Embed Size (px)
Citation preview

Cell Injury, Adaptation & Death
Dr. Nabila Hamdi
MD, PhD

B5.114 [email protected]
Please visit • Internet: http://pbt.guc.edu.eg
• Intranet: \\ Faculties\ Pharmacy &Biotechnology\ Pharmacology & Toxicology/Pathology/Dr. Nabila

Course Structure
Assessment
Methods Weight
Quizzes (best 2 out of 3) 20%
Assignments 5%
Mid-term exam 30%
Final exam 45%
The midterm and final exams are computer based - case oriented
problems
6th semester
Dr. Ahmed Ihab PL1
Dr. Hend EL Tayebi PL2
Dr. Nabila Hamdi PL3
Pathology & Histology PHTX 621
Cell Injury Inflammation Tissue Healing & Repair Immune Disorders Neoplasia
Course content

How to study?
Lectures Tutorials
evelivesey.deviantart.com
Basic Science Cell, molecule
Clinical Practice Symptoms
Etiology
Pathogenesis
Pathology is the study of suffering
pathos logos
Why Pathology?

ILOs
• Describe the major mechanisms whereby most injurious agents exert their effects
• Understand the examples of cell injury stated in this lecture
• Describe cell changes that occur with atrophy, hypertrophy, hyperplasia, metaplasia, and dysplasia, and state general conditions under which these changes occur
• State and discuss patterns of reversible/irreversible cell injury
• Differentiate cell death associated with apoptosis and necrosis
• Compare the pathogenesis of dystrophic and metastatic calcifications
• Define intracellular accumulations and cite examples
• Understand the process of aging

Outline I. Causes of Cell Injury
II. Mechanisms of Cell Injury 1. General Biochemical Mechanisms
2. Ischemic & Hypoxic Injury
3. Ischemia/Reperfusion Injury
4. Free Radical-Induced Cell Injury
5. Chemical Injury
III. Cellular Adaptation to Injury 1. Atrophy
2. Hypertrophy
3. Hyperplasia
4. Metaplasia
5. Subcellular Responses to Injury
6. Intracellular Accumulations
7. Pathologic Calcification
III. Reversible/Irreversible Injury
IV. Apoptosis/Necrosis
V. Ageing


http://ww2.odu.edu/~czemlin/heartattacks.html

Causes of Cell Injury
Cell Injury
Oxygen Deprivation Hypoxia: low O2 cc Ischemia: reduced blood supply
Chemical Agents poisons, air pollutants, insecticides, CO, ethanol, therapeutic drugs…
Infectious Agents
Immunologic Reactions autoimmune reactions, allergic reactions…
Genetic Defects Hb S Sickle cell anemia Enzyme metabolic diseases
Nutritional Imbalances Protein-calorie insufficiency Vitamin deficiencies Obesity, animal fat…
Physical Agents Trauma, radiation, electric shock, extremes of temperatures…
Aging Cellular senescence
Viruses, rickettsiae, bacteria, fungi, protozoans and worms

Mechanisms of Cell Injury General Biochemical Mechanisms
Cell injury results from functional and biochemical abnormalities in one or more of several essential cellular components. The most important targets of injurious stimuli are (1) mitochondria, the sites of ATP generation; (2) cell membranes, on which the ionic and osmotic homeostasis of the cell and its organelles depends; (3) protein synthesis;
(4) the cytoskeleton; and (5) the genetic apparatus of the cell.

Mechanisms of Cell Injury ATP Depletion
Depletion of ATP to less than 5% to 10% of normal levels has widespread effects on many critical cellular systems

Mechanisms of Cell Injury Oxygen in Cell Injury
The critical role of oxygen in cell injury Ischemia causes cell injury by reducing cellular oxygen supplies,
whereas other stimuli, such as radiation, induce damage by toxic activated oxygen species
http://www.kaomp.org/new/board_view.htm?table_name=photo_0&currPage=13&aq_id=2&aq_type=&aq_value=

Mechanisms of Cell Injury Mitochondrial Damage

Mechanisms of Cell Injury Calcium Influx
ATP-dependent calcium transporters (Ischemia/Toxins)

Mechanisms of Cell Injury Defects in Membrane Permeability
The most important sites of membrane damage during cell injury are the mitochondrial membrane, the plasma membrane, and membranes of lysosomes.

Ischemic and Hypoxic Injury
Ischemia is the most common cause of cell injury in clinical medicine
Ischemia injures tissues faster than does hypoxia !
Why?
Anaerobic glycolysis (less efficient)
Anaerobic glycolysis No delivery of substrates
If oxygen is restored, all of these disturbances are reversible. If ischemia persists, irreversible injury and necrosis ensue.

Free Radical-Induced Injury
The Stance of Antioxidants in Brain Tumors By Pinar Atukeren and M. Ramazan Yigitoglu
Sources of reactive oxygen species in the human body
Antioxidant defense mechanisms (II): enzymatic mechanisms José A. Hernández Cortés. Research Scientist (CEBAS-CSIC)

Free Radical-Induced Injury
Cu2+/Fe2+
Endogenous or exogenous antioxidants (e.g., vitamins E, A, and C, and β-carotene)
Cell Injury. David S. Strayer Emanuel Rubin Copyright ©2009 Lippincott Williams & Wilkins

Ischemia/Reperfusion Injury
Oxygen paradox
ROS generation
Inflammation
Calcium Influx
Medicine, Mediators of Lethal Reperfusion Injury: the Oxygen Paradox, by Ernst
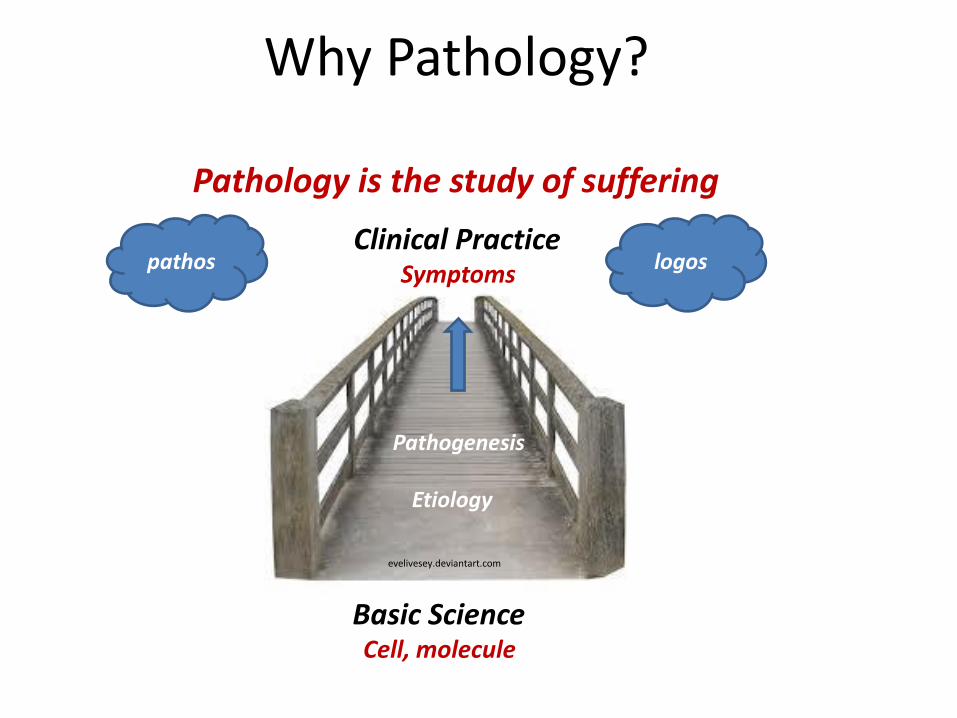
Chemical Injury
Some chemicals act directly • Mercuric chloride poisoning • Antineoplastic chemotherapeutic agents
Other chemicals must be first converted to reactive toxic metabolites • Carbon tetrachloride CCl4 CCl3
• Liver toxicity "fatty liver“ within 2 hours!
• Acetaminophen overdose Acute liver failure
Direct binding to critical molecular component or cellular organelle
Cellular Adaptation to Stress Atrophy
Shrinkage in the size of the cell by the loss of cell substance.
When a sufficient number of cells is involved, the entire tissue or organ diminishes in size, becoming atrophic.
Although atrophic cells may have diminished function, they are not dead.

Cellular Adaptation to Stress Atrophy
Aging (senile atrophy). Note that loss of brain substance narrows the gyri and widens the sulci. The meninges have been stripped from the right
half of each specimen to reveal the surface of the brain.
Loss of endocrine stimulation of the uterus after menopause
Physiologic Atrophy
Brain atrophy Uterus atrophy

Cellular Adaptation to Stress Atrophy
Loss of innervation
Pathologic Atrophy
A Practical Guide to Clinical Medicine, University of California, San Diego
Immobilization of a limb after fracture
source: http://soopastank.wordpress.com

Cellular Adaptation to Stress Atrophy
Pathologic Atrophy Inadequate nutrition
http://emedicine.medscape.com/article/932104-clinical
Dr. Drew on Angelina Jolie: ‘I see malnutrition’ Celebs, By Dan Schenek,
Diminished blood supply
Constriction of proximal portion of renal artery with ischemic atrophy of the involved kidney
http://www.pathology.vcu.edu/education/PathLab/pages/renalpath/rpsr/images/ras_sr/

Cellular Adaptation to Stress Hyperplasia
Hyperplasia is characterized by an increase in cell number.
Hyperplasia takes place if the cell population is capable of replication.
Hyperplasia can be physiologic or pathologic.

Cellular Adaptation to Stress Hyperplasia
Hormonal hyperplasia Compensatory hyperplasia
Female breast in puberty and pregnancy Liver regeneration after lobar resection
http://whydetox.net/liver-detoxification
Physiologic Hyperplasia
Growth and development of the breast during pregnancy. Ducts and glands undergo marked hyperplasia in preparation for lactation. Ductal proliferation is predominantly controlled by estrogen (E), whereas gland
differentiation is a progesterone (P) effect facilitated by estrogen.
The Breast During Pregnancy and Lactation, Julia V. Johnson and Daniel H. Riddick
Mitotic activity in the remaining cells begins as early as 12 hours later, eventually restoring the liver to its normal weight

Cellular Adaptation to Stress Hyperplasia
Pathologic Hyperplasia
Hyperplasia of the endometrium
Excessive hormonal stimulation
(leads to abnormal menstrual bleeding)
To distinguish from the physiologic hyperplasia during a normal menstrual cycle !!

Cellular Adaptation to Stress Hyperplasia
A. Normal epidermis. B. Epidermal hyperplasia in psoriasis, shown at the same magnification as in A. The epidermis is thickened, owing to an increase in the number of squamous cells.
Cell Injury. David S. Strayer Emanuel Rubin Copyright ©2009 Lippincott Williams & Wilkins
Pathologic Hyperplasia
Epidermal hyperplasia Papillomaviruses cause skin warts
(Virus-induced growth factor stimulation)

Cellular Adaptation to Stress Hypertrophy
Hypertrophy is an increase in the size of cells resulting in increase in the size of the organ.
There are no new cells, just bigger cells, enlarged by an increased amount of structural proteins and organelles.
Hypertrophy can be physiologic or pathologic and is caused either by increased functional demand or by specific hormonal stimulation.
Occurs when cells are incapable of dividing (heart & skeletal muscle)

Cellular Adaptation to Stress Hypertrophy
Myocardial hypertrophy Cross-section of the heart of a patient with long-standing hypertension
shows pronounced, concentric left ventricular hypertrophy.
Cell Injury. David S. Strayer Emanuel Rubin Copyright ©2009 Lippincott Williams & Wilkins
http://aminoacidstudies.org/muscle-growth/
Skeletal muscle hypertrophy (after weightlifting)
Physiologic Hypertrophy Pathologic Hypertrophy

Cellular Adaptation to Stress Hypertrophy + Hyperplasia
The massive physiologic enlargement of the uterus during pregnancy occurs as a consequence of estrogen-stimulated smooth muscle hypertrophy and smooth muscle hyperplasia
Gravid uterus

Cellular Adaptation to Stress Metaplasia
Metaplasia is a reversible change in which one adult cell type (epithelial or mesenchymal) is replaced by another adult cell type.
Cells sensitive to a particular stress are replaced by other cell types better able to withstand the adverse environment.
Cellular Adaptation to Stress Metaplasia
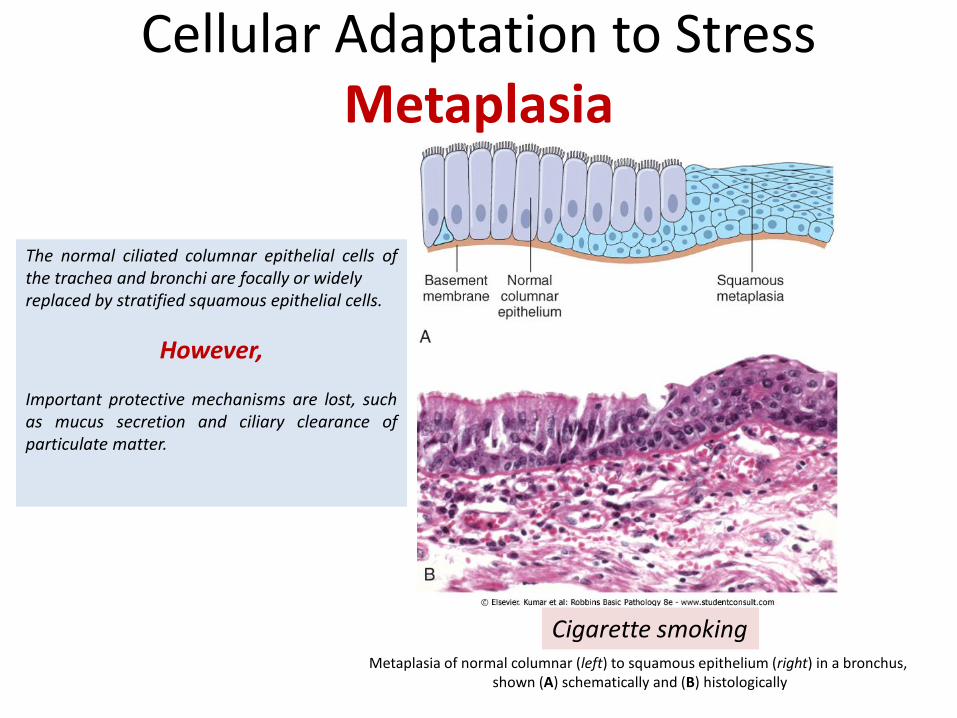
The normal ciliated columnar epithelial cells of the trachea and bronchi are focally or widely replaced by stratified squamous epithelial cells.
However, Important protective mechanisms are lost, such as mucus secretion and ciliary clearance of particulate matter.
Metaplasia of normal columnar (left) to squamous epithelium (right) in a bronchus, shown (A) schematically and (B) histologically
Cigarette smoking

Cellular Adaptation to Stress Metaplasia
Gastroesophageal reflux disease (GERD)
Stuart Jon Spechler, JAMA, August 14, 2013, Vol 310, No. 6

Atrophy, hypertrophy, hyperplasia and metaplasia are reversible changes!

Subcellular Response to Injury
Lysosomal Catabolism
Lipofuscin

Intracellular Accumulations
• Fats (fatty liver)
• Cholesterol and cholesterol esters (foam cells in atherosclerosis)
• Glycogen (diabetes mellitus or glycogen storage
diseases)
• Pigments
- Exogenous: carbon (an example is coal dust)
- Endogenous: lipofuscin ("wear-and-tear pigment“)
Figure: Mechanisms of intracellular accumulation. (1) Abnormal metabolism, as in fatty change in the liver. (2) Mutations causing alterations in protein folding and transport, so that defective molecules accumulate intracellularly. (3) A deficiency of critical enzymes responsible for breaking down certain compounds, causing substrates to accumulate in lysosomes, as in lysosomal storage diseases. (4) An inability to degrade phagocytosed particles, as in carbon pigment accumulation.

Intracellular Accumulations
Fatty liver (Steatosis)
A, The possible mechanisms leading to accumulation of triglycerides in fatty liver. Defects in any of the steps of uptake, catabolism, or secretion can lead to lipid accumulation. B, High-power detail of fatty change of the liver. In most cells the well-preserved nucleus is squeezed into the displaced rim of cytoplasm about the fat vacuole. (Courtesy of Dr. James Crawford, Department of Pathology, University of Florida School of Medicine, Gainesville, Florida.)
Alcohol
CCl4
Malnutrition

Pathologic Calcification Dystrophic
Calcification of the aortic valve (important cause of aortic stenosis in the elderly)
A view looking down onto the unopened aortic valve in a heart with calcific aortic stenosis
Dystrophic calcification is the abnormal deposition of calcium salts in dead or dying tissues, in the absence of calcium metabolic derangements

Pathologic Calcification Metastatic
Increased secretion of PTH (primary parathyroid tumors or production of PTH-related
protein by other malignant tumors)
Destruction of bone (accelerated turnover, immobilization, tumors)
Vitamin D-related disorders (vitamin D intoxication)
Renal failure (phosphate retention leads to secondary hyperparathyroidism)
Hypercalcemia
deposition in normal tissues
Metastatic calcification is the deposition of calcium salts in normal tissues and almost always reflects some derangement in calcium metabolism

Reversible &Irreversible Cell Injury

Pattern of Tissue Necrosis Coagulative Necrosis
• Coagulative necrosis is a form of tissue necrosis in which the component cells are dead but the basic tissue architecture is preserved for at least several days.
• It is characteristic of infarcts (areas of ischemic necrosis) in all solid organs except the brain.
A, A wedge-shaped kidney infarct (yellow) with preservation of the outlines. B, Microscopic view of the edge of the infarct, with normal kidney (N) and necrotic cells in the infarct (I). The necrotic cells show preserved outlines with loss of nuclei, and an inflammatory infiltrate is
present (difficult to discern at this magnification).

Pattern of Tissue Necrosis Liquefactive Necrosis
• Liquefactive necrosis is seen in focal bacterial or, occasionally, fungal infections.
• Occurs in hypoxic death of cells within the central nervous system (obscure reasons?)
• liquefaction completely digests the dead cells, resulting in transformation of the tissue into a liquid viscous mass (inflammatory cells)
Liquefactive necrosis: An infarct in the brain, showing dissolution of the tissue.

Pattern of Tissue Necrosis Caseous Necrosis
Caseous necrosis is encountered most often in foci of tuberculous infection. The term "caseous" (cheese-like) is derived from the friable yellow-white appearance of the area of necrosis.
A tuberculous lung with a large area of caseous necrosis containing yellow-white and cheesy debris
Pattern of Tissue Necrosis Fat Necrosis
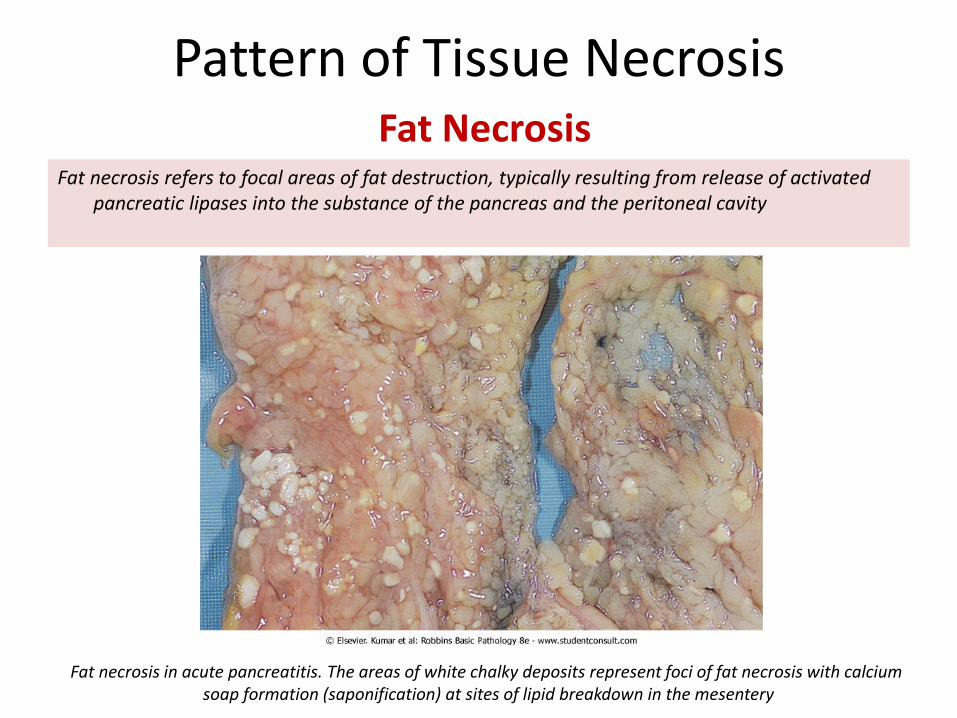
Fat necrosis refers to focal areas of fat destruction, typically resulting from release of activated pancreatic lipases into the substance of the pancreas and the peritoneal cavity
Fat necrosis in acute pancreatitis. The areas of white chalky deposits represent foci of fat necrosis with calcium soap formation (saponification) at sites of lipid breakdown in the mesentery

Pattern of Tissue Necrosis Gangrenous Necrosis
It is usually applied to a limb, generally the lower leg, that has lost its blood supply and has
undergone coagulative necrosis. When bacterial infection is superimposed, coagulative necrosis
is modified by the liquefactive action of the bacteria and the attracted leukocytes.
The affected skin is dark red to black and there is a large area of ulceration. (amputated diabetic leg)
http://studentbsmu.blogspot.com/2011/11/gangrenous-necrosis-lower-limb.html

Apoptosis Apoptosis is a pathway of cell death that is induced by a tightly regulated suicide program in which cells destined to die activate enzymes capable of degrading the cells' own nuclear DNA and nuclear and cytoplasmic proteins. Fragments of the apoptotic cells then break off, giving the appearance that is responsible for the name (apoptosis, "falling off")
Physiologic eliminates cells that are no longer needed • Destruction of cells during embryogenesis • Endometrial cell breakdown during the menstrual cycle • Regression of the lactating breast after weaning • Neutrophils in an acute inflammatory response • Lymphocytes at the end of an immune response
Pathologic eliminates cells that are genetically altered or injured beyond repair • DNA damage: Radiation, cytotoxic anticancer
drugs, extremes of temperature (via TP53) • Accumulation of misfolded proteins • Cell injury in certain infections • Pathologic atrophy

Necrosis/Apoptosis
(a) SEM of an apoptotic cell, 5000 × magnification (b) SEM of a necrotic cell, 5000 × magnification
Reprinted from the Purdue CDROM Vol 4, Purdue University with permission. Publisher: J. Paul Robinson

Necrosis/Apoptosis
Apoptosis: a critical process in homeostasis, Research Apoptosis http://www.biooncology.com/research-education/apoptosis/introduction/critical

Aging
Telomeres are short repeated sequences of DNA present at the linear ends of chromosomes that are important for ensuring the complete replication of chromosome ends and for protecting the ends from fusion and degradation. When somatic cells replicate, a small section of the telomere is not duplicated, and telomeres become progressively shortened. The ends of chromosomes cannot be protected and are seen as broken DNA, which signals cell cycle arrest. The lengths of the telomeres are normally maintained by nucleotide addition mediated by an enzyme called telomerase.

References
ROBBINS Basic Pathology 8th Edition Basic Pathology 7th Edition, by Kumar, Cotran and Robbins Source of the cover cell image http://timothyjoseph.net/kill-or-be-killed/