-
FUNCIN DE CLULA BETA Y
TRATAMIENTO
EN DIABETES MELLITUS TIPO 2
Dr. Frederick Massucco R.
Servicio de Endocrinologa HNGAI
- Pronunciamiento de Consenso
( JCEM septiembre 2010 )
Endocrine Society- Reston, Virginia, 2009
Objetivo:
- Revisar los mecanismos de falla de clula beta en DM tipo 2 y
sus implicancias clnicas para proteger o evitar tempranamente el
deterioro de la misma.
- ANTECEDENTES
- DM 2 es una enfermedad progresiva.
- Patognesis compleja
. Predisposicin gentica
. Ganancia ponderal
. Deficiencia en la accin y secrecin de insulina
. Elevada produccin endgena de glucosa
EVIDENCIA: DM2 = disminucin masa funcional
de cls. Beta, que no adapta secrecin de
insulina a la creciente resistencia a la insulina.
-
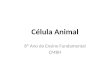
United Kingdom Prospective Diabetes Study (UKPDS)
UK Prospective Diabetes Study (UKPDS 34) Group. Lancet.
1998;352:854-65.
TRATAMIENTO INTENSIVO E INCREMENTO DE HbA1c EN EL TIEMPO
Median HbA1c (%)
Conventional
Insulin
Chlorpropamide
Glibenclamide (glyburide)
Metformin
0
3
0
6
7
8
9
6
9
10
Time From Randomization (years)
Upper limit of normal range (6.2%)
ADA goal
ADA action
-
PATOGNESIS
Substancial falla de clula beta,se piensa ocurre en una etapa
temprana de la progresin de la enfermedad, antes del
diagnstico.UKPDS: capacidad secretoria de clula beta se encontr
mermada en un 50% al momento en que se hizo el diagnstico de
Diabetes.Cambios equilibrados en insulinosensibilidad y funcin de
clula beta ( ndice de disposicin ) se rompe antes del desarrollo
franco de DM TIPO 2 EN PCTES CON CLULAS BETA SUSCEPTIBLES.
-
Hepatic
glucose
output
Insulin
resistance
Glucose uptake in muscle and fat
Glucagon
(alpha cell)
Insulin
(beta cell)
Hyperglycemia
Islet-cell dysfunction
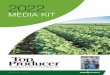
MECANISMOS FISIOPATOLGICOS
Adapted with permission from Kahn CR, Saltiel AR. Joslins
Diabetes Mellitus. 14th ed.
Lippincott Williams & Wilkins; 2005:145168.
Del Prato S, Marchetti P. Horm Metab Res. 2004;36:775781.
Porte D Jr, Kahn SE. Clin Invest Med. 1995;18:247254.
Pancreas
Liver
Adipose
tissue
Liver
Muscle
*
Major Pathophysiologic Defects in Type 2 Diabetes
Speaker Notes
This diagram depicts the impact of type 2 diabetes on the
feedback loop that regulates glucose homeostasis.
In type 2 diabetes, insulin resistance is increased and insulin
secretion is impaired.1
Most patients with type 2 diabetes have insulin resistance.
Pancreatic beta cells attempt to increase insulin secretion to
compensate for insulin resistance. However, when beta-cell function
is impaired, hyperglycemia develops.1
By the time diabetes is diagnosed, beta-cell function has
already decreased substantially and continues to decline over
time.1
Once insulin secretion is impaired, an imbalance between insulin
and glucagon can develop. Elevated glucagon levels lead to an
increase in hepatic glucose production.1
Likewise, with decreased secretion of insulin, less glucose is
taken up by the muscle and adipose tissue.2
References:
1.Del Prato S, Marchetti P. Beta- and alpha-cell dysfunction in
type 2 diabetes. Horm Metab Res. 2004;36:775781.
2.Porte D Jr, Kahn SE. The key role of islet dysfunction in type
2 diabetes mellitus. Clin Invest Med. 1995;18:247254.
Purpose:
To explain the 3 core pathophysiologic defects of type 2
diabetes.
Takeaway:
Insulin resistance, beta-cell dysfunction, and elevated hepatic
glucose production each contribute to hyperglycemia in type 2
diabetes.
- ESTUDIO LONGITUDINAL EN INDIOS PIMA
- Tolerantes normales a la glucosa, obesos,
insulinorresistentes que no progresan a DM 2
. AUMENTA INSULINO SECRECIN EN 30%
. DISMINUYE INSULINOSENSIBILIDAD EN 11%
- Progresores: normoglicemia-ITG-DM2
. DISMINUYE INSULINOSECRECIN EN 78%
. DISMINUYE INSULINOSENSIBILIDAD EN 14%
- FALLA PROGRESIVA DE CLULA BETA
FACTORES
GENTICOS
ADQUIRIDOS
PROT. METABOLISMO GLUCOSA
MOLCULAS INVOLUCRADAS EN
EFECTO BIOLGICO INSULINA
FACTORES DE TRANSCRIPCIN
GLUCOTOXICIDAD
LIPOTOXICIDAD
INCREMENTO AMILOIDE
POLIPEPTDICO DE LOS
ISLOTES
CITOKINAS INFLAMATORIAS
-
DISMINUIDA LIBERACIN DE INSULINA
PROLONGADA EXPOSICIN A NIVELES
MODERADAMENTE ELEVADOS DE GLUCOSA
DESENSIBILIZACIN DE CLULA BETA
INCREMENTO DE APOPTOSIS
FALLA EN RPTA. TEMPRANA DE CL. BETA
ATENUADA SEGUNDA FASE DE LIBERACIN DE INSULINA
MANIFESTACIONES DE FALLA DE CLULA BETA
A.- ALTERACIONES FUNCIONALES
- MANIFESTACIONES DE FALLA DE CLULA BETA
B.- DEFECTOS CUALITATIVOS
- Disrupcin de los ritmos de secrecin pulstil y procesamiento
del pptido precursor Proinsulina a Insulina activa.
. No diabticos: conversin es casi completa, quedando
2% de proinsulina intacta.
. Diabticos: Proinsulina intacta se eleva en 4 a 5 veces.
- MANIFESTACIONES DE FALLA DE CLULA BETA
C.- DEFECTOS ANATMICOS Y CELULARES DE LAS CLULAS BETA
TASA NETA
CRECIMIENTO
REPLICACIN CL. BETA
+
TAMAO CL. BETA
+
NEOGNESIS CL. BETA
APOPTOSIS
DE CLULA
BETA
=
-
DM tipo 2 apoptosis replicacin
clula beta neognesis
>
- MANIFESTACIONES DE FALLA DE CLULA BETA
C.- DEFECTOS ANATMICOS Y CELULARES DE CLULA BETA( CONT.)
- Debido a que la evaluacin morfolgica de las clulas beta
humanas pueden slo ocurrir postmorten, la mayor parte del
conocimiento proviene de estudios en roedores, la informacin acerca
de cambios anatmicos y celulares especficos asociados a DM2 en
humanos es an muy limitada.
- Butler y colaboradores: Diabetes 52:102-110,2003
- Estudio examin el tejido pancretico
obtenido de autopsias.
. 90 obesos ( 30 no diabticos, 19 con ITG y 41 con diabetes) y
32 sujetos no obesos ( 16 no diabticos y 16 con diabetes).
. Volumen celular en individuos con diabetes y prediabetes fue
menor que los no diabticos del mismo peso.
-
PREVINIENDO, RETRASANDO Y REVIRTIENDO LA FALLA DE CLULA BETA
Estudios animales: funcin y/o masa de clulas beta, son parmetros
modificables, especialmente en etapas tempranas de la
enfermedadEvidencia clnica tambin lo sugiere:
- Finnish Diabetes Prevention Study y el U.S Diabetes Prevention
Program, mostraron una reduccin del 58% en la incidencia de
diabetes entre pctes. con ITG tratados con dieta y ejercicio por 3
aos.
- Incidencia de diabetes en tratados con Metformina se redujo en
un 31%.
- STOP-NIDDM, Acarbosa, menos DM en 25%.
-
PREVINIENDO,RETRASANDO Y REVIRTIENDO LA FALLA DE CLULA BETA
Asociacin entre la reduccin aguda de glucosa y el mejoramiento en
la respuesta secretoria insulnica sugiere mejoramiento en la funcin
de clula beta.Comparar y evaluar los efectos en la funcin de la
clula beta de terapias farmacolgicas usadas para controlar la
hiperglicemia es necesariamente inferencial, dada la escasez de una
medida universal.Sin embargo, muchos ensayos cortos en pacientes
recin diagnosticados de diabetes sugieren una asociacin entre
preservacin de cl. Beta y ms durable control glicmico.
-
PREVINIENDO,RETRASANDO Y REVIRTIENDO LA FALLA DE CLULA BETA
TIAZOLIDENDIONASEn ensayos clnicos, parecen mejorar la funcin de
clula beta en pctes. con DM 2, induciendo tambin un control
glicmico durable.ADOPT: Estudio a doble ciego, randomizado y
controlado, que compar la durabilidad del control glicmico entre
4360 pacientes recientemente diagnosticados de DM2 tratados con
Rosiglitazona, Metformina o Gliburide por una media de 4 aos.
-
ADOPT
Treatment Difference at 4 Years
RSG vs MET 0.13 (0.22 to 0.05), P=.002
RSG vs SU 0.42 (0.50 to 0.33), P
-
PREVINIENDO,RETRASANDO Y REVIRTIENDO LA FALLA DE CLULA BETA
TIAZOLIDENDIONASDREAM
Disminucin en un 62% de progresin a diabetes en pacientes con
intolerancia a la glucosa que reciban Rosiglitazona.
ACT NOW
Redujo la aparicin de diabetes en 81% de pacientes intolerantes
a la glucosa tratados con Pioglitazona.
Cambios en los ndices de disposicin=mejoramiento en
insulinosensibilidad y funcin de clula beta.
-
(DREAM)
No. at Risk
Rosiglitazone2635253824141310217
Placebo2634247021501148177
The DREAM Trial Investigators. Lancet. 2006;368:1096-1105.
60% risk reduction of development of diabetes or death was seen
with rosiglitazone This reduction was additive to standard
counseling on healthy eating and exercise
HR = 0.40 (0.35-0.46); P
-
PREVINIENDO, RETRASANDO Y REVIRTIENDO LA FALLA DE CLULA BETA
INCRETINASAgonistas de GLP-1 e inhibidores de DPP-IV
- Agonistas de GLP-1, proveen remplazo farmacolgico del pptido
incretina.
- Inhibidores de DPP-IV, elevan niveles endgenos de incretinas
al bloquear su inactivacin.
. Incrementan secrecin de insulina glucosa
dependiente.
. Disminuyen secrecin de Glucagon.
. Inhiben el vaciamiento gstrico.
. Reducen el apetito.
-
PREVINIENDO,RETRASANDO Y REVIRTIENDO LA FALLA DE CELULA BETA
GLP-1 y sus anlogos relacionados, han mostrado en modelos animales,
incrementar la masa de clulas beta por inhibicion de apoptosis,
promoviendo proliferacin de clulas de los islotes y estimulando
diferenciacin de clulas no insulino secretoras.Si es que estos
efectos ocurren en humanos es an desconocido.
-
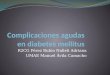
EFECTO INCRETINA ESTA DISMINUIDO EN PACIENTES CON DM 2
Adapted with permission from Nauck M et al. Diabetologia
1986;29:4652. Copyright 1986 Springer-Verlag.
Time, min
Control Subjects
(n=8)
IR Insulin, mU/L
180
60
120
0
Normal Incretin Effect
180
60
120
0
Subjects With Type 2 Diabetes
(n=14)
Diminished Incretin Effect
Time, min
IR Insulin, mU/L
Oral glucose load
Intravenous (IV) glucose infusion
80
60
40
20
0
80
60
40
20
0
*
The Incretin Effect Is Diminished in Subjects With Type 2
Diabetes
Speaker Notes
In 1964, it was demonstrated that the insulin secretory response
was greater when glucose was administered orally through the
gastrointestinal tract than when glucose was delivered via IV
infusion. The term incretin effect was coined to describe this
response involving the stimulatory effect of gut hormones known as
incretins on pancreatic secretion.1,2
The incretin effect implies that nutrient ingestion causes the
gut to release substances that enhance insulin secretion beyond the
release caused by the rise in glucose secondary to absorption of
digested nutrients.1
Studies in humans and animals have shown that the incretin
hormones GLP-1 and GIP account for almost all of the incretin
effect,3 stimulating insulin release when glucose levels are
elevated.4,5
Although the incretin effect is detectable both in healthy
subjects and in those with diabetes, it is abnormal in those with
diabetes, as demonstrated by the study shown on the slide.6
In this study, patients with type 2 diabetes and weight-matched,
metabolically healthy control subjects were given glucose either
orally or IV to achieve an isoglycemic load.
In those individuals without diabetes (shown on the left), the
plasma insulin response to an oral glucose load was far greater
than the plasma insulin response to an IV glucose load (incretin
effect)that is, the pancreatic beta cells secreted much more
insulin when the glucose load was administered through the
gastrointestinal tract.
In patients with type 2 diabetes (shown on the right), the same
effect was observed but was diminished in magnitude.
The diminished incretin effect observed in patients with type 2
diabetes may be due to reduced responsiveness of pancreatic beta
cells to GLP-1 and GIP or to impaired secretion of the relevant
incretin hormone.7,8
Purpose:
To introduce the concept of the incretin effect in healthy
individuals and the abnormality in patients with type 2
diabetes.
Takeaway:
Gastrointestinal ingestion of glucose stimulates a greater
insulin response than that seen from IV glucose infusion. This
effect is significantly decreased in patients with type 2 diabetes.
The response is largely attributed to the effect of incretins.
References:
1.Creutzfeldt W. The incretin concept today. Diabetologia.
1979;16:7585.
2.Creutzfeldt W. The [pre-] history of the incretin concept.
Regul Pept. 2005;128:8791.
3.Brubaker PL, Drucker DJ. Minireview: glucagon-like peptides
regulate cell proliferation and apoptosis in the pancreas, gut,
and
central nervous system. Endocrinology. 2004;145:26532659.
4.Drucker DJ. Biological actions and therapeutic potential of
the glucagon-like peptides. Gastroenterology. 2002;122:531544.
5.Ahrn B. Gut peptides and type 2 diabetes mellitus treatment.
Curr Diab Rep. 2003;3:365372.
6.Nauck M, Stckmann F, Ebert R, Creutzfeldt W. Reduced incretin
effect in type 2 (non-insulin-dependent) diabetes. Diabetologia.
1986;29:4652.
7.Creutzfeldt W. The entero-insular axis in type 2
diabetesincretins as therapeutic agents. Exp Clin Endocrinol
Diabetes. 2001;
109(suppl 2):S288S303.
8.Nauck MA, Heimesaat MM, rskov C, Holst JJ, Ebert R,
Creutzfeldt W. Preserved incretin activity of glucagon-like peptide
1
[7-36 amide] but not of synthetic human gastric inhibitory
polypeptide in patients with type-2 diabetes mellitus. J Clin
Invest. 1993;91:301307.
-
Mean Change in A1C, %
A1C
CI=confidence interval. *Compared with placebo. Least-squares
means adjusted for prior antihyperglycemic therapy status and
baseline value. Difference from placebo. Combined number of
patients on JANUVIA or placebo. ||P
-
Add-on to pioglitazone study2
Mean Baseline A1C: 8.0%, 8.1%
Mean Change in A1C From Baseline, %
(sitagliptin): Significativa Reduccin de HbA1C
cuando se agreg a Metformina o pioglitazona
24-week change from baseline
n=224
Metformin
+ JANUVIA
1.0
0.8
0.6
0
1.0
0
Mean Change in A1C From Baseline, %
0.7%
Mean Baseline A1C: 8.0%
P
-
Porcentage de pacientes que alcanzaron A1C
-
IMPLICANCIAS TERAPUTICAS
Prescindiendo de sus potenciales efectos en clula beta pueden ser
mantenidos en el tiempo , en la determinacin del valor clnico de
estas modalidades teraputicas se debe considerar la frecuencia de
hipoglicemias, los mecanismos de accin, los eventos adversos, la
tolerabilidad y el costo.Finalmente, es imperativo determinar si la
preservacin de la masa y/o funcin de clula beta mejoran las tasas
de morbimortalidad, reducen las complicaciones y/o mejoran la
calidad de vida del paciente diabtico.
-
IMPLICANCIAS TERAPUTICAS
Paradigma fisiopatolgico para la decisin mdica
De Fronzo: algoritmo teraputico que combina dieta y ejercicio
con mltiples drogas para corregir y posiblemente revertir la
progresiva falla de clula beta que ya est establecida en
intolerancia a la glucosa.
Estilo de vida
+
TZD + Metformina
+ Exenatide.
0
0.1
0.2
0.3
0.4
0.5
0.6
012345
0
10
20
30
40
50
PlaceboJANUVIA
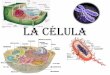
Postprandial GLP
Postprandial GLP
-
-
1 levels are decreased in
1 levels are decreased in
people with IGT and Type 2 diabetes
people with IGT and Type 2 diabetes
Toft
-
Nielsen et al.
J
Clin
Endocrinol
Metab
.
2001
20
15
10
5
0
0
60
120
180
240
Time (min)
GLP
-
1 (pmol/l)
*
*
*
*
*
*
*
*
Meal
NGT
T2DM
IGT
*
P