Embed Size (px)
Citation preview

1
Central East Local Health Integration Network CEO Report to the Board
August 24, 2011 The following is a compilation of some of the major activities/events undertaken during the month of July in support of the Central East LHIN’s Strategic Directions;
a) Transformational Leadership, b) Quality and Safety, c) Service and System Integration, and d) Fiscal Responsibility.
Transformational Leadership: The LHIN organization will demonstrate accountability and systems-thinking in all decision-making and leadership actions, reward innovation which is aligned with the Integrated Health Service Plan (IHSP) 2010 - 2013 and model fair, transparent, and honest interaction with one another and with Health Service Providers. Service and System Integration/Quality and Safety: The LHIN organization will create an integrated system of care that is easily accessible, sustainable and achieves good outcomes. Healthcare will be people-centred in safe environments of quality care. The Central East LHIN is working towards achievement of the Strategic Aims of the 2010-2013 IHSP; 1. Save a Million Hours of Time Patients Spend in the Emergency Departments by 2013; and 2. Reduce the Impact of Vascular Disease by 10% by 2013 (2010-2013 IHSP).
Save a Million Hours of Time Spent in the ER Department Emergency Department Process Improvement Program (ED PIP): Wave 4, the last wave of Emergency Department-Performance Improvement Program (ED PIP), has begun with full participation from all remaining Central East LHIN Pay-for-Results (P4R) designated hospitals: Rouge Valley Ajax-Pickering (RVAP), Rouge Valley Centenary (RVC), Lakeridge Health Bowmanville (LHB), and Lakeridge Health Oshawa (LHO). Lakeridge Health – Port Perry (LHPP) is also being included in the Lakeridge Health Corporation (LHC) implementation. The Kick-Off provincial forum for Wave 4 took place on May 25, and the diagnostic forum took place on July 14. The remaining Central Training Forums are scheduled as follows:
Early Pilot September 15, 2011
Roll-out December 1, 2011
ED Pay for Results (P4R) Year III: Emergency Department (ED) performance results for Year III were available to the LHIN, Cancer Care Ontario (CCO), and the Ministry of Health and Long-Term Care (MOHLTC), in the last week of May. However, MOHLTC has not yet published the final formula for recovery of the fixed-funding or to suggest what the recovery formula may be for Physician Initial Assessment (PIA) funding. Therefore, there is no update, at this time further from the information included in the CEO‘s report from May 2011.
2
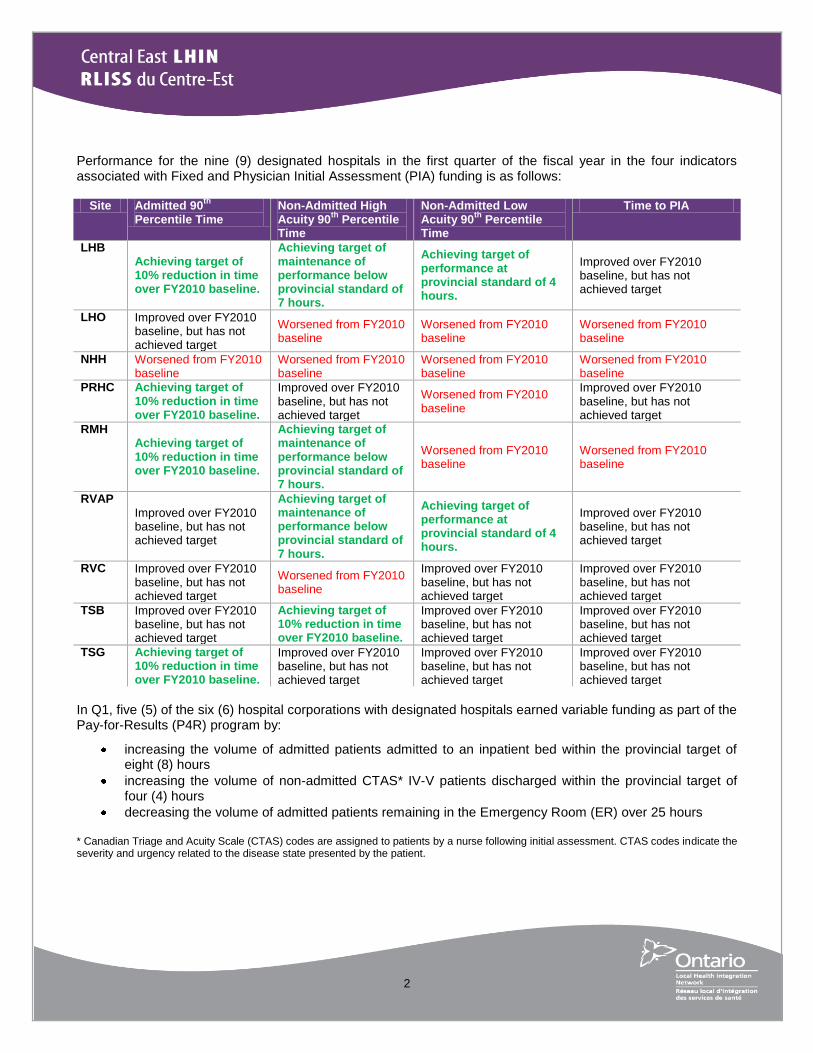
Performance for the nine (9) designated hospitals in the first quarter of the fiscal year in the four indicators associated with Fixed and Physician Initial Assessment (PIA) funding is as follows:
Site Admitted 90th
Percentile Time
Non-Admitted High Acuity 90
th Percentile
Time
Non-Admitted Low Acuity 90
th Percentile
Time
Time to PIA
LHB Achieving target of 10% reduction in time over FY2010 baseline.
Achieving target of maintenance of performance below provincial standard of 7 hours.
Achieving target of performance at provincial standard of 4 hours.
Improved over FY2010 baseline, but has not achieved target
LHO Improved over FY2010 baseline, but has not achieved target
Worsened from FY2010 baseline
Worsened from FY2010 baseline
Worsened from FY2010 baseline
NHH Worsened from FY2010 baseline
Worsened from FY2010 baseline
Worsened from FY2010 baseline
Worsened from FY2010 baseline
PRHC Achieving target of 10% reduction in time over FY2010 baseline.
Improved over FY2010 baseline, but has not achieved target
Worsened from FY2010 baseline
Improved over FY2010 baseline, but has not achieved target
RMH Achieving target of 10% reduction in time over FY2010 baseline.
Achieving target of maintenance of performance below provincial standard of 7 hours.
Worsened from FY2010 baseline
Worsened from FY2010 baseline
RVAP
Improved over FY2010 baseline, but has not achieved target
Achieving target of maintenance of performance below provincial standard of 7 hours.
Achieving target of performance at provincial standard of 4 hours.
Improved over FY2010 baseline, but has not achieved target
RVC Improved over FY2010 baseline, but has not achieved target
Worsened from FY2010 baseline
Improved over FY2010 baseline, but has not achieved target
Improved over FY2010 baseline, but has not achieved target
TSB Improved over FY2010 baseline, but has not achieved target
Achieving target of 10% reduction in time over FY2010 baseline.
Improved over FY2010 baseline, but has not achieved target
Improved over FY2010 baseline, but has not achieved target
TSG Achieving target of 10% reduction in time over FY2010 baseline.
Improved over FY2010 baseline, but has not achieved target
Improved over FY2010 baseline, but has not achieved target
Improved over FY2010 baseline, but has not achieved target
In Q1, five (5) of the six (6) hospital corporations with designated hospitals earned variable funding as part of the Pay-for-Results (P4R) program by:
increasing the volume of admitted patients admitted to an inpatient bed within the provincial target of eight (8) hours
increasing the volume of non-admitted CTAS* IV-V patients discharged within the provincial target of four (4) hours
decreasing the volume of admitted patients remaining in the Emergency Room (ER) over 25 hours * Canadian Triage and Acuity Scale (CTAS) codes are assigned to patients by a nurse following initial assessment. CTAS codes indicate the severity and urgency related to the disease state presented by the patient.
3
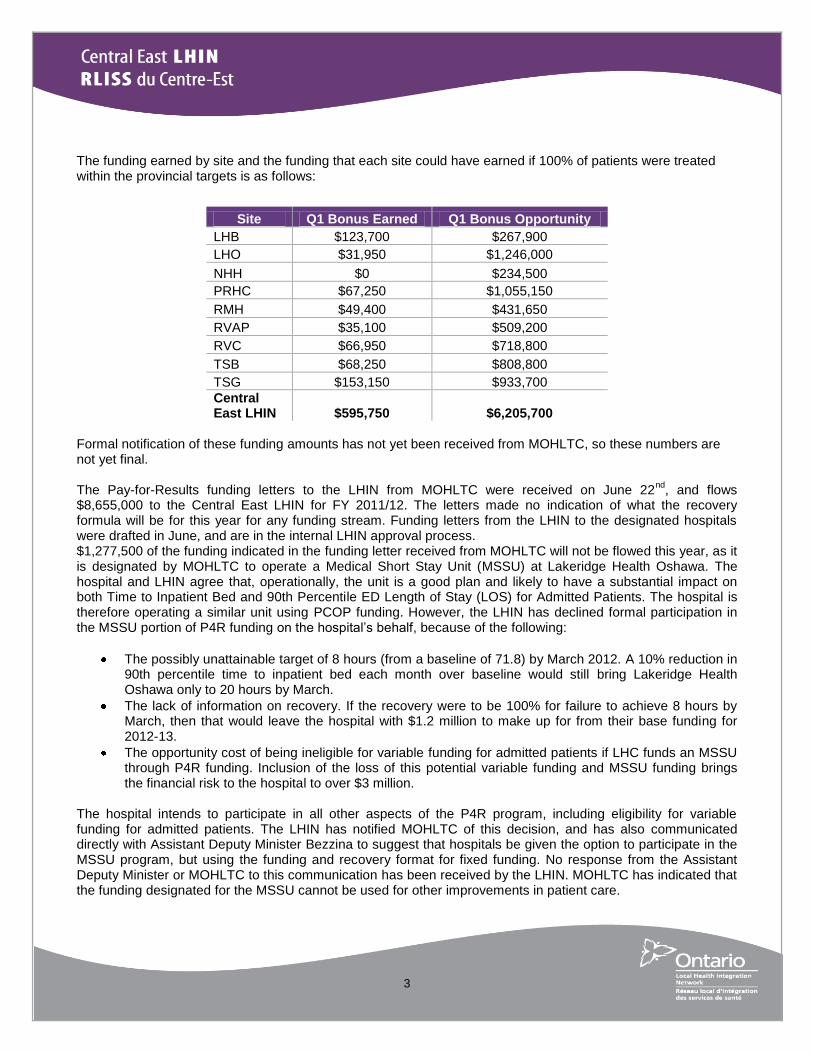
The funding earned by site and the funding that each site could have earned if 100% of patients were treated within the provincial targets is as follows:
Site Q1 Bonus Earned Q1 Bonus Opportunity
LHB $123,700 $267,900
LHO $31,950 $1,246,000
NHH $0 $234,500
PRHC $67,250 $1,055,150
RMH $49,400 $431,650
RVAP $35,100 $509,200
RVC $66,950 $718,800
TSB $68,250 $808,800
TSG $153,150 $933,700
Central East LHIN $595,750 $6,205,700
Formal notification of these funding amounts has not yet been received from MOHLTC, so these numbers are not yet final. The Pay-for-Results funding letters to the LHIN from MOHLTC were received on June 22
nd, and flows
$8,655,000 to the Central East LHIN for FY 2011/12. The letters made no indication of what the recovery formula will be for this year for any funding stream. Funding letters from the LHIN to the designated hospitals were drafted in June, and are in the internal LHIN approval process. $1,277,500 of the funding indicated in the funding letter received from MOHLTC will not be flowed this year, as it is designated by MOHLTC to operate a Medical Short Stay Unit (MSSU) at Lakeridge Health Oshawa. The hospital and LHIN agree that, operationally, the unit is a good plan and likely to have a substantial impact on both Time to Inpatient Bed and 90th Percentile ED Length of Stay (LOS) for Admitted Patients. The hospital is therefore operating a similar unit using PCOP funding. However, the LHIN has declined formal participation in the MSSU portion of P4R funding on the hospital‘s behalf, because of the following:
The possibly unattainable target of 8 hours (from a baseline of 71.8) by March 2012. A 10% reduction in 90th percentile time to inpatient bed each month over baseline would still bring Lakeridge Health Oshawa only to 20 hours by March.
The lack of information on recovery. If the recovery were to be 100% for failure to achieve 8 hours by March, then that would leave the hospital with $1.2 million to make up for from their base funding for 2012-13.
The opportunity cost of being ineligible for variable funding for admitted patients if LHC funds an MSSU through P4R funding. Inclusion of the loss of this potential variable funding and MSSU funding brings the financial risk to the hospital to over $3 million.
The hospital intends to participate in all other aspects of the P4R program, including eligibility for variable funding for admitted patients. The LHIN has notified MOHLTC of this decision, and has also communicated directly with Assistant Deputy Minister Bezzina to suggest that hospitals be given the option to participate in the MSSU program, but using the funding and recovery format for fixed funding. No response from the Assistant Deputy Minister or MOHLTC to this communication has been received by the LHIN. MOHLTC has indicated that the funding designated for the MSSU cannot be used for other improvements in patient care.
4
The Chair of the Provincial ED LHIN Lead group has indicated that there may be an opportunity for the ED LHIN Leads to make recommendations to MOHLTC about recalibration of the Pay for Results program for future years. The provincial Emergency Room (ER) / Alternative Level of Care (ALC) Performance Leads and LHIN Senior Directors are evaluating options to present to MOHLTC. Hospital Scorecards: Monthly scorecards have been developed, tracking the following seven (7) Emergency Department/Alternative Level of Care (ED/ALC) indicators for all Central East LHIN hospitals:
Emergency Medical Services (EMS) Offload Time
90th Percentile ED Length of Stay (LOS) for Admitted Patients (MLPA indicator)
90th Percentile ED Length of Stay (LOS) for Non-Admitted Complex Patients (MLPA indicator)
90th Percentile ED Length of Stay (LOS) for Non-Admitted Minor/Uncomplicated Patients (MLPA
indicator)
90th Percentile time to Physician Initial Assessment (PIA) (P4R indicator)
ALC-LTC Volume (HSAA indicator)
% Alternate Level of Care (ALC) Days (MLPA indicator)
% Hospital Discharges Before 11:00am These monthly scorecards are sent to designated hospital staff accompanied by a LHIN request for a rationale for a given site‘s performance or a plan for how to correct underperformance when necessary. June data will be posted by Cancer Care Ontario in the first few weeks of August, and scorecards will be sent out when this source data becomes available. Home First: The Home First philosophy and the business processes supporting it have been initiated at all eight (8) Central East LHIN acute medical hospitals. Ontario Shores Centre for Mental Health Sciences (OSCMHS) will have its implementation later in FY2011. To date, over 4000 patients have been served through the initiatives supporting the Home First philosophy. The Central East Community Care Access Centre (CECCAC) has project-led the implementation of Home First, including the formation of a LHIN-wide Steering Committee and Implementation Teams and Sustainability Committees at each hospital. Business processes in support of the Home First philosophy are being adopted relatively smoothly at all hospitals across the LHIN with the exception of Lakeridge Health Corporation. Bi-weekly meetings between the Lakeridge Health Corporation senior team and the Central East LHIN senior team are now in place to improve Lakeridge uptake of the Home First philosophy, business processes, and outcomes. The sentinel indicator of Home First is the ALC to Long-Term Care designation rate. As the culture at each hospital changes, the expectation of all staff and all partner organizations is that every admitted patient will be discharged home at the end of his or her acute length of stay, which will then decrease the number of patients designated as ALC. Because ALC patients are discharged from the hospital on a regular basis, a drop in the designation rate will result in a drop in the overall ALC patient volume, which will free up acute inpatient beds. This freeing up of capacity is, in turn, expected to reduce the ED length of stay for Admitted patients. A reduction in the total volume of ALC-LTC designated patients is a requirement in each hospital‘s HSAA. Home First has been successful to date, and further success is expected as the culture is embedded at each hospital. The partnerships that have been developed among the CCAC, the hospitals, and the community service organizations, as a part of Home First, are expected to facilitate further work in 2011-12. The Central East CCAC‘s leadership and industry in rolling out this implementation has been exemplary.
5
GAIN (Geriatric Assessment and Intervention Network): The GAIN Steering Committee met on July 13. Data was presented up to the end of May 2011. During the month of May, there were 223 referrals in total to the four (4) GAIN clinics. Of these, 98 were attributed to TSH, 76 to LHC, 32 to PRHC and 26 to RVHS. Due to some implementation hurdles being experienced at RVHS, LHIN staff and lead GAIN staff of RVHS met to determine how best to move forward. A plan was established and the plan of action will facilitate that a RVHS clinic be fully staffed and operational by the end of August. An overarching communication plan has been developed for all clinics. A branding exercise for the clinics is also underway. The clinics are evolving as a new service in the LHIN, building linkages within and amongst hospitals as well as with community partners. Specialized Geriatric Services – Regional Governance: With the Central East LHIN‘s Board of Director‘s approval to proceed with the establishment of an entity to govern a regional program for specialized geriatric services, an Expression of Interest for a Host Agency was developed and circulated widely to the LHIN‘s health service providers. The Host Agency‘s role will include managing and implementing a recruitment process for entity staff, securing appropriate space, equipment and back office supports for the entity and working with other partners and the LHIN in selecting the initial governance authority for regional specialized geriatric services. The end of this calendar year has been set as the goal by which all three tasks will be completed. A proposal selection team is being assembled. A ―Q&A‖ teleconference sponsored by the LHIN will be held August 9, the deadline for submission of Expressions of Interest is August 16, and the review team meets August 19 with the intent to present a recommendation to the LHIN Board at its August 24, 2011 meeting. Assisted Living Services for High Risk Seniors (ALS-HRS): The Central East LHIN intends to fund new capacity in providing services to high risk seniors living in the community as set out in the Assisted Living Services for High Risk Seniors Policy, 2011 (ALS-HRS) which came into effect on January 1, 2011. A standardized review process was completed in July which scored proposals based on Service Delivery, Compliance, Priority Population, Implementation Factors and Cost of Service. Recommendations will be forwarded for Board approval at the August 2011 Board meeting. The ALS-HRS program represents an important step in meeting a known gap in service that has been identified through stakeholder reports and feedback and confirmed by the findings set out in the Sustainable Access to Community Healthcare Services report. In order to ensure an efficient service, there will need to be a coordination of assessment and delivery services between the Central East Community Care Access Centre (CECCAC) and successful provider(s) within the Community Support Services sector and the CECCAC has played a key role in identification of needs-based ―clusters‖ for purposes of this project. Projected initiation of the program is October 3, 2011. Senior Friendly Hospitals: On July 21, all LHINs across the province received the recently revised ―Provincial Senior Friendly Hospital (SFH) Strategy‖. The Strategy highlights many of the areas the Central East LHIN is excelling at in providing senior friendly practices, and also identified priority areas LHIN wide. The final revised strategy will be released in mid-August in preparation for the LHIN CEO meeting on September 29 when the CEOs will have an opportunity to accept and approve the report. The report will be made available to the hospitals following the September 29 meeting. A LHIN-wide working group will be established in August/September to brainstorm and strategize next steps in the implementation and roll-out phase of the senior friendly initiatives and recommendations. Transitional Care Program: The Transitional Care Program in the Central East LHIN consists of the following: RVHS (20 rehab beds), NHH (8 restorative beds), PRHC (7 interim LTC beds) and Strathaven (15 convalescent care beds). Q1 data reports
6
were submitted to the MOHLTC and to Cancer Care Ontario using the Transitional Care Program Reporting System (TCPRS), which is coordinated through the LHIN office for purposes of populating the Stocktake report. In Q1 2011/12, a high occupancy level was achieved at all sites and Length of Stay (LOS) was managed well within the target range. Excluding the seven (7) interim Long-Term Care beds at PRHC, there were a total of 87 discharges from April to June - only three (3) to long-term care. Residents First Quality Improvement Project: The Central East LHIN Quality Improvement Coach, Cheryl Rosell, is proceeding with engagement of Long-Term Care Homes (LTCHs) across the Central East LHIN but will be taking a more focused approach given the large number of homes in Central East and a revised coaching engagement strategy from Health Quality Ontario. The continued level of engagement with each home is to be finalized following initial contact and Cheryl has reported increasing levels of interest for the Residents First program and activity with the Homes. NPSTAT (Nurse Practitioners Supporting Teams Averting Transfers) Program: In July, a subgroup of the NPSTAT Steering Committee met to discuss the projected deficit at a special budget meeting. The group agreed on an approach to reduce costs through standardized group practices and the need to redesign the service delivery model of the program. The next budget iteration and ideas for a revised approach will be developed and discussed at the August Steering Committee meeting. Mental Health and Addictions (MH&A): Staff have travelled across the LHIN to meet with health service providers regarding the ongoing integration initiatives. A meeting was scheduled on July 7 with Ontario Shores, Lakeridge Health, and the Canadian Mental Health Association – Durham branch around increasing the use of Community Treatment Orders (CTOs) and the accompanying case management for people who are being released from the Forensic Unit under specific circumstances. It was agreed that this would be an opportunity to support clients during their reintegration into the community. Staff met with representatives of the Central East Network of Specialized Care to discuss ways in which the Central East LHIN can work with this network to ensure that people with dual diagnoses are receiving the services they require. Psychogeriatrics was raised as an area for development amongst the service providers in our region, as it relates to challenges faced by dually-diagnosed individuals in need of specific care models. This was an excellent beginning step in this process, which promises to develop further over time. Staff will be attending a meeting of this network in the fall. Central East LHIN staff met with Susan Engles of the Scarborough Hospital (TSH) to discuss the Manse Road Housing Program, and TSH‘s plans for redevelopment. The Scarborough Quadrant group met on July 20 to discuss systemic issues and obtain a better understanding of how the Scarborough health service providers are working together. These discussions will be ongoing. Central East LHIN staff was pleased to approve the Salvation Army‘s plan to continue with their ―Support within Housing Program‖. This has been completed in partnership with the Toronto Central LHIN, and has presented an opportunity to increase service volumes within the existing funding envelope. The Central East LHIN‘s SDI Co-Lead was invited to the ―SAMHSA‖ (Substance Abuse and Mental Health Services Administration) conference in Baltimore, Maryland this past month, to provide insight and expertise in the area of Emergency Department Diversion for people who are at risk of suicide. Information shared at the conference will form the basis for the recommendations that will form the Anti-Suicide Strategy for the United States. This has been noted as an emergent issue in all areas of that nation, with numbers on the rise, particularly in those under the age of twenty-five. Although we have had some information regarding the implementation of the Minister‘s Ten Year Mental Health and Addiction Strategy, we have not received specific
7
details relevant to our HSP‘s in the Central East LHIN. Announcements are expected to be made in the coming months. Community Mental Health North East Cluster: The Canadian Mental Health Association (CMHA) – Kawartha Lakes Branch and CMHA – Peterborough Branch are collaborating with the Central East LHIN to explore integration opportunities in the Northeast The Team has been meeting biweekly since April 2011. The goal is to develop a new service delivery model that will better serve local residents, reach out to clients in underserviced areas, make efficient use of existing resources and strengthen partnerships amongst the two organizations and other providers in the Cluster. Accomplishments to date include the development of a number of tools to support the integration discussions including service mapping and the compilation of key operational information In July, the Integration Planning Team engaged key stakeholders through focus groups and an on-line survey. Potential integration opportunities have been identified current efforts are focusing on the analysis of potential options, while considering the input received from stakeholders and objectives of the initiative. At the present time, the goal is to identify a new draft service delivery model by September for further consultation in October with the intent to deliver the Team‘s recommendation to the respective boards in November 2011. Utilization Management Software Request For Proposals (RFP): The RFP for this tool was published on April 19 to the Public Sector selection site (MERX), and responses were due on May 30. Three responses were received to the RFP. A review by the evaluation team, including representatives from the LHIN, the CCAC, and hospitals narrowed the field to two vendors to provide a presentation—these presentations took place on June 20. Follow up information and clarification on pricing has been undertaken with some further strategizing required by the evaluation team.
Reducing the Impact of Vascular Disease by 10% (save 10,000 patient hospital days) by 2013 Vascular Health Strategic Aim Coalition (VHSAC): The Vascular Health Strategic Aim Coalition was formed in May 2010 to provide leadership to the achievement of the Vascular Health Strategic Aim. The Coalition is comprised of 15 individuals from acute, community and LTC Home sectors. This Strategic Aim Coalition is Co-Chaired by Helen Brenner, VP Northumberland Hills Hospital and Dr. Andrew Steele, Nephrologist, Lakeridge Health Corporation. In June the Central East LHIN endorsed the Coalition‘s proposed Vascular Health Strategy. The Strategy is aligned to the emerging areas of ‗unmet need‘ in the provincial Integrated Vascular Health Strategy. The Central East LHIN has been approached by Ontario‘s Cardiac Care Network (CCN) to contribute to the development of a province-wide Vascular Health Strategy – a meeting with CCN will be held in August. The VHSAC met in July to proceed with the development of the implementation and tactical plan to action the approved Central East LHIN Vascular Health Strategy. This work will continue into September. In July the LHIN Senior Team met with VHSAC leadership and members representing the Regional Diabetes Centre, Ontario Renal Network, and the Ontario Stroke Network. Discussion focused on the Stroke Network scorecard and several of the red indicators for the Central East LHIN. The Stroke Network discussed the establishment of Stroke Centres of Excellence. A caution rose related to transportation issues, as a barrier to access for outpatient stroke care if care is concentrated in a center of
8
excellence. The benefit of inter-professional care for patients with multi-co morbidities (renal/diabetes/possibly stroke) and the similarity of needs across these disease conditions for care from allied health resources were identified. Next steps will include a consultation session/meeting in September to discuss opportunities for cross collaboration across systems. The Regional Diabetes Coordinating Centre will host and offer meeting space. Chronic Kidney Disease (CKD) – Renal Care System In 2010, the province created the Ontario Renal Network (ORN), organized to align to provincial LHIN boundaries. A Central East LHIN Advisory body comprised of medical and administrative leadership from the three (3) Regional Renal Programs: Peterborough and Area (PRHC), Durham (LHC) and Scarborough (TSH) were established. The ORN Regional Director is Jay Wilson and the Clinical Lead is Dr. Andrew Steele. ORN Hospital Accountability Agreements: Year-end reconciliation of volumes have been gathered and expected to be sent out in mid-August. Programs were also asked to account for the volumes associated with the new funding of Modality Education and Access preparation. Rouge Valley Continuous Renal Replacement Therapy (CRRT): A Business Case and draft Tri-Partnership agreement have been completed and sent to the Ontario Renal Network (ORN) for review and approval. Ontario Renal Plan: The ORN is gathering feedback to develop a vision and plan for the Chronic Kidney Disease (CKD) care system in Ontario over the next three years. The Central East LHIN Regional Steering committee and stakeholder input included the following CKD system priorities:
Engage Primary care teams and community based services to support/manage the patients in the early CKD stages - this aligns with the Central East LHIN Vascular Health Strategy;
Ensure equitable access* for Fistula creation across the LHIN. Formalize and strengthen the vascular partnership between PRHC and LHC;
Address In-Centre Capacity (localized), balanced with the growth of Home Modalities - this aligns with the Central East LHIN Vascular Health Strategy;
Formalize pre and post transplantation follow-up in partnership with St. Michael‘s Hospital;
Address barriers to transportation across the LHIN, in particular to reduce the burden on the elderly cohort living on a fixed income (common theme from several stakeholders);
Provide capacity to better manage the complexity of medical and psychiatric challenges (i.e. psychiatric patients requiring hemodialysis, aging patients with dementia and cognitive impairment, Long-Term Care patients requiring Hemodialysis (HD).
Provincial emerging themes (these are emerging/draft themes which will be refined following the consultation):
Redefine the current model of care and move towards a balance of community versus hospital care
Increase use and engagement with Primary Care, particularly for the care of patients in the earliest CKD stages
The potential for Renal Campuses with ―one-stop shopping‖ for services along the entire care continuum
The potential for Centres of Excellence while avoiding inequity of access
Achieve a truly patient-centered, innovative system of care that enhances partnerships, and integrates community-based and hospital services
9
ORN will now seek broader stakeholder input through Regional Administrative Leads Network of Ontario (RALNO) and the Kidney Foundation of Ontario (KFO). Executive Lead ORN – Treva McCumber is leaving the ORN effective August 8, a replacement is to be determined. In the interim, the Regional Directors will report to Helen Angus VP at ORN.
Supporting an Integrated Roll-out of the Ontario Diabetes Strategy Central East LHIN Diabetes Regional Coordinating Centre (DRCC): The DRCC has been established to organize, integrate and coordinate regional diabetes programming that includes primary care, specialty care and diabetes education programs and other community resources. Central East LHIN has the highest rates of diabetes of all the 14 LHINs. Complex Care Diabetes Centres (CCDCs) Under the leadership of the Diabetes Regional Coordination Centre and Marsha Watts, leaders in diabetes care from across multiple Central East LHIN HSPs collaborated to develop and submit to the Ministry, a proposal to establish a Complex Care Diabetes program for Central East LHIN. The Central East LHIN was one of three LHINs offered this opportunity. The Central East Local Health Integration Network (Central East LHIN) diabetes stakeholders, with the Central East Community Care Access Centre (CECCAC) as the Program Sponsor, have developed an Innovative Diabetes Care Delivery Model that will provide the infrastructure to support complex diabetes care throughout the Central East LHIN by improving care coordination, patient system and clinical navigation and access to existing and needed services within all three geographic planning clusters of the Central East LHIN (Durham, North East Cluster, and Scarborough). A single site CCDC to serve the entire Central East LHIN would not achieve the objectives of the proposal nor maximize patient experience, leverage capacity in the current system or population outcomes. The proposed model includes CCDC sites distributed throughout the three Central East LHIN clusters and cited within the hospitals that host Regional Chronic Kidney Disease (CKD) Programs: The Scarborough Hospital, Lakeridge Health Corporation and Peterborough Regional Health Centre. Partnerships with other Central East LHIN HSPs to support care will be essential as the CCDC develops. The following HSPs participated during the proposal development and identified their contributions toward an effective CCDC – Ontario Shores Centre for Mental Health Sciences (diabetics with mental health needs), Carefirst, Scarborough Centre for Healthy Communities.; the Charles H. Best Diabetes Centre (Type 1 Diabetics), Ross Memorial Hospital, the Rouge Valley Health System and the Scarborough Centre for Healthy Communities. Engagement of these collaborating stakeholders and other HSPs will continue during implementation. The core functions of the Central East LHIN CCDC model are centralized triage and access to services, coordinated care delivery, effective and supportive disease management. Involvement of the patient‘s primary care provider is a central principle for effective treatment and on-going management of patient needs. The core functions include the following:
intake & assessment of needs;
service care planning;
reassessment; case conferencing and, case closure
clinical service coordination and system navigation / case management;
monitoring and follow-up ;
care plan implementation;
10
The partners collaborating on this initiative have developed relationships over their shared work in the area of diabetes; the collaborative approach to the development of this proposal has created a common vision, and strengthened the relationships necessary to quickly begin planning and implementation for a LHIN-wide CCDC. If selected by MOHLTC, the Central East LHIN CCDC would be able to begin seeing patients within 6 months from government approval with full implementation at all sites in Central East LHIN by April 1, 2012. The CCDC anticipates serving 1400 complex diabetes patients per year. Central East LHIN Self Management Program: In April 2010, after successful completion of the Central East LHIN Self Management Training for Consumers and Caregivers project, a permanent Central East LHIN Self Management program was created under the leadership of the CECCAC. This was the first provincial roll-out of a LHIN-wide Self Management Program. A LHIN and CCAC Memorandum of Understanding (MOU) are in place. From April 1 – June 30, 2011 (Quarter 1) the program delivered twenty-seven "Living a Healthy Life" workshops throughout the LHIN and reached over 340 individuals. The clinician training side of our program has strengthened significantly over the first quarter with the addition of a Coordinator supported by the Ontario Diabetes Strategy to focus specifically on clinician training and mentorship. A mentorship steering committee is being assembled and additional mentors will be trained to provide mentorship supports to graduates to increase results in this area. Recruitment of Self-Management Champions has begun to promote self-management practices within health care organizations across the LHIN. The Ontario Diabetes Strategy (ODS) Self-Management Project team has been in active communication with the CECCAC and self-management lead agencies from other LHINs about the funding package of $296,300 for 2011-12. This additional funding presents an excellent opportunity for our Central East LHIN Self-Management Program to engage in quality improvement and service expansion. The Central East LHIN Self Management program is an active leader in the provincial Community of Practice that has been created from among the ODS self-management lead agencies across Ontario. www.healthylifeworkshop.ca
Transformational Leadership Integration: Most of the Integration activities have centered on the work being done in the Northeast Cluster regarding CMHA Peterborough and CMHA Kawartha Lakes. Initial discussions are also underway with mental health providers in the Durham Cluster. The Integration Team is in the process of finalizing the Integration Tool Kit, and an Integration Repository has been developed that tracks Integrations that have been completed, those in process, and those that are in development. Once this has been finalized, the Repository will be posted on SharePoint and updated on a cyclical basis, much in the same manner as the CEO report is produced. This will provide an up to date listing of the Central East LHIN‘s Integration activities, past, present and future. The Team is also working on processes for prioritizing Integration initiatives and a plan for implementing. To date, staff have prioritized integration activities where either risk or other factors have presented opportunities and are in alignment with the Central East LHIN‘s Clinical Services Plan/IHSP.
11
Central East LHIN Hospice Palliative Care Network (CEHPCN): The month of July has largely been spent working on the Central East Strategy for Hospice Palliative Care. A presentation was made to the Primary Care Working Group which was very well received and supported the need for a coordinated effort. The draft strategy was sent out to various community stakeholders for input (e.g., Rainbow Health Ontario, Community Development Council of Durham) to ensure that it fairly addresses the needs of diverse communities. The Network intends to submit their draft Strategy to the LHIN staff team for consideration and advice on next steps in September. The Network Coordinator will be presenting at the National Hospice Palliative Care Conference, taking place in St. John‘s Newfoundland in early September. This presentation will focus on rural hospice care, the needs of rural communities and the development of care options in the Central East LHIN.
French Language Health Services (FLHS) French Language Services Implementation Plan (FLSIP): A revised version of The Central East LHIN‘s FLSIP following the agreement with the Entity #4 has been submitted to the Senior Team for their review. Translation Policy: A translation policy has been drafted based on the OPS Communications in French Directive. The Translation Policy will be presented to the Senior Team early August 2011 and then to the Audit Committee for approval. French Language Website: A meeting between the Communication Lead, the web designer and the FLS Coordinator will take place in early August 2011. In order to facilitate the construction of the French website and because of the ongoing updates to the English website, French sections of the site will go live as they are developed. Meeting with the Entity Planning Agent: The first meeting between the Planning Agent from the Entity #4 and the Central East LHIN FLS Coordinator took place early August 2011. Several topics were reviewed such as the Entity; the Central-East LHIN and the LHINs in general; our Francophone population as well as the revised number of Francophones in the Central-East LHIN based on the new definition; the identified and designated HSPs, the FLHS Collaborative – its current and future role, the Joint Action Plan and more specifically we discussed the ―self-management‖ of diabetes. The outcome was a decision to have a joint meeting between the FLS Coordinators from the three LHINs and the Entity‘s two Planning agents. We also agreed to have a similar regional meeting with the HSPs offering the ―self-management‖ programs in the three LHINs. Meeting with FLS Coordinators
FLS Coordinators of Toronto Central, Central, North Simcoe Muskoka and Central East met early July 2011 to
discuss and exchange on several issues:
The role of the French Language Health Planning Entities (FLHPE) in advising the LHINS in identifying or designating an agency under the FLSA. The LHIN has the final say in this.
The role of FLS coordinators with the arrival of the Entities.
The impact of the amendment aims at granting greater services in French to Francophone in their interaction with CCAC (Community Care Access Corporations).
12
The impact of the Ontario Regulation 284-11 made under the French-Language Services Act, 1986 aims at ensuring that francophone have access to provincial government services in French provided by third parties by eliminating loopholes.
The next meeting is scheduled for September 13, here, at the Central East LHIN.
Aboriginal Services First Nations Health Advisory Circle and Métis, Non-Status and Inuit Health Advisory Circles: The Central East LHIN Métis, Non-Status and Inuit Health Advisory Circle did not meet in July due to the holiday plans of the members. The Circle will meet again on August 24, 2011. The major task of the Circle at this point is to oversee the administration of the Métis Health Needs Survey that is being conducted in partnership with the Southeast LHIN. We are also working to re-establish the membership of those organizations who have not been attending meetings. The First Nations (FN) Circle met on July 6, 2011 at the Scugog First Nation. Representatives from the Central East Stroke Network attended, along with their local contacts. Their presentation and resource materials were very well received, and plans were discussed to have the Stroke Network attend the FN and provide presentations to their communities. The other topic of interest was the follow up on the Alderville FN concerns regarding the Cancer rates in their community. This has raised a larger issue of data, and what is both gathered and available to Aboriginal communities in the LHIN and in the Province. Cancer Care Ontario has been approached in order to arrange a meeting, and the FN Health Advisory Circle is awaiting their response. Brian Joyce of the Oshawa Community Health Centre (CHC) has asked to attend each of the Aboriginal Health Planning Circles in order to provide a presentation of the services they have available, and to discuss how the Oshawa CHC might effectively support Aboriginal communities in the Central East LHIN. The FN Circle will meet again in September. We are in the process of arranging a joint meeting between the two Circles as outlined in the Terms of Reference for each. The purpose of the joint meeting is to discuss common concerns and to communicate with each other regarding the activities of each Circle. This date will be provided to the Senior Team and Board of the Central East LHIN as soon as it has been finalized.
Service and System Integration/Quality and Safety
Provincial ALC Team Visit: Staff have developed an internal response to the recommendations contained in the report provided by Dr. Walker. While there are areas for improvement, to a great extent, the recommendations have been met. It is extremely difficult for a team of individuals to understand everything that is happening within a 48 hour stay. Dr. Walker‘s team had a mammoth task which resulted in some new ideas as well as some ideas that we were in the midst of implementing but didn‘t get to communicate clearly. Staff will continue to ensure the necessary uptake of solutions that will move us towards our MLPA targets.
Focus on Accessible Health Care Ontario eHealth Blueprint: As presented by eHealth Ontario, the 2015 Blueprint sets out the foundation upon which Central East LHIN will collaborate to deliver Ontario‘s electronic health record (EHR) by 2015. This Blueprint builds from previous iterations of Ontario‘s technology architecture framework – including the 2007 Blueprint – and is part of a technology refresh program. The refresh is designed to better enable us, our partner agencies and other key stakeholders to realize the potential we can achieve by building on our strengths locally and provincially. The

13
refresh program will ultimately include more than just the Blueprint – it will encompass the logical, or detailed architecture; asset inventory; the EHR roadmap – all supported by a strong governance structure. An information session was held on July 21, eHealth Ontario staff delivered and shared the Blueprint, and future direction on other refresh initiatives as they are being scheduled over time. Chief Information Officers, Information Management Information Technology Directors were present along with eHealth Steering Committee members, the Primary Care Working Group, VP/CNE, and members from the eHealth Clinical Advisory Group. The Central East LHIN eHealth team will focus on revising the eHealth strategic plan based on the Blueprint and the tactical roadmap that is expected to be published by eHealth Ontario in September/October timeframe. Timely Discharge Information Systems (TDIS) – Phase I and II: The Timely Discharge Information System (TDIS) has been developed to ensure family doctors and other community physicians receive the information concerning a patient‘s hospital stay within 72 hours of transcription from the hospital. TDIS continues to add new physicians weekly to receive live transmission of patient discharge summaries and reports directly into their information systems. All four (4) client management system (CMS) vendors (OSCAR, Purkinje, P&P Data Systems, Abelmed) completed their Physician Interface development and user acceptance testing. 14 pilot physicians are now turned over to receive live data via TDIS. There are 150+ physicians currently receiving discharge summaries and other reports into their clinical management systems (CMS) via TDIS. More than 10,000 reports are being accessed on a monthly basis and early feedback supports the fact that clinicians are better able to make timely and informed decisions for patient care. Proposed phase 3 plans are to include the delivery of laboratory results and pathology reports, the proposals were submitted to eHealth Ontario and cGTA for consideration. The support for the expansion is positive. The next steps are to determine the magnitude of costs and submit a formal change request to cGTA for funding allotment. The TDIS project champion, Dr. Chris Jyu will be presenting on TDIS at the Healthcare Interoperability Summit on September 29. eReferral – Primary Care to Specialty: The eReferral–Primary Care to Specialty pilot project will automate referrals from Primary Care physicians to a Specialist or Specialty Services jointly with the South East LHIN and Central East LHIN. The goal is to improve the process, provide two-way communication for these physicians and provide tools for primary care to improve the referral process. Staff have been assigned the responsibility to assist with the finalization of User Acceptance Testing for signoff, with a focus on stakeholder engagement to bring on Physicians to adopt the system for the Mental Health referral pathway, as well as looking for opportunities to expand beyond Mental Health referrals.
Enablers – e-Health: CCIM – Community Care Information Management – Tool Adoption The CCIM project consists of supporting the implementation of the Human Resources Information System (HRIS) and the various Common Assessment tools (CAT) within the Central East LHIN. Two CCIM tools are being implemented that impact the Hospitals and CCAC sectors, namely OCAN and IAR, which will allow hospitals to view all assessments by patient in a central repository and storage environment for OCAN and RAI-MH. OCAN – Ontario Common Assessment of Need Tool: A total of 15 Health Service Provides (HSPs) in the Central East LHIN are participating in the implementation of the Ontario Common Assessment of Need (OCAN) and the Integrated Assessment Record (IAR). Privacy &
14
Security Implementation Training will be held on August 17 and 24 in Oshawa and Peterborough (respectively) HSPs continue to participate in regular teleconferences with Coordinators, Executive Leads and Technology Leads.Typically these teleconferences are for the HSPs and CCIM to discuss any challenges, issues and progress through implementation. IAR - Integrated Assessment Record Repository and Viewer: This initiative is being rolled out to include the CCAC assessment and the RAI-MH for Hospital mental health inpatients the target completion date is November 2011. CCIM has been identified to provide project support, funding (partial), training, helpdesk, and implementation support implementing in all LHINs. Central East LHIN will be providing coordination and communication support. Together with the Central, Toronto Central, Central West, South West and North Simcoe Muskoka LHINs, Central East has joined an IAR steering committee to facilitate planning and shared decision making. One time implementation funds will be made available by the Community Mental Health CAP Project Team to support eligible expenses of the HSP's implementation of OCAN. The Project Team will provide Implementation Funds to support the successful completion of the Implementation Project Milestones. The Implementation Funds are to be used by the HSP only to support its expenses of the Implementation Project including hardware, software, resource backfill and administrative costs. OHRS/MIS - Ontario Health Care Reporting Standards/Management Information Systems: The LTCH OHRS/MIS Project is dedicated to implementing OHRS – provincial reporting standards for collecting financial and statistical data - across the LTCH sector. The OHRS/MIS standards will ensure consistent and accurate reporting, which will enable both the province and LTCH sector to have improved access to useful information for sharing best practices, enhancing operations, tracking trends, planning and bolstering accountability. After completing OHRS training, homes can choose a software solution- free of charge during implementation - to facilitate their OHRS/MIS submissions. On June 23, the Central East LHIN and representatives from CCIM met with Long Term Care Home sector stakeholders from across the Central East region. The event provided the LHIN and CCIM with an opportunity to show how OHRS/MIS could support the sector's achievement of the LHIN's Strategic Aims. There are seven (7) LTC homes that have implemented, are in progress, or that have shown interest in implementing one of CCIM‘s offered software solutions: Community Support Services Common Assessment Project (CSS CAP) In order to better meet the diverse needs of a broad client base, the CSS sector has identified the opportunity to implement a standardized assessment. The interRAI Community Health Assessment (CHA) is the instrument chosen to make this vision the new reality. The interRAI CHA is a standard tool for community support services that allows for data collection on a wide selection of community support services to support evidence-based care while informing future program development and resource allocation. The Central East LHIN is extending an invitation to representatives from across the Community Support Service (CSS) agencies in the LHIN to express their interest in participating in a new Central East LHIN CSS CAP Steering Committee The objective of the working group is to provide direction, escalate or resolve any issues over scope, business boundaries, and quality of deliverables as part of the Central East LHIN CSS sector implementation of the interRAI CHA common assessment. In addition, the steering committee will keep stakeholders informed of any potential impact on their areas of work, and act as messengers and sponsors for project communications.
15
cGTA – ConnectingGTA: ConnectingGTA is a project with the five (5) GTA LHINs structured to ―integrate electronic patient information from across the care continuum, and make it available at the point-of-care, to improve the patient and clinician experience‖. The ConnectingGTA project will allow 700 service providers to securely share patient health information across the five (5) GTA Local Health Integration Networks (LHINs). Currently, electronic health information is contained in silos within the system. Over time, all 700 service providers will be connected under one ―electronic roof‖ – allowing patient information to move from one service provider to another within the system. With the release of the ConnectingGTA Back-End Request for Proposals (RFP), the project team has now updated the multi-year timeline based on recently completed milestones and input from the project‘s Steering Committee. Activities for the month ahead include the ongoing procurement activities for cGTA‘s Back-End components (Clinical Data Repository, Health Information Access Layer), developing requirements for the cGTA Front-End component (Provider Portal) and working with Foundational Initiatives to increase the sharing of clinical data at the local levels, including populating the Ontario Laboratories Information System (OLIS). A Bidder‘s Conference was held on July 14, and the responses to the first set of questions have been shared via MERX. Vendor responses indicate significant interest in the project and the team is now focusing on finalizing members for the various evaluation committees. Steering Committee members have now confirmed the selection criteria and process to determine the first wave of participants that will contribute and use the ConnectingGTA solution. Health Service Provider executives will be invited to learn more about the project, as well as about the site selection criteria and process at the information sessions
Fiscal Responsibility: Resource investments in the Central East LHIN will be fiscally responsible and prudent: Funding and Allocations: The following funding letters were issued in July:
2011-12 Opening Base Allocation letters for all sectors. Since the funding reflects base and annualized funding provided last year, the performance requirements are as per the H-SAA / M-SAA agreements. 2011-12 Municipal Taxation for Hospitals $308K – MOHLTC provides a nominal payment for all public and specialty psychiatric hospitals as compensation in lieu of Municipal Taxes. The funding is calculated at the rate of $75 per ―Rated Bed‖.
2010-11 ED Pay for Results Q4 Premium funding to Hospitals $601K – This one-time funding is part of the Variable Incentive Payment component of the Pay-for-Results Program and acknowledges that the hospital exceeded the number of patients treated within the 4 and 8 hour targets above baseline at a rate of $100 per minor/uncomplicated patient discharged within 4 hours and $500 per admitted patient meeting the eight hour target.
2010-11 one-time converted to base funding $4M. This funding is through the Aging at Home (AAH) Strategy Year 3 and represents a continuation of 2010/11 one-time funding which was later converted to base funding.
CCAC Care Connector one-time funding $255K – one-time funding for salary and benefits for 3 CECCAC based Care Connectors (RN or RPN), representing additional hours of nursing service and resulting in an increase to Full-Time Equivalent (FTE) positions.
Durham Mental Health Services one-time Urgent Priority Funding (UPF) $400K – To provide 10 new Crisis Beds to the Elliot House facility (Durham Area) effective April 1, 2011.
16
Chronic Care Funding for Hospitals $49K – This is one-time funding of $.82 per day per occupied chronic care bed provided in lieu of a co-payment increase.
2011-12 CCAC Nurse-led Long Term Care Outreach Team Project $250K – This funding is intended to cover the salary and benefits for 3 full-time equivalent nursing positions.
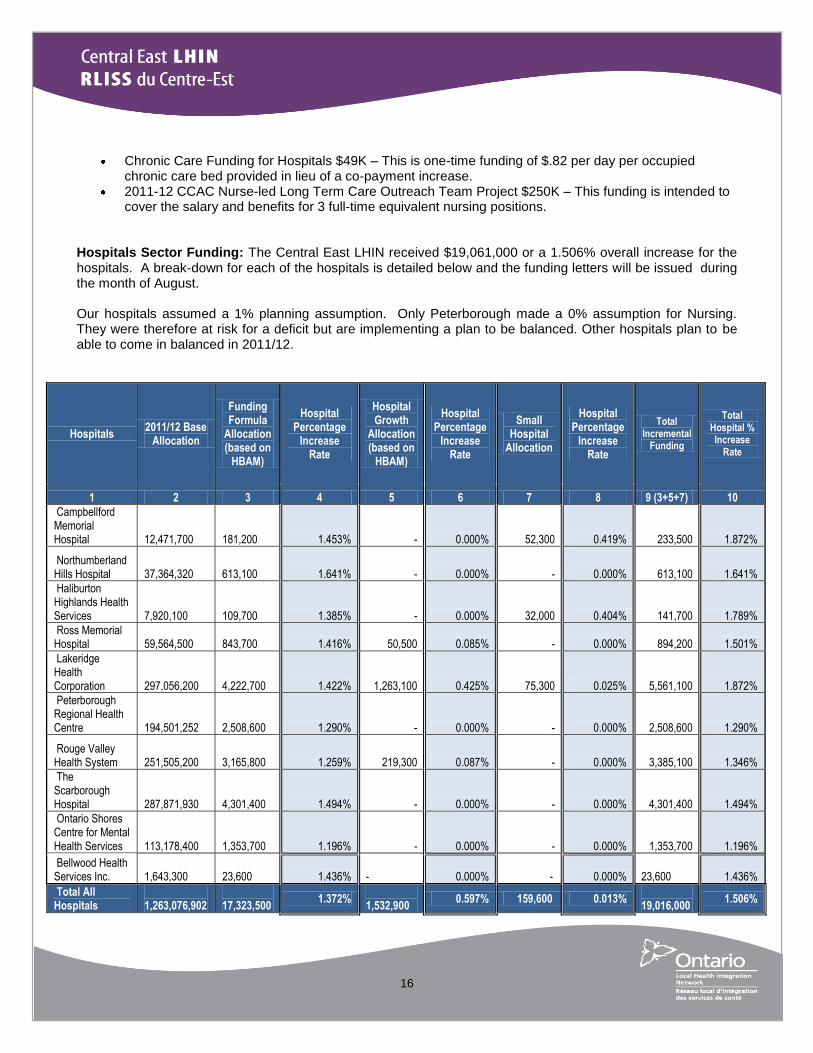
Hospitals Sector Funding: The Central East LHIN received $19,061,000 or a 1.506% overall increase for the hospitals. A break-down for each of the hospitals is detailed below and the funding letters will be issued during the month of August. Our hospitals assumed a 1% planning assumption. Only Peterborough made a 0% assumption for Nursing. They were therefore at risk for a deficit but are implementing a plan to be balanced. Other hospitals plan to be able to come in balanced in 2011/12.
Hospitals 2011/12 Base
Allocation
Funding Formula
Allocation (based on
HBAM)
Hospital Percentage
Increase Rate
Hospital Growth
Allocation (based on
HBAM)
Hospital Percentage
Increase Rate
Small Hospital
Allocation
Hospital Percentage
Increase Rate
Total Incremental
Funding
Total Hospital % Increase
Rate
1 2 3 4 5 6 7 8 9 (3+5+7) 10
Campbellford Memorial Hospital
12,471,700
181,200 1.453%
- 0.000%
52,300 0.419%
233,500 1.872%
Northumberland Hills Hospital
37,364,320
613,100 1.641%
- 0.000% - 0.000%
613,100 1.641%
Haliburton Highlands Health Services
7,920,100
109,700 1.385%
- 0.000%
32,000 0.404%
141,700 1.789%
Ross Memorial Hospital
59,564,500
843,700 1.416%
50,500 0.085% - 0.000%
894,200 1.501%
Lakeridge Health Corporation
297,056,200
4,222,700 1.422%
1,263,100 0.425%
75,300 0.025%
5,561,100 1.872%
Peterborough Regional Health Centre
194,501,252
2,508,600 1.290%
- 0.000% - 0.000%
2,508,600 1.290%
Rouge Valley Health System
251,505,200
3,165,800 1.259%
219,300 0.087% - 0.000%
3,385,100 1.346%
The Scarborough Hospital
287,871,930
4,301,400 1.494%
- 0.000% - 0.000%
4,301,400 1.494%
Ontario Shores Centre for Mental Health Services
113,178,400
1,353,700 1.196%
- 0.000% - 0.000%
1,353,700 1.196%
Bellwood Health Services Inc.
1,643,300
23,600 1.436%
- 0.000% - 0.000%
23,600 1.436%
Total All Hospitals
1,263,076,902
17,323,500
1.372% 1,532,900
0.597% 159,600 0.013% 19,016,000
1.506%
17
The 1.5% increase to the hospital sector allocated the three components of the funding increase to base budgets as follows. (Note that in 2010/11, the Ministry provided separate funding for high growth and small hospitals in addition to funding formula increase. For 2011-12, these three components are part of the overall 1.5% increase). See Appendix A for more information on the 2011/12 Hospital Allocation Funding Methodologies.
Funding Formula increase for 2011-12 is based on HBAM methodology. . High Growth funding allocation is targeted to approximately 25 percent of hospitals serving
Ontario‘s fastest growing communities based on HBAM service growth between 2009/10 and 2011/12.
For Small Hospital funding, small hospitals and small sites of multi-site corporations are funded if they have less than 2,700 acute inpatient/day surgery HBAM weighted cases per year for the past two years (equivalent to 2,500 PAC weighted cases used previously). Allocation is pro-rated based on 2010/11 base budgets of eligible hospitals.
Hospital Capital Issues: Several major projects are being reviewed by MOHLTC in terms of where they fit in their multi-year investment plan:
Ross Memorial Hospital (RMH) – near final reviews and settlement is in progress for the restructuring/expansion project: The construction project consisted of new construction and renovations to accommodate new rehabilitation services (16 beds), new adult mental health services (15 beds) and expanded complex continuing care services (11 new beds, 59 total beds). The hospital now has capacity for 218 beds.
As well RMH‘s construction of a 15 station 7,080 sq.ft. (5,710 sq.ft of new space; renovation of 1,370 sq.ft) dialysis unit as a satellite of the Peterborough Regional Health Centre‘s (PRHC) Chronic Kidney Disease Centre was approved for construction. A 2-storey addition will be required to support and accommodate the 15 station dialysis program on the ground floor, and to shell in (at the hospital‘s sole cost) the 2nd floor (5,747 sq.ft.) for potential future growth. The Hospital is working with the ministry to proceed with the settlement of final costs.
We are pleased to announce that RMH‘s proposed upgrade to key Infrastructure Systems (East Wing: Air Handling, Mechanical, Electrical, and Life Safety Systems; West Wing: Air Handler) and request for funding has been approved (less than $10M small project).
Peterborough Regional Health Centre (PRHC): The MOHLTC has now confirmed that PRHC can tender the Nicholls building demolition project without Ministry permission to do so. PRHC and the Ministry are now working with the construction monitor to finalize the forms and other paperwork in order to see a settlement on this project. Hospital Sector Performance: Results for the 2010/11 fiscal year were provided in June. Hospital performance for six months ending September 30, 2011, will be received in October 2011. Following staff review, a summary will be provided as part of the November CEO Report. Broader Public Sector Accountability Act, 2010 (BPSAA) Reporting: Following discussion at the June Hospital CCAC Financial Leadership Group (HCFLG) meeting, hospitals have now been provided with a directive with respect to Reporting Requirements under the BPSAA. This Directive is issued by the Minister of Health and Long-Term Care under the authority of subsection 15(3) of the Act and every hospital is required to comply.
18
Every hospital is required to submit to the Central East LHIN, the required attestation, approved by the hospital‘s Board covering the Reporting Period (i.e. April 1 to the following March 31), by June 30 of every year. Every hospital is required to post its Board-approved attestations on its public website by August 31st of each year. Every hospital must complete an expense report, in the prescribed form, for each Designated Individual, and post the completed form in an area on its public website that is clearly and readily accessible to the public. Every hospital must post the required information on a semi-annual basis beginning in the 2011/2012 Fiscal Year. Expenses must be posted no later than 60 days following the end of the semi-annual reporting period. Each posting must include the required information in respect of all expenses approved within the applicable period. Every hospital shall submit its Reports to the Central East LHIN by June 30th every year, starting in 2012. The reporting period will be from April 1, 2011 to March 31, 2012.
Community Sector Funding/Multi-Sector Service Accountability Agreement (M-SAA): In a letter dated July 22, 2011, the Ministry informed the Central East LHIN that it would provide $9,773,400 or 3% in new annualized base funding effective April 1, 2011 for the 2011-2012 funding year to support specific investments in the community sector, subject to the following conditions:
a. 1.5% of the 3% base increase is to be allocated to all community health service providers as a base increase to maintain and/or enhance service delivery;
b. The LHINs will have the flexibility to allocate the remaining 1.5% of the 3% base increase to targeted priorities identified by the ministry as follows:
Community Care Access Centre (CCAC)
LHIN-wide Home First (Service Maximums)
School Health Support Services
Support for implementing new nursing initiatives Community Support Services (CSS)
Adult day programs for frail elderly and/or those with cognitive impairments
Caregiver services/respite services
Homemaking to support frail clients to remain independent in the community Assisted Living Services in Supportive Housing (ALSSH)
Support the implementation of the updated Assisted Living Services for High Risk Seniors policy
Community Mental Health & Addictions (CMH&A)
Enhanced services for youth and young adults Community Health Centres (CHC)
Increase services to those at high risk for emergency room admissions
Support to implement new nursing initiatives
c. The LHIN shall amend its Multi-Sector Accountability Agreement (M-SAA) with its health service provider to reflect the new funding increase to the health service provider and any conditions or performance expectations related to this increase.
19
In the interest of consistency in communicating the increase to the health service providers, the Central East LHIN participated in a LHIN-wide CEO teleconference on August 2, 2011 to establish Process, Principles and Actions for the 3% LHIN allocation. The Central East LHIN will implement a 1.5% (i.e., the first half of the 3%) increase to the base funding provided to health service providers for each of the following community services: Community Care Access Centres; Community Support Services; Assisted Living Services in Supportive Housing; Community Mental Health and Addictions Services; Acquired Brain Injury Services; and Community Health Centres. The calculation of the 1.5% increase is based on each provider‘s 2011/12 opening eligible base funding allocation. This excludes one-time funding amounts, psychiatric outreach medical salaries, base physician compensation, base sessional fees, and related annualization of same. This 1.5% increase is being provided to enable the HSP to maintain or enhance the delivery of existing services and is subject to the same terms and conditions set out in the current M-SAA. The Central East Community Care Access Centre (CECCAC), expressed concerns that if CECCAC was not allocated the full 3%, it would be further challenged regarding the sustainability of the Home First program. Please see attached monthly report submitted by the CCAC in Appendix B. CHC/CSS/CMHA Performance and Risks: The 2010/11 Performance Reports have been received. Staff are analyzing the submissions and following up with agencies on performance issues. It is expected that a 2010/11 M-SAA Performance Dashboard will be provided to the Central East LHIN Board in August. Capital projects Port Hope Community Health Centre (CHC) Diabetes renovation project – The Port Hope CHC is in need of additional space to house their third Diabetes Education Clinic (DEC) and has applied to the Ministry for approval to use current physician funding for this purpose. Brock CHC has received approval to proceed with tendering a contract for their new building. This will eventually provide much needed space, all in one location, for the CHC to provide the required services to their community. The Youth Centre expansion renovation project is just beginning. They have received approval to go to tender on the renovation and are planning to start construction in September. Web Enabled Reporting System/Self Reporting Initiative Update: The Health Data Branch (HDB) within the Ministry of Health and Long-Term Care (MOHLTC) is implementing the Self Reporting Initiative (SRI) to replace the current Web Enabled Reporting System (WERS) to support the Ministry‘s commitment to implementing new technologies. SRI will be replacing WERS in 2012 as WERS is no longer a sustainable system. The MOHLTC has just completed a communication notice to extend WERS access from July 31, 2011 to be available during the SRI deployment. WERS access during the deployment stage will allow for a period of transition between systems. Dates for SRI communication, training, data migration and demos will be communicated by HDB before November 2011.
MLPA Performance Requirements and Risks: In May, the Central East LHIN met all surgical and diagnostic imaging (DI) Wait Times targets, except for MRI. Regarding MRI, the Ministry-specified target of 63 days will be difficult to meet. The Central East LHIN has provided analysis to the Ministry that demonstrate this target is overly aggressive. Repatriation of Central East LHIN residents continues to be a factor especially at Lakeridge Health Corporation (LHC). Residents find it more convenient to now access MRI services locally, driving up the demand and wait times.
20
Central East LHIN staff had a meeting with all Diagnostic Imaging (DI) directors in July to understand their challenges/issues to reach the 63 day target. The DI Working Group Chair, along with other members of the DI Working Group have been invited to the monthly Wait Times Strategy Working Group meetings to work more closely in achieving the Wait Times target. One of the planned mitigation strategies is to purchase additional MRI volumes in the fourth quarter from savings resulting from delays in installing new MRI machines at two of our hospitals. The LHIN will also provide evidence-based analysis on repatriations to the Ministry to illustrate the impact on our ability to meet the 63 day target. Hospital Service Accountability Agreement (H-SAA): The Joint Ministry-LHIN workgroup on Hospital Accountability Agreement negotiations plans to provide guidelines on the 2012-13 negotiations in September. Central East LHIN, through the Hospital-Community Care Access Centre Financial Leadership Group (HCFLG) has begun work by asking the hospitals to begin developing assumptions on hospital expenditure categories. Health System Indicator Initiative (HSII): The purpose of the HSII is to establish a systemized approach in the identification, development, maintenance and reporting of performance indicators by coordinating the expertise of various health system partners. These partners include representatives from the LHINs, Ministry of Health and Long-Term Care (MOHLTC) and health service providers from the community, long-term care and hospital sectors. Updates from phase 2: The HSII Steering Committee, with the help of the All Sector Strategy Consultation Team, is focused on identifying gaps within the LHIN Performance Indicator Framework and assessing opportunities for development in preparation for the next cycle of the Service Accountability Agreements (SAAs). The HSII Technical Working Group, with the help of the Sector-Specific Technical Consultation Team, identified that the technical specification documents for the indicators of the Multi-Sector Service Accountability Agreement (M-SAA) and Hospital Service Accountability Agreement (H-SAA) need to be refined. Therefore, one subgroup for M-SAA and one for H-SAA were formed to complete this work. Long Term Care Homes Service Accountability Agreement (L-SAA): The Ministry of Health and Long-Term Care (the ―Ministry‖) has recently amended the following documents listed in Schedule F of the L-SAA to reflect increases in funding:
LTCH Level-of-Care (―LOC‖) Per Diem Funding Policy
LTC Home LOC Per Diem Funding Summary.
Copies of each of the revised documents are included with this letter and can be found on the Ministry‘s public website at: http://www.health.gov.on.ca/english/public/program/ltc/15_facilities.html#8 The effective date of this amendment to the L-SAA is April 1, 2011. The funding increases are subject to the conditions set out in LOC Per Diem Funding Policy, April 1, 2011 and Long Term Care Homes will begin to receive the increased per diems in August including lump sum retroactive payment for increases effective April 1, 2011 and July 1, 2011.
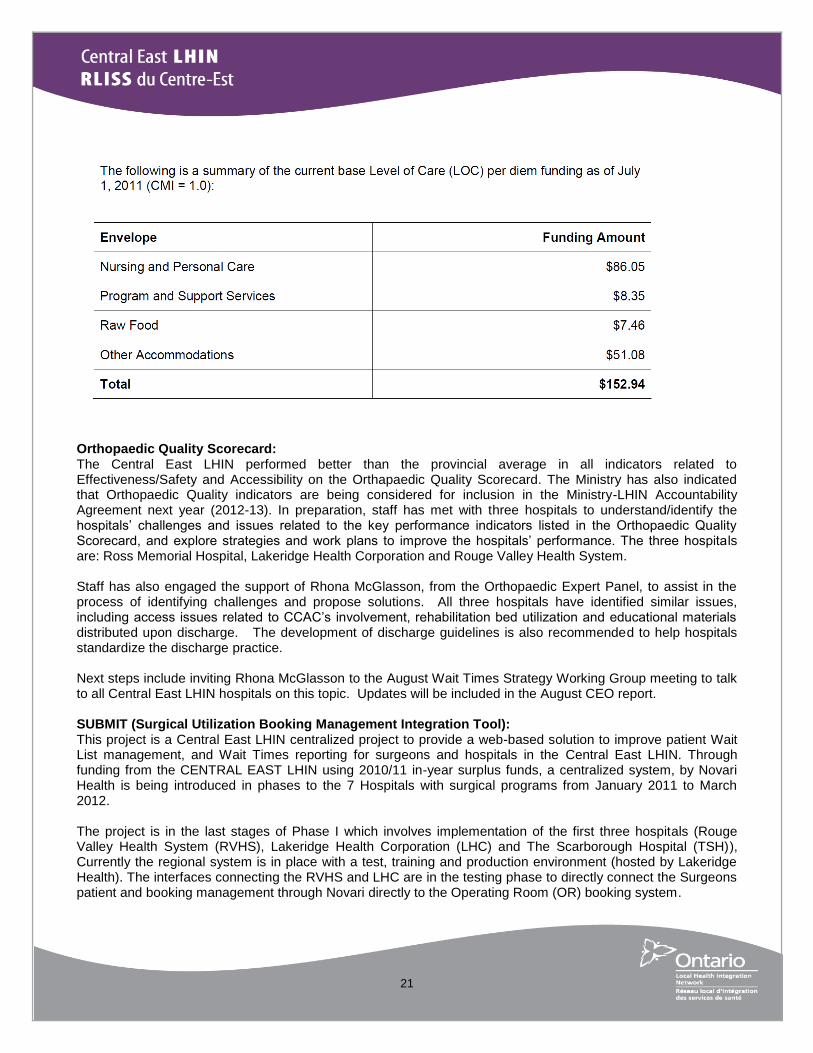
21
Orthopaedic Quality Scorecard: The Central East LHIN performed better than the provincial average in all indicators related to Effectiveness/Safety and Accessibility on the Orthapaedic Quality Scorecard. The Ministry has also indicated that Orthopaedic Quality indicators are being considered for inclusion in the Ministry-LHIN Accountability Agreement next year (2012-13). In preparation, staff has met with three hospitals to understand/identify the hospitals‘ challenges and issues related to the key performance indicators listed in the Orthopaedic Quality Scorecard, and explore strategies and work plans to improve the hospitals‘ performance. The three hospitals are: Ross Memorial Hospital, Lakeridge Health Corporation and Rouge Valley Health System. Staff has also engaged the support of Rhona McGlasson, from the Orthopaedic Expert Panel, to assist in the process of identifying challenges and propose solutions. All three hospitals have identified similar issues, including access issues related to CCAC‘s involvement, rehabilitation bed utilization and educational materials distributed upon discharge. The development of discharge guidelines is also recommended to help hospitals standardize the discharge practice. Next steps include inviting Rhona McGlasson to the August Wait Times Strategy Working Group meeting to talk to all Central East LHIN hospitals on this topic. Updates will be included in the August CEO report. SUBMIT (Surgical Utilization Booking Management Integration Tool): This project is a Central East LHIN centralized project to provide a web-based solution to improve patient Wait List management, and Wait Times reporting for surgeons and hospitals in the Central East LHIN. Through funding from the CENTRAL EAST LHIN using 2010/11 in-year surplus funds, a centralized system, by Novari Health is being introduced in phases to the 7 Hospitals with surgical programs from January 2011 to March 2012. The project is in the last stages of Phase I which involves implementation of the first three hospitals (Rouge Valley Health System (RVHS), Lakeridge Health Corporation (LHC) and The Scarborough Hospital (TSH)), Currently the regional system is in place with a test, training and production environment (hosted by Lakeridge Health). The interfaces connecting the RVHS and LHC are in the testing phase to directly connect the Surgeons patient and booking management through Novari directly to the Operating Room (OR) booking system.
22
Successes have been observed at RVHS with improved processes for registration. For example Novari provides the ability for the registration staff to receive electronic information on a new surgical patient and return the information to the surgeon‘s office view to meet the Wait Time Information System (WTIS) time requirement without extra phone / fax effort. In addition, the requirement of the ‗booking package‘ will no longer be necessary to send to registration because of the electronic view. Further work to develop the standard pre-populated forms with surgical information (i.e. Consent, the information sheet produced for the patient, etc.) is being developed and has been identified as saving time and resources in both the surgeon‘s office as well as the Pre-Operative area. Cancer Care Ontario (CCO) identified in July 2011, a new set of WTIS requirements for implementation to include Wait Times 1 (the wait between the Referral Date and the Surgical Consult Date), 2 (the wait between the Decision to Treat Date and the Procedure Date minus Dates Affecting Readiness to Treat (DARTs)), additional services and moving hospitals to a more automated method of reporting which will be completed by March 2012. The SUBMIT project has hospitals moving to the fully automated process called ―complex integration‖ and will, once CCO identifies the new requirement, provide the fields to submit additional information on Wait Times 1 and 2 (through Novari). The Phase II hospitals were not slated to be on the Novari application until March 2012 and the CCO access to care team has identified that once their project is completed in March 2012 they cannot guarantee and have no new project planning to allow the Phase II hospitals to submit their reporting automated through the Novari application. The Project Manager is working with the Central East LHIN, the hospitals and CCO to determine the mitigation strategy. Potential mitigation strategies being discussed include:
1. RMH would have the ability to move into the CCO plan for Phase I (requiring a move up of the implementation date by 30 days)
2. PRHC, CMH & NHH require a new interface to be built to connect the Meditech system, therefore would not be able to be incorporated into Phase 1 (insufficient time). The mitigation option is to work with CCO to develop a plan for after March 31, 2012 and implement workarounds until the plan is available for these hospitals.
Hospital-Community Care Access Centre Financial Leadership Group (HCFLG): The group identified Data Centre and Transcription as back office functions that they would like to prioritize for integration. The group was informed about 2011/12 Ministry LHIN Performance Agreement (MLPA) performance indicator targets negotiated with the Ministry of Health and Long-Term Care (MOHLTC) and their attention was drawn towards the Magnetic Resonance Imaging (MRI) Scan indicator target, which is lower than the past year‘s actual performance. Strategies to utilize unspent MRI funding allocation were discussed as well. The group would like the individual hospital level performance indicator dashboards to be regularly presented. It was agreed that in August all hospitals will work on completion of a standard template for budget assumptions in preparation for the 2012/2015 Hospital Annual Planning Submission (HAPS)/Hospital Service Accountability Agreement (HSAA) process. A sub-group has been established to work on public reporting of expenses in compliance with Ministry Expense and Procurement Directives and the sub-group will submit their report on November 30, 2011. The 2012/13 Hospital Planning assumptions were sent out to the hospitals by the Chair of the HCFLG to collect information regarding each hospital‘s inflation assumptions. This information will be shared at the next HCFLG meeting at the end of August, followed by a discussion on joint planning assumptions to guide the 2012-15 hospital accountability agreement.
23
Diagnostic Imaging (DI) Working Group: The Diagnostic Imaging Group has not formally met over the summer; however, most of the members participated in a teleconference jointly with the Wait Times Strategy Working Group to discuss the challenges associated with meeting the MLPA MRI target set for 2011/12. At the beginning of August, a webinar training session was sponsored by the LHIN and delivered by Lydia Antalfy, Chair of the DI Working Group. The webinar, which had approximately 25 participants from hospitals across the LHIN, was designed to train diagnostic imaging booking staff on the appropriate use of Dates Affecting Readiness To Treat (DART). DART is a tool to adjust wait times recorded when mitigating circumstances, such as patient availability, occur. The effectiveness of the training will be evaluated by measuring the implementation of DART over the next few months. Revised CT Designation Forms and Process: The Ministry of Health and Long-Term Care recently released an updated CT Scanner Protocol and Business Case. The document is now more closely aligned to the principle and developing policy for devolution of the Own-Funds Capital decision-making process.
Community Engagement Community Engagement is the foundation of all activity at the Central East LHIN. Being more responsive to local needs and opportunities requires ongoing dialogue and planning with those who use and deliver health services. Engagement with a wide range of stakeholders can be conducted at various levels including informing and educating; gathering input; consulting; involving and empowering. To assist us in tracking our Community Engagement activities, an ongoing Calendar of Events is kept up to date and shared weekly with staff. It documents all engagement activities with a wide range of stakeholders. Many of these events are also posted on the CE LHIN website: http://www.centraleastlhin.on.ca/showcalender.aspx. Below are listings of recent activities that the Central East LHIN Staff have been involved with:
On July 19th, The Youth Centre in Ajax and the Port Hope Community Health Centre (CHC) kindly
provided tours of their facilities to Deborah Hammons. In an effort to continue to increase the awareness of our Board members of the types of health services and facilities in the Central East LHIN, a tour has been arranged of the Port Hope CHC prior to the August Board meeting.
Further opportunities to update our local Members of Provincial Parliament (MPPs) were realized with a joint meeting of John O‘Toole, MPP Durham; Christine Elliott, MPP Whitby/Oshawa and Jerry Ouellette, MPP Oshawa on July 26. Attending from the LHIN was Wayne Gladstone, Deborah Hammons and Karen O‘Brien. It was a very positive meeting that allowed for an update on the activities in the Central East LHIN as well as an opportunity for the MPPs to ask specific questions relating to services in their communities. A meeting with MPP Brad Duguid is scheduled in August.
On July 27th, the Central East LHIN Board was given a tour of The Scarborough Hospital‘s two
campuses (Birchmount and General) and held the July Board meeting at the General campus. The tours provided an insight into some interesting programs and services offered at each campus.
On August 9th, Deborah Hammons and Wayne Gladstone attended the official opening of the Central
East CCAC Alternate Care Setting Clinic in Oshawa. Also in attendance was Jerry Ouellette, MPP, Oshawa.
Upcoming Municipal Council presentations are scheduled for: o August 17
– Peterborough County Council
o August 17 – Northumberland County Council
The Central East LHIN website continues to be a primary vehicle for both communication and engagement with our stakeholders. From July 1 - 31, 2011 there were 6,212 visits made by 3,365 visitors. There were 18,306
24
pages viewed. After the splash page, the page with the biggest number of hits is the Careers page with 1,248 unique views. During July there don‘t appear to be any patterns in when people visit the website but there was a spike on July 11
th and July 13
th when the ―LHIN leads‖ page was updated and web-alerted to include Dr. Gary
Mann and the ―Funding‖ page was updated and web-alerted to show investments by sector and each health service provider.
We are continuing to encourage people to subscribe to the website in order to be alerted to new content as it is posted. This will ensure our communities are informed, educated, can provide input, be involved and consulted on the work being done to create an integrated system of care that provides better care, better health and better value for money.
Central East LHIN Operations
Audit Committee The consolidated quarterly report – Q1 April 2011 to June 2011 was presented at the Audit Committee for review as well as the Board Governance budget, travel expenses and per diems claims. These reports are reviewed on a quarterly basis by the Audit committee of the Board. Organizational Review – Survey The redesign of the Central East LHIN (LHIN) structure started in 2009-10, the LHIN held focus groups with staff to obtain input on what type of organization the LHIN needed to be. Since then, the LHIN has implemented a number of initiatives to re-organize and re-position the organization using the following rationale as identified in the original planning discussions:
1. Strategic Growth 2. Culture Change 3. Organization Growth
The time has come for the LHIN to review the progress made and identify next steps; therefore, the LHIN developed a survey for employees to comment and provide feedback on how to continue to improve the way we operate and work together as an organization. The results of the survey will be reported to the Board of Directors in the fall of 2011. Performance Management Program The Performance Management Program cycle includes the completion of the newly implemented Individual Development Plans (IDP), an IDP is a development tool that is used to enhance knowledge, skills, and abilities both in the short and long-term. The IDP process is a follow-up development activity to the Performance Evaluation process and is an opportunity for the supervisory managers to manage a development plan for the employee to develop your skills, competencies and career in concert with fulfilling the Central East LHIN business goals.
Staffing Announcement Jenny Greensmith has officially resigned from her full-time position as the Health Planner, although she will be working with the Central East LHIN on reports, projects on an occasional contract basis.
Ministry Announcements Ontario’s Infrastructure Loan program is expanding: to include additional not-for-profit sectors that provide infrastructure for families and people in local communities, such as the Association of Ontario Health Centres. Eligibility for the program is being expanded to not-for-profit organizations that own or operate community hubs
25
where both community health and social services are offered, as well as not-for-profit sports and recreation organizations that provide facilities to serve the needs of Ontarians. By expanding the program, Ontario is helping not-for-profits to acquire debt financing to help meet their infrastructure needs, increase their access to infrastructure financing and improve health care and social services in communities. eHealth Project Management office: eHealth Ontario has been given direction to flow $600,000 in funding to each LHIN to support the operation of eHealth Project Management Offices for fiscal 2011-12. The funding will be delivered in July and November of this year. Behavioural Supports Ontario (BSO) program: In May 2011, all LHINs submitted Expressions of Interest to participate in the BSO program. The implementation of a BSO program is intended to enhance services for older adults with behaviours associated with complex and challenging mental health, dementia or other neurological conditions. Northwestern Ontario Health System Fires: Province-led teleconferences were held daily during the peak periods of concern with representatives from all LHINs as well as the Emergency Management Branch of the Ministry. A debrief call was scheduled for August 11, where a suggestion for Aboriginal sensitivity training and communication training was suggested as a helpful tool for public health officials in host communities. Overall public health units thought that there was a better coordination of health information sharing in comparison to a previous evacuation involving the James Bay area Health Canada identified the need to have a single ―point person‖ as liaison between Ministry of Health and nursing stations in evacuation communities. It was identified that the LHIN role in emergencies needs to be clearly defined and made more formal. The Emergency Management Branch has been discussing the LHIN role in Emergencies with the MOH, a separate debrief is being planned with the CEOs of the LHINs. As a result of the contingency measures, it became evident to some host communities that access to services in these remote communities is challenging (i.e. drug treatment). All agencies that were being involved in the various planning stages early in the evacuation showed strengths and improvement compared to activities during the H1N1 issue. The biggest challenge that was identified was the absence of a master list of where evacuees were sent to making it difficult for community leaders to follow up with families as well as for community nurses to follow up with those who were high-risk or had high medical needs. There has been discussion regarding the health sector having input into choice of host communities as it seemed to be a municipal decision whether to take evacuees or not, and Public Health Units and LHINs were not always involved in the decision making. All evacuees have been repatriated home. The fires are under control and it continues to rain in the north, the issue is being closely monitored by the Ministry.
Other Announcements Grandview Children’s Centre: has been selected as the lead agency for the ―Durham Applied Behaviour Analysis (ABA)-based Services‖ and has partnered with Lake Ridge Community Support Services and Resources for Exceptional Children and Youth for the delivery of this service, as well as the University of Ontario Institute of Technology for evaluation purposes.
Dr. Joan Lesmond: passed away on August 5. Dr. Lesmond was a prominent member of the health care community; she participated in a number of LHIN events as a facilitator and supported both the ―Cultural Diversity and Equity‖ and ―Self-Management‖ projects. Dr. Lesmond‘s accomplishments will be remembered and her valued teachings have set the foundation for advancements in nursing education and community-based
26
health care. More about her amazing contributions in Ontario and around the world can be accessed at: http://www.legacy.com/obituaries/thestar/obituary.aspx?n=joan-lesmond-gayle&pid=153000666&fhid=12318. Mr. Gilles Barbeau: member of the Board of Director of Entity #4, passed away Saturday August 6, 2011. Mr. Barbeau was a busy volunteer. He was involved with the Bendale Acres Centre in Scarborough and the Centres d‘Accueil Héritage, in Toronto. He was also chair of the French Language Services Planning Committee of Toronto. Rouge Valley implements the new “Patient Navigator” role in its Emergency Department: Tagged as an innovative approach to patient care, this new position in the emergency department is helping to get patients into an emergency doctor‘s care more quickly. A registered nurse has been assigned to the role Monday-Thursday, and is responsible for managing a patient‘s journey through the Emergency Department (ED) to ensure that clinical services are delivered within the targeted timeframes for our LHIN. Rouge Valley has also reported improvement rates for patient satisfaction under the new model. Respectfully Submitted,
Deborah Hammons Chief Executive Officer Central East Local Health Integration Network
27
Appendices
Appendix A
Allocation Funding Methodologies Overview (3).pdf
Appendix B
CECCAC Report to the CE LHIN July 22-11.pdf
Appendix C
Symposium 2011 Report.pdf
Appendix D
OTN Annual Report.pdf
Appendix E
HSAA Newsletter July 2011.pdf
Appendix F
9 Central East LHIN Report.pdf
Appendix G
OIVHSCommunique.pdf





























