Embed Size (px)
DESCRIPTION
Central Okanagan PALLIATIVE MED REC Home and Community Care. Background. Palliative Clients who are admitted to Hospice for Pain and Symptom Management (PSM). - PowerPoint PPT Presentation
Citation preview

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Central Okanagan
PALLIATIVE
MED REC
Home and Community Care

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Background
• Palliative Clients who are admitted to Hospice for Pain and Symptom Management (PSM).
• Patient risk = loss of pain control; anxiety around uncertainties in medication also causes increased pain levels
• Hospice temporarily located within a Residential setting until stand- alone site is ready

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Background
• Multidiscliplinary team – Community, Acute, Residential, and Cancer Centre
• Goals are to:– Expedite transitions– Prevent Adverse Drug Events in
transitions• Project started just prior to Learning Session
1 in Saskatoon• Project charter draft written prior to LS1

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Aim #1
4 Aim Statements:
1. Create Best Possible Medication History (BPMH) for 95% of the identified Palliative group within 24 hrs of admission to Hospice, and identify the discrepancies. The target date is Apr. 30, 2008.

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Aim #2 & #3
• Reconcile 100% of the identified discrepancies within 48 hrs of admission, by Apr. 30, 2008.
• Create a Best Possible Medication Discharge Plan (BPMDP) for 95% of patients transitioning back to the Community, by Apr. 30, 2008.

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Aim #4
4. Reduce Edmonton Symptom Assessment System (ESAS) score for symptom management by 50% by Apr. 30, 2008.
(ESAS scores nine symptoms – pain, tiredness, nausea, depression, anxiety, drowsiness, appetite, wellbeing and shortness of breath - on a scale from 0 to 10, with 10 being the worst possible symptom score. A reduced score would show improvements in symptom management.)

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Team Members
• Community Care Manager• Director, Residential Services• Clinical Practice Consultant, Home Care Nursing
(HCN)• Clinical Resource RN’s (Acute, Hospice & HCN
Palliative Care)• Cancer Centre RN• Pharmacists (Clinical & Community)• Family Practitioner• Quality Improvement (SHN) Rep

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Changes Tested
Who is completing BPMH?
Clinical resource nurse.
• Tested may different forms, only to fine tune an already existing form created in our acute care setting.

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Changes Tested
2. Tested best timing to complete BPMH to have an accurate completed Med Rec done.
a) BPMH within 48hrs of admission with a goal of 1 week to Med Rec by Physician.
b) BPMH within 24hrs of admission with a goal of 1 week to Med Rec by Physician
c) BPMH on admission with Med Rec within 24 hrs of admission.

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Results
1. Forms tested….. Ours fine tuned. Tested 6 forms.
2. Timing….. We found doing a BPMH on admission to unit resulted in physicians completing the reconciliation soon after admit, with physician cooperation completing the Med Rec with appropriate, accurate orders.

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Results
3. Clients are often admitted to unit when CRN is not available. The target group is not always having a Med Rec completed with in the target timeframe.
4. Process Map prior to Med Rec created.
• Process map and limited data follows…

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
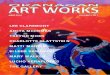
Process Map Prior to Med Rec
Med Rec for the Palliative Client in the Central Okanagan - PROCESS BEFORE INSTITUTION OF MED REC
Res
iden
tial
(Dou
glas
Fir
[DF])
Res
iden
tial
(Dou
glas
Fir
[DF])
BC
CA
CSI
BC
CA
CSI
Com
mun
ity
Com
mun
ity
Acu
te (KG
H)
Acu
te (KG
H)
Phy
sici
anPhy
sici
an
Palliative Client
Patient Discharge (Stable / Expiry)
PRE MED REC Process Map prepared by:
H. Morgan, QI DeptSept 18, 2007
GP, Oncologist, PSM Physicians
Meds listed in chart DNR Document
CSI RN Health Assessment Form Medication Record (form)
Community RN
Acute RN
(through ER or Direct Admit to Ward)
Private-Practice Community Pharmacist
Accesses drug info from PharmaNet
Hospice RN/ LPN
CSI PharmacistAccesses drug info from
PharmaNet
Med Hx PharmaNet Patient Family Meditech CSI Pharmacist Consultation Notes
(GP)
ADMIT to COK Palliative Program
Med Hx Transfer information
only
Palliative Response Team
(24 hr Physician Response)
Medication Profile*
Patient Family MRP Discharge Orders MAR (Meditech) Med bottles CSI List Community
Pharmacy Pixalere
Med Hx Patient Family Previous health records (Meditech) PharmaNet
EHS List CSI List (faxed to ward M-F, 0800 –
1600 hrs only)
NO REVIEW OF MEDS
ON ADMISSION
NOTES
1. PSM = Pain & Symptom Management2. MEDITECH = one system common to all intake points for clients3. Community Medication Profile contains information on:dose, route, frequency, start date, physician, pharmacy, and who administers the medication

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Results
June: incomplete data ; CRN away. BPMH complete = 1
July (after July 23) P&SM admits = ? BPMH complete = 0
August P&SM admits = ? BPMH complete = 4
September (to date) P&SM admits = ? BPMH complete = 2

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Results
Run Charts of your Key Measures• Insert your run charts here
(More than one slide may be necessary)
• Annotate your run charts with specific changes you’ve tested

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Example of Annotated Graph:Improved Access
(delete this slide before saving)
0
5
10
15
20
25
30
35
40
45
May-02 Jun-02 Jul-02 Aug-02 Sep-02 Oct-02 Nov-02 Dec-02
Provider Back from Vacation
Began backlog reducion
Cross Trained Staff Protocols Tested
Protocols
Reduced Appt types

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Keys to Success and Lessons Learned
• We need to expand our team educate and include bedside nurses in the process with 1 or 2 to take on the role of champions when the CRN is not available to complete the BPMH.

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Keys to Success and Lessons Learned
• One person completing the BPMH is too heavy a load!
• Persistence! We need to persevere with follow up to get the physicians understand the importance of completing the med rec.
• Process takes longer than anticipated; but well-designed form shortens and smoothes out the process.

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Next Steps
• We are aiming for hospice staff buy in and participation in creating a BPMH for each pain and symptom management client admitted to the hospice unit.
• Adopt a BPMH/Med Rec form that includes our measurement components.
• Include ESAS (Edmonton Symptom Assessment Scale) measurements on admit and discharge for all the Med Rec clients.

Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Contact Information
• Dianne Stockwell (Clinical Resource Nurse)[email protected](250) 862-4109
• Faye Burch (Director, Residential Services)[email protected](250) 870-5784
• Holly Morgan (Clinical QI Coordinator)[email protected](250) 862-4300 Ext 7210