Embed Size (px)
Citation preview

Neil S. Silverman, MD
Center for Fetal Medicine & Women’s Ultrasound, LA
Clinical Professor, Dept. of Obstetrics and Gynecology
Division of Maternal-Fetal Medicine
David Geffen School of Medicine at UCLA

Vaccine Importance and Strategies
Children have benefited the most from vaccines in terms of declines in disability and death, primarily because vaccination programs are generally targeted to children
In 1994, reported that 50,000-70,000 adults compared to 500 children died each year from vaccine-preventable illnesses
(Fedson D, JAMA 1994)
More than 50% of cases of significant vaccine-preventable illnesses reported to the CDC in 2004 occurred in individuals > 15 years old
Many of the most vulnerable adults are seen in practices that provide health care to women
Immunization services have not historically been part of obgyn care
Need to address benefit of vaccination both for women and for the long-term health of their children

Vaccination: Key Areas
Influenza (focus on pregnancy
and HCWs)
Tdap (tetanus, diphtheria,
pertussis)
Physician protection/liability
Inadvertent vaccination
Side effects/complications

Influenza

Influenza and Pregnancy
Increased morbidity/hospitalization rates for pregnant women
in every trimester compared to rates in nonpregnant persons
(Dodds L et al, CMAJ 2007)
When no comorbidities: risk ratio 1.7 (1st tri) – 5.1 (3rd tri)
With comorbidities: risk ratio 2.9 (1st tri) – 7.9 (3rd tri)
Increased risks of maternal deaths reported in pan-epidemics
(CDC 2007)
Newer live-attenuated nasal flu vaccine should not be given in
pregnancy, or in those > 65 years old (GYN)
Demonstrated benefit for mothers and newborns
Immunization with the trivalent inactivated flu vaccine
(TIV) is recommended for all pregnant women
(ACOG CO #608, Sept 2014; CDC 2013)

Neonatal Benefits of Maternal Influenza Vaccination
Flu vaccine not recommended for children < 6 months of age
Pregnant women have been shown to have protective levels of anti-influenza antibodies after vaccination
(Munoz FM, AJOG 2005)
Passive transfer of antibodies that might provide protection from vaccinated women to neonates has been reported
(Englund JA et al, J Infect Dis 1993; Reumen PD et al, Ped Infect Dis J 1987)
Retrospective clinic-based study in 1998-2003 showed (nonsignificant) trend toward fewer episodes of newborn respiratory illness among newborns of vaccinated pregnant women (Black SB ,Am J Perinatol 2004)

Neonatal Benefits of Maternal
Influenza Vaccination (2)
Randomized study of flu vaccine during
pregnancy to assess neonatal impact:
NEJM, Sept 2008, Zaman K, et al
340 women received either flu vaccine or
pneumococcal vaccine (Hopkins study group in
Bangladesh)
63% lower risk of lab-confirmed neonatal influenza in
children of vaccinated moms, up to 6 months of age
1st study to definitively show benefit to women and
children

Zaman K et al, NEJM 2008

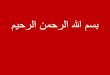
Influenza Vaccination of Pregnant Women and
Protection of their Infants (2014)
Report on 2 double-blind R-PC trials of trivalent influenza
vaccine in pregnant women with and without HIV infection
Study cohorts: 2116 pregnant women without and 194
pregnant women with HIV infection (South Africa)
At 1 month after vaccination, seroconversion rates and
rates of antibody titers were significantly higher for vaccine
recipients vs placebo in both cohorts (90-97% vs 25-44%)
Vaccine efficacy (placebo vs vaccine)
HIV-uninfected women/infants: 3.6% infection rate vs 1.9%
HIV-infected women: 17% infected vs 7.0%
Madhi SA, et al. NEJM, Sept 2014

Kaplan–Meier Estimates of Percentages of Confirmed Cases of Influenza According to Cohort and Study Group.
Madhi SA et al. N Engl J Med 2014;371:918-931.

So..why aren’t more pregnant women
vaccinated against influenza?
Lack of information
Variability in flu severity year-to-year
Current flu season ending: mildest in CA in
recent years
“Short memory” syndrome
Concerns over risk for pregnancy
Provider interest: concerns over
reimbursement, litigation
Confusion over recommendations

Recommendations of ACIP for Maternal
Influenza Vaccination
1964-1966: Any stage of pregnancy
1966-1969: HR conditions, any gestational age
1969-1974: No mention of maternal immunization
1974-1976: Pregnancy not an indication
1976-1977: No evidence to document influenza a risk
1977-1981: Evaluate pregnant as non-pregnant
1981-1986: Vaccinate HR pregnant women
1987-1995: Vaccinate HR pregnant women in any age
1995-1997: HR at any gestational age; others 3rd trimester
1997-2004: HR at any time, other in 2nd and 3rd trimester
2004-2008: Women pregnant during influenza season at any trimester

Are we barriers to vaccination during pregnancy?
Prospective survey study during 3 months of flu season
• Among responding women, only 22% reported discussing flu
vaccine with doctor, and only 8% were vaccinated
More physicians said they discussed vaccine with patients
than did patients say it was discussed (74% v 22%; p<0.01)
Physicians were more likely to vaccinate if: Aware of CDC guidelines (RR 2.6; 1.1-5.9)
Gave vaccinations in their office (RR 1.2; 1.01-1.4)
Had received flu vaccine themselves (RR 1.9; 1.3-2.8)
Study demonstrated gaps in both groups’ understanding
of benefit of vaccine for both pregnant women &
newborns
Silverman NS, Greif A. J Repro Med, Nov 2001

HCW Vaccinations 2013-14
Overall influenza coverage rate
for 2013-14 season was 75.2%
Coverage was > 90% for;
1. Physicians, regardless of work setting
2. HCW with employer vaccination
requirement, regardless of work setting
Majority of vaccinated HCWs (77.3%)
reported receiving vaccine at work
If vaccines not required at work:
80%: vaccine if free and on-site > 1 day
62%: vaccine if free and on-site only 1 day
49%: vaccine if not available on-site
MMWR: Sept 19, 2014


MMWR, Sept 19, 2014

MMWR, Sept 19, 2014
, Sept 19, 2014




Doctors ARE Covered:
National Childhood Vaccine Injury Act
www.hrsa.gov/vaccinecompensation
Established by Congress in 1986
Began operation 1988
No-fault federal compensation
program
Alternative to tort system

NCVI Act
Table of injury established for each vaccine
Alleged injury must be on the table
Financed by $0.75 tax per antigen and each tax must be passed by congress
Time limits for inquiries

But this is a Childhood Vaccine
Injury Act, right? Yes, but it covers all vaccines that are part of the
childhood vaccination schedule, regardless of who’s getting them e.g.: Influenza, hepatitis B, varicella, tetanus
Requires health-care provider who administers VCIP-covered vaccines to record, either in an office log or the recipient’s permanent medical record: Date of vaccine, manufacturer and lot #, name and title of
person administering the vaccine
Also requires reporting of adverse vaccination reactions to Vaccine Adverse Event Reporting System (VAERS) 800-338-2382 or http://vaers.hhs.gov



Influenza Antivirals and Pregnancy
Issue initially arose with H1N1 (A strain), since it
was susceptible, choice was between oseltamavir
and zanamavir Both OK in pregnancy; rimantidine also OK , only IF susceptible
Neuraminidase inhibitors usually also effective against B strains
Oseltamavir, as a systemic agent, may be
preferable
Treat mother and, possibly, fetus: does cross placenta
Treatment dose: 75 mg BID X 5 days
Ideally, within 2 days after onset of symptoms
Prophylactic dose: 75 mg daily X 10 days
Exposure window: 7 days

BUT:
Vaccination is
ALWAYS
better than
treatment

2014-15 Influenza Vaccine (MMWR, Aug 15, 2014)
In June 2014, the ACIP voted on updated recommendations
for use of trivalent seasonal influenza vaccine for the 2014-
2015 influenza season.
Expanded vaccination recommendations for adults were
established in 2009 to include all adults. Therefore, all
people age 6 months and older are now recommended to
receive annual influenza vaccination.
The 2014–2015 trivalent vaccine is identical to last year’s:
A/California/7/2009 (H1N1)-like, A/Texas/50/2012 (H3N2)-
like, and B/Massachusetts/2/2012-like antigens.
Recombinant trivalent vaccine available for persons with severe egg
allergy (anaphylaxis): FluBlok®. Nasal vaccine NOT an alternative.
Quadrivalent vaccine also available but no CDC recommendation

Influenza Vaccine:
Preparations and Preservatives
Quadrivalent vaccine also available but no
ACIP/CDC or ACOG recommendation or
preference 1,2
Recombinant trivalent vaccine available for
persons with severe egg allergy (anaphylaxis):
FluBlok®. (allergy no longer an “excuse”)
Thimerosal: a mercury-containing preservative
used in multi-dose vials of the vaccine
Thimerosal-free formulations are available, NO
scientific evidence that thimerosal-containing vaccines
result in adverse effects in newborns whose mothers
got them during pregnancy 1
1. CDC/MMWR 2013. 2. ACOG 2014

Pertussis and Tdap

Pertussis Epidemiology
Pertussis is
— an endemic human disease that peaks
every 3 to 5 years
— increasingly being reported in adolescents
and adults; immunity wanes
• In 2005, ~60% of cases ≥11 years of age*
Adolescents and adults serve as vectors of
infection for non-immune infants, in whom disease
is often quite severe
Probably not a disease reservoir
— Prolonged carriage most likely does not occur
*CDC. Pertussis Surveillance Report, Oct 14, 2006. Weeks 1-52 (final data)

Tetanus-Diphtheria-Pertussis Vaccines:
New Considerations
Tetanus booster recommendations have not changed:
every 10 years, with pregnancy no exception (toxoid)
DTP typically a childhood vaccine, with adults receiving Td
boosters
However, rates of pertussis infection have soared in
US despite childhood vaccination
Pertussis is highly contagious and spread easily by inhalation
of respiratory droplets or aerosols
Cases reported to CDC have doubled between 2003 and
2004, and are higher than any year since 1959
Adults and adolescents accounted for 67% of cases in 2006

Why here? Why now?
Pertussis cyclical
— Epidemics occur every 3-5 yrs when enough
susceptible people accumulate in population
to sustain widespread transmission
— Last US epidemic in 2005 (nationwide)
Susceptible people increase in population due to — New birth cohorts of unvaccinated infants
— Waning population immunity from vaccine or disease
(and less chance for boosting opportunities)
— Parental choice not to vaccinate children, etc.
Unclear why California most affected state so far
— Speculation: may have less population immunity than
other states because (until recently) one of only 11 states not
having requirement that all middle school students receive Tdap
Courtesy of Kathleen Harriman, California Dept of Public Health
?



Why the New Pertussis-containing
Vaccines?
Newer vaccine is an acellular pertussis-containing
preparation (Tdap): presumed better and more
durable immunogenicity
Approved in 2005 for individuals 11-64 years of age
Compensates for waning immunity (5-10 yrs) from old vaccine
DTaP is similar vaccine in pediatric formulation, with
3-5 X as much diphtheria component
Higher amount of pertussis component also is pediatric
preparation
Upper case “D” for pediatric formulation, lower case “d” for
adult formulation (same for “P” vs “p”)
Tetanus components equivalent

Pertussis: Common Questions (1)
A child or adult who has had pertussis can
(uncommonly) get the disease again, so vaccination is
recommended
Reinfection may present as persistent cough rather than
typical pertussis
After a tetanus-prone injury, in an adult whose last
booster was > 2 years ago?
Give Tdap, not Td or tetanus toxoid (TT) alone (can give Td
only if prior Tdap can be documented)
Age no excuse: TT became available in 1938, routinely used in
1944
No documentation → assume to be unimmunized

Pertussis: Common Questions (2)
Tdap can be given at same visit as other vaccines
Different site, using a separate syringe (don’t mix)
Mixed clinic setting (peds/adult) and an adult got DtaP
in error instead of Tdap
No harm to adult
Age limitations?
Both current commercially available Tdap formulations are
licensed for ages 11 and up. Recent ACIP/CDC
recommendations (June 2011): approved for ages > 65

New Tdap Urgency: CA Outbreak
Largest pertussis outbreak in 65 years in CA in 2010
9120 cases statewide; 304 cases through same time in 2009
10 infant deaths
Studies have shown that household contacts, most
often mothers, are the most common source of
pertussis in infants (Wendleboe AM, Ped Infect Dis J, 2009)
CA Dept. of Public Health, CDC, and CA-ACOG
endorsed vaccinating women during pregnancy
At least 2 weeks before contact with young infants
Household contacts are also to be vaccinated
Health-care personnel and childcare workers also
need to be vaccinated


2010-2011 ACIP Pertussis Recommendations
October 2010
— No interval necessary between Td and Tdap
(Previously: 2-year interval recommended)
— Tdap for adults ≥65 years of age with infant contact
— One dose Tdap for un-/under-immunized children 7-10
years of age
February 2011
— All healthcare personnel (HCP) who have not
received Tdap should receive ASAP
— Healthcare facilities should take steps to encourage
Tdap, including providing at no cost
http://www.cdc.gov/vaccines/recs/acip/

http://www.cdc.gov/vaccines/recs/acip/slides-jun11.htm#pertussis

How to Best Protect the Infant Tdap during Pregnancy!
Gall SA, AJOG 2011;204;334.e1-5.

Tdap during Pregnancy:
Safety and Immunogenicity
Randomized clinical trial evaluating Tdap during
pregnancy or postpartum
Significantly higher pertussis antibodies if Tdap
given during pregnancy compared to postpartum
in both women and in their infants at birth (p< 0.001)
No increased risk in serious adverse events in
women or infants, other than injection site
reactions in women
Pertussis antibodies in newborns did not alter
infant responses to Dtap vaccine in infancy
Munoz FM, et al. JAMA , May 2014

http://www.msnbc.msn.com/id/43502623/ns/health-
pregnancy

Pertussis Recommendations Current Landscape
All health care personnel
All adults, adolescents
After wound (instead of Td)
7-10 yo, if not completely immunized
Cocooning—including GRANDPARENTS
Antepartum—2nd or 3rd trimester
If not antepartum, give postpartum

Other Vaccines & Issues

Inadvertent vaccinations
Issue arises when a live attenuated vaccine (MMR or varicella)
is administered to a women whose early pregnancy was
undiagnosed
Rubella
Congenital rubella syndrome (CRS) reported with rubella infection in any
trimester
However, no proven vaccine-caused cases of CRS in either the US or
UK registries with current RA27/3 vaccine (MMWR, RR-8, 1998)
Varicella
Nonpregnant women who are vaccinate are counseled to avoid
pregnancy for 1 month (MMWR, RR-11, 1996)
Current Varivax® registry data report no attributable cases of congenital
varicella syndrome
Varicella or rubella vaccination during early pregnancy should not
be regarded as reasons to terminate pregnancy (MMWR, RR-15, 2006)

Outreach to Ob-Gyns

Visit our Website:
www.immunizationforwomen.org