Embed Size (px)
Citation preview

CELLULITIS IN ADULTS April 2018 Page 1 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
Cellulitis in Adults Medicine > Infectious diseases > Cellulitis
POAC Provider
Resources
Pasifika Hauora Māori Updates to this care
map
Provider and patient
resources Care map
information
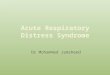
Clinical presentation
History Examination
Suspected Sepsis Consider differential
diagnoses
Immediate transfer to
hospital
Assessment of
severity
RED FLAG or Severe
(Eron Class III or IV)
Moderate
(Eron Class II)
Minor
(Eron Class I)
Refer to hospital High dose oral therapy Oral therapy
GP review after 48 hrs Follow-up 5-7 days
Deteriorating or is
becoming systemically
unwell
Not responding Responding
Exclusions for Commence community Follow-up 5-7 days community IV therapy IV therapy
Refer to hospital
GP review after 48 hrs
Deteriorating or is
becoming systemically
unwell
Not responding Responding
IV therapy continued Commence oral
therapy
Refer to hospital
GP review after 48hrs Follow-up 5-7 days
Seek specialist advice Oral therapy

CELLULITIS IN ADULTS April 2018 Page 2 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
1. Provider and patient resources
Provider resources:
• Probenecid
• use READ code M08
• District Nursing Service referral form
• POAC Transfer of Care/Handover form
Patient resources:
• Cellulitis Patient Information Resource
• Te Ara Whānau Ora Brochure
2. Updates to this care map
Date of latest publication: Feb 2018
• Where referral to DNS is listed, added the following note:
• NB: if referring to DNS, send referral form immediately
Re-published: July 2017
This care map has been updated in line with consideration to evidence based guidelines. Below summarises key changes made to
the pathway:
• high dose oral therapy as first option for treatment for moderate cellulitis
Re-published: July 2015
Please see the care map’s Provenance for additional information on references, accreditations from national clinical bodies,
contributors, publication schedule, and the editorial methodology.
3. Hauora Māori
Māori are a diverse people and whilst there is no single Māori identity, it is vital practitioners offer culturally appropriate care when
working with Māori Whānau. It is important for practitioners to have a baseline understanding of the issues surrounding Māori health.
This knowledge can be actualised by (not in any order of priority):
• acknowledging Te Whare Tapa Wha (Māori model of health) when working with Māori Whānau
• asking Māori clients if they would like their Whānau or significant others to be involved in assessment and treatment
• asking Māori clients about any particular cultural beliefs they or their Whānau have that might impact on assessment and
treatment of the particular health issue (Cultural issues)
• consider the importance of Whānaungatanga (making meaningful connections) with their Māori client / Whānau
• knowledge of Whānau Ora, Te Ara Whānau Ora and referring to Whānau Ora Navigators where appropriate
• having a historical overview of legislation that has impacted on Māori well-being
For further information:
• Hauora Māori
• Central PHO Māori Health website

CELLULITIS IN ADULTS April 2018 Page 3 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
4. Pasifika
Pacific Cultural Guidelines (Central PHO) 6MB file
Our Pasifika community:
• is a diverse and dynamic population:
• more than 22 nations represented in New Zealand
• each with their own unique culture, language, history, and health status
• share many similarities which we have shared with you here in order to help you work with Pasifika patients more effectively
The main Pacific nations in New Zealand are:
• Samoa, Cook Islands, Fiji, Tonga, Niue, Tokelau and Tuvalu
Acknowledging The FonoFale Model (pasifika model of health) when working with Pasifika peoples and families.
Acknowledging general pacific guidelines when working with Pasifika peoples and families:
• Cultural protocols and greetings
• Building relationships with your pasifika patients
• Involving family support, involving religion, during assessments and in the hospital
• Home visits
• Contact information
Pasifika Health Service - Better Health for Pasifika Communities:
• the Pasifika Health Service is a service provided free of charge for:
• all Pasifika people living in Manawatu, Horowhenua, Tararua and Otaki who have long term conditions
• all Pasifika mothers and children aged 0-5 years
• an appointment can be made by the patient, doctor or nurse
• the Pasifika Health Service contact details are:
• Palmerston North Office - 06 354 9107
• Horowhenua Office - 06 367 6433
• Better Health for Pasifika Communities brochure
Additional resources:
• Ala Mo'ui - Pathways to Pacific Health and Wellbeing 2014-2018
• Primary care for pacific people: a pacific health systems approach
• Tupu Ola Moui: The Pacific Health Chart Book 2004
• Pacific Health resources
• List of local Māori/Pacific Health Providers
• Central PHO Pacific Health website
5. POAC Provider Resources
POAC Management of Moderate Cellulitis in Adults - poster
POAC Provider Checklist - Cellulitis in Adults:
• area marked with washable pen
• no exclusions to community pathway
• no allergies or hypersensitivity to the prescribed medications
• patient information provided
• follow up appointment arranged

CELLULITIS IN ADULTS April 2018 Page 4 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
• clinical notes faxed to Accident and Medical Centre if follow up required over weekend
• referral to District Nursing Team (if appropriate) and prescription:
• phone: (06) 350 8100
• fax: (06) 350 8102
• referral to District Nursing Service (NB: send referral immediately to DNS)
• if ordering IV antibiotics from the PN hospital pharmacy:
• fax the patient prescription to (06) 350 8271 - ensure you label it 'POAC'
• Cellulitis Medications Pack checked against prescription
• prescriber to ensure correct patient details on Cellulitis Medications Pack
• medications dispensed by DOCTOR and given to patient for home administration
• The provider checklist is printable.
POAC Transfer of Care/Handover form
POAC Referral Centres - Contact List (contains phone and fax numbers)
POAC Eligibility Criteria:
• primary provider MUST be registered with POAC to claim POAC services - for more information please contact 027 247 8106
• POAC eligibility criteria
6. Care map information
In scope:
• covers diagnosis and management of:
• bacterial cellulitis
• erysipelas
• post operative surgical wounds - requires consultation with relevant specialist team
• those aged 16 years and over
Out of scope:
• if the patient has a history of immediate penicillin hypersensitivity (severe skin rash including welts, features of anaphylaxis,
angioedema) or any cephalosporin allergy then CefAZOLIN should not be prescribed and specialist advice is required
• use of intravenous antibiotics with an eGFR <35
• severe illness/signs of sepsis
• management of bacterial cellulitis and erysipelas in secondary care
• those aged less than 16 years of age
• diabetic foot infections - refer to General Surgery
• deep penetrating wounds
• bites - animals or human
• chemotherapy/neutropenic
Definition:
• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue:
• erysipelas is a form of cellulitis with:
• marked superficial inflammation
• typically affecting the face or extremities with a sharply demarcated, raised edge
• the lower limbs are the most common sites affected by cellulitis and erysipelas, but other areas can be affected:
• i.e. the ears, trunk, fingers, and toes

CELLULITIS IN ADULTS April 2018 Page 5 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
Aetiology:
• cellulitis around wound infections is commonly caused by:
• Staphylococcus aureus
• -haemolytic streptococci
• Bacteroides species
• anaerobic cocci
• most common infective organisms in adults are Staphylococcus aureus and Streptococci (especially Streptococci pyogenes)
• cellulitis due to Streptococcus pneumoniae may also occur in patients with underlying conditions such as alcoholism,
diabetes mellitus, intravenous drug abuse, or systemic lupus erythematosus
• Haemophilus influenzae cellulitis, particularly of the orbit, occurs in children up to three years of age
• facial cellulitis due to Streptococcus pneumoniae has also been described and occurs mainly in children
Incidence and prevalence: • UK hospital incidence data reported 69,576 episodes of cellulitis and 516 episodes of erysipelas between 2004 and 2005
• cellulitis infections of the limb accounted for most of these infections (58,824 episodes)
• recurrence is very common
Risk factors [5]:
• lymphodeoma
• leg ulcer
• venous eczema
• insect bite
• traumatic wounds
• obesity
• immunosuppression
• tinea pedis (athlete's foot)
• previous episodes
• leg oedema for
• diabetes mellitus (DM) vdr v
• intravenous (IV) drug use
• alcoholism
7. Clinical presentation
Symptoms and signs:
• acute onset:
• affected area of skin is red, hot, painful, tender, shiny and swollen
• inflammation is initially localised but may spread rapidly
• cellulitis usually affects one limb − this is dependent on the cause of cellulitis
• blisters or bullae may develop over infected area
• red streaks leading from area of infection may indicate lymphangitis
• sepsis is suggested by systemic symptoms:
• malaise
• fever, rigors or sweats
• nausea or vomiting
• rapid pulse or breathing

CELLULITIS IN ADULTS April 2018 Page 6 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
Complete history and examination.
NB: If clinical signs are bilateral, consider alternative diagnoses, such as venous stasis dermatitis (varicose eczema) bilateral
cellulitis is rare.
8. History
• previous infection in same area
• period of skin discomfort
• speed of progression
• period of systemic symptoms:
• malaise
• fever
• nausea • shivering
• rigors
• any skin trauma, e.g. tinea pedis (athlete's foot), ulcers or bites
• assess for co-morbid conditions:
• previous episodes
• chronic venous insufficiency
• oedema and lymphoedema
• lymphatic or vascular surgery
• obesity
• diabetes mellitus (DM)
• immunosuppression
• intravenous (IV) drug use
• skin trauma or skin breakdown, especially venous leg ulcers
• assess nature of any injury and risk of contamination, which predisposes to infection with unusual organisms
• pain out of context with the clinical impression of infection may be an indication of necrotising fasciitis
• ask if other family members have similar problems
9. Examination
When examining the affected area, consider the following:
• look for signs of systemic toxicity:
• pyrexia
• tachycardia
• tachypnoea
• hypotension or organ hypoperfusion e.g. new confusion
• examine infected area, looking particularly for:
• extent of inflammation
• erythema and oedema
• raised skin temperature
• blue or purple discolouration
• sloughing
• blistering
• necrosis
• rapid progression (if previously examined):
• consider demarcating the infected area with a washable pen in order to assess treatment efficacy

CELLULITIS IN ADULTS April 2018 Page 7 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
• look for focal point of infection
• disproportionately high or low levels of pain relative to physical findings may be an indication of necrotising fasciitis
• palpate regional lymph nodes
• assess for overlying sensation and check distal pulses − alteration in these may indicate necrotising fasciitis or compartment
syndrome
• an abscess if present and is suitable for surgical drainage:
• this should be performed or referred for this to be performed at the Hospital
NB: If clinical signs are bilateral, consider alternative diagnoses, as bilateral cellulitis is rare.
10. Suspected Sepsis
Early Identification of Sepsis
Sepsis must be considered if the patient reports any of the following:
• fevers
• rigors
• tachycardia
• hypotension
• altered mental state/confusion
A patient may have sepsis if the following criteria are met:
• any symptoms consistent with infection being present AND
• two or more of the following Systemic Inflammatory Response Syndrome (SIDS) criteria:
• temperature > 38.5 or < 35 degrees celsius
• pulse >90 beats/minute
• RR >20/minute
• WCC >12 or <4
In addition, if the patient has symptoms or signs of organ dysfunction, they have 'severe sepsis' e.g. confusion, reduced urine
volume, delayed capillary refill.
Management of Sepsis:
Refer patient immediately to hospital. If there is going to be delay in the patient's transfer to ED, initiate the following treatment:
IV antibiotics:
i. Target = administer < 1 hour of determining that the patient has sepsis
ii. Broad spectrum and full loading dose
iii. target antibiotic choice to identified
Empiric stat dose = ceftriaxone 2gm IV.
iv. IV fluids:
1. Titrate fluids therapy to measured goals/targets
• systolic >90mmHg
• MAP >65mmHg
• U/O >0.5ml/kg/hr
• Other e.g. improving confusion or capillary refill
2. Early aggressive fluids boluses = 500 - 1000mls, repeated 30 - 60 minutes
11. Consider differential diagnoses
Consider the following:
• varicose eczema; however, this is usually bilateral with crusting, scaling, itch, dull red colour
• lipodermatosclerosis

CELLULITIS IN ADULTS April 2018 Page 8 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
• deep vein thrombosis (DVT), but this does not usually cause significant erythema; see DVT Pathway
• peripheral vascular disease
• panniculitis
• vasculitis
• oedema and venous insufficiency
Less common conditions that may present with similar signs and symptoms to cellulitis include :
• necrotising fasciitis
• gangrene
• acute gout
• adverse drug reactions
• metastatic cancer (carcinoma erysipeloides)
• compartment syndrome • osteomyelitis or septic arthritis
• stings and bites
13. Assessment of severity
Classification of cellulitis (devised by Eron) should serve as a useful guide to admission or treatment decisions.
14. RED FLAG or Severe (Eron Class III or IV)
Class III: admit to Hospital as per red flags:
• significant systemic upset:
• acute confusion
• tachycardia
• tachypnoea
• hypotension
• cold sepsis
• hypothermia (blunted immune response in the elderly)
• or unstable co-morbidities
• or limb-threatening infection due to vascular compromise
• in adults P> Systolic BP maybe early septic shock
Class IV: admit to Hospital as per red flags (transfer by ambulance):
• sepsis syndrome
• or severe life-threatening infection such as necrotising fasciitis
Consider urgent referral/consultation for admission to hospital for the following:
• post-operative surgical wounds - refer to General Surgery
• symptoms or signs of class III or IV cellulitis
• severe systemic illness, eg fever, or nausea, and vomiting
• co-morbidity that may complicate or delay healing
• eg peripheral vascular disease, chronic venous insufficiency, morbid obesity, immunosuppression, intravenous drug use
• severe lymphoedema (gross swelling of the limb)
• periorbital infection
• patients with suspected necrotising fasciitis
• cellulitis that has spread from an adjacent structure, (eg osteomyelitis) or through the blood (bacteraemia) is a serious concern

CELLULITIS IN ADULTS April 2018 Page 9 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
Generalised signs of necrotising fasciitis or myonecrosis can be indistinguishable from cellulitis, but are strongly suggested by:
• RAPID spread and onset
• dusky purple or black discolouration
• cutaneous numbness
• skin necrosis with or without crepitus
• pain [2] − out of proportion to clinical signs
• significant systemic upset (see above)
15. Moderate (Eron Class II)
For patients with moderate cellulitis, oral therapy is highly encouraged and should be considered as a first option. Class II or Moderate severity:
• mild systemic illness (temp<38.5, P<100)
• or systemically well but with a co-morbidity such as:
• peripheral vascular disease
• chronic venous insufficiency
• morbid obesity
16. Minor (Eron Class I)
Class I or Minor severity:
• no signs of systemic toxicity
• no uncontrolled co-morbidities
These patients are suitable for oral therapy initially. Clear education is required about the condition and the use of oral antibiotics
medicines to ensure ongoing concordance with medicines.
18. High dose oral therapy
Antibiotic Treatment - First Choice:
• Flucloxacillin 1g qid, for seven days (to be taken with food)
• for more severe cases consider boosting (at least for the first few days) with Probenecid 500mg tds to qid with food
• Probenecid dose reduction in renal impairment required:
• if eGFR 35-60, 250mg tds to qid with food
• if eGFR <35 do not use Probenecid
• NB: The above treatment regime and patient response should be reviewed after 48hrs
OR (if flucloxacillin not tolerated)
• Cefalexin 1g, qid for seven days.
• for more severe cases consider boosting (at least for the first few days) with Probenecid 500mg tds to qid with food
• Probenecid dose reduction in renal impairment required:
• if eGFR 35-60, 250mg tds to qid with food
• if eGFR <35 do not use Probenecid
• NB: The above treatment regime and patient response should be reviewed after 48hrs
Antibiotic Treatment - Alternatives:
• Clindamycin 300mg - 450mg, tds-qid, for seven days (requires consultation with ID Physician or on-call medical consultant)
OR (if MRSA present)

CELLULITIS IN ADULTS April 2018 Page 10 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
• Co-trimoxazole 160+800mg (2-4 tablets), two to three times daily for five - seven days (maximum dose of 12 tablets per day)
19. Oral therapy
Antibiotic Treatment - First Choice:
• Flucloxacillin 500mg - 1000mg, qid for seven days (to be taken with food):
• if patient weighs >100kg, prescribe 1g - 1.5g, qid for the first 2 days, then reduce to 500mg - 1000mg for the next 5
days (to be taken with food)
OR (if flucloxacillin not tolerated) • Cefalexin 500mg - 1000mg, qid for seven days:
• if patient weighs >100kg, prescribe 1g - 1.5g, qid for the first 2 days, then reduce to 500mg - 1000mg for the next 5
days (to be taken with food)
Antibiotic Treatment - Alternatives:
• Roxithromycin 150mg, bd or 300mg daily, for seven days
• Erythromycin 400mg, qid
OR (if MRSA present)
• Co-trimoxazole 160+800mg (two tablets), bd for five - seven days
Caution with renal impairment:
• Flucloxacillin/cefalexin if eGFR <10 dose modification required - contact Renal team (06) 356 9169
• Co-trimoxazole if eGFR 15-30 dose modification required. Use half normal dose if eGFR 15-30; avoid if eGFR <15 unless no
alternatives are available - contact Renal team (06) 356 9169
If any questions consult with Infectious Diseases physician or on-call medical physician - phone (06) 356 9169.
20. Follow-up 5-7 days
Follow-up is required after 5 - 7 days to ensure resolution of cellulitis. If unresolved, review patient and consider:
1. extending oral therapy
OR
2. prescribing clindamycin - this requires consultation with infectious diseases physician (if not available contact on call
physician)
3. prescribing IV therapy
Consider predisposing factors and refer to Community Clinical Nurses - Long Term Conditions as appropriate. If recurrent lower limb
cellulitis, consider referral to infectious diseases or dermatology for further advice. If the wound is not healing or the patient is at high
risk of recurrence secondary to suspected arterial or venous disease consider referral to the District Nursing Service for ongoing
management and Doppler assessment.
• NB: if referring to DNS, send referral form immediately
21. GP review after 48 hours
Improvement is indicated by wrinkling of skin, reduced pain and often decreased swelling.
Response to treatment may be slow and it's reasonable to continue oral therapy provided there is no deterioration in the patient's
condition. NB: Redness of the skin may persist for some time after resolution of the infection.
23. Responding
Persistent or progressive redness in the first 24 hrs does not always indicate failed oral treatment. Improvement is indicated by
wrinkling of the skin, reduced pain and often decreased swelling. As long as the global clinical picture is of a well patient continue
oral antibiotics. Educate regarding limb elevation to assist recovery.

CELLULITIS IN ADULTS April 2018 Page 11 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
24. Not responding
Consider IV therapy if not responding.
Consider blood tests for FBC, CRP and creatinine to help guide management, particularly for the elderly or high-risk patients.
25. Exclusions for community IV therapy
Exclusions for community IV management include:
• if the patient has a history of immediate penicillin hypersensitivity (severe skin rash including welts, features of anaphylaxis,
angioedema) or any cephalosporin allergy then CefAZOLIN should not be prescribed and specialist advice is required
• use of intravenous antibiotics with an eGFR <35
• severe illness/signs of sepsis
• management of bacterial cellulitis and erysipelas in secondary care
• those aged <16 years of age
• diabetic foot infections - refer to General Surgery
• deep penetrating wounds
• bites - animals or human
• chemotherapy/neutropenic
26. Commence community IV therapy
For patients with moderate cellulitis, oral therapy (includes probenecid- boosted regimes) should be considered as a
first option. If a patient fails a trial of oral antibiotics, and is still clinically stable, then the commencement of IV antibiotic
therapy is appropriate.
Suitability for community IV management - refer to criteria.
NB:
• Note exclusion criteria
• See guidelines below for dose adjustments required if BMI >35 or impaired renal function
Standard dosages BMI <35:
eGFR >55:
• CefAZOLIN 2g IV daily
• Probenecid 1g oral twice daily with food
eGFR 35 - 55:
• CefAZOLIN 2g IV twice daily
• NB: Probenecid not given
Weight adjusted doses:
Additional doses needed only for the first 2 days thereafter standard doses apply as per eGFR
BMI 35 - 40 OR weight 100kg - 150kg:
• CefAZOLIN 3g IV twice daily (12 hourly)
• NB: Probenecid not given
BMI is 40 OR weight >150kg:
• consult with Clinical Pharmacist on call for advice
Note:
• if the patient has a history of immediate penicillin hypersensitivity (severe skin rash including welts, features of anaphylaxis,
angioedema) or any cephalosporin allergy then CefAZOLIN should not be prescribed and specialist advice is required. Consult

CELLULITIS IN ADULTS April 2018 Page 12 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
with the on-call Infectious Diseases physician - (06) 356 9169.
• options include vancomycin, clindamycin, co-trimoxazole or teicoplanin.
• if the patient has a history of mild penicillin allergy/hypersensitivity (mild rash, gastrointestinal symptoms), then CefAZOLIN may
be prescribed.
• overnight doses of antibiotics not recommended between the hours of 10pm-8am (unless there are special clinical/social
circumstances) - refer to dosing frequency guide
Provider Checklist:
• mark area with washable marker pen • prescribe analgesia if appropriate - avoid NSAIDS as they may aggravate BHC infections
• consider referral to District Nursing Service if unable to manage wound or if the patient does not have good access to their
general practice (i.e. are immobile, particularly those patients with lower limb cellulitis or those patients that live rurally)
• NB: if referring to DNS, send referral form immediately
• provide patient with information about cellulitis
• schedule follow - up appointment for review
• consider taking baseline blood tests (FBC, CRP, creatinine) - particularly for elderly and high-risk patients
Follow-up after 48 hours is mandatory for patients that are prescribed IV therapy. If not able to follow-up the patient, arrange for an
Accident and Medical Centre to review patient - complete Transfer of Care/Handover form. Clinical documentation will need to be
forwarded to the nominated Accident and Medical Centre.
27. Follow-up 5-7 days
Follow-up is required after 5 - 7 days to ensure resolution of cellulitis. If unresolved, review patient and consider:
1. extending oral therapy
OR
2. discussion with infectious diseases physician- options may include prescribing clindamycin - this requires specialist
endorsement (06) 356 9169
Consider predisposing factors and refer to Community Clinical Nurses - Long Term Conditions as appropriate. If the wound is not
healing or the patient is at high risk of recurrence secondary to suspected arterial or venous disease consider referral to the District
Nursing Service for ongoing management and Doppler assessment.
• NB: if referring to DNS, send referral form immediately
29. GP review after 48 hours
Improvement is indicated by wrinkling of skin, reduced pain and often decreased swelling. Response to treatment may be slow. NB:
Redness of the skin may persist for some time after improvement of the infection.
As long as the global clinical picture is of a well patient, commence oral antibiotics and give last IV dose on day 3.
NB: If patient has been referred to District Nursing Service, send update from review immediately.
If there is not satisfactory progress at this stage, consider extending IV therapy.
If the patient is deteriorating, the patient must be discussed with Infectious Diseases physician or acute on-call medical
physician prior to continuing IV treatment - phone (06) 356 9169.
31. Responding
Persistent redness does not always indicate failed treatment. Improvement is indicated by wrinkling of the skin, reduced pain and
often decreased swelling. As long as the global clinical picture is of a well patient transition to oral antibiotics.

CELLULITIS IN ADULTS April 2018 Page 13 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
Educate regarding limb elevation to assist recovery.
32. Not responding
Consider extending IV therapy for a further 2 days if not responding. Consider blood tests for FBC, CRP and creatinine to help guide
management, particularly for the elderly or high-risk patients.
Consider consulting with the Infectious Diseases physician or on-call medical physician if there is a poor or slow response to
treatment - (06) 356 9169.
33. Commence oral therapy
Antibiotic Treatment - First Choice:
• Flucloxacillin 500mg, qid for seven days (to be taken with food) - if patient weighs >100kg, prescribe 1g, four times daily,
for seven days (to be taken with food)
OR (if flucloxacillin not tolerated)
• Cefalexin 500mg, qid for seven days
Antibiotic Treatment - Alternatives:
• Roxithromycin 150mg, bd or 300mg daily, for seven days
• Erythromycin 400mg, qid
OR (if MRSA present)
• Co-trimoxazole 160+800mg (two tablets), bd, for five - seven days
34. IV therapy continued
Standard dosages BMI <35:
eGFR 35 - 55:
• CefAZOLIN 2g IV twice daily
eGFR > 55:
• CefAZOLIN 2g IV daily
• Probenecid 1g oral twice daily
Weight adjusted doses:
Patients will have now completed 48 hours of high dose IV antibiotics and can now be changed to standard doses
depending on eGFR
Note:
• if the patient has a history of immediate penicillin hypersensitivity (severe skin rash including welts, features of anaphylaxis,
angioedema) or any cephalosporin allergy then cephazolin should not be prescribed and specialist advice is required. Consult
with the on-call Infectious Diseases physician or on-call medical physician - (06) 356 9169
• options include vancomycin, clindamycin, co-trimoxazole or teicoplanin
• If the patient has a history of mild penicillin allergy/hypersensitivity (mild rash, gastrointestinal symptoms), then cephazolin may
be prescribed
• overnight doses of antibiotics not recommended between the hours of 10pm-8am (unless there are special clinical/social
circumstances) - please refer to dosing frequency guide
Provider Checklist:
• mark area with washable marker pen
• prescribe analgesia if appropriate
• consider referral to District Nursing Service if unable to manage wound or if the patient does not have good access to their
general practice (i.e. are immobile, particularly those patients with lower limb cellulitis or those patients that live rurally)

CELLULITIS IN ADULTS April 2018 Page 14 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
• NB: if referring to DNS, send referral form immediately
• provide patient with information about cellulitis
• schedule follow-up appointment for review
• consider taking baseline blood tests (FBC, CRP, creatinine) - particularly for elderly and high-risk patients
36. GP review after 48 hours
Improvement is indicated by wrinkling of skin, reduced pain and often decreased swelling.
NB: If patient has been referred to District Nursing Service, send update from review immediately.
If the patient is deteriorating or not improving, the patient must be discussed with Infectious Diseases physician or on-call
medical physician prior to continuing IV treatment - phone (06) 356 9169.
37. Follow-up 5-7 days
Follow-up is required after 5 - 7 days to ensure resolution of cellulitis. If unresolved, review patient and consider:
1. extending oral therapy
OR
2. discussion with infectious diseases physician - options may include prescribing clindamycin - this requires specialist
endorsement (06) 356 9169
Consider predisposing factors and refer to Community Clinical Nurses - Long Term Conditions as appropriate. If the wound is not
healing or the patient is at high risk of recurrence secondary to suspected arterial or venous disease consider referral to the District
Nursing Service for ongoing management and Doppler assessment.
• NB: if referring to DNS, send referral form immediately
38. Seek specialist advice
If patient not improving, discuss with Infectious Diseases physician or on-call medical physician for guidance on future treatment -
phone (06) 356 9169.
39. Oral therapy
Antibiotic Treatment - First Choice:
• Flucloxacillin 500mg, qid for seven days (to be taken with food) - if patient weighs >100kg, prescribe 1g, qid for seven days
(to be taken with food)
OR (if flucloxacillin not tolerated)
• Cefalexin 500mg, qid for seven days
Antibiotic Treatment - Alternatives:
• Roxithromycin 150mg, bd or 300mg daily, for seven days
• Erythromycin 400mg, qid
OR (if MRSA present)
• Co-trimoxazole 160+800mg (two tablets), bd, for five - seven days

CELLULITIS IN ADULTS April 2018 Page 15 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
Cellulitis in Adults
Provenance Certificate
Overview
Overview | Editorial methodology | References | Contributors | Disclaimers
This document describes the provenance of MidCentral District Health Board’s Cellulitis in Adults pathway. This pathway is regularly updated to include new, quality-assessed evidence, and practice- based knowledge from expert clinicians. Please see the Editorial Methodology section of this document for further information.
This localised pathway was last updated in July 2017.
For information on changes in the last update, see the information point entitled ‘Updates to this care map’ on each page of the pathway.
One feature of the “Better, Sooner, More Convenient” (BSMC) Business Case, accepted by the Ministry of Health in 2010, was the development of 33 collaborative clinical pathways (CCP).
The purpose of implementing the CCP Programme in our DHB is to:
• Help meet the Better Sooner More Convenient Business Case aspirational targets, particularly the following:
o Reduce presentations to the Emergency Department (ED) by 30%
o Reduce avoidable hospital admissions to Medical Wards and Assessment Treatment and Rehabilitation for over-65-year-olds by 20%
o Reduce poly-pharmacy in the over-65-year-olds by 10%
• Implement a tool to assist in planning and development of health services across the district, using evidence-based clinical pathways.
• Provide front line clinicians and other key stakeholders with a rapidly accessible check of best practice;
• Enhance partnership processes between primary and secondary health care services across the DHB.
To cite this pathway, use the following format:
Map of Medicine. Medicine. MidCentral District View. Palmerston North: Map of Medicine; 2014 (Issue 1).
Editorial methodology
This care map was based on high-quality information and known Best Practice guidelines from New
Zealand and around the world including Map of medicine editorial methodology. It has been checked by
individuals with front-line clinical experience (see Contributors section of this document).
Map of Medicine pathways are constantly updated in response to new evidence. Continuous evidence
searching means that pathways can be updated rapidly in response to any change in the information
landscape. Indexed and grey literature is monitored for new evidence, and feedback is collected from
users year-round. The information is triaged so that important changes to the information landscape are
incorporated into the pathways through the quarterly publication cycle.

CELLULITIS IN ADULTS April 2018 Page 16 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
References
This care map has been developed according to the Map of Medicine editorial methodology. The content of this care map is based on high-quality guidelines and practice-based knowledge provided by contributors with front-line clinical experience. This localised version of the evidence-based, practice- informed care map has been peer-reviewed by stakeholder groups and the CCP Programme Clinical Lead.
Clinical Resource Efficiency Support Team (CREST). Guidelines on the management of cellulitis in adults.
Belfast: CREST; 2005. Available from: http://www.gain-ni.org/Library/Guidelines/cellulitis-guide.pdf
Hedström, S. A., & Kahlmeter, G. U. N. N. A. R. (1980). Dicloxacillin and flucloxacillin twice daily with
probenecid in staphylococcal infections. A clinical and pharmakokinetic evaluation. Scandinavian journal
of infectious diseases,12(3), 221.
Krogsgaard, M. R., Hanson, B. A., Slotsbjerg, T., & Jensen, P. (1994). Should Probenecid be Used to Reduce
the Dicloxacillin Dosage in Orthopaedic Infections? A Study of the Dicloxacillin‐Saving Effect of
Probenecid.Pharmacology & toxicology, 74(3), 181-184.
Contributors
MidCentral DHB’s Collaborative Clinical Pathway editors and facilitators worked with clinical stakeholders such as front-line clinicians and pharmacists to gather practice-based knowledge for its care maps.
The following individuals contributed to the update of this care map:
Dr Paul Cooper, Medical Director & Clinical Director Acute Care, Central PHO (Primary Care Clinical Lead)
Dr Ann MacIntyre, Infectious Diseases Specialist, MidCentral DHB (Secondary Care Clinical Lead)
Dr Richard Everts, Specialist Physician, Medical Microbiologist, Infectious Diseases Specialist, Nelson Hospital
Beth McPherson, Clinical Nurse Specialist (Lead), Acute Care Team, Health Care Development
Leanne Bell, Clinical Nurse Specialist (Lead), Acute Care Team, Health Care Development
Kim Vardon, CCP Programme, Central PHO (Editor)
The following individuals contributed to the original development of this care map:
Dr Paul Cooper, General Practitioner, Te Waiora/Medical Director, Acute Care, Central PHO
(Primary Care Clinical Lead)
Dr Rudyard Yap, Infectious Diseases Physician, MidCentral Health (Secondary Care Clinical Lead)
Dr Mark Beale, Clinical Director of Medicine, MidCentral Health
Lorraine Welman, Chief Pharmacist, MidCentral Health
Denise White, Nursing Projects Lead, MidCentral Health
Chris Hewison, Microbiologist, Medlab Central
Deborah Davies, Clinical Nurse Specialist (Lead), Primary Health Care, Health Care Development, MidCentral Health
Jess Long, Programme Manager, Collaborative Clinical Pathways Programme, MidCentral DHB
(Editor)
Leanne Bell, Clinical Nurse Specialist, Acute Care, Health Care Development
Ben Hickman, Clinical Pharmacist, Hospital Pharmacy, MidCentral Health

CELLULITIS IN ADULTS April 2018 Page 17 of 17
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
Disclaimers
Clinical Board Central PHO, MidCentral DHB
It is not the function of the Clinical Board Central PHO, MidCentral DHB to substitute for the role of the clinician, but to support the clinician in enabling access to know-how and knowledge. Users of the Map of Medicine are therefore urged to use their own professional judgement to ensure that the patient receives the best possible care. Whilst reasonable efforts have been made to ensure the accuracy of the information on this online clinical knowledge resource, we cannot guarantee its correctness and completeness. The information on the Map of Medicine is subject to change and we cannot guarantee that it is up-to-date.