-
8/17/2019 Cellular Response to Tissue Hypoxia and Its
Involvenment in Progression
1/8
Pathology International 2005; 55: 603–610
Blackwell Science, LtdOxford, UKPINPathology
International1320-54632005 Japanese Society of PathologyOctober
200555106036 10Review ArticlePhysiology and pathology of hypoxiaE.
Ikeda
Correspondence: Eiji Ikeda, MD, PhD, Department of
Pathology,
Keio University School of Medicine, 35 Shinanomachi,
Shinjuku-ku,
Tokyo 160-8582, Japan. Email: [email protected]
Received 18 April 2005. Accepted for publication 20 April
2005.
Review Article
Cellular response to tissue hypoxia and its involvement
indisease progression
Eiji Ikeda
Department of Pathology, Keio University School of Medicine,
Shinjuku-ku, Tokyo, Japan
Multicellular organisms show adaptive reactions for their
survival when they are exposed to an atmosphere with
reduced oxygen concentration. These reactions include
increase in respiratory volume, switch from aerobic to
anaerobic metabolism, erythropoiesis and angiogenesis.
For these reactions, cells must change the expression ofseveral
hypoxia-responsive molecules such as erythropoi-
etin and vascular endothelial growth factor. Hypoxia-
responsible element (HRE) was delineated in the genes of
hypoxia-responsive molecules as the sequence indispens-
able for their hypoxia-induced transcriptional activation,
and hypoxia-inducible factor 1 (HIF-1) was identified as
a transcriptional factor that binds to HRE and regulates
the expression of various hypoxia-responsive molecules.
Increasing evidence has revealed that HIF-1 is a key mole-
cule regulating the cellular response to tissue hypoxia.
HIF-
1 is composed of two subunits, HIF-1αααα and HIF-1ββββ,
and
HIF-1 activity depends mainly on the intracellular level of
HIF-1αααα protein, which is regulated to be in inverse
relationto the oxygen concentration by an oxygen-dependent
enzyme, prolyl hydroxylase 2 (PHD2). Thus, cells respond
to tissue hypoxia by sensing the oxygen concentration as
the enzyme activity of PHD2, regulating the HIF-1 activity
and consequently changing the expression of various
hypoxia-responsive molecules. Cellular response con-
trolled by hypoxia-HIF-1 cascade is also involved in patho-
logical situations such as solid tumor growth, diabetic
retinopathy and rheumatoid arthritis. Under these patholog-
ical situations, the activation of hypoxia-HIF-1 cascade
often leads to the acceleration of disease progression.
Understanding an aspect of disease progression triggered
by tissue hypoxia might provide a clue to new therapeutic
strategies for intractable diseases.
Key words: angiogenesis, diabetic retinopathy, disease
pro-
gression, erythropoietin, HIF-1, hypoxia, rheumatoid
arthritis,
tumor, ubiquitin, VEGF
Under physiological conditions, cells in multicellular
organ-
isms utilize oxygen as the source of energy. Oxygen in the
air is taken into the body from lungs, and transported to
peripheral tissues by red blood cells. Oxygen supply
insuffi-
cient for the need of tissues makes it difficult for the cells
toperform adequate aerobic metabolism, resulting in the
impairment of their physiological functions. Severe hypoxia
causes necrosis of tissues, which might lead to the death of
an organism. Under hypoxic situations, organisms have sev-
eral reactions. For example, in the acute phase of hypoxic
stress, the cells change their metabolism from aerobic to
anaerobic states, and the organisms increase the respiratory
volume to take in a greater amount of oxygen from the atmo-
sphere. As chronic reactions, erythropoiesis as well as
angio-
genesis into ischemic tissues are promoted. Both the
erythropoiesis and angiogenesis can improve the efficiency
of oxygen transportation to peripheral tissues. These reac-tions
under hypoxia are thought to be acquired by organisms
during evolution in order to survive even if the oxygen con-
centration of the atmosphere is reduced due to unexpected
causes. However, it should be noted that these adaptive
reactions would be the cause of disease progression and
determine the prognosis of patients with solid tumors, dia-
betic retinopathy and rheumatoid arthritis. In this review,
how
cells, tissues or organisms respond to hypoxic stimuli, and
how those hypoxia-induced reactions would lead to the accel-
eration of disease progression, are summarized, with refer-
ence to the remodeling of the vascular system under hypoxic
situations.
CELLULAR RESPONSE TO TISSUE HYPOXIA
The gene expression profile of cells under hypoxia differs
from that under normoxia, and the production of certain
growth factors, cytokines and enzymes is known to be con-
trolled by oxygen concentration in tissues.1 These
molecules,
which can be called ‘hypoxia-responsive molecules’, include
erythropoietin (EPO),2 vascular endothelial growth
factor
mailto:[email protected]:[email protected]
-
8/17/2019 Cellular Response to Tissue Hypoxia and Its
Involvenment in Progression
2/8
604 E. Ikeda
(VEGF),3 tyrosine hydroxylase,4 phosphoglycerate
kinase 1
and lactate dehydrogenase A,5 most of which are
implicated
in adaptive processes of organisms to hypoxic circum-
stances, for example, erythropoiesis, angiogenesis, increase
in respiratory volume and switch of metabolism to an anaer-
obic state. Among these molecules, EPO and VEGF have
been intensively studied with regard to the molecular
mech-anisms of their hypoxic induction, and the results have
pro-
vided a valuable clue to the molecular background of
cellular
response to hypoxia.
Mechanisms of hypoxia-induced expression of EPO
EPO was originally recognized as a hormone to stimulate
erythroid progenitor cells to promote
erythropoiesis.2 Recent
studies have revealed a broad range of EPO functions, which
are not confined to erythropoiesis, and it is now accepted
that EPO is also involved in the proliferation,
differentiationand anti-apoptosis of non-erythroid cells such as
endothelial
cells, vascular smooth muscle cells, neurons and neuronal
progenitor cells.6 EPO is generated by the fetal liver
during
development and the kidney after birth. Hep3B cells from
hepatocellular carcinoma, which can produce EPO in
vitro ,
have been used to analyze the molecular mechanisms of
EPO expression.2,7 Expression of EPO is known to be
con-
trolled by the oxygen concentration in the atmosphere, and
hypoxia stimulates the production of EPO through upregula-
tion of the transcription of the EPO gene. Through
analyses
of the EPO gene, Wang and Semenza delineated a
sequence of the hypoxia-responsible element (HRE) in
the3′-flanking region of the EPO gene that is essential
for
hypoxia-induced transcriptional activation, and further
identi-
fied the existence of a binding factor to the HRE, which is
designated hypoxia-inducible factor 1 (HIF-1).7 Binding
of
HIF-1 to the HRE was shown to be inversely related to the
oxygen concentration around the cells. It was further demon-
strated that the binding of HIF-1 to the HRE sequence is
also
enhanced in cells that do not produce EPO, implying the
general involvement of HRE and HIF-1 in the cellular
response to hypoxia that is not confined to the change in
the
transcriptional rate of EPO gene.8
Involvement of HIF-1 in the hypoxia-induced expression
of VEGF
Angiogenesis is one of the important adaptive reactions to
restore the oxygen transport to ischemic tissues. It is true
that angiogenesis improves blood supply to focal tissues,
but
the angiogenesis itself often becomes a trigger of disease
progression, which is later discussed in the present
article.
Proliferation of blood vessels is determined by the balance
between angiogenic and antiangiogenic activities in the
focal
tissues. Accumulated evidence has demonstrated that,
among the vasoactive molecules, VEGF is the central growth
factor controlling various physiological and pathological
angiogenesis, and therefore the formation of new blood
vessels depends mainly on the protein level of VEGF in
tissues.
9–11
The VEGF gene contains eight exons (exons 1–8),
which
enables VEGF to have several isoforms by alternative splic-
ing, i.e. VEGF121, VEGF145, VEGF165, VEGF189 and
VEGF206
in the human.10,11 Among these isoforms, major
isoforms
expressed in various pathological situations such as solid
tumor growth, diabetic retinopathy and rheumatoid arthritis
are VEGF121, VEGF165 and VEGF189.10–13 The
sequences
encoded by exons 6 and 7 are rich in basic amino acids, and
therefore confer high binding affinity to the extracellular
matrices as well as low diffusibility to VEGF189, which con-
tains the amino acids from both exons 6 and 7. In contrast
to VEGF189, VEGF121, which lacks the amino acids encodedby both
exons 6 and 7, is highly diffusible in tissues.
VEGF165, which contains the amino acids encoded by exon
7 but not those by exon 6, has intermediate biochemical
properties between VEGF121 and VEGF189 in the context
of
diffusibility in tissues.10,11 The difference in
biochemical prop-
erties leads to the difference in biological properties
between
the isoforms, and the involvement of VEGF in the progres-
sion of certain diseases is shown to be dependent on the
expression pattern of isoforms.12,13 As concerns the
recep-
tors for VEGF, two high-affinity receptors, VEGFR-1 (Flt1)
and VEGFR-2 (KDR/Flk1), have been identified.10,11 In
addi-
tion to these high-affinity receptors, neuropilin-1, which
isoriginally known to be a factor regulating the formation of
synapses between neurons, was found to associate with
VEGFR-2 to form the isoform-specific receptor complex for
VEGF165.14
Similarly to EPO, the expression of VEGF is controlled by
oxygen concentration, and angiogenesis into hypoxic tissues
can be triggered by hypoxia-induced expression of
VEGF.9,15,16 Various types of in vitro cultured
cells can pro-
duce VEGF in response to hypoxia. Analyses of the human
VEGF gene have revealed that the consensus binding
site
for HIF-1 exists in the 5′-flanking region, and that the
binding
of HIF-1 to the VEGF gene is indispensable for the
transcrip-tional activation of VEGF by hypoxia.3,17 Thus,
hypoxia-
induced expression of both EPO and VEGF is under the
control of HIF-1. Subsequently, the expression of various
hypoxia-responsive molecules other than EPO and VEGF is
also shown to be controlled by HIF-1, demonstrating that
HIF-1 is a key molecule to regulate the cellular response to
hypoxia.18–21
Through analyses of hypoxia-induced expression of VEGF,
it was also demonstrated that hypoxia can increase the
VEGF mRNA level by inhibiting the degradation of
mRNA.3,22
-
8/17/2019 Cellular Response to Tissue Hypoxia and Its
Involvenment in Progression
3/8
Physiology and pathology of hypoxia 605
As regards the mechanisms of VEGF mRNA
stabilization,
the destabilizing sequences, together with the factors that
bind to those sequences in hypoxic cells to stabilize the
mRNA, have been reported in 5′-untranslated, coding and
3′-untranslated regions.23,24
Among the isoforms of VEGF, a difference in the contribu-
tion to disease progression is noted. A crucial role
forVEGF165 in the angiogenesis of diabetic retinopathy
and
rheumatoid arthritis was suggested through analyses of sur-
gically resected samples.12,13 However, until now, there
have
been no definitive data concerning the mechanisms of
isoform-specific expression of VEGF.
As concerns the expression of VEGF receptors, VEGFR-
1 expression is upregulated in hypoxic endothelial cells,
and
promoter analysis delineated the sequence responsible for
hypoxia-induced transcriptional activation of VEGFR-1,
which contains the consensus binding site for HIF-1.
Hypoxic induction of VEGFR-2 is somewhat controversial,
although VEGFR-2 expression by hypoxia was reported withan in
vivo experimental system. This hypoxic induction of
VEGFR-2 is thought to be indirect and mediated by other
molecules that are induced by hypoxia, because the consen-
sus binding site for HIF-1 was not found in the
VEGFR-2
gene.10
HIF-1 and HIF family
As aforementioned, HIF-1 is a factor controlling the tran-
scriptional rates of various hypoxia-responsive molecules in
response to the oxygen concentration around cells.20
ActiveHIF-1 is a heterodimer composed of two subunits,
HIF-1α
and HIF-1β, both of which belong to a protein superfamily
containing the basic helix–loop–helix (bHLH) and the Per–
Arnt–Sim (PAS) domains.25 In general, members of the
bHLH-PAS protein superfamily are involved in cellular func-
tions that are activated in response to the changes of envi-
ronment.21,26 They include arylhydrocarbon receptor
(AhR)
and arylhydrocarbon receptor nuclear translocator (Arnt) for
the pollution of the environment, period (Per) for the
circa-
dian rhythm, single-minded (Sim) for the development of
central nervous system and trachealess (Trh) for the devel-
opment of salivary glands and trachea. HIF-1β, which waslater
found to be identical to Arnt, is constitutively expressed
independent of environmental oxygen concentration, while
the expression of HIF-1α is negligible under normoxia
and
induced under hypoxia. Up to now, HIF-1α, HIF-2α and
HIF-
3α have been identified and cloned as the members of
HIFα
family that can dimerize with HIF-1β and bind to HRE in
the
genes of hypoxia-responsive molecules. HIF-2α is also
known as endothelial PAS domain protein 1 (EPAS 1), HIF-
1-like factor (HLF) or HIF-1-related factor (HRF). HIF-3α
appears not to activate the transcription of target genes
due
to the lack of the transcription activation domain.21
Among
HIFα family members, HIF-1α is thought to be the key
mol-
ecule regulating the cellular response to various
physiologi-
cal and pathological hypoxia, although the critical role of
HIF-2α, not HIF-1α, is noted in certain pathological
situations.21,27
Regulation of the intracellular level of HIF-1αααα and
the
cellular sensor for oxygen concentration
Mechanisms of hypoxia-induced expression of HIF-1α have
been intensively studied, and the intracellular level of
HIF-1α
protein under reduced oxygen concentration was found
to be increased mainly through stabilization of the protein.
Turnover of HIF-1α protein is regulated by the
ubiquitin–
proteasome system, in which target proteins are degraded
by proteasome depending on the ubiquitylation of pro-
teins.28,29
Ubiquitylation of the target proteins is catalyzed bythe
enzyme complex composed of E1 (ubiquitin-activating
enzyme), E2 (ubiquitin-conjugating enzyme) and E3 (ubiq-
uitin ligase). Under normoxia, the level of HIF-1α protein
is
kept low through rapid ubiquitylation and subsequent protea-
somal degradation. HIF-1α protein becomes susceptible
to
rapid ubiquitylation through hydroxylation of proline
residues
at Pro-402 and Pro-564 by prolyl hydroxylase 2 (PHD2),
which requires oxygen for its enzyme activity.30–32 In
cells
under hypoxia, the ubiquitylation and subsequent degrada-
tion of HIF-1α protein is suppressed due to the decrease
in
PHD2 activity, and therefore the level of HIF-1α
protein
increases. In addition, the activity of HIF-1 as a
transcriptionfactor is also controlled by hydroxylation of
HIF-1α protein.
Hydroxylation of asparagine residue at Asn-803 inhibits the
interaction between HIF-1α protein and p300, which is
essential for the transcriptional activity of
HIF-1.33 Because
the factor inhibiting HIF (FIH) that hydroxylates Asn-803 of
HIF-1α protein is also an oxygen-dependent enzyme, the
transcriptional activity of HIF-1 increases under hypoxia
due
to the suppressed hydroxylation at Asn-803.34,35 Namely,
cells
can control the transcription of HIF-1-regulated genes by
sensing the oxygen concentration as the activities of
oxygen-
dependent enzymes PHD2 and FIH, and consequently reg-
ulating the intracellular level as well as the
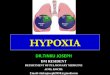
transcriptionalactivity of HIF-1 (Fig. 1).36
The ubiquitin–proteasome system degrades the proteins
with target specificity. This target specificity is attributed
to
the E3 component of the enzyme complex, and the E3 com-
ponent responsible for ubiquitylation of HIF-1α protein
was
found to be identical to the product of the von
Hippel–Lindau
tumor suppressor gene (pVHL; Fig. 1).37,38 This finding
shed
light on the tumorigenesis of renal cell carcinoma,
pheochro-
mocytoma and hemangioblastoma because pVHL is often
mutated in these tumors.
-
8/17/2019 Cellular Response to Tissue Hypoxia and Its
Involvenment in Progression
4/8
606 E. Ikeda
TISSUE HYPOXIA AND DISEASE PROGRESSION
Pathological tissues often become hypoxic as the result of
vascular obstruction with thrombi, vascular compression by
increased tissue hydrostatic pressure, increased tissue cell
density and so forth. Tissue hypoxia plays an important role
in determining the clinical course of certain diseases, for
example solid tumor growth, diabetic retinopathy and rheu-
matoid arthritis, and the contribution of tissue hypoxia to
disease progression is often mediated by the remodeling of
vasculature such as angiogenesis and loss of tissue-specific
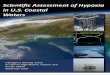
vascular structures (Fig. 2).
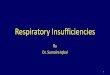
Figure 1 Cellular response to hypoxia. Cells sense the oxygen
concentration as the activities of oxygen-dependent enzymes,
prolyl
hydroxylase 2 (PHD2) and factor inhibiting hypoxia-inducible
factor (FIH), which determine the hypoxia-inducible factor-1
(HIF-1) function and
consequently the transcriptional rates of HIF-1-regulated genes.
Under normoxia (blue arrows), the intracellular level of
HIF-1α is kept low
by rapid ubiquitylation and subsequent proteasomal degradation,
which depend on the hydroxylation of proline residues by PHD2; the
activity
of HIF-1α as a transcription factor is also inhibited by
the hydroxylation of asparagine residue by FIH. In contrast, under
hypoxia (red arrows),
both the intracellular level and the transcriptional activity of
HIF-1α increase as a result of suppressed PHD2 and FIH
activities, respectively.
Consequently, HIF-1α forms a heterodimer with
HIF-1β and changes the transcriptional rates of
HIF-1-regulated genes under hypoxia. pVHL,
product of the von Hippel–Lindau tumor suppressor gene.
p V H L
HIF-1
AsnPro
p300
p300OH OH
pVHL
HIF-1
AsnPro
HIF-1
HIF-1
HIF-1
AsnPro
p300
PHD2, FIH
Normoxia
Hypoxia
Proteasomal degradationUbiquitylation
Inhibition of transcriptional activity
[Nucleus]
Changes in transcriptional rates
HIF-1-regulated genes
Suppression of proteasomal degradation
Increased transcriptional activity
[Oxygen-dependent enzymes]
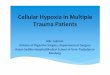
Figure 2 Physiological and patholog-
ical reactions to tissue hypoxia. Physi-
ological reactions of a multicellularorganism under hypoxia
share com-
mon pathways with pathological reac-
tions causing the disease progression.
Hypoxia
Disease progressionRemodeling of vascular system
Angiogenesis Solid tumor growth
Diabetic retinopathyRheumatoid arthritis
of HIF-1 regulated genes
Erythropoietin
VEGF
Tyrosine hydroxylase
Phosphoglycerokinase 1
Lactate dehydrogenase A
VEGFR-1
Physiological reactions
Pathological reactions
Erythropoiesis
Angiogenesis
Metabolic changes
Loss of tissue-specific properties
Vascular occlusion
Anti-apoptosis
Changes in the expression
Survival of cells, tissues
and organisms
-
8/17/2019 Cellular Response to Tissue Hypoxia and Its
Involvenment in Progression
5/8
Physiology and pathology of hypoxia 607
Solid tumor
Oxygen concentration inside solid tumors is reduced, and
there are studies to show the contribution of intratumoral
hypoxia to the tumor aggressiveness and poor prognosis of
patients.39,40 Resistance to chemotherapy and radiation
ther-
apy can be attributed, at least in part, to the hypoxic
conditionof tumor cells.41 Hypoxia confers these aggressive
properties
on the tumors through either the remodeling of tumor vascu-
lature or the direct phenotypic changes of tumor cells
themselves.
Growth of solid tumors is angiogenesis dependent. As the
tumor mass becomes larger, tumor cells, especially at the
center of the mass, are exposed to the more hypoxic condi-
tion, and tumor cells cannot proliferate to form a mass
beyond
a few millimeters in diameter without angiogenesis. Occur-
rence of angiogenesis confers the properties of continuous
growth as well as metastasis on the tumor, and therefore it
can be said that the angiogenic switch is a critical
checkpointduring tumor progression.42 It has been
demonstrated that
among angiogenic or antiangiogenic factors, the level of
VEGF is most highly correlated with the degree of angiogen-
esis in various kinds of tumors.43,44 A critical role for
HIF-1α
in tumor progression has also been noted through analyses
of various tumors, although there are tumors in which HIF-
2α, not HIF-1α, is essential for tumorigenesis.27,45
Overex-
pression of HIF-1α in tumor tissues and its correlation
with
degree of tumor angiogenesis as well as poor prognosis have
been demonstrated in patients with tumors such as brain
tumors, endometrial carcinomas, ovarian carcinomas, breast
carcinomas and head and neck tumors.46–51
Although studieswith mouse xenograft transplantation
models have yielded
contradictory results regarding the role of HIF-1α in
tumori-
genesis,52–54 a study focusing on the transition from
avascular
to vascular tumors demonstrated that nuclear localization of
HIF-1α and subsequent VEGF upregulation in tumor cells
are
important for initiating tumor angiogenesis.42 The question
is
raised regarding the trigger of nuclear accumulation of HIF-
1α in tumor cells during the course of tumor
progression.
Although HIF-1 can be activated by non-hypoxic pathways,
hypoxia inside the growing tumor mass is the most probable
candidate for the activation of HIF-1α cascade in tumor
cells,
and this hypothesis is supported by the data that both
HIF-1α and VEGF expression are upregulated predominantly
in
tumor cells around the necrotic areas of highly vascularized
tumor mass in glioblastoma.15,16,46 Therefore, it can be
true
that angiogenesis triggered by the hypoxia-HIF-1α-VEGF
cascade plays an important, even if not essential, role in
tumor progression to the more aggressive phenotypes.
Hypoxia accelerates tumor growth and metastasis by act-
ing directly on tumor cells themselves.41 Tumor cells
under
hypoxia can acquire anti-apoptotic and chemoresistant prop-
erties through changes in the expression of
apoptosis-related
molecules, and the involvement of HIF-1α in the tumor
progression to anti-apoptotic phenotype was reported.55
Genomes of tumor cells become unstable under hypoxic
conditions,56 and hypoxia can be the selective pressure
for
the expansion of clones with anti-apoptotic, treatment-
resistant or highly metastatic potential.57 Hypoxia itself
can
be a cause of tumor resistance to therapy because somedrugs and
radiation require oxygen for their toxicity.58
It is interesting to note that pVHL is identical to the E3
component of the enzyme complex responsible for the ubiq-
uitylation and subsequent degradation of HIF-1α.37,38
In
tumor cells that have mutations in pVHL, HIF-1α-mediated
transcription of VEGF is constitutively activated due to the
impaired ubiquitylation of HIF-1α. Thus, independent of the
intratumoral oxygen concentration, the tumor growth can be
accelerated by continuous angiogenesis. However, involve-
ment of mechanisms other than that mediated by over-
production of VEGF are suggested in pVHL-related
tumorigenesis.27,59,60
Diabetic retinopathy
Retinopathy is one of the major complications of diabetes
mellitus and an important cause of adult
blindness.61,62 The
clinical course of diabetic retinopathy is divided into
three
stages: background, preproliferative and proliferative
diabetic
retinopathies. The site attacked primarily in diabetic
retinop-
athy is the blood vessel, and the visual acuity of patients
is
impaired as a result of the vascular remodeling of retinal
vasculature by, for example, vascular occlusion, breakdownof the
blood–retinal barrier (BRB) and angiogenesis. In par-
ticular, retinal angiogenesis that appears in the stage of
pro-
liferative retinopathy leads to serious outcomes such as
vitreous hemorrhage and tractional retinal detachment.
Breakdown of BRB impairs the visual acuity of patients by
causing retinal edema.
Retinal angiogenesis in proliferative retinopathy results in
the formation of fibrovascular tissue that extends from the
retina to the vitreous body and generates adhesion between
them. Through analyses of the vitreous fluid and fibrovascu-
lar tissue from the diabetic retinopathy patients, the
degree
of retinal angiogenesis is shown to be correlated with thelevel
of VEGF protein in the eye.12 Production of VEGF in the
eye of diabetic retinopathy patients can be enhanced by
tissue hypoxia that is thought to be present in the retina
from
a relatively early stage of diabetic retinopathy.
Correlation
between the HIF-1α-mediated VEGF induction in the retina
and the breakdown of BRB is also demonstrated in diabetic
animal models.63 Thus, in addition to the increased
retinal
glucose concentration and the accumulation of advanced
glycation end-products in retinal tissues, tissue hypoxia is
believed to be an important trigger of disease progression
-
8/17/2019 Cellular Response to Tissue Hypoxia and Its
Involvenment in Progression
6/8
608 E. Ikeda
in diabetic retinopathy through the remodeling of retinal
vasculature.
Rheumatoid arthritis
Rheumatoid arthritis is a systemic inflammatory disease of
unknown etiology that mainly involves the joints in the form
of proliferative synovitis. In the affected joints, synovial
tis-
sues proliferate into the joint spaces, exhibiting
hyperplasia
of synovial lining cells as well as inflammatory cell
infiltration
and angiogenesis in sublining layers. As the disesase
progresses, extracellular matrices, especially those of
artic-
ular cartilage, are degraded by proteinases produced by the
proliferating synovial tissues, resulting in the deformation
of
affected joints. Synovial angiogenesis that is initiated at
the
relatively early stage of rheumatoid arthritis enables
inflam-
matory cells to access the synovial tissues, and the inflam-
matory cells in turn promote the angiogenesis by producing
various vaso-active cytokines such as interleukin-8. Thus,
the
angiogenesis and inflammatory cell infiltration interact to
accelerate disease progression, and the critical role of
syn-
ovial angiogenesis in the establishment of proliferative
syno-
vitis has been demonstrated with arthritic animal
models.64,65
Analysis of the surgical specimens of rheumatoid arthritis
has
revealed that synovial angiogenesis depends on the induc-
tion of VEGF synthesis in synovial tissues.13 Together
with
the findings that inflamed synovial tissues are under
hypoxia66
and that the level of HIF-1α protein is elevated in
rheumatoid
synovial tissues,66–68 tissue hypoxia and
HIF-1α-mediated
expression of VEGF are thought to be essential for disease
progression of rheumatoid arthritis by promoting angiogene-
sis. The role of tissue hypoxia in the prolongation of the
synovial inflammatory process of rheumatoid arthritis has
been also highlighted by the finding that hypoxia represses
activation-induced cell death of lymphocytes by supporting
their survival through the hypoxia–HIF-1α cascade.68
CONCLUSION
Progression of certain diseases shares mechanisms with the
physiological cellular response to tissue hypoxia, which are
originally thought to be acquired by multicellular organisms
for their survival under unexpected hypoxic stress. Under-
standing of disease progression from the aspect of tissue
hypoxia is expected to provide targets of new therapeutic
strategies for intractable diseases.
REFERENCES
1 Scheurer SB, Rybak JN, Rosli C, Neri D, Elia G. Modulation
of gene expression by hypoxia in human umbilical cord vein
endothelial cells: A transcriptomic and proteomic study.
Pro-
teomics 2004; 4: 1737–60.
2 Krantz SB. Erythropoietin. Blood 1991; 77:
419–34.
3 Ikeda E, Achen MG, Breier G, Risau W. Hypoxia-induced
tran-
scriptional activation and increased mRNA stability of
vascular
endothelial growth factor in C6 glioma cells. J Biol
Chem 1995;
270: 19 761–66.
4 Czyzyk-Krzeska MF, Furnari BA, Lawson EE, Millhorn DE.
Hypoxia increases rate of transcription and stability of
tyrosinehydroxylase mRNA in pheochromocytoma (PC12) cells. J
Biol
Chem 1994; 269: 760–64.
5 Firth JD, Ebert BL, Pugh CW, Ratcliffe PJ.
Oxygen-regulated
control elements in the phosphoglycerate kinase 1 and
lactate
dehydrogenase A genes: Similarities with the erythropoietin
3′
enhancer. Proc Natl Acad Sci USA 1994; 91: 6496–500.
6 Li F, Chong ZZ, Maiese K. Erythropoietin on a tightrope:
Bal-
ancing neuronal and vascular protection between intrinsic
and
extrinsic pathways. Neurosignals 2004; 13:
265–89.
7 Semenza GL, Wang GL. A nuclear factor induced by hypoxia
via de novo protein synthesis binds to the human
erythropoietin
gene enhancer at a site required for transcriptional
activation.
Mol Cell Biol 1992; 12: 5447–54.
8 Wang GL, Semenza GL. General involvement of hypoxia-
inducible factor 1 in transcriptional response to hypoxia.
Proc Natl Acad Sci USA 1993; 90: 4304–8.
9 Risau W. Mechanisms of angiogenesis. Nature 1997;
386:
671–74.
10 Ferrara N. Molecular and biological properties of
vascular
endothelial growth factor. J Mol Med 1999; 77:
527–43.
11 Ferrara N, Gerber HP, LeCouter J. The biology of VEGF and
its receptors. Nat Med 2003; 9: 669–76.
12 Ishida S, Shinoda K, Kawashima S, Oguchi Y, Okada Y,
Ikeda
E. Coexpression of VEGF receptors VEGF-R2 and neuropilin-
1 in proliferative diabetic retinopathy. Invest Ophthalmol Vis
Sci
2000; 41: 1649–56.
13 Ikeda M, Hosoda Y, Hirose S, Okada Y, Ikeda E. Expression
of vascular endothelial growth factor isoforms and their
recep-
tors Flt-1, KDR, and neuropilin-1 in synovial tissues of
rheuma-
toid ar thritis. J Pathol 2000; 191: 426–33.
14 Soker S, Takashima S, Miao HQ, Neufeld G, Klagsbrun M.
Neuropilin-1 is expressed by endothelial and tumor cells as
an
isoform-specific receptor for vascular endothelial growth
factor.
Cell 1998; 92: 735–45.
15 Plate KH, Breier G, Weich HA, Risau W. Vascular
endothelial
growth factor is a potential tumour angiogenesis factor in
human gliomas in vivo . Nature 1992; 359:
845–48.
16 Shweiki D, Itin A, Soffer D, Keshet E. Vascular
endothelial
growth factor induced by hypoxia may mediate
hypoxia-initiated
angiogenesis. Nature 1992; 359: 843–45.
17 Damert A, Ikeda E, Risau W. Activator-protein-1 binding
poten-
tiates the hypoxia-inducible factor-1-mediated
hypoxia-induced
transcriptional activation of vascular-endothelial growth
factor
expression in C6 glioma cells. Biochem J 1997;
327 (Pt 2):
419–23.
18 Semenza GL. Hypoxia-inducible factor 1: Control of oxygen
homeostasis in health and disease. Pediatr Res 2001;
49: 614–
17.
19 Semenza GL. Hypoxia-inducible factor 1: Oxygen
homeostasis
and disease pathophysiology. Trends Mol Med 2001; 7:
345–
50.
20 Semenza G. Signal transduction to hypoxia-inducible factor
1.
Biochem Pharmacol 2002; 64: 993–98.
21 Covello KL, Simon MC. HIFs, hypoxia, and vascular
develop-
ment. Curr Top Dev Biol 2004; 62: 37–54.
22 Ikeda E, Damert A, Risau W. Molecular mechanisms of
hypoxia-induced angiogenesis. In: Ishimura Y, Shimada M,
-
8/17/2019 Cellular Response to Tissue Hypoxia and Its
Involvenment in Progression
7/8
Physiology and pathology of hypoxia 609
Suematsu M, eds. Oxygen Homeostasis and its Dynamics .
Tokyo: Springer, 1998; 388–99.
23 Levy NS, Chung S, Furneaux H, Levy AP. Hypoxic
stabilization
of vascular endothelial growth factor mRNA by the
RNA-binding
protein HuR. J Biol Chem 1998; 273: 6417–23.
24 Dibbens JA, Miller DL, Damert A, Risau W, Vadas MA,
Goodall
GJ. Hypoxic regulation of vascular endothelial growth factor
mRNA stability requires the cooperation of multiple RNA
elements. Mol Biol Cell 1999; 10: 907–19.25 Wang GL,
Jiang BH, Rue EA, Semenza GL. Hypoxia-inducible
factor 1 is a basic-helix-loop-helix-PAS heterodimer
regulated
by cellular O2 tension. Proc Natl Acad Sci USA 1995; 92:
5510–
14.
26 Kewley RJ, Whitelaw ML, Chapman-Smith A. The mammalian
basic helix-loop-helix/PAS family of transcriptional
regulators.
Int J Biochem Cell Biol 2004; 36: 189–204.
27 Kondo K, Klco J, Nakamura E, Lechpammer M, Kaelin WG Jr.
Inhibition of HIF is necessary for tumor suppression by the
von
Hippel-Lindau protein. Cancer Cell 2002; 1:
237–46.
28 Semenza GL. HIF-1 and tumor progression: Pathophysiology
and therapeutics. Trends Mol Med 2002; 8: S62–7.
29 Mazure NM, Brahimi-Horn MC, Berta MA et al. HIF-1:
Master
and commander of the hypoxic world. A pharmacological
approach to its regulation by siRNAs. Biochem
Pharmacol 2004; 68: 971–80.
30 Berra E, Benizri E, Ginouves A, Volmat V, Roux D,
Pouyssegur
J. HIF prolyl-hydroxylase 2 is the key oxygen sensor setting
low
steady-state levels of HIF-1alpha in normoxia. EMBO
J 2003;
22: 4082–90.
31 Ivan M, Haberberger T, Gervasi DC et al. Biochemical
purifica-
tion and pharmacological inhibition of a mammalian prolyl
hydroxylase acting on hypoxia-inducible factor. Proc Natl
Acad
Sci USA 2002; 99: 13 459–64.
32 Pereira T, Zheng X, Ruas JL, Tanimoto K, Poellinger L.
Identi-
fication of residues critical for regulation of protein
stability and
the transactivation function of the hypoxia-inducible
factor-
1alpha by the von Hippel-Lindau tumor suppressor gene prod-
uct. J Biol Chem 2003; 278: 6816–23.
33 Lando D, Peet DJ, Whelan DA, Gorman JJ, Whitelaw ML.
Asparagine hydroxylation of the HIF transactivation domain a
hypoxic switch. Science 2002; 295: 858–61.
34 Lando D, Peet DJ, Gorman JJ, Whelan DA, Whitelaw ML,
Bruick RK. FIH-1 is an asparaginyl hydroxylase enzyme that
regulates the transcriptional activity of hypoxia-inducible
factor.
Genes Dev 2002; 16: 1466–71.
35 Hewitson KS, McNeill LA, Riordan MV et
al. Hypoxia-inducible
factor (HIF) asparagine hydroxylase is identical to factor
inhib-
iting HIF (FIH) and is related to the cupin structural family.
J
Biol Chem 2002; 277: 26 351–55.
36 Haddad JJ. Oxygen-sensing mechanisms and the regulation
of
redox-responsive transcription factors in development and
pathophysiology. Respir Res 2002; 3: 26.
37 Maxwell PH, Wiesener MS, Chang GW et al. The tumour
sup-
pressor protein VHL targets hypoxia-inducible factors for
oxy-
gen-dependent proteolysis. Nature 1999; 399:
271–75.
38 Cockman ME, Masson N, Mole DR et al. Hypoxia
inducible
factor-alpha binding and ubiquitylation by the von Hippel-
Lindau tumor suppressor protein. J Biol Chem 2000;
275: 25
733–41.
39 Hockel M, Schlenger K, Hockel S, Aral B, Schaffer U,
Vaupel
P. Tumor hypoxia in pelvic recurrences of cervical cancer.
Int
J Cancer 1998; 79: 365–69.
40 Stadler P, Becker A, Feldmann HJ et al. Influence of
the
hypoxic subvolume on the survival of patients with head and
neck cancer. Int J Radiat Oncol Biol Phys 1999; 44:
749–
54.
41 Williams KJ, Cowen RL, Brown LM, Chinje EC, Jaffar M,
Stratford IJ. Hypoxia in tumors: Molecular targets for anti-
cancer therapeutics. Adv Enzyme Regul 2004; 44:
93–108.
42 Fang J, Yan L, Shing Y, Moses MA. HIF-1alpha-mediated up-
regulation of vascular endothelial growth factor, independent
of
basic fibroblast growth factor, is important in the switch to
the
angiogenic phenotype during early tumorigenesis. Cancer
Res
2001; 61: 5731–5.
43 Hasan J, Byers R, Jayson GC. Intra-tumoural microvessel
den-sity in human solid tumours. Br J Cancer 2002; 86:
1566–77.
44 Loureiro RM, D’Amore PA. Transcriptional regulation of
vascu-
lar endothelial growth factor in cancer. Cytokine Growth
Factor
Rev 2005; 16: 77–89.
45 Talks KL, Turley H, Gatter KC et al. The expression
and
distribution of the hypoxia-inducible factors HIF-1alpha and
HIF-2alpha in normal human tissues, cancers, and tumor-
associated macrophages. Am J Pathol 2000; 157:
411–21.
46 Zagzag D, Zhong H, Scalzitti JM, Laughner E, Simons JW,
Semenza GL. Expression of hypoxia-inducible factor 1alpha in
brain tumors: Association with angiogenesis, invasion, and
pro-
gression. Cancer 2000; 88: 2606–18.
47 Birner P, Gatterbauer B, Oberhuber G et al. Expression
of
hypoxia-inducible factor-1 alpha in oligodendrogliomas: Its
impact on prognosis and on neoangiogenesis. Cancer
2001;92: 165–71.
48 Sivridis E, Giatromanolaki A, Gatter KC, Harris AL,
Koukourakis
MI. Association of hypoxia-inducible factors 1alpha and
2alpha
with activated angiogenic pathways and prognosis in patients
with endometrial carcinoma. Cancer 2002; 95:
1055–63.
49 Birner P, Schindl M, Obermair A, Breitenecker G,
Oberhuber
G. Expression of hypoxia-inducible factor 1alpha in
epithelial
ovarian tumors: Its impact on prognosis and on response to
chemotherapy. Clin Cancer Res 2001; 7: 1661–8.
50 Bos R, Zhong H, Hanrahan CF et al. Levels of
hypoxia-inducible
factor-1 alpha during breast carcinogenesis. J Natl Cancer
Inst
2001; 93: 309–14.
51 Koukourakis MI, Giatromanolaki A, Sivridis E et al.
Hypoxia-
inducible factor (HIF1A and HIF2A), angiogenesis, and chemo-
radiotherapy outcome of squamous cell head-and-neck cancer.
Int J Radiat Oncol Biol Phys 2002; 53: 1192–202.
52 Carmeliet P, Dor Y, Herbert JM et al. Role of
HIF-1alpha
in hypoxia-mediated apoptosis, cell proliferation and tumour
angiogenesis. Nature 1998; 394: 485–90.
53 Hopfl G, Wenger RH, Ziegler U et al. Rescue of
hypoxia-
inducible factor-1alpha-deficient tumor growth by wild-type
cells
is independent of vascular endothelial growth factor.
Cancer
Res 2002; 62: 2962–70.
54 Maltepe E, Keith B, Arsham AM, Brorson JR, Simon MC. The
role of ARNT2 in tumor angiogenesis and the neural response
to hypoxia. Biochem Biophys Res Commun 2000; 273:
231–38.
55 Erler JT, Cawthorne CJ, Williams KJ et al.
Hypoxia-mediated
down-regulation of Bid and Bax in tumors occurs via hypoxia-
inducible factor 1-dependent and -independent mechanisms
and contributes to drug resistance. Mol Cell Biol
2004; 24:
2875–89.
56 Young SD, Marshall RS, Hill RP. Hypoxia induces DNA over-
replication and enhances metastatic potential of murine
tumor
cells. Proc Natl Acad Sci USA 1988; 85: 9533–37.
57 Graeber TG, Osmanian C, Jacks T et al.
Hypoxia-mediated
selection of cells with diminished apoptotic potential in
solid
tumours. Nature 1996; 379: 88–91.
58 Teicher BA. Hypoxia and drug resistance. Cancer
Metastasis
Rev 1994; 13: 139–68.
59 Pugh CW, Ratcliffe PJ. The von Hippel-Lindau tumor
suppres-
sor, hypoxia-inducible factor-1 (HIF-1) degradation, and
cancer
pathogenesis. Semin Cancer Biol 2003; 13: 83–89.
-
8/17/2019 Cellular Response to Tissue Hypoxia and Its
Involvenment in Progression
8/8
610 E. Ikeda
60 Maranchie JK, Vasselli JR, Riss J, Bonifacino JS, Linehan
WM,
Klausner RD. The contribution of VHL substrate binding and
HIF1-alpha to the phenotype of VHL loss in renal cell carci-
noma. Cancer Cell 2002; 1: 247–55.
61 Frank RN. Diabetic retinopathy. N Engl J Med 2004;
350: 48–
58.
62 Cunha-Vaz J, Bernardes R. Nonproliferative retinopathy in
dia-
betes type 2. Initial stages and characterization of
phenotypes.
Prog Retin Eye Res 2005; 24: 355–77.63 Poulaki V, Qin
W, Joussen AM et al. Acute intensive insulin
therapy exacerbates diabetic blood–retinal barrier breakdown
via hypoxia-inducible factor-1alpha and VEGF. J Clin
Invest
2002; 109: 805–15.
64 Oliver SJ, Cheng TP, Banquerigo ML, Brahn E. Suppression
of collagen-induced arthritis by an angiogenesis inhibitor,
AGM-
1470, in combination with cyclosporin: Reduction of vascular
endothelial growth factor (VEGF). Cell Immunol 1995;
166:
196–206.
65 Storgard CM, Stupack DG, Jonczyk A, Goodman SL, Fox RI,
Cheresh DA. Decreased angiogenesis and arthritic disease in
rabbits treated with an alphavbeta3 antagonist. J Clin
Invest
1999; 103: 47–54.
66 Distler JH, Wenger RH, Gassmann M et al.
Physiologic
responses to hypoxia and implications for hypoxia-inducible
factors in the pathogenesis of rheumatoid arthritis.
Arthritis
Rheum 2004; 50: 10–23.
67 Hollander AP, Corke KP, Freemont AJ, Lewis CE. Expressionof
hypoxia-inducible factor 1alpha by macrophages in the rheu-
matoid synovium: Implications for targeting of therapeutic
genes to the inflamed joint. Arthritis Rheum 2001;
44: 1540–
44.
68 Makino Y, Nakamura H, Ikeda E et al. Hypoxia-inducible
factor
regulates survival of antigen receptor-driven T cells. J
Immunol
2003; 171: 6534–40.