-
7/23/2019 Ceramic Inlays Clinical Assessment and Survival
Rate
1/10
Ceramic Inlays: Clinical Assessment andSurvival Rate
Massimo FuzziVGiorgio Rappellib
Purpose This study evaluates th e olinical behavior of oeramic
inlays piaced during the past deca de.Materials and Methods One
hundred eighty-two inlays were examined in 66 patiehts. The
interval be-tween placement and assessment was oh average 5.9 years
2.7, ranging from 2 to 11.7 years. Restora-tions still present at
the time of evaluation were clinically assessed according to
modified USPHS criteria.Kaplan-Meier statistical analysis was used
to assess the survival rate.
Results According to USPHS criteria, good results were obtained
for color match, marginal discoloration,recurrent caries, contour,
and marginal integrity. Six inlays failed: four for endodontic
reasons, one due torecurrent caries, and the other due to fracture.
The results indicate that a success rate of 95% could bepredicted
at 11.5 years.
Conclusion The lack of recurrent canes, the ohiy slight changes
ih marginal discoloration and colormatch, combined with the
excellent longevity prove that ceramic inlays are a valuable tool
for the restora-tion of posterior teeth.J Adhesive Dent 1999; 1;
71-79. Submitted for publication: 0 6.10 98 : accepted for
publicai/on: 05.11,98.
he challenge of repro duc ing natural e stheticshas been present
for several decades, with a
nstant improvement of restorative materials andiicatjon
techniques.
Since 1882, when Herbst introduced the first ce-mic in iays ,2^
grea t progress has been ma de.
ay, than ks to improv em ents in adhe sion tech-ues and mater ia
l character is t ics , indi rec t ce-
mic restorations are one of the ai ternatives toalgam,
particularly in large cavities, enabling the
hetic demands of patients to be met for theirte rior
teeth.2.7.11.25.26 j ^ j g typ e of re sto ra tio no strengthens
the tooth structure and preservestai tissue to a large extent.^
ate practice. Bologna, Itaiy.vate practice, Osimo (An),
itaiy
nt requests Dr Massimo Fuzzi 7 Piazza P.ta Mascareila.8 Boiogna.
Itaiy Fax: ++39 051 240513; E-mail: SAOS FUZZimasianet.it
Porcelain remains the materiai of choice for nat-urai-looking,
esthetic restorations, due to its excel-lent optical qualities,
indirect fabrication process,and favorable bioiogical response.
However, investi-gations on the longevity and ciinical behavior of
ce-ramic inlays are insuffioient.
in 1992, Mrmann and Krejct^^ estimated a suo-cess rate with the
Cerec system of 75% after 5years. That same year, Studer et ai^o
reported asurvival rate of 98% based on 130 iPS Empress in-lays,
examined at 186 months. In 1994, Reiss^^examined 1000 Cerec-type
inlays and, using the Ka-pian-Meier survivai analysis, found a
success rateof 9 1 % after 6 years. In 1994, Moaci< and
Rouieti^exam ined porcelain inlays piaced by studen ts andfound a
survivai rate of 75% after 4 years. In 1995,Roule t ts assessed 123
in iays wi th the Kapian-iVleier analysis and found a success rate
of 76% at6 years. The failures were due to fractures and en-dodo
ntic causes, partiy related to extended applica-t ions. Studer and
coworkers^^ published data in19 96 on 13 0 IPS-Empress iniays,
reporting a sur-
vivai rate of 97.5% after 2 years, in 1996, Qual-t roug h and
Wilson ^ obta ine d a success ra te of
-
7/23/2019 Ceramic Inlays Clinical Assessment and Survival
Rate
2/10
Fuzzi/Rappeili
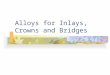
Fig 1 The margins of the prepa ration are placed on theenamel.
The dentin side, when neoessary, is reoonstruotedwith a
glass-ionomer photooured base.
Fig 2 The impression w ith poiyether ma teriai reprothe de tails
of the prepa ration, A fluid m steriai (Pbiue, ESPE, See feid,
Germany) is applied to the thioi^er m aterial [Imp regum , ESPE,
See feid, Germaplied to the tray.
8 2% from 50 ceramic inlays examined at 3 years.In 1997,
Fradeani et ai^ reported a 96% successrate over 125 iPS-Empress
inlays examined at 4.5years. That same year, Roulet^* reported a 4%
an-nual faiiure rate of Dicor porcelain inlays.
The present study assesses the survival rate andciinicai condit
ion of porcelain inlays provided byone of the authors in his
ciinicai practice over theperiod 1986 to 1996,
M TERI LS ND METHODS
One hundred eighty-two porcelain inlays were exam-ined in 66
patients, 41 female and 26 male. Pa-tient age ranged from 23 to 50
years. The iniaysincluded occiusai restorations (11),
mesio-occlusal(35), occluso-distal (45), mesio-occlusal-distal
(63)and cus pal-cove rage restora tions (28), Cavity pre pa-rations
with ai i margins iocated in enamei werecompleted in each tooth
using Cerinlay diamondburs (Intensiv, Viganelio-Lugano,
Switzeriand) (Fig1) , Fuil-arch impressions including the
preparationswere taken using a polyether impression
material(Impregum, FSPF, Seefeid, Germany) (Fig 2), whilethe
opposing arch was replicated with an algnatei m p r e s s i o n . F
e r m i t a c r y l i c ( I v o c i a r, Vi v a d e n t ,Schaan,
Liechtenstein) or a reiated material wasused to make temporary
restorations.All restorations w ere made by the same techn
icianusing Microbond Natural f ired ceramics (Austenal
Dental-Austenal Internationai Inc, Chicago, IL, USA)
in the period from 1986 to 1990 and Fortucera mic s (W illiam
s-lvociar, Am hers t, New USA) from 1 9 9 1 to 1 99 6. L uting was
carwith a rubber dam in place, Cavex Protect (Cavex, Haarlem,
Holland, by Kuraray Co Ltdwas used to protect the external part of
theduring luting; the varnish was applied withand removed with
alcohol after luting the (Fig 3). The fitting surface of the
ceramic tions was etched with hydrofiuoric acid (HF the t echn ic i
an a f t e r t ry- in . S i ianiza t ion wSilane (3IVI De ntal
Produc ts D ivision , St PUSA) was carried out by the dentist just
being. Enamel and dentin were etched and The adh esiv e used in the
pe r iod f ro m 1
1992 was Scotchbond 2 (3M Dental Produsion, St Paul, MN , USA);
en am el w as etch37% p hosphoric acid for 30 s, rinsed, and
bonding agent was used to achieve adhesion
1993 to 1996, Scotchbond MP (3M Dentucts Division, St Paui, MN,
USA) was useadhesive . A 10% maie ic ac id or 37% phoacid was
applied to the enamei for 30 s andden tin for 15 s; after rins ing
and ge ntly dthin layer of primer w as appiied to the de ntbonding
agent was used to achieve adhesioluting materials used were
dual-cured comUltra-Bond (Den Mat Corp, Santa Maria, Cfrom 1986 to
1990 and indirect PorceiainDentist Bo nding (3M Dental P roducts
DivPaul, M N, USA) in the period from 1 9 9 1 Following restoration
placement, excess lu
-
7/23/2019 Ceramic Inlays Clinical Assessment and Survival
Rate
3/10
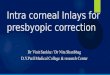
3 A varnish is applied to the external surface of the prepa-ion
to faciiitate the removal of the composite after polymer-tion. A
transp arent st icky wax is applied to the occlusalt to facilitate
the manipulation of the inlay.
ig 4 The finished case, 1 year after completion.
ial was removed with sponge pellets, brush, andper floss. The
luting composite was light curedm all aspects (5 min totai). The
varnish, rubber
m, and excess lu ting m aterai were removed. Oc-usion was then
checked and adjusted. Diamondishing burs and rubber points were
used for fin-
hing margins (Fig 4).Ali patients were enroiied in a 3-to
6-month peri-
ontai maintenance program consisting of remoti-t ion , r e ins t
ruc t ion o f o ra l hyg iene measures ,ofessional tooth cleaning,
and fiuoridation. Thisre was provided by a dental hygienist.The
restorations still present at the time of as-ssment were evaiuated
clinically by a suitablyined operator using modified USPHS cri
teria^iable 1). The margins were checked with a Hu-iedy XP 23/OW
(Hu-Friedy, Chicago iL, USA] ex-orer. Color was assessed under
Siroiux iliumina-n (Siemens AG, Bensheim, Germany). The time
apsed from the date of luting until the iast checks 2 to 11.7
years.
The oiinicai variables (color match, marginal dis-loration,
recurrent caries, contour, marginal in-ri ty) were tabled using the
stat is t ical programS for W indows, ve rs ion 6 .08.2- ' A con di
t ion al
aiysis of the iniays and onlays still intact at thet observation
was performed on those variableswhich several values of bravo or
worse had
en recorded. To reconstruct the changes in theiables, the med
ian dura tion (5 years and 13 2
ys) was used to create two subgroups: recent vs.er restorations.
The subgroup recent included
89 and the subgroup older 87 inlays. The frequencyof alph a
vaiues in the two groups was comp aredby means of the exact
analogue of the chi-squaretest . i^ A iarger percentage of alpha in
the group ofmore recent restorations was interpreted as a
trendtowards better values over time, without necessarilyproviding
an explanation ofthe cause.
Those inlays no longer present at the time of as-
sessment were considered failures. Failures werec la s s i f i
ed accord ing to cause : a ) f r ac tu res ; b )caries: c)
endodontic reasons: d) unacceptable es-thetics; e] periodontal
problems.
To display the life expectancy of the inlays andonlays,
Kaplan-Meier survivai curves were piotted,both for the whole sample
and separateiy for per-manen t mola r s and p remola r s . The s t
a t i s t i ca lprogram SOLC 4,0 for D0S22 was used for
calcu-lations .i^ For the whole sample, 95% confidence in-tervals
were constructed by multiplying by 1.96 the
estimated standard error of the probabiiity of sur-vival at the
time of each failure.
R SULTS
Assessment of USPHS criteria showed 100% alphaconcerning
recurrent caries. Color match analysisof older restorations yielded
57% alpha and 43%bravo: recent restorations were rated 8 1 %
alphaand 19% bravo (Fig 5), Marginal disc olora tion in
older restorations was rated 83% alpha and 17%bravo, whiie
recent restorations scored 94% alpha
-
7/23/2019 Ceramic Inlays Clinical Assessment and Survival
Rate
4/10
Fuzzi/Rappeii
Table Criteria for the clinical evaluation of the inlays
Category Rating Characteristic
Color matoh Alpha
Bravo
Charlie
Marginaldisoo oration
Recurrentcaries
Marginalintegrity
Oscar
Aipha
Bravo
Alpha
Bravo
Alpha
Chariie
Alpha
The restoration appears to match the shade ahd transiucehcyof
adjaoent tooth tissues.The restoration does hot m atch the shade
and transiuoency ofadjacent tooth tissues, but the mismatch is
within the normairange of tooth shades.The restoration does hot
match the shade and transiucehcy ofadjacent tooth structure, ahd
the mismatch is outside the hor-mal range of tooth shades and
transiucency.The restoration cannot be examined without using a
mouthmirror.There is no visual evidence of marginal discoloration
differentfrom the color of the restorative m atenai and from the
coior ofthe adjacent tootli structure.There is visuai evidence of
marginai discoloration at the junc-tion of the tooth structure and
the res toration, but the disool-oration has not penetrated
aiongthe restoration in a puipai di-rection.There is visual
evidence of marginai discoioration at the junc-tion of the tooth
structure and the restoration tha t has pene-trated aiongthe
restoration in a puipai direction.There is no visual evidence of
dark, deep discolorationadjacent to the restoration.There is visual
evidenoe of dark, deep discoioration adjacentto the restoration but
not directly associated with cavosurfaoemargins).The restoration is
a continuation of existing anatomic form oris siightiy fiattene d.
When the side of the explorer is piacedtangentiaiiy aoross the res
toration, it does not touch two op-posing oavosurface line angles
at the sam e time .Asur faoeoo noavity is evident. When the side of
an expiorer isplaced tangen tiaiiy aoross a restoration, the
explorer touchestwo opposing oavosurface iine angies at the same
time, but
the dentin or base is not exposed.There is a ioss of restorative
subs tance so th at a surface con-cavity S evident and the base
and/or dentin is exposed.
The expiorer does not catch w hen drawh across the surface ofthe
restoration toward the too th, or, if the explorer doesoatoh,there
is no visible crevice aion gth e periphery of the restora-tion.The
expiorer catches and there is visibie evidence of a orevice,into
whioli the explorer penetrates, indicating th at the edge ofthe
restoration does not adapt ciosely to the tooth struc ture.The
dentin is not exposed, and the restoration is not m obiie,Tlie
expiorer penetrates a orevice defect tha t extends to
thedentin-enamei junc tion.
and 6 bravo (Fig 6, Marginal integrity was rated
alpha in all restorations except five assessed as
bravo. Contour received bravo scores in 2 cases
and alpha in all others (Tab 2 and Tab 3) (Figs 7, 8),
Of the 182 iniays examined, 6 fai led. Of these
fai lures, 4 were caused by endodontic probiems
and occurred during the first 6 months after ce-
mentation. One failure occurred after 3 years due
to fracture, and another was caused by recurrent
caries after 8 years. Five fai lures took piace in mo-
iars and one in a premolar. Using the Kaplan-Meier
analysis, the survivai index at 11.5 years was 95 ,
and the values, calculated with a 95 confidence
interval (CI), ranged from 86.5 to 98, 1 (Fig 9).
Separating the results of the premoiars from those
of the mol ars, the survivai rate of the premolar
restorations was 99 , while the survival rate of the
molar restorations was 90,2 after 11,5 years
(Fig 10),
-
7/23/2019 Ceramic Inlays Clinical Assessment and Survival
Rate
5/10
Fuzzi/Rappelli
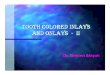
5 A ciinicai exam ple of 3 ceramic restorations after 11ars. The
onlays on teeth 16 and 15 have been evaiuated asavo for color
match, while the restoration on tooth 14 hasen evaluated as
aipha.
i 6 The marginal discoloration of two iniays after 4 years ina
patient who smotes. Some points of the occlusal and proxi-mai
margins of tooth 14 are stained.
7 MOD iniays on tooth 36 anO 37, OD inlay on tooth 35.te the
good ohromatic and marginai adap tation.
i 8 Radiographie verifications of the previous case. Noticethe
absence of overhangs and the good marginal adaptation.
Table 2 Results of the clinical evaluation of 3ll 176 inlays
examined
Recurrent canesMarginal integrityContourMarginal
discolorationColor match
176176176176176
176 (100 ) (0 )171 [97.2 | 5 (2.8 )174 (98.4 ) 2 (1.6 )15 6 88.6
] 20 (11.4 ]122(89 .3 ) 54(30 .7 )
Table 3 Marginal discoioration and coior match of recent < 5
y) vsolder {> 5 y) restorations; 0.05 ChiMest)
Marginal discoloration Cclor match
Recent restorationsOlder restorations
Aipha Bravo Alpha Bravo84 (94 ) 5 (6 ) 72 (81 ) 17 (19 )72(83 )
15(17 ) 50(57 ) 37(43 )
-
7/23/2019 Ceramic Inlays Clinical Assessment and Survival
Rate
6/10
Fuzzi/Rap pe 11
Kstill intact
ss%9S
9 2
9 0
8fl%
86
T - . , .,
1' 1 2
sjrviMlrBtt
: 3
0 2 4 S 8 10 12 Ye a r s Fig 9 Kaplan-Meier survivuated for the
totai number and 9 5% con fidence interv
%sl i l l i n l ac l190% -|
98 %
9B %
94%
92%
90%
r
0 2 4 6 a 10 12
S4iii>lars
-38 premolars
Fig 10 Kapian-Meier survrestorations in premolars a<
0.05).
D I S C U S S I O N
All the inlays assessed were found to be clinicaiiysatisfactory.
Exampies are shown in Figures 11a-l l d . No recurrent caries was
observed, which is in
aooordance with the findings of Stenberg and Mats-son,28
Tidehagand and Gunne,^ berg et al,25 andKrejci e t a l . "
The oontour was assessed as alpha in 98.4% ofthe oa ses. The
same results were obtained by Cavelet al," who, however, examined
31 inlays only 6months after luting, and Krejci et al .^ ' ' who
as-sess ed 1 0 iniays at 1 8 mo nths . Stude r et aP*^ ex-amined
130 inlays at 18 months (6 months) andassessed the contour of 87%
of the restorations asalpha. Cerutti and ooworkers^ reported 84%
alpha
contours on 109 Cerec CAD/CAM inlays 6 yearsafter luting.
Marginai integrity was assessed as oases and alpha in ail the
others. Romarginai gaps in 14% of inlays. Krejci an important
difference between the interproximai margins. We did not obs
ference, aithough our assessment was clinical examination with
the expiorer,cas were made for a scanning eieotronexamination.
The quality of the color matoh decrcantly as a function of time
(Tabie 3).not expect ceramics to change color ovfact might be due
both to the experitechnician in choosing the coior of tand to the
dentist 's choice of the iutinBetter resuits on coior match
were
Studer et a l^f and Krejci e t ai . l ' Bess iiVIolin,3 who
found 54% of assessed i
-
7/23/2019 Ceramic Inlays Clinical Assessment and Survival
Rate
7/10
g l i a Initiai case of the right upper qua drant. The gold
in-ys had interproxim ai overhangs , therefore preventing correotai
hygiene.
ig l i b The view of the oeramic iniays 1 mo nth after
plment.
g l i e An ooclus ai view after 5 years ig l i d An occiusai
view after 13 years.
n acceptab le color ma tch, attributes this resultocciusal
adjustment conducted after cementing;Dicor-type inlays, this is
assumed to remove the
ost superficial layer of colored ceramics, exposinge bulk
ceramic.
The values for marginal discoloration were alsognificantiy
different, depending on whether thestorations were oider or more
recent (Tabie 3), Itnot known, however, if this discrepancy is due
to
technical improvement or to a deterioration of thementing
oomposite which supposedly occurs with
me.Using Kaplan-Meier analysis, the inlays' 11,5 yrvivai rate
was 95%, Other studies, conducted onsim iiar nu m ber of resto
ratio ns, have aiso re-rted favorable findings.29-30 Molin and
Karisson^^
amined 20 5 Optec inlays after 1 to 32 mon ths.our restorations
were lost and 3 had fractured. In
a study by berg et a\ ^ the influence of the lutingmaterial on
the longevity of ceramic inlays wasvestigated. After a 3-year
observation period, thelays luted with composite resin showed
significafewer failures (2 failures out of 59 restoratio
than those cemented with glass-ionomer cementfailures out of
59). Van Dijken et aP^ evaluated fired felspathic ceramic inlays
luted with glionomer cement and composite cement afteryears. As
with berg et al. Van Dijken et al foubetter results forthe inlays
cemented with compite (93% success rate) than the inlays luted
wglass-ionomer cement (76%), Rouiet^s found 9failures among 123
Dicor inlays over a period to 82 months, failures being due to
fracture (7),dodontic problems (4), and postoperative pain
No differences were found between the luting mrials (three
different luting composites). Premo
-
7/23/2019 Ceramic Inlays Clinical Assessment and Survival
Rate
8/10
Fuzzi/Rappeiii
tended to show a better success rate; however, the
difference was not statistically significant, Molin
and Karisson '' reported a 90 success rate after 3
years: this was obtained by calculating the survival
rates of iniays performed by 10 dentists who pre-
sented very different results. This finding empha-
sizes the sensitivity of the ceramic iniay technique
and the dependence on personal operator skill andclinical
experience. Operator ability and care in ap-
plying the technique can be the main factors infiu-
encing the success rate.
In many studies, the main reason for failure
seems to be the fracture of inlays. Quaitrough and
Wiison,20 examining 50 cerami c iniays after 3
years, found 18 failures due to fracture. All fail-
ures reported by Fradeani et al were due to frac-
ture. Isidor and Brondum^s obtained even less
favorabie results after 57 months with 12 failures
out of 25 inlays, 10 of which were fractures. The se-
lection of cases, particulariy if bruxism patients are
invoived, must also be taken into account when
evaluating the mechanicai properties of ceramics.
It shouid also be noted that 4 of the 6 failures re-
ported in the present study occurred in the same
patient for endodontic reasons (puipitis), and that
these restorations were carried out 11.5 years ago,
when iess oiinicai information was avaiiabie about
the adhesive technique and microleakage controi.
CONCLUSIONS
Taking into account that this single-center study
was conducted without using a control group, the
following conclusions may be drawn:
1 . Within the observation time (up to 11,5 years),adhesively
luted oeramic inlays showed no recur-
rent caries.
2 . The slight occurrence of marginal discolorationover ti me
(17 bravo for inlays older than 5
years) is still clinically acceptable.
3. The color match of the ceramic inlays was found
to be better in the recent restorations subgroup
than in the older restorations subgroup.
4 . After 11.5 years, a survival rate of 95 of all theceramic
inlays must be considered as excellent.
5. The survival rate of premolar inlays (99 ) was
superior to that of molar inlays (90 ).
REFERENCES
1. berg CH, Van D ijken JWV. Olofsson AL. Threson of fired
ceramic inlays cemented with coglass ionomer cement. Acta Odontol
Scan149.
2. Banks RG. Conservative posterior ceramic rerature review. J
Prosthet Dent 1990;B3;619-6
3. Bessihg C, Molin M. An in vivo study of glass ceraminiays.
Acta Odontol Scand 1990 :48:351 -35
4. Cavei WT, Keisey WP, Barkmeier WW, et a l. A pilothe clinicai
evaiuation of castabie ceramic inlayscure resin cement.
Quintessence Int 1988:1
5. Gerutti A, Vehturi G. Putignano A, Prati C. Six-yeaevaiuation
of 109 Cad/C am inlays. Ma drid: lstract 29 5|, 1997.
6. Cvar J and Ryge G. Criteria for the Ciihical Etai Restorative
Materials, USPHS PublicatiSan Francisco: U.S. Government Printing
Of
7. Dietschi D Holz J, Restauration des dents posSuisse
Odontostom 1990:10 0:1325-1 332.
8. Douglas WH. Methods tc improve fracture reteeth, in: Vanherie
G, Smith DC {eds). PosterResm Dentai Restorative Materiais. Proc
3MNetherlands: Peter Szulc Pubi Co, 1985: 4 3 3
9. Fradeani M, Aqu ilano A, Bassein L. Longitudinpressed
glass-ceramic inlays for four and half yethet Dent
1997;78:346-353.
10 . Fu ii M. Porcelain bonded restoration. In: DG. Fuizi M,
Prati C (eds). Adhesion in RestorativeProceedings ofthe
International Symposium87-97.
11. Garber DA, Goldstein RE. Porcelain and comonlays. Chicago:
Quintessence, 1 99 4.
12. Hihtze JL. SOLO S tatistical system BMDP SCork, ireland,
1991 (Survivai Anaiysis Modu
13 . Isidor F, Brondum K, A ciinjcal evaiuation of porceiJ
Prosthet Dent 1995:74:140-144.
14. Krejci i, Krejci D, Lutz F. Ciinicai evaiuation of a
newgiassed ceramic iniay material over 1.5 years. Quint
1992:23:181-186.
15 . Mehta C, Patel N Statxact Turbo, StatisticaiExact Non param
etric inference. U ser s Maware Corporation, Cambridge, MA, 1992
.
16 . Molin M, Karisson S. A clinical evaluation of the Osystem.
Acta Odontol Scand 1992:50:227-2
17. Molm M, Karisson S. A 3 year clinical follow-upramic (Optec)
inlay system. Acta Odont54:145-149.
18 . Mrmann W, Krejci i. Computer-designed inlaysin situ:
clinical performance and scanning scopic evaluation. Quintessence
Int 199 2:23:109
19 . Noack MJ, Rouiet JF, Survivai rates and m of Dicor iniays
after 4 yea r s | abs t rac t759] . J D1994;73:196,
20. Quaitrough AJE, Wilson NHF, A 3-year ciinporceiaih iniay
system. J Dent 1 996 :24:3 17-
21. Quaitrough AJE, Wilson NHF, Smith GA. TAn historical view.
Oper Dent 19 90:1 5:61 -7
22. Reiss B, Kiinische Langzeiterfahrungen mit
1994:38:30-33.
-
7/23/2019 Ceramic Inlays Clinical Assessment and Survival
Rate
9/10
Fuzzi/Rappelli
Rouiet JF. The longevity of giass ceramic iniays [abstract 3
6],J Dent Res 1995:74:405,Roulet JF, Longevity of giass ceramic
iniays and am aigam -re-sults up to 6 years. Clin Orai Invest 19 97
:1 :40 ^6 ,Rouiet JF, Degrange M Ihlay restorations, J Caiif Dent
Assoc1996:24:48-62,
Roulet JF, Herder S, Bonded ceramio inlays, Chicago:
Quintes-sence , 19 91 .SAS institute Inc., SAS Procedures Guide,
Version 6 ThirdEdition, Second p nnting, Gary, NC, 199 2 .Stenberg
R Matsson L Ciinical evaiuation of giass oeramicinlays Dicor), Aota
Odontoi Scand 1993 :51:91-97.Studer S, Lehner C, Brodbecii U
Scharer P, Short term re-sults of IPS-Empress ihlays and oniays , J
Pros thodont1996:5:277-287,Studer S, Lehner C, Schrer P.
Glass-ceramic iniays and on-lays made by IPS em press: first
clinicai resuits, J Dent Res1992:71:658,Tidehag P, Gunne J, A
2-year ciinic ai foilow-up study of iPSEmpress ceramic inlays, IntJ
Prosthcdont 1995:8:456-460.
Van Dijken JWV, Aberg HC, et al. Five year evaluation of
oe-ramic inlays [abstract 72]. J Dent Res 1996:75:13 02 ,
New Frontiers inAdhesive Dentistry
HYBRIDIZ TION OF
D E N TAT, H RD TISSUES
HYBRIDIZATION OF DENTAL HARD TISSUESNobuo Nakabayashi and David
H . Pashley
The hybridization of dentina process that cre-ates a
molecular-level mixture of adhesive poly-mers and dental hard
tissuesgives clinicians aversatile new material useful in a wide
array ofadvanced dental treatments. As the first
in-depthexploration of the suhject this book covers thedevelopment
present understanding and futureresearch areas of this
multifunctional dental mate-rial A thorough review of the current
literaturerounds out the text.
Valuable for students researchers and clini-cians seeking a
greater understanding of resinhybridization of tooth structure.
CONTENTS
Evolution of Dendn-Resin Bonding Properties of Dentin Acid
Conditioning and Hybridization of
Substrates4 Characterization of the Hybrid Layer5 The Quality of
the Hybndized Dentin6 Clinical Applications of Hybrid Layer
Formation
2 9 p p. 80 iHus some in coior :ISBN 0 87417 575 9 C3047; US
S40
To ORDER
CallToll Free 1-800-621-0387or Fax 1-630-682-3288
book
Visit our web site http://www qijintpub com
-
7/23/2019 Ceramic Inlays Clinical Assessment and Survival
Rate
10/10