; and (5) poor porcelain-zirconia bonding.
More well-considered hypotheseshave included: (1) residual stresses
arising fromthermo-mechanical parameters; 27 (2)
auto-catalytictransformation during porcelain ring; 28 and
(3)enhanced auto-catalytic transformation of green-machined
structures at mouth temperature. 29 As yetunpublished research from
three different sourcesstrongly supports residual stresses within
the porcelain
developing as a result of too rapid cooling: (1)fractographic
evidence for a crack originating 0.5 mmbelow the porcelain surface
(Susanne Scherrer, Univer-sity of Geneva); (2) optical
interferometer measures of residual stress in fast-cooled versus
slow-cooled zirco-nia crowns (Drs Norbert Thiel and Michael
Tholey,Vita, with collaborators at the Fraunhofer Institute);and
(3) measures of thermal gradients across fast-cooled crowns of up
to 160 C (Drs Norbert Thiel andMichael Tholey, Vita). In addition,
many clinicalauthorities report that they stopped having
porcelainproblems when they enforced a slow-cooling protocol
(including Drs Avi Sadan and Ed McLaren personal
communications). One paper given at the 2010 meetingof the
International Association for Dental Research(IADR) on clinical
data from four private practicesreported only 2% porcelain chipping
in two to threeyears for 702 prostheses (authors D Nathanson, S
Chu,H Yamamoto and C Stappert). These cliniciansreported that their
laboratories were aware of the needto cool slowly. Numerous dental
material companiesnow include a caution to slow cool in written and
web-based informational materials. This continues to be anactive
area of research.
Allceramics aresusceptible tosubcritical crackgrowthand
corrosion effect caused by water, which breaks thebond between
atoms at the crack tip, leading to slowgrowth of cracks, resulting
in a decrease of materialsstrength. Partially-stabilized
zirconia-based materialsare uniquely susceptible to auto-catalytic
transformationof the crystals from tetragonal to monoclinic at
relatively
low temperatures called low temperature degradation(LTD). 30
While generally studied at autoclave tempera-tures of a few hundred
degrees centigrade, signicantpercentages of transformation can be
extrapolated asbeing possible at oral temperatures using
activationenergy data from ceramics literature (Chevalier). 29
Another striking clinical study presented at the 2010IADR
examined partially-stabilized zirconia discsembedded in the anges
of mandibular partial dentures,demonstrating a much higherrate of
transformation foradental zirconia in two to three years
thanpredicted for anengineering zirconia by Chevalier (author Tomaz
Kos-mac , Jozef Stepfan Institute).
Water can catalyze the process at surface grainboundaries and
the transformation of crystal continuesfrom layer to layer through
the entire body, leading tomicrocrack formation, grain pullout and
a decrease instrength. 18 This phenomenon was particularly
impor-tant in causing the failure of zirconia hip
prosthesessubmitted to autoclave sterilization. Although
theinformation presented above raises concern, bothpublished
clinical trials and those presented at interna-tional research
meetings evidenced no bulk fracture indental restorations under the
observation time, indicat-ing that LTD has no major inuence on the
clinical
behaviour of dental restorations.31
Maximizing durability
Understanding how to maximize durability owsfrom understanding
clinical failure and the factorsinuencing the stress state at
failure that are withinour clinical control. Efforts to understand
clinicalfailure of single crowns has involved studying
fracturesurfaces (fractography), nite element modelling
anddeveloping a clinically-valid laboratory test. 32 Theseall
demonstrate that the main mechanism of failuredoes not involve
damage from wear facets but
Fig 9. Both central incisors were restored with veneered
zirconiacrowns (Y-Z, Vita). Mirror shot (top) demonstrates vital
translucency.
2011 Australian Dental Association 93
Ceramic materials in dentistry
-
8/12/2019 Ceramic Materials in Dentistry
11/13
stresses on the cementation surface due to occlusalloading.
Figure 10 is a cartoon representation of niteelement modelling
illustrating this stress state. Theseengineering analyses point to
four clinical techniquesfor maximizing durability: (1) provide
maximumocclusal thickness for the ceramic (strength increaseswith
the square of the thickness); (2) use the highestelastic modulus
(stiffness) substrate possible; i.e.metal or ceramic versus
resin-based composite); (3)bond the restoration, ceramic-cement and
cement-tooth (or substructure); and (4) develop broad, notpinpoint,
occlusal contacts.
This thickness-squared relationship is illustrated inFig 11 from
calculations using the analytical solution of Hsueh. 33 For
example, predicted failure loads for alithium disilicate
restoration increase from 1400 N toover 2000 N with a ceramic
thickness increase from1.6 mm to only 1.8 mm. Higher elastic
modulus
(stiffness) substructures decrease the stress for anygiven load.
This effect has also been validated fromclinical study of
all-ceramic crowns. 34,35 Failure loadsof crowns have been found to
be doubled with bondingin laboratory testing (L May, JR Kelly,
University of Connecticut, unpublished research) and this effect
hasbeen veried in retrospective clinical studies of bothinlays and
crowns. 36,37 Figure 10 also predicts that forany given total
thickness there is little to no structuralimprovement from making
the higher strength ceramicthicker. This counter-intuitive
prediction is beingveried in laboratory testing (R Yau, P
Rungruanga-nunt, JR Kelly, University of Connecticut,
unpublisheddata) and may allow crowns to be maximized foraesthetics
without decreasing durability. Failure stressesalso increase with
decreased wear facet size, e.g. failureloads as a function of
loading piston diameter were:1 mm = 343 N; 2 mm = 382 N; and 3 mm =
522 N. 38
Etching and bonding
Ideal bonding involves having microstructural struc-tures within
the ceramic that can be selectively attackedby acids (etched) at a
higher rate than surrounding
ceramic leaving micromechanical features for cementinltration.
The selective etching of crystalline leucite,leaving behind
microscopic glassy crypts, is the mostcommon dental example. A
second requirement forgood bond formation relates to the size of
thestructure(s) formed by etching and how well they arestill
attached to the remaining bulk ceramic. Forexample, some selective
etching of In-Ceram aluminais possible but the scale of roughness
that develops isinsufcient for good bond formation.
Polycrystallineceramics can be etched, revealing the
boundarybetween crystalline grains, but these etched
grainboundaries provide little micromechanical retention.
Chemical bonding is possible with virtually all dentalceramics,
but only with the use of resin cementscontaining special adhesive
molecules. The durabilityof chemical bonding between resin cements
and sub-structure ceramics has not been denitively
addressed.Laboratory data suggests that bonds can
decreasesignicantly during water storage. 39
Aesthetic considerations
Achieving a lifelike match requires the clinician technician to
choose a base ceramic having an appro-priate translucency (value in
the Munsell system) for thepatient. For a single anterior tooth,
all ceramics havesufcient longevity based on clinical trial data,
so thechoice can be made on aesthetic capability alone. Newresearch
on comparative translucencies is in prepara-tion that will update
decades-old information.
Three things need to be measured and recorded forcommunication
with the dental laboratory: (1) baseshade (gingival one-half to
one-third); (2) incisalenamel characterization; and (3) surface
gloss. Base
shade is best determined within a rational shade
Fig 11. Calculated loads to reach 360 MPa (breaking strength of
lithium disilicate) for three different thicknesses as a function
of
varying core thickness (remainder veneer).
Fig 10. Failure stresses are linearly related to the elastic
modulusdifferent (ceramic-substrate) and to the square of the
ceramic
thickness.
94 2011 Australian Dental Association
JR Kelly and P Benetti
-
8/12/2019 Ceramic Materials in Dentistry
12/13
system such as 3-D Master (Vita). Numerous auto-mated shade
taking devices are also available, with themost highly regarded
from laboratory research beingthe EasyShade (Vita).
Ceramic systems offer different levels of translu-cency and
colour control. These are best learned byclinical practice. In
general, an aesthetic match is best
achieved by specifying a ceramic system offering thesame
translucency as the case being matched. Cur-rently available
ceramics are organized below bytranslucency measurements (L Spink,
P Rungruanga-nunt, JR Kelly, University of Connecticut,
unpub-lished research).
Many all-ceramic systems are clinically indicated forsingle-unit
anterior teeth, including most in Table 1.Thus, clinicians are free
to choose a system offering thebest aesthetic match. 7 Good choices
(i.e. well-studiedclinically) for posterior single-unit teeth
includeIn-Ceram alumina (Vita), Empress Esthetic (Ivoclar),e.max
Press or CAD (Ivoclar) and zirconia-based(various). 7 Only the
zirconia systems are indicated formulti-unit xed prostheses.
Glazing versus polishing
Auto glazing (ring in air) and polishing are twooptions for
nishing the surface of aesthetic porcelains.These two techniques
received recent attention in areview of a number of studies
comparing preparedsurfaces using visual, microscopic and
prolometrymeasures. 40 All studies agree that glazing can produce
asmooth porcelain surface. However, polishing can
produce as smooth a surface that can be moreaesthetically
similar to natural enamel. Many author-ities favour polishing given
that a higher level of controlis possible over nal surface nish and
that an addedring can add problems and time to the
deliveryappointment.
Repair
Approaches to the repair of porcelains have beenreviewed
relatively recently. 41 Repair often offers bothdentist and patient
a cost-effective alternative to
replacement. Repair involves the bonding of resin-
based products to remaining porcelain. The porcelain-resin bond
is formed by both etching the surface tocreate micromechanical
attachment features and by theapplication of silane coupling agents
to provide somechemical interaction between the silicon-based
ceramicand carbon-based resins. It is reported that porcelainrepair
systems form durable bonds to fractured porce-lain and exposed
metal surfaces. 41
SUMMARY
Ceramics are widely used in dentistry due to theirability to
mimic the optical characteristics of enameland dentine as well as
for their biocompatibility andchemical durability. Most highly
aesthetic ceramics arelled glass composites based on
aluminosilicate glassesderived from mined feldspathic minerals. One
commoncrystalline ller is the mineral leucite, used in
relatively
low concentrations in porcelains for metal-ceramicsystems and in
higher concentrations as a strengtheningller in numerous
all-ceramic systems. In general, thehigher the fraction of
polycrystalline components,the higher the strength and toughness of
a ceramic.The development of substructure ceramics for
xedprosthodontics represents a transition towards
fullypolycrystalline materials. While the strength rating of
adental ceramic can be a meaningful number, it is notreally an
inherent property and varies due to testingparameters that are
often not well controlled tooptimize clinical relevance. Fracture
toughness is a farmore inherent measure of the structural potential
of aceramic and represents a more easily compared value.Clinical
data for all-ceramic systems is becomingincreasingly available and
results exist for manycommercial materials, providing guidance
regardingclinical indications.
REFERENCES1. Plumb JH. In the Light of History. New York: Delta,
1971:59
65.2. Kingery WD, Vadiver PB. Ceramics Masterpieces: Art,
Structure,
and Technology. New York: Free Press, 1986:322.3. Gleeson J. The
Arcanum: The Extraordinary True Story. Warner
Books, 2000:336.4. Ring ME. Dentistry: An Illustrated History.
New York: Harry N
Abrams Inc., 1985:108211.5. Orlowski HJ, Koenig CJ. Thermal
expansion of silicate uxes in
the crystalline and glassy states. JACS 1941;24:8084.6.
Weinstein M, Weinstein LK, Katz S, Weinstein A. Fused Porce-
lain-to-Metal Teeth. US Patent no. 3 052 982. 1962.7. Della Bona
A, Kelly JR. The clinical success of all-ceramic res-
torations. J Am Dent Assoc 2008;139:8S13S.8. Starling LB,
Stephan JE, Stroud RD. Shrink-free ceramics and
method and raw batch for the manufacturer thereof. US Patentno.
4 265 669. 1981.
9. Sozio RB, Riley EJ. The shrink-free ceramic crown. J
ProsthetDent 1983;49:182187.
Table 1. Recommendation for use of an all-ceramicrestoration
based on translucency (MO denotesmoderate opacity and HO denotes
high opacity)
High translucency Moderate translucency Low translucency
Empress Esthetic Vita Y-Z zirconia e.max Press HO
e.max Press e.max Press MO In-Ceram zirconiaEmpress CAD Vita
aluminaIn-Ceram Spinell In-Ceram alumina
Lava zirconia
2011 Australian Dental Association 95
Ceramic materials in dentistry
-
8/12/2019 Ceramic Materials in Dentistry
13/13
10. Della Bona A, Mecholsky JJ Jr, Barrett AA, Griggs JA.
Charac-terization of glass-inltrated alumina-based ceramics. Dent
Mater2008;24:15681574.
11. Hornberger H, Marquis PM. Mechanical properties and
micro-structure of In-Ceram, a ceramic-glass composite for
dentalcrowns. Glastech Ber Sci Technol 1995;68:188194.
12. Mo rmann WH, Brandestini M. Cerec-System: computerized
in-lays,onlays and shellveneers. Zahnarztl
Mitt1987;77:24002405.
13. Andersson M, Ode n A. A new all-ceramic crown. A
dense-sintered, high-purity alumina coping with porcelain. Acta
Od-ontol Scand 1993;51:5964.
14. Raigrodski AJ. Clinical and laboratory considerations for
the useof CAD CAM Y-TZP-based restorations. Pract Proced
AesthetDent 2003;15:469476.
15. Filser FT. Direct ceramicmachining of dental restorations.
Zurich:Swiss Federal Institute of Technology Zurich, 2001. PhD
thesis.
16. Filser F, Kocher P, Gauckler LJ. Net-shaping of ceramic
compo-nents by direct ceramic machining. Assembly
Autom2003;23:382390.
17. Denry I, Kelly JR. State of the art of zirconia for dental
appli-cations. Dent Mater 2008;24:299307.
18. Kelly JR, Denry I. Stabilized zirconia as a structural
ceramic: anoverview. Dent Mater 2008;24:289298.19. Denry IL. Recent
advances in ceramics for dentistry. Crit Rev
Oral Biol Med 1996;7:134143.20. Kelly JR. Ceramics in
restorative and prosthetic dentistry. Annu
Rev Mater Sci 1997;27:443468.21. Giordano R. A comparison of
all-ceramic restorative systems:
Part 2. Gen Dent 2000;48:3840, 43-45.22. Weinstein M, Weinstein
AB. Porcelain covered metal-reinforced
teeth. US Patent no. 3 052 983. 1962.23. McLean JW, Hughes TH.
The reinforcement of dental porcelain
with ceramic oxides. Br Dent J 1965;119:251267.24. Grossman DG.
Cast glass-ceramics. Dent Clin North Am
1985;29:725739.
25. Heffernan MJ, Aquilino SA, Diaz-Arnold AM, et al.
Relativetranslucency of six all-ceramic systems. Part I: core
materials. JProsthet Dent 2002;88:49.
26. Heffernan MJ, Aquilino SA, Diaz-Arnold AM, et al.
Relativetranslucency of six all-ceramic systems. Part II: core and
veneermaterials. J Prosthet Dent 2002;88:1015.
27. Swain MV. Unstable cracking (chipping) of veneering
porcelainon all-ceramic dental crowns and xed partial dentures.
ActaBiomater 2009;5:16681677.
28. Tholey MJ, Swain MV, Thiel N. SEM observations of
porcelainY-TZP interface. Dent Mater 2009;25:857862.
29. Kim JM, Covel NS, Guess PC, Rekow ED, Zhang Y. Concerns of
hydrothermal degradation in CAD CAM zirconia. J Dent
Res2010;89:9195.
30. Kobayashi K, Kuwajima H, Masaki T. Phase change
andmechanical properties of ZrO2-Y2O3 solid electrolyte afteraging.
Solid State Ionics 1981;3-4:489493.
31. Kelly JR. Dental ceramics: current thinking and trends. Dent
ClinNorth Am 2004;48:513530.
32. Kelly JR, Rungruanganunt P, Hunter B, Vailati F.
Developmentof a clinically validated bulk failure test for ceramic
crowns. JProsthet Dent 2010;104:228238.
33. Hsueh CH, Miranda P. Modeling of contact-induced
radialcracking in ceramic bilayer coatings on compliant substrates.
JMater Res 2003;18:12751283.
34. Malament KA, Socransky SS. Survival of Dicor
glass-ceramicdental restorations over 14 years. Part II: effect of
thickness of Dicor material and design of tooth preparation. J
Prosthet Dent1999;81:662667.
35. Malament KA, Socransky SS. Survival of Dicor
glass-ceramicdental restorations over 16 years. Part III: effect of
luting agentand tooth-substitute core structure. J Prosthet Dent
2001;86:511519.
36. van Dijken JW, Ho glund-Aberg C, Olofsson AL. Fired
ceramicinlays: a 6-year follow up. J Dent 1998;26:219225.
37. Malament KA, Socransky SS. Survival of Dicor
glass-ceramicdental restorations over 14 years: Part I: survival of
Dicor com-plete coverage restorations and effect of internal
surface acidetching, tooth position, gender, and age. J Prosthet
Dent1999;81:2332.
38. Yi Y, Kelly JR. Effect of occlusal contact size on
interfacialstresses and failure of a bonded ceramic: FEA and
monotonicloading analyses. Dent Mater 2008;24:403409.
39. Kern M, Thompson VP. Bonding to glass inltrated
aluminaceramic: adhesive methods and their durability. J Prosthet
Dent1995;73:240249.
40. al-Wahadni A, Martin DM. Glazing and nishing dental
porce-lain: a literature review. J Can Dent Assoc
1998;64:580583.
41. Latta M, Barkmeier WW. Approaches for intraoral repair of
ceramic restorations. Compend Contin Educ Dent 2000;21:635639.
Address for correspondence:Dr J Robert Kelly
University of Connecticut Health Center263 Farmington
AvenueFarmington, CT 06030
USAEmail: [email protected]
96 2011 Australian Dental Association
JR Kelly and P Benetti