Embed Size (px)
Citation preview
![Page 1: Cellulitis in Adults - WRHN in Adults.pdf• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue [1]: • Erysipelas is a form of cellulitis caused by](https://reader034.pdfslide.us/reader034/viewer/2022050716/5e37a2a00fa2bc6b5a461882/html5/thumbnails/1.jpg)
Cellulitis in AdultsA-Z Localised Whanganui Pathways > Infectious Diseases > Cellulitis
Published: 15-Dec-2017 Valid until: 31-Dec-2018 Printed on: 28-Feb-2018 © Map of Medicine Ltd This care map was published by Whanganui District. A printed version of this document is not controlled so may not be up-to-date with thelatest clinical information.
Page 1 of 11
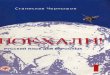
Care mapinformation
Updates to this caremap
Information resourcesfor patients and carers
Hauora Maaori Pacific
Clinical presentation
History
ExaminationRed FlagsImmediate transfer toED/WAM for triage
Consider differentialdiagnoses
Moderate Severity Mild Severity
Standard oral Therapy
Community IV Therapy
No Improvement Improvement
Deteriorating orbecoming systemicallyunwell
Not responding Responding
Consult Hospital Switch to oral therapy
Lifestyle Management
Information resourcesfor clinicians
Consider Boosted Oraltherapy
Deterioratingor becomingsystematically unwell
POAC funding still indevelopment
![Page 2: Cellulitis in Adults - WRHN in Adults.pdf• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue [1]: • Erysipelas is a form of cellulitis caused by](https://reader034.pdfslide.us/reader034/viewer/2022050716/5e37a2a00fa2bc6b5a461882/html5/thumbnails/2.jpg)
Cellulitis in AdultsA-Z Localised Whanganui Pathways > Infectious Diseases > Cellulitis
Published: 15-Dec-2017 Valid until: 31-Dec-2018 Printed on: 28-Feb-2018 © Map of Medicine Ltd This care map was published by Whanganui District. A printed version of this document is not controlled so may not be up-to-date with thelatest clinical information.
Page 2 of 11
1 Care map information
Quick info: In Scope:
• covers the diagnosis and management of:
• bacterial cellulitis
• erysipelas in primary care
• adults 15 years of age and over
Out of Scope:
• management of bacterial cellulitis and erysipelas in secondary care
• diabetic foot infections
• penetrating wounds
• bites
• post-operative surgical wounds
• abscesses
• children under 15 years of age
Definition:
• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue [1]:
• Erysipelas is a form of cellulitis caused by streptococcal infection of the dermis, with:
• marked superficial inflammation
• typically affecting the face or extremeties with a sharply demarcated, raised edge
• the lower limbs are the most common sites affected by cellulitis [2] and erysipelas, but other areas can be affected i.e. theears, trunk, fingers, and toes
Aetiology:
• most common infective organisms in adults are:
• Staphylococcus aureus and Streptococci (especially Staphylococcus pyogenes [2]):
• bacteroides species
• anaerobic cocci
• cellulitis due to Streptococcus pneumoniae may also occur in patients with underlying conditions such as alcoholism,diabetes Mellitus, intravenous drug abuse, or Systemic Lupus Erythematosus
Risk factors:
• lymphoedema
• leg ulcer
• venous eczema
• insect bite
• traumatic wounds
• damage to local venous or lymphatic drainage systems
• obesity
• immunosuppression
• Tinea Pedis (athlete's foot)
• previous episodes
• leg oedema
• Diabetes Mellitus (DM)
• intravenous (IV) drug use
• alcoholism
References:[1] BPAC NZ, Cellulitis: skin deep and spreading across New Zealand, Best Practice Journal, Issue 68, June 2015[2] Clinical Resource Efficiency Support Team (CREST),Guidelines on the Management of Cellulitis in Adults, Belfast, 2005
![Page 3: Cellulitis in Adults - WRHN in Adults.pdf• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue [1]: • Erysipelas is a form of cellulitis caused by](https://reader034.pdfslide.us/reader034/viewer/2022050716/5e37a2a00fa2bc6b5a461882/html5/thumbnails/3.jpg)
Cellulitis in AdultsA-Z Localised Whanganui Pathways > Infectious Diseases > Cellulitis
Published: 15-Dec-2017 Valid until: 31-Dec-2018 Printed on: 28-Feb-2018 © Map of Medicine Ltd This care map was published by Whanganui District. A printed version of this document is not controlled so may not be up-to-date with thelatest clinical information.
Page 3 of 11
2 Information resources for patients and carers
Quick info:Resources for patients and carers:
• Cellulitis: What to Expect
• Cellulitis IV Treatment handout
• Patient Information Cellulitis
3 Information resources for clinicians
Quick info:Resources for clinicians:
• Policy Adult Cellulitis Management Guidelines
• New Zealand Formulary (NZF) - Link with the medications
• flucloxacillin
• cefalexin
• clindamycin
• cefazolin
• probenecid
• contrimoxazole/trimethoprim+sulphamethoxazole
• Noids on injectable drugs - page on how to give the drugs, waiting times
• Process for IV certification - Contact WDHB IV education - 06 348 1234
4 Updates to this care map
Quick info:Date of publication: December 2017This care map has been developed in line with consideration to evidenced based guidelines. For further information on contributorsand references please see the Pathway's Provenance Certificate.
5 Hauora Maaori
Quick info:As a practitioner you will work with Maori whanau/families. Each Maori whanau is diverse with their own set of values and beliefs,inherited, practised and passed down from generation to generation.There are some important things that you should be mindful of when working with Maori individuals and their whanau from a holisticapproach to working in a Whanau ora or family / whanau centred way.Key enablers that you should be aware of when working with Maori whanau/families are:
• building relationships and gaining trust
• effective communication with whanau /families
• understanding and involving whanau/ families in the treatment planning and care management
• practical things to be mindful of when working with Maori whanau so that you do not breech Tikanga/Principles and practicesthat are important in Te Ao Maori/the Maori world
Common terms and definitions are noted here.
6 Pacific
Quick info:Our pasifika community:
![Page 4: Cellulitis in Adults - WRHN in Adults.pdf• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue [1]: • Erysipelas is a form of cellulitis caused by](https://reader034.pdfslide.us/reader034/viewer/2022050716/5e37a2a00fa2bc6b5a461882/html5/thumbnails/4.jpg)
Cellulitis in AdultsA-Z Localised Whanganui Pathways > Infectious Diseases > Cellulitis
Published: 15-Dec-2017 Valid until: 31-Dec-2018 Printed on: 28-Feb-2018 © Map of Medicine Ltd This care map was published by Whanganui District. A printed version of this document is not controlled so may not be up-to-date with thelatest clinical information.
Page 4 of 11
• is a diverse and dynamic population
• more than 22 nations represented in New Zealand
• each with their own unique culture, language, history, and health status
• share many similarities which we have shared with you here in order to help you work with pasifika patients more effectively
The main Pacific nations in New Zealand are
• Samoa, Cook Islands, Fiji, Tonga, Niue, Tokelau and Tuvalu
Acknowledging The FonoFale Model (pasifika mode of health) when working with pasifika peoples and families.Acknowledging general pacific guidelines when working with pasifika peoples and families:
• cultural protocols and greetings
• building relationships with your pacific patients
• involving family support, involving religion, during assessments and in the hospital
• home visits
• pasifika phrasebook
7 POAC funding still in development
Quick info:Primary Options for Acute Care funding is still in development and is yet to be finalised at the time of publication.
8 Clinical presentation
Quick info:Symptoms and signs:
• acute onset:
• affected area of skin is red, hot, painful, tender, and swollen
• inflammation is initially localised but may spread
• bilateral leg erythema is unlikely to be cellulitis. It is more commonly due to heart failure and occasionally due to IVC thrombis
• blisters or bullae may develop over infected area
• red streaks leading from area of infection equals lymphangitis
• sepsis is suggested by systemic symptoms:
• malaise
• fever
• anorexia or nausea
• rigors
• sweats
9 History
Quick info:History:
• previous infection in same area
• period of skin discomfort prior to onset of erythema
• speed of progression
• period of systemic symptoms:
• malaise
• fever
• nausea
![Page 5: Cellulitis in Adults - WRHN in Adults.pdf• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue [1]: • Erysipelas is a form of cellulitis caused by](https://reader034.pdfslide.us/reader034/viewer/2022050716/5e37a2a00fa2bc6b5a461882/html5/thumbnails/5.jpg)
Cellulitis in AdultsA-Z Localised Whanganui Pathways > Infectious Diseases > Cellulitis
Published: 15-Dec-2017 Valid until: 31-Dec-2018 Printed on: 28-Feb-2018 © Map of Medicine Ltd This care map was published by Whanganui District. A printed version of this document is not controlled so may not be up-to-date with thelatest clinical information.
Page 5 of 11
• shivering
• rigors
• any skin trauma, ulcers or bites
• assess for co-morbidities:
• previous episodes
• recent surgery to affected area
• chronic venous insufficiency
• oedema and lymphoedema
• lymphatic or vascular surgery
• obesity
• Diabetes Mellitus (DM)
• immunosuppression
• intravenous (IV) drug use
• skin breakdown, especially venous leg ulcers
• pain out of context with the clinical impression of infection may be an indication of necrotising fasciitis. This is a surgicalemergency. Discuss with emergency physician.
• ask if other family members have similar problems
10 Immediate transfer to ED/WAM for triage
Quick info:WAM Phone number: 06 3481 300ED number: 06 348 1223Fax number: 06 3481 299Refer immediately to ED if:
• significant clinical concerns e.g: shortness of breath or chest pain, patient feeling light headed or rapid pulse
• suspected pulmonary embolus (PE), or the patient is acutely unwell and/or has active multiple co-morbidities
11 Red Flags
Quick info:Contact ED doctor on 06 3481223 and arrange transfer for ED:
• significant systemic upset:
• acute confusion
• tachycardia
• tachypnoea
• hypotension
• hypothermia (blunted immune response in the elderly)
• or unstable co-morbidities
• or limb-threatening infection due to vascular compromise
• or severe life-threatening infection such as necrotising fasciitis
Consider urgent referral/consultation for admission to hospital for the following:
• compartment syndrome
• surgical post operative cellulitis around wound site
• severe systemic illness, e.g. fever, or nausea, and vomiting
• co-morbidity that may complicate or delay healing:
• e.g. peripheral vascular disease, chronic venous insufficiency, morbid obesity, immunosuppression, intravenous drug use
• periorbital infection
![Page 6: Cellulitis in Adults - WRHN in Adults.pdf• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue [1]: • Erysipelas is a form of cellulitis caused by](https://reader034.pdfslide.us/reader034/viewer/2022050716/5e37a2a00fa2bc6b5a461882/html5/thumbnails/6.jpg)
Cellulitis in AdultsA-Z Localised Whanganui Pathways > Infectious Diseases > Cellulitis
Published: 15-Dec-2017 Valid until: 31-Dec-2018 Printed on: 28-Feb-2018 © Map of Medicine Ltd This care map was published by Whanganui District. A printed version of this document is not controlled so may not be up-to-date with thelatest clinical information.
Page 6 of 11
• patients with suspected necrotising fasciitis
• cellulitis that has spread from an adjacent structure (e.g. osteomyelitis) or through the blood (bacteraemia) is a serious concern
Generalised signs of necrotising fasciitis or myonecrosis can be indistinguishable from cellulitis, but are strongly suggested by:
• dusky purple or black discolouration
• tense oedema
• cutaneous numbness
• skin necrosis with or without crepitus
• pain - out of proportion to clinical signs
12 Examination
Quick info:When examining the affected area, consider the following:
• look for signs of systemic toxicity:
• pyrexia
• tachycardia
• tachypnoea
• hypotension or organ hypoperfusion, e.g. new confusion may relate to hypotension secondary to septicaemia. also fever maycause confusion
• examine infected area, looking particularly for:
• extent of inflammation
• erythema and oedema
• raised skin temperature
• blue or purple discolouration
• sloughing
• blistering
• necrosis
• rapid progression (if previously examined):
• look for focal point of infection
• disproportionately high or low levels of pain relative to physical findings may be an indication of necrotising fasciitis
• palpate regional lymph nodes
• assess for overlying sensation and check distal pulses - alteration in these may indicate necrotising fasciitis or compartmentsyndrome
• an abscess if present and is suitable for surgical drainage:
• this should be performed or referred for this to be performed at the hospital
NB: if clinical signs are bilateral, consider alternative diagnoses, as bilateral cellulitis is rare.
13 Consider differential diagnoses
Quick info:Consider the following:
• varicose eczema
• deep vein thrombosis (DVT), refer to Deep Vein Thrombosis care map
• peripheral vascular disease
• panniculitis / vasculitis
• oedema and venous insufficiency
Less common conditions that may present with similar signs and symptoms to cellulitis include:
• stings and bites
![Page 7: Cellulitis in Adults - WRHN in Adults.pdf• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue [1]: • Erysipelas is a form of cellulitis caused by](https://reader034.pdfslide.us/reader034/viewer/2022050716/5e37a2a00fa2bc6b5a461882/html5/thumbnails/7.jpg)
Cellulitis in AdultsA-Z Localised Whanganui Pathways > Infectious Diseases > Cellulitis
Published: 15-Dec-2017 Valid until: 31-Dec-2018 Printed on: 28-Feb-2018 © Map of Medicine Ltd This care map was published by Whanganui District. A printed version of this document is not controlled so may not be up-to-date with thelatest clinical information.
Page 7 of 11
• gangrene
• acute gout
• adverse drug reactions
• compartment syndrome
• osteomyelitis or septic arthritis
• necrotising fasciitis (see Red Flags box)
14 Moderate Severity
Quick info:For patients with moderate cellulitis, oral therapy should be considered as a first option:
• mild systemic illness (temperature <38, P<90, Systolic BP >100, resp. rate <20)
• or systemically well but with a co-morbidity such as:
• peripheral vascular disease
• chronic venous insufficiency
• morbid obesity
• poorly controlled diabetes
15 Mild Severity
Quick info:Minor severity:
• no signs of systemic toxicity
• no uncontrolled co-morbidities
These patients are suitable for oral therapy initially and hence would not activate a Coordinated Primary Options (CPO) episode.Clear education is required about the condition and the use of oral antibiotics medicines to ensure ongoing concordance withmedicines:
• Cellulitis: What to Expect
Ensure rest and elevation
16 Standard oral Therapy
Quick info:Antibiotic Treatment - First Choice:
• Flucloxacillin 500mg - 1g, four times daily, for seven days (to be taken on empty stomach)
OR (if penicillin-related rash)
• Cefalexin 500mg, four times daily, for seven days
Note in renal impairment - CLcr 10-40mL/min 250mg to 500mg 8 hourly CLcr <10mL/min 250mg 8 hourlyAntibiotic treatment if history of anaphylaxis to penicillin:
• Clindamycin 300mg 6 hourly for seven days (if patient greater than 150kg then dose 450mg 6 hourly for seven days) -Clindamycin script must be endorsed - "For the treatment of Cellulitis as per Map of Medicine and patient has a severe penicillinallergy"
OR if MRSA suspected
• Co-trimoxazole 160+800mg (two tablets), twice daily, for seven days
• Clindamycin 300mg 6 hourly for seven days (if patient greater than 150kg then dose 450mg 6 hourly for seven days) -Clindamycin script must be endorsed - "For the treatment of Cellulitis as per Map of Medicine and MRSA suspected"
![Page 8: Cellulitis in Adults - WRHN in Adults.pdf• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue [1]: • Erysipelas is a form of cellulitis caused by](https://reader034.pdfslide.us/reader034/viewer/2022050716/5e37a2a00fa2bc6b5a461882/html5/thumbnails/8.jpg)
Cellulitis in AdultsA-Z Localised Whanganui Pathways > Infectious Diseases > Cellulitis
Published: 15-Dec-2017 Valid until: 31-Dec-2018 Printed on: 28-Feb-2018 © Map of Medicine Ltd This care map was published by Whanganui District. A printed version of this document is not controlled so may not be up-to-date with thelatest clinical information.
Page 8 of 11
17 Consider Boosted Oral therapy
Quick info:Boosted Antibiotic Treatment:Consider using probenecid in combination with antibiotics:
• Probenecid 500mg three times daily for seven days WITH Flucloxacillin 1g, three times daily, for seven days (to be taken withfood) [1]
NB. Meals may slow, but do not decrease the overall bioavailability. Therefore Flucloxacillin can be given with food. NB. Dose adjustment in renal impairment - Creatinine clearance less than 30ml per minute : Patient does not requireprobenecid boosting.
18 No Improvement
Quick info:Follow-up is required if no improvement or deterioration after 48-72 hours:
• boosted oral therapy (oral antibiotic + probenecid) - move to boosted oral therapy in moderate severity
19 Improvement
Quick info:Remind:
• reinforce need to complete antibiotics
• rest and elevate
PreventionAdvise the person that prevention of cellulitis includes taking good care of any break in the skin. This can be done by informing theperson to:
• use own towel and soap
• make sure that any cuts, grazes or bites are kept clean
• keep good hand hygiene
• maintain healthy diet and proper exercise
• wash the wound daily with soap and water
• keep the wound covered with a plaster or dressing
• ensure plaster or dressing is changed if it becomes wet or dirty
• watch for signs of infection. Redness, pain and drainage all signal possible infection and the need for medical evaluation
• update tetanus status:
• high risk wounds: animal, human bites and puncture injuries
Diabetic PatientsPeople with diabetes and those with poor circulation need to take extra precautions to prevent skin injury. Good skin care measuresinclude the following:
• inspect your feet daily. Regularly check your feet for signs of injury so you can catch infections early
• moisturise your skin regularly. Lubricating your skin helps prevent cracking and peeling
• trim your fingernails and toenails carefully. Take care not to injure the surrounding skin
• protect your hands and feet
• wear sturdy, well-fitting shoes or slippers
• avoid walking barefoot in areas, for example, in garages, on a littered beach, or in the woods
• promptly treat infections on the skin's surface (superficial), such as athlete's foot. Superficial skin infections can easily spreadfrom person to person
Preventing recurrent cellulitis
![Page 9: Cellulitis in Adults - WRHN in Adults.pdf• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue [1]: • Erysipelas is a form of cellulitis caused by](https://reader034.pdfslide.us/reader034/viewer/2022050716/5e37a2a00fa2bc6b5a461882/html5/thumbnails/9.jpg)
Cellulitis in AdultsA-Z Localised Whanganui Pathways > Infectious Diseases > Cellulitis
Published: 15-Dec-2017 Valid until: 31-Dec-2018 Printed on: 28-Feb-2018 © Map of Medicine Ltd This care map was published by Whanganui District. A printed version of this document is not controlled so may not be up-to-date with thelatest clinical information.
Page 9 of 11
People who experience frequently recurring cellulitis, such as those with lymphoedema, may consider a trial of prophylacticantibiotics (e.g. amoxycillin 500mg bd or doxycycline 100mg od) on a long-term basis. This must be seen as an option of last resort,as long-term antibiotics are not without obvious risks.
20 Deteriorating or becoming systematically unwell
Quick info:Refer to ED (Contact ED doctor on 06 348 1223 and arrange transfer for ED) if:
• significant clinical concerns e.g: shortness of breath or chest pain, patient feeling light headed or rapid pulse
• suspected pulmonary embolus (PE), or the patient is acutely unwell and/or has active multiple co-morbidities
21 Community IV Therapy
Quick info:Cefazolin 2g IV plus Probenecid 1 gram once daily."If patient cannot tolerate 1 gram once daily of probenecid, consider splitting dose to 500mg twice daily".or if Probenecid containdicated - Cefazolin 2gm IV 12 hourly.Information regarding IV Therapy Patients:
• Probenecid Infomation Sheet (for prescribers)
• Cellulitis IV treatment patient handout
Provider checklist:
• mark area with a fine permanent pen
• prescribe analgesia if appropriate
• for IV administration over the weekend or after hours (consider timing of doses and adjust accordingly +/- 2 hours), considerreferral for urban practices to Whanganui Accident and Medical Centre and rural practices to District Nursing
• Urban - Consider treatment in practice or referral in the first instance to another agreed provider such as WAM. If IVadministration needed over the weekend or after hours consider WAM.
• Rural - Continue rural process with District Nursing process - - if they are immobile, the district nurse needs a medication chartfor administration
• IV medication can be given by any certified IV doctor or nurse.
• consider referral to District Nursing Service if unable to manage wound or if the patient does not have good access to theirgeneral practice (i.e. are immobile, particularly those patients with lower limb cellulitis or those patients that live rurally)
• provide patient with information about cellulitis
• consider taking baseline blood tests (FBC, creatinine) - particularly for elderly and high-risk patients
• check renal function (creatinine clearance) MdCalc
22 Deteriorating or becoming systemically unwell
Quick info:Refer to ED (Contact ED doctor on 06 348 1223 and arrange transfer for ED) if:
• significant clinical concerns e.g: shortness of breath or chest pain, patient feeling light headed or rapid pulse
• suspected pulmonary embolus (PE), or the patient is acutely unwell and/or has active multiple co-morbidities
23 Not responding
Quick info:Consider extending IV therapy for a further three days if not responding. Consider blood tests for FBC and creatinine to help guidemanagement, particularly for elderly or high-risk patients. Do not exceed more than six days without consultation with InfectiousDiseases physician.Consider alternative diagnoses.
![Page 10: Cellulitis in Adults - WRHN in Adults.pdf• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue [1]: • Erysipelas is a form of cellulitis caused by](https://reader034.pdfslide.us/reader034/viewer/2022050716/5e37a2a00fa2bc6b5a461882/html5/thumbnails/10.jpg)
Cellulitis in AdultsA-Z Localised Whanganui Pathways > Infectious Diseases > Cellulitis
Published: 15-Dec-2017 Valid until: 31-Dec-2018 Printed on: 28-Feb-2018 © Map of Medicine Ltd This care map was published by Whanganui District. A printed version of this document is not controlled so may not be up-to-date with thelatest clinical information.
Page 10 of 11
24 Responding
Quick info:Persistent or progressive redness in the first 24 hours does not indicate failed treatment. Improvement is indicated by:
• wrinkling of the skin
• reduced pain
• decreased swelling
As long as the global clinical picture is of a well patient, prescribe oral antibiotics. Repeat education regarding limb elevation to assistrecovery.
25 Consult Hospital
Quick info:Contact ED doctor on 06 3481223.
26 Switch to oral therapy
Quick info:Continue with oral therapy following IV therapy. Either use "Boosted Antibiotic Treatment" or "Antibiotic Treatment - No Probenecid"protocols below.Boosted Antibiotic Treatment
• Probenecid 500mg three times daily for seven days WITH Flucloxacillin 1g, three times daily, for seven days (with food)
• Probenecid Infomation Sheet (for prescribers)
Antibiotic Treatment - No Probenecid
• Flucloxacillin 500mg, four times daily, for seven days
OR (if flucloxacillin not tolerated)
• Cefalexin 500mg, four times daily, for seven days
OR (if penicillin-related rash)
• Cefalexin 500mg, four times daily, for seven days
• Note in renal impairment - CLcr 10-40mL/min 250mg to 500mg 8 hourly
CLcr <10mL/min 250mg 8 hourlyAntibiotic treatment if history of anaphylaxis to penicillin:
• Clindamycin 300mg 6 hourly for seven days (if patient greater than 150kg then dose 450mg 6 hourly for seven days) -Clindamycin script must be endorsed - "For the treatment of Cellulitis as per Map of Medicine and patient has a severe penicillinallergy"
OR if MRSA suspected
• Co-trimoxazole 160+800mg (two tablets), twice daily, for seven days
• Clindamycin 300mg 6 hourly for seven days (if patient greater than 150kg then dose 450mg 6 hourly for seven days) -Clindamycin script must be endorsed - "For the treatment of Cellulitis as per Map of Medicine and MRSA suspected"
NB. Meals may slow, but do not decrease the overall bioavailability. Therefore Flucloxacillin can be given with food.NB. Dose adjustment in renal impairment - Creatinine clearance less than 30ml per minute : Patient does not requireprobenecid boosting.
27 Lifestyle Management
Quick info:Prevention
![Page 11: Cellulitis in Adults - WRHN in Adults.pdf• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue [1]: • Erysipelas is a form of cellulitis caused by](https://reader034.pdfslide.us/reader034/viewer/2022050716/5e37a2a00fa2bc6b5a461882/html5/thumbnails/11.jpg)
Cellulitis in AdultsA-Z Localised Whanganui Pathways > Infectious Diseases > Cellulitis
Published: 15-Dec-2017 Valid until: 31-Dec-2018 Printed on: 28-Feb-2018 © Map of Medicine Ltd This care map was published by Whanganui District. A printed version of this document is not controlled so may not be up-to-date with thelatest clinical information.
Page 11 of 11
Advise the person that prevention of cellulitis includes taking good care of any break in the skin. This can be done by informing theperson to:
• use own towel and soap
• make sure that any cuts, grazes or bites are kept clean
• keep good hand hygiene
• maintain healthy diet and proper exercise
• wash the wound daily with soap and water
• keep the wound covered with a plaster or dressing
• ensure plaster or dressing is changed if it becomes wet or dirty
• watch for signs of infection. Redness, pain and drainage all signal possible infection and the need for medical evaluation
• update tetanus status:
• high risk wounds: animal, human bites and puncture injuries
Diabetic PatientsPeople with diabetes and those with poor circulation need to take extra precautions to prevent skin injury. Good skin care measuresinclude the following:
• inspect your feet daily. Regularly check your feet for signs of injury so you can catch infections early
• moisturize your skin regularly. Lubricating your skin helps prevent cracking and peeling
• trim your fingernails and toenails carefully. Take care not to injure the surrounding skin
• protect your hands and feet
• wear sturdy, well-fitting shoes or slippers
• avoid walking barefoot in areas, for example, in garages, on a littered beach, or in the woods
• promptly treat infections on the skin's surface (superficial), such as athlete's foot. Superficial skin infections can easily spreadfrom person to person
Preventing recurrent cellulitisPeople who experience frequently recurring cellulitis, such as those with lymphoedema, may consider a trial of prophylacticantibiotics (e.g. amoxycillin 500mg bd or doxycycline 100mg od) on a long-term basis. This must be seen as an option of last resort,as long-term antibiotics are not without obvious risks.
![Page 12: Cellulitis in Adults - WRHN in Adults.pdf• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue [1]: • Erysipelas is a form of cellulitis caused by](https://reader034.pdfslide.us/reader034/viewer/2022050716/5e37a2a00fa2bc6b5a461882/html5/thumbnails/12.jpg)
Provenance Certificate – Cellulitis in Adults
Overview |
Accreditations |
Editorial methodology
|
References |
Contributors |
Disclaimers
Overview This document describes the provenance of Whanganui Regions Cellulitis Pathway. This localised pathway was updated in December 2017. The purpose of implementing the CCP Programme in our District is to:
Enhance accuracy of referrals
Use best practice guidelines
Have all information found in one place
Enhance partnerships and collaboration across services
Improve patient outcomes through seamless care across primary and secondary care
To cite this pathway, use the following format: Map of Medicine – Medicine/Infectious diseases/cellulitis and erysipelas - Whanganui View. Map of Medicine; 2017.
Editorial methodology This care map has been based on a Map of Medicine Care Map developed according to the Map of Medicine editorial methodology. The content of the Map of Medicine care map is based on high quality guidelines and practice-based knowledge provided by contributors with front-line clinical experience (see contributors section of this document). This localised version of the evidence-based, practice informed care map has been peer-reviewed by the WDHB and WRHN Collaborative Clinical Directors and Leaders Forum and with stakeholder groups.
Consumer engagement Development of the Whanganui Collaborative Clinical Pathways focuses on person-centred care and an experience based co-design approach where consumers are invited to consult with the Health Promoter / Community Developer (who sits on each pathway working group). Consumers are asked prior if possible, or if not at the very start of the pathway process to share their experiences to assist in designing services that work for them and their families, critiquing and feeding back on suitable consumer information and resources which can then be incorporated into the pathways. Feedback obtained ensures we address consumer challenges and needs within the pathway and provide suitable services, information and resources for consumers. Additional information on patient centred care is provided by following this link and experience based co-design of health care services at http://www.kingsfund.org.uk/projects/ebcd.
References
1 BPAC NZ, Cellulitis: skin deep and spreading across New Zealand, Best Practice Journal, Issue 68, June 2015
2 Clinical Resource Efficiency Support Team (CREST),Guidelines on the Management of Cellulitis in Adults, Belfast, 2005
Contributors The following individuals have contributed to this care map:
Rick Nicholson – GP, Aramoho Health Centre
Ken Young – GP, Bulls Medical Centre
Louise Allsopp – Manager – Patient Safety, WDHB
Fiona Corbin – Clinical Advisory Pharmacist, WRHN
Mohammed Issa – Pharmacist, WDHB
Sharon Duff - Health Promotion Advisor, WRHN
Julie Nitschke - Clinical Director, WRHN (Facilitator)
![Page 13: Cellulitis in Adults - WRHN in Adults.pdf• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue [1]: • Erysipelas is a form of cellulitis caused by](https://reader034.pdfslide.us/reader034/viewer/2022050716/5e37a2a00fa2bc6b5a461882/html5/thumbnails/13.jpg)
Gerard Gregory – Collaborative Pathways Facilitator, WRHN (Editor)
Disclaimers CCP Leadership Team, Whanganui.
It is not the function of the CCP Leadership Team to substitute for the role of the clinician, but to support the clinician in enabling access to know-how and knowledge. Users of the Map of Medicine are therefore urged to use their own professional judgement to ensure that the patient receives the best possible care. Whilst reasonable efforts have been made to ensure the accuracy of the information on this online clinical knowledge resource, we cannot guarantee its correctness and completeness. The information on the Map of Medicine is subject to change and we cannot guarantee that it is up-to-date.