Embed Size (px)
Citation preview

� cell transdifferentiation does not contribute topreneoplastic/metaplastic ductal lesions of thepancreas by genetic lineage tracing in vivoOliver Strobel*, Yuval Dor†, Amy Stirman*, Amanda Trainor*, Carlos Fernandez-del Castillo*, Andrew L. Warshaw*,and Sarah P. Thayer*‡
*Department of Surgery, Massachusetts General Hospital and Harvard Medical School, Boston, MA 02114; and †Department of Cellular Biochemistryand Human Genetics, The Hebrew University–Hadassah Medical School, Jerusalem 91120, Israel
Edited by Kathryn V. Anderson, Sloan–Kettering Institute, New York, NY, and approved January 11, 2007 (received for review July 25, 2006)
Inflammatory injury to the pancreas results in regeneration ofnormal tissue and formation of metaplastic lesions of a ductalphenotype. These metaplastic ductal lesions (MDL) are calledtubular complexes (TC), mucinous metaplasia, or pancreatic intra-epithelial neoplasia. Because they are regularly found in chronicpancreatitis and pancreatic cancer, their formation is thought torepresent a step in inflammation-mediated carcinogenesis. Despitethese lesions’ ductal character, their origin is controversial. All knownpancreatic cell lineages have been suggested as the origin. In vitrostudies suggest that differentiated cells in the pancreas remain highlyplastic and can transdifferentiate as a mechanism of regeneration andmetaplasia. In vivo studies suggest that islets, specifically � cells, maybe the cell of origin. However, in vitro studies are subject to ductal cellcontamination, and previous in vivo studies interpret static datarather than direct evidence. Using genetic lineage tracing in vivo, weinvestigate whether transdifferentiation of � cells contributes toregeneration or metaplasia in pancreatitis. RIP-CreER;Z/AP mice wereused to heritably tag � cells in the adult pancreas. Injury by ceruleinpancreatitis resulted in regeneration of normal tissue and metaplasiawith formation of two distinct types of TC and mucinous lesions.Lineage tracing revealed that none of these MDL are of � cell origin;nor do � cells contribute to regeneration of normal acinar and ductaltissue, which indicates that the plasticity of differentiated pancreaticislet cells, suggested by earlier static and in vitro studies, plays no rolein regeneration, metaplasia, and carcinogenesis in vivo.
metaplasia � pancreatitis � pancreatic intraepithelial neoplasia
T issue injury can result in regeneration of normal tissue and inmetaplasia. Metaplasia is often seen in response to chronic
injury and can occur by selective cellular proliferation or death orby transdifferentiation. Cell lineages in the pancreas include exo-crine (acinar and ductal) and endocrine cells. Inflammation of thepancreas results in the formation of metaplastic lesions of a ductalphenotype (MDL) that are consistently found in chronic pancre-atitis (CP) and specimens of pancreatic cancer. Therefore, this‘‘ductal’’ metaplasia is thought to represent a condition withincreased risk of neoplasia. In the literature, two definitions havebeen used to describe MDL in the pancreas: tubular complexes(TC) and mucinous metaplasia or pancreatic intraepithelial neo-plasia (PanIN) (1, 2). TC, defined as cylindrical tubes with a widelumen lined by a monolayer of flat duct-like cells (3–5), are foundin pancreatic development, regeneration, in CP, and in cancer(5–8). In some studies, TC exhibited a high cell turnover and werethought to have regenerative potential, including islet regeneration(5, 9). A progression of TC to neoplasia has been suggested inrodent models of chemical carcinogenesis (1, 10, 11) and transgenicmouse models (12). Misexpression of mucins in pancreatic cancerhas shifted the focus to mucinous metaplastic lesions (MML), whichare classified in the PanIN system according to their grade of atypiaand risk of neoplasia (2, 13).
Despite the ductal character of TC and MML, their cellularorigin remains controversial; ductal (14), acinar (12, 15), islet (16)
cells, and all lineages (1) have been proposed as the cell of originof MDL. Transdifferentiation of islet cells, specifically � cells, isproposed as a likely source of metaplasia/neoplasia in several in vitroand in vivo studies (17). In vitro, isolated pancreatic islets have beenreported to transform to duct-like structures expressing ductalmarkers and to acquire genetic alterations typical of pancreaticcancer, such as K-ras mutations and p16 deletion (18–20). How-ever, in vitro studies do not necessarily mirror in vivo events.Furthermore, in vitro studies are subject to cell contamination: theobservation of ductal cells in cultured isolated islets/islet cells couldbe a result of proliferation of ductal cells contaminating thepreparation. The genetic alterations observed in vitro may conse-quently be artifacts of long-term culture. In vivo, the location ofMDL within histologic preparations of islets has been used tosupport their islet cell origin. Intrainsular metaplastic ductal lesionshave been described in specimens of pancreatic cancer (21), ingenetically engineered mice that overexpress EGF-like growthfactors in � cells (22), and in a hamster model of chemicalcarcinogenesis (17). Clearly, the colocalization of MDL within isletsobserved by snapshot analysis of morphology or the momentaryexpression of lineage markers can be suggestive, but remain purelydescriptive and do not justify conclusions about dynamic processes,including transdifferentiation and the cellular origin of ductallesions. Furthermore, functional methodologies, in which selectivechemical or genetic depletion of � cells inhibited, while stimulationof � cell neogenesis promoted, the development of metaplasia andcancer, led investigators (17, 23–26) to infer an ‘‘unequivocal roleof � cells in transdifferentiation and, thus the carcinogenesisprocess’’ (17). Although these functional studies show that thepresence of � cells may modify the formation of ductal lesions, theydo not allow conclusions about their role as the cell of origin.
This question can be answered only by a method that allows thefate of a specific cell type and its progeny to be traced in adult tissue.With advances in transgenic technology, it has become possible togenetically label specific cell lineages and to trace their fate in vitroand in vivo. Such genetic lineage tracing is not subject to theabove-mentioned weaknesses of previous studies and has recently
Author contributions: O.S., Y.D., and S.P.T. designed research; O.S., A.S., and A.T. per-formed research; Y.D. and S.P.T. contributed new reagents/analytic tools; O.S., Y.D.,C.F.-d.C., A.L.W., and S.P.T. analyzed data; and O.S. and S.P.T. wrote the paper.
The authors declare no conflict of interest.
This article is a PNAS direct submission.
Freely available online through the PNAS open access option.
Abbreviations: CP, chronic pancreatitis; HPAP, human placental alkaline phosphatase;MDL, metaplastic ductal lesions; MML, mucinous metaplastic lesions; PanIN, pancreaticintraepithelial neoplasia; PAS, periodic acid/Schiff reagent; TC, tubular complexes.
‡To whom correspondence should be addressed at: Department of Surgery, MassachusettsGeneral Hospital, 15 Parkman Street, WACC 460, Boston, MA 02114. E-mail:[email protected].
This article contains supporting information online at www.pnas.org/cgi/content/full/0605248104/DC1.
© 2007 by The National Academy of Sciences of the USA
www.pnas.org�cgi�doi�10.1073�pnas.0605248104 PNAS � March 13, 2007 � vol. 104 � no. 11 � 4419–4424
CELL
BIO
LOG
Y
Dow
nloa
ded
by g
uest
on
Mar
ch 4
, 202
1

been used to show that � cells are formed by self-duplication in thehealthy adult pancreas (27). To date, there are no lineage tracingstudies on the cellular origin of metaplastic lesions or regenerationof the injured pancreas.
Here, we use genetic lineage tracing in a mouse model ofpancreatitis to investigate whether transdifferentiation between �cells and exocrine lineages contributes to regeneration or to theformation of MDL. RIP-CreER mice (27), in which � cells arelabeled with a tamoxifen-inducible Cre/lox system, were crossed tothe reporter strain Z/AP (28), in which Cre-mediated recombina-tion results in constitutive and heritable expression of humanplacental alkaline phosphatase (HPAP). In bigenic RIP-CreER;Z/AP mice, tamoxifen exposure labels adult � cells andtheir progeny with HPAP expression. We induced acute andchronic pancreatitis in tamoxifen-injected RIP-CreER;Z/AP miceand found that the resulting MDL were not HPAP-tagged and thusnot of � cell origin. Moreover, HPAP expression remained specificfor � cells, and the fraction of tagged � cells remained stable inpancreatitis, indicating that transdifferentiation between � cellsand exocrine lineages does not contribute to regeneration afterinflammation.
ResultsTubular Formations Are a Heterogeneous Group of Lesions. Differentauthors use the terms ‘‘tubular formations’’ and ‘‘tubular com-plexes’’ in different models of both acute and chronic pancreatitisor pancreatic cancer to designate a heterogeneous group of similarbut distinct lesions.
We observed three distinct types of lesions, two of which areconsistent with the definition of TC as cylindrical tubes with a widelumen lined by a monolayer of flat, duct-like cells (3–5). The thirdtype is consistent with mucinous metaplasia. To analyze theselesions separately, we characterized them as follows.
1. TC lined by a few large, flat cells. Lesions with a wide, emptylumen lined by a few (typically 4–5) flat wide cells (Fig. 1A)whose sparse cytoplasm exhibits staining characteristics similarto acinar cells. ‘‘Intermediate’’ figures can be observed betweenacini with slightly widened lumen and such TC, leading to thesuggestion that TC are derived from acinar cells through acinaratrophy or acinar-to-ductal metaplasia (4, 8, 29).
2. TC lined by many small cells. Lesions with an empty lumen linedby a variable number of flat small cells (Fig. 1B). Because thecells are small, larger diameters result in higher cell numbers inthe epithelial lining. These ‘‘duct-like’’ TC are seen more oftenwith increasing acinar loss, often show a complex arrangementwith branching, and can form fields composed almost entirely ofTC (Fig. 1B). Similar observations may have led to the sugges-tion that these lesions represent proliferating ductules. Frequent
expression of endocrine markers in fields of TC may suggesteither that TC are derived from islets or that they may representa pathway for islet regeneration (9).
3. MML. The epithelial cells of MML are not flat, but vary inheight according to the extent of mucin expression. Their lumenis variable in diameter and can contain secreted mucins. Somelesions exhibit abundant supranuclear mucin and flat, basallylocated nuclei oriented perpendicularly to the basement mem-brane (Fig. 1C), features characteristic of early PanIN (2, 13).Their mucin is often periodic acid/Schiff’s reagent (PAS)- andAlcian blue-positive. Although these lesions do not fulfill thecriteria of flat cells, some authors name them TC; others use theterms metaplastic ducts, metaplastic ductal lesions, or PanIN(12, 22, 30, 31).
Distinguishing among these lesions may enable us to betterevaluate their cells of origin.
MDL Are Not of � Cell Origin. Because � cells were heritably taggedbefore induction of pancreatitis, lesions derived from tagged � cellsshould express HPAP even if they have undergone completetransdifferentiation to another cell type, such as ductal cells.However, not all � cells are labeled, and the likelihood of capturingthe event of a � cell-derived lesion is a function of the efficiency ofthe tagging system. The applied system reproducibly resulted inHPAP expression in 55% of � cells in controls. Tagging has noadverse effects on the pancreas, including � cell function (27).Assuming that it also has no effect on formation of MDL, a taggingefficiency of 50% results in a likelihood of at least 50% that a �cell-derived lesion is HPAP�. The fraction of tagged � cells for eachanimal was used to calculate the expected number of HPAP�
lesions. This hypothetical number was then compared with thenumber of tagged lesions actually observed.
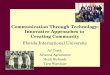
Comparison of expected vs. observed tagged events suggests thatnone of the observed types of MDL are of � cell origin. A total of245 TC with a few large cells were found (Fig. 2 A–C). If ‘‘large-cellTC’’ were derived from � cells, �125.5 HPAP� events would beexpected. In fact, only two (0.8%) large-cell TC were HPAP�.Similarly, 2,231 TC with small cells were identified (Fig. 2 D–F).Hypothesizing � cell origin, one would expect �1,115.5 to beHPAP�. However, only four (0.2%) ‘‘small-cell TC’’ were HPAP�;the vast majority again were not labeled (Fig. 2 D and E). Inde-pendent of the duration of injury (Fig. 2 C and F), neither type ofTC was derived from � cells.
MML were identified first by PAS staining (Fig. 3 A and B).Because PAS� mucins can be expressed at a low level in the normalpancreas, whereas Alcian blue� mucins are found only in meta-plastic lesions, we confirmed metaplastic transformation by serialAlcian blue stains (Fig. 3 C and D). In HPAP/PAS double stains,397 MML were identified. Given the tagging efficiency, one wouldexpect �208.4 MML with HPAP expression. However, only two(0.5%) of these lesions were HPAP� (Fig. 3 A and B). Of all PAS�
lesions, 223 lesions were identified in serial sections and were Alcianblue� (Fig. 3 C and D). Of these, 117.1 would be expected to beHPAP� if they were of � cell origin. However, only the same twotagged events were found in serial sections, indicating that MMLare not of � cell origin.
For each lesion, binomial testing was used to determine thelikelihood that the observed distribution of events could occur bychance if the lesions were derived from � cells. Given the numbersfor expected and observed tagged events, the likelihood that thisdistribution was observed by chance, and that the observed lesionswere derived from the nontagged pool of � cells, is extremely low(binomial P � 0.000001) for all three types of lesions.
To exclude the possibility of false-negative results from epige-netic inactivation of the Z/AP reporter during inflammation andmetaplastic transformation, specimens of additional animals withCP for 6 wk (6wCP) were stained for LacZ activity. HPAP� cells
Fig. 1. Pancreatitis results in formation of several types of metaplasticlesions. (A) TC with few large cells. (B) TC with many small cells. (C) MMLcomposed of cells with abundant supranuclear mucin (arrowheads), which isfrequently Alcian blue� (turquoise). (Scale bar, 100 �m.)
4420 � www.pnas.org�cgi�doi�10.1073�pnas.0605248104 Strobel et al.
Dow
nloa
ded
by g
uest
on
Mar
ch 4
, 202
1

with an intact reporter are expected to be LacZ� (28). Both TC andMML were indeed LacZ�, demonstrating a functional reporter inthese lesions (Fig. 4 A and B).
In single animals with CP, HPAP expression was identified at avery low frequency (0.0–0.4%) in morphologically normal acinarcells (Fig. 4 C and D) and in a small number of metaplastic lesions(Figs. 2 and 3 and Fig. 4 E–G). HPAP/insulin double stainingrevealed that these events did not reflect isolated � cells, but HPAPexpression in non-insulin-producing cells (Fig. 4 C and D).
We cannot exclude the possibility that these findings representextremely rare events of true � cell transdifferentiation. However,one other hypothesis is that they represent false-positive resultsbecause of aberrant alkaline phosphatase (ALP) activity in non-�
cells. To test this possibility, we performed several control exper-iments. First, to determine whether these tagged cells could resultfrom aberrant expression of endogenous ALP in response toinflammation, nontransgenic littermates were subjected to chronicinflammation. No ALP activity was identified in nontransgeniclittermates (data not shown), excluding expression of endogenousALP as a source of false-positive results. Second, to determinewhether inherent leakiness of the transgenic system could result infalse positives, we analyzed bigenic mice injected with tamoxifenbut not subjected to pancreatitis. Absent HPAP activity in non-�cells in these healthy controls excluded false-positive HPAP ex-pression due to leakiness (data not shown). Third, to assess whetherinflammation may result in aberrant HPAP transgene activation,
Fig. 2. Analysis of expected vs. observed tagged events indicates that TC with a few large cells (A–C) and TC with many small cells (D–F) are not of � cell origin. Openbars represent total number of observed lesions. Gray bars indicate expected hypothesized number of HPAP� events. Black bars represent the number of observedHPAP� lesions. (A and D) For both types of TC, the number of observed events is far lower than the number of expected events. The likelihood that this distributionoccurred by chance is extremely low (*, binomial P � 0.000001). (B and E) HPAP staining shows strong � cell tagging (blue) within islets and complete absence of taggingin TC (arrowheads) as well as acinar cells, stromal cells, and ducts (arrows). (C and F) These results are independent of the duration of pancreatitis. AP, acute pancreatitis.3wCP and 6wCP, 3-wk and 6-wk chronic pancreatitis, respectively. (Scale bar, 100 �m.)
Fig. 3. Analysis of expected vs. observed tagged events indicates MML are not of � cell origin. (A and B) Lesions observed in HPAP/PAS double stains (magenta, mucin).(C and D) Lesions additionally identified in serial Alcian blue stains (turquoise, mucin). (A and C) Colored bars show the number of lesions observed. Gray bars showthe expected/hypothesized number of HPAP� events. Black bars represent the number of observed HPAP� lesions. The number of observed events is far lower thanthe number of expected events. The likelihood that this distribution occurred by chance is extremely low (*, binomial P � 0.000001). (B) HPAP/PAS stains show strong� cell tagging (blue) within islets and complete absence of labeling in MML. (C and D) The majority of MML observed in A and B also stain with Alcian blue, supportingmetaplasia. (Scale bar, 100 �m.)
Strobel et al. PNAS � March 13, 2007 � vol. 104 � no. 11 � 4421
CELL
BIO
LOG
Y
Dow
nloa
ded
by g
uest
on
Mar
ch 4
, 202
1

we analyzed bigenic mice with CP that were not tamoxifen-injected.In these animals, aberrant HPAP expression was infrequentlyobserved in acinar cells (1–2 acini per cut) (Fig. 4H). In tamoxifen-injected animals with CP the events of HPAP� TC and mucinouslesions had a low frequency (0.2–0.8%), similar to HPAP expres-sion in acini (0.0–0.4%). Together, these data suggest that taggedlesions may indeed represent false-positive observations rather thanvery infrequent events of true � cell transdifferentiation.
Thus, based on direct lineage tracing in vivo, � cell transdiffer-entiation does not contribute to the formation of MDL observed inchemically induced pancreatitis.
Transdifferentiation Between � Cells and Exocrine Cells Does NotContribute to Regeneration. In previous in vitro studies, transdiffer-entiation of � cells has been discussed not only as the origin of MDLbut also as a source of regeneration of normal exocrine andendocrine tissue (9, 17, 32–34). However, the role of transdiffer-entiation in vivo remains unclear. Thus, we used the same lineage-tagging strategy to determine whether transdifferentiation of � cellswas important in the in vivo regenerative response after chemicalpancreatitis.
Acute cerulein pancreatitis induces severe injury with loss of�10% of acinar cells and almost complete regeneration within 96 h(35). In the chronic model, repetitive injury over a period of 3–6 wkshould result in replacement of the majority of exocrine tissue. Thishypothesis is supported by the extensive increase in Ki-67- andBrdU-positive nuclei observed in acinar, centroacinar and ductalcells in CP vs. controls [supporting information (SI) Fig. 6 A and B].In controls, islet cells exhibited a relatively low cell turnover, withKi-67 expression or BrdU incorporation (72 h exposure) in �2% of
cells (SI Fig. 6A). Surprisingly, this low proliferation rate in islets isnot enhanced in CP, in contrast to the markedly increased cellturnover observed in the exocrine pancreas (SI Fig. 6B).
The low rate of cell turnover in islets and the high rate in theexocrine pancreas alone suggest that endocrine-to-exocrine trans-differentiation cannot play a major role in exocrine regeneration.
As direct evidence by lineage tracing, � cell transdifferentiationto exocrine cells occurring during CP would be detected as HPAP�
acinar or ductal cells. HPAP was never observed in normalpancreatic ducts or in intra-or juxta-insular ducts (SI Fig. 7),indicating that � cells did not contribute to ductal regeneration. Asexplained in detail above (Fig. 2), HPAP expression was observedonly very rarely (0.0–0.4%) in acinar cells in CP, most likely due toinflammation-mediated HPAP expression (Fig. 4 C–H). Even ifthese events represent true � cell transdifferentiation, this mecha-nism would be insignificant and insufficient to account for exocrineregeneration.
Conversely, transdifferentiation of acinar and ductal cells or TChas been proposed as a mechanism of � cell renewal in severalstudies (9, 32, 33, 36, 37). A recent lineage tracing experimentreveals that � cells can be generated from acinar cells in vitro (38).In contrast, it has been shown by lineage tracing in vivo that in thenormal adult pancreas and after pancreatectomy, preexisting � cellsrather than other cells are the source of new � cells (27). Thus, wewanted to determine whether transdifferentiation may play a rolein � cell renewal in the setting of inflammatory injury. New � cellsgenerated during the course of pancreatitis are labeled only if theyare progeny of labeled � cells but not if they are derived from anonlabeled source, such as acinar or ductal cells or TC. Replen-ishment of preexisting islets with new � cells from a nonlabeled
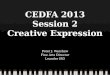
Fig. 5. Transdifferentiation between exocrine cellsand � cells does not contribute to regeneration. (A)Stable percentages of islets (black bars) and endocrineclusters (gray bars) with tagged � cells in controls andpancreatitis. (B and C) HPAP staining (blue) reveals thattagging remains specific for � cells and stable in re-sponse to inflammation. Ducts and acinar tissue remainHPAP�. (D) Tagging of � cells remains stable in pancre-atitis. (E and F) HPAP (blue)/insulin (brown) doublestaining demonstrates that tagging remains specific for� cells. (Scale bars, 100 �m.)
Fig. 4. Control experiments. (A and B) Functionalreporter system. MDL (arrowheads) are LacZ� in X-galstains; � cells, where Cre activity removed LacZ, areLacZ� (A). (C–H) Observed tagged events may resultfrom inflammation-mediated transgene activation.Comparison of HPAP (C) and HPAP/insulin doublestains (D) reveals single events of tagged non-� cellswithin the exocrine pancreas. (E–G) Examples of thevery rare occurrence of HPAP� MDL (arrowheads). (E)TC with many small cells, (F) TC with few large cells, and(G) MML. Rare occurrences of HPAP� acinar cells arealso identified (arrow in F). (H) HPAP expression in anacinus (arrow and insert) and absent HPAP expressionin an islet (*) in non-tamoxifen-injected animals withCP identify inflammation-mediated HPAP expressionas a possible mechanism for false-positive results.
4422 � www.pnas.org�cgi�doi�10.1073�pnas.0605248104 Strobel et al.
Dow
nloa
ded
by g
uest
on
Mar
ch 4
, 202
1

source would yield a decreased percentage of tagged � cells in islets.Maintenance of the � cell population by self-duplication wouldresult in stable tagging.
Both frequency and distribution of labeled � cells remainedstable during pancreatitis (Fig. 5). Tagging remained stable even insmall clusters of endocrine cells, which are thought by some torepresent newly formed endocrine tissue caught during coalescence(Fig. 5A) (39–41). Thus, islet neogenesis and replenishment ofpreexisting islets by transdifferentiation of an unlabeled source,including acinar and ductal cells as well as TC, was not observed (SIDiscussion).
These results indicate that transdifferentiation of � cells does notplay a role in exocrine regeneration in pancreatitis and that � cellrenewal in the inflamed pancreas appears to occur by self-duplication rather than by transdifferentiation.
DiscussionThe pancreas is composed of a variety of cell types. Epithelial celllineages include acinar and ductal cells as well as endocrine cells, themajority of which are � cells. Injury to the adult pancreas results inregeneration of normal epithelium and in a metaplasia of ductalphenotype. Results from various in vitro studies and in vivo modelsof pancreatic injury suggest that transdifferentiation among thedifferent cell lineages may play a role in both regeneration andmetaplasia. Transdifferentiation of � cells has been discussed as amechanism of exocrine regeneration, metaplasia and cancer for-mation, and conversely, transdifferentiation of exocrine cells hasbeen implicated in � cell regeneration. Recently, it has been shownby lineage tracing that in the normal adult pancreas and afterpancreatectomy, new � cells are generated by self-duplication ofpreexisting � cells (27). However, all studies on the role of � cellsin metaplasia published to date are based on interpretation of thestatic expression of lineage markers and lack direct evidence bylineage tracing. Our first objective, therefore, was to investigate bylineage tracing in the adult pancreas in vivo whether � cells are theorigin of MDL or of normal exocrine regeneration. Our secondobjective was to elucidate whether in the setting of pancreatitis �cells themselves may be regenerated by transdifferentiation or, asdemonstrated for the normal pancreas, by self-duplication. Inhuman disease, the observation of the same MDL and K-rasmutations in chronic pancreatitis and in cancer has led to theassumption that ductal metaplasia occurs in inflammation and is anearly step in cancer formation. The cerulein model of pancreatitiswas chosen because it histologically mirrors the MDL found inhuman disease and results in the different MDL with sufficientfrequency to draw statistically solid conclusions from lineage trac-ing results. The cerulein model has been frequently used to studythe extent and mechanisms of regeneration after pancreatitis (7, 35,42, 43), including a recent study to reveal the recapitulation ofdevelopmental programs in the adult regenerative response (44).Using Cre-loxP-based genetic tracing, we show that � cells contrib-ute neither to exocrine regeneration nor to formation of metaplasiain pancreatitis. Further, we show that severe exocrine injury doesnot result in enhanced endocrine cell turnover, and we find noevidence of � cell renewal through transdifferentiation of otherlineages in pancreatitis.
The cerulein model induces a variety of MDL that can be dividedinto two major groups: TC and MML. Whereas TC were originallydefined as cylindrical tubes with an often dilated lumen lined by amonolayer of flattened duct-like cells (3, 4), for lack of a stringentclassification comprising all metaplastic lesions, the term has alsobeen used for other lesions, including mucinous ones. This lack ofclassification may explain the controversial results regarding theirorigin and significance. In contrast, mucinous metaplasia has beenused specifically for mucinous lesions that are more stringentlydefined in the PanIN classification for the human pancreas (2) andin mouse models of pancreatic disease (13). However, this nomen-clature does not encompass all early metaplastic changes seen in
inflammation. To do justice to these lesions and their possibleorigin, we distinguish two distinct types of TC and MML.
All these lesions are distributed throughout the exocrine pan-creas, as typically observed in human disease. Intra- and juxta-insular ducts were never identified as tagged and are not a major siteof metaplasia. Previous studies reporting formation of metaplasticlesions predominantly in or beside islets used a potent carcinogenor transgenic misexpression of growth factors targeted to islets toinduce these lesions (17, 22). In this study, metaplastic lesionsformed in the setting of CP through repetitive inflammatory injurymay more closely reflect the early events of human disease. Directlineage tracing excludes � cells as a significant source of metaplasticlesions formed during pancreatitis. The possibility that lesions werenot tagged because by chance they were all derived from nontagged� cells was excluded by binomial testing based on the assumptionthat a given lesion originated from a single cell. Although suchclonal expansion is a common mechanism later in cancer formation,it is unlikely to play a role in the formation of early metaplasticlesions. However, if a lesion was formed by nonclonal expansionthrough transdifferentiation of several � cells, then the likelihoodof detecting HPAP� cells within these lesions would be even higher.
Whereas the significance of TC is controversial, mucinous meta-plasia is thought to represent an early event in the formation ofcancer from normal pancreatic epithelium (2). The MML observedin the current model express both PAS- and Alcian blue-positivemucins, mirroring the metaplastic and neoplastic mucin expressionseen in human and mouse PanIN. However, progression to high-grade atypia or invasive cancer was not observed. Thus, our studyshows that � cells are not the cellular origin of lesions thought to beearly cancer precursors but does not demonstrate this for pancreaticcancer per se.
Pour and colleagues (23–25, 45) have shown that metaplasia/neoplasia in the pancreas appear to depend on the presence of �cells. Although our results show � cells do not directly contributeas cells of origin, they may contribute to metaplasia and carcino-genesis by indirect mechanisms such as altered signaling. Further,the present study does not formally exclude the possibility thattransdifferentiation of an islet cell lineage other than � cells maycontribute to metaplasia. However, the observed low proliferationin islets and the distribution of MML away from islets argue againstnontagged endocrine cells as progenitors.
The second question addressed here is the role of transdiffer-entiation in regeneration of normal tissue. The cerulein modelresults in considerable exocrine damage and regeneration (35).Transdifferentiation of � cells, which would result in labeling ofother lineages, was not seen in normal ductal cells and only veryinfrequently in acinar cells. Although we cannot exclude veryinfrequent events of true � cell transdifferentiation, our controlexperiments suggest that this rare expression of HPAP is morelikely the result of inflammation-mediated transgene activation.Thus, our results reveal that transdifferentiation of � cells does notcontribute to exocrine regeneration in the cerulein model.
Furthermore, the frequency and distribution of labeled � cellsremained stable in the pancreatitis groups compared with baselinecontrols. Islet neogenesis by transdifferentiation of an unlabeledsource, which would include acinar and ductal cells as well as TC,was not observed. Surprisingly, we did not see a significant increasein endocrine proliferative activity in response to pancreatitis. Thefrequency of proliferating cells observed in pancreatitis is notsignificantly different from that seen in controls; both are consistentwith the low (2–3%) � cell turnover in rats (46) and a low (4–5%)BrdU incorporation of � cells in mice found at 1 wk (27). Althoughwe did not see increased islet cell turnover in pancreatitis, extrap-olation of this baseline turnover suggests that enough new � cellswere generated during the chase period of up to 6 wk to detecttransdifferentiation from unlabeled sources as the predominantsource of new � cells. The stable percentages of tagged endocrineclusters and islets provide evidence against islet neogenesis from
Strobel et al. PNAS � March 13, 2007 � vol. 104 � no. 11 � 4423
CELL
BIO
LOG
Y
Dow
nloa
ded
by g
uest
on
Mar
ch 4
, 202
1

exocrine lineages and suggest that in the inflamed pancreas � cellsare renewed by self-duplication, as in the normal pancreas (27).However, the model may not be sensitive enough to exclude alow contribution of acinar-to-� cell transdifferentiation (38) (SIDiscussion).
In summary, we observed three different types of MDL, includ-ing mucinous metaplasia. In vivo lineage tracing with stringentcontrol experiments revealed that transdifferentiation of � cellsdoes not play a role in the formation of these metaplastic lesions inpancreatitis. Moreover, transdifferentiation of � cells does notcontribute to exocrine regeneration, and we found no evidence of� cell renewal from exocrine lineages. These results suggest that theplasticity of differentiated cells, which has been suggested based onin vitro studies, does not necessarily play a role in pancreaticregeneration, metaplasia and carcinogenesis in vivo. To our knowl-edge, no other studies have used genetic lineage tracing to inves-tigate transdifferentiation and the formation of metaplastic lesionsin adult tissue in vivo. For the pancreas, similar studies need to beperformed for acinar and ductal lineages to further elucidate theprocess of metaplasia and hopefully one day define the cell of originof pancreatic cancer.
Materials and MethodsIn Vivo Lineage Tracing. RIP-CreER;Z/AP mice were genotyped byPCR as described in ref. 30. Tamoxifen (Sigma–Aldrich, St. Louis,MO) was injected subcutaneously every second day in five doses of4 mg as described in ref. 27. Pancreatitis was induced 2.5 wk afterthe last tamoxifen injection.
Experimental Pancreatitis. All experiments were approved by theMassachusetts General Hospital Subcommittee on Research An-imal Care. Pancreatitis was induced by the cerulein model (35, 47,48). Acute pancreatitis (AP) was induced by 6 hourly i.p. injectionsof 50 �g/kg cerulein (Sigma–Aldrich) after a fasting period of 12 h(AP, n � 6). CP was induced by three series of injections per weekfor 3 (3wCP, n � 4) or 6 wk (6wCP, n � 7). Bigenic animals withoutpancreatitis (n � 7) served as healthy controls. Further controlswere bigenic animals with 6wCP but without tamoxifen exposure.Pancreata were harvested 48 (AP) or 72 (CP) h after the lastinjection. Specimens were fixed in 4% paraformaldehyde at 4°C for5 h, dehydrated, and embedded in paraffin.
Histology and Immunohistochemistry. Expression of HPAP andLacZ was identified as described (27, 28). Mucin was identified byPAS and Alcian blue (pH 2.8) staining, using standard protocols.Expression of insulin, HPAP, Ki-67, and BrdU incorporation wereidentified by immunohistochemistry. Antigen retrieval was per-formed at pH 8 for HPAP and at pH 6 for insulin, Ki-67 and BrdU(BioGenex, San Ramon, CA). Primary antibodies used were:insulin (1:100; Santa Cruz Biochemicals, Santa Cruz, CA), HPAP(1:400; Santa Cruz Biochemicals), Ki-67 (1:25; Dako, Carpinteria,CA), and BrdU (1:100; Abcam, Cambridge, MA). Biotinylatedsecondary antibodies were applied at a dilution of 1:1,000. Expres-sion was visualized with diaminobenzidine (Zymed Laboratories,South San Francisco, CA). Slides were counterstained with hema-toxylin or nuclear fast red.
Quantitative Analysis. Percentage of tagged cells. For each animal, thefraction of tagged islets and small clusters of �15 � cells wasdetermined by analyzing the entirety of doubly or serially HPAP/insulin-stained sections through the entire pancreas. Tagging of �cells was quantified by using serial HPAP and insulin stains bycounting individual cells in three randomly selected islets peranimal.Morphologic analysis: MDL. In the cerulein model, TC are distributedthroughout the pancreas. Analysis (quantification and tagging) ofTC was performed by counting events in three 100� high-powerfield per cut in three cuts per animal. MML were observed withmuch lower frequency, only in CP, and were analyzed in the entiretyof three HPAP/PAS double stains and serial Alcian blue stains peranimal.Statistical analysis. Graphs represent absolute numbers (for lesions)or the mean � SEM (for tagging). The likelihood that the differ-ences between expected and actually observed numbers of taggedlesions were due to chance was evaluated by binomial testing.
We thank D. Melton for the RIP-CreER and Z/AP mouse strains and D.Dorer for help with binomial calculations. This work was supported by theGerman Research Foundation and the Surgery Foundation HeidelbergLautenschlager Scholarship (O.S.), the Juvenile Diabetes Research Foun-dation (2-2005-171), the Israel Science Foundation, the National Institutesof Health Beta Cell Biology Consortium, and the Barbara S. GoodmanCareer Development Award from the Israel Cancer Research Fund (Y.D.),and the National Insitutes of Health, the American College of SurgeonsClowes Award, and the Lustgarten Foundation (S.P.T.).
1. Bockman DE, Guo J, Buchler P, Muller MW, Bergmann F, Friess H (2003) Lab Invest 83:853–859.2. Hruban RH, Adsay NV, Albores-Saavedra J, Compton C, Garrett ES, Goodman SN, Kern SE,
Klimstra DS, Kloppel G, Longnecker DS, et al. (2001) Am J Surg Pathol 25:579–586.3. Iovanna JL (1996) Int J Pancreatol 20:77–84.4. Willemer S, Adler G (1989) Dig Dis Sci 34:46–55.5. Lechene dlP, Iovanna J, Odaira C, Choux R, Sarles H, Berger Z (1991) Pancreas 6:298–306.6. Hisaoka M, Haratake J, Hashimoto H (1993) Differentiation 53:163–172.7. Elsasser HP, Adler G, Kern HF (1986) Pancreas 1:421–429.8. Bockman DE, Boydston WR, Anderson MC (1982) Am J Surg 144:243–249.9. Wang GS, Rosenberg L, Scott FW (2005) Lab Invest 85:675–688.
10. Longnecker DS, Curphey TJ, Kuhlmann ET, Schaeffer BK (1983) J Natl Cancer Inst 71:1327–1336.11. Jimenez RE, Z’graggen K, Hartwig W, Graeme-Cook F, Warshaw AL, Fernandez-del Castillo
C (1999) Am J Pathol 154:1223–1229.12. Wagner M, Luhrs H, Kloppel G, Adler G, Schmid RM (1998) Gastroenterology 115:1254–1262.13. Hruban RH, Adsay NV, Albores-Saavedra J, Anver MR, Biankin AV, Boivin GP, Furth EE,
Furukawa T, Klein A, Klimstra DS, et al. (2006) Cancer Res 66:95–106.14. Bordalo O, Goncalves D, Noronha M, Cristina ML, Salgadinho A, Dreiling DA (1977) Am J
Gastroenterol 68:278–285.15. Tokoro T, Tezel E, Nagasaka T, Kaneko T, Nakao A (2003) Pancreatology 3:487–496.16. Pour PM, Schmied BM (1999) Int J Pancreatol 25:181–193.17. Pour PM, Pandey KK, Batra SK (2003) Mol Cancer 2:13.18. Jamal AM, Lipsett M, Sladek R, Laganiere S, Hanley S, Rosenberg L (2005) Cell Death Differ
12:702–712.19. Schmied B, Liu G, Moyer MP, Hernberg IS, Sanger W, Batra S, Pour PM (1999) Carcinogenesis
20:317–324.20. Muscarella P, Knobloch TJ, Ulrich AB, Casto BC, Moniaux N, Wittel UA, Melvin WS, Pour
PM, Song H, Gold B, et al. (2001) Gene 278:235–243.21. Schmied BM, Ulrich AB, Matsuzaki H, Li C, Friess H, Bochler MW, Andron-Sandberg A,
Adrian TE, Pour PM (2000) Int J Pancreatol 28:187–197.22. Means AL, Ray KC, Singh AB, Washington MK, Whitehead RH, Harris RC, Jr, Wright CV,
Coffey RJ, Jr, Leach SD (2003) Gastroenterology 124: 1020–1036.23. Pour PM, Kazakoff K, Carlson K (1990) Cancer Res 50:1634–1639.24. Bell RH, Jr, Pour PM (1987) Cancer Lett 34:221–230.25. Pour PM, Kazakoff K (1996) Am J Pathol 149:1017–1025.
26. Pour PM (1997) Front Biosci 2:D271–D282.27. Dor Y, Brown J, Martinez OI, Melton DA (2004) Nature 429:41–46.28. Lobe CG, Koop KE, Kreppner W, Lomeli H, Gertsenstein M, Nagy A (1999) Dev Biol 208:281–292.29. Iovanna JL, Odaira C, Berger Z, Sarles H (1988) Pancreas 3:433–438.30. Stanger BZ, Stiles B, Lauwers GY, Bardeesy N, Mendoza M, Wang Y, Greenwood A, Cheng
KH, McLaughlin M, Brown, D. et al. (2005) Cancer Cell 8:185–195.31. Hingorani SR, Petricoin EF, Maitra A, Rajapakse V, King C, Jacobetz MA, Ross S, Conrads
TP, Veenstra TD, Hitt B, A. et al. (2003) Cancer Cell 4:437–450.32. Baeyens L, De Breuck S, Lardon J, Mfopou JK, Rooman I, Bouwens L (2005) Diabetologia 48:49–57.33. Lardon J, Huyens N, Rooman I, Bouwens L (2004) Virchows Arch 444:61–65.34. Lardon J, Bouwens L (2005) Differentiation 73:278–286.35. Gomez G, Lee HM, He Q, Englander EW, Uchida T, Greeley GH, Jr (2001) Exp Biol Med
(Maywood) 226:692–700.36. Rooman I, Lardon J, Flamez D, Schuit F, Bouwens L (2001) Gastroenterology 121:940–949.37. Chen Y, Chong MM, Darwiche R, Thomas HE, Kay TW (2004) Am J Pathol 165:913–921.38. Minami K, Okuno M, Miyawaki K, Okumachi A, Ishizaki K, Oyama K, Kawaguchi M, Ishizuka
N, Iwanaga T, Seino S (2005) Proc Natl Acad Sci USA 102:15116–15121.39. Paris M, Bernard-Kargar C, Berthault MF, Bouwens L, Ktorza A (2003) Endocrinology 144:2717–
2727.40. Waguri M, Yamamoto K, Miyagawa JI, Tochino Y, Yamamori K, Kajimoto Y, Nakajima H,
Watada H, Yoshiuchi I, Itoh N, et al. (1997) Diabetes 46:1281–1290.41. Wang RN, Kloppel G, Bouwens L (1995) Diabetologia 38:1405–1411.42. De Lisle RC, Grendell JH, Williams JA (1990) Pancreas 5:381–388.43. Gebhardt A, Ackermann W, Unver N, Elsasser HP (2004) Cell Tissue Res 315:321–329.44. Jensen JN, Cameron E, Garay MV, Starkey TW, Gianani R, Jensen J (2005) Gastroenterology
128:728–741.45. Pour PM, Weide L, Liu G, Kazakoff K, Scheetz M, Toshkov I, Ikematsu Y, Fienhold MA,
Sanger W (1997) Am J Pathol 150:2167–2180.46. Bonner-Weir S (2001) Diabetes 50(Suppl 1):S20–S24.47. Van Laethem JL, Marchant A, Delvaux A, Goldman M, Robberecht P, Velu T, Deviere J (1995)
Gastroenterology 108:1917–1922.48. Neuschwander-Tetri BA, Burton FR, Presti ME, Britton RS, Janney CG, Garvin PR, Brunt EM,
Galvin NJ, Poulos JE (2000) Dig Dis Sci 45:665–674.
4424 � www.pnas.org�cgi�doi�10.1073�pnas.0605248104 Strobel et al.
Dow
nloa
ded
by g
uest
on
Mar
ch 4
, 202
1