Embed Size (px)
Citation preview

Central Line Associated Blood Stream Infection Prevention Project
Gabrielle Hanlon, Project ManagerTony Burrell, Chair ANZICS Steering Committee

Background• ~ 300 ICU CLABSI/yr in Australia• Costs $14,000 per case
extra $AU4.3 million
• 3,000 extra bed days• Attributable mortality 4-20%• CLABSI preventable

BackgroundCLABSI reduction projects• Pronovost (2006) & others (15yrs)• NSW CLAB ICU (2007-08) 3.0 → 1.2/1,000• WA Safety and Quality Investment for Reform
(SQuIRe) Program 2006 → 0.55/1000

This project
• ACSQHC funded ANZICS• National project• Adult & paed ICU• Public & private• Build on existing work

Objectives• Decrease rate of CLABSI in Australian ICUs to
<1/1000 line days• Accurately and consistently measure the rate
of CLABSI in ICUs throughout Australia• Timely reporting to clinicians• Benchmarking

Preparation• Review current practice (April/May 2010)
• Surveillance– Definition– Reporting method & timeframe
• ICU– CVL insertion– Knowledge of surveillance

SurveillanceAcross Australia• Majority data collected by ICPs• A few ICUs collected some data• Not all jurisdictions did CLABSI surveillance• Inconsistent definitions, reporting (method &
timing), benchmarking• Variable practises in private sector• No national reporting or benchmarking

ICU practice ICU Directors/Nurse Managers Survey• 53/100 ICUs: 24 doctors, 39 RNs (not NSW, ACT)
• Variable knowledge of surveillance processes• Some did not know CLABSI rate “but it’s low”• Variable compliance with “best practice” re
CVL insertion

ICU practiceCVL insertion – total 51 ICUs• have trolley/pack 76%• wear hats 43%• wear masks 43%• Chlorhex handwash 88%• sterile gown & gloves 100%• Chlorhex & alcohol skin prep 100%• full body draping 41%

Clinical practice
CVL insertion & maintenance• Chlorhex patch 20%• Impregnated CVC 59%• Chlorhex body-wash 25%

Schedule First • Outcome assessment & national reporting
both require– national definition – implementation/interpretation guide
Then• improve CVL insertion practises

National definition • minimise change if possible• numerator - NHSN 2008• denominator - line days • implementation guide inc “other infection”
definitions

National definition
Am J Infect Control 2008:36;309-32


National definition
• All jurisdictions adopting as able• New surveillance commencing

National reporting • No duplication at any step• Jurisdictions forward data to ANZICS if they
already collect it (hospital-level data only) • Some individual public & private hospitals
forward data to ANZICS (if above n/a)

National reporting • ANZICS generate reports
– Self vs other SA ICUs– Self vs other in same CICM level/other PICUs nationally– Self vs all in Australia
• Secure log-in• Access:
– ICU director & NUM – Inf Cont
– ? other

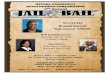
Monthly reportingICU CLABSI rate compared to other CICM Level I
0
1
2
3
4
5
6
7
Janu
ary
Febru
ary
Mar
chApr
ilM
ayJu
ne July
Augus
t
Septe
mbe
r
Octobe
r
Novem
ber
Decem
ber
Time period: 2010
CL
AB
SI r
ate
pe
r 1
000
lin
e d
ays
Max-Q3
IQR
Q1-min
0-min
CLABSI rate of Identified ICU
Mean

Annual reportYearly CLABSI rate summary for <insert name of hospital & ICU ID>
2.5 1 3 2 10
0.5
1
1.5
2
2.5
3
3.5
4
Mean Identified ICUannual CLABSI rate
Mean CICM Level 1annual CLABSI rate
Mean <Jurisdiction>annual CLABSI rate
Mean national annualCLABSI rate
Benchmark CLABSI rate
Time period: January - December 2010
CL
AB
SI
rate
per
100
0 li
ne
day
s

Interim goals Foundations• National definition √• Implementation (interpretation) guide √• National reporting √
Now• Improve CVL insertion practises

Improving Central Line Insertion

Quality not research
However....• Based on evidence derived from research• Focus on
– sustainable practice vs short intervention– process & outcomes – ongoing measurement

Method - Clinical Practice Improvement
Too complex & time-consuming ...

MethodKeep It Simple• Measure CLABSI• Incorporate change into usual practise • Measure CLABSI• Review individual cases (ICU & IC +/- ID)• Check compliance with insertion process• Keep measuring CLABSI & review

Approach• Assumptions relevant to Australia
– multidisciplinary clinical team– ward rounds occur twice/day
• Establish multi-disciplinary project teams– ICU director & nurse manager or senior dr & ns– Infection Control/ID support– Others as appropriate

Intervention • Joint medical & nursing responsibility• Insertion & maintenance guideline based on
– NHMRC/ACSQHC Guidelines– CDC– Expert group– Core items– Optional items

Insertion Maximum barrier precautions• Hat• Mask• CHG handwash • Sterile gloves & gown• CHG & ETOH skin prep & allow to dry• Full-body drape• Maintain aseptic technique

Checklist

“Reminder”
Proceduralist acknowledges he/she would like to be reminded if he/she misses one of the steps below; eg. “ I would like you to watch me and if you see that I forget an important step in the procedure I want you to tell me”


Other suggestions• CVC (inc swan & vascath) trolley• Appropriate site• Options if rate higher than goal
– chlorhexidine patch at insertion site– impregnated CVC– daily chlorhexidine body wash
• Maintenance– Very limited re-wiring of existing lines– Replace lines with a blocked lumen– No disconnection & re-connection of lines (inc HF)

Guideline contents• Scope• Definitions• Selecting a central line• Selecting a site• Aseptic technique • Maximum barrier precautions• Stopping the procedure if asepsis breached• Daily review
– local infection– need for line

Guideline contents• Line replacement inc re-wiring• Blocked lumens• Changing fluids & administration sets• Needleless connectors• Dressings• CHG patches• Drug administration (CHG & ETOH swabs)• CHG body wash

Support Website • CVC insertion & maintenance guideline • References• Audit tools/checklist• Line day calculator• Secure discussion forum
ANZICS CLABSI Reporting Program

What now? • Establish CLABSI reporting process• Form the team - Dr, Ns, ICP, ?other• Review your protocol• Identify changes required & materials needed (eg.
trolley, big drapes, ?culture)
• Develop education strategies for all staff• Implement changes• Check compliance• Review CLABSI rate & compliance

Counting line-daysLine day counts should be done• 3 times a week, eg. Mon, Wed, Fri• At the same time • By asking the question: Does this patient have a
central line, PA catheter/swan, swan sheath, vascath (or other haemofiltration catheter), or a PICC?
This job does not require nursing/technical knowledgeThis is done by Infection Control in Vic & WA public ICUs

Counting line-daysMon Tues Wed Thurs Fri Sat Sun
Bed 1 1 0 0
Bed 2 0 1 1
Bed 3 0 1 1
Bed 4 1 1 0
Total 2 3 2
1 means the patient in that bed has at least 1 central line0 means either the bed is empty, or the patient doesn’t have a central line